reflections on - cmccglearninghub.org.uk · presentation 25-year-old right-handed female. 6/12...
TRANSCRIPT

Reflections on neurology.
Janet Suckley, January 2016
Presentation
25-year-old right-handed female.
6/12 history of right hand little finger ‘sticking out’(Wartenberg’s sign).
No other MSK/neurological symptoms.
Otherwise well and taking no regular medication.
PMH, FH, DH & SH all unremarkable.

Investigations
Nerve conduction studies – normal right ulnar nerve at wrist and elbow, no localized nerve pathology.
USS right little finger – normal findings.
MR right wrist & hand – normal findings.
Why MR and USS of the hand?
Rupture of the deep transverse metacarpal ligament between the ring and little fingers can present with ulnar deviation of the little finger with extension (Wheatley et al.,1998).
Inability to adduct or flex the finger at the metacarpophalangeal joint: consider rupture of the radial sagittal band, collateral ligament, and junctura tendinum (Lourie et al., 1999).
Examination
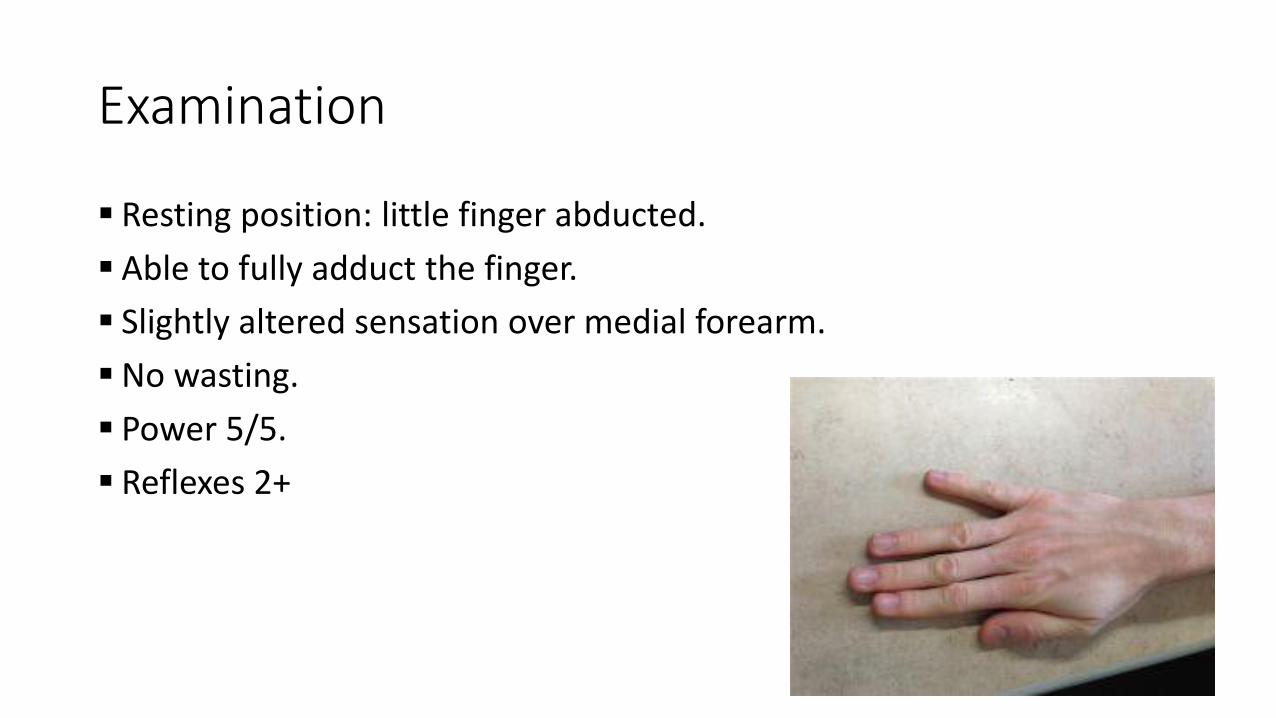
Resting position: little finger abducted.
Able to fully adduct the finger.
Slightly altered sensation over medial forearm.
No wasting.
Power 5/5.
Reflexes 2+

Plan
MR cervical spine (and thoracic outlet).
Neurology input.

Neurologist’s advice
Add MR brain - contralateral parietal brain lesion (rare).
Consider other rarities, such as palmaris brevis spasm syndrome.
If nil found, refer to neurology.

Palmaris brevis spasm syndrome (Serratrice et al., 1995)
Involuntary dimpling of the hypothenar eminence.
Rare, benign.
Innervation: superficial branch of the ulnar nerve.
Not under voluntary control.
Related to entrapment neuropathies of the ulnar nerve and C8 radiculopathies, but exact mechanism unclear.
Botulinum toxin is the treatment of choice.
Anderson et al. (2005)
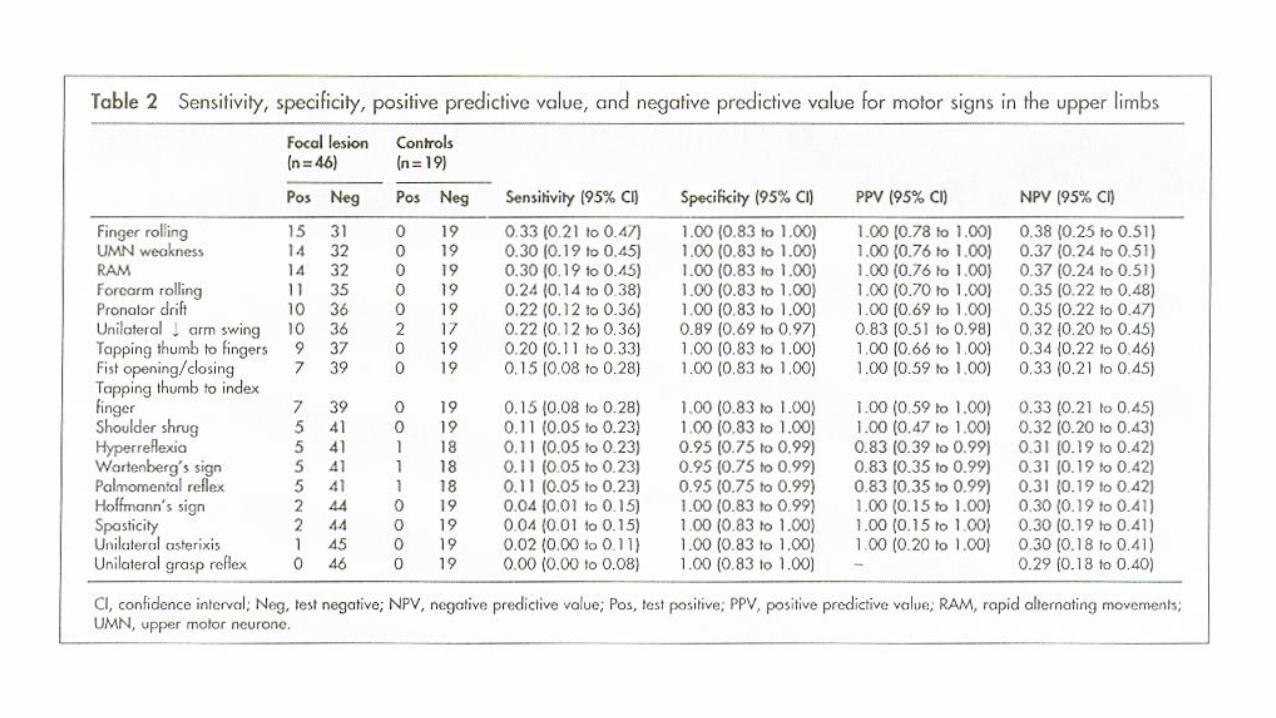
Objective: to determine the sensitivity and specificity of clinical tests for detecting focal lesions in the brain – a prospective blinded study.
Methods: 46 patients with a focal cerebral hemisphere lesion without obvious focal signs and 19 controls with normal imaging were examined using a battery of clinical tests.
Conclusion: The neurological examination has a low sensitivity for detecting early cerebral hemisphere lesions in patients without obvious focal signs.

The upper limb test findings with the greatest sensitivities for detecting a focal lesion were abnormal finger and forearm rolling (click here), UMN weakness (click here ), impaired rapid alternating movements or dysdiadochokinesis (click here) and pronator drift (click here). All these tests had a specificity of 1.0
Wartenberg’s sign was present bilaterally in 17% of the focal lesion group and 11% of the controls.

Kilgus et al.(2003)
5 cases of permanent little finger abduction. Clinical, imaging and electrodiagnositc tests revealed different pathologies:
Ulnar nerve lesion.
Hyperactivity of abductor digiti minimi (palmaris brevis syndrome).
Syringomyelia.
Ligament injury.
Local muscle damage secondary to wearing a tight cast.
Reflection Ulnar nerve lesions

Questions to be considered in a patient with a suspected ulnar neuropathy (Stewart, 2006):
Is it really an ulnar neuropathy?
Where is it: elbow or wrist?
If not an ulnar neuropathy, what is it: C8 or T1 radiculopathy, plexus lesion, spinal cord lesion, anterior horn cell lesion, other?

Motor examination Ulnar nerve lesions
Stewart (2006) Look for wasting and claw hand.
Examination of the several ulnar-innervated intrinsic hand muscles can be restricted to just two: the 1st dorsal interosseous and abductor digiti minimi. And in the forearm, the two ulnar-innervated muscles: flexor carpi ulnaris and flexor digitorum profundus of the 4th & 5th digits.
The main differential diagnoses are C8 radiculopathy (T1 radiculopathy is very rare) and brachial plexopathies - which cause weakness of the median-innervated muscles, so be sure to test the abductor pollicis brevis (the main muscle involved in carpal tunnel syndrome) and the median-innervated long flexors of the thumb and index finger.

Stoker et al. (2014)
The ulnar nerve innervates all intrinsic hand muscles except the abductor pollicis brevis, flexor pollicis brevis, opponens pollicis, and lateral two lumbricals, which are innervated by C8 and T1 via the median nerve. By examining these five muscles, one can clinically differentiate cubital tunnel syndrome from C8–T1 radiculopathies.

Median nerve muscles (all thumb muscles except adductor pollicis):
Lateral two lumbricals
Opponens pollicis
Abductor pollicis brevis
Flexor pollicis brevis
Ulnar nerve muscles:
Abductor pollicis
Lumbricals (flex MCP and extend IP joints)
Palmar interossei (adduct fingers: Pad)
Dorsal interossei (abduct fingers: Dab)

Sensory abnormalities that extend more than about 2cm above the wrist crease indicate involvement of the brachial plexus or C8 & T1 nerve roots.
Use and abuse of physical signs in neurology (O’Brien, 2014)
‘The history is overwhelmingly the most important part of a neurological assessment’.
‘The main use of neurological signs is in the more precise localisation of a lesion already indicated by the history and to answer the classical questions: can this all be due to a single focal lesion? Must it be due to multiple lesions? Or is it a system disease? Rarely is a single sign by itself diagnostic of a particular disease, though a cluster of signs may be almost diagnostic’.
‘Choose signs that clearly and reliably identify pathology, such as the plantar response, or are key to the localisation of the lesion such as an absent reflex. These are hard signs … there should be a strong bias to the use of hard signs’.

‘An extensor plantar response is a hard sign for pathology somewhere in the UMN pathway but a very soft sign for localisation: it is even rather a poor sign for lateralisation, unless it is known whether the lesion is above or below the foramen magnum’.
‘A Horner’s syndrome is a superb lateralising sign but a poor localising sign’.
‘An absent reflex is hard on all criteria, though often irrelevant’.

‘Some signs are useful if present, but useless if absent… weakness of flexor digitorum profundus to the little finger is a good example, and if it is affected in an ulnar nerve lesion, the lesion must be at or above the elbow, but it may be normal in lesions at the elbow’.
The absence of a sign may give useful information in localisation, for example, the absence of a Horner’s syndrome in lower brachial plexus palsy’.

‘In addition to selecting hard signs, there should be a bias towards the use of motor signs because it is common for motor deficit to be relatively under-reported and examination often reveals more signs than might be expected from the patient’s account’.
When examining the motor system… it is of course the movement, not the muscle, which is tested. Ideally, (the test) should ‘help in the differentiation between upper and lower motor neuron lesions; it should have a single root innervation, it should help identify an individual peripheral nerve lesion and preferably the level of the lesion. The principal muscle should be visible so that wasting or fasciculation can be seen… with some preference given to muscle which haven an easily elicitable reflex’. If these criteria are applied, the list of movements to test is actually quite short’. (Table 1)


Problem Differential diagnosis
Weakness Sensory loss Reflex loss
Wrist drop C7 Radial nerve
Triceps, flexor carpi radialis, sternal head pectoralis major Triceps, brachioradialis
Middle finger Snuff box area
Triceps Brachioradialis
Foot drop L5 Common peroneal nerve
Hip abduction, hamstrings, weak eversion, toe drop and foot drop Foot drop, weak eversion, toe drop
Lateral side lower shin, dorsum of foot Lateral side lower shin, dorsum of foot
± ankle ± hamstring None
Harrison (1996)

The NeurAxis (Clark, 2007)
1. Cerebral hemispheres 2. Brainstem 3. Cerebellum 4. Spinal cord 5. Anterior horn cells/cranial nerve nuclei 6. Nerve root 7. Plexus 8. Peripheral nerve 9. Neuromuscular junction 10. Muscle

Structure and function
Dysfunction or damage at any of these levels produces a relatively distinct pattern of signs and symptoms.
- A cervical cord problem will produce weakness of all 4 limbs, but will
spare the face.
- A cerebellar problem will cause ataxia, but no sensory loss.
- An inability to process language: the centre for language is located in
the dominant cerebral hemisphere, which is on the left 95% of the
time (occasionally on the right in left-handed individuals).



References
• Anderson, N. E., et al. (2005). "Detection of focal cerebral hemisphere lesions using the neurological examination." Journal of Neurology, Neurosurgery & Psychiatry 76(4): 545-549.
• Kilgus, M., et al. (2003). "[Wartenberg's Sign of Ulnar Nerve Lesion. A Contribution to Pathophysiology and to the Differential Diagnosis]." Handchir Mikrochir Plast Chir 35(4): 251-258.
• Lourie, G. M., et al. (1999). "Abducted, hyperextended small finger deformity of nonneurologic etiology." J Hand Surg Am 24(2): 315-319.
• O’Brien, M. D. (2014). "Use and abuse of physical signs in neurology." Journal of the Royal Society of Medicine 107(10): 416-421.
• Serratrice, G., et al. (1995). "Palmaris brevis spasm syndrome." Journal of Neurology, Neurosurgery, and Psychiatry 59(2): 182-184.
• Stewart, J. (2006). "Ulnar neuropathies: where, why, and what to do?" Practical Neurology 6(4): 218-229.
• Stoker, G. E., et al. (2014). "Differentiating C8–T1 Radiculopathy from Ulnar Neuropathy: A Survey of 24 Spine Surgeons." Global Spine Journal 4(1): 1-6.
• Wheatley, M. J., et al. (1998). "Closed rupture of the deep transverse metacarpal ligament: diagnosis and management." j Hand Surg Am 23(3): 524-528.