red font = answers added after research;
TRANSCRIPT
RED FONT = ANSWERS ADDED AFTER RESEARCH; Green Highlighted # = REPEAT QUESTION May 2019: 1.Molecular mechanism for HPV (inactive protongene)? Inactivate proto-oncogene P53
Expression of high-risk HPV E6 and E7 genes in primary human keratinocytes effectively facilitates their immortalization (59, 96). ... They can undergo malignant progression after extended growth in tissue culture or when additional oncogenes such as ras or fos are expressed 2. Insulin- fastest acting insulin but shortest duration of action Fast acting insulin includes lispro, aspart (NovoLog), Glulisine (Apidra) 3. Articaine max carpule for 150 lb guy = 6 carpules
Max dose is 3.2mg/lb or 7mg/kg Math ---> (3.2mg x 150lb )= 480mg for max dose, now since Articaine is 4%, it becomes 40mg/ml. Now you will do (40mg/ml x 1.8ml)= 72mg a carpule. So do 480mg/72mg= 6.666 and round down to 6 carpules max. 4. Recommended tylenol dosage for kid (10-12mg per kg every 3 hours, 25 mg for every 6 hours)
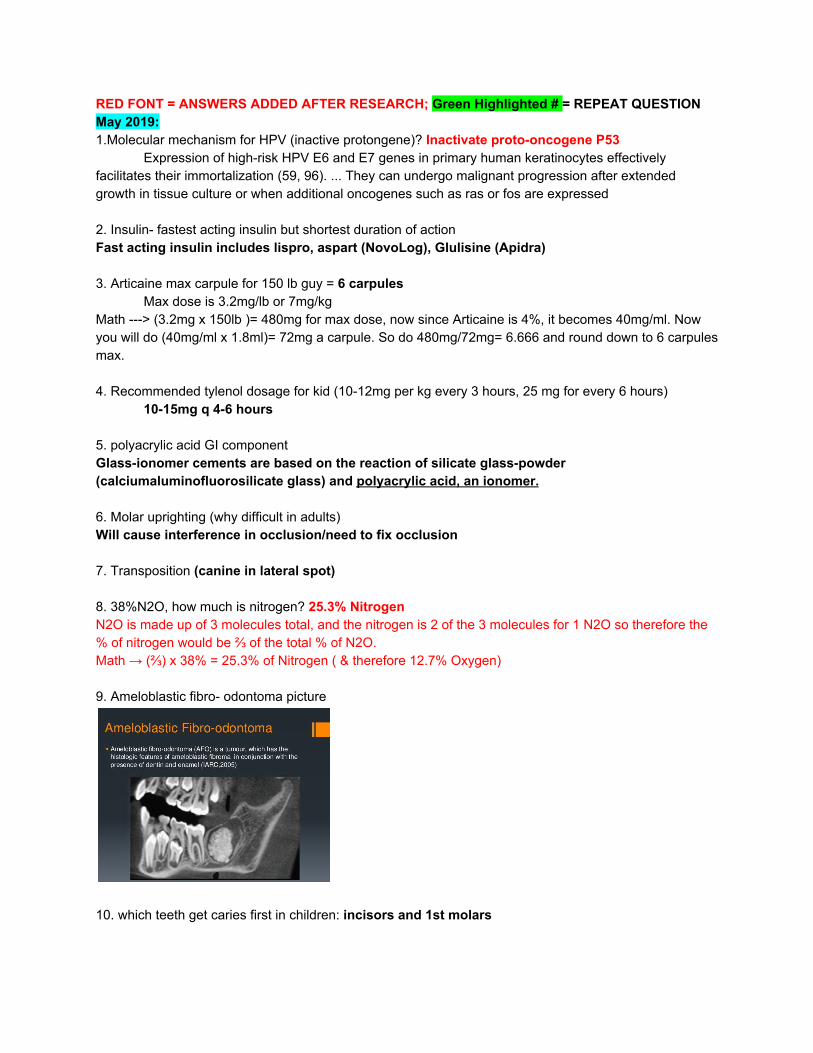
10-15mg q 4-6 hours 5. polyacrylic acid GI component Glass-ionomer cements are based on the reaction of silicate glass-powder (calciumaluminofluorosilicate glass) and polyacrylic acid, an ionomer. 6. Molar uprighting (why difficult in adults) Will cause interference in occlusion/need to fix occlusion 7. Transposition (canine in lateral spot) 8. 38%N2O, how much is nitrogen? 25.3% Nitrogen N2O is made up of 3 molecules total, and the nitrogen is 2 of the 3 molecules for 1 N2O so therefore the % of nitrogen would be ⅔ of the total % of N2O. Math → (⅔) x 38% = 25.3% of Nitrogen ( & therefore 12.7% Oxygen) 9. Ameloblastic fibro- odontoma picture
10. which teeth get caries first in children: incisors and 1st molars
11. if doing a prep and pulpal floor is perpendicular, which likely to expose? max 1st molar (medial inclination of Max 1st molar makes it more susceptible to pulpal exposure) 12. what is wheezing? inflammation/vibration Difficulty exhaling 13. amount of epi that you give % for anaphylaxis? 0.3%
0.2-0.5mL for adults ; 0.01 mL for kids 14. Non rigid 6 unit, when can you use? (in pier FPD) 15. what is the best casting for RPD? Strongest removable framework (gold-pallidium titanium), Type 4 Casting 16. External splinting favored over internal splinting why? Less reduction; allow healing of the PDL, maintain tooth position
○ Internal Splint – inside cavity pre ○ External Splint – No involving tooth preparation, usually confined to anterior teeth – allow
healing of the pdL, maintain tooth position
17. class II ANB is larger 18. labial bow, what does that do?
Labial bow in retainer retrudes the anterior teeth 19. Calculate attachment loss Determine attachment loss by calculating measurement of CEJ to sulcus (depth of pocket)
Ex. recession is 2mm and probing depth is 1mm, attachment loss = 3mm 20. what most likely to injure during distal wedge? Lingual nerve 21. what teeth are anesthetized when IANB? Long buccal?
IANB anesthetize mandibular teeth and surrounding hard and soft tissue up to the midline (does not reach buccal soft tissue of molars)
Long buccal gets the buccal soft tissue of molars 22. Pt is getting a buccal vestibulopathy, what kind of dissection would you do? Supraperiosteal 23. If you give someone bag ventilation not connected to oxygen, what is the amount of oxygen they’re receiving- 21% 24. Proportional relationship of width of pontic in FPD related to the width of the fpd span 25. Bacteria that causes root caries - Strep Mutans, Lactobacillus, Actinobacillus 26. Molar tipping- most common negative effect - occlusal interference
27. Primary teeth most involved in perio - 1st mandibular molar 28. Half life calculation 29. Why do you aspirate bone lesion before surgical exploration- To check if its a vascular lesion 06/05/19: 1.know pterygomandibular raphe and muscle junctions
The pterygomandibular raphe (pterygomandibular ligament) is a ligamentous band of the buccopharyngeal fascia, attached superiorly to the pterygoid hamulus of the medial pterygoid plate and inferiorly to the posterior end of the mylohyoid line of the mandible.
● Its medial surface is covered by the mucous membrane of the mouth. ● Its lateral surface is separated from the ramus of the mandible by a quantity of adipose
tissue. ● Its posterior border gives attachment to the superior pharyngeal constrictor muscle. ● Its anterior border attaches to the posterior edge of the buccinator.
2. Border molding lingual flange - MYLOHYOID 3. radiograph of pterygomaxillary fissure- teardrop 4. Eagle syndrome - calcified stylohyoid ligament 5. radiograph stylohyoid 6. know ectodermal dysplasia- congenital anodontia/ hypodontia, sweat hair and skin gland problems 7. % roots of MB root maxillary molar Maxillary 1st molar: 40% for 3, 60% for 4 Maxillary 2nd molar: 60% for 3 and 40 % for 4 Mandibular 1st molar: 70 % for 3, 30% for 4 Mandibular 2nd molar: 90 % for 3 and 5% for 4 8. rectangular wire in orthodontics - advantage is rotation of crown and root Control crown and root movement - torque 9. know desensitization a treatment or process that diminishes emotional responsiveness to a negative, aversive or positive stimulus after repeated exposure to it. Systematic desensitization- 3 steps: Construct a hierarchy, relaxation exercises, associate components of hierarchy with relaxation state 10. what does tin do in porcelain making? (has something to do with corrosion in amalgam) (In PFM, the metal has indium which is tin and iron - oxidative elements for porcelain to bond with alloy) - provide chemical bonding

11. diabetic patient what do you tell him prior to IV sedation? (TQ- about eating and medications) No eating or taking medication prior to sedation 12. ALOT of endo and ethics 13. Where is the A in cephalometric SNA - the deepest point in the maxillary concavity 14. know how to treat cytomegalovirus - Ganciclovir or valacyclovir 15. two questions on ectodermal dysplasia - sparse hair; missing teeth Ectodermal dysplasia = X-linked conditions in which there are abnormalities of 2 or more ectodermal structures (ex. Hair (sparse hair), teeth, nails, sweat glands (will have hypohydrotic child = sweating dysfunction, abnormal reduction of sweating due to heat), salivary glands, cranial-facial structure, digits). During tooth bud development, it frequently results in congenitally absent teeth (in many cases, a lack of a permanent set and/or in the growth of teeth that are peg-shaped or pointed.
Teeth develop abnormally causing anodontia or oligodontia (partial). Retained primary teeth. CONICAL shaped anterior teeth.
● Having hypodontia (FEWER number of teeth) will cause alveolar bone deficiency (prevent/undermine formation of alveolus)
● Less teeth, reduced alveolar ridge development so the vertical dimension of the lower face is reduced
16. radiograph showing dentinal dysplasia - normal color teeth, PARL, Short blunted apices
17. adrenal gland for hair loss 18. drug that prevents bleeding and fibrinolysis after surgical extraction - Tranexamic Acid? 19. know ludwigs angina - emergency Serious bilateral cellulitis (CT infection) of the floor of the mouth (submandibular and sublingual spaces), if left untreated may obstruct the airways and has complications including edema of glottis. 20. kid skeletal class 3 what most likely decreases with age? ANB
21. gingival floor most likely recurrent caries ● Gingival margin of class II through class V restorations is where the recurrent caries showed up
the most
22. better fracture resistance for amalgam: beveling Axio-Pulpal line angle Resistance: 1st = Flat floors, rounded angles (bevel in axiopulpal line angles to reduce stress and increase resistance) Retention: 1st = BL walls converge, 2nd = retention grooves/occlusal dovetail 23. Dovetail or beveling axio-pulpal line angle
- Dovetail occlusal = retention for amalgam - Beveling axio-pulpal line angle = resistance of fracture for amalgam
24. know substance P relation to opioids- substance P is pain receptor that is blocked by opioids
- Both endogenous opioids and somatostatin inhibit the release of substance P from central and peripheral endings.
25. Mandibular NOT Maxillary related to ear pain - high occlusion can refer pain to ear 26. Potassium (K+) sparing diuretics (Midamor, Dyrenium) 27. Lisinopril causes unproductive cough? Yes, Its an ACE Inhibitor. 28. Disadvantage of band and loop--------> No vertical occlusal stop 29. Posterior cross bite, where you should place the bands Lingual of maxillary and buccal of mandibular 30. Slob rule with vertical angulations - if same direction its lingual 31. What palatal groove is associated with the most periodontal disease? Palatogingival groove (or radicular lingual groove (RLG)) most common on maxillary lateral incisors 32. Bisphosphonates - for multiple myeloma 33. OS Instruments: -Max lateral - #65 Bayonet-shaped forceps or #150 maxillary universal forceps -Premolar- Mandibular → #74 ash forcep or #151A; Maxillary → #150 max universal -Cryer elevator and east/west elevator - to remove root tips in mandibular molars Day 2 is case studies: some said they kinda got rocked and the questions dealt a lot with Orthodontics. (6/05/19): -didn’t get specific questions from her (not that close to her lol) but did get the name of the docs she studied from and she said she had about 40% TQs from those on Day 1 but No TQs for Day 2 and that it was hard. -there was a lot of oral path and pharm -i also had a lot of ethics so reading the ADA code is really your best bet
June 2019:
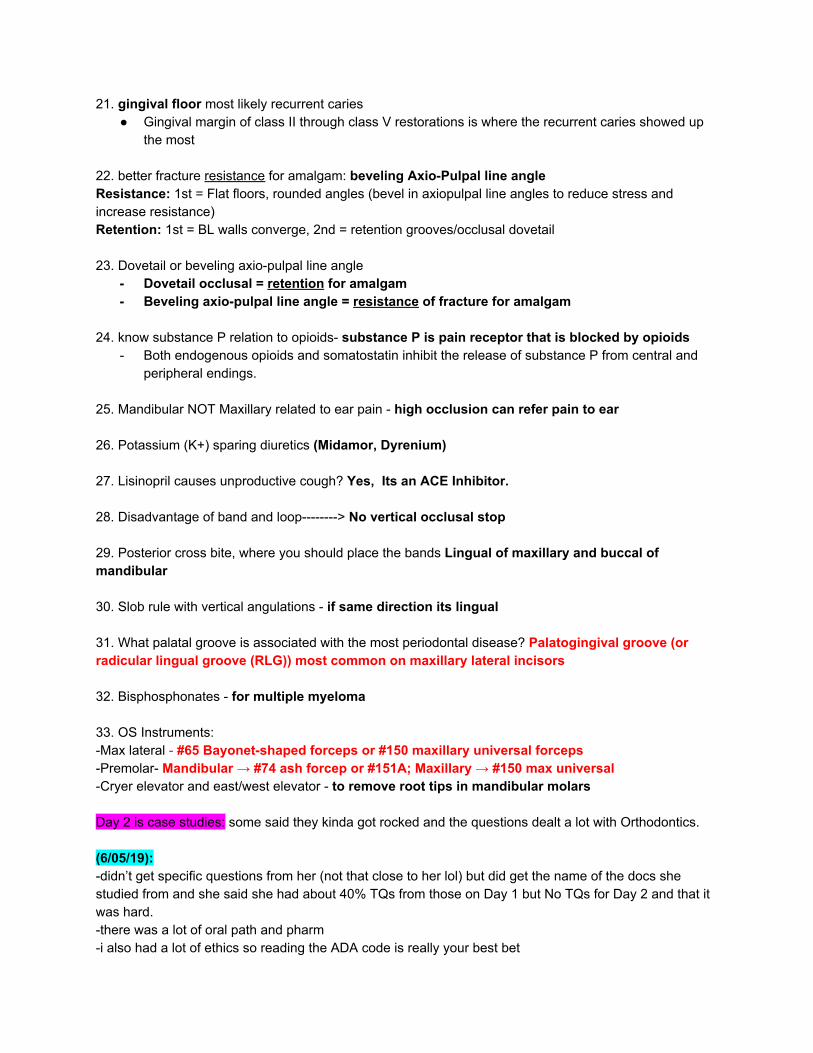
1.Know gemination, fusion and transposition
Gemination: Tooth gemination is a dental phenomenon that appears to be two teeth developed from one. There is one main crown with a cleft in it that, within the incisal third of the crown, looks like two teeth, though it is not two teeth. The number of the teeth in the arch will be normal. (1 root 2 crowns)
Fusion: Union of two adjacent teeth in both primary and permanent dentitions. The number of teeth in the arch will be one less. (2 roots 1 crown)
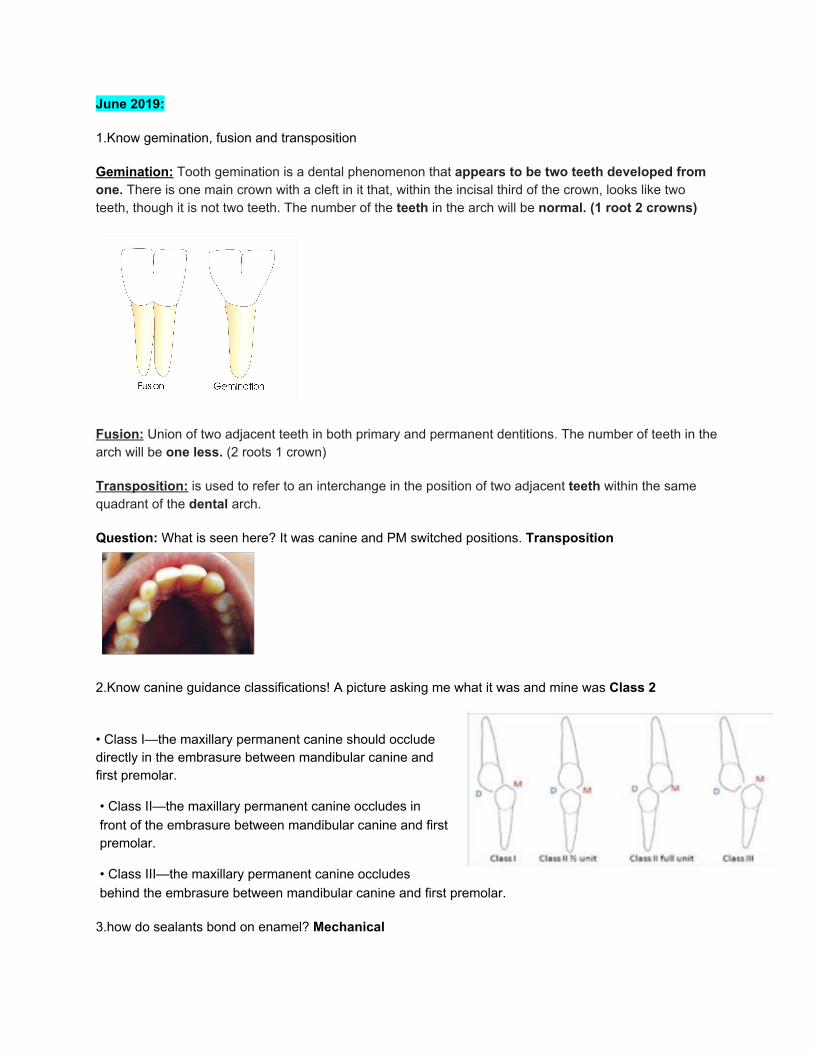
Transposition: is used to refer to an interchange in the position of two adjacent teeth within the same quadrant of the dental arch.
Question: What is seen here? It was canine and PM switched positions. Transposition
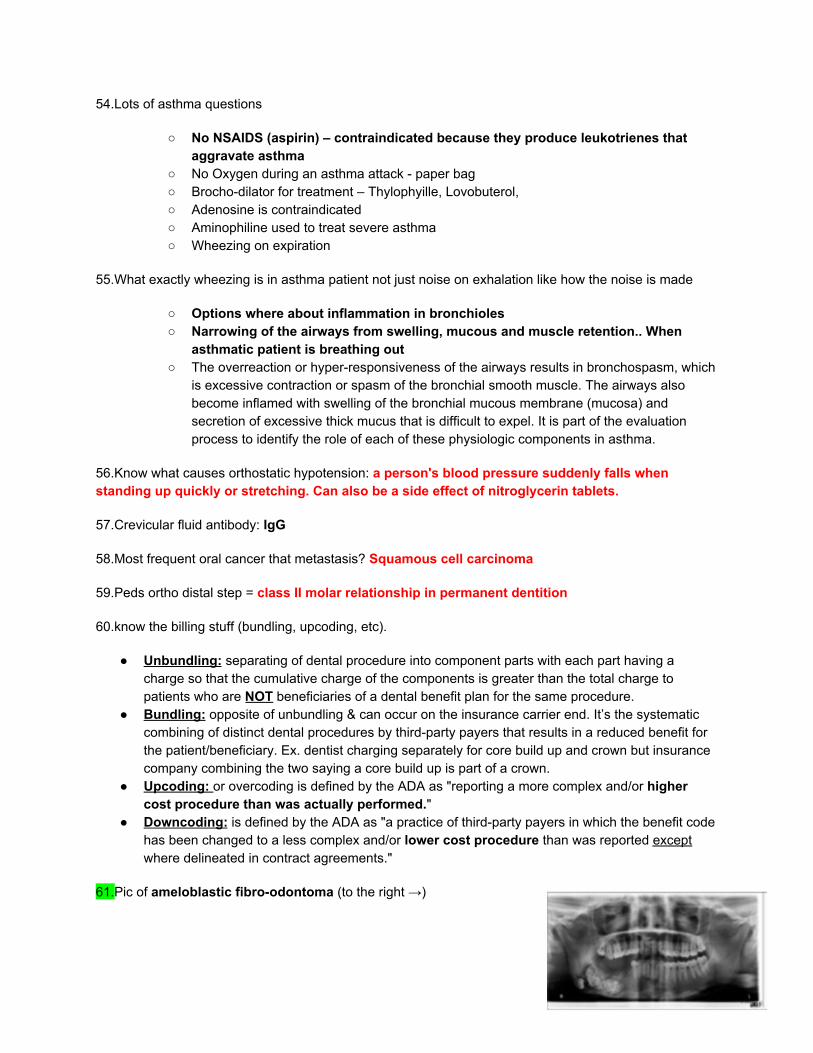
2.Know canine guidance classifications! A picture asking me what it was and mine was Class 2
• Class I—the maxillary permanent canine should occlude directly in the embrasure between mandibular canine and first premolar.
• Class II—the maxillary permanent canine occludes in front of the embrasure between mandibular canine and first premolar.
• Class III—the maxillary permanent canine occludes behind the embrasure between mandibular canine and first premolar.
3.how do sealants bond on enamel? Mechanical

4.Many questions with endo diagnosis of pulpal and apical. They were so easy and straightforward just know differences
○ know the symptoms for reversible, irreversible, and whether its necrosis. ■ Reversible Pulpitis: inflammation should resolve and the pulp return to normal;
response to thermal testing is severe, momentary pain lasting 1-2 sec after removal of stimulus
■ Symptomatic Irreversible Pulpitis: vital inflamed pulp is incapable of healing. Additional descriptors include: moderate to severe pain that lingers from thermal testing, spontaneous pain, referred pain.
■ Pulp Necrosis: indicates death of the dental pulp. The pulp is usually nonresponsive to pulp testing.
○ Know that percussion is how you diagnose if its symptomatic apical perio ○ Know chronic perio has a sinus tract ○ Know EPT doesn’t give you pulpal status nor does it not give you pulp health.
5.Patient with HIV gets refused for treatment by dentist, what does this violate from ADA code of conduct? Justice
○ (Know ALL codes of conduct I had diff examples about 7 questions)
6.Patient had crown and want to check pulpal diagnosis. What do you use? Thermal Test
7.How to distinguish endo lesion from perio lesion? Percussion
8.Silane coupling agents will bind with hydroxyl groups in filler.
● The silanols coordinate with metal hydroxyl groups on the inorganic surface to form an oxane bond with elimination of water.
9.What is EDTA? Chelating agent- removes smear layer (inorganic material)
10.What causes ankylosis? Replacement resorption
11.After RCT, you make a post space with drill and use paper point to dry canal. You see blood on paper point what does that mean? Ledge formed (was only option that would lead to a perforation)
12.Light transillumination shows both cracked tooth & craze lines*
○ Used for diagnosing cracked tooth. ○ Cracked tooth → only half of the tooth will light up (until it hits the fracture line) ○ Craze lines → the entire tooth will light up still
13.Max dose for 2% lidocaine with 1:100,000 epinephrine? 7 mg/kg for adult; 4.4 mg/kg for pediatrics
14.Critical pH of developing cavity? pH 5.5

15.What incision do you do on an edentulous patient to remove tori?Incision on ridge near tori and flap it
○ Vertical flaps ○ Incision on the tori ○ Incision on ridge near tori and flap it (I chose this because I know you avoid vertical
flaps on lingual because of Lingual n injury. You also don’t flap right on top of tori.) if patient has teeth the answer would include an incision around teeth in sulcus and then flap it.
16.What dental anomaly would result in a delay of eruption? Dilaceration
17.Which represents position on the spectral wavelength? Hue
18.When get infection in premolar mandibular area and lingual plate is intact and drains where? Buccal area?
○ Submental area (my brain was fried at this point and I was in between this and buccal area so didn’t care just chose this but not sure)
○ Submandibular area-----> would only drain here only if the tooth was a 2nd Molar or 3rd molar that have their roots BELOW the mylohyoid m. and the LINGUAL plate gets perforated from the periapical infection.
○ Sublingual area-----> would only drain here only if the tooth was a mandibular PM and 1st Molar that have their roots ABOVE the mylohyoid m. and the LINGUAL plate gets perforated from the periapical infection.
○ Buccal area------>should be this answer because the lingual plate was intact so it could not have drained in any of the areas listed above other than the buccal area.
19.Random questions, like what's "Shaping" for Behavioral management - providing positive reinforcement for the approximation of behavior you are trying to achieve
20.Difference in primary root size and permanent? Slender and longer roots
21.What lesion if it involved a tooth would widen the pdl? Osteosarcoma
22.Mandibular molar had 3 canals, took xray from mesial aspect what’s the order you see the canals? Mesial lingual-mesial buccal-distal
23.Primary teeth most often involved in perio? 1st mandibular molar
24.Another question order of primary teeth most affected by caries (listed in order) 1st Mandibular Molars > 1st Maxillary Molars > 2nd Mandibular Molars > 2nd Maxillary Molars
25.3 loss of attachment calculations - like probing 6mm, FGM 2mm apical to CEJ how much attachment was lost? 8mm
26.The proportional relationship of the width of the pontic in FPD. related to the width of the fpd span

27.what bacteria initiates caries? S. mutans
28.What bacteria progresses caries but doesn’t initiate them? lactobacillus
29.bacteria in perio of pregnant lady? Prevotella intermedia
30.Molecular mechanism of HPV? MOA for DNA Virus – inhibit proto-oncogenes P53, and works on human keratinocytes
31.articaine max carpules for 154 lb? 6 carpules
○ Articaine (4%) – 7mg/kg max recommended dose ■ 154/2.2 = 70kg ■ 70 x 7mg = 490 ■ 490/72 = 6.88888
32.Recommended tylenol dose for kids per day (25-50 3x a day?)? 5x daily Tylenol (10-15mg every 4-6 hours)
33.Something about a buccal vestibulopathy what kind of dissection? supraperiosteal
○ Vestibuloplasty – can be performed to increase the depth of the vestibule using skin grafts – used for denture/RPD fabrication
○ Incision made on the alveolar ridge and a supraperiosteal dissection is made to the depth.
34.Insulin short acting = lispro, Aspart & Glulisine
○ Short Acting: Lispro (15mins), Aspart (15min), Glulisine (15min) ○ Long Acting: NPH (1-4hr), Glargine (1-4hr), Detemir (1-4hr)
35.Glass ionomer polyacrylic Acid → is the ionomer portion of the GI
36.A couple questions on molar up righting → will cause interference in occlusion/need to fix occlusion
37.A few questions on glass ionomer (advantages/how it works)
○ Low stress bearing areas ○ Less wear resistance ○ Releases fluoride ○ High Caries Risk patients – Class V
38.Labial bow does what? Labial bow in retainer retrudes the anterior teeth
○ Is present anterior to the maxillary incisors, extending distally to eliminate the pressure from the buccal musculature – metal part that lays flush across the anterior incisors.

39.One advantage of External vs internal splint? allow healing of the PDL, maintain tooth position
○ Internal Splint – inside cavity pre ○ External Splint – No involving tooth preparation, usually confined to anterior teeth – allow
healing of the pdL, maintain tooth position
40.Class 2 girl ANB will be larger? ANB
○ ANB – 2 to 4 degrees Class I ○ >5 degrees Class II ○ <1 degree Class III
41.Epinephrine Amount for anaphylaxis? 0.3
○ 0.2 to 0.5 adults to treat anaphylaxis ○ .01 mL kids to treat anaphylaxis
42.Tipping questions (ortho)
○ Easiest/fastest tooth movement ○ Center of rotation at root apex
43.Most common reason to not do distal wedge? Not enough keratinized tissue
44.What gets numbed with IAN and what gets numbed with lingual?
○ IAN – Everything, but soft tissue of the molars ○ Lingual - lingual gingiva and adjacent mucosa of the mandible
45.Bohn nodules
○ Multiple small gingival nodules resulting from cystification of rests of dental lamina.
○ Cysts of newborns
46.Macrocytic anemia is vitamin B deficiency
○ Microcytic – Iron deficiency ○ B-12 – Pernicious anemia ○ Aplastic Anemia – Bone Marrow defect/Not enough new blood cells
47.Why do you bag instruments before sterilizing? To allow them to remain sterilized after the cycle
48.Picture of geographic tongue (it was a picture with only lateral border of tongue showing and looked like similar to SCC but wasn’t they were tricky) it affects the filiform papilla

49. X-ray zygomatic process (yellow line on pano →)
50.Two different questions pointing to pano saying what is this radiolucent line indicating? Airspace (its when patient doesn’t put tongue on roof of mouth and creates airspace)
51.X-ray transposition (lateral and canine switched in x-ray →)
○ When teeth within the same quadrant switch position – difficult to treat
52.X-ray taurodontism (enlarged pulp chamber as seen below)
53.Gingival margin trimmer vs hatchet: Both Enamel Hatchet and Gingival Margin Trimmer are hatches but GMT has curved blade and angled cutting edge while Enamel Hatchet has cutting edge in plane of handle. Main advantage of using GMT is the curved angle of the blade
● Gingival margin trimmer – designed to produce a proper bevel on gingival enamel margins of proximo-occlusal preparations. The blade is curved (similar to a spoon excavator) and the primary cutting edge is at an angle to the axis of the blade.
● Hatchet – The ordinary hatchet has the cutting edge of the blade directed in the same plane as that of the long axis of the handle and is bibeveled; used primarily on anterior teeth for preparing retentive areas.
54.Lots of asthma questions
○ No NSAIDS (aspirin) – contraindicated because they produce leukotrienes that aggravate asthma
○ No Oxygen during an asthma attack - paper bag ○ Brocho-dilator for treatment – Thylophyille, Lovobuterol, ○ Adenosine is contraindicated ○ Aminophiline used to treat severe asthma ○ Wheezing on expiration
55.What exactly wheezing is in asthma patient not just noise on exhalation like how the noise is made
○ Options where about inflammation in bronchioles ○ Narrowing of the airways from swelling, mucous and muscle retention.. When
asthmatic patient is breathing out ○ The overreaction or hyper-responsiveness of the airways results in bronchospasm, which
is excessive contraction or spasm of the bronchial smooth muscle. The airways also become inflamed with swelling of the bronchial mucous membrane (mucosa) and secretion of excessive thick mucus that is difficult to expel. It is part of the evaluation process to identify the role of each of these physiologic components in asthma.
56.Know what causes orthostatic hypotension: a person's blood pressure suddenly falls when standing up quickly or stretching. Can also be a side effect of nitroglycerin tablets.
57.Crevicular fluid antibody: IgG
58.Most frequent oral cancer that metastasis? Squamous cell carcinoma
59.Peds ortho distal step = class II molar relationship in permanent dentition
60.know the billing stuff (bundling, upcoding, etc).
● Unbundling: separating of dental procedure into component parts with each part having a charge so that the cumulative charge of the components is greater than the total charge to patients who are NOT beneficiaries of a dental benefit plan for the same procedure.
● Bundling: opposite of unbundling & can occur on the insurance carrier end. It’s the systematic combining of distinct dental procedures by third-party payers that results in a reduced benefit for the patient/beneficiary. Ex. dentist charging separately for core build up and crown but insurance company combining the two saying a core build up is part of a crown.
● Upcoding: or overcoding is defined by the ADA as "reporting a more complex and/or higher cost procedure than was actually performed."
● Downcoding: is defined by the ADA as "a practice of third-party payers in which the benefit code has been changed to a less complex and/or lower cost procedure than was reported except where delineated in contract agreements."
61.Pic of ameloblastic fibro-odontoma (to the right →)
62.Mostly hypertensive meds, diabetes, and hypothyroidism
63.Mumps transmission includes? Airborne pathogen
64.Why is heparin given IV?
○ Contraindicated IM – due to hematomas, pain ○ To reverse heparin you give protamine sulfate ○ CI with Ginko Biloba
65.If you compare the radiation dose of person working in nuclear power plant and that of a dental assistant (or whoever takes x-ray in a dental setting), how much will the dosage of that person be? 1/5 times of the nuclear worker (question and answer from DanMan file 2019 question 724)
○ 50msv/year (0.05sv/year)– is the standard that people should have (the max radiation dosage for a dental professional per year)
○ Workers of nuclear plant, how much radiation permitted yearly = 5 rem/ 5000 mrem yearly (on average, a nuclear worker receives approx. 150 mrem (0.15 rem) of occupational exposure a year)
○ 1 sv = 100 rem
66.Leukoedema?
○ Bi-lateral opacification of the buccal mucosa ○ Goes away when you stretch it
67. Not a reason why a post would break- because of the material of the post
○ (yes to not enough ferrule, parafunctional habits, occlusion).
68. MOA montelukast- is a selective leukotriene receptor antagonist of the cysteinyl leukotriene CysLT 1 receptor which blocks leukotrienes activities to cause asthma symptoms.
○ Leukotriene receptor antagonist used to treat asthma and seasonal allergies ○ Montelukast inhibits bronchoconstriction due to antigen challenge.
Day 2
1.Old women 86 years old came in with dry mouth, red inflamed tongue with white stuff that wipes off. Her chief complaint was lower left PM area was in extreme spontaneous pain. What was the cause?
○ Xray was pano, you had to squint and see that there was radiolucency around apex, answer was symptomatic apical periodontitis
○ What was her tongue issue? Candidiasis, lichen planus. ○ Her son called and said she fell on ice and chipped composite that was distal of #8,
which you again had to squint and see it was small, and only a small composite. What do you do? I said replace composite. Options had full ceramic crown, veneer. I thought since she’s old and it was a small composite you wouldn’t just do a crown for it.

○ What would be the least thing you would use for a placement of crown #18? Field Porcelain crown
2. 25 year old male came in with meds amitriptyline for depression. Chief complaint is lump on post palate. He also had lesions on tongue. cross bite on right.
○ what angle classification is he? ■ Class 1 ■ Class 2 mod 1 ■ Class 2 mod 2 (it was hard to tell but he was def this)
○ What can be done to fix his cross bite? ■ Buccal tipping of max (his teeth were lingually tipped and pushing them buccal
would resolve it) ○ Why was his enamel white spotted?
■ Amelogenesis imperfecta ■ Dentinogenesis imperfect ■ Fluorosis ■ I was in between fluorosis and amelogenesis
imperfecta. I chose Fluorosis because it didn’t seem so bad like a defect in enamel. Looked similar to this nothing severe
3.Patient came in with cervical lesions and smoking for 22 packs/years with crazy amount of cavities. #8 RCT and lingual amalgam. Know if medications cause xerosomia or was it smoking 22 packs a year.
4.Mechanism of ibuprofen- Non-selective cox-1 & cox- 2 that Reversibly Binds
5.Mechanism of carbamazepine- sodium channel blocker
○ Tx: Trigeminal Neuralgia and Manic depressive illness
6.RPD design which one can’t you do for distal extension of 29. 29 has existing DO composite, what would you do for RPD? Change restoration to amalgam or Survey crown
7.Rita case
8.Man was shot. Wife is his caregiver? because he’s legally incompetent.
9.Old lady with ugly teeth but good bones and gums? gingivitis?
● She also was on a million meds and had impacted third molars and pain in left premolar vestibule and lower lip but couldn’t see shit in pano.. what was the cause of pain? Periocoronitis, abscess of premolar, cyst of third molars referred pain
● Other dentist told old lady to get veneers on 5 and 12, what do you tell her? “If you’re interested in cosmetics let me tell you all your options”

10.Girl with a million piercings in pano, 24 and 25 feel loose? due to trauma of tongue ring
○ first step- patient education ○ identify tongue ring in pano
11.Canine classifications!
○ Class 1: when the mesial slope of the maxillary canine coincides with the distal slope of the mandibular canine. Maxillary Canine sits perfectly in the embrasure space between the mandibular 1st PM and canine.
12.Crossbite due to what?
○ Angle Class III malocclusion usually associated with anterior cross bite ■ Reverse Overjet – Anterior crossbite (usually class III)
○ Posterior Crossbite ■ Dental – patient with adequate palatal width ■ Skeletal – inadequate palatal width
○ Unilateral crossbites are usually due to a mandibular shift
13. Not ideal overjet and overbite due to what? Pacifiers and Finger Sucking or Primary Canine Loss
○ Pacifiers and finger sucking may cause increased overjet, decreased overbite and posterior crossbite
○ Primary canine loss – increased overbite – after lingual collapse, the mandibular incisors erupt further, increasing overbite.
14.Kid with ADHD
○ Medication could be: ■ Methylphenidate (Concerta, Ritalin, Metadate)
■ Nausea, hypertension ■ Atomoxetine (Straterra)
■ Hypertension, dry mouth, nausea ■ Amphetamine/dextroamphetamine (Adderall)
■ Adverse: Dry mouth, headache, nausea, hypertension ○ Treatment Modifications:
■ Depends on age and severity ■ Shorter Appointments ■ Step-by-Step verbal reinforcement
June 2019: 1.Ankylosis → replacement resorption 2.Apex closes → 2.5- 3.5 years after eruption
3.Freys Syndrome - auriculotemporal syndrome when nerve is damaged causing sympathetic fibers to cause eating and flushing of the face, while parasympathetic fibers cause increase in salivation unilaterally. Use minor’s starch- iodine test. Treatment includes surgery, atropine medication (local injections) and scopolamine creams. 4.Potassium (K+) sparing diuretics: Midamor and Dyrenium 5.root caries → glass ionomer 6.glass ionomer → zinc oxide (acts as the antibacterial activity when added to glass ionomer cement) 7.LED composite light vs halogen curing light: LED curing light faster for curing materials and more lightweight, portable, and effective compared to the halogen curing lights. What is NOT an advantage of LED cure in comparison to Halogen? Curing Depth
● LED: produce a blue light in the 400-500 nm range, with a peak wavelength of about 460nm. They are more lightweight, portable and effective compared to the halogen curing lights. They produce less heat and do not require a fan to cool it. LED curing lights cure material much faster than halogen lamps. Light intensity is 1,000 mW/cm2
● Halogen: most frequent polymerization source used in dental offices. It provides a blue light between 400- 500nm, with an intensity of 400-600 mW/cm2. Drawbacks include: large amount of heat it generates so it needs a built in ventilating fan, larger unit, must be plugged in (cannot be cordless), time needed to fully cure the material is much more than the LED curing light.
8.Monteleukast leukotrienes - inhibit leukotrienes for the treatment of asthma 9.Sulfonamide - compete with PABA in folic acid synthesis, decreasing folic acid 10.Sulfonylureas → increase insulin release from beta cells of pancreas 11.beta 1 agonist doesn’t do what? Doesn’t act as a smooth muscle relaxant to be used for treating asthma or COPD (that is Beta-2 Agonists job)
● Beta-1 agonist ARE medications that increases the heart rate and blood pressure. Beta-1 agonists stimulate adenylyl cyclase activity and opening of calcium channels. Cardiac stimulants.
● Beta-1 agonists are used for Bradycardia (slow heart rate), Bradyarrhythmias, Acute Heart Failure and Cardiogenic Shock.
12.acute herpetic gingivostomatitis → primary herpes, HSV 1 or 2, children and adults ● Symptoms include: Malaise, fever, lymphadenopathy, vesicles in oral cavity, gingival
swelling/erythema, can remain latent, reactivation with UV exposure/ trauma/ immunosuppression
13.infective mononucleosis - EBV 14.ludwigs angina → emergency
● Serious bilateral cellulitis (CT infection) of the floor of the mouth (submandibular and sublingual spaces), if left untreated may obstruct the airways and has complications including edema of glottis.

15.cleidocranial dysplasia vs. mandibulofacial Dysostosis (MDF) AKA Treacher Collins Syndrome: With Treacher collins syndrome (MDF) patient will have hypoplasia (missing) zygomatic bone whereas with Cleidocranial dysplasia the patient will have hypoplasia (missing) clavicle.
● Cleidocranial Dysplasia: Multiple unerupted supernumerary teeth, Retention of primary teeth, delayed eruption of permanent teeth, Missing clavicle. It is the delayed ossification of midline structures. Will give you very narrow facial structures.
● Mandibulofacial Dysostosis (MDF) (Treacher Collins Syndrome): Mandibular hypoplasia, malformed ear, lower eyelids, ear pinna. No mental retardation associated with the syndrome. Will have ear abnormalities. Loss (hypoplasia) of the zygomatic bone.
16.whose most likely to need general anesthesia? 2 year old with early childhood caries 17.anterior crossbite non skeletal caused by what? Maxillary tipping lingual and mandibular tipping buccal (Angles class III Malocclusion)
● Skeletal deformation: Maxilla not completely developed (most common tooth involved is maxillary lateral, fix this ASAP regardless of age)
● Non skeletal deformation: Maxillary tipping lingual, and mandibular tipping buccal (Angles Class III malocclusion)
18.class III furcation down to within 5mm of apex → extract and implant 19.what’s the max dose of lidocaine (in mg) for a 12 year old thats 16 kg? 70.4mg of lidocaine
● Math: 16kg X (4.4 mg/kg) =70.4 mg June 11th & 12th ***Do Mastermind (everyone who claimed they had the shitty version of the exam and had no TQs later on found out that a lot of the TQs were on this document that they hadn’t looked at…. So basically do Mastermind and Super doc and you will be gucci) 1.Bimaxillary protrusion know what it is. (Two questions)
● one a definition: Bimaxillary protrusion refers to a protrusive dentoalveolar position of maxillary and mandibular dental arches that produces a convex facial profile. both mandibular and maxillary dentoalveolar protruding.
● one was an answer of when to use class 2 correcting maxilla gear? Bimaxillary Protrusion
2.Seizures - encephalotrigeminal telangiectasia 3.Cognitive restructuring? psychotherapeutic process of learning to identify and dispute irrational or maladaptive thoughts (talking about everything you’re afraid of)
4.Ameloblastoma vs fibroma: Ameloblastoma is a true odontogenic tumor whereas Fibroma is a connective tissue tumor that is NOT really a tumor.
● Ameloblastoma: most common TRUE odontogenic tumor, benign but aggressive. Multilocular radiolucency, superimposed over posterior teeth and more common in the posterior mandible. Often associated with impacted teeth.
● Fibroma: most common CT tumor, Reactive, NOT TRUE tumor. Caused by chronic trauma or irritation. Fibrous hyperplasia of oral mucosa. (could be keratinized white nodule on palate) Firm, smooth, pink, elevated papule/nodule. Common site is the TONGUE → due to trauma.
5.Primary first mandibular for most cause of space loss mandibular 2nd molar cause of space loss. ● Premature loss of posterior teeth priority: 2nd Molar > 1st Molar > Canine > Incisor
6.Least recurring: irritational fibroma (is most common CT tumor) AOT (Adenomatoid Odontogenic Tumor) 7.Lamina dura = 6 weeks in utero 8.Which one affects saliva production when using alpha? It will act on nicotinic or muscarinic ganglion -Anticholinergics MOA = inhibit binding of acetylcholine to muscarinic and nicotinic receptors. These receptors are found in eye, secretory glands and nerve endings to smooth muscle cells. 9.PMN (Neutrophils) In crevicular fluid of periodontitis 10.Which orthodontic appliance is tissue and tooth? Nance appliance (NOT quad helix) 11.What doesn’t cause Hypertension? Corticosteroids? - No they cause drug-induced hypertension- TR; maybe Mecamylamine and Hexamethonium that are ganglionic blockers and produce orthostatic HYPOtension? -TR 12.Ethics exceeds legal duties 13.Stimulus changes behavior for modification 14.What % of MB2 root in maxillary 1st molar? 20,40,60,80
● Maxillary 1st Molar: 40% for 3 roots, 60% for 4 roots 15. Macroglossia caused by all the following except? amyloidosis, hypothyroidism, acromegaly, or hyperparathyroidism 16.Lateral perio cyst → roots of mandibular premolars 17.Neurofibroma → mandibular Premolars 18. What’s stronger ibuprofen 600 or Tylenol 500------> you need RX for Ibuprofen 600mg 19.Lower canine facially positioned - gingival recession 20.What’s not causing her recession on 6? Systemic - (yes was brush,erosion, ortho)

21.Diabetes type 1- ketoacidosis with hyperglycemia (ketone breath) 22. Most common dental emergency- syncope 23.Most common lymphoma of the jaw? The most common Primary Intraosseous Lymphoma is non-Hodgkin's large cell type. 24.Histoplasmosis resembles ? Recurrent herpes, painful ulcers look like cancer 25.Side effects of nitroglycerin - headache, orthostatic hypotension, flushing 26.Multiple neuro sarcomas in what disease? Neurofibromatosis (Von Recklinghausen’s disease) 27.Lower Canine far facially positioned- mobility or recession? Recession 28.40 year old posterior crossbite- surgery? Palatal expander - Surgery (Suture osteotomy?) 29.Mucocele - what to do? Exfoliative biopsy? Excisional, incisional 30.Patient need analgesic- to give except: ibuprofen, tramadol, Tylenol, Tylenol 3.... I put tramadol, but it may be Tylenol 3?
● Tramadol monotherapy does not usually provide adequate analgesia. 31.Too dark pic- too much developer 32.Little contrast and light pic: too little exposure time 33.Least affected by water? Pvs, siloxane, polyether 34.Intrusion: wait to erupt or splint ? reposition and splint if permanent tooth intruded 5mm 35.Where ankylosis happens- external replacement Replacement resorption 36.Symptoms of Transient Ischemic Attack (TIA) → tingling fingers light headed and disoriented then pass out 37.Most common neoplasm → adenocarcinoma 38.Tylenol and aspirin are antipyretic and analgesic (anti inflammatory never tylenol) 39.ORN mandible only 40.Know clinical trial
● Use randomization and blinding to compare effects of treatment with non-treatment. This is the Gold Standard for establishing cause and effect. Trials to evaluate the effectiveness and safety of medications or medical devices by monitoring their effects on large groups of people.

41.Know cross sectional Vs cohort → cross sectional studies cannot distinguish between cause and effect whereas cohort studies can.
● Cross sectional: epidemiological study that looks at the entire population at one point in time. Cross sectional studies are used to determine prevalence. They are relatively quick and easy but do NOT permit distinction between cause and effect.
● Cohort: prospective study of one or more samples. Cohort studies are used to study incidence, causes, and prognosis. Because they measure events in chronological order they can be used to distinguish between cause and effect.
42. Where to detect furcation maxillary molar- midfacial, mesiopalatal, mid distal 43.Know modified Widman flap uses and procedure
● it’s full thickness ● Expose roots for planing to have direct vision.
44.First sign of multiple myeloma - bone pain 45.Distractive osteogenesis (DO) is hard because of time (long term follow up; 2 hospital procedures) and patient/parent compliance 46.Potassium (K+) sparing diuretic- spironolactone (also aldosterone antagonist), also Midamor and Dyrenium 47.If patient had kidney dialysis when do you dentally treat them? 1 day after 48.Short abutment in FPD- what to do? Full crown (for better retention), reverse 3/4 crown, inlay, or onlay? 49.AOT → rare recurrence 50.10-21 days before early periodontitis (initial early established ) July 2019 1.Retruded tongue- problem with retaining mandibular denture
● If the tongue is in a retruded position, the denture will be unstable, has no retention and will be easily dislodged.
2.Remove hyperplastic tissue → before fabricating new complete denture 3.Flabby tuberosities-resect 4.Lateral sliding flap- increase attached gingiva for anteriors (AKA pedicle flap) 5.neurapraxia definition = mild injury with not axonal damage, spontaneous recovery within 4 weeks
● Neurapraxia is a disorder of the peripheral nervous system in which there is a temporary loss of motor and sensory function due to blockage of nerve conduction, usually lasting an average of six to eight weeks before full recovery.
6.First treatment for NUG- Chlorhexidine rinse with Debridement (only give antibiotics if patient has systemic disease like HIV or is running a fever)----> If ABX needed, use Metronidazole 7.Best area for osseointegration - mandibular anterior 8.Triad- glossoptosis, retrognathic mandibular, micrognathia (also high arch palate, cleft palate or absent gag reflex) - Pierre Robin Syndrome 9.Phenothiazide - tardive dyskinesia 10.Kelly Combination syndrome - when you have a maxillary complete denture over mandibular Class 1 Kennedy RPD.
● Has 5 characteristics: overgrowth of maxillary tuberosity, papillary hyperplasia of hard palate, bone loss in maxillary anterior, mandibular anteriors super erupt, and bone loss under distal extension of mandibular
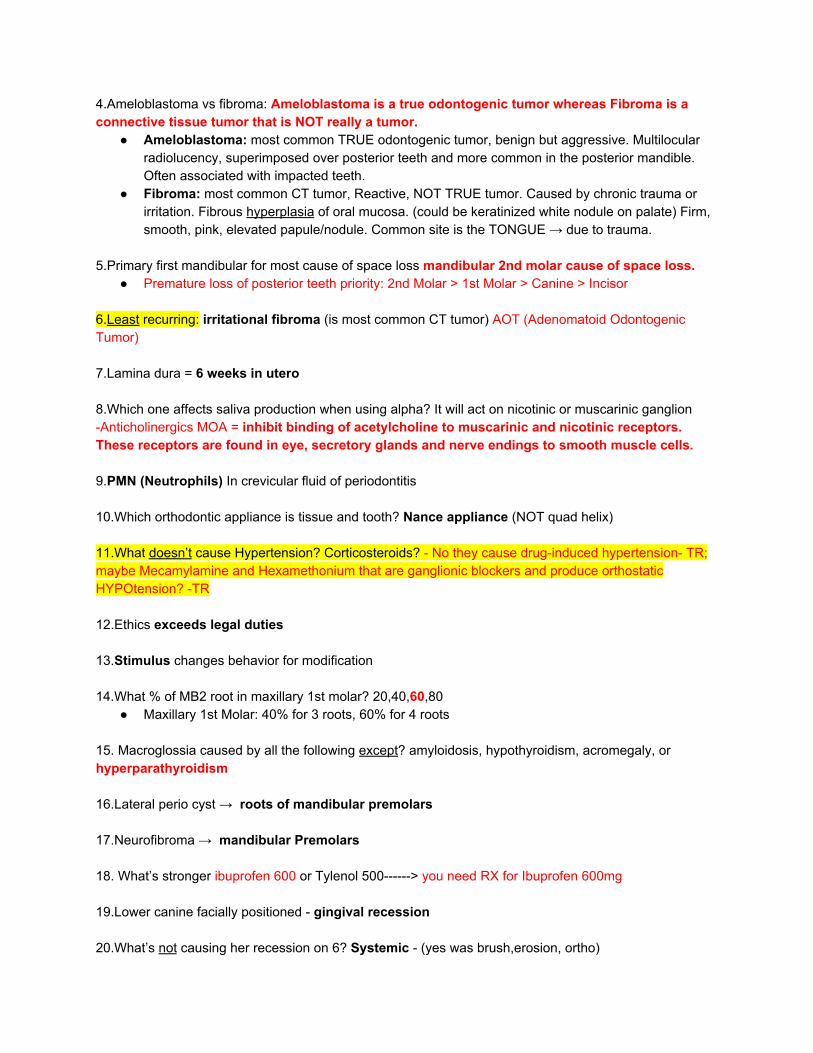
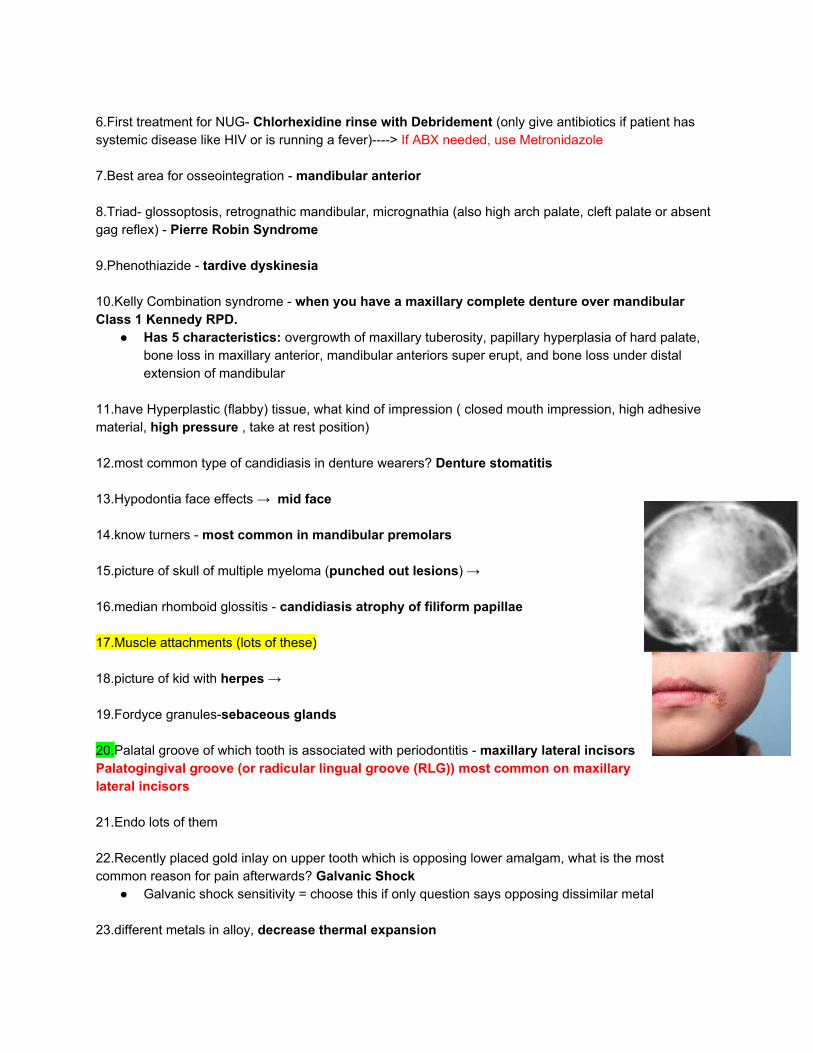
11.have Hyperplastic (flabby) tissue, what kind of impression ( closed mouth impression, high adhesive material, high pressure , take at rest position) 12.most common type of candidiasis in denture wearers? Denture stomatitis 13.Hypodontia face effects → mid face 14.know turners - most common in mandibular premolars 15.picture of skull of multiple myeloma (punched out lesions) → 16.median rhomboid glossitis - candidiasis atrophy of filiform papillae 17.Muscle attachments (lots of these) 18.picture of kid with herpes → 19.Fordyce granules-sebaceous glands 20.Palatal groove of which tooth is associated with periodontitis - maxillary lateral incisors Palatogingival groove (or radicular lingual groove (RLG)) most common on maxillary lateral incisors 21.Endo lots of them 22.Recently placed gold inlay on upper tooth which is opposing lower amalgam, what is the most common reason for pain afterwards? Galvanic Shock
● Galvanic shock sensitivity = choose this if only question says opposing dissimilar metal 23.different metals in alloy, decrease thermal expansion

24.Tooth #30 has huge MOD amalgam that is deep, it hurts when he eats french bread. What is the cause? Root Fracture (Fractured Tooth) 25.know signs of shock (see list below)
● Cool, clammy skin ● Pale or ashen skin ● Rapid pulse ● Rapid breathing ● Nausea or vomiting ● Enlarged pupils ● Weakness or fatigue ● Dizziness or fainting ● Changes in mental status or behavior, such as anxiousness or agitation
26.know MOA of propranolol - non selective beta blocker that reduces cardiac output and inhibits renin secretion
27.Ptergonandibular raphe ! 4 questions! Know their muscles (mesial is the mouth, lateral is the ramus, anterior is the buccinator, and posterior is the superior pharyngeal constrictor) 28.needle is inserted where in IANB. (muscle - buccinator, infection - pterygomandibular space) 29.Dentinal dysplasia (DD) vs dentinogenesis imperfecta (DI) vs Amelogenesis imperfecta (AI) = Amelogenesis imperfecta affects the ENAMEL of teeth, Dentinogenesis imperfecta and Dentinal Dysplasia both affect the DENTIN of teeth. Imperfectas (DI & AI) can be treated with restorations whereas Dentinal Dysplasia CANNOT.
● Dentinal Dysplasia: Loss in organization of dentin in primary and permanent teeth. It is Autosomal Dominant and has 2 types. Teeth are NOT good candidates for restorations.
○ Type 1 “rootless teeth”. Normal coronal enamel and dentin, roots shortened due to disorganized radicular dentin, teeth mobile and premature exfoliation. Chevron pulps and short roots in permanent dentition; obliterated pulp chambers in primary teeth.
○ Type 2 (resembles dentinogenesis imperfecta) in that root length is normal, but crowns are blue-brown translucent, bulbous, and have cervical constriction. Again primary teeth have obliterated pulp; permanent teeth have thistle tube and contain pulp stones.
● Dentinogenesis Imperfecta (DI): Autosomal Dominant, affects formation of dentin, may be seen with osteogenesis imperfecta. Has blue brown discoloration/translucence (Blue Sclera), bulbous crowns with cervical constriction and early obliteration of pulp and canals. Shell tooth appearance (normal enamel, thin dentin, large pulp chamber). Teeth are very prone to damage and breakage like with amelogenesis imperfecta. Treatment for these teeth include full coverage of teeth with close to normal shaped crowns and roots, overlay denture.
● Amelogenesis Imperfecta (AI): Amelogenesis imperfecta is a group of rare genetic conditions in which the outer layer of the teeth (enamel) fails to develop properly. People with amelogenesis imperfecta will have small, yellow, or brown teeth that are very prone to damage and breakage. They will show rapid attrition, excessive calculus deposition and gingival hyperplasia. Is usually Autosomal Dominant. Can cause hypoplastic pitting enamel.
30.SNA/ SNB ● SNA This angle represents the relative anterioposterior position of the maxilla to the cranial base ● SNB This angle represents the relative anterioposterior position of the mandible to the cranial
base ● SNA-SNB = ANB which is the angle that represents the relative A/P position of the maxilla to the
mandible and is used to find skeletal class. Normal ANB is 2-3 degrees. (Class I) 31.which did point A stand for ? deepest concavity of maxilla 32.Which LA for a pregnant person? Mepivacaine (no epinephrine in it therefore no Vasoconstrictive properties) 33.Which doesn’t involve ions- propranolol 34.Amicar- what is it? aminocaproic acid is used to promote blood clotting, used during or after surgery when excessive bleeding is expected. 35.Benzodiazepines MOA → (Key word is FREQUENCY) Enhance GABA binding to GABA receptor, increase frequency of chloride channel opening → decrease neuronal firing 36.Know recall interval for periodontitis in adults - 3 months 37. Ulcerated papilla- NUG (ANUG) 38.sedation of pulp- zinc eugenol 39.when do you not use calcium hydroxide? is contraindicated in pulpotomy in a child (primary teeth) because it causes irritation of the pulp, leading to internal resorption in primary teeth; also contraindicated in adults whose pulp has been symptomatic for the last month. 40.Difference between treatment for aggressive periodontitis and NUG - attachment loss is seen much more in aggressive periodontitis.
● The treatment difference would be the use of ANTIBIOTICS. For Aggressive periodontitis you do Surgery (SRP) with Tetracycline, Metronidazole w/ amoxicillin (different combo of antibiotics) whereas with NUG you start with Debridement, Chlorhexidine rinse and OHI (and only prescribe antibiotics if pt has HIV or fever)
41.Root canal obliteration (calcified canal) → Pulp canal obliteration (calcified canal) does not, in itself, indicate need for treatment. It is seen in Dentinogenesis imperfecta and dentinal dysplasia. 42.Amyloidosis is? disease that occurs when a substance called amyloid builds up in your organs. Oral manifestations are Macroglossia, decreased mobility, yellow nodule on lateral surface. Also has deposition on salivary gland leading to xerostomia.

43. pic of pedunculated wart 44.ankylosis or pulpal obliteration if extraoral dry time is long 45.Root canal response times
● Vitality Scanner (EPT) ○ Normal response ranges are: Incisors 10–40, Bicuspids 20–50, Molars 30–70, Necrotic
80 46.Addison’s - hypotension, hyperpigmentation due to adrenal insufficiency 47.Peutz-Jegher’s Syndrome- internal polyps 48.hypercementosis and possibly hyperparathyroidism
● Hypercementosis: excess deposition of cementum on normal radicular cementum. ● Hyperparathyroidism: is a condition in which one or more of the parathyroid glands become
overactive and secrete too much parathyroid hormone (PTH). This causes the levels of calcium in the blood to rise, a condition known as hypercalcemia. (Secondary HPT caused by renal failure)
49.Type of Anchorage and diastema closure - finger springs for mesiodistal tipping 50.rectangular wire purpose - movement of crown and root 51. indirect sympathomimetic - amphetamines, tyramines, ephedrine 52. CDC or EPA for controlling water lines 53.pubertal gingivitis and treatment- OHI 54. Definition of chronic abscess - (key word is SINUS TRACT) Chronic Apical Abscess is an inflammatory reaction to pulpal infection and necrosis characterized by gradual onset, little or no discomfort and an intermittent discharge of pus through an associated sinus tract. 55. Turn over if long junctional epithelium → Will be formed on cementum & is re-established in 1-3 weeks 56. Black men not correct for HPV highest incidence----> White girls 57. Ferric sulfate left at apex. What will happen to it? Ferric sulphate, produces local and reversible inflammatory response to oral soft tissues, but no toxic or harmful effects have been published in dental or medical literature.The most common radiographic finding seen was internal resorption and calcific metamorphosis. Ferric sulfate is a very strong haemostatic agent.
58. lateral translation mounted in semi- adjustable articulate, what movement will make---> White gurls ● Working side contact during laterotrusion ● Lateral translation movement or bennett angle
○ Bennett angle → angle described by the orbiting condyle during laterotrusive movements. Semi-adjustable articulators allow for a bennett angle movement only in a straight line.
59. occlusal waxing? 60. neurapraxia= mild injury with not axonal damage, spontaneous recovery within 4 weeks 61. acute radiation exposure symptoms = nausea, vomiting, headache, and diarrhea 62. amantadine- antiviral and antiparkinson 63. Naloxone what type of intrinsic and affinity = NO intrinsic activity, HIGH Affinity
● Used to treat morphine (opioid) overdose, antagonist 64. multiple questions on sign of opioid overdose
● Symptoms: respiratory depression, euphoria, sedation, dysphoria (unease), analgesia, antitussive, constipation, urinary retention, vomiting/nausea (trigger medullary CTZ)
● Overdose: coma, miosis (pupil constrict, pin-point pupils), hypothermia, respiratory depression (loss of sensitivity of medullary respiratory center to CO2), hypotension
65. side effects of nitroglycerin = headache, orthostatic hypotension, flushing 66. enlarged skull, dementia .... what syndrome? Alzheimer’s 67. Type of radiation for MRI----> Radiowaves 68. Bunch of questions about articulator settings 69. Red complex bacteria = P. gingivalis, Tannerella forsythia, treponema denticola 70. NUG with fever and lymphadenopathy do all except? chemotherapeutic rinse, debridement, steroids, antibiotics (such as penicillin or metronidazole) 71. Most likely type of root to have a ledge (short, long, curved, thin) 72. Know all about specificity, sensitivity
● Specificity: percent of persons without the disease who are correctly classified as not having it ○ True Negative (TN)-Those who are ACTUALLY disease free ○ False positive (FP)- Those that are misdiagnosed as not as being disease free
● Sensitivity: percent of persons with the disease who are correctly classified as having the disease
○ True Positive (TP) - Those that actually have it ○ False negative (FN) - Those that are misdiagnosed as not having it
73.for taking CR what do you want in your bite registration ( cusp tips? Slight show-through)

74. Why do you adjust the articulator 1 mm open on the second molar? Had this question and went with the answer that talked about making it easier to correct the balanced occlusion or something like that… the other answer choices didn’t seem right. -TR 75. Which of the following only work on cyclooxygenase 76. 14 year old boy. Did RCT #30 still painful. Osteosarcoma? (this one is painful swelling) Fibrous dysphasia (this one is not painful swelling) 77. Mandibular canine was more facial what will happen? ( recession, excessive mobility, overbite and excessive?) 78. Mandibular extrusion causes what in the anterior? Causes increased anterior facial height with the Extrusion of posterior teeth causes the mandible to rotate downward and back in the absence of growth. 79.Relation of incisors during s-ch-z sounds( in contact, almost contacting) ---> Closest speaking space, determines VDO. 80. Anterior teeth contact when they making s-Chris-z sound ( overbite....) ---> Excessive VDO 81. Patient has excessive scar due to electric shock on face at the angle of mouth. How does it affect dentition (move facial, improper arch form?) Scarring from electrical burn = lingual inclination of teeth or Decreased VDO (both correct hopefully) -- From DanMan File 2019 82. 4 Q on prophylactic antibiotic? Preventive (prophylactic) antibiotics prior to a dental procedure are advised for patients with:
1. Artificial/prosthetic heart valves 2. History of infective endocarditis 3. Certain specific, serious congenital (present from birth) heart conditions, including:
○ unrepaired or incompletely repaired cyanotic congenital heart disease, including those with palliative shunts and conduits
○ a completely repaired congenital heart defect with prosthetic material or device, whether placed by surgery or by catheter intervention, during the first six months after the procedure
○ any repaired congenital heart defect with residual defect at the site or adjacent to the site of a prosthetic patch or a prosthetic device
4. Cardiac transplant that develops a problem in a heart valve. 83. Least likely in osteogenesis imperfecta → scalloping at dej? (it is considered the brittle bone disease) 84. Confidence interval because why? You need to be in the 95%
● A 95% confidence interval is a range of values that you can be 95% certain contains the true mean of the population. This is not the same as a range that contains 95% of the values.

85. Null hypothesis was self study vs. conventional study (attending lecture). What is the independent variable ? Self Study or Attending Lecture = Independent Variable
● A researcher conducting a research between student’s self studying and those attending lectures what is the independent variable? students participating in research, material studied, Students results, Lecture of self study
○ ATTENDING LECTURE or SELF STUDY (INDEPENDENT VARIABLE)** ○ STUDENTS RESULT (DEPENDENT VARIABLE)
86. Clindamycin prophylactic dose → Adults: 600mg orally 1 hour prior to appointment; Children: 20mg/kg orally 1 hour prior to appointment 87. What to use when cementing veneers → dual cure (resin cement) 88. Fixed rpd using premolar as abutment with short clinic crown that is non various. What you do to tooth ( I lay, mod only, reverse 3/4 crown, full crown) 89. Lateral flap used for → increase attached gingiva for anteriors (AKA pedicle flap); used for root coverage on gingival recession teeth. 90. Radiograph makes what to bone? ( under/over estimates none change) underestimate (It cannot show you the F/L width of the alveolar bone -TR) Question from mastermind #217: Xray taken of a guy with a crater defect, what is true? Xray underestimates the real size of the crater. 91. Most common factor of caries ( decreased saliva, bacteria present) 92. Patient has no carious lesions but has a high amount of strep mutants in biology test → means they are high caries risk 93. Primary dentition first molar has something → wide contact or wide occlusal table 94. At 4 years of age 2nd perm premolar is not coming in least likely for ( resorbed roots, has occlusal restoration) 95. Which is not a succedaneous tooth → first molar 96. Canine and incisor contacting at working movement but non working side does not contact ( group function , protrusive, anterior, balanced) 97. Flabby tissue anterior taking impression what do you do ( closed mouth impression, high adhesive material, high pressure , take at rest position) 98. Max complete/ man rpd where do you want contact for lateral working movement? Balanced occlusion 99. Draw 2mm line for custom tray everywhere except?? Posterior palatal seal area

100. Best material for large graft (replace a lot of the mandible)? ( autogenous graft, freeze dried (allogenic graft)) 101. Sulfonamide MOA---> interferes with folic acid synthesis by preventing addition of para-aminobenzoic acid (PABA) into the folic acid molecule through competing for the enzyme dihydropteroate synthetase. 102. MOA antilogust (sp?) drug? 103. Ulcers everywhere palate and throat → primary, aphthous 104. Vertical Fractured tooth but patient is asymptomatic and pulp is healthy, what do you do? rct (contraindicated), extract, crown 105. Splint mandibular incisors why? patient uncomfortable with mobility, help with perio? 106. Use for maxillary premolar #17, 23, 150,151 107. Opaque at Incisal 1/3 of crown why? Under reduced 108. Facial reduction of veneer? 0.5mm 109. Most hygienic Pontic → Sanitary/hygienic pontic and conical (Both are most hygenic pontics, but not that esthetic at all. 110. Ensure best pontic how? scratch the cast, passive fit with tissue, gold at gingival 111. Percent of stannous fluoride given at office? 8% 112. Internal bleaching how long do you wait before facial bonding? 1 week 113. Intrusion 5 mm what do you do? Observe for primary, permanent - orthodontics 114. Best x-ray: short Wavelength, High Energy
● Filtration is a mechanism where the low quality, long wavelength x-rays are absorbed from the exiting beam.
115. Pulpotomy on molar, places cotton pellets but still bleeding what do you do? remove extra tissue tags and add more cotton pellet, use lido, use hemostatic agent? 116. Self reabsorbed suture that last the longest? chronic, chromic gut, silk 117. What will fuse like epiphyseal plate? fontanelles, synchondrosis 118. 40 year old with posterior cross bite. What treatment? quad helix, palatal expander, suture osteotomy?
119. What causes hemorrhaging after radiation exposure? ( neutropenia, methem) ● radiation depletes the body of platelets.
120. Patient gets maxillary denture and immediate starts salivate. What system? ( reflexive, sympathetic.. something like that?) 121. Pedal edema, high diastolic, shortness of breath = copd, CHF (Congestive Heart Failure) 122. What is the mesio-distal dimension of implant from adjacent tooth? 3mm, 1.5mm (implant to adjacent tooth = 1.5mm; implant to implant distance = 3mm) 123. What gives ledging during endo procedure?
A. Jumping too quick from small to large hand file B. Using high RPM on rotary handpiece
124. What is the purpose of a facebow?Translates relationship of maxilla to terminal hinge axis July 18, 19, 20: 1.Ton of questions on CPR
● Compression rate in CPR = 120/minute ● Minimum depth to which you have to compress the chest? 1.5 inches ● Performing CPR and the chest is NOT rising, why? The head is not tilted and chin lifted up
enough to clear the airway from the tongue, you hand is not holding the mask all the way sealed, more options I can’t remember.
2.Calculate amount of epi in 1.7cc 2% lidocaine 1:50,000 → Answer was 34mcg 3.A lot of questions on beta blockers 4.Worst type of force for a single implant (choices were vertical, horizontal, oblique, axial) → horizontal 5.Radiograph 25 year old kid giant radiopacity on distal root of molar, no symptoms tooth was vital. → didn’t know if it was cementoblastoma or complex odontoma
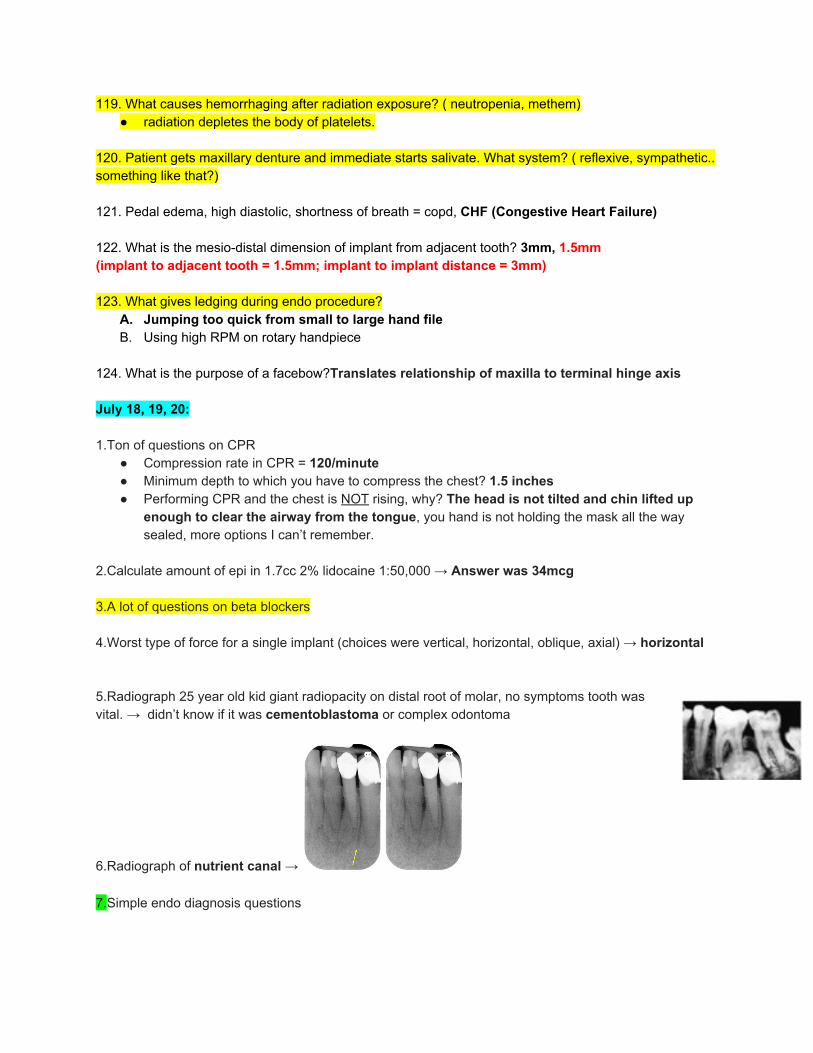
6.Radiograph of nutrient canal → 7.Simple endo diagnosis questions

8.Most frequently impacted tooth (3rd molars weren’t an option) → Mandibular 3rd Molar > Maxillary 3rd Molar > Maxillary Canine 9.Most frequently missing tooth → 3rd Molars > Mandibular 2nd PM > Maxillary Lateral Incisors > Maxillary 2nd PM 10.Which tooth has most consistent number of canals? Maxillary Central and Maxillary Lateral Incisors 11.Fusion vs gemination question (Fusion = Two Separate Canals)
● Gemination: Tooth gemination is a dental phenomenon that appears to be two teeth developed from one. There is one main crown with a cleft in it that, within the incisal third of the crown, looks like two teeth, though it is not two teeth. The number of the teeth in the arch will be normal. (1 root 2 crowns)
● Fusion: Union of two adjacent teeth in both primary and permanent dentitions. The number of teeth in the arch will be one less. (2 roots 1 crown)
12.A case scenario with a radiograph of the skull it was super hard to see but it was either multiple myeloma or Paget’s disease (I believe it was Paget’s)
● Multiple Myeloma = punched out lesions
● Paget’s Disease = cotton wool appearance 13.Max 3rd molar with divergent roots → hemisection 14.Extracting mandibular 3rd molar and distal root disappears.. which space did it go into.. pterygomandibular space (submandibular space) 15.Trismus which muscle is affected.. Choices were lateral pterygoid, medial pterygoid, masseter, buccinator, temporalis 16.Some Periocoronitis question about what would it look like if it turned into chronic → a mild persistent inflammation of the area; Chronic Pericoronitis is seen on x-ray as flame-like appearance distal to the mandibular 3rd molar.

17.Some random surgery (I think intraoral vertical Ramus osteotomy.. don’t quote me on that) which nerve can it damage.. inferior alveolar nerve.. other choice was lingual nerve, mylohyoid, submental 18.You perforate the sinus during an extraction and a root tip goes in, what do you do? I put take a pano and inform the patient.. other choices were make the perforation bigger and try to extract it, do nothing, and some other answer that was wrong 19.Case scenario about an old lady that had radiation for cancer and has a diastema and wants to close it. #8 had an apicoectomy and the root was super short and #9 had RCT also but the root wasn’t as short. What do you do to close the space? Veneers (I put this), extract and implants (obv not), full coverage crowns (didn’t put this because crown:root ratio would’ve been fucked), ortho, don’t treat her 20.Another case where a guy had a huge Caries on #29 and was in pain but had 65gry of radiation or something in the past. What do you do? RCT (I put this), pulpotomy, Extract, leave it alone 21.Question on how to extract mandibular premolar.. 151 forceps 22.Which tooth most common for alveolar osteitis (dry socket).. choices were mandibular 3rd molar, mandibular 1st molar, max 3rd molar, another tooth 23.All except question on how to treat dry socket.. I think the answer dealt with prescribing antibiotics 24.Most common reason for fracture of kids 1-3 years old or something like that.. uncoordinated movements 25.A question on what nerve is a branch of the (can’t remember the name of the nerve might have been infraorbital) but choices were PSA, MSA, ASA, and two RANDOM fucking nerves I’ve never heard of on my life I picked one of the random ones that sounded like it dealt with the upper lip
● The infraorbital nerve emerges from the infraorbital foramen and gives off four branches: the inferior palpebral, external nasal, internal nasal, and the superior labial branches, which are sensory to the lower eyelid, cheek, and upper lip.
26.Patient had ecchymosis in her right eye after you gave a maxillary injection what happened? I put blunt trauma unrelated to procedure, other choices all had to do with injecting into the artery. I don’t think my answer is correct but the choices all sounded the same so � ♂ 27.3 questions on SLOB rule 28.Know definition of osteotomy vs ostectomy
● Osteotomy: surgery where bone is cut to shorten, lengthen, or change its alignment as is done with orthognathic surgeries and distraction osteogenesis. (LeFort 1 surgery)
● Ostectomy: An ostectomy is a procedure involving the removal of bone. In dentistry it refers specifically to the removal of bone surrounding a tooth in an attempt to eliminate an adjacent periodontal pocket.
29.Know definitions of Ethics terms well ● Beneficence- “Do good”. ● Patient Autonomy- “Self-governance”.

● Non-maleficence- “Do no harm”. Dentists are to keep skills and knowledge up-to-date and practice within their limits in order to protect the pt from harm.
● Justice- “Fairness”. ● Veracity- “Truthfulness”.
30.You randomly get lip paresthesia what could it be.. Malignancy or angle fracture
● Angle Fracture (Mandibular Fracture) ● Osteosarcoma
31.Arch length is measured from mesial of which teeth.. max 1st molars
● Arch Length: Distal 2nd PM to Distal 2nd PM OR Mesial 1st Molar to Mesial 1st Molar ● Arch Width: Inter-canine space
32.How long do you splint Avulsion for.. 7-10 days 33.Peds questions on distal step, mesial step
● Distal Step: class II molar relationship in permanent dentition ● Mesial Step: either class I or class III molar relationship in permanent dentition
34.Which one is most common type of occlusion in PRIMARY teeth? flush terminal plane 35.Which defect is best perio prognosis. Choices were 3-walled, 2-walled, 1-walled 36.Which ethnic group has the most chronic periodontitis? Black males 37.Which cells will you find in periodontitis? PMN 38.Which bacteria causes Caries? Strep mutants 39.Lactobacillus TQ (doesn’t start caries but progresses them) 40.Pregnant patient with acute apical abscess when can you treat her? Choices were immediately? (since could spread and become ludwig angina?)- TR, 1st trimester, 2nd trimester, or 3rd trimester.. if you do endo you have to take xrays so � ♂ 41.neurofibromatosis question → Multiple neuro sarcomas in what disease? 42.Peutz-Jeghers question → internal polyps (also seen in Gardner’s syndrome) 43.Gardners syndrome question → multiple osteomas in jaws (syndrome associated with multiple odontomas) 44.Plaque index used for patient motivation 45.All are associated with perio disease except.. choices were diabetes, smoking, oral hygiene, diet (nutritional deficiencies)

46.True false question about lowest social economic people and poor periodontal health ● The study revealed that oral hygiene awareness and periodontal conditions are significantly
associated with socio-economic status of an individual. (Lower social economic people will have poorer periodontal health)
47.What is the main component of primary vs secondary occlusal trauma.. amount of force, bone support (Difference between primary and secondary occlusal trauma? PDL involvement and remaining amount of supporting bone). 48.Down syndrome question what do they have...I think I put macroglossia.. forgot the answer choices one of them was rampant Caries (nope) 49.Definition of biological width.. choices had 2mm and 3 mm. The 3 mm choice included gingival sulcus. I went with the 2mm choice CT and JE 50.How to determine attachment loss (shoutout Dr. Sonny) calculating measurement of CEJ to sulcus (depth of pocket); Pocket Depth is measured from the FGM to the base of the pocket 51.How to determine attached gingiva
● Place your probe on the outside of the tissue and measure from the gingival margin to the mucogingival junction. Now measure the sulcus or pocket depth (probing depth). Subtract the probing depth from the outside measurement of the gingiva, and you will have the width of attached gingiva
52.What don’t you do at PMT appointment? Choices were → root plane pockets 1-3mm, observe oral hygiene, schedule patient for restorative work, update med hx 53.Molar with class 2 furcation what can’t you do in treatment plan? GTR, Extraction with implant placement, hemisection with prosthetic crown placement, converting class II to a class I furcation 54.Contraindication of RCT? vertical root fracture 55.What acts as a hemostatic agent during vital pulp therapy? Calcium hydroxide or sodium hypochlorite (NaOCl) 56.Most common seizure in kids.. Febrile 57.Antibiotic therapy have minimal effect for? Chronic periodontitis 58.Just did perio surgery what’s the best way to clean interproximal? Proximal brush, toothpick, waterpick irrigation, floss 59.What’s cause of leakage with rubber dam? Holes punched too close

60.First sign of pit and fissure Caries? Explorer catch, enamel discoloration 61.Know all the different types of fluoride
● TYPE OF FLUORIDE: ● Type of fluoride in water → fluorosilicate acid (hydro fluorosilicate) – most commonly used,
sodium fluorosilicate, and sodium fluoride ● Types of Fluoride used in toothpaste → Stannous fluoride (most effective), Sodium Fluoride
(NaF), Sodium Monofluorophosphate o Stannous fluoride may stain o Type of Fluoride NOT in toothpaste = Acidulated Fluoride (1.23% concentration → only used in dental office)
● Do NOT use this type of fluoride on a patient with multiple porcelain crowns ● Patient with lots of fillings, implants, amalgam, composite, PFMs → use
1.1% Sodium Fluoride (NaF) o However this type of fluoride is NOT useful in managing caries in the elderly
62.What do you prescribe 4 year old with lots of Caries? All the fluorides were listed I put SDF but � ♂ 63.Know tetracycline well → Tetracycline for periodontal infections (better penetration, stays in bone tissue longer) Tetracycline: bacteriostatic, protein synthesis inhibitor (30s) ; does NOT decrease gingival crevicular fluid (GCF) flow
• Block activity of collagenase, bind to 30S (block AA linked tRNA) • Is usually NOT used because they can cause yeast infections as well as opportunistic infections • Tetracycline can be chelated with Calcium, Magnesium and Iron
o Don’t take iron supplements, multivitamins, calcium supplements, antacids, or laxatives within 2 hours before or after taking tetracycline. Antacids and milk reduce the absorption of tetracycline.
• Tetracycline effects the Dentin, causes intrinsic stain o Age that you took tetracycline which resulted in enamel hypoplasia or tetracycline staining:
§ Primary teeth→ before 4 months in utero § Permanent teeth → birth
Do NOT give codeine or tetracycline to lactating female 64.Know penicillin well → Penicillin for odontogenic infections Penicillin is bactericidal and inhibits peptidoglycan cell wall by binding to transpeptidase
• It is a GREAT drug to give because it is → cheap, low toxicity, and not a lot of people are allergic to it • Mechanism of Action of Penicillin (Bactericidal against gram (+)) is closely related to Keflex (Cephalexin) • If patient is allergic to penicillin then could have cross reactivity with Cephalosporins as well. • Transpeptidase enzyme is inhibited by Penicillin • Has decreased effectiveness in abscess/cyst due to Hyaluronidase (penicillin is unable to reach organism/ can’t penetrate the cyst barrier) • Penicillin CANNOT be taken with ERYTHROMYCIN or TETRACYCLINE!!! They are antagonists (cidal + static) so they cancel each other out

65.Pemphigus vs pemphigoid which one causes the ocular issue? Pemphigoid ● Autoantibodies target basement membrane, Ocular →
Subconjunctival fibrosis, adhesions, scarring (blindness)
66.Question on gracey curette and how it’s shaped ● Lower ⅓ (⅓ including the tip) → edge of curette you want to be in
contact at the line angle of tooth ● Apical ⅓ → part of curette that adapts to the tooth
67.Lip swells after taking an impression.. angioedema 68.What happens after alginate impression sets.. syneresis or imbibition
● If the alginate impression is left out in the dry atmosphere then syneresis happens (exudation of liquid component of gel that leads to alginate shrinkage)
● If the alginate impression is left in water/ wet environment then imbibition happens (process of absorbing water that leads to alginate expansion)
69.ANUG (NUG) questions.. buzz word ulceration of interdental papilla 70.Girl has her first period (menarche).. it shows signs of? Choices were emotional maturity, Dental maturity, skeletal maturity, some other maturity that was wrong 71.Picture of ulcers above MGJ (so on the alveolar mucosa = non-keratinized).. aphthous or herpetic
● Aphthous ulcers in non-keratinized tissue ● herpes in keratinized tissue
72.All are anticonvulsant drugs except.. know them all Anticonvulsants: Phenytoin (Dilantin), Valproic Acid, Carbamazepine, Clobazam, Diazepam (Valium), Divalproex, Eslicarbazepine Acetate, Ethosuximide, Gabapentin, Lacosamide, Methsuximide, Oxcarbazepine, Perampanel, Phenobarbital, Pregabalin, Rufinamide, Tiagabine Hydrochloride, Vigabatrin, Clonazepam, Clorazepate, Ezogabine, Felbamate, Lamotrigine, Lorazepam, Primidone, Topiramate, Zonisamide 73.Contraindication to doing a distal wedge.. no attached (keratinized) gingiva 74.Advantage of supragingival crown prep vs subgingival.. choices were less damage to soft tissue during impression or more retention 75. healing after flap surgery with membrane.. choices were junctional epithelium moves apically or PDL cells move coronally (occlusally) 76.How many mm per day does epithelium grow over connective tissue? 0.5-1mm 77.What is not an advantage of porcelain veneer vs composite restoration? 2 visits required 78.Need to replace a large portion of mandible, which graft do you do? Autogenous
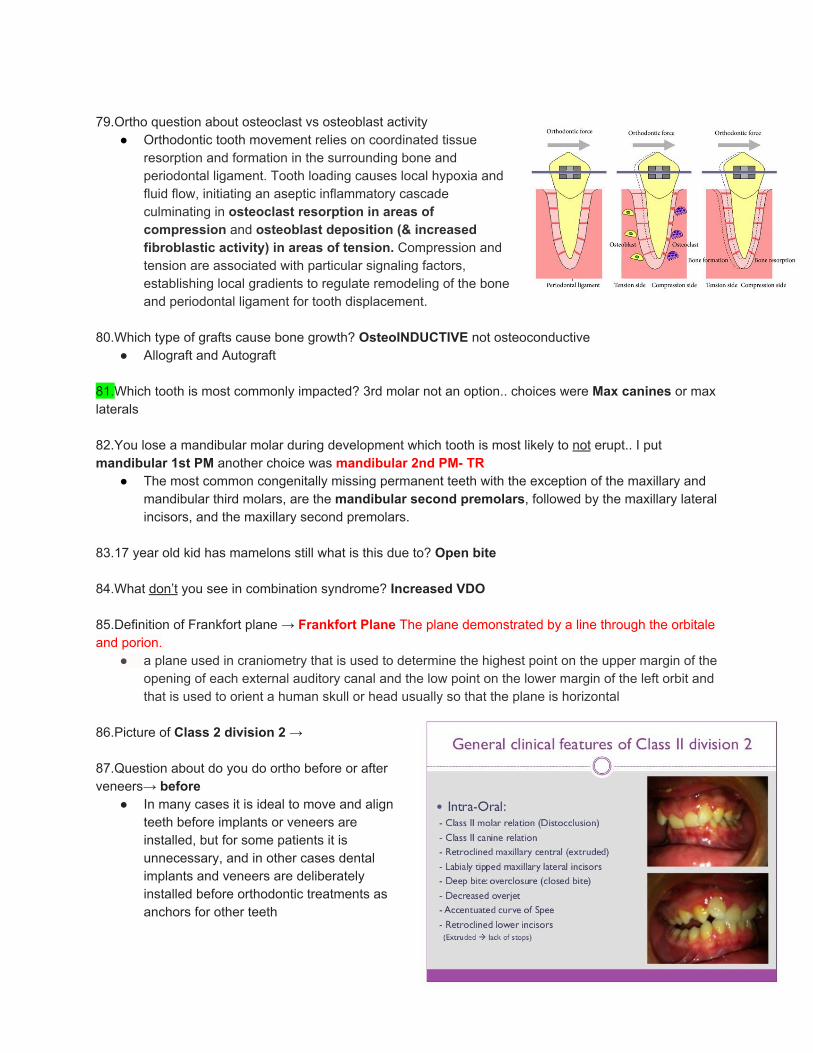
79.Ortho question about osteoclast vs osteoblast activity
● Orthodontic tooth movement relies on coordinated tissue resorption and formation in the surrounding bone and periodontal ligament. Tooth loading causes local hypoxia and fluid flow, initiating an aseptic inflammatory cascade culminating in osteoclast resorption in areas of compression and osteoblast deposition (& increased fibroblastic activity) in areas of tension. Compression and tension are associated with particular signaling factors, establishing local gradients to regulate remodeling of the bone and periodontal ligament for tooth displacement.
80.Which type of grafts cause bone growth? OsteoINDUCTIVE not osteoconductive
● Allograft and Autograft 81.Which tooth is most commonly impacted? 3rd molar not an option.. choices were Max canines or max laterals 82.You lose a mandibular molar during development which tooth is most likely to not erupt.. I put mandibular 1st PM another choice was mandibular 2nd PM- TR
● The most common congenitally missing permanent teeth with the exception of the maxillary and mandibular third molars, are the mandibular second premolars, followed by the maxillary lateral incisors, and the maxillary second premolars.
83.17 year old kid has mamelons still what is this due to? Open bite 84.What don’t you see in combination syndrome? Increased VDO 85.Definition of Frankfort plane → Frankfort Plane The plane demonstrated by a line through the orbitale and porion.
● a plane used in craniometry that is used to determine the highest point on the upper margin of the opening of each external auditory canal and the low point on the lower margin of the left orbit and that is used to orient a human skull or head usually so that the plane is horizontal
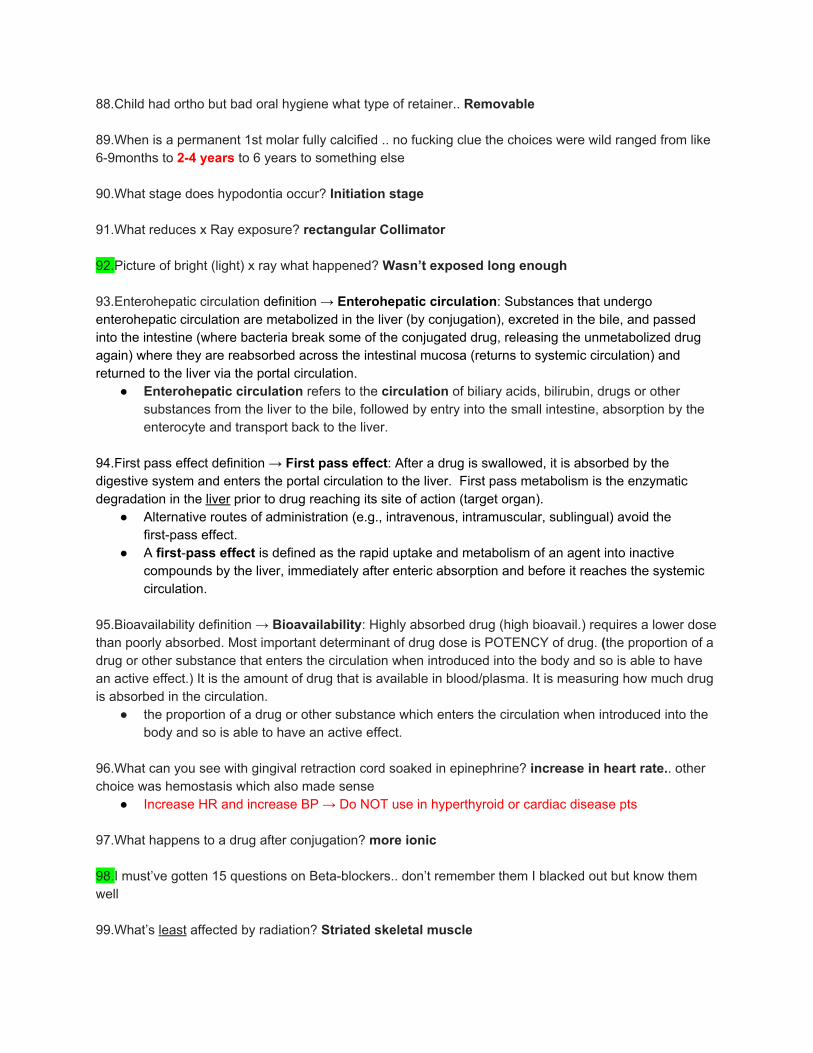
86.Picture of Class 2 division 2 → 87.Question about do you do ortho before or after veneers→ before
● In many cases it is ideal to move and align teeth before implants or veneers are installed, but for some patients it is unnecessary, and in other cases dental implants and veneers are deliberately installed before orthodontic treatments as anchors for other teeth
88.Child had ortho but bad oral hygiene what type of retainer.. Removable 89.When is a permanent 1st molar fully calcified .. no fucking clue the choices were wild ranged from like 6-9months to 2-4 years to 6 years to something else 90.What stage does hypodontia occur? Initiation stage 91.What reduces x Ray exposure? rectangular Collimator 92.Picture of bright (light) x ray what happened? Wasn’t exposed long enough 93.Enterohepatic circulation definition → Enterohepatic circulation: Substances that undergo enterohepatic circulation are metabolized in the liver (by conjugation), excreted in the bile, and passed into the intestine (where bacteria break some of the conjugated drug, releasing the unmetabolized drug again) where they are reabsorbed across the intestinal mucosa (returns to systemic circulation) and returned to the liver via the portal circulation.
● Enterohepatic circulation refers to the circulation of biliary acids, bilirubin, drugs or other substances from the liver to the bile, followed by entry into the small intestine, absorption by the enterocyte and transport back to the liver.
94.First pass effect definition → First pass effect: After a drug is swallowed, it is absorbed by the digestive system and enters the portal circulation to the liver. First pass metabolism is the enzymatic degradation in the liver prior to drug reaching its site of action (target organ).
● Alternative routes of administration (e.g., intravenous, intramuscular, sublingual) avoid the first-pass effect.
● A first-pass effect is defined as the rapid uptake and metabolism of an agent into inactive compounds by the liver, immediately after enteric absorption and before it reaches the systemic circulation.
95.Bioavailability definition → Bioavailability: Highly absorbed drug (high bioavail.) requires a lower dose than poorly absorbed. Most important determinant of drug dose is POTENCY of drug. (the proportion of a drug or other substance that enters the circulation when introduced into the body and so is able to have an active effect.) It is the amount of drug that is available in blood/plasma. It is measuring how much drug is absorbed in the circulation.
● the proportion of a drug or other substance which enters the circulation when introduced into the body and so is able to have an active effect.
96.What can you see with gingival retraction cord soaked in epinephrine? increase in heart rate.. other choice was hemostasis which also made sense
● Increase HR and increase BP → Do NOT use in hyperthyroid or cardiac disease pts 97.What happens to a drug after conjugation? more ionic 98.I must’ve gotten 15 questions on Beta-blockers.. don’t remember them I blacked out but know them well 99.What’s least affected by radiation? Striated skeletal muscle
100.Epinephrine + propranolol cause.. increased BP (also Decreases HR) 101.Xerostomia what do you check for? Cervical Caries 102.Xylitol works best as? chewing gum 103.What is the first sign of hypoxia during general anesthesia? (pulse oximetry? -TR) 104.What’s the least effective way of telling if your Parkinson’s patient is in pain? reading his facial expressions but � ♂ the other choices seemed wrong 105.Most common disorder for elderly? Depression 106.Main sign of Dementia?.. short term memory loss 107.What receptor do benzodiazepines work on? GABA 108.Some question about addiction and dependency that didn’t make sense 109.All are side effects of corticosteroids except.. Hypoglycemia 110.Temporal arteritis leads to.. vision loss
● Symptoms include headaches, jaw pain, vision loss, fever, and fatigue. Diagnosis usually requires biopsy of the temporal artery.
● The condition needs prompt treatment with steroid medications to prevent permanent vision loss.
111.Sickle cell anemia is a _____ mutation? Nonsense, missense, sense ● Single point mutation (AKA Missense mutation)
112.Definition of panic attack.. choices included fear and anxiety was kinda tricky but key word to know it was panic attack was “impending doom”
● Panic attacks usually produce a sense of unreality, a fear of impending doom, or a fear of losing control.
● Increase heart rate, hypertension, light headedness, diaphoresis, and feeling of impending doom is a sign of? Panic Attack
113.2 year old Kid weighs like 16 pounds what’s the max dose of lidocaine? 154.88mg or (4 cartridges of 2% Lidocaine with 1:100,000 epinephrine)
● Math: 16lbs * 2.2 kg/lb = 35.2kg * 4.4 mg/kg = 154.88mg / 36mg (lidocaine in 1 cartridge) = 4.3 cartridges
114.A couple questions about emergencies.. each patient had a different condition then something happened to them.. what do you do first? check if conscious other choices were call 9-1-1, start CPR, something else 115.Area of infection how do you anesthetize? Block (IANB)

116.Pulse for a 4 year old.. 110 ● (12 yr. old is 75; adult is 70)
117.26 month old child with 12 carious teeth, how do you treat? General anesthesia 118.What’s false about placing pins in amalgam? Larger sized pins are better 119.How does tetracycline work? Inhibits protein synthesis 120.Veneer done a month later is discolored what happened? Something about amine leakage (microleakage) 121.Pt taking tetracycline, what’s contraindicated? Penicillin 122.Pt is taking penicillin, what’s contraindicated? Erythromycin (or tetracycline) 123.Maxillary sinusitis, which antibiotic do you prescribe? Amoxicillin with clavulanic acid (Augmentin) 124.Kennedy class 3 what provides support? Occlusal rest 125.Question about what happens if no indirect retention on an RPD? Dentures lifts up away from tissue side 126.What is not a noble metal? 4 random elements I Didn’t know the answer
● titanium (Ti), niobium (Nb), and tantalum (Ta) are NOT considered Noble Metals ● Noble metals: gold, platinum, palladium, rhodium, ruthenium, iridium, osmium
127.Why does a chromium-cobalt framework not corrode? surface oxide layer, because of the noble metal component
● The presence of noble metals in alloys increases resistance to corrosion. 128.Primary stress bearing areas of RPD? Hard palate and Buccal shelf 129.Purpose of major connector? Stability and rigidity 130.Purpose of reciprocating arm? So the clasp doesn’t get dislodged as you’re trying to seat it � ♂
● Stabilization (resists the lateral forces exerted by the retentive arm when it passes through the height of contour)
● Denture is stabilized against horizontal movements, acts as an indirect retainer (prevents minor rocking)
131. 0.3mm irregularity in your die for your crown what do you do? adjust from intaglio, retake impression and send it back, fuck with the cement ratio (don’t do this!), and something else 132.A patient with moveable flabby inflamed tissue in the maxillary anterior and wants a new denture what do you do? place tissue conditioner and re-evaluate in 2 weeks, surgically remove tissue, take impression for new denture, make new denture that will immobilize flabby tissue
133.What is at the distal extension of your complete denture? Choices were Hamular notches or fovea palatini
● Hamular notch is the depression distal to the maxillary tuberosities. It is used as a landmark for the correct extension of the upper denture.
● Fovea Palatini are the landmark for the posterior border extension of the upper denture. 134.How do you check for fremitus? Mouth in MICP, mandible in retruded position, lateral working, or balancing?
● As a test to determine the severity of periodontal disease, a patient is told to close his or her mouth into maximum intercuspation and is asked to grind his or her teeth ever so slightly. Fingers placed in the labial vestibule against the alveolar bone can detect fremitus.
135.Why would you remove palatal torus? Seems easy but none of the answers made any sense so � ♂
● Remove it if it prevents seating of denture and to increase posterior palatal seal ● Should be removed if tori is 3mm anterior to vibrating line (interferes with posterior palatal seal)
136.What does facebow do? Translates relationship of maxilla to terminal hinge axis 137.Why do you do remount index? Preserve facebow transfer 138.Which sounds for VDO? “S” sounds 139.What don’t you do at wax try-in appointment? I put take facebow.. other choices were confirm VDO, confirm esthetics, other obvious answers 140.Border molding what movement do you do to capture right and left lateral borders? Don’t remember answers I put the one that was most logical
● Massage the cheek and have the patient pucker and smile. The cheek is lifted outward, upward, inward, backward and forward to active movement of the frenum.
141.While setting condylar inclination on articulator using protrusive movements what do you do with the pin? Lift it up (the incisal guide pin on articulator should be raised out of contact with incisal guide table) 142.Most commonly seen? cleft lip, amelogenesis imperfecta, ectodermal dysplasia, dentinogenesis imperfecta (cleft lip and palate in US is 1:700) 143.What resembles epiphyseal plate? Synchondrosis
144.Sturge Webber syndrome? Port wine stain 145.Deaf patient how do you communicate? speak directly to him and wait for interpretation 146.You are least likely to get sued by a patient if you exhibit this trait? I HAVE NO IDEA choices were you have a likeable personality, you are competent, you have good communication skills (answer I went with today- TR), something else

147.How do you establish rapport? Don’t remember choices ● Understanding patient’s feeling and talking with patient
148.How to manage anxious patient? Let him speak 149.Patient has only had 1 cavity her whole life went to a dentist and dentist said she has 6 cavities you look at the dentists radiographs and don’t see any cavities but she does have an incipient lesion starting to form on one tooth what do you recommend the patient do? I don’t know about this one I put to have her report the dentist to the national board but another choice was to defend the other dentist’s opinion and treatment plan for the incipient lesion which kinda made sense but idk 150.3 questions on desensitization
● a treatment or process that diminishes emotional responsiveness to a negative, aversive or positive stimulus after repeated exposure to it.
● Systematic desensitization- 3 steps: Construct a hierarchy, relaxation exercises, associate components of hierarchy with relaxation state
151.2 questions on sensitivity/specificity. Know how to calculate them
● Specificity: percent of persons without the disease who are correctly classified as not having it ○ True Negative (TN)-Those who are ACTUALLY disease free ○ False positive (FP)- Those that are misdiagnosed as not as being disease free ○ Specificity = TN/ TN + FP
● Sensitivity: percent of persons with the disease who are correctly classified as having the disease
○ True Positive (TP) - Those that actually have it ○ False negative (FN) - Those that are misdiagnosed as not having it ○ Sensitivity = TP/ TP + FN
152.Adverse drug reaction who do you report it to? FDA 153.Some question about HIPPA 154.Another question about who is in charge of nitrous lines and maintenance? I put OSHA but I didn’t know 155.Dentist did not accept copay.. Overbilling 156.Question about elderly abuse..it happens mostly in nursing homes 157.Who is least likely to get radiation exposure or something? Choices were dental assistant, dental hygienist, dentist,.... Id assume Dentist? (don’t most dentists get their assistants to take the xrays now adays? -TR) 158.What test must you get every year to work in health profession? I put TB cause we have to get one every year but another choice was Hep B and that’s what TQs say � ♂ (Final Answer = TB!!) 159.Chi square vs t-Test question that I guessed.. t-Test is for small sample size, Chi square is for large sample size
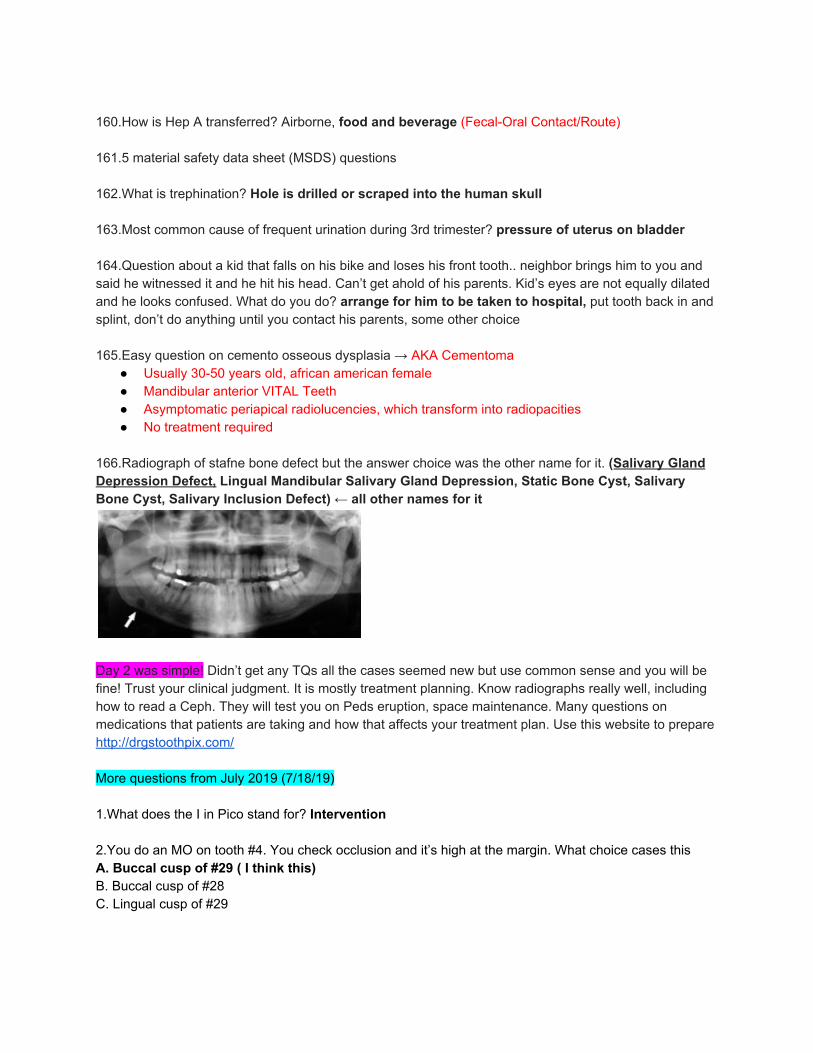
160.How is Hep A transferred? Airborne, food and beverage (Fecal-Oral Contact/Route) 161.5 material safety data sheet (MSDS) questions 162.What is trephination? Hole is drilled or scraped into the human skull 163.Most common cause of frequent urination during 3rd trimester? pressure of uterus on bladder 164.Question about a kid that falls on his bike and loses his front tooth.. neighbor brings him to you and said he witnessed it and he hit his head. Can’t get ahold of his parents. Kid’s eyes are not equally dilated and he looks confused. What do you do? arrange for him to be taken to hospital, put tooth back in and splint, don’t do anything until you contact his parents, some other choice 165.Easy question on cemento osseous dysplasia → AKA Cementoma
● Usually 30-50 years old, african american female ● Mandibular anterior VITAL Teeth ● Asymptomatic periapical radiolucencies, which transform into radiopacities ● No treatment required
166.Radiograph of stafne bone defect but the answer choice was the other name for it. (Salivary Gland Depression Defect, Lingual Mandibular Salivary Gland Depression, Static Bone Cyst, Salivary Bone Cyst, Salivary Inclusion Defect) ← all other names for it
Day 2 was simple! Didn’t get any TQs all the cases seemed new but use common sense and you will be fine! Trust your clinical judgment. It is mostly treatment planning. Know radiographs really well, including how to read a Ceph. They will test you on Peds eruption, space maintenance. Many questions on medications that patients are taking and how that affects your treatment plan. Use this website to prepare http://drgstoothpix.com/ More questions from July 2019 (7/18/19) 1.What does the I in Pico stand for? Intervention 2.You do an MO on tooth #4. You check occlusion and it’s high at the margin. What choice cases this A. Buccal cusp of #29 ( I think this) B. Buccal cusp of #28 C. Lingual cusp of #29

3.Where do you place the anterior teeth for a complete denture for proper esthetics (not sure of the answer) A. Labial to the ridge B. On the ridge? - I feel like thats where they always make us set our teeth…. (this is the option I went with today- TR) C. Lingual to the ridge D. touching the opposing dentition 4.What’s the worst wall to be restored by GTR A. One wall defect 5.If you have an infection in the lateral pharyngeal space what muscle is involved? A. Medial pterygoid 6.Tooth is vital and there is scalloped borders (literally just that) A. Traumatic bone cyst 7.1st sign of multiple myeloma A. Bone pain 8.What’s the best to replace or restore with GTR A. Wide three wall furcation B. Class 2 furcation (correct) 9.Most causes of suppurations A. Actinomycosis 10.Pediatric patient that has Carries and uncooperative A. Parents holds them down (correct) B. Pappoz restrained C. General anesthesia 11.Digitals MOA A. Positive inotropic (literally just those two words) 12.What is the treatment for SV arrhythmia A. Quinindine 13.What do you look at first in an emergency patient A. Medical history ( correct answers) B. Medication that the patient is 14.Injecting into the parotid gland causes facial paralysis. Comparing to the location of inferior alveolar nerve injection where would the needle be positioned? A. Anterior B. Posterior (if you inject too posteriorly you will enter the parotid gland)
C. Higher up 15.What’s the minimum number of neutrophils you could see a pediatric patient before dismissal (no freaking clue) <1,000/mm3 : defer elective dental care. A. 1300>x B. 1000>x C. 1500<x 16.What nerve supplies facial nerve A. V B. VIII (correct) C. II 17.Which HPV causes most cancer or related the most to the mouth. (Not sure) Research indicates that approximately 70 percent of cases of oropharynx cancer is caused by HPV16. A. 6 B. 11 C. 16 18.Which has the least number of canals? A. Maxillary central (correct answer) B. Mandibular central 19.What percent does the mandibular canine have 2 canals A. 5 % B. 9 % C. 16 % (15% according to some endo website) 20.Select the correct Order (neither one looked correct) A. Plaque control, caries control, SRP, Perio surgery B. Caries control, plaque control, SRP, Perio surgery 21.Which one is not a bacteriostatic A. Azithromycin B. Vancomycin (correct answer) C. Clarithromycin 22.Which one antibiotic can fight parasites and Fungal A. Metronidazole 23.Calculate the mean! Gave a bunch of numbers then told you the total of all of them = 30 and there were 10 numbers in the set so the answer was 3- TR 24.What’s the only thing your dental assistant can do A. Take a final impression for a fixed RPD B. Sign and verify lab script C. Take primary impression (correct answer)

25.What’s not true about dementia? (Asked me 3 times) A. Something about long term memory loss (correct answer) B. They don’t have problems comprehending and talking to people 26.Properties of glass Ionomer other than releasing fluoride (asked me 3 times) A. Has high esthetic B. Has high wearing strength. C. Chemical bonding to Dentin and enamel (correct answer- also they changed it in the other question from chemical bond to ionic bond) 27.Trismus of lateral pterygoid. A. Medial pterygoid 28.Primary tooth was avulsed, what do you do A. Nothing. You don’t reimplant primary teeth 29.Same tqs about direct and indirect pulp capping (4-6 questions)
● Two different types of pulp cap are distinguished. ● In direct pulp capping, the protective dressing is placed directly over an exposed pulp
○ One stage procedure ○ It is only feasible if the exposure is made through non infected dentin and there is no
recent history of spontaneous pain (i.e. irreversible pulpitis) ○ Placement of Calcium Hydroxide (CaOH) or MTA over exposure and then place
restoration on top. ○ Indications for Direct Pulp Cap:
■ Immature/mature permanent teeth with simple restoration needs ■ Recent trauma less than 24hours exposure of pulp / mechanical trauma
exposure (during restorative procedure) ■ Minimal or no bleeding at exposure site ■ Normal sensibility test ■ Not tender to percussion ■ No periradicular pathology ■ Young patient
● In indirect pulp capping, a thin layer of softened dentin, that if removed would expose the pulp, is left in place and the protective dressing is placed on top.
○ Stepwise caries removal is a two-stage procedure over about six months. ○ the dentist intentionally leaves the softened dentin/decay in place, and uses a layer of
protective temporary material (CaOH or MTA) which promotes remineralization of the softened dentin over the pulp and the laying down of new layers of tertiary dentin in the pulp chamber.
○ A temporary filling is used to keep the material in place, and about 6 months later, the cavity is re-opened and hopefully there is now enough sound dentin over the pulp (a "dentin bridge") that any residual softened dentin can be removed and a permanent filling can be placed.
○ Indications for INdirect Pulp Cap: ■ indicated in a permanent tooth diagnosed with a normal pulp with no symptoms
of pulpitis or with a diagnosis of reversible pulpitis.

30.Use Zinc oxide Eugenia for primary teeth and the apex is NOT closed. (tq) 31.Alcoholic guy. What test would you do. A. INR (correct) B. Look at glucose in blood C. CBC 32.Nitrates and nitriles what’s your mechanism of action? A. Vasodilation of the arteries 33.Stafne bone cyst which is not A. Located between canine and premolar mandibular (correct) B. Below IAN 34.Swelling after you spray air into pocket? A. Subcutaneous emphysema 35.Pregnant in supine position will get a lot of pressure A. Inferior vena cava 36.What position do you put this pregnant lady in? A. Left side 37.Drug of choice for status epilepticus? A. Diazepam 38.Action of benzodiazepine A. They work on GABA 39.Pain medication with amoxicillin for an adult? A. 50mg B. 1g C. 2g (correct) 40.By which mechanism of action are tetracycline and penicillin antagonist? No clue
● Tetracycline is bacteriostatic whereas penicillin is bactericidal. The two mechanisms of action (CIDAL + STATIC) cancel each other out because you need bacterial growth to actually use penicillin, but you don’t have that growth when you prescribe tetracycline. Antagonists. Tetracycline will DECREASE the efficacy of Penicillin.
41.Penicillin is a good antibiotic because? A. Low toxicity 42.You cannot take multivitamins when you are taking which drug? A. Tetracycline 43.Which medication do you take to stop excessive salivation
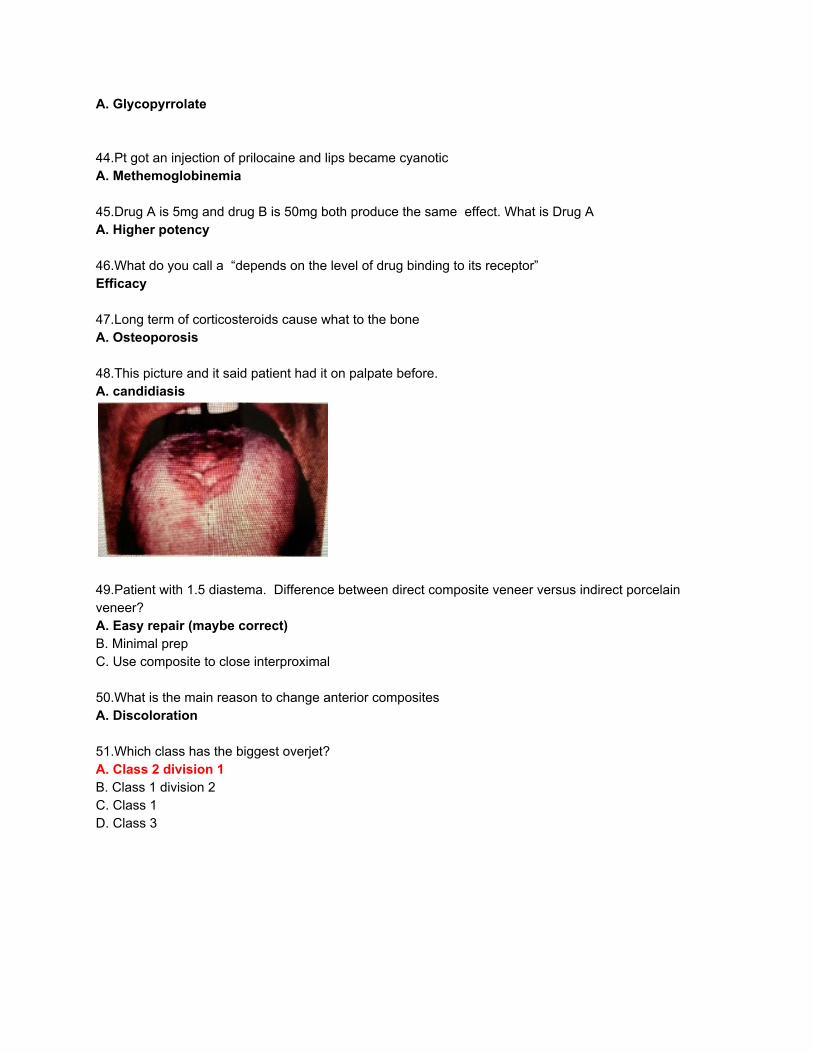
A. Glycopyrrolate 44.Pt got an injection of prilocaine and lips became cyanotic A. Methemoglobinemia 45.Drug A is 5mg and drug B is 50mg both produce the same effect. What is Drug A A. Higher potency 46.What do you call a “depends on the level of drug binding to its receptor” Efficacy 47.Long term of corticosteroids cause what to the bone A. Osteoporosis 48.This picture and it said patient had it on palpate before. A. candidiasis
49.Patient with 1.5 diastema. Difference between direct composite veneer versus indirect porcelain veneer? A. Easy repair (maybe correct) B. Minimal prep C. Use composite to close interproximal 50.What is the main reason to change anterior composites A. Discoloration 51.Which class has the biggest overjet? A. Class 2 division 1 B. Class 1 division 2 C. Class 1 D. Class 3

52.Where is melanoma found most intraorally? A. Gingival and buccal mucosa B. Gingival and hard palate C. Tongue and buccal mucosa D. lip and hard palate → I went with this today but had no idea just kept thinking of the picture of the melanotic macule on that patient’s lip but not even sure that is the same thing as what the question was asking for… dumbass strikes again haha TR) 53.Broken root tip what do you do (tq) A. Get hemostasis so you can visualize it 54.PA of posterior maxillary showing sinus and asked what is this Inverted Y. What combines those (tq) ….. Such a dumbass sometimes I swear hahaha A. Nasal floor and maxillary sinus 55.Recurrent Ranula what do you A. Excision 56.Recurrent Ranula what do you (same question with a different answer) A. Marsupialization 57.Sialolith where do you find it? A. Wharton’s duct A2. Submandibular gland 58.When does Taurodontism occur embryonically A. Morphodifferentiation (size and shape) (occurs during tooth morphogenesis) 59.Cavernous sinus thrombosis happens because A. Congestive heart failure B. Subcutaneous Abscess on upper maxilla (correct) 60.Lugwig angina A. Edema of the glottis 61.Where do you put the margin of the posterior crown? Not sure (I’d say either above or at the gingival level for purposes of gingival health- TR) A. Above the gingival → went with this option today since it said where would you place it if you can… and it would be supragingival so that it’s not messing with the gingiva - TR B. below the gingiva C. at the gingival 62.Side effect of opioids A. Constipation (correct answers) B. Hypertension 63.Target lesions A. Erythema multiforme

64.Chemo receptor target zone A. CTZ 65.Drug vs placebo all have in common except? A. Pharmacologic activity B. Psychological dependence 66.Dry heat and high-pressure instrumentation which one do you not do? A. Wrap instrument in a plastic bag B. Wrap instrument with a paper bag C. Wrapped instruments with a cloth D. Put instruments in a closed metal box? High pressure in closed box make a bomb?? TR 67.MOA of carbidopa A. Preventive Depletion of levodopa and replenish dopamine 68.Patient has neck injury and having difficulty breathing A. Call EMT B. Adjust head so he is able to breath C. Cricothyrotomy (maybe this) 69.Where is SNA A. Point on the chin B. Pre-maxilla in between anterior nasal spine and between anterior teeth (something like that. I think this is correct)
● SNA This angle represents the relative anterioposterior position of the maxilla to the cranial base ● the deepest point in the maxillary concavity is the “A” point of SNA
70.How to tell the difference between condensing osteitis versus idiopathic sclerosis A. Vitality 71.A hole in the bone showing/exposing a root A. Fenestration 72.What is considered Secondary preventative care A. Oral hygiene B. Fill pits and fissure (I think this??) 73.What happens with white spot lesions (not sure of the answer) THIS FUCKING QUESTION…. A. You’ll have carries in the first year B. You’ll have caries in the second year C. Unsure of possible future outcomes → as soon as it showed up I thought fuck me I looked everywhere for this answer online and couldnt find it…. But it wont show up on my exam… and then there she was…. D. Nothing will happen if you leave it 74.Which percent in the United States have fluoride in their water A. 30%

B. 50% C. 74% ( I think this since the other tq said 65-70%) 75.Elementary school with kids having a lot of interproximal Caries what is the best way to go about this A. Find a near by dental office B. Take radiograph C. Apply fluoride into water 76.Community water has how much fluoride (maybe 0.2 or 0.6) A. 0.2 B. 0.7 C. 1.2
● U.S. Public Health set optimal fluoride = 0.7–1.2 ppm for public water. ● Food and Nutrition Board recommends public water supplies be fluoridated when levels are
significantly below 0.7 mg/L. 77.What is associated with Osteogenesis Imperfecta? A. Dentinogenesis Imperfecta (Both have blue sclera) 78.A picture like the one to the right and asked if you take a radiograph what would you expect? A. Dentinogenesis imperfecta 79.Patient came in for an emergency with an enlarged and inflamed buccal tissue around Maxillary premolar that is necrotic. What’s the first step A. Drain and Incise (maybe correct) B. Antibiotic C. Root canal treatment 80.Pulse of a 4year old (tq) A. 110 81.Bisphosphonates MOA A. Inhibition of osteoclast 82.What does the Articular disc do? (Which way is the articular disc most displaced?) A. Anterior-medially 83.What is not involved in Elevation → Lateral Pterygoid A. Synergism between medial and lateral ptyergoid (this was a tq. Not sure if the answer) OLD TQ from Mastermind #115: you have some guy and their jaw is closing - which muscle is LEAST involved in closing the jaw? Synergism between lateral and medial pterygoids?
● Muscles elevating the jaw: masseter, temporal, medial pterygoid, and SUPERIOR belly of lateral pterygoid
84.Where do you bevel on amalgam to increase resistance A. Axis pulpal (correct) B. Dovetail
85.When do you stop taking Coumadin (there was no option of continued treatment without stopping medication) A. 1 day B. 3 days C. 7 days (correct) 86.How long does Aspirin stay in your system A. 7 days. (Irreversibly inhibits platelet aggregation) 87.Patient feels nauseous on nitrous what do you do? A. Switch to 100% oxygen 88.On an articulator you set teeth at 20 degrees and then you figure out it was wrong and you change it to 45 degree. What do you do? A. Increase the compensatory curve (You could also decrease incisal guidance - TR) 89.Turners Tooth question A. Trauma before birth B. Trauma/infection for posterior tooth after birth (correct) 90.Drug that makes you extremely violent and have psychotic behavior except A. Alcohol B. Amphetamines C. Cannabis D. Opioids August 23rd : Day 1: All questions from Lilly Pulitzer document from the July 18, 19, and 20 section. Day 2: Very subjective crap, horrible x-rays, etc. Can’t remember that many cases, the ones I do are below: Case 1: 8 y/o fell and loss front incisor #F and #E is slightly darker and has a sinus tract. 1. what’s boil on top of gum? Sinus tract from #E 2. #E was mobile, but #8 was about to erupt, extract or monitor and let #8 erupt? Monitor Case 2: case where little girl has bad breath and a lot of caries with history of multiple tonsillitis episode treated with abx. Radiograph shows lots of caries. Mom brought her in because she was being bullied for bad breath and hygiene is really bad. 1. How to improve her oral hygiene? OHI, demonstrate how to brush, and floss. 2. What is causing bad breath? Recurrent tonsil infections. Caries don’t cause bad breath. 3. How to treat issue with bad breath and tonsillitis? Refer for tonsillectomy. 4. What method to also help with oral hygiene? Have parents brush and floss her teeth. Case 3: Guy with interim maxillary rpd that replaces only anterior teeth, complains of food getting stuck on upper teeth. Has a bunch of health issues and bunch of meds. 1. #4 and #13 have really bad caries seen on radiograph, you start to excavate for caries and get pulp exposure on both, whats the next thing you do? Evaluate restorability or go straight to do RCT, post, and core.

2. Radiographs show a radiolucent lesion on #12, in the PA and bitewing its in different spots (angulation), question asks what is it? Based on his caries charting it’s a smooth surface caries. 3. Red mucosal tissue underneath his interim RPD in anterior/palate region, what was it? Either candida or food impaction irritation (not sure). 4. If you were to place implants in the front, which would not be a consideration? Maintenance of caries status 5. Which would be the best maxillary RPD for this patient in regards to cost, esthetics, etc.? Either replace the regular missing teeth, 6, 7 and 8 or other option was replace 6, 7,8, 4 and 13 (I picked this because it mentioned cost, and it would save the patient from doing RCT and crowns on 4 and 13). Case 4: Guy who has an accident and his front teeth were slightly chipped and he wanted them repaired or made even. 1. What would be the initial treatment for his chipped max incisors? Options were, resin, veneer, crown, or recontour. (I chose recontour because his teeth were very minimally chipped and the question made it seem like which would be your first initial treatment and that was least invasive). 2. What doesn’t this patient need? Scaling and root planning 3. How to recontour mandibular teeth? Ortho extrusion and gingival graft Case 5: Farmer for 40+ years, smokes, and uses smokeless tobacco. 1. White lesion on lip near vermillion border, what was it? From years of working out in the sun (or maybe smokeless tobacco)??? Not sure. 2. What was present on this guys lip? Excess keratin Random questions that I can’t remember what cases they were linked to: 1. What crown material would you use? Lithium disilicate 2. Patient has a cough due to what meds? Lisinopril 3. What is albuterol? B2 agonist 4. You give several carpules of LA to a kid and he started getting confused, altered consciousness, etc. why? LA overdose. 5. Diabetic patient, in history it states they don’t eat often with their medication, about to start a procedure, they get altered state of consciousness, BP drops, what’s happening? Hypoglycemia 6. Bunch of crap from kids eruption, make sure to review cephs, and ortho. 7. What is the radioopacity in front of C4 on a ceph? Hyoid bone 8. What is the line intersecting roots of #2 and #6? Max palatine processes 9. Patient just wants denture on the upper, what don’t you do out of choices given? Maxillary sinus lift. August 29th 1.Know drugs that you shouldn’t give epinephrine with 2.Know drug interactions 3.Know how the drugs work (MOA) and what happens with certain diseases Fire Drill Day:
1.What’s the concentration of acidulated phosphate fluoride is used in the dental office? 1.23%
2.Sealants - mechanical micro retention binding to tooth
3.Prolonged, unstimulated night pain suggests which of the following conditions of the pulp? a. Irreversible pulp
4.How do you test a tooth to differentiate between chronic periodontitis and supperative (acute) periodontitis? Percussion
5.Most reliable way to test vitality of a tooth? Thermal test
6.What is the initial treatment of a combination perio and endo lesion? Perform endo with RCT first. 7.You do pulpotomy, check with cotton, still bleeding what do you do? Lido to get hemostasis, remove more pulp tissue and check again, formocresol?
8.Cracked tooth w/o pulpal involvement, how u restore? RCT, crown*, amalgam, composite
9.Necrotic tooth with open apex, why do u do specification? so u can have proper seal for obturation.
10. B1 receptor effect: Beta 1 receptor for heart, vasodilator lungs (WRONG B2) 11.Tramadol effect :confused disoriented, high bp what is pt experiencing 12.Un treated scar on face what will it do? irregular arch decreased vertical ridge and tooth development (lingual inclination of teeth or decreased VDO) anterior will be flared missing teeth 13.Penicillin allergy what type of sensitivity? Type I
14. How many mL in one TABLEspoon? 15mL (5mL in 1 TEAspoon)
15. Being out of pano trough
16. KNO3 as? Desensitizer
17. Pulp capping most successful? Age, Good Seal, Anatomy of Exposure, an isolated field
18. Where do you probe maxillary furcation? ML, DL, Facial
19. Epinephrine and Histamine what kind of reaction? Antagonist
20. Intruded primary max incisor 3 year old what do you do with tooth? Leave it alone?

21. How long do you splint after tooth has been avulsed? 1-2 weeks or 7-10 days
22. Semilunar incision? Apicoectomy of max central or premolar
23.Distal pocket with minimal KG what is the CI? Gingivectomy distal wedge
24.Longest lasting anesthetic? Bupivacaine 1:200,000, Articaine, Lidocaine 1:20,000, Mepivacaine
25.Why is occlusal table of primary teeth small? BL walls converge, Short MD length, Circular cusps, constricted CEJ with parallel BL walls
26.5 year old loses tooth which tooth would create problem? Primary 2nd molar
27.Chlorox for endo → NOT chelating agent
28.Peg lateral what is most likely? Unerupted max central, unerupted max lateral, impacted 3rd molars
29. pH that enamel starts to demineralize? pH 5.5 (critical pH of developing cavities)
30. What is the most important etiologic factor in getting caries? Saliva pH, Bacteria (or Refined Sugar), Fluoride treatment, saliva flow
31.For a lesion in enamel that has remineralized, what most likely is true?
a. The enamel has smaller hydroxyapatite crystals than the surrounding enamel b. The remineralized enamel is softer than the surrounding enamel c. The remineralized enamel is darker than the surrounding enamel d. The remineralized enamel is rough and cavitated
32.Where does caries start for proximal caries (class II)? Apical to proximal contact
33.Least efficient at testing vitality: thermal test, EPT, something about dentin
34. 40 year old patient with all 32 teeth. No cavities. Has stain and catch in pit of molar. What do you do? Watch and observe, sealant, composite
35. What would cause displacement of odontoblastic processes? Thermal, desiccation, mechanical, chemical
36.Burs for smoothing out preps? More flutes and shallow (this is what red burs are), more flutes and deeper, less flutes and shallow, less flutes and deeper
37.What is the most important thing for retention? Surface area
38. What causes the most retention of crown? Axial taper, surface area, surface roughness, retention grooves
39.What could be the reason you see opaque white porcelain in the incisal ⅓ facial of the PFM crown? Inadequate reduction of the inciso facial part of the tooth

40.The modified ridge lap pontic how should it touch the gum? Barely touch it (lightly contacts buccal side of ridge)
41.Most important when selecting shade? Value, translucency, chroma, hue, color
42.Supplies upper lateral eyelid? Lacrimal Nerve →
43.Infraorbital nerve branches from? Maxillary nerve (V2)
44. Red complex has 3 bacterias: P. gingivalis, Tannerella Forsythia, Treponema Denticola
45.Something about permissive occlusal splints: for parafunctional, myofascial pain? - TR
46. 65 year old patient shows several new caries in molars and premolars class V, what material would you use? Amalgam, composite, glass ionomer
47. Lasers and LED lights dont cure all resins because some resins photoinitiators have required light sources out of its range. True and correct logic
48. Which is NOT recommended for final FPD cast (or cast impression) impression? Reversible hydrocolloid, Irreversible hydrocolloid, Polysulfide, PVS
49.Abfraction (flexure of tooth)
50. Which syndrome has rash on cheeks, ulcers, kidneys, etc? Lupus
51. Separation (separation of basement membrane)? Benign mucous membrane pemphigoid
52. Both systemic and topical anti-fungal? Fluconazole
53. What problem causes bilateral angular cheilitis? High vertical dimension, low interocclusal space (low VDO), high occlusal distance
54. 85% of people have herpes
● 65-90% worldwide, 80-85% USA
55.Lesion on the palate that is verrucous and pedunculated? Papilloma
56. Pseudoepitheliomatous hyperplasia: granular cell tumor
57.Mixed density lesion in a young child? AOT
58. All of the following are differential diagonsis for Dentinogenesis Imperfecta except? Ectodermal dysplasia, amelogenesis imperfecta, enamel dysplasia, dentinal dysplasia, enamel hypoplasia (AI)
59. Malignant potential? Osteosarcoma
60. What causes pseudomembranous colitis? refers to swelling or inflammation of the large intestine (colon) due to an overgrowth of Clostridium Difficile (C. difficile) bacteria
61. Sialolithiasis (calcified salivary stone) is found where? Submandibular duct (wharton’s)
62. Sialoliths are most common in what gland? Submandibular gland and duct
63. What does tuberculosis lesion in the oral cavity look like? Large ulcer
● Painful non-healing indurated often multiple ulcers most frequently affected sites were the tongue base and gingiva. The oral lesions look like irregular ulceration or a discrete granular mass.
64. What is primary source of radiation to the operator when taking x-rays? Radiation left in the air, scatter from the patient, scatter from the walls, leakage from the x-ray head
65. What does collimation do? Reduces x-ray beam size/diameter and volume of irradiated tissue, reduces area of exposure
66. X-ray tube target metal is made out of? Tungsten (Target = tungsten/ Filter = Aluminum)
67. What does it look like on a pano when your patient moves during the pano? A vertical blur line (vertical distortion corresponding to when they moved) vs. horizontal defect
68.What kind of x-ray to visualize a supernumerary? Panoramic? -TR
69. If change from 8mm cone to 16mm, how much exposure time do you need to increase by? 2, 4, 6, 8
70. Which is greater risk for ORN? IV bisphosphonates for a year, radiation 65 grays
71. CASE: Patient on Zoledronic Acid → Osteonecrosis
72. What is the best way to test clotting function on a patient taking Warfarin? INR
73. Allergic to aspirin do NOT give? Acetaminophen, Codeine, Ibuprofen
74. Ginseng is an antiplatelet (interferes with coagulation -- NOT given with aspirin) Patient on warfarin, aspirin (Don’t mix the two)
75. Sign of hypoglycemia → bradycardia, Mydriasis (pupil dilation), Diaphoresis (Sweating), Mental confusion
76. CI for endo? Recent MI
77. Problem with Diabetes? Poor Healing
78. Hyperventilation causes Tachycardia and Tachypnea (rapid breathing after injection)
79. Treat Status Epilepticus: Midazolam (Versed)
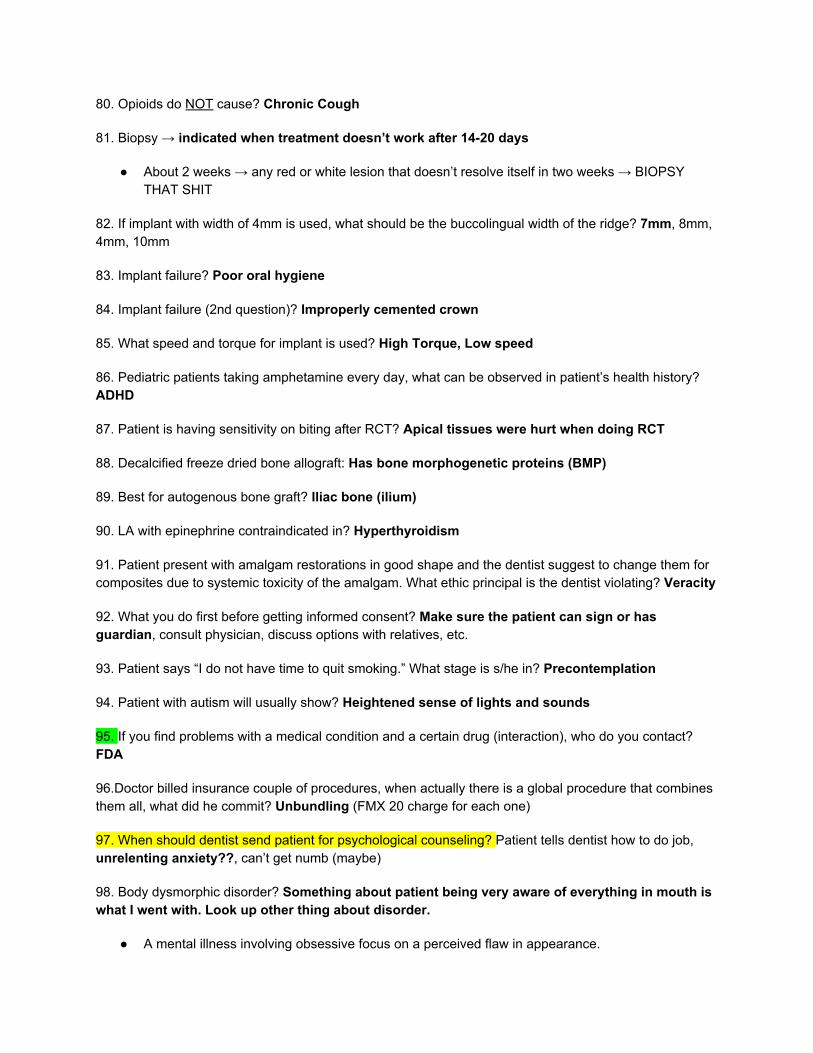
80. Opioids do NOT cause? Chronic Cough
81. Biopsy → indicated when treatment doesn’t work after 14-20 days
● About 2 weeks → any red or white lesion that doesn’t resolve itself in two weeks → BIOPSY THAT SHIT
82. If implant with width of 4mm is used, what should be the buccolingual width of the ridge? 7mm, 8mm, 4mm, 10mm
83. Implant failure? Poor oral hygiene
84. Implant failure (2nd question)? Improperly cemented crown
85. What speed and torque for implant is used? High Torque, Low speed
86. Pediatric patients taking amphetamine every day, what can be observed in patient’s health history? ADHD
87. Patient is having sensitivity on biting after RCT? Apical tissues were hurt when doing RCT
88. Decalcified freeze dried bone allograft: Has bone morphogenetic proteins (BMP)
89. Best for autogenous bone graft? Iliac bone (ilium)
90. LA with epinephrine contraindicated in? Hyperthyroidism
91. Patient present with amalgam restorations in good shape and the dentist suggest to change them for composites due to systemic toxicity of the amalgam. What ethic principal is the dentist violating? Veracity
92. What you do first before getting informed consent? Make sure the patient can sign or has guardian, consult physician, discuss options with relatives, etc.
93. Patient says “I do not have time to quit smoking.” What stage is s/he in? Precontemplation
94. Patient with autism will usually show? Heightened sense of lights and sounds
95. If you find problems with a medical condition and a certain drug (interaction), who do you contact? FDA
96.Doctor billed insurance couple of procedures, when actually there is a global procedure that combines them all, what did he commit? Unbundling (FMX 20 charge for each one)
97. When should dentist send patient for psychological counseling? Patient tells dentist how to do job, unrelenting anxiety??, can’t get numb (maybe)
98. Body dysmorphic disorder? Something about patient being very aware of everything in mouth is what I went with. Look up other thing about disorder.
● A mental illness involving obsessive focus on a perceived flaw in appearance.

● Body dysmorphic disorder is a mental disorder in which you can't stop thinking about one or more perceived defects or flaws in your appearance — a flaw that, to others, is either minor or not observable. But you may feel so ashamed and anxious that you may avoid many social situations.
99. Mycobacterium is the benchmark for? Disinfection
100. What fibers are involved in pulp testing? A delta
101. What is NOT included in the ADA Code of Ethics? Credential needs to be a dentist (licensure) (Licensure by credential), advertising, patient values, fees
102. Washing an X-ray film? To remove the processing chemicals
103. Acute adrenal insufficiency? Hypotension
104. Mode of action of ultrasonic? Vibration
105. All of the following drugs cause gingival hyperplasia except? Verapamil, Diltiazem (Calcium channel blocker), Phenytoin (Dilantin), Nifedipine, Cyclosporine. (Digoxin would be the one that does NOT cause it so if it gives this option pick it)
● All of the above drugs DO CAUSE THIS, but the question asked which DOESNT so IDK which answer to go with??
106. Apical position flap are contraindicated in what location? Maxillary palatal
107. Crown lengthening procedure, what would you do? Modified woodman flap or Apical reposition flap with osteotomy and ostectomy?
108. Which is contraindicated in 2nd molar region to reduce deep pocket with limited attached gingiva? Gingivectomy
109. FGM 1mm apical to CEJ 3mm probing. How much Attachment loss? 4mm
110. What is caused by smoking? COPD, Emphysema (Emphysema is a type of COPD)
111. CASE: 50ish year old guy needs RCT on #9 thats calcified. What would you most likely include in treatment consent? Perforation?, file separation (I put perforation but not sure though)
112. 40 year old with posterior cross bite, how to treat? Surgery (Suture osteotomy?)
113. Distobuccal denture? Masseter
114. Radiation to jaw? Cervical Caries
115. Tuberculosis lesion? Tonsilitis and Ulceration

116. Anticonvulsant drug for? Myelgia, Parafunctional habits, Neuropathic pain (Glossopharyngeal neuralgia and Trigeminal Neuralgia [Tic Douloureux and atypical facial pain])
117. Sealant and fissures therapy retention by? Retention with groove and pit mechanically, chemical, hybrid layer
118. Conscious Sedation? Patient can speak normally, patients eyes open, patient has body defense response
119. An examination of a complete denture patient reveals that the retromolar pad contacts the maxillary tuberosity at the occlusal vertical dimension. To remedy this situation, which of the following should be performed?
a. Reduce the maxillary tuberosity by surgery b. Cover the tuberosity with a metal base c. Increase the occlusal vertical dimension d. Reduce the retromolar pad by surgery
120. During try-in of mandibular denture, you want to check for? Full movement of the tongue and do all working movements
121. Patient feels fullness of upper lip after delivery of complete denture. Overextended labial flange
122. What will happen if mouth is opened while performing maxillary border molding? Coronoid process will block buccal extension
123. Posterior buccal extension of a mandibular complete denture is limited by? Masseter muscle
124. Patient has sickle cell anemia and has a thrombolytic crisis, what could precipitate this? Nitrous Oxide/ Oxygen use, Cold, Trauma, Infection
● Sickle cell anemia is seen exclusively in black patients. Periods of unusual stress or of O2 deficiency (Hypoxia) can precipitate a sickle cell crisis.
125. Most common in third molar extraction? Fracture, dry socket, paresthesia
126. Anti fungal effective in topical and systemic? Ketoconazole, Fluconazole
127. What is the effect of pKa on local anesthetic? Onset
128. Pure radiolucency? Ameloblastic Fibroma, AOT, Ameloblastic Fibroma Odontoma
129. Lymphadenopathy + being sick for 2-3 days + Petechia + Sore Mouth? Mononucleosis
130. Traumatic cyst → Aspiration biopsy
August 26th (pretty much Strawberry Pie File from my comparison… any answers in Red are from what the Strawberry Pie file says is the correct answer)
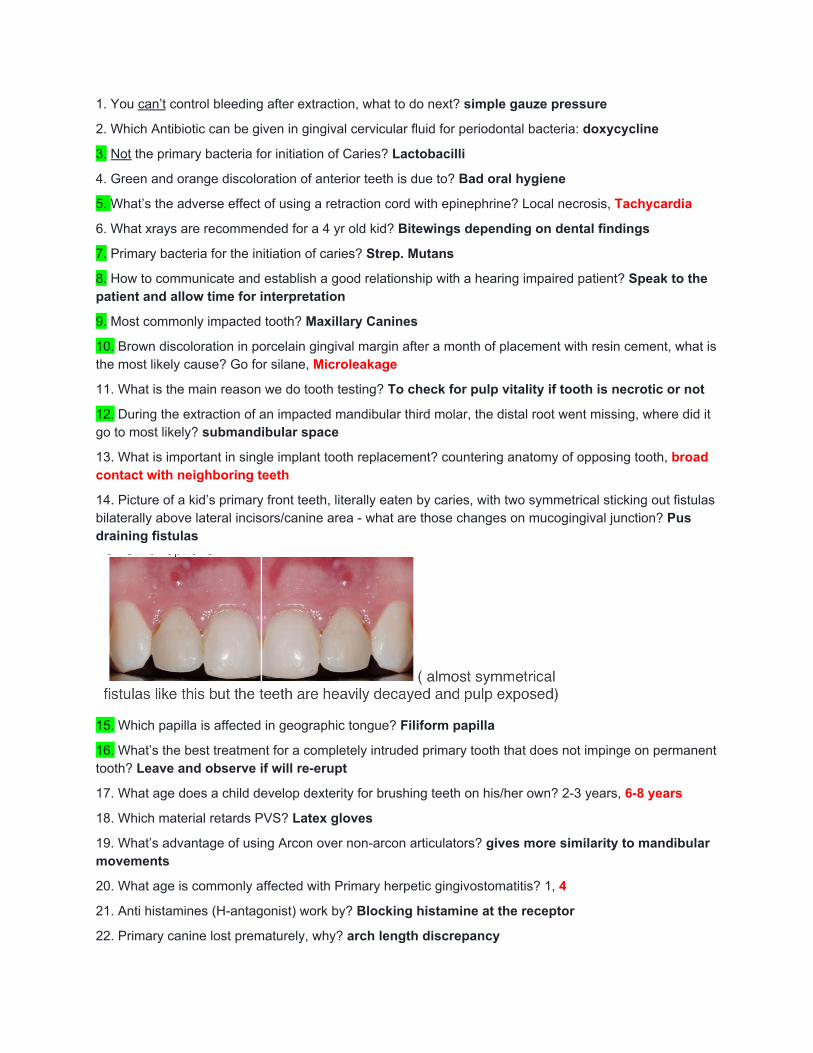
1. You can’t control bleeding after extraction, what to do next? simple gauze pressure
2. Which Antibiotic can be given in gingival cervicular fluid for periodontal bacteria: doxycycline
3. Not the primary bacteria for initiation of Caries? Lactobacilli
4. Green and orange discoloration of anterior teeth is due to? Bad oral hygiene
5. What’s the adverse effect of using a retraction cord with epinephrine? Local necrosis, Tachycardia
6. What xrays are recommended for a 4 yr old kid? Bitewings depending on dental findings
7. Primary bacteria for the initiation of caries? Strep. Mutans
8. How to communicate and establish a good relationship with a hearing impaired patient? Speak to the patient and allow time for interpretation
9. Most commonly impacted tooth? Maxillary Canines
10. Brown discoloration in porcelain gingival margin after a month of placement with resin cement, what is the most likely cause? Go for silane, Microleakage
11. What is the main reason we do tooth testing? To check for pulp vitality if tooth is necrotic or not
12. During the extraction of an impacted mandibular third molar, the distal root went missing, where did it go to most likely? submandibular space
13. What is important in single implant tooth replacement? countering anatomy of opposing tooth, broad contact with neighboring teeth
14. Picture of a kid’s primary front teeth, literally eaten by caries, with two symmetrical sticking out fistulas bilaterally above lateral incisors/canine area - what are those changes on mucogingival junction? Pus draining fistulas
15. Which papilla is affected in geographic tongue? Filiform papilla
16. What’s the best treatment for a completely intruded primary tooth that does not impinge on permanent tooth? Leave and observe if will re-erupt
17. What age does a child develop dexterity for brushing teeth on his/her own? 2-3 years, 6-8 years
18. Which material retards PVS? Latex gloves
19. What’s advantage of using Arcon over non-arcon articulators? gives more similarity to mandibular movements
20. What age is commonly affected with Primary herpetic gingivostomatitis? 1, 4
21. Anti histamines (H-antagonist) work by? Blocking histamine at the receptor
22. Primary canine lost prematurely, why? arch length discrepancy
23. Which occlusion is the most common in primary teeth? flush terminal plane ( AKA edge to edge)
24. Bimaxillary effect: relation of both jaws to the cranial base both jaws proclined
25. Case, patient with porcelain crown, a lot of caries, what would you suggest: all overnight treatments and had to pick which fluoride would be best; acidulated / 1.1% neutral fluoride / 0.4% not neutral
26. Which teeth most likely to be crowded/blocked out of mandibular arch? 2nd premolars
27. What doesn’t affect implant treatment planning? Age, Smoking history, Quality of the bone, Location
28. Best prognosis for implant? Anterior mandible
29. Nitrous oxide contraindicated in? first trimester only
30. Contraindication for using Nitrous oxide? Nasal congestion
31. Contraindicated with asthma, what can precipitate the attack? Aspirin
32. MOA of ibuprofen: reversible (non selective COX1 & COX2), irreversible platelet inhibition,
33. MRI is best used for TMJ to see: Disc
34. FAS syndrome (Fetal Alcohol Syndrome), what is characteristic: mid-face discrepancy
35. Most common abnormality among the following? Cleft lip and palate
36. diagnosis of lesion on the xray? ( stafne cyst) Salivary gland intravasation
37. Hepatitis A route of infection?Food and drink
38. Additional innervation to teeth is most likely from which nerve, since the LOWER molars didn’t anesthetize well? Mylohyoid nerve
39. Mandibular nerve exits the skull via? Foramen ovale
40. Most dental financing is from? Self-pay
41. Which cyst is not in bone? nasolabial
42. Progressing paresthesia of the lip is most likely due to? Malignancy
43. Firm painful nodule next to mental foramen? Traumatic neuroma
44. Neurofibromatosis - multiple neuro sarcomas, cafe au lait, lisch nodules of the iris
45. Hairy tongue, which papillae affected? filiform
46. Large amalgam MOD restoration, crack of the restoration in the isthmus, no symptoms, what is the best approach now? replace the entire restoration
47. Gutta percha outside of the apex after filling, what do you do? observe for now and wait for symptoms
48. How do you put the beaks on the tooth while extracting, pick false: parallel to the long axis, on the crown, as far as you can towards the roots
49. Subgingival caries, what do you do? crown lengthening
50. You are prepping the tooth for a crown, but realized, that the step is only 1 mm away from the alveolar crest, what do you do? crown lengthening
51. Plaque index is used mainly for: Patient motivation
52. A child’s behavior problem can be managed by desensitization if the basis of the problem is Fear
53. Disadvantages of oral sedation include which of the following? Unpredictable absorption of drugs from the GI tract
54. Auxiliary resistance from features in fixed dental prostheses such as boxes and grooves should ideally be located? Proximally
55. Which of the following would be LEAST likely to lead to the development of root surface caries on facial surfaces? Streptococcus sanguis dominating adjacent plaque
56. When a light beam passes through a mass, it reduces in intensity as it’s absorbed and reflected from different material surfaces, what does this describes? Refraction
57. A displaced fracture of the mandible courses from the angle to the third molar. This fracture is potentially difficult to treat with a closed reduction because of? Distraction of the fracture segments by muscle pull
58. Which of the following substances is contraindicated for a patient taking ginseng? Aspirin
59. What would explain leaking from rubber dam clasps on buccal surface of mandibular molar? Holes punched too close
60. Which term refers to a physician or dentist performing an operation for which there was no consent? Battery
61. A 32-year-old male patient reports a history of having been hospitalized for psychiatric evaluation, and is currently taking taking lithium carbonate on a daily basis. Which of the following diseases does this patient most likely have? Bipolar disorder
62. The patient should sign the informed consent for surgery? After a full discussion of the surgical treatment plan
63. Distinctly blue color of the sclera is a feature of which of the following conditions? Osteogenesis imperfecta (& Dentinogenesis Imperfecta)
64. A 16-year-old patient has a long history of mild pain in the area of the mandibular left first molar. Radiographs reveal deep caries in the tooth with an irregular radiopaque lesion apical to the mesial root. Which of the following represents the most likely diagnosis? Condensing osteitis
65. 6-year-old patient is uncooperative during treatment. Which of the following techniques is indicated? Voice control
66. Hypotensive effect and itching from oxycodone is due, in part, to its? Release of histamine
67. Which of the following does NOT produce a pharmacologic decrease in saliva production? Pilocarpine (Salagen) (Atropine, Scopolamine and Glycopyrrolate all DO decrease saliva production)

68. Which of the following is difficult to accomplish with extrinsic characterization of metal ceramic restorations? Increase value
69. The rubber dam does NOT protect patients from which of the following? Mercury vapors when removing old amalgams
70. Which of the following is responsible for creating a green discoloration in the marginal area of the metal ceramic restoration? Copper; (Other places of PFM turn green is due to Silver)
71. Removal of amalgam overhangs should be accomplished as part of initial therapy. Re-evaluation of the periodontal case should occur 4-6 weeks after the completion of the scaling and root planning procedures. Both statements are true
72. A patient has a severe tooth-size/arch-length discrepancy in the maxillary arch. Which of the patient’s permanent maxillary teeth are most likely to be blocked out of the arch? Canines
73. Which of the following contributes most to a successful pulp capping procedure? An isolated field
74. Which of the following has the greatest impact on the success of a periodontal flap procedure? Level of postoperative plaque control
75. The most common form of periodontal disease seen in school-aged children is? Marginal gingivitis
76. The procedure of choice for vertical maxillary excess is? LeFort I osteotomy
77. Periodontal flaps are frequently extended into non-diseased areas for adequate access to the diseased sites. These non-diseased root surfaces are not instrumented. The flaps are returned to their previous level where the flap collagen fibers reunite with the Sharpey’s fibers in the cementum of the root surfaces. Which of the following types of healing is described? Reattachment
78. Who is associated with the least risk of inhaling N2O? Patient
79. When adjusting the condylar guidance for protrusive relationship? the incisal guide pin on the articulator should be raised out of contact with the incisal guided table.
80. Deepest part of occlusal rest for RPD? Fossa
81. Swelling on lip after taking impression: Angioedema
82. During endodontic treatment you encounter a ledge inside the canal, What to do? Taka a smaller file and try to pass by
83. For big osseous defect, which graft is better? Autologous graft (Autogeneous graft)
84. Case. Patient comes with bilateral bone expansion, and complains about Dentures won’t fit? Paget’s disease
85. Open bite more than 8 mm, what you'll do? Le Fort 1 osteotomy
86. Boys and girls in school age study (want to do a study to compare DMFT of girls and boys in school, which test to use?): T-Test
87. Which medication to use for Benzodiazepines reversal: Flumazenil
88. A 20 yrs old patient with multiple jaw cysts, you suspect that he has syndrome so you refer him to specialist, what’s the most probable diagnosis? Gorlin , multiple OKC
89. The amount of radiation on a panoramic RX is compared to? 4 bitewings
90. What do you check in the wax try in Except: Obtain facebow record
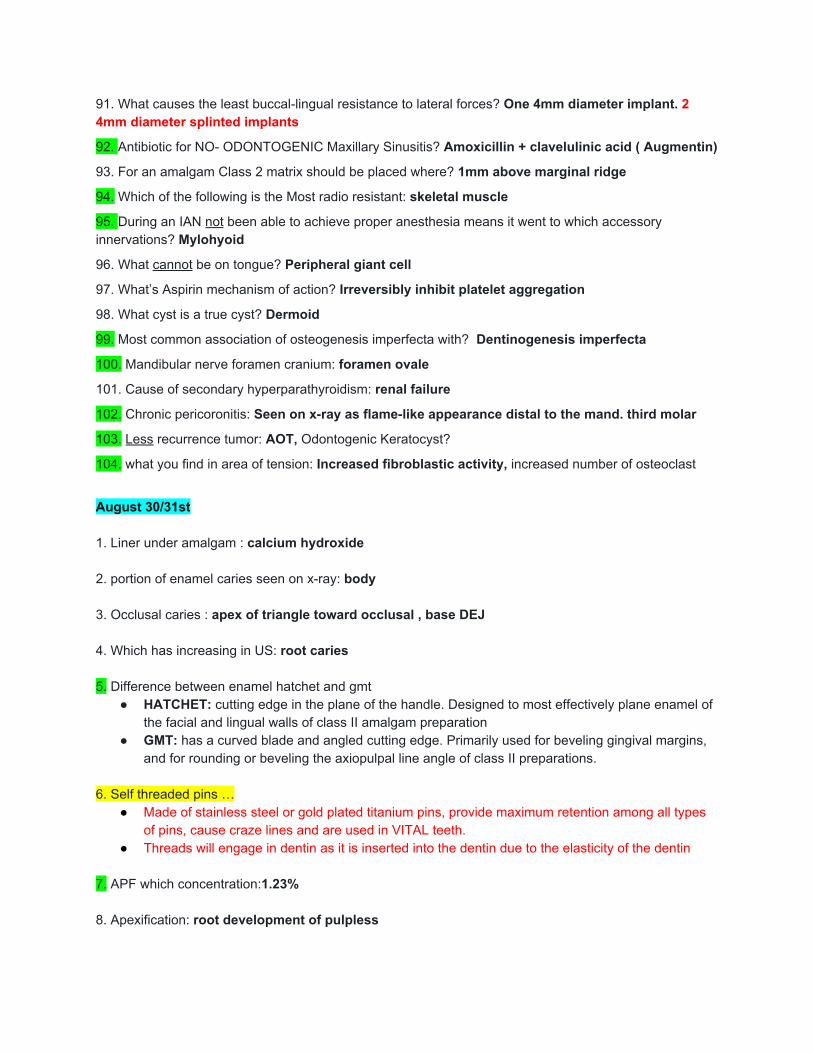
91. What causes the least buccal-lingual resistance to lateral forces? One 4mm diameter implant. 2 4mm diameter splinted implants
92. Antibiotic for NO- ODONTOGENIC Maxillary Sinusitis? Amoxicillin + clavelulinic acid ( Augmentin)
93. For an amalgam Class 2 matrix should be placed where? 1mm above marginal ridge
94. Which of the following is the Most radio resistant: skeletal muscle
95. During an IAN not been able to achieve proper anesthesia means it went to which accessory innervations? Mylohyoid
96. What cannot be on tongue? Peripheral giant cell
97. What’s Aspirin mechanism of action? Irreversibly inhibit platelet aggregation
98. What cyst is a true cyst? Dermoid
99. Most common association of osteogenesis imperfecta with? Dentinogenesis imperfecta
100. Mandibular nerve foramen cranium: foramen ovale
101. Cause of secondary hyperparathyroidism: renal failure
102. Chronic pericoronitis: Seen on x-ray as flame-like appearance distal to the mand. third molar
103. Less recurrence tumor: AOT, Odontogenic Keratocyst?
104. what you find in area of tension: Increased fibroblastic activity, increased number of osteoclast
August 30/31st 1. Liner under amalgam : calcium hydroxide 2. portion of enamel caries seen on x-ray: body 3. Occlusal caries : apex of triangle toward occlusal , base DEJ 4. Which has increasing in US: root caries 5. Difference between enamel hatchet and gmt
● HATCHET: cutting edge in the plane of the handle. Designed to most effectively plane enamel of the facial and lingual walls of class II amalgam preparation
● GMT: has a curved blade and angled cutting edge. Primarily used for beveling gingival margins, and for rounding or beveling the axiopulpal line angle of class II preparations.
6. Self threaded pins …
● Made of stainless steel or gold plated titanium pins, provide maximum retention among all types of pins, cause craze lines and are used in VITAL teeth.
● Threads will engage in dentin as it is inserted into the dentin due to the elasticity of the dentin 7. APF which concentration:1.23% 8. Apexification: root development of pulpless
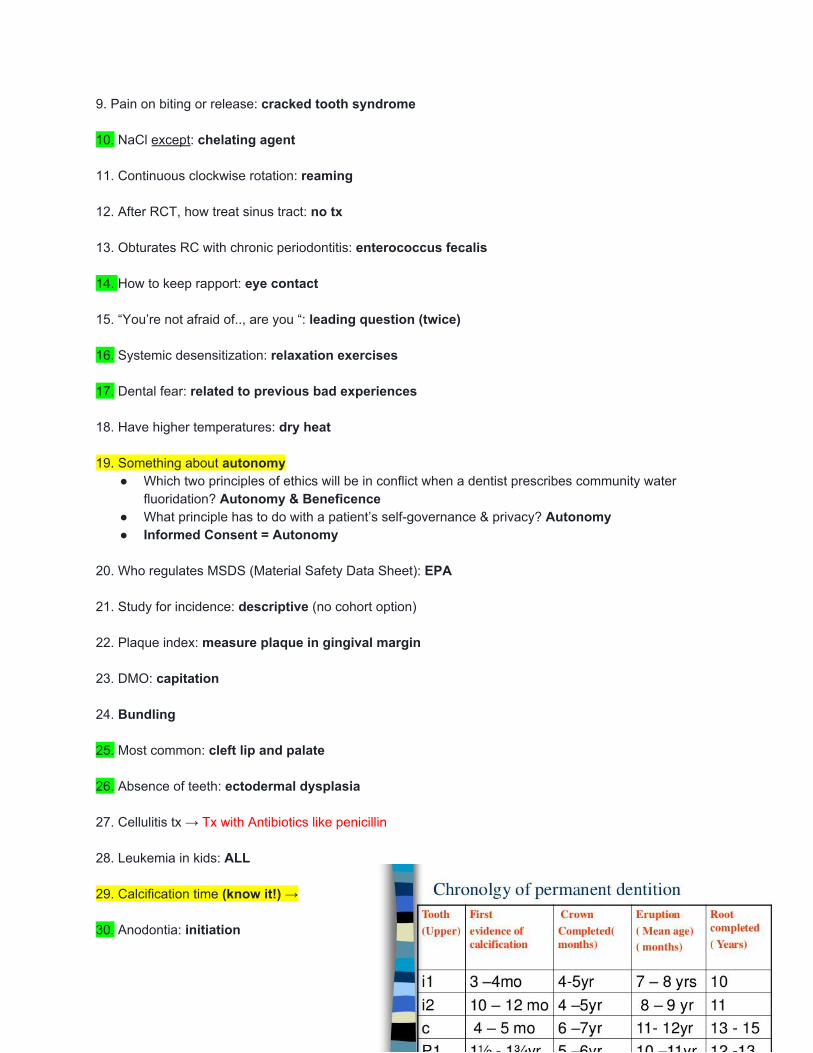
9. Pain on biting or release: cracked tooth syndrome 10. NaCl except: chelating agent 11. Continuous clockwise rotation: reaming 12. After RCT, how treat sinus tract: no tx 13. Obturates RC with chronic periodontitis: enterococcus fecalis 14. How to keep rapport: eye contact 15. “You’re not afraid of.., are you “: leading question (twice) 16. Systemic desensitization: relaxation exercises 17. Dental fear: related to previous bad experiences 18. Have higher temperatures: dry heat 19. Something about autonomy
● Which two principles of ethics will be in conflict when a dentist prescribes community water fluoridation? Autonomy & Beneficence
● What principle has to do with a patient’s self-governance & privacy? Autonomy ● Informed Consent = Autonomy
20. Who regulates MSDS (Material Safety Data Sheet): EPA 21. Study for incidence: descriptive (no cohort option) 22. Plaque index: measure plaque in gingival margin 23. DMO: capitation 24. Bundling 25. Most common: cleft lip and palate 26. Absence of teeth: ectodermal dysplasia 27. Cellulitis tx → Tx with Antibiotics like penicillin 28. Leukemia in kids: ALL 29. Calcification time (know it!) → 30. Anodontia: initiation
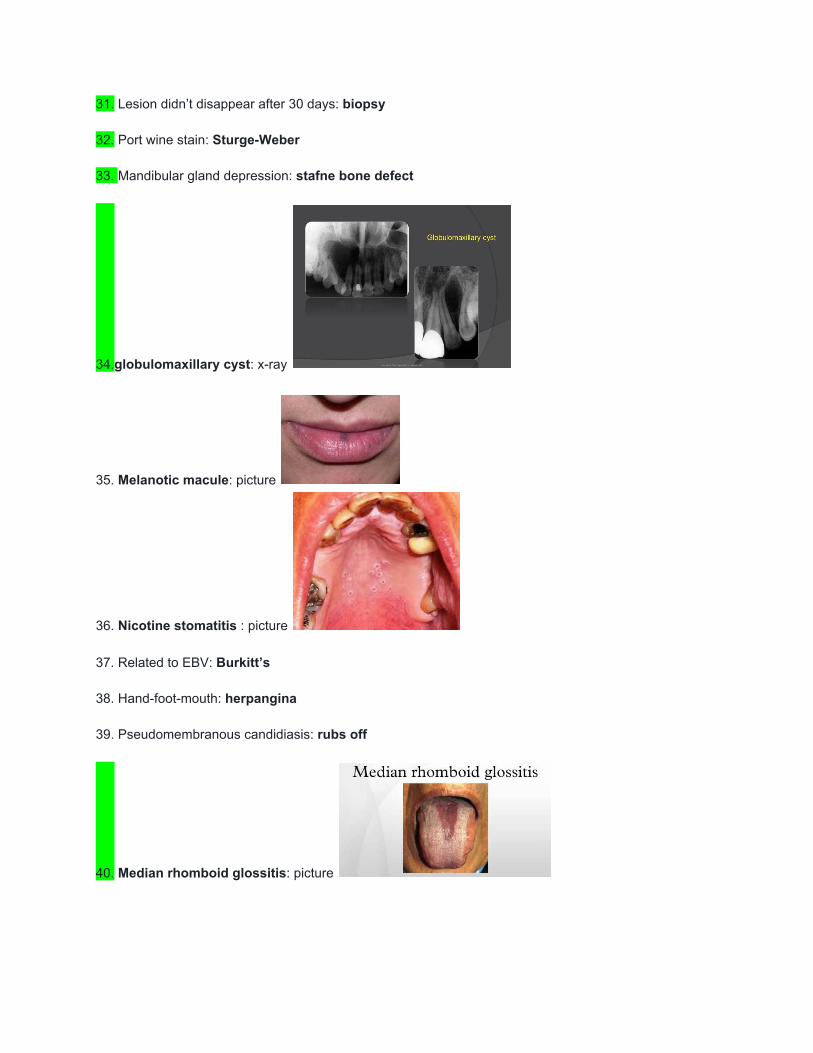
31. Lesion didn’t disappear after 30 days: biopsy 32. Port wine stain: Sturge-Weber 33. Mandibular gland depression: stafne bone defect
34.globulomaxillary cyst: x-ray
35. Melanotic macule: picture
36. Nicotine stomatitis : picture 37. Related to EBV: Burkitt’s 38. Hand-foot-mouth: herpangina 39. Pseudomembranous candidiasis: rubs off
40. Median rhomboid glossitis: picture
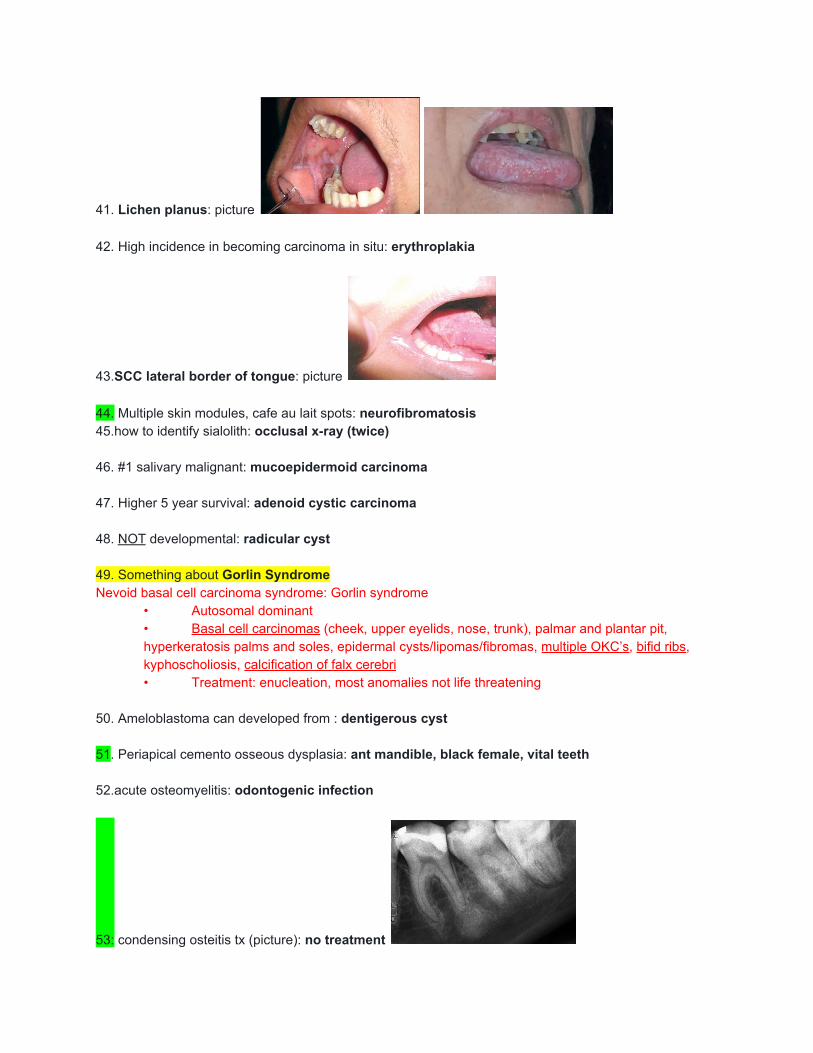
41. Lichen planus: picture 42. High incidence in becoming carcinoma in situ: erythroplakia
43.SCC lateral border of tongue: picture 44. Multiple skin modules, cafe au lait spots: neurofibromatosis 45.how to identify sialolith: occlusal x-ray (twice) 46. #1 salivary malignant: mucoepidermoid carcinoma 47. Higher 5 year survival: adenoid cystic carcinoma 48. NOT developmental: radicular cyst 49. Something about Gorlin Syndrome Nevoid basal cell carcinoma syndrome: Gorlin syndrome
• Autosomal dominant • Basal cell carcinomas (cheek, upper eyelids, nose, trunk), palmar and plantar pit, hyperkeratosis palms and soles, epidermal cysts/lipomas/fibromas, multiple OKC’s, bifid ribs, kyphoscholiosis, calcification of falx cerebri • Treatment: enucleation, most anomalies not life threatening
50. Ameloblastoma can developed from : dentigerous cyst 51. Periapical cemento osseous dysplasia: ant mandible, black female, vital teeth 52.acute osteomyelitis: odontogenic infection
53: condensing osteitis tx (picture): no treatment
54. Epi- histamine type of antagonism: physiological 55. Epi reversal: prazosin 56. Asthma contraindication: aspirin/ nsaid 57. Methemoglobinemia signs: cyanotic lips 58. Non ionized base: more lipid soluble 59. Anesthetic blocks: Sodium channel 60. 2% lidocaine: 36 mg 61. Midazolam: amnesia 62. BDZ reversal : flumazenil 63. Cimetidine: H2 receptor 64. Sulfa, methotrexate: folic acid inhibitor 65. Penicillin cross allergy to : cephalexin (MOA are closely related to each other) 66. Metronidazol: do not take alcohol 67. Coumadin and broad spectrum antibiotics: Broad spectrum antibiotics enhance the action of coumadin anticoagulants because of the reduction of Vitamin K sources.(Antibiotic medications are associated with an increased risk of bleeding among patients receiving warfarin.) 68. NSAID: ceiling analgesia 69. Cholinergic actions: salivation, lacrimation, urination, defecation 70. Treats xerostomia: pilocarpine 71. pedal edema, dyspnea, orthopnea: CHF 72. Warfarin which test: PT, INR?
● INR deals with PT; The higher the INR, the greater the anticoagulant effect (more bleeding, higher PT value)
73. INR:2 : do implant 74. After 3m extraction: ibuprofen + hydrocodone 75. Children controlled asthma: ASA 2

76. NO contrindication: psychotic disorder 77. NO nausea : turn off, give 100% O2 78: peri -mucositis: soft tissue inflammation 79. Cement retained implant → Need more interocclusal space for cement retained implants 80. Complete Denture buccal vestibule: buccinator 81. Combination syndrome Kelly Combination syndrome - when you have a maxillary complete denture over mandibular Class 1 Kennedy RPD.
● Has 5 characteristics: overgrowth of maxillary tuberosity, papillary hyperplasia of hard palate, bone loss in maxillary anterior, mandibular anteriors super erupt, and bone loss under distal extension of mandibular
82. Complete Denture clicking when speaking: excessive VDO (or decreased interocclusal distance (freeway space) → 83. “S” sound: teeth almost touch 84. palatal seal: compensates shrinkage of resin 85. Horseshoe strap: palatal torus 86. ClassIII MOD 1: palatal strap 87.prevents distal extension of rpd ‘loose’: indirect retainer 88.retentive clasp should seat: passively 89. Vitallium
● Vitallium is a trademark for an alloy of 65% cobalt, 30% chromium, 5% molybdenum, and other substances. The alloy is used in dentistry and artificial joints, because of its resistance to corrosion.
90. Less gingival tissue: facial pm 91. Retraction cord: epinephrine (will cause increase in HR) 92. Minimal height gingival incisal to crown: 4 mm molars 93 . Short clinical crown: buccal grooves for retention, proximal grooves increase retention/resistance on short teeth 94. Connectors for pfm should increase what for resistance: height

95. More stable: PVS ( no polyether in options) 96. Highest Coefficient of Thermal Expansion (CTE): composite 97. Eugenol: inhibits polymerization of resin 98. Zirconia: luting cement 99. Aging values: decreases 100. Non working interferences: LUBL 101. Biological width: JE+ CT 2mm 102. Best for GTR: 3 wall defect 103: LAP: 1M (IDK what the hell LAP stands for -TR) 104.pellicle formation: within seconds 105.plaque 72 hours: anaerobic gram negative (-) bacteria 106. First step in perío do: plaque control and patient education 107. Maintenance phase: every 3 months 108. Increase perio Risk factor: smoking 109. Gracey 13-14: posterior distal 110. Split thickness: mucosa and submucosa 111. Gingivectomy: external bevel 112. Gingivectomy: secondary intention healing 113. Osteoplasty : non supporting bone 114: autograft: osteogenic (ONLY ONE) 115: host modulation therapy: periostat 116. kVp: energy
● kVp: ability for the beam to penetrate tissues, energy ● YOU WANT TO HAVE HIGH kVp AND LOW mA for MOST penetration
117. Latent period: from exposure to onset of symptoms

118. Wavelength affected by: kVp 119. Pterygomandibular raphe: buccinator, sup phar. Constrictor
The pterygomandibular raphe (pterygomandibular ligament) is a ligamentous band of the buccopharyngeal fascia, attached superiorly to the pterygoid hamulus of the medial pterygoid plate and inferiorly to the posterior end of the mylohyoid line of the mandible.
● Its medial surface is covered by the mucous membrane of the mouth. ● Its lateral surface is separated from the ramus of the mandible by a quantity of adipose
tissue. ● Its posterior border gives attachment to the superior pharyngeal constrictor muscle. ● Its anterior border attaches to the posterior edge of the buccinator.
120. Inferior alveolar + lingual nerve block: extract entire quadrant of teeth 121. Distance between implants: 3mm (distance between implant and adjacent tooth = 1.5mm) 122. Best place for implant : anterior mandible