reducing health disparities with serious mental … the population without a seriots mental illness....
TRANSCRIPT

Chapter Os*Chapter 05 4116rtg 11:04 AM Page 62 -+-
Reducing Health Disparities for People with Serious
Mental Illness: Development and Feasibility of aPeer Health Navigation Intervention
fohn S. Brehl<e, Elizabeth Siantz, Rohini Pahwa, Erin Kelly,Louise Tallen, and Anthony Fulginiti
People with serious mental illness die, on average, twenty-fle gears earlier than those
in the population without a seriots mental illness. This disparity is largely due to treat-able medical conditions that remain unaddressed due to factors at the client, treattnent,providen dinic, and splstem levels of health and mental health service delivery, Thisarticle describes the development, initialimplementation, andfeasibility oJ the Bridge,a peer-staffed care linkage motlel situated in a mental health clinic that addresses bati-ers at multiple levels ol service delivery by connecting clients to physical health services
and developing client skills that result in self-management of health care. The tsridge
,A was developed collaborativelg with interventionists, clinic staff, and mental health peers
Y andrelieslargely onaninvivo approach.
Keg words: health; health disparities; health navigation; intervention; seriousmental illness
People living with serious mental illness in the United States die, on average,
twenty-five years earlier than those without a serious mental illness, largely due topreventable medical conditions and suboptimal medical care (Parks, Svendsen,
Singer, & Foti, 2006). Studies have found a higher incidence of certain physical
disorders, such as diabetes (Dickerson et al., 2006; Lestet Tritter, & Sorohan,2005), obesity (Parks et al., 2006), high cholesterol or dyslipidemia (Dalmau,
Bergman, & Brismar, 1997), metabolic and cardiovascular problems (Brunero &Lamont, 2010; Deakin et a1., 2010), and cancer (Brown, 1998), among people
John S. Brekke, PhD, is professor at the School of Social Work, University of Southern California,Los Angeles. Also at the School of Social Work, University of Southern California, Los Angeles,Elizabeth Siantz. MSW, is a PhD student; Rohini Pahwa, MSW is a PhD candidate; Louise Tallen,PhD, is project manager; and Anthony Fulginiti, MSW is a PhD student. Erin Kelly. PhD, is post-
doctoral fellow at the Health Services Research Center, University of California, Los Angeles. Thispilot study was funded with support from the UniHealth Foundation, and the Los Angeles BasinClinical Translational Science Institute at the University of Southern California.
@ 20t I Lyceum Books, Inc., Best Practices in Mental Health, Vol. 9, No. 1, March 201 l

Chapter Os-Chapter 05 4t16l1g 11:04 AM Page 63 S
Reducing Health Disparities Jor People with Serious Mental lllness 63
with serious mental illness. When combined with a serious mental illness, physi-cal illness can lead to other health conditions (Dickerson et al., 2005) and to aquality of life lower than that of both the general population and individuals withmental iilness alone (Desai, Rosenheck, Druss, & Pearlin, 2002; Dickerson et al.,200ti). These negative health consequences can affect other recovery goals suchas housing, vocational training, and education (Bazelon Center for Mental HealthLaw [BCMHL],2OO4).
lndividuals with serious mental illness also face numerous barriers to access
and use oi health care services needed to prevent and manage chronic diseases atmultiple levels of the service delivery system (De Hert et al., 2011; Druss, Rask, &Katon, 2008). At the system level, the chasm between the health and mentalhealth care systems impedes access to ca-re in both systems and reduces coordina-tion of services (Miller, Druss, Dombrowski, & Rosenheck, 2003). Environmentalbarriers include difficulties in finding a specialist, long waits in clinics, trans-portation dfficulties, geographical distance, and cost (Dickerson et al., 2003:
Jeste, Gladsjo, Undamet & Lacro, 1996). Provider-level barriers lbr people withserious mental illness include Iimited training of mental health professionals inattending to their physical health concerns (Brown, 1998), limited training of pri-mary care physicians in working with people with serious mental illness (Leigh,Stewart, & Mailios, 2006), and the stigma endured during encounters with healthproviders (Goldberg et al., 2OO7). At the individual level, additional barriers mayresult from mistrust of the system, lack of knowledge and resources, and behav-ioral or cognitive challenges in understanding and accessirlg services, along witheducational, cultural, and language hurdles (Bradford, Coleman, & Cunningham,2007; Cohen & Krauss, 2003; Dickey, Normand, Weiss, Drake, & Azeni, 2002).
The high incidence of comorbid diseases among people with serious mental ill-ness contributes to the high cost of health care for those who receive specialtymental health services (BCMHL, 2004), leading to increasing demands for solu-tions, nationally and internationally (Hedberg & Skiirstiter, 2009; Kane, 2009;Maj, 2009; Shattell, Donnelly, Scheyett, & Cuddeback, 2011). The integration ofhealth and mental heaith services is a means to address the fragmentation ofhealth and mental health service systems (Anderson & Knickman, 2001; Drusset al., 2008; Goldberg, 1999). This article will discuss the conceptual model,development, and feasibility of an innovative community-based health navigatorintervention for people Iiving with serious mental illness.
Models for Integrating Services
The Bazelon Center for Mental Health Law (2004) has identitied the followingmodels for integrating health and mental health services for individuals with seri-ous mental illness: (1) embedding of health care providers within mental healthprograms, (2) full-service health and mental health delivery programs housed inthe same agency, and (3) collaboration between independent health and mentalhealth providers. The lrst two models involve co-situated care, and the third is a
I
9

I
CnaOt"r os-Chapter 05 4t16t1s 11:04 AM Page 64 -e-
IY
64 BestPractices in Mental Health
care linkage model. These approaches address different barriers to care. Althoughco-situated approaches would appear to address more barriers, they require sig-nificant change in both health care policy and the structure and Iinancing of ser-
vice delivery (Goldberg, 1999). For example. although co-situated service pro-grams show some impact, they are still challenged by separate funding streams forhealth and mental health services. Another barrier to integration is the differencein reimbursement plans for health and mental health services (BCMHL, 2004).Even with Medicaid. individuals with serious mental illness are served throughfee-for-service arrangements, whereas physical health is addressed via managedcare services (Goldberg, 1999). Moreover, integrating care contracts does notnecessarily result in more integrated and efficient services (Laws, Gabriel, &McFarland, 2002; Stroul, Pires. & Armstrong, 2001;Vogel, 2001).
The third model, care linkage, improves collaboration between independenthealth and mental health providers and could be implemented in the context ofmany existing financing and service structure arrangements. One randomizedstudy has shown increased utilization of primary care service by individuals rn ithserious mental illness, increased preventative care visits, and better health out-comes when separate health and mental health services are coordinated by anurse case manager (Druss. von Esenwein. et al., 2010). Although care iinkagedoes not require co-situated health and mental health care, the use of highly paidprofessionals may introduce other cost considerations.
Care Linkage and Peer Providers
A promising alternative to care linkage provided by professionals is the use ofpeer providers to deliver these services (New Freedom Commission on MentalHealth, 2003). Peer providers bring their own experience of living with a mentalillness to assist clients with serious mental illness. Peers are one of the most rapidlygrowing segments of the mental health workforce in the United States (Druss,
Zhao, et al., 2010), and peer-run interventions are becoming prominent in therecovery Iiterature (Rosenick & Rosenheck, 2008; Solomon, 2004). Peers can be
trained to work in a variety of settings to promote recovery and wellness (Cook,
2005; Davidson et al., 1999; Davidson, Chinman, Se1ls, & Rowe, 2006; Rosenick& Rosenheck, 2008; Solomon,2OO4), and potentially offer more cost-effective ser-
vices than other options (Battaglia, Rolofl Posner, & Freund, 2007; Jandorf et al.,2006; Steinberg et al., 2006). Furthermore, this peer provider option can offertraining and employment opportunities to persons with serious mental illness andprovide them with a stronger role and voice within these systems, a key goal of theRecovery Movement.
Peer interventions build on the experience and sensitivities of peers to focus onpractical issues of access and utilization of health services. For example, individu-als with a history of cancer have been used to help women with breast canceraccess services (Darnell, 2007; Dohan & Schrag, 2005), Similarly, HIV/AIDS
o

I CnaOter os-Chapter 05 4t16t13 11:04 AM Page 6s -e-
Reducing Health Disparities Jor People with Serious Mentallllness 65
services have applied this model to reduce barriers to service utilization (Bradford
et al., 2007), and such models are thought to be an effective strategy for address-
ing obstacles to accessing health care services. At present, only one randomizedpilot trial, in which trained peers led manualized group pyschoeducation classes
on chronic disease management for participants with serious mental illness, hasbeen completed (Druss, i4hao, et al., 2010). Compared to participants whoreceived treatment as usual, participants who completed the course showedhigher rates of utilizing primary care services (68.4% vs. 51.9%), more patientengagement in self-managing their health and health care, and higher quality ofphysical health. These results. although promising, may also suggest that patientsmay require signiticantly more assistance to see substantial improvements in well-being.
Given the potential benefits of a care linkage model with peer providers, theauthors developed and impiemented an intensive, individualized, peer health nav-igator intervention to facilitate access to physical health care for people diagnosedwith serious mentai ilhess who are engaged in the publicly funded mental healthsystem in Los Angeles.
Theoretical Framework for Peer Health Navigation
Improving the physical health of people living with serious mental illness is acomplex challenge, resulting from numerous factors at the levels of the individual,the provider, the health care system, and the broader geographic and sociopoliti-cal environment. A sound conceptual framework is important for organizing themultipie factors that contribute to the use of health services and the physicaihealth status of people living with serious mental iliness, and can provide a roadmap for addressing factors to be targeted by an intervention.
The conceptual model underlying this intervention tailors Gelberg, Andersen,and Leake's (2000) Behavioral Model of Health Service Use for Vulnerable Popu-lations (BMHSUVP) for those with serious mental illness. Gelberg and colleaguesposit that health services usage is determined by a combination of predisposingcharacteristics (demographic, social structure, and health beliefs), enablingresources (personal/family and community), need for care (perceived and evalu-ated), and personal health care habits (diet. exercise, and self-care). lmportantly,this model includes not only factors that lead to health care utilization, but also
factors that influence the effectiveness of those services. To tailor this modei forthose with serious mental illness, a series of focus groups and interviews was con-ducted with clients, stafi and administrators from health care and mental healthcare agencies. Based on the information obtained in these interviews, it becameapparent that the BMHSWP model omits some important factors that suppress
health service utilization among those with serious mental illness-namely severepsychiatric symptoms, stigma, and system bifurcation. The adapted theoreticalmodel is shown in figure 1,

=t(!Pco
loc,trtOJ
E#
o
{r-E'o
OJ
EoUFfoE(I'Lo't(!
-C(Ua!
=oo-aLJcDiI
+
I
Cnanteros-Chapteros 4/16/13 11:04AM Page66 -e-
66 Best Practices in Mental Health
oEg -------->
oA
I
- r----:-lts l€ e.9 IF lr.9= IE <_ lgEalE llrElA-|
-ol> I-G le-.E ltO loll <!- lE -.-c IEE iE lErsi- ltE-"
tgl Ilul I .el9l<_ leE qto-t to = El;^l ltE H
l+l r----j-lll I rI ll l=,r€I I ls=€
lE l-- l; s;I I l.:sl:I I I O d, Ilrl lEis
l'll=lorl l.> gI E I t'= E
l-ol Is ; ilEl - I*En-:l;l lE EsEtlltlllPl | -l8l l.s E
ltl-- lg-ril'l l5_1::
a>!ooC -N.9 bE EE
5E E5E xf t*= .sta.E ;;E
qa q 6! 6oA'i.idi
Pofr-E lxE ,€e'E= bu- Ee; cii 6E5 -9"U".9E il= I6 h! A iiE.g€Ee e fiE +gE:^:: g:3 frf;
e!, EE=a- sH,Ec
i ;gii:elsfiE E EE= ;*eef;
o-
- s ;:e:g# * =: E-- E.-,9 E f E;9;g E -EEE E6 F9q." g; E;;€:Es EeEeE;EsE-E€f q
PesE ;iEieCg I;ScSs9! iE=s;ai-"i; g- ^j ni E;^ia$-i6N ddP
-+-
-l_
Y

Chapter 0s-Chapter 05 4t16t1g 11:04 AM Page 67 -e-
Reducing HealthDisparities Jor People with Serious Mentallllness 67
The model's predisposing domain includes participant demographics such as
age, gender, and marital status; health beliefs including values concerning healthand illness; attitudes toward health services and knowledge of disease: factors
related to social structure including ethnicity, level of education, employment sta-
tus, social netrvorks, occupation. religion, acculturation, immigration status, lit-eracy, living conditions. victimization. and psychoiogical resources (e.g., mastery.
coping, selfl-esteem. cognitive abiliry and substance abuse). Even if services
are accessed, clients with serious mental illness may be predisposed to negative
experiences with physiclans as symptoms of their disorder, and cognitive deficits
can make communication more difficult and stressful (Berren, Santiago, Zent, &Carbone, 1999).
The enabling domain includes personal and community characteristicsrequired for the hea-lth care interaction to take place (Gelberg et al., 2000). Theproposed model includes personal and family resources such as access to a regu-Iar source of care, insurance, income, social support, perceived barriers to care,
self-help skills, ability to negotiate the system, and communiry resources such as
establishing residence and availability of health services, case management,transportation, telephone, and other information sources.
The need domain includes self-assessment or professional assessment thathealth services are required to treat health conditions specilic to an adult Iivingwith serious mental illness. Clients' perceptions and clinicians' evaluations oftheir clients' physical health status may be inlluenced by the presence of seriousmental illness (Gelberg et al., 2000). Physical health treatment and preventive
care such as cervical screenings, mzlmmograms. and immunizations (Carney,
Allen, & Doebbeling, 2002; Druss, Rosenheck, Desai. & Perlin, 2002) may be given
secondary priority relative to care for active psychiatric symptoms, maintainingstable housing, and financial insecurity (BCMHL, 2004).
Personal health behaviors play an important role in service needs (Gelberg et
al., 2000). Diet, exercise habits, self-care habits, and substance use can have pow-erful influences on hea-lth status (Compton, Daumit, & Druss, 2006). Even ifhealth habits are not poor, increased morbidity and mortality associated with seri-
ous mental iliness can be traced, in part, to second-generation antipsychotic med-
ications currently used to treat this condition. Studies have linked weight gain,
dyslipidemia, diabetes, insulin resistance, and metabolic syndromes to these med-
ications (Gianfrancesco, Grogg, Mahmoud, Wang, & Nasrallah, 2002; Hippisley-
Cox, Vinogradova, Coupiand, & Parker, 2007; Kreyenbuhl, 1999). Clients may be
reluctant to seek out medical care due to concerns that they will be judged orblamed by their physicians for their self-care habits, motivational deficits, and lowself-esteem (Dickerson et al., 2006). Moreover, clients who have difficulties inthese domains are particularly likely to have difficulty adhering to treatmentregimes or following a physician's inskuctions.
Stigma has a pervasive influence on the receipt of health care among those
with serious mental illness. Stigma refers to imputed personal characteristics thatidentily persons as being undesirably different from normal, and may result in
o

I CnrOt"r os-Chapter 05 4tt6h3 11t04 AM Page 68 1)
68 Best Practices in Mental Health
negative self-attributions as well as devaluation by others (Link & Phelan, 2001).When the stigma is mental illness. negative attitudes can Iead to avoidance anddiscrimination on the grounds of perceived unacceptability or inferiority. The con-sequences of stigma can include decreased life opportunities, loss of independentfunctioning, and decreased use of physical health services among people livingwith serious mental illness (BCMHL. 20O4). Moreover, recognizing oneself as amember of the deva,lued group can have negative effects on one's self-concept(Link, 1987; Link & Phelan, 2001; Scheff, 1994) and lead to fear of discrimina-tion and feelings ol shame. Physical health providers are not immune to stigma-tizing attitudes and behaviors toward individuals with serious mental illness(Goldberg et al., 2007). These attitudes may be rooted in the fear of unpredictablebehavior and concern with regard to an individual's noncompliance with treat-ment. Some primary care providers report concerns that people with serious men-tal illness may become bizarre, agitated, disorganized, or even violent in their wait-ing rooms (BCMIIL, 2004). These negative attitudes can cause individuals livingwith serious mental ilhess to receive poor qualily of care from the physical healthcommunity (Goldberg et al., 2OO7).
System bifurcation is the separation of physical and mental health services,
which poses a serious issue for those with chronic mental and physical healthissues. At a system level, at least four types of separation between mental andphysical health care may exacerbate the problems for persons with serious mentaiillness:
1. geographic, or lack of colocated medical and mental health services;
2. financial, including but not limited to separate funding streams for medicaland mental health services;
3. organizational, or difficulty in sharing information and expertise across
these systems; and4. cultural, or provider focus on particular symptoms or disorders rather than
on the persons with those problems (Druss & Newcomer, 2007).
Bifurcation discourages people with a mental illness from accessing and utiliz-ing services (Lieberman & Coburn, 1986). Current insurance policies reinforcethis bifurcation because neither Medicare nor Medicaid pays for two services onthe same visit. The Los Angeles County Department of Health Services has sug-gested that the cost of treating a person with serious mental illness can be tentimes that of treating a client without mental illness in a public health clinicbecause clinics are paid a flat fee regardless of case complexity. This provides littleincentive for doctors or clinlcs to treat those with serious mental illness. Mentalhealth professionals are unable to provide health services, as physical health careis beyond their scope of practice or training and is not reimbursed by mentalhealth funding streams (Brown, 1998). Hence, even colocated services requiremultiple visits and pose structural barriers to adequate care, and in addition to theIiscal divide, the separation of the professional cultures of physical and mental

Chapter Os-Chapter 05 4t16t1g 11:04 AM Page 69 -e-
Reducing Health Disparities for People with Serious Mental lllness 69
health systems can cause mutual mistrust and rivalry (BCMHL, 2004). Differ-ences between physical and mental health care provision can also exist in terms ofinformation storage and sharing, software compatibility, privacy rules, and pro-fessional standards.
This understanding of the multifaceted challenges of integrating health andmental health care for the population with serious mental illness led to the devel-opment of the Bridge peer health navigator intervention.
The Bridge: A Peer Health Navigator lntervention
The Bridge health navigator intervention was developed using a coliaborativeapproach including the members of the research team, service providers, andpeers. The intervention was based on the model, presented above, of the barriersthat Iead to problematic health access, utilization, and outcomes for people livingwith serious mental illness. The model addresses system bifurcation and practi-tioner issues, and is designed to assist clients regardless of their symptom severityor functional level. The use of peer intervention can help ameliorate stigma forclients, as peer erperiences with mental illness may provide a common ground tobuild rapport, an essential component of this type of intervention. The Bridgeintervention moderates the impact o[ the factors that impede both service utiliza-tion and health outcomes by strengthening the enabling factors and amelioratingthe suppressing factors. The four components of the intervention are assessmentand planning, coordinated linkages, consumer education, and cognitve-behavioralstrategies. A cenha-l goal of the Bridge is to give clients the skills and experiencenecessary to self-manage their health care activities to the greatest degree possible
after the intervention ends.
Assessing and Planning
In order to plan what assistance is needed, the navigator tahes the clientthrough a thorough assessment of his or her health status, current use of healthservices, and experience with accessing and using health services, as weil as bar-riers encountered. This process results in a collaborative health navigation plan,which includes the client's health care and welhess goals (Mueser et al.. 2006). Astep-by-step strategy is then developed to guide the goal-directed activity and toprovide a basis for monitoring progress. This activity increases clients' awareness
of their health care needs and their history of health care service use, whichincreases their motivation to participate in navigation and sell'-managementstrategies.
Coordinated Linkages
Based on an integrated care linkage model (BCMHL, 2OO4), coordinated link-ages consist of several activities that assist clients as they navigate the health caresystem, including helping them make appoinfments, communicate with a range of

Chapter Os-Chapter os 4t16t'13 11:04 AM Page 70 -e-
70 Best Practices in Mental Health
medical care providers, and ensure follow-up care; handling pharmacy and spe-
cialty care issues; and ensuring adherence to medical treatment plans. This modelwas drawn partly from patient navigation interventions developed for people withcancer and people with HIV (BattagJia et aJ., 2OO7; Bradford et al., 2OO7; Darnell,2007; Dohan & Schrag, 2005: Jeste et al., 1996; Steinberg et al., 2006). Peer nav-igator experiences, with both their mental illness and their navigation of physicalhealth and mental health services, make them uniquely sensitive to and arvare ofchallenges their peers face. The method is also based on the principles of AssertiveCommunity'l'reatment (Stein & Test, 1980; Test et al., 1991), in that an in vivoapproach to Iinkage and training activities is stressed. Compared to models thatpredominantly use a classroom training approach, (e.g., Goldberg et al., 2013), theBridge features an in vivo approach that develops self-management skills in real-world health care settings. The in vivo approach is important because these real-world health care settlngs are ideal for teaching and learning self-managementskills that are sustainable.
Consumer Education
The third intervention component is consumer education, which is based onprinciples of patient education (Prohaska & Lorig, 2000). Patient education is the-oretically rooted in the health belief model, in which an individual's response toillness is rooted in his or her beliefs about health and health care, Hence, provid-ing knowledge to alter health beliefs can lead to better subjective perceptions ofhealth and better decisions about illness and its management (Goldman & Quinn,1988; Prohaska & Lorig, 2000). For the current intervention, the consumer edu-cation component includes education about the health care system, how to part-ner with medical providers, treatment compliance, self-advocacy, appropriateinteraction skills, and health and wellness issues (such as regular health care, diet,and exercise), as well as education about health benelits and entitlements.
Cognitive-Behavioral Strategies
The fourth intervention component is the use ol cognitive-behavioral strate-gies to support behavior change and maintenance with regard to health care uti-lization, and is based on cognitive-behavioral and social learning theory (Dobson
& Hamilton, 2002), Central to the intervention is a method for guiding the behav-ioral work, rvhich is expressed explicitly and succinctly as for them, with them, by
them. Using behavioral strategies oi modeling, role playing. coaching, and fading,peer navigators enhance client skill development, using a systematic process thatentails gradually shifting navigation activities to the client (fading) with the aim ofmaximizing the client's management of his or her health care to the greatest
extent possible.
As an example, making a medical appointment by phone can be challenging.At first, the navigator makes the appointment with the client watching and lis-
+

] Cnanter Os-Chapter 05 4116t13 11:04 AM Page 71 -e
Reducing Health Disparities for People with Serious Mental lllness 7l
tening on speaker phone (/or them. or modeling). The next time, the client makesthe call with the navigator present as a coach, or as the recepfionist in a role play(with them, or coaching). Finally, the navigator fades and lets the client make thephone cail independently (by them) while continuing to act as a reinforcer, sup-porter, or collaborative problem solver if complications arise. Although theauthors prefer in vivo coaching and learning, role playing can also be done ifclients have sufficient skill. These strategies are complemented by user-friendlyself-instructional and self-help cognitive-behavioral strategy guides for the peernavigator. This training method is used for all skill building aspects of the inter-vention and becomes the foundation lor self-management.
ln addition to these four components, the intervention also addresses screening
il*".rlt"*"-ent, intervention ta-rget points, the intervention timeline, and out-
Screening and Client Engagement
The Bridge intervention is based on appropriate screening and engagement.The authors have developed a six-item screening tool that targets current healthproblems and health service use. The tool is designed so that an inclusionaryresponse on any one of the six items indicates the need for health navigation. Thescreen can be administered in a self-report or interview format (in person or byphone). It has been used by health navigators, by case managers, and by staff aspart of agency intake forms. Once a positive screen occurs, the navigator meetswith the client (ideally in person) and uses an engagement script that details thenavigator intervention, the roles of the navigator and the client, the activities thatwill occur, and the timeline. One agency has used orientation groups to screen andengage clients.
Intervention Target Points
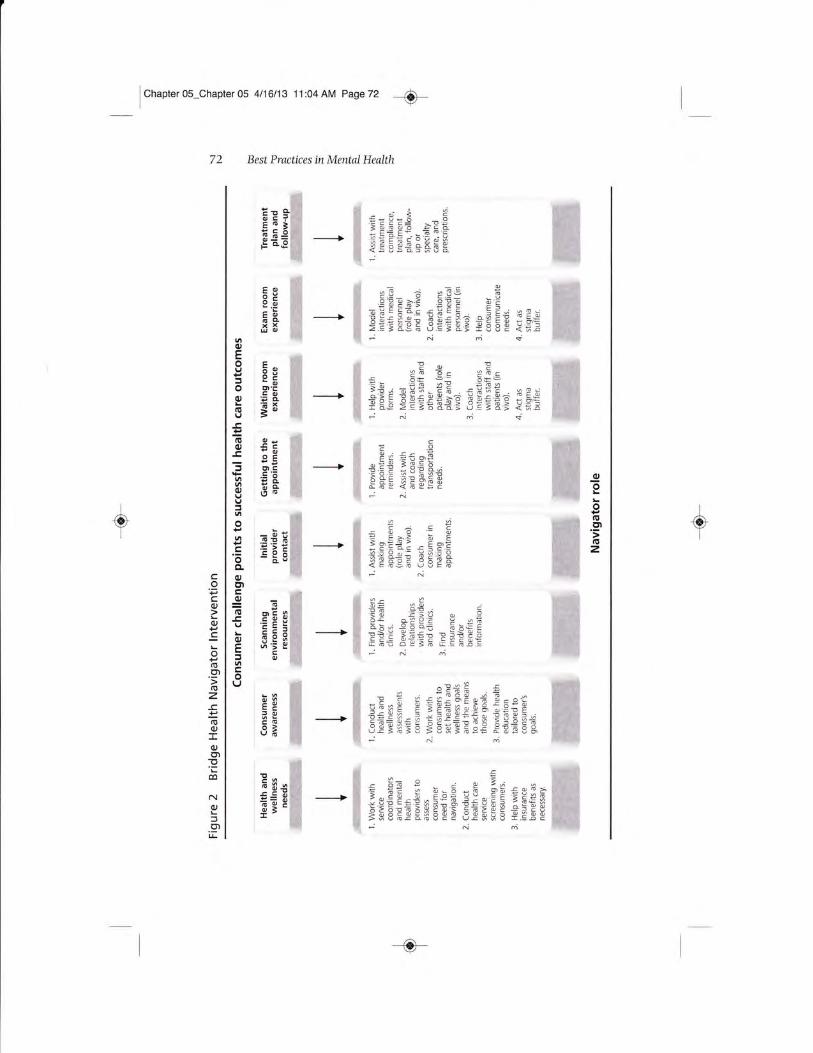
In practice, there are eight challenge points, identilied as critical junctures byprior research and focus groups, at which peer navigators may intervene to facilitate successful health care utilization. Figure 2 presents these points for interven-tion as well as the navigator role at each point. As can be seen, they range from
:,j::, ^**""ess of health care needs, through resource location, to follow-up
Intervention Timeline
The Bridge is implemented in two phases. Phase one is characterized by fre,quent in-person contact between the peer health navigator and the client. This isan intensive lbur-month phase du-ring which the navigator engages and helps theclient complete an initial assessment, collaborates with the client to develop healthand wellness goals and create a navigation plan, works with the client toward
-o-
ICn"Ot"ros-Chapter05 4/16/13 11:O4AM Page72 e
ffi
ffiffi
ffi
ffi
ffi
ffi
ffi
ffi
E- a i 2
S E;;;* =EEEt t E= E+ -E o =*
ffi iEEEc+Br[E;
EttotrE63E.Lq
#rE?ieE€f;ffi EEEb= EEE FE
- ffi sE;ag;sE€aessEt;F*
Eo6Pe.EtsoEA,r6
tr
89EOEOg5
f5OE9.S.=oPOgF
;cgic=
ffi En E!sE---------> ffi oEt 53=9 .
ff E+E ritsEE
#a6=-E E =
*c : c 7
Ea'ffi*H;.acgisEeE
#t; .*€o . E*El o< o,P- u 6H
-------* m =-; =
9Er"; =
S+EE:gi EE! oP36 [=E;.9
NM
o
PE EeE=r!9;.;'; E
Eo
* .- 9oo? <* p 2.=IE$E.*t-"-=
--* E
s,€E=E!Ei€;E*ff+Ea
dEffi = 3= e - i E E, - e
-------- ffi i sEE*! * 5:'- :;
' ;s E Er g
ffi SEEEESftEEE SEEsE fEEE
Best Practices in Mental Health
*ffi
Effi+Hg:*!
ffiA#gBffi*tHffiffi
ffiWD
ffi
#ffiffi
ffi
ffi EE =e. -. n5.ffi5 6E s
--* m Er* eEE,i;e sEite i$*-
ffi =*E
9EE€E ri +
geoIE
.9Gz
ffi
ffi
Effi
ffi
!
P=76!,flt
9B:oa6.qB
72
<i

] Cn"Ot", Os-Chapter 05 4116113 11:04 AM Page 73 -e-
+
Reducing Health Disparities for People with Serious Mentallllness 73
achieving the goals, helps the client navigate through the health care system, andprovides active health education and skill building to shape and reinforce positivebehavior and move the client toward more independence. An in vivo navigationapproach is preferred for modeiing and coaching, although this depends on clientpreference and skill. This means that navigators routinely accompany clients ondoctor, pharmacy, and lab visits in order to build their competence and indepen-dence, and to help with the tralsition to self-management.
Phase two is a two-month step-down phase in which clients' health activitiesbecome increasingly more independent. In phase fwo, the health navigator con-nects with the client via phone or in person once a week or as needed to check onhis or her progresst help troubleshoot emerging health-care-related issues; andprovide support for the client to facilitate progress toward established goals, revisegoals, or set new goals. The length of phase two depends on the needs of the ciientas some clients require step-down support for longer than others.
Although a timetable has been offered for the intervention, it is a general guide-Iine aad subject to variation based on the intensity of client need. The authorshave found that individualization of both phases is critical, as clients progress atdifferent rates in Iearning the skills flor autonomous health navigation and self-management.
Outcomes
Outcomes targeted by the Bridge intervention have been classified as proximalor distal. Proximal health outcomes include increased use of ambulatory and out-patient care, decreased usage of emergency room and urgent care health services,improved health stafus, increased health care self-efficacy, greater satisfactionwith health care, and higher health-related quality of life. Distal outcomes includebetter general life satisfaction, improved functional outcomes, and higher self-esteem.
Feasibility Test of the Bridge
Clinic Sites
The Bridge peer health navigator intervention was implemented at two outpa-tient mental health clinics in Los Angeles. Both sites are part of a large contractprovider called Pacific Clinics that serves 3,500 clients annually and has largenumbers of clients in need of assistance with coordinating health care services.The sites were selected because of their willingness and capacity to participate inimplementing this pilot intervention. The clients were enrolled in full-service part-nerships that targeted the most functionally impaired and highest users of mentalhealth services, those with histories of homelessness, or those most in need ofengagement in intensive mental health services. The intervention featured lowcaseloads (20:1) and was based on an Assertive Community Treatment approach(Gilmea Stefancic, Manning, Ettner, & lbemberis, 2010).
-o-

Chapter os-Chapter 05 4/16^3 11:04 AM Page74 -<D-
++
74 Best Practices in Mental Health
Peer Navigator Qualifi cations
Because the peer navigator is a crucial component of this intervention, mem-bers of the research team and service providers reviewed the qualificationsrequired to be a successful navigator. Several local agencies offer a comprehensivepeer mental health worker training program that combines ten weeks of class-room instruction with six weeks of intensive internship at a mental health agency.It was agreed that peer health navigators should participate in an oflicial trainingprogram to learn the skills nsssttaly for working in a mental health clinic setting.Other mutually approved qualifications for a peer navigator were good communi-cation skills. flexibililv, ability to work well in a variety of settings, capacity todevelop rapport with peers, and comfort in communicating with mental healthand medical professionals.
Navigator Training
Peer health navigator training was initially conducted at one of the participat-ing sites. The navigator was placed at the site and worked with different teams. Hespent two months shadowing clinic nurses, team leaders, and service providers toget a sense of the operation, workllow and ethos of the clinic. After this two-month period. the navigator began working with clients to pilot test the assess-
ment tools and began testing the navigator model. During this time, he received in-depth training with the research team about the health navigator model and thetheory supporting it, background on understanding the scope of the problem, set-ting boundaries, avoiding dual relationships, setting up a supervision plan. deal-ing with stress on the job, and becoming integrated into the staff culture of theclinic.
Manual Development
Using intbrmation gathered from the needs assessment combined with thestage model of manual deveiopment (Carroll & Nuro, 2002), the authors havemanualized the Bridge intervention. The stage model proposes three differentstages for manual development (Carroll & Nuro, 2002; Carroll & Rounsaville,2008). The advantage of this model is that it leads to a manual that is well testedin a variety of settings and with different populations. A drawback is the length oftime needed to move from bench to clinic. which contributes to a disconnectbetween research and practice that needs to be addressed (Dobson & Hamilton,2002; Moras, 2002). Thus, the authors used a modified version of the stagemodel, which emphasizes working closely and continuously with practitioners toensure that the manual is applicable to the real world and to allow it to be dissem-inated more quickly (Moras, 2002). lb do this, a manual development workinggroup was created, including members of the research team, clinic staff, and thehealth navigator. This working group method allowed the authors to receive con-tinuous feedback on the manual contents, and resu-lted in ongoing relinement andimproved utility in a real-world setting.
e

I Cnanter 0s-Chapter 05 411611g 11:04 AM Page 75 -O
Reducing Health Disparities for People with Serious Mental lllness 7 5
The manual includes detailed instructions, scripts, and forms for screening,engagement, assessment, goal setting, planning for medical visits (physician, lab,or pharmacy), post-visit review and monitoring progress. It also explicates the/ortlrcm, with them, fu1 thenr training method and offers client education material.
Fidelity and Monitoring
The authors have developed protocols for establishing and maintaining fidelityto the Bridge, as well as strategies for monitoring the extent of implementation atan agency. The fidelity tool consists of rating the navigator's competence inaccomplishing the critical elements of the intervention. This evaluation is basedon in vivo observation, verbal case descriptions, and record review. The extent ofimplementation is monitored via a software program that requires the navigatorto list both client contacts and contacts on behalf of the client, as well as the loca-tion, length, and topic of each contact.
Results fiom Pilot Data
Preliminary data on the feasibility, outcomes, and implementation of the Bridgehave been obtained from seven clients who received the intervention during thisearly developmental phase. Concerning outcomes, data have been received fromfour clients who completed baseline and foilow-up assessments after six months ofthe intervention. These four clients showed positive changes in the total number ofcurrent health problems (baseli-ne ll = 6.5, SD = 0.7; follow-up M= 4.O, SD = 0.8;Mann-Whitney z = -2,4, p < .03) and an increase in the number of health screen-ings in the previous six months (baseline M = 1.75, SD = 1.00, follow-upM= 4.25, SD = 1.9; Mann-Whitney z= 2.7, p < .06). The number of medical hos-pital admissions began low and stayed low. as did the number of emergency roomvisits for physical problems. There was a decline in the number of outpatient visitsto primary care providers in the previous six months (baseline &I = 6.5, SD = 4.6:follow-up M = 3.3, SD = 3.4) that r,r,as not statistically significant. According to thenavigator, this reduction r,ras due to better follow-up care procedures that reducedvisits for the same health problems over time. Based on these highly preliminarydata, there is some suggestion that the intervention could be related to improvedhealth status and more appropriate use of outpatient services.
Pilot data on the quantity of client contacts were also analyzed. Of the sevenfully engaged clients, the average contacts made with or on their behalf were 2.3per week, with a range of 1.4 to 2.8 contacts per week. Eighty percent of the con-tacts were with the ciient, and 20 percent were with another person on behalf ofthe client, These contacts spread somewhat evenly between in-person (60%) andphone contacts (40%). Based on field notes kept by the navigator, the duration ofthe contacts ranged from under five minutes to over four hours. The navigatorreported that he moved to the step-down phase with all ciients, during whichthe contacts decreased by over 75 percent as clients transitioned to more self-management of their health care.
-tictI

cI
Chapter Os-Chapter OS 4t16113 11:04 AM Page 76 -e-
76 Best Practices in Mental Health
The range of health-related issues among pilot clients was enormous. Six ofseven clients had not had any routine care from a primary care physician in sev-eral years. Most identified their psychiatrist as their primary medical care doctor.Only one individual had had an eye exam in the previous five years. Oniy oneclient had a regular dentist. One individual had ongoing foot lesions that resultedin repeated hospitalizations due to inadequate treatment follow-up. Most clientsused the hospital as their routine health care provider. The navigator securedhealth benefits for one undocumented Latino and accompanied most clients ondoctor visits. During these visits issues ranged from communication problemswith nurses and doctors to difficulties handing the waiting room and exam roomexperiences. There were also frequent problems with treatment compliance thatresulted in ongoing and increasingly serious health problems and overuse ofemergency services. One individual was too anxious to take public transportationto the medical clinic, so the navigator first accompanied her and sat next to her onthe bus; on subsequent trips he sat several seats behind her, and then he drovebehind the bus as she rode alone, all to encourage independence through reducednavigator presence.
Best Practice for Work with Persons with Severe Mental Illness
There were many navigator contacts to ensure follow-up care and treatmentcompliance. Pharmacy interactions and managing multiple medications werefound to be common difficu,lties for clients. Pharmacy personnel were pleased towork with the navigator as they reported challenges in working with individualswith serious mental illness. Health care physicians and nurses were generally wel-coming to the navigator and most often allowed him into the examining room.Once they had worked r,t ith the navigator, physicians actively engaged his servicesand felt he improved the effectiveness of the medical .rdsit.
Because the work can be stressful, supervision and support of the peer naviga-tor is a crucial aspect of this intervention. To address this, the peer health naviga-tor met weekly, or as needed, with the project manager to debrief, talk about whatwas working and not working, and discuss any troubling situations. The healthnavigator also participated in weekly team meetings to discuss navigation-relatedissues with the project team.
Agency Integration
The authors have found that rvorking closely with mental health agency staffis critical to adequately integrating peer health navigation into the agency clinicalmodel. For example, staff suggested that the peer health navigator be included inteam meetings, and that goals and treatment plans be shared (considering com-pliance issues) so that coordination and integration could be achieved. Otherforms of inclusion and communication have developed over time that facilitate theintegration of health navigator services. lf mental health agencies have not previ-ously integrated peers into their approach, professional staff are required to takeon additional work.

ChapterOs-Chapter 05 4116113 11:04AM Page77 -S-
Reilucing Health Disparities for People with Serious Mental Illness 7 7
Next Steps
The purpose o[ this article was to describe the development, implementation,and feasibility of a peer health navigator intervention called the Bridge. Theauthors developed the Bridge peer health navigator intervention for many rea-sons. Several service models have been advocated for dealing with the physicalhealth of those with serious mental illnesses, yet models of care that integrate carethrough co-situation of services require multiple structural and financial changesto the existing health ca-re system. A care linkage model, such as the Bridge,improves collaboration between independent health and mental health providers,and can be used in the context of many existing financing and service structurearrangements. The use of peer health navigators is an emerging best practice foraddressing health needs of people living with serious mental illness. There is accu-mulating evidence that peer-based services can improve outcomes in health andin other aspects of recovery among people living with serious mental illness, andare also cost effective (Rosenick & Rosenheck, 2008).
The results from the feasibility work reported here are encouraging. Theauthors are currently analyzing data from a small randomized trial (n = 24) ofthe Bridge intervention, and are refining the treatment manual. They are alsoworking on an agency implementation and sustainability protocol, which will bemanualized to deal with both administrative and intervention integration issuesat the staff level, and they have developed protocols for training new peer healthnavigators. Nonpeer paraprofessionals and professionals have recently beentrained in the Bridge intervention, but the use of professionals has proven difficuitdue to cost considerations. Finally, the Bridge intervention was developed using apopulation with serious mental illness that was very functionally impaired andliving in an urban area. As the effectiveness of this intervention is investigatedfurther, it will be important to consider the degree to which the intensity of theintervention and its in vivo approach are required for other less chailenged popu-lations and settings.
References
Anderson, G., & Knickman, J. R. (2001). Changing the chronic care system tomeet people's needs. Health Affairs, 20(6),146-160.
Battaglia,'I'. A., Roloff, K., Posner, M. A., & Freund, K. M. (2OO7),Improvingfollow-up to abnormai breast cancer screening in an urban population:A patient navigation intervention, Cancer 709(Slpp1. 2), 359-367.
Bazelon Center for Mental Health Law. (2004). Get it together: How to integratephysical andmentalhealth care Jor people with serious mental disorders.
Washington, DC: Author. Refrieved from http://www.bazelon.org/News-Publications/Publications/.
Berren, M. R., Santiago,l.M.,Zent, M. R., & Carbone, C. P. (1999). Health careutilization by persons with severe and persistent mental illness. Psychi-
atric Services, 5 0(4), 5 59-5 61.
o-

Chapter 0s-Chapter 05 4t16113 11:04 AM Page 78 e
78 Best Practices in Mental Health
Bradford, J. B., Coleman, S., & Cunningham, W. (2OO7). HIV system navigation:An emerging model to improve HfV care access. AIDS patient care and
SIDs, 21(Suppl. I), S49-S58.Brown, V (1998). Untreated physical health problems among women diagnosed
with serious mental illness. /ournal ol the American MedicalWomen's Asso-
ciation, 5 i(4), 159-160.Brunero, S., & Lamont, S. (2010). Health behaviour beliefs and physical health
risk factors for cardiovascuiar disease in an outpatient sample of con-sumers with a severe mental illness: A cross-sectional survey. lnterna-
tional JotLrnal of Nursing. 47(6), 7 53-7 60.
Carney, C. P., Allen, J., & DoebbelinC, B.N, (2OO2). Receipt of clinical preventive
medical services among psychiatric patients. Psychiatric Services. 53(8),1028-1030.
Carroll, K. M., & Nuro, K. F. (2002). One size cannot Iit all: A stage model forpsychotherapy manual development. Clinic al P sy cholo gy : S cienc e and
P ractic e, 9 (4), 39 640 6.
Carroll, K. M., & Rounsaville, B.l. (2008). Efficacy and effectiveness in develop-ing treatment manuals. In A. M. Nezu & C. M. Nezu (Eds.), Evidence-based
outcomes research: A practicoJ guide to conducting randomized controlled trials
lor psychosocial irterventions (pp. 279-243). New York: Oxford UniversityPress.
Cohen, J. W, & Krauss, N. A. (2003). Spending and service use among people
with the Iifteen most costly medical conditions. Health Aflairs, 22(2),129-13U.
Compton, M. T., Daumit, G. L,, & Druss, B. G. (2006). Cigarette smoking and
overweight/obesity among individuals with serious mental illnesses:
A preventive perspective. Harvard Review of Psychiatry, 14(4),212-222.Cook, |. A. (2005). "Patient-centered" and "consumer-djrected" mentalhealth services.
Report repared for the Institute of Me&cine, Committee on Crossing the
Quality Chasm-Adaptation to Mental Health and Addictive Disorders.
University of Illinois at Chicago.
Dalmau, A., Bergman, B., & Brismar, B. (1997). Somatic morbidity in schizo-phrenia-A case control study. Pubiic Health, 117(6),393-397.
Darnell, I. S. (2007). Patient navigation: A call to action. Social Work, 52(L),8 1-84.
Davidson. L., Chinman, M., Kloos, B., Weingarten, R., Stayner, D., & lbbes, J. K.(7999), Peer support among individuals r,tith severe mental illness:
A review of the evidence. ClinicalPsychology: Science and Practice, 6(2),165-187.
Davidson, L., Chinman, M., Sells, D., & Rowe, M. (2006). Peer support among
adults with serious menta-l illness: A report from the field. Schizophrenia
tsulletin, 3 2(3), 443450.
cI

+
Chapter Os-Chapter 05 4l16t1g 11 :04 AM Page 79 -e-
Reducing Health Disparities for People with Serious Mentallllness 79
Deakin, B., Ferrier, N., Holt, R. I. G., Millar, H., Nutt, D., Reynolds, G., . . . Taylor, D,(2010). The physical health cha-Ienges in patients with severe mental ill-ness: Cardiovascular and metabol-ic isks. lournal oJ P sychopharmacology,24(Suppl. l), i-8.
De Hert, M., Correll, C. U., Bobes, 1., Cetkovich-Bakmas, M., Cohen, D., Asai, 1., . . .
Leucht, S. (2011). Physical iliness in patients with severe mental disor-ders. I. Prevalence, impact of medications and disparities in health care.World Psychiatry, 10(l), 52-7 7.
Desai, M. M., Rosenheck, R. A., Druss, B. G., & Perlin, J. B. (2002). Mental disor-ders and quality of diabetes care in the veterans health administration.Amer ic an I ournal of P sy chiatr A, 1 5 9 (9\, 1 5 8 4-1 5 9 0.
Dickerson, F. B., Brown, C. H., Daumit, G. L., Ujuan. F., Goldberg, R. W,Wohlheiter, K., & Dixon, L. B. (2006). Health status of individuals withserious mental illness. Schbop hrenia tsulletin, 3 2(3), 5 84-5 8 9.
Dickerson, F. B., Brown, C. H., Fang, L., Goldberg. R. W, Kreyenbuhl, J.,Wohlheiter, K., & Dixon, L. B. (2008). Quality of life in individuals withserious mental illness and type 2 diabetes. Psychosomatics, 49(2),109-1 14.
Dickerson, E B., Goldberg, R. W., Brown, C. H., Kreyenbuhl, I., Wohiheiter, K.,Fang, L., . . . Dixon, L. B. (2005). Diabetes knowledge among personswith serious mental illness and type 2 diabetes. Psychosomatics, 46(5),418-424.
Dickerson, F. B., McNary, S. W., Brown, C. H., Kreyenbuhl, J., Goldberg. R. W, &Dixon, L. B. (2003). Somatic healthcare utilization among adults withserious mental illness who are receMng community psychialric services.Medical Care, 47(4), 5 60-57 O.
Dickey, B., Normand, S. T., Weiss, R. D,, Drake, R. E., & Azeni, H. (2002). Medicaimorbidity, mental illness, and substance use disorders. Medicallllness andSevere Mental lllness, 5 3(7), 8 67-867 .
Dobson, K. S., & Hamilton, K, E. (2002). The stage model for psychotherapymanual development: A valuable tool for promoting evidence-basedpractice. Clinical P sy cholo gy : S cienc e and P ractic e, 9 (4), 4O7 4O9 .
Dohan, D., & Schrag, D. (2005). Using navigators to improve care of underservedpatients. Cancer, 704(4), 84ll-U5 5.
Druss, B., & Newcomer, I. QOOT). Challenges and solutions to integrating mentaland physical health care. lournal of ClinicalPspychiatry, 68(4), eO9.
Druss, B. G., Rask, K., & Katon, W I. (2008). Major depression, depression treat-ment and quality of primary medical care. General Hospital Psychiatry,30(r),20-25.
Druss, B. G., Rosenheck, R. A., Desai, M. M., & Perlin, l. B. (2002). Quality ofpreventive medical care for patients with mental disorders. Medical Care,
40(2),1,29-736.

I
cn"ot"r Os-Chaprer 05 4l16t1g l 1:04 AM Page 80 e
8O Best Practices in MentalHealth
Druss, B. G., von Esenwein, S. A., Compton, M. T., Rask, K. 1., Zhao, L., & Parker,
R. M. (2010). A randomized trial of medical care management for com-munity mental health settings: The primary ca.re access, referra-I, andevaluation (PCARI) study. Arn erica n I ournal ol P sy chiatry, 1 6 7 (2),
1 5 1-1 59.Druss, B. G., Zhao, L., von Esenwein, S,, Bona, J. R., Fricks, L., Jenkins-Tucker, S.,
. . . Lorig, K. (2010). The Health and Recovery Peer (HARP) Program:A peerJed intervention to improve medical self-management for personswith serious mental illness. Schizophrenia Research, 1 1 8( 1-3), 264-27 O.
Gelberg, L., Andersen, R. M., & leake, B. D. (2000). The behavioral model forvulnerable populations: Application to medical care use and outcomes forhomeless people. Health Services Research, 34(6), 127 3-7302.
Gianfrancesco, F. D., Grogg, A. L., Mahmoud, R. A., Wang, R., & Nasrallah, H. A.(2OO2). Differentia] effects of risperidone, oianzapine, clozapine, and con-ventional antipsychotic on type 2 diabetes: Findings from a large healthplan datab ase . I our nd of Clinic al P sy chiatr 11, 6 3( 1 0), 9 2O-9 30.
Gilmer, T., Stefancic, A., Manning, W., Ettner, S., & Tsemberis, S. (2010). Effect offull-service partnerships on homelessness, use and costs of mental healthservices, and quality of life among adults with serious mental illness.Ar chive s of G eneral P sy chiatrpl, 6 7 (6), 6 4 5 -6 5 2.
Goldberg, R. I. (1999). Financial incentives influencing the integration of mentalhealth care and primary care. Psychiatric Services, 50, lOTl-1O75.
Goldberg, R. W., Dickerson, F., Lucksted, A., Brown, C. H., Weber, E., Tenhula,W N., . . . Dixon, L. B. (2013). Living well: An intervention to improveself-management of medical illness for individuals with serious mentalillness. Psychiatric Services, 64(1), 5l-57.
Goldberg, R. W., Kreyenbuhl, J. A., Medoff, D. R., Dickerson, F. B., Wohlheiter, K.,Fang, L. J., . . . Dixon, L.B. (2OO7). Quality of diabetes care among adultswith serious mental illness. Psychiatric Services,58(4), 536-543.
Goldman, C. R., & Quinn, F. (1988). Effects of a patient education program inthe treatment of schizophrenia. Hospital Community Psychiatry, j9(3),282-286.
Hedberg, I., & Skdrsiiter, I. (2009). The importance of health for persons withpsychiatric disabilities. Journal ol Psychiatric and Mental Health Nursing,16(5),45s467.
Hippisley-Cox, J., Vinogradova, Y., Coupland, C., & Parker, C. (2OO7). Risk ofmaiignancy in patients with schizophrenia or bipolar disorder: Nested
case-control study. Archives of G ene ral P sy chiatr y, 6 4(12), 1 3 6 8-l 3 7 6.
Jandorl L., Fatone, A., Borker, P. V., Levin, M., Esmond, W., Brenner, B., . . .
Redd, W. H. (2006). Creating alliances to improve cancer preventionand detection among urban medically underserved minority groups.
Cancen 707(Snppl. 8), 2043-2051.feste, D. V, Gladsjo, J. A., Lindamer, L. A., & Lacro, J. P (1996). Medical comor-
bidity in schizophrenia. Schizophrenia Bulletin, 22(3), 4L343O.
-o

] Cnaoter os*Chapter 05 4t16t1s 11:04 AM Page 81 -A-
+
Reducing Health Disparities for People with Serious Mental Illness 81
Kane, |. M. (2009). Creating a health care team to manage chronic medical ill-nesses in patients with severe mental illness: The public policy perspec-
tiv e. l our nal of Clinc al P sy chiatry, T0( Suppl. 3), 3 7 42.Ifteyenbuhl, I. A. (1999). Coruelates of psychopharmacologic treatment outcomes for
schizophrenia (Doctoral dissertation). Retrieved from http://hdl,handle.net/lO713/1240.
Laws, K., Gabriel, R., & McFarland, B. (2002). Integration and its discontents:Substance abuse treatment in the Oregon health pla* Health Affairs,21(4),284-289.
Leigh, H., Stewart, D., & Mallios, R. (2006). Mental health and psychiatry train-ing in primary care residency programs. II. What skills and diagnoses aretaught, how adequate, and what affects training directors' satisfaction?General Hospital Psychiatry, 2 ll(3), 19 5-204.
Lester, H. E., Tritter, J. Q., & Sorohan, H. (2005). Providing primary care forpeople with serious mental illness: Focus group study. British Medical
I ournal, 3 3 0(7 5 0O), 7122-7728.Lieberman, A. A., & Coburn, A. F-. (1986). The health of the chronically men-
tally ill: A review of the literature. Community MentalHealthlournal,22(2), 104-176.
Link, B. G. (1987). Understanding labeling effects in the area of mental disor-ders: An assessment of the effects of rejection. American SociologicalReview, 52,96-112.
Link, B. G., & Phelan, I. C. (2001). Conceptualizing stigma. AnnualReview ofSociology, 27 , 363-385.
Maj, M. (2OO9). Physical health care in persons with severe mental illness:A public health and ethical priority. World PsplchiatrA, 8(l),1-2.
Miller, C. L., Druss, B. G., Dombrowski, E. A., & Rosenheck, R. A. (2003). Barriersto primary medical care among patients at a community mental healthcenter. Psychia tric Services, 54(8 ), 1 1 5 8-1 1 60.
Moras, K. (2002). A tool to advance the effectiveness and dissemination ofempirically supported psychotherapies and the NIMH public healthresearch agenda. Clinic al P sg cholo gy : S cienc e and P ractic e, 9 (4), 4 2 5 4 3 O.
Mueser, K. 1'., Meyer, P. S., Penn, D. L,, Clancy, R., Clancy, D. M., & Salyers, M. P.
(2006). The illness management and recovery program: Rationale, devel-opment, and preliminary findings. Schizophrenia Bulletin, 32(Suppl. 1 ),s32-S43.
New Freedom Commission on Mental Heaith. (2003). Achieving the promise:
Transforming mental health care in America. Final report (DHHS Pub. No.SMA-03-3 8 32). Rockville, MD; Author.
Parks, 1., Svendsen, D., Singer, P, & Foti, M. E. (2006). Morbidity andmortality inpeople with serious mental i.llness. Alexandria, VA: National Association ofState Mental Health Program Directors (NASMHPD) Medical DirectorsCouncil. Accessed at http://www.nasmhpd.org/docs/publications/MDCdocs/ MortalityandMorbidityFinalReport0 8. 1 t3.0 8 .pdf.
e

j Cnapter os-Chapter 05 4/16/13 1 l:04 AM Page 82 -O-I'
82 Best Practices in Mental Health
Prohaska, T. R., & Lorig, K. (2000). The role of theory in patient education. InK. Lorig (Ed.), Patient education: A practical approach (3rd ed.). ThousandOaks, CA: Sage,
Rosenick, S, G., & Rosenheck, R. A. (2008). Integrating peer-provided services:
A quasi-experimental study of recovery orientation, confidence, andempowerment. P sg chiatric Seruices, 5 9( 1 1 ), 1 3 O 7-1 3 1 4.
Schefl T. (1994). Being mentallg ill: A sociological theory (3rd ed.). Chicago:Aldine.
Shattell, M. M., Donnelly, N., Scheyett, A., & Cuddeback, G. S. (2011). Assertivecommunity treatment and the physical health needs of persons withsevere mental illness: Issues around integration of mental health andphysical health. lournal of American P sgchiatric Nurses Association, 7 7 (L),
57-63.Solomon, P. (2004). Peer support/peer provided services underlying processes,
benefits, and critical ingredients. Psgchiatric Rehabilitationlournal, 27(4),39240t.
Stein, L. I., & Test, M. A. (1980). An alternative to mental health treatment. I.Conceptual model, treatment program, and clinical evaluation. Archives
ol General P sychiatry, i 7 (4), 39 2-39 7 .
Steinberg, M. L., Fremont, A., Khan, D. C,, Huang, D., Knapp, H., Karaman, D., . . ,
Streeter, O, E. (2006). Lay patient navigator program implementation forequal access to cancer care and clinical trials. Cancen 107(Ll),2669-2677.
Stroul, B. A., Pires, S. A., & Armstrong, M. (2001). Healthcare Reform Tracking
Project: Tracking state managed care relorms as theg ffict children and adoles-
cents with behavioral health disorders and their families: 2000 State Survey.
Research and Training Center for Children's Mental Health, Departmentof Child and Family Studies, louis de Ia Parte Florida Mental Health Institute, University of South Florida.
Test, M. A., Knoedler, W H., Allness, D. J., Burke, S. S,, Brown, R. L., & Wallisch,L. S. (1991), Long-term community care through an assertive continu-ous treatment team. In C, A. Tamminga and S. C. Schulz (Eds.), Advancas
inneuropsgchiatrg anilpsychopharmacology: Schizophreniaresearch (Vol. 1,pp. 239 -246). New York: Raven Press.
Vogel, C. (2001). Mentalhealth"boundaries" inMedicaid managedcare. Princeton,Nl: Mathematics Policy Research, Inc.