recurrent stroke prevention: y an update on the. aspirin plus extended-release dipyridamole c....
TRANSCRIPT

1
Recurrent Stroke Prevention: An Update on the
Evidence and Opportunity in Ischemic Stroke or TIAIschemic Stroke or TIA
Case-Based Review of Guidelines forPractitioners Who Care for Patients With
Ischemic Stroke or TIA
Impact of Stroke in the United StatesOf all CVDs, stroke is the third leading cause of death Annual incidence– 780,000 strokes
600,000 first attacks180,000 recurrent attacks
1 % f k h ld d b TIA15% of strokes are heralded by TIAOne-third of TIAs may be considered cerebral infarctions based on diffusion-weighted MRI results90-day risk of stroke after TIA: 3%–17% – Highest risk within the first 30 days
American Heart Association. Heart Disease and Stroke Statistics–2008 Update. Dallas, Texas: American Heart Association; 2008 Rosamond W et al. Circulation. 2008;117(4);e25
CVD = cardiovascular disease; MRI = magnetic resonance imaging
Estimates of the Cost of Stroke
Average cost of ischemic stroke within 30 days
• $13,019 (mild)• $20,346 (severe)
Mean lifetime costof ischemic stroke
• $140,048
$65.5 billion* in 2008*Estimated direct and indirect costs American Heart Association. Heart Disease and Stroke Statistics–2008 Update. Dallas, Texas: American Heart Association; 2008; Rosamond W et al. Circulation. 2008;117(4);e25
Estimates of Long-term Risk of Stroke After Ischemic Stroke or TIA
Percentage of Patients Experiencing Stroke
TimeAfter TIA1
(%)After Stroke2
(%)
30 days 4–8 3–10
1. Feinberg WM et al. Stroke. 1994;25(6):13202. Sacco RL. Neurology. 1997;49(5 suppl 4):S39
30 days 4 8 3 10
1 year 12–13 10–14
5 years 24–29 25–40
Putative Risk Factors for Stroke RecurrenceEarly stroke recurrence
Stroke subtype– High for large artery, extra- and intracranial occlusive disease
Elevated blood glucoseHTN
kLate stroke recurrence Age HTNHeart disease (CHD, HF, AF) DM and hyperglycemia
Prior stroke or TIA
Sacco RL et al. Neurology. 1999;53(7 suppl 4):S15
AF = atrial fibrillation; CHD = coronary heart disease; DM = diabetes mellitus; HF = heart failure; HTN = hypertension
Defining Stroke Subtype Is an Important Consideration in Recurrent Stroke Prevention
Hemorrhagic stroke12%Other
5%
Cryptogenic30% Atherosclerotic
cerebrovascular
Ischemic stroke88%
Cardiogenicembolism
20%
Small vesseldisease
“lacunae”25%
cerebrovasculardisease
20%
Albers GW et al. Chest. 2004;126(3 suppl):438S Thom T et al. Circulation. 2006;113(6):e85

2
Prevention of Recurrent Stroke
Evaluation for risk factors– HTN, DM, hyperlipidemia
Evaluation for cause– Arterial diseases, heart diseases– Coagulopathies
Management of risk factors– Lifestyle and medications
Antithrombotic therapySurgical or endovascular interventions
Sacco RL et al. Stroke. 2006;37(2):577
Case PresentationCase Presentation
65-Year-Old Woman With 15-Year History of HTN
Chief complaint– Presented to the ED after a 30-minute spell of
transient right-sided face and arm weakness after exercising today
Past medical history– HTN ×15 years
Medications – HCTZ 25 mg once daily
ED = emergency department; HCTZ = hydrochlorothiazide
65-Year-Old Woman With 15-Year History of HTN
Physical exam – BP 149/95 mm Hg; HR 80 BPM and regular– Neurologic examination normal except for slight
weakness of the right arm and leg (NIH Stroke Scale score = 2)( )
Laboratory examination– Total cholesterol = 230 mg/dL– LDL-C = 120 mg/dL– HDL-C = 39 mg/dL – Other laboratory tests unremarkable
BP = blood pressure; BPM = beats/minute; HDL-C = high-density lipoprotein cholesterol; HR = heart rate; LDL-C = low-density lipoprotein cholesterol; NIH = National Institutes of Health
65-Year-Old Woman With 15-Year History of HTN
Diagnostic studies– EKG normal– Transthoracic echocardiography showed LVH– MRA of the head and neck was unremarkable– MRI of the head
EKG = electrocardiogram LVH = left ventricular hypertrophy MRA = magnetic resonance angiography
MRI Diffusion-Weighted Imaging (DWI)
LeftRight

3
65-Year-Old Woman With 15-Year History of HTN
Diagnostic studies– EKG is normal– Transthoracic echocardiography showed LVH– MRA of the head and neck was unremarkable– MRI of head shows DWI abnormality
predominantly of left posterior limb of internal capsule consistent with ischemic injury
Guidelines for Management of TIAGuidelines for Management of TIA
Johnston SC et al. Ann Neurol. 2006;60(3):301
Definitions of Classes and Levels of Evidence: AHA/ASA 2006 Stroke Prevention Guidelines
Class I Evidence or general agreement that procedure or treatment is useful and effective
Class II Conflicting evidence or divergence of opinion of usefulness/efficacy
Class IIa Weight of evidence or opinion is in favor
Class IIb Usefulness/efficacy is less well established by evidence or opinion
Class III Evidence and/or general opinion that usefulness/effectiveness does not exist and may be harmful
LOE A Derived from multiple RCTs
LOE B Derived from a single RCT or nonrandomized studies
LOE C Expert opinion or case series
Sacco RL et al. Stroke. 2006;37(2):577
AHA/ASA = American Heart Association/American Stroke Association RCT = randomized clinical trial LOE = level of evidence
Recent TIA: A Neurologic Emergency
Risk of stroke after TIA – 10.5% occurred within 90 days and half occurred within
2 days (Kaiser-Permanente HMO study)
Risks may have been previously underestimated1% 2% at 7 days and 2% 4% at 30 days– 1%─2% at 7 days and 2%─4% at 30 days
True risk– Up to 10% at 7 days and as high as 15% at 30 days
Time window for prevention is brief– 17% of TIAs occur on the day of stroke– 43% during the 7 days prior to stroke
Rothwell PM. Nat Clin Pract Neurol. 2006;2(4):174
Predicting Risk of Stroke After TIA:ABCD2 Score for 2- or 7-Day Risk of Stroke
A Age ≥60 years 1 point
B Blood pressure SBP >140 mm Hg or DBP ≥90 mm Hg 1 point
C Clinical featuresUnilateral weakness 2 pointsSpeech disturbance without
k 1 point
Johnston SC et al. Lancet. 2007;369(9558):283 Rothwell PM et al. Lancet. 2005;366(9479):29
weakness p
D Duration of symptoms
≥60 minutes 2 points10–59 minutes 1 point
D Diabetes Diabetes 1 point
Maximum score 7 points
DBP = diastolic blood pressure; SBP = systolic blood pressure

4
ABCD2 Is Predictive of 2-Day Risk of Stroke in Patients With TIA
ABCD2 Score Level of Risk2-Day Stroke Risk
(%)
6–7 High 8.1
Johnston SC et al. Lancet. 2007;369(9558):283
g
4–5 Moderate 4.1
0–3 Low 1.0
Traditional TIA Symptoms and Signs*: Carotid Territory (1974)
Symptom Sign
1. Motor dysfunction Weakness, clumsiness, paralysis of 1 or both limbs on same side
2. SensoryNumbness, loss of sensation, and paresthesias of 1 or both limbs on same side; without spread or marchside; without spread or march
3. Speech/language Aphasia4. Vision Loss in 1 eye or part of 1 eye5. Vision Homonymous hemianopia6. Multiple Combination of above
Heyman A et al. Stroke.1974;5:277
*Symptoms/sign can last up to 24 hours
TIA: New Definition Is Proposed (2002)Definition
Brief episode of neurologic dysfunction caused by focal brain or retinal ischemiaClinical symptoms typically lasting less than 1 hourNo evidence of cerebral infarction (using advanced neuroimaging techniques)q )Urgent brain imaging is recommended
Albers GW et al. N Engl J Med. 2002;347(21):1713
Rationale• Traditional definition is out of date and no longer consistent with current
concepts of brain ischemia• Most TIAs are short lived, and advanced imaging techniques may show
cerebral ischemic injury
National Stroke Association (NSA) Guidelines for the Management of TIAs
Factor CommentHospitalization • Consider within 24–48 hours of first TIA
• Timely hospital referral of recent (within 1 week) TIA and hospital admission is generally recommended in the case of crescendo TIAs, symptoms longer than 1 hour, symptomatic carotid stenosis >50%, known cardiac-source embolism, hypercoagulable state, or appropriate California or ABCD score
• Hospitals/practitioners should have local admission policy and referral policy for specialists’ assessments
• Local written protocols for diagnostic testingLocal written protocols for diagnostic testing
Clinical evaluation • Specialized clinic for rapid assessment and evaluation within 24–48 hours
Timing of initial assessment
• For recent TIA, need same-day access to imaging such as CT/CTA, MRI/A, and/or CUS
• If not admitted to hospital, rapid (within 12 hours) access to urgent assessment and investigation
• If TIA occurred in past 2 weeks and the patient was not hospitalized, prompt (24–48 hour) investigations (CUS, blood work, EKG, echocardiogram) needed
Johnston SC et al. Ann Neurol. 2006;60(3):301
CT/CTA = computed tomography/computed tomographic angiography CUS = carotid ultrasound
NSA Guidelines for the Management of TIAs: Evaluation
Factor Comment
General EKG, CBC, serum electrolytes, creatinine, fasting blood glucose, lipids
Brain imaging CT/CTA or MRI/A; TCD is complementary
Doppler ultrasound; CTA and/or MRA for supra-aortic
Carotid imaging
pp ; pvessels if Doppler not reliable or CEA considered; conventional angiogram if Doppler and MRA/CTA discordant or not feasible
Cardiac evaluation
TTE or TEE in patients younger than 45 years when neck, brain, and hematology studies negative for cause
Johnston SC et al. Ann Neurol. 2006;60(3):312
CBC = complete blood countCEA = carotid endarterectomyTCD = transcranial Doppler TEE = transesophageal echocardiogramTTE = transthoracic echocardiogram
Medical and Surgical Management of TIAs
NSA and AHA/ASA guidelines for use of antithrombotic therapies, CEA, EC-IC bypass, and medical risk-factor modification for TIA patients are comparable
These prevention strategies in TIA and ischemic stroke patients plus angioplasty and stenting are reviewed in subsequent sections of this activity according to 2006 and 2008 AHA/ASA guidelines
Johnston SC et al. Ann Neurol. 2006;60(3):301Sacco RL et al. Stroke. 2006:37(2):577 Adams RJ et al. Stroke. 2008;39(5);1647
EC-IC = extracranial-intracranial
5
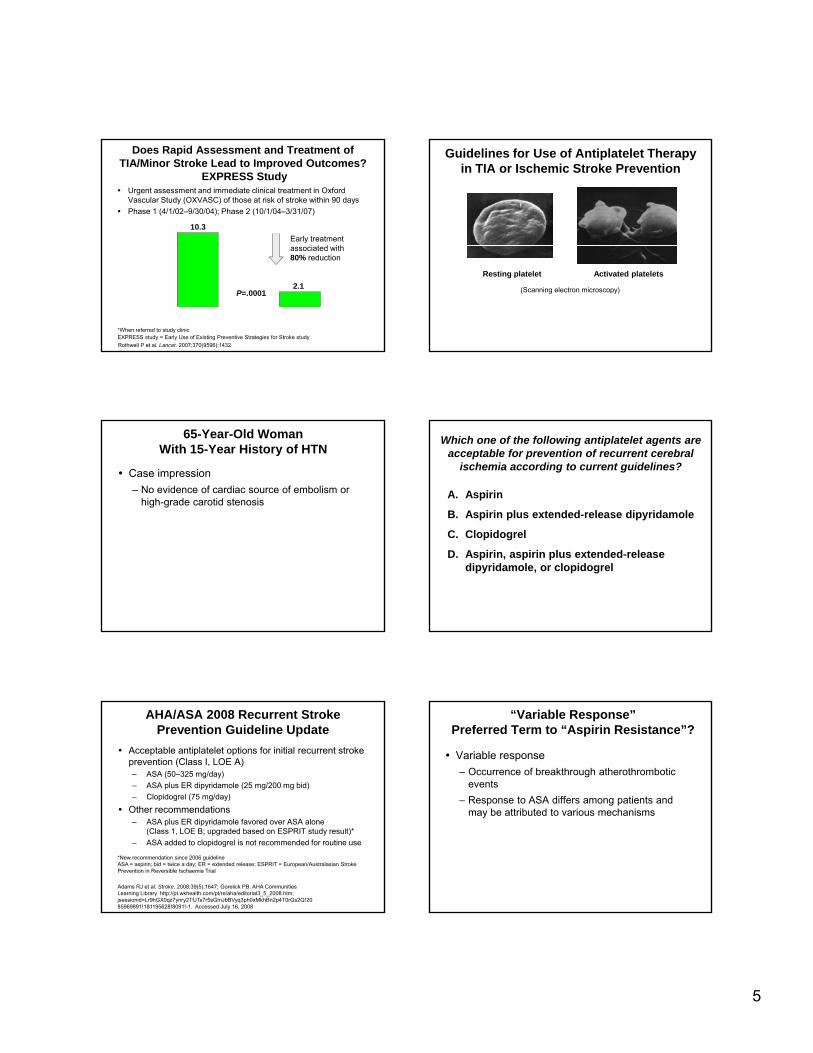
Does Rapid Assessment and Treatment of TIA/Minor Stroke Lead to Improved Outcomes?
EXPRESS StudyUrgent assessment and immediate clinical treatment in Oxford Vascular Study (OXVASC) of those at risk of stroke within 90 daysPhase 1 (4/1/02–9/30/04); Phase 2 (10/1/04–3/31/07)
10
12
Stro
ke* (
%)
10.3Early treatment
i t d ith
Rothwell P et al. Lancet. 2007;370(9596):1432
0
2
4
6
8
Phase 1 Phase 290-D
ay R
isk
of R
ecur
rent
S
2.1P=.0001
*When referred to study clinic EXPRESS study = Early Use of Existing Preventive Strategies for Stroke study
associated with 80% reduction
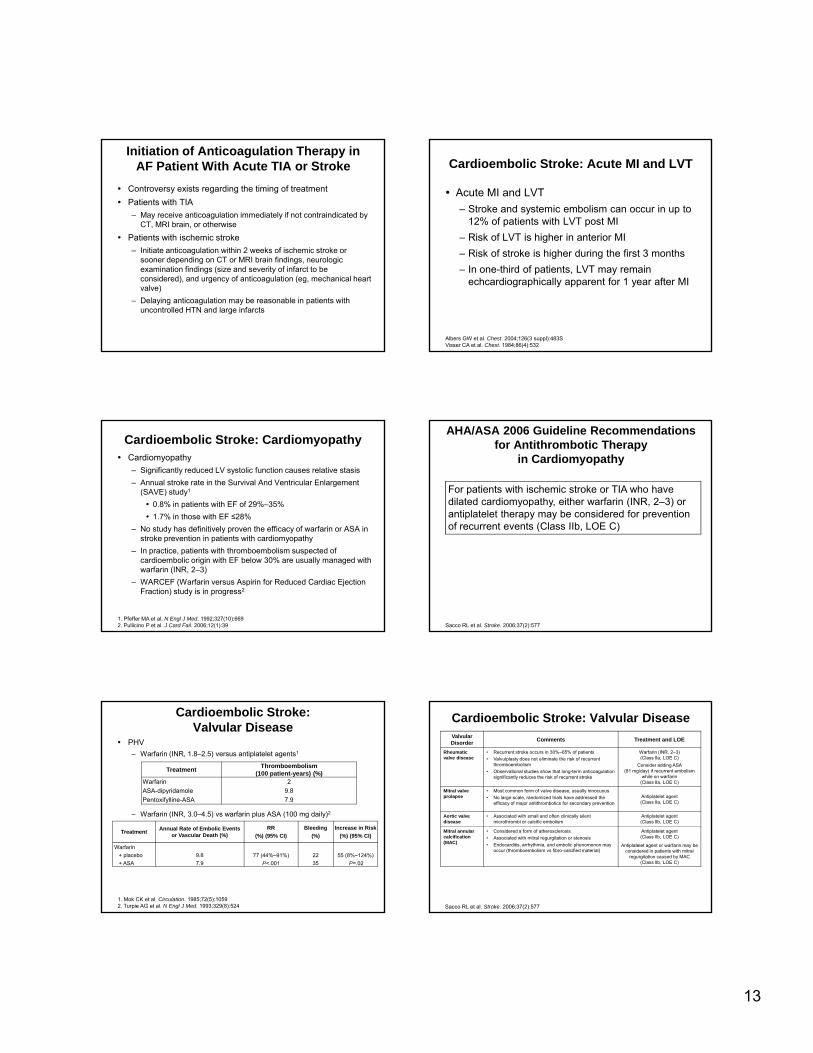
Guidelines for Use of Antiplatelet Therapy in TIA or Ischemic Stroke Prevention
Resting platelet Activated platelets
(Scanning electron microscopy)
65-Year-Old Woman With 15-Year History of HTN
Case impression– No evidence of cardiac source of embolism or
high-grade carotid stenosis
Which one of the following antiplatelet agents are acceptable for prevention of recurrent cerebral
ischemia according to current guidelines?
A. Aspirin
B. Aspirin plus extended-release dipyridamole
C. Clopidogrel
D. Aspirin, aspirin plus extended-release dipyridamole, or clopidogrel
AHA/ASA 2008 Recurrent Stroke Prevention Guideline Update
Acceptable antiplatelet options for initial recurrent stroke prevention (Class I, LOE A)– ASA (50–325 mg/day) – ASA plus ER dipyridamole (25 mg/200 mg bid)– Clopidogrel (75 mg/day)
Oth d tiOther recommendations– ASA plus ER dipyridamole favored over ASA alone
(Class 1, LOE B; upgraded based on ESPRIT study result)* – ASA added to clopidogrel is not recommended for routine use
Adams RJ et al. Stroke. 2008;39(5);1647; Gorelick PB. AHA Communities Learning Library. http://pt.wkhealth.com/pt/re/aha/editorial3_5_2008.htm; jsessionid=Lr9hGX0qz7ynry2TfJTs7r5sGmJbBVyq3ph0xMkhBn2p4T0rGs2Q!2085969891!181195628!8091!-1. Accessed July 16, 2008
*New recommendation since 2006 guidelineASA = aspirin; bid = twice a day; ER = extended release; ESPRIT = European/Australasian Stroke Prevention in Reversible Ischaemia Trial
“Variable Response”Preferred Term to “Aspirin Resistance”?
Variable response– Occurrence of breakthrough atherothrombotic
events– Response to ASA differs among patients and
may be attributed to various mechanisms

6
Cellular factorsInsufficient suppression
of COX-1Overexpression of COX-2 mRNA
Erythrocyte-induced platelet activation
Genetic polymorphisms
COX-1GP IIIa receptor
Collagen receptor
Clinical factorsFailure to prescribe
NoncomplianceNonabsorption
Interaction with ibuprofen
Aspirin Resistance: More Than Just a Laboratory Curiosity?
ASA resistance
platelet activationIncreased norepinephrineGeneration of 8-iso-PGF2α
Adapted with permission from Bhatt DL. J Am Coll Cardiol. 2004;43(6):1127
Collagen receptorvWF receptor
Interaction with ibuprofenInteraction with naproxen
COX = cyclo-oxygenase; GP = glycoprotein; mRNA = messenger ribonucleic acid; PGF2α = prostaglandin F2 alpha; vWF = von Willebrand factor
Study population 20,333 patients with recent stroke (within 90 days of study entry)
Study drugs ASA/ER dipyridamole vs clopidogrel and telmisartan vs placebo
Study design Multinational (more than 21 countries and 600 sites), randomized, double-blind, placebo-controlled, 2 x 2 factorial design
PRoFESS Trial
telmisartan vs placeboPrimary end point Time to first recurrent stroke
Anticipated data 2008
Secondary end point Stroke, MI, or vascular death; major bleeding; stroke or major hemorrhage
Diener HC et al. Cerebrovasc Dis. 2007;23:368
MI = myocardial infarction; PRoFESS = Prevention Regimen For Effectively Avoiding Second Strokes
PRoFESS Trial: Preliminary ResultsPrimary end point– Across an average observation time of 2.5 years, rates of first
recurrent stroke were similar (9.0% ASA + ER dipyridamole vs 8.8% clopidogrel; HR 1.01, 95% CI 0.92−1.11)
Bleeding – More frequent in ASA + ER dipyridamole group
Boehringer Ingelheim. News Release. PRoFESS® results announced at XVII European Stroke Conference. http://www.boehringer-ingelheim.com/corporate/news/press_releases/detail.asp?ID=5534. Accessed August 12, 2008
More frequent in ASA ER dipyridamole group (major hemorrhagic events: 4.1% vs 3.6%; HR 1.15, 95% CI 1.00−1.32, P=.06)
Benefit-risk ratio– Similar between groups (11.7% ASA + ER dipyridamole vs
11.4% clopidogrel; HR 1.03, 95% CI 0.95−1.11, P=.50)
CI = confidence interval; HR = hazard ratio
Guidelines for Medical Risk Factor Management in Patients With g
TIA or Ischemic Stroke
65-Year-Old Woman With 15-Year History of HTN
Diagnosis– Patient was diagnosed with a lacunar or small artery
territory infarction syndrome
Treatment– She did not receive intravenous tPA therapy since she had
only a very minor neurologic impairment– After the MRI head study was reviewed in the ED, she was
treated with ASA 81 mg/day– Her BP was initially not treated
Within 48 hours of the neurologic symptoms, her neurologic examination was normal
tPA = tissue plasminogen activator
When it is deemed safe to lower BP following the initial phase of acute ischemic stroke, what is
the long-term target BP?
A. <140/90 mm Hg
B. <130/80 mm Hg
C. <120/70 mm Hg
D. <110/75 mm Hg

7
Which one of the following statements best characterizes the use of statin therapy for
recurrent stroke prevention?
A. There is no proof that statin therapy reduces stroke risk
B. Statin therapy reduces stroke risk, but is not py ,safe; fatal liver disease is common
C. Statin therapy reduces stroke and major cardiovascular risks
D. Statin therapy reduces stroke risk, but does not reduce major cardiovascular risks
Which one of the following statements best characterizes smoking as a
risk factor for stroke?
A. Environmental (passive) smoke increases the risk of stroke
B. Smoking is a risk factor for ischemic, but not g ,hemorrhagic stroke
C. Smoking increases the relative risk of stroke by 5 to 10 times
D. Smoking cessation leads to reversal of stroke risk after 20 years
Statin therapy and lipid lowering– Based on the SPARCL results, statin therapy with intensive lipid-
lowering effects is indicated for patients with LDL-C in the 100–190 mg/dL range, atherosclerotic ischemic stroke or TIA, and no known CHD to reduce occurrence of stroke and vascular events (Class I, LOE B)*
AHA/ASA 2008 Recurrent Stroke Prevention Guideline Update
– Target goal for cholesterol lowering for those with CHD or symptomatic atherosclerotic disease
LDL-C level of <100 mg/dL or LDL-C <70 mg/dL for very high-risk persons (those with multiple risk factors)
*New recommendation since 2006 guidelineSPARCL = Stroke Prevention by Aggressive Reduction in Cholesterol Levels trial
Adams RJ et al. Stroke. 2008;39(5);1647; Gorelick PB. AHA Communities Learning Library. http://pt.wkhealth.com/pt/re/aha/editorial3_5_2008.htm;jsessionid=Lr9hGX0qz7ynry2TfJTs7r5sGmJbBVyq3ph0xMkhBn2p4T0rGs2Q!2085969891!181195628!8091!-1. Accessed July 16, 2008
AHA/ASA 2006 Recommendations for Lifestyle and Risk Factor Management in TIA or Ischemic Stroke
Factor Recommendation LOE
HTN Initiate Rx when safe; individualize Rx; consider BP reduction of 10/5 mm Hg with a diuretic and ACEI Class I, LOE A
DM Rigorous control of BP and lipids; aim for hemoglobin A1c ≤7%
Class I, LOE AClass IIa, LOE B
SmokingDiscontinue smokingCounseling, NRT, and oral smoking-cessation medications
Class I, LOE CClass IIa, LOE Bmedications
Alcohol useEliminate heavy drinking or reduceMen ≤2 drinks/day and non-pregnant women 1 drink/day
Class I, LOE AClass IIb, LOE C
Obesity Goal BMI 18.5 to 24.9 kg/m2 and waist circumference women (<35 inches) and men (<40 inches) Class IIb, LOE C
Physical activity If capable, at least 30 minutes of moderate-intensity exercise daily Class IIb, LOE C
ACEI = angiotensin-converting enzyme inhibitor; BMI = body mass index; NRT = nicotine replacement therapy; Rx = treatment
Sacco RL et al. Stroke. 2006:37(2):577
Improving Patient AdherenceImproving Patient Adherence
Established Therapies Are Consistently Underused in all Patient Types
46
39
3024
44
36
2830
40
50
60
s N
ot R
ecei
ving
en
The
rapy
(%)
Antiplatelets Lipid lowering Statin
Bhatt DL et al. JAMA. 2006;295(2):180
1418 1819 19
0
10
20
CAD (n=40,258)
CVD(n=18,843)
PAD (n=8273)
Multiple Risk Factors (n=12,389)
Patie
nts
Prov
e
CAD = coronary artery disease; PAD = peripheral artery disease

8
65-Year-Old Woman With 15-Year History of HTN
Patient is now taking a diuretic, ACEI, statin, and ASA plus ER dipyridamole for recurrent stroke prevention
What steps might be taken to assure adherence to the treatment regimen?
Steps to Consider to Enhance Adherence to TIA or Recurrent Stroke Prevention Regimen
Awareness or recognition of stroke risk and risk factorsQualitative determination of recurrent stroke riskAwareness of risk factor numbers (eg, BP, blood ( gglucose, serum cholesterol)Establish multimodality maintenance approach
American Stroke Association broadcast on Primary Stroke Prevention, October 2007
Recurrent Stroke PreventionSuccessful Maintenance of Treatment by
Multimodality Approach
Motivation from family members Reminders and encouragement from medical office staff Pharmacy reminders to renew medicationsPharmacy reminders to renew medicationsPhysician report cards: Is the patient meeting target numbers?
American Stroke Association broadcast on Primary Stroke Prevention, October 2007
What Can Stroke Teams Do?
In-hospital initiation of secondary prevention therapies to increase treatment utilization and adherence in the long term Adopt a systematic management approach in coordination with primary care physicians to help optimize post-stroke care
Ovbiagele B et al. Neurology. 2004;63(7):1217; Ovbiagele B et al. Stroke. 2004;35(12):2879; Ovbiagele B et al. Stroke. 2008;39(6):1850
Cardioembolic Stroke ManagementCardioembolic Stroke Management
65-Year-Old Woman With 15-Year History of HTN
On physical examination, the patient’s pulse is noted to be irregularly irregular. A bedside EKG is ordered
Patient is diagnosed with cardioembolic stroke secondary to AF

9
Which one of the following therapies is recommended to prevent stroke recurrence for
a high-risk patient with atrial fibrillation?
A. Aspirin
B. Clopidogrel
C. Ximelagatran
D. Warfarin
Secondary Stroke Prevention:Cardioembolic Stroke
Cardioembolic stroke is responsible for ~20% of ischemic strokesHigh risk of recurrence if not treated properlyUnderlying cardiac disease*– Nonvalvular AF (50%)– LVT (33%)– Valvular heart disease (25%)– Cardiomyopathy with low EF (25%)
Cerebral Embolism Task Force. Arch Neurol. 1989;46(7):727Pujadas Capmany R et al. Int J Cardiol. 2004;95(2-3):129
*Patients may have more than 1 underlying cardiac conditionEF = ejection fraction; LVT = left ventricular thrombus
Risk factors for recurrent stroke in patients with AF
Age
Cardioembolic Stroke: AF
Persistent and paroxysmal AF are potent risk factors for recurrent stroke
CHFHTNDM
Prior thromboembolism (TIA or stroke)
CHF = congestive heart failure
Outcome Warfarin (INR goal of 2–3) Antiplatelet agents
Stroke reduction (%) 64 (95% CI 49-74%) 22 (95% CI 6-35%)NNT for 1 year for secondary stroke prevention (n) 14 34
Warfarin1
Anticoagulation
Ximelagatran (investigational)Ximelagatran (investigational)– Oral direct thrombin inhibitor that does not require coagulation
monitoring – SPORTIF-V: 36 mg twice daily was not inferior to warfarin (INR,
2–3) for stroke prevention in AF2
– Potential risk of hepatotoxicity– Not approved by FDA for use
1. Hart RG et al. Ann Intern Med. 2007;146(12):8572. Albers GW et al. JAMA. 2005;293(6);690
FDA = US Food and Drug Administration; INR = international normalized ratio; SPORTIF-V = Stroke Prevention Using Oral Thrombin Inhibitor in Atrial Fibrillation V
1. For patients with ischemic stroke or TIA with persistent or paroxysmal (intermittent) AF, anticoagulation with adjusted-dose warfarin (target INR, 2.5; range, 2–3) is recommended (Class I LOE A)
AHA/ASA 2006 Guideline Recommendationsfor Antithrombotic Therapy in AF
(Class I, LOE A)
2. For patients unable to take oral anticoagulants, ASA 325 mg/day is recommended (Class I, LOE A)
Sacco RL et al. Stroke. 2006;37(2):577
1. For patients with an ischemic stroke or TIA caused by an acute MI in whom LVT is identified by echocardiography or another form of cardiac imaging, oral anticoagulation is reasonable, aiming for an INR of 2–3 for at least
AHA/ASA 2006 Guideline Recommendations for Antithrombotic Therapy
in Acute MI With LVT
3 months and up to 1 year (Class IIa, LOE B)
2. ASA should be used concurrently for ischemic CAD during oral anticoagulant therapy in doses up to 162 mg/day (Class IIa, LOE A)
Sacco RL et al. Stroke. 2006;37(2):577

10
Guidelines for Symptomatic Extracranial Carotid Occlusive
Disease Management
65-Year-Old Woman With 15-Year History of HTN
On physical examination, a carotid bruit is heard on the left side CTA of the neck shows 70%–99% stenosis of the proximal portion of the left ICA
ICA = internal carotid artery
65-Year-Old Woman With 15-Year History of HTN
Diagnosis: symptomatic left extracranial ICA stenosis
Which of the following is recommended as first-line treatment of high-grade, symptomatic,
extracranial carotid artery stenosis?
A. Extracranial to intracranial bypass
B. Warfarin
C. Carotid endarterectomy
D. Aspirin plus extended-release dipyridamole
North American Symptomatic Carotid Endarterectomy Trial (NASCET)1
• 659 patients with symptomatic stenosis randomized to CEA or medical management• Only patients with ≥5-years life expectancy were included• Perioperative stroke/death rate 5.8%
Stenosis (%) Results70–99 2-year risk of stroke was 9% with CEA and 26% with medical therapy
5 year risk of stroke was 15 7% with CEA and 22 2% with medical
Secondary Stroke Prevention: Symptomatic Extracranial Carotid Occlusive Disease
50–695-year risk of stroke was 15.7% with CEA and 22.2% with medical therapyLess benefit for women and patients with retinal stroke/TIA
<50 No significant benefit of CEA
Carotid Endarterectomy Trialist Collaboration2
• Pooled data from European Carotid Surgery Trial and NASCET• In the CEA arm, benefits were greatest among patients randomized within
2 weeks of symptoms
1. North American Symptomatic Carotid Endarterectomy Trial Collaborators.N Engl J Med. 1991;325(7):4452. Rothwell PM et al. Lancet. 2004;363(9413):915
1. For patients with recent TIA or ischemic stroke within the last 6 months and ipsilateral severe (70%–99%) carotid artery stenosis, CEA by a surgeon with a perioperative morbidity and mortality rate of <6% is recommended (Class I, LOE A)
2. For patients with recent TIA or ischemic stroke and ipsilateral moderate (50%–69%) carotid stenosis, CEA is recommended depending on patient-specific factors such as age, gender, comorbidities, and severity of initial
AHA/ASA 2006 Guideline Recommendations for CEA
symptoms (Class I, LOE A)
3. When the degree of stenosis is <50%, CEA is not routinely indicated (Class III, LOE A)
4. When CEA is indicated for patients with TIA or stroke, surgery within 2 weeks is suggested rather than delaying surgery (Class IIa, LOE B)
Sacco RL et al. Stroke. 2006; 37(2):577

11
Among patients with symptomatic severe stenosis (>70%) in whom the stenosis is difficult to access surgically, medical conditions are present that greatly increase the risk for surgery, or other specific circumstances exist such as radiation-induced stenosis or restenosis after CEA, CAS is not inferior to endarterectomy and may be considered (Class IIb, LOE B). CAS is reasonable when performed by operators with established periprocedural morbidity and mortality rates of 4% to 6%, similar to that observed in trials of CEA and CAS
AHA/ASA 2006 Guideline Recommendations for Carotid Angioplasty and Stenting
mortality rates of 4% to 6%, similar to that observed in trials of CEA and CAS (Class IIa, LOE B)
Special Note:The results of the EVA-3S and SPACE studies were published after the 2006 AHA/ASA guidelines became available. EVA-3S and SPACE have added data which support clinical equipoise in relation to CAS. We await the results of Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST) to clarify the role of CAS in the management of patients with extracranial occlusive disease.
Sacco RL et al. Stroke. 2006;37(2):577
Guidelines for Symptomatic Intracranial Carotid Occlusive
Disease Management
65-Year-Old Woman With 15-Year History of HTN
Physical examination is unremarkableCerebral vascular diagnostic workup shows no cardiac source of embolism, and both carotid arteries are patent with no evidence of h d i ll i ifi t t ihemodynamically significant stenosisHead MRA is ordered, which shows a proximal left MCA stenosis
MCA = middle cerebral artery
65-Year-Old Woman With 15-Year History of HTN
Diagnosis: large artery intracranial occlusive disease (LAICOD)
Which one of the following is recommended as first-line treatment for large artery intracranial
occlusive disease?
A. Antiplatelet therapy
B. Anticoagulant therapy
C. Angioplasty and stenting
D. Extracranial to intracranial bypass
Ethnic Group Reported Frequency of LAICOD in Patients With Stroke (%)
Secondary Stroke Prevention:Symptomatic Intracranial
Carotid Occlusive DiseaseWorldwide LAICOD is a common and well-defined stroke subtypeCertain population groups may be at higher risk for LAICOD
Relative risk of intracranial atherosclerotic stroke in the United States– Hispanics vs whites: 5.00 (95% CI 1.69 to 14.76)– African Americans vs whites: 5.85 (95% CI 1.82 to 18.73)
ChineseKorean
South AsianThai
35–50565447
Gorelick PB et al. Stroke. 2008;39(8):2396

12
LAICOD: Risk of Recurrent CerebralIschemic Stroke in Key Clinical Trials
EC-IC Bypass Study1
– 1377 patients with symptomatic ICA or MCA stenosis randomized to either surgery or medical management
– Patients with symptomatic carotid siphon or MCA stenosis had an annual stroke rate of 8%–10%
– No significant benefit for EC-IC was shownWarfarin-Aspirin Symptomatic Intracranial Disease Trial (WASID)2
Outcomes in WASID ASA (%) Warfarin (%)
Ischemic stroke 20.4 17.0Ischemic stroke in the territory of the stenotic vessel 15.0 12.1
Disabling or fatal ischemic stroke 8.9 6.2
– 569 patients with symptomatic 50%–99% IC stenosis– INR goal of 2–3– Mean follow up of 1.8 years
1. The EC/IC Bypass Study Group. N Engl J Med. 1985;313(19):11912. Chimowitz MI et al. N Engl J Med. 2005;352(13):1305
For patients with hemodynamically significant intracranial stenosis who have symptoms despite medical therapies (antithrombotics, statins, and other treatments for risk factors), the usefulness of endovascular therapy (angioplasty and/or stent placement) is uncertain and is considered investigational
AHA/ASA 2006 Guideline Recommendations for Treatment of LAICOD
With Endovascular Therapy
(Class IIb, LOE C)1
Special Note:The results of the NIH registry on use of Wingspan stent for symptomatic 70%–99% intracranial arterial stenosis were published after the 2006 AHA/ASA guidelines. Based on these results, NIH has funded a study called Stenting vs Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS)2 to study the possible benefit of stenting for symptomatic intracranial artery stenosis.
1. Sacco et al. Stroke. 2006; 37(2):5772. Stenting vs Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis. http://clinicaltrials.gov/ct2/show/NCT00576693?term=SAMMPRIS&rank=1. Accessed August 21, 2008.
Conclusions
TIA and ischemic stroke are important risk factors for recurrent cerebral ischemia
Recurrent stroke is preventable
NSA guidelines for the management of patientsNSA guidelines for the management of patients with TIA and AHA/ASA guidelines for recurrent stroke prevention are useful clinical tools to reduce the risk of recurrent cerebral ischemia
Appendix I Additional Slides
Polytherapy for Recurrent Stroke Prevention: Opportunity for Reduction of Subsequent Stroke Risk
20
30
40
50
60
70
80
90Untreated
Treated
r Maj
or V
ascu
lar E
vent
Rat
e (%
)
12 meta-analyses (106 studies, 210,926 patients)Combination of
– Diet– Exercise– ASA (ASA + dipyridamole)– Statin (high dose)
A tih t i d
Adapted with permission from Hackam DG, Spence JD. Stroke. 2007;38(6):1881
0
10
Cartoid stenosis
AF Diabetes Smoking
5-Ye
ar
RRR (%) 90 86 84 87ARR (%) 41 67 27 25NNT (n) 2 1 4 4
Benefits of combination therapy in patients with CVD and specific subtypes or comorbidities
– Antihypertensive drug (aggressive BP lowering)
Predicted 5-year major vascular event rate
– RRR 80% (90%)– ARR 20% (22%)– NNT 5 (5) – Residual 5-year risk 5% (3%)
ARR = absolute risk reduction; NNT = number needed to treat; RRR = relative risk reduction
Predicting Stroke Risk in AF: Who Benefits Most?
Multivariate Analysis of Pooled Data
Clinical Risk Factors RRPrevious stroke or TIA 2.5 ×History of HTN 1.6 ×Diabetes 1.7 ×Increasing age (per decade) 1.4 ×
Hughes M et al. Thromb Haemost. 2008;99(2):295
RR = relative risk
13
Initiation of Anticoagulation Therapy in AF Patient With Acute TIA or Stroke
Controversy exists regarding the timing of treatmentPatients with TIA– May receive anticoagulation immediately if not contraindicated by
CT, MRI brain, or otherwise
Patients with ischemic stroke– Initiate anticoagulation within 2 weeks of ischemic stroke or
sooner depending on CT or MRI brain findings, neurologic examination findings (size and severity of infarct to be considered), and urgency of anticoagulation (eg, mechanical heart valve)
– Delaying anticoagulation may be reasonable in patients with uncontrolled HTN and large infarcts
Cardioembolic Stroke: Acute MI and LVT
Acute MI and LVT – Stroke and systemic embolism can occur in up to
12% of patients with LVT post MI– Risk of LVT is higher in anterior MI– Risk of stroke is higher during the first 3 months– In one-third of patients, LVT may remain
echcardiographically apparent for 1 year after MI
Albers GW et al. Chest. 2004;126(3 suppl):483SVisser CA et al. Chest. 1984;86(4):532
Cardioembolic Stroke: CardiomyopathyCardiomyopathy– Significantly reduced LV systolic function causes relative stasis– Annual stroke rate in the Survival And Ventricular Enlargement
(SAVE) study1
0.8% in patients with EF of 29%–35%1.7% in those with EF ≤28%
N t d h d fi iti l th ffi f f i ASA i– No study has definitively proven the efficacy of warfarin or ASA in stroke prevention in patients with cardiomyopathy
– In practice, patients with thromboembolism suspected of cardioembolic origin with EF below 30% are usually managed with warfarin (INR, 2–3)
– WARCEF (Warfarin versus Aspirin for Reduced Cardiac Ejection Fraction) study is in progress2
1. Pfeffer MA et al. N Engl J Med. 1992;327(10):669 2. Pullicino P et al. J Card Fail. 2006;12(1):39
For patients with ischemic stroke or TIA who have dilated cardiomyopathy, either warfarin (INR, 2–3) or antiplatelet therapy may be considered for prevention of recurrent events (Class IIb LOE C)
AHA/ASA 2006 Guideline Recommendations for Antithrombotic Therapy
in Cardiomyopathy
of recurrent events (Class IIb, LOE C)
Sacco RL et al. Stroke. 2006;37(2):577
Cardioembolic Stroke:Valvular Disease
PHV– Warfarin (INR, 1.8–2.5) versus antiplatelet agents1
Treatment Thromboembolism (100 patient-years) (%)
Warfarin 2ASA-dipyridamole 9.8Pentoxifylline-ASA 7.9
– Warfarin (INR, 3.0–4.5) vs warfarin plus ASA (100 mg daily)2
1. Mok CK et al. Circulation. 1985;72(5):10592. Turpie AG et al. N Engl J Med. 1993;329(8):524
Treatment Annual Rate of Embolic Events or Vascular Death (%)
RR(%) (95% CI)
Bleeding(%)
Increase in Risk(%) (95% CI)
Warfarin+ placebo 9.8 77 (44%–91%)
P<.00122 55 (8%–124%)
P=.02+ ASA 7.9 35
Valvular Disorder Comments Treatment and LOE
Rheumatic valve disease
• Recurrent stroke occurs in 30%–65% of patients• Valvulplasty does not eliminate the risk of recurrent
thromboembolism• Observational studies show that long-term anticoagulation
significantly reduces the risk of recurrent stroke
Warfarin (INR, 2–3)(Class IIa, LOE C)
Consider adding ASA (81 mg/day) if recurrent embolism
while on warfarin (Class IIa, LOE C)
Mitral valve prolapse
• Most common form of valve disease, usually innocuous• No large-scale, randomized trials have addressed the
efficacy of major antithrombotics for secondary preventionAntiplatelet agent(Class IIa, LOE C)
Cardioembolic Stroke: Valvular Disease
Aortic valve disease
• Associated with small and often clinically silent microthrombi or calcific embolism
Antiplatelet agent(Class IIb, LOE C)
Mitral annular calcification (MAC)
• Considered a form of atherosclerosis• Associated with mitral regurgitation or stenosis• Endocarditis, arrhythmia, and embolic phenomenon may
occur (thromboembolism vs fibro-calcified material)
Antiplatelet agent(Class IIb, LOE C)
Antiplatelet agent or warfarin may be considered in patients with mitral
regurgitation caused by MAC(Class IIb, LOE C)
Sacco RL et al. Stroke. 2006;37(2):577

14
1. For patients with ischemic stroke or TIA who have modern mechanical PHVs, oral anticoagulants are recommended, with an INR target of 3.0 (range, 2.5–3.5) (Class I, LOE B)
2. For patients with mechanical PHV who have an ischemic stroke or systemic embolism despite adequate therapy with oral anticoagulants, ASA 75–100 mg/day in addition to oral,
AHA/ASA 2006 Guideline Recommendationsfor Antithrombotic Therapy in Valvular Disease
anticoagulants, ASA 75 100 mg/day in addition to oral, anticoagulants and maintenance of the INR at a target of 3.0 (range 2.5–3.5) are reasonable (Class IIa, LOE B)
3. For patients with ischemic stroke or TIA who have bioprosthetic heart valves with no other source of thromboembolism, anticoagulation with warfarin (INR, 2–3) may be considered (Class IIb, LOE C)
Sacco RL et al. Stroke. 2006;37(2):577
PHV = prosthetic heart valve
Cardioembolic Stroke:PFO
PFO– Prevalence in patients ≥45 years is ~26%– Atrial septal aneurysm affects ~2%– 4-year risk of stroke recurrence
2.3% in patients with PFO15.2% in patients with PFO and atrial septal aneurysm
– Increased risk of stroke in patients with large right-to-left shunt– Higher prevalence of PFO in patients with cryptogenic stroke– PFO in Cryptogenic Stroke Study
No statistically significant difference in the rate of recurrent stroke in patients with or without PFO or among those treated with ASA or warfarin
– Randomized Evaluation of Recurrent Stroke Comparing PFOClosure to Established Current Standard of Care Treatment (RESPECT) study and others are comparing percutaneous PFO closure versus medical treatment for recurrent stroke prevention
Cruz-González I et al. Rev Esp Cardiol. 2008;61(7):738
1. Antiplatelet therapy is reasonable to prevent a recurrent event (Class IIa, LOE B)
2. Warfarin is reasonable for high-risk patients who have other indications for oral anticoagulation (Class IIa, LOE C)
AHA/ASA 2006 Guideline Recommendations for Recurrent Stroke Prevention for PFO
3. Insufficient data exist to make a recommendation about PFO closure in patients with a first stroke and PFO
4. PFO closure may be considered for patients with recurrent cryptogenic stroke despite optimal medical therapy (Class IIb, LOE C)
Sacco RL et al. Stroke. 2006;37(2):577
PFO = patent foramen ovale
Guidelines for Carotid Dissection Stroke Management
65-Year-Old Woman With 15-Year History of HTN
Patient complains of neck pain on the left sideOn physical examination, there is a left partial Horner syndrome (ptosis and miosis)Bedside carotid duplex is performedp p
65-Year-Old Woman With 15-Year History of HTN
Bedside carotid duplex shows a double lumen in the proximal left ICA (picture above)Diagnosis: left extracranial ICA dissection
How should subsequent cerebral ischemia be prevented in a patient with a symptomatic carotid artery dissection?

15
Secondary Stroke Prevention: Arterial Dissections
Extracranial arterial dissections– Common with atherosclerotic disease– Frequent in young patients– May be spontaneous or traumatic (neck manipulation,
hyperextension, lifting) – More commonly detected in extracranial arteries– Location includes mostly regions where the arteries are
mobile and not anchoredAnterior circulation: cervical portion of the ICAPosterior circulation: segments of the vertebral arteries (V1 and V3)
Caplan LR. Nat Clin Pract Neurol. 2008;4(1):34
Arterial Dissections: Pathophysiology
Tear in tunica media results in bleeding in arterial wallBlood dissects longitudinally spreading distally and proximallyTear of intima permits clots to enter lumenExpansion of intramural hemorrhageExpansion of intramural hemorrhage narrows lumen causing stasis, activation of platelets, and the coagulation cascadeMain dissection plane can lie between the media and adventitia creating a pseudoaneurysmRupture through adventitia into the intracranial circulation causes subarachnoid hemorrhage
Adapted with permission from Caplan LR. Nat Clin Pract Neurol. 2008;4(1):34
2003 Cochrane Database review1
– Poor quality studies comparing ASA to warfarin– ASA is likely to be effective and safer than warfarin– Further studies are needed
Arterial Dissections:Treatment
Due to the pathophysiology (red thrombi) most experts recommend anticoagulantsAnnual risk of stroke recurrence in carotid dissection is low (0.3% per year)2
1. Lyrer P, Engelter S. Cochrane Database Syst Rev. 2003;(3):CD0002552. Touzé E et al. Neurology. 2003;61(10):1347
1. For patients with extracranial arterial dissection, use of warfarin for 3 to 6 months or use of antiplatelet agents is reasonable (Class IIa, LOE B)
2 Beyond 3 to 6 months long-term antiplatelet therapy
AHA/ASA 2006 Guideline Recommendations for Antithrombotic Therapy
in Cerebral Artery Dissection
2. Beyond 3 to 6 months, long term antiplatelet therapy is reasonable. Anticoagulant therapy beyond 3 to 6 months may be considered among patients with recurrent ischemic events (Class IIb, LOE C)
Sacco RL et al. Stroke. 2006;37(2):577
Stroke Management in Patients With Aortic Arch Atheroma
Secondary Stroke Prevention:Aortic Arch Atheroma
Prevalence and severity of aortic arch atheroma (AAA) increases with age1
90% of the cases are stable and AAA progresses slowly over timeUnclear if AAA is a source of emboli or a marker of an increased risk of
Type of AAA Odds Ratio of StrokeSimple 2.3
Complex 7.1
atherosclerotic diseaseRisk of stroke is higher in patients with complicated AAAs (ie, >5 mm in thickness, ulcerated plaque, and mobile)2
1. Molina CA et al. Cerbrovasc Dis. 2007;24(suppl 1):84 2. Adapted with permission from Jones EF et al. Stroke. 1995;26(2):218

16
AAA TreatmentNew York University Atheroma Group1
– Statin therapy was protective against embolic events
– No protective effect with warfarin or antiplatelet agents
Antiplatelet therapy is usually used in patients with stroke or TIAN d fi iti t d h d t i d if f i i iNo definitive study has determined if warfarin is superior to antiplatelet agents for treatment of AAAAortic Arch Related Cerebral Hazard Trial (ARCH) is comparing clopidogrel + ASA vs oral anticoagulation in preventing brain infarction, brain hemorrhage, MI, peripheral embolism, and vascular death2
1. Tunick PA et al. Am J Cardiol. 2002;90(12):1320 2. Aortic Arch Related Cerebral Hazard Trial (ARCH). http://clinicaltrials.gov/ct2/show/NCT00235248. Accessed July 16, 2008
SAPPHIRE EVA-3S SPACE
Hypotheses CAS is not inferior to CEA for high-risk patients
CAS is not inferior to CEA for symptomatic carotid stenosis
CAS is not inferior to CEA for symptomatic carotid stenosis
Patients (n) 334 527 1200
Degree of stenosis (%) >50 symptomatic or 60 99 t ti ≥50 t ti
Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators (SAPPHIRE)1,2
Endarterectomy Versus Stenting in Patients with Symptomatic Severe Carotid Stenosis (EVA-3S)3
Stent-Supported Percutaneous Angioplasty of the Carotid Artery Versus Endarterectomy (SPACE)4
Carotid Angioplasty and Stenting: Summary of Key Studies I
*P=.004 for noninferiority; **P=.09 for noninferiority; CAS = carotid artery stenting
g (%) y p>80 asymptomatic 60–99 symptomatic ≥50 symptomatic
Primary end point Death, stroke, or MI within 30 days after procedure or
death/ipsilateral stroke between 30 days and 1 year
Composite of stroke or death within 30 days posttreatment
Ipsilateral stroke (ischemic or hemorrhagic) or death within
30 days postprocedure
Primary outcome (CEA vs CAS) (%) 20.1 vs 12.2* 3.9 vs 9.6 6.34 vs 6.84**
Early termination Slow recruitment Safety and futility reasons No further funding
1. Yadav JS et al. N Engl J Med. 2004;351(15):1493; 2. Gurm HS et al. N Engl J Med. 2008;358(15):1572; 3. Mas JL et al. N Engl J Med. 2006;355(16):1660; 4. SPACE Collaborative Group. Lancet. 2006;368(9543):1239
SAPPHIRE EVA-3S SPACE
Trial conclusion CAS is not inferior to CEA for high-risk patients at 6 months, 1 year,
and 3 years
Rates of stroke or death at 1 month and 6 months are
lower in CEA
Trial failed to prove noninferiority of CAS vs CEA
High risk for CEA Required Not required Not required
Symptomatic patients (%) 29 100 100
Operator experienceCAS Required periprocedural risk <6% 39% done by operators in No prespecified experience in
Carotid Angioplasty and Stenting: Summary of Key Studies II
CAS
CEA
Required periprocedural risk <6%
Required periprocedural risk <6%
39% done by operators in training
≥25 CEAs performed in prior year before enrollment
No prespecified experience in CAS
≥25 CEAs performed
Stent type 2 stents (same manufacturer)
5 stents (different manufacturers)
3 stents (different manufacturers)
Protection device Mandatory (only 1 system)
Tried in 92% (any of 7 systems)
Used in 27% (any of 5 systems)
1.Yadav JS et al. N Engl J Med. 2004;351(15):1493; Gurm HS et al. N Engl J Med. 2008;358(15):1572; Mas JL et al. N Engl J Med. 2006;355(16):1660; 4. SPACE Collaborative Group. Lancet. 2006;368(9543):1239
Study Outcome (%)WASID1
Ischemic stroke, brain hemorrhage, or death from vascular causes (primary outcome)*
ASAWarfarin
22.121.8
EC-IC Bypass Study Group2
Is an EC-IC anastomosis better than medical treatment for symptomatic No
Treatment of LAICOD Based Upon Key Clinical Trials
Is an EC IC anastomosis better than medical treatment for symptomatic LAICOD?**
No
NIH registry on use of WingspanTM stent for 70%–99% intracranial stenosis3
Stroke or death within 30 days or stroke in the territory (1–6 months)Restenosis (50% or more)
1425
1. Chimowitz MI et al. N Engl J Med. 2005;352(13):13052. The EC/IC Bypass Study Group. N Engl J Med. 1985;313(19):11913. Zaidat OO et al. Neurology. 2008;70(17):1518
*Major hemorrhage occurred more frequently in warfarin vs ASA group (8.3% vs 3.2%; HR 0.40; 95% CI 0.18-0.84; P=.01)**Carotid Occlusion Surgery Study (COSS) is ongoing and retesting the hypothesis of benefit for EC-IC bypass
Recurrent Stroke Prevention in Other Cerebrovascular Conditions
Condition Comments Treatment and LOE
Hyper-homocysteinemia
• Hyperhomocysteinemia is associated with a 2x risk of stroke• Vitamin Intervention for Stroke Prevention (VISP) study, reduction
of total homocysteine after nondisabling cerebral infarction had no effect on vascular outcomes
• Are there subgroups who might receive benefit from multivitamin therapy?
Daily vitamin B6, B12 and folate(Class IIa, LOE B)
Inherited
• Weak association between FVL, PTGM, MTHFR, APCR, and stroke in adults; more clear in younger age groups
• No studies comparing antiplatelets to warfarin for secondary
Antiplatelet or anticoagulants(Class IIa, LOE C)
Anticoagulants if recurrent
Secondary Stroke Prevention:Other Specific Conditions
thrombophilia • No studies comparing antiplatelets to warfarin for secondary prevention have been done
• Evaluate for alternative mechanism
Anticoagulants if recurrent thrombosis
(Class IIb, LOE C)
Antiphospholipid (APL) antibodies
• Associated with venous and arterial occlusive disease• In Warfarin vs Aspirin Recurrent Stroke Study/Antiphospholipid
Antibodies and Stroke Study (WARSS/APASS) collaboration, the risk of vascular occlusive events in patients with ischemic stroke and APL was not different in patients treated with ASA or warfarin
Antiplatelet(Class IIa, LOE B)
Anticoagulants if APL syndrome with occlusive disease in multiple organs, miscarriages, and livedo reticularis
(Class IIa, LOE B)
APCR = activated protein C resistance; FVL = factor V Leiden; MTHFR =methylenetetrahydrofolate reductase C677T mutation; PTGM = prothrombin G20210A mutation
Sacco RL et al. Stroke. 2006;37(2):577

17
Condition Comments Treatment and LOE
Cerebral venous sinus thrombosis
• Venous infarctions are frequently hemorrhagic • More frequent in patients with hypercoagulable states• Anticoagulant superior to placebo
Anticoagulants (even in the presence of hemorrhagic
infarction)(Class IIa, LOE B)
Sickle cell disease
• In Stroke Prevention Trial in Sickle Cell Anemia (STOP), children with mean flow velocity ≥200 cm/sec at MCA (measured noninvasively by TCD) were randomized to exchange transfusion (goal: HbS <30%) or placebo
• Annual stroke rate was 1% in children undergoing
Risk factor control and antiplatelet agents
(Class IIa, LOE B)Blood transfusion to reduce HbS
Secondary Stroke Prevention:Other Specific Conditions
Sickle cell disease • Annual stroke rate was 1% in children undergoing transfusion and 10% in those not receiving transfusion
• Small studies suggested that hydroxyurea reduces the risk of stroke recurrence
• High risk of moyamoya disease
Blood transfusion to reduce HbS to <30%–50% of total Hb,
hydroxyurea, and bypass surgery for advanced occlusive disease
(Class IIb, LOE C)
Postmenopausal hormone therapy
• In Women's Estrogen for Stroke Trial (WEST) and Women’s Health Initiative (WHI) studies, women assigned to hormonal replacement had a higher risk of stroke compared with placebo
Postmenopausal hormone therapy is not recommended
(Class III, LOE A)
Sacco RL et al. Stroke. 2006;37(2):577
HbS = sickle cell hemoglobin
Appendix II References
Adams RJ. Big strokes in small persons. Arch Neurol. 2007;64(11):1567-1574.
Adams RJ, Albers G, Alberts MJ, et al. Update to the AHA/ASA recommendations for the prevention of stroke in patients with stroke and transient ischemic attack. Stroke. 2008;39(5);1647-1652.
Adler Y, Fink N, Spector D, Wiser I, Sagie A. Mitral annulus calcification—a window to diffuse atherosclerosis of the vascular system. Atherosclerosis. 2001;155(1):1-8.
Albers GW, Amarenco P, Easton JD, Sacco RL, Teal P. Antithrombotic and thrombolytic therapy for ischemic stroke: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 suppl):483S-512S.
Albers GW, Caplan LR, Easton JD, et al. Transient ischemic attack—proposal for a new definition. N Engl J Med. 2002;347(21):1713-1716.
Albers GW, Diener HC, Frison L, et al. Ximelagatran vs warfarin for stroke prevention in patients with nonvalvular atrial fibrillation: a randomized trial. JAMA. 2005;293(6):690-698.
American Heart Association. Heart Disease and Stroke Statistics—2008 Update. Dallas, Texas: American Heart Association; 2008.
Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women's Health Initiative randomized controlled trial. JAMA. 2004;291(14):1701-1712.
Assistance Publique-Hôpitaux de Paris; National Health and Medical Research Council, Australia; sanofi-aventis; Bristol-Myers Squibb. Aortic Arch Related Cerebral Hazard Trial (ARCH). http://clinicaltrials.gov/ct2/show/NCT00235248. Accessed July 22, 2008.
Bhatt DL. Aspirin resistance: more than just a laboratory curiosity. J Am Coll Cardiol. 2004;43(6):1127-1129.
Bhatt DL, Steg PG, Ohman EM, et al. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA. 2006;295(2):180-189.
Caplan LR. Dissections of brain-supplying arteries. Nat Clin Pract Neurol. 2008;4(1):34-42.
Cardiogenic brain embolism. The second report of the Cerebral Embolism Task Force. Arch Neurol. 1989;46(7):727-743.
Casas JP, Hingorani AD, Bautista LE, Sharma P. Meta-analysis of genetic studies in ischemic stroke: thirty-two genes involving approximately 18,000 cases and 58,000 controls. Arch Neurol. 2004;61(11):1652-1661.
Chimowitz MI, Lynn MJ, Howlett-Smith H, et al. Comparison of warfarin and aspirin for symptomatic intracranial arterial stenosis. N Engl J Med. 2005;352(13):1305-1316.
Coulshed N, Epstein EJ, McKendrick CS, Galloway RW, Walker E. Systemic embolism in mitral valve disease. Br Heart J. 1970;32(1):26-34.disease. Br Heart J. 1970;32(1):26 34.
de Bruijn SF, Stam J. Randomized, placebo-controlled trial of anticoagulant treatment with low-molecular-weight heparin for cerebral sinus thrombosis. Stroke. 1999;30(3):484-488.
De Silva DA, Woon FP, Pin LM, Chen CP, Chang HM, Wong MC. Intracranial large artery disease among OCSP subtypes in ethnic South Asian ischemic stroke patients. J Neurol Sci. 2007;260(1-2):147-149.
The EC/IC Bypass Study Group. Failure of extracranial-intracranial arterial bypass to reduce the risk of ischemic stroke. Results of an international randomized trial. N Engl J Med. 1985;313(19):1191-1200.
Engelter ST, Brandt T, Debette S, et al. Antiplatelets versus anticoagulation in cervical artery dissection. Stroke. 2007;38(9):2605-2611.
Feinberg WM, Albers GW, Barnett HJ, et al. Guidelines for the management of transient ischemic attacks. From the Ad Hoc Committee on Guidelines for the Management of Transient Ischemic Attacks of the Stroke Council of the American Heart Association. Circulation. 1994;89(6):2950-2965.
Fulkerson PK, Beaver BM, Auseon JC, Graber HL. Calcification of the mitral annulus: etiology, clinical associations, complications and therapy. Am J Med. 1979;66(6):967-977.
Gorelick PB. Practice Perspective on the AHA/ASA 2008 Update for Recurrent Cerebral Ischemia Prevention. http://pt.wkhealth.com/pt/re/aha/editorial3_5_2008.htm;jsessionid=Lr9hGX0qz7ynry2TfJTs7r5sGmJbBVyq3ph0xMkhBn2p4T0rGs2Q!2085969891!181195628!8091!-1. Accessed July 22, 2008.
Gorelick PB, Wong KS, Bae HJ, Pandey DK. Large artery intracranial occlusive disease. A large worldwide burden but a relatively neglected frontier. Stroke. 2008;39(8):2396-2399.
Gurm HS Yadav JS Fayad P et al Long-term results of carotid stenting versus endarterectomy in high-riskGurm HS, Yadav JS, Fayad P, et al. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med. 2008;358(15):1572-1579.
Hackam DG, Spence JD. Combining multiple approaches for the secondary prevention of vascular events after stroke: a quantitative modeling study. Stroke. 2007;38(6):1881-1885.
Handke M, Harloff A, Olschewski M, Hetzel A, Geibel A. Patent foramen ovale and cryptogenic stroke in older patients. N Engl J Med. 2007;357(22):2262-2268.
Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146(12):857-867.
Holley KE, Bahn RC, McGoon DC, Mankin HT. Spontaneous calcific embolization associated with calcific aortic stenosis. Circulation. 1963;27:197-202.
Homma S, Sacco RL, Di Tullio MR, Sciacca RR, Mohr JP; PFO in Cryptogenic Stroke Study (PICSS) Investigators. Effect of medical treatment in stroke patients with patent foramen ovale: patent foramen ovale in Cryptogenic Stroke Study. Circulation. 2002;105(22):2625-2631.
Hughes M, Lip GY, Guideline Development Group, National Clinical Guideline for Management of Atrial Fibrillation in Primary and Secondary Care, National Institute for Health and Clinical Excellence. Stroke and thromboembolism in atrial fibrillation: a systematic review of stroke risk factors, risk stratification schema and cost effectiveness data. Thromb Haemost. 2008;99(2):295-304.
Johnston SC, Nguyen-Huynh MN, Schwarz ME, et al. National Stroke Association guidelines for the management of transient ischemic attacks. Ann Neurol. 2006;60(3):301-313.
Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet. 2007;369(9558):283-292.
J EF K l JM C l fi P T ki AM D GA P i l ti th A i d d t i kJones EF, Kalman JM, Calafiore P, Tonkin AM, Donnan GA. Proximal aortic atheroma. An independent risk factor for cerebral ischemia. Stroke. 1995;26(2):218-224.
Levine SR, Brey RL, Tilley BC, et al. Antiphospholipid antibodies and subsequent thrombo-occlusive events in patients with ischemic stroke. JAMA. 2004;291(5):576-584.
Lyrer P, Engelter S. Antithrombotic drugs for carotid artery dissection. Cochrane Database Syst Rev. 2003;(3):CD000255.
Mas JL, Arquizan C, Lamy C, et al. Recurrent cerebrovascular events associated with patent foramen ovale, atrial septal aneurysm, or both. N Engl J Med. 2001;345(24):1740-1746.
Mas JL, Chatellier G, Beyssen B, et al. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355(16):1660-1671.

18
Medical University of South Carolina and US National Institutes of Health. Stenting vs Aggressive Medical Management for Prevention Recurrent Stroke in Intracranial Stenosis. http://clinicaltrials.gov/ct2/show/NCT00576693?term=stenting&rank=9. Accessed July 22, 2008.
Meissner I, Whisnant JP, Khandheria BK, et al. Prevalence of potential risk factors for stroke assessed by transesophageal echocardiography and carotid ultrasonography: the SPARC study. Stroke prevention: assessment of risk in a community. Mayo Clin Proc. 1999;74(9):862-869.
Mok CK, Boey J, Wang R, et al. Warfarin versus dipyridamole-aspirin and pentoxifylline-aspirin for the prevention of prosthetic heart valve thromboembolism: a prospective randomized clinical trial. Circulation. 1985;72(5):1059-1063.
Molina CA, Santamarina E, Alvarez-Sabín J. Cryptogenic stroke, aortic arch atheroma and patent foramen ovale. Cerebrovasc Dis. 2007;24(suppl 1):84-88.
N th A i S t ti C tid E d t t T i l C ll b t B fi i l ff t f tidNorth American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. N Engl J Med. 1991;325(7):445-453.
Pfeffer MA, Braunwald E, Moyé LA, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N Engl J Med. 1992;327(10):669-677.
Pujadas Capmany R, Arboix A, Casañas-Muñoz R, Anguera-Ferrando N. Specific cardiac disorders in 402 consecutive patients with ischaemic cardioembolic stroke. Int J Cardiol. 2004;95(2-3):129-134.
Pullicino P, Thompson JL, Barton B, et al. Warfarin versus aspirin in patients with reduced cardiac ejection fraction (WARCEF): rationale, objectives, and design. J Card Fail. 2006;12(1):39-46.
Rothwell PM. Does transient ischemic attack deserve emergency care? Nat Clin Pract Neurol. 2006;2(4):174-175.
Rothwell PM, Eliasziw M, Gutnikov SA, Warlow CP, Barnett HJ; Carotid Endarterectomy Trialists Collaboration. Endarterectomy for symptomatic carotid stenosis in relation to clinical subgroups and timing of surgery. Lancet. 2004;363(9413):915-924.
Rothwell PM, Giles MF, Flossmann E, et al. A simple score (ABCD) to identify individuals at high early risk of stroke after transient ischaemic attack. Lancet. 2005;366(9479):29-36.
Sacco RL. Risk factors, outcomes, and stroke subtypes for ischemic stroke. Neurology. 1997;49(5 suppl 4):S39-S44.
Sacco RL, Wolf PA, Gorelick PB. Risk factors and their management for stroke prevention: outlook for 1999 and beyond. Neurology. 1999;53(7 suppl 4):S15-S24.
Sacco RL, Adams R, Albers G, et al. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Stroke. 2006;37(2):577-617.
Schievink WI. Spontaneous dissection of the carotid and vertebral arteries. N Engl J Med. 2001;344(12):898-906.
SPACE Collaborative Group, Ringleb PA, Allenberg J, et al. 30 day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised non-inferiority trial. Lancet. 2006;368(9543):1239-1247. [Published correction in Lancet. 2006;368(9543):1238]
Steiner MM, Di Tullio MR, Rundek T, et al. Patent foramen ovale size and embolic brain imaging findings among patients with ischemic stroke. Stroke. 1998;29(5):944-948.
Szekely P. Systemic embolism and anticoagulant prophylaxis in rheumatic heart disease. Br Med J. 1964;1(5392):1209-1212.
Thom T, Haase N, Rosamond W, et al. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2006;113(6):e85-e151. [Published corrections in Circulation. 2006;113(14):e696; Circulation. 2006;114(23):e630]
Toole JF, Malinow MR, Chambless LE, et al. Lowering homocysteine in patients with ischemic stroke to prevent recurrent stroke, myocardial infarction, and death: the Vitamin Intervention for Stroke Prevention (VISP) randomized controlled trial. JAMA. 2004;291(5):565-575.
Touzé E, Gauvrit JY, Moulin T, et al. Risk of stroke and recurrent dissection after a cervical artery dissection: a multicenter study. Neurology. 2003;61(10):1347-1351.
Tunick PA Nayar AC Goodkin GM et al Effect of treatment on the incidence of stroke and other emboli inTunick PA, Nayar AC, Goodkin GM, et al. Effect of treatment on the incidence of stroke and other emboli in 519 patients with severe thoracic aortic plaque. Am J Cardiol. 2002;90(12):1320-1325.
Turpie AG, Gent M, Laupacis A, et al. A comparison of aspirin with placebo in patients treated with warfarin after heart-valve replacement. N Engl J Med. 1993;329(8):524-529.
Viscoli CM, Brass LM, Kernan WN, Sarrel PM, Suissa S, Horwitz RI. A clinical trial of estrogen-replacement therapy after ischemic stroke. N Engl J Med. 2001;345(17):1243-1249.
Visser CA, Kan G, Meltzer RS, Lie KI, Durrer D. Long-term follow-up of left ventricular thrombus after acute myocardial infarction. A two-dimensional echocardiographic study in 96 patients. Chest.1984;86(4):532-536.
Ware RE, Zimmerman SA, Schultz WH. Hydroxyurea as an alternative to blood transfusions for the prevention of recurrent stroke in children with sickle cell disease. Blood. 1999;94(9):3022-3026.
White H, Boden-Albala B, Wang C, et al. Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation. 2005;111(10):1327-1331.
Wong LKS. Global burden of intracranial atherosclerosis. Int J Stroke. 2006;1(3):158-159.
Yadav JS, Wholey MH, Kuntz RE, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493-1501.
Zaidat OO, Klucznik R, Alexander MJ, et al. The NIH registry on use of the Wingspan stent for symptomatic 70-99% intracranial arterial stenosis. Neurology. 2008;70(17):1518-1524.