reimagining leadership: a pathway to thrive in a covid-19
TRANSCRIPT

Reimagining Leadership: A Pathway to Thrive in a COVID-19 WorldBenjamin Anderson, MBA, MHCDS Vice President, Rural Health and HospitalsColorado Hospital Association

A story of a little boy named
David.

David loves to learn.

David loves to build.

David lovesto play.

David loves sports.

David loves to be outside.

David loves mud.

David lovesto work.

David works for ice cream.

David wants to be a police officer.

David also wants to be a farmer (like his papa).

David is funny.

David has a soft, humble heart.

David loves his siblings.

David loves his mommy.

David’s favorite story.

The day David met Goliath.

Sr. Mary Jean Ryan, FSMBoard Chair, SSM Health System
1st National Malcom Baldrige Award Healthcare Recipient
“Systems heal people. Systems harm or kill people. Developing good
systems requires good strategy.”



https://jamanetwork.com/journals/jamasurgery/fullarticle/2566219

Are these issues stemming from individual choice, or are they more systemic?

Root Causes of Death Strategy Map
Provider Responses and Individual Accountability
Individual Accountability
Individual and Community Accountability
Health Care Policy
Public Health and Organizational Policy
Community, Economic, Education and Social Policy
Outcomes
Heart, Cancer, Stroke, Pulmonary, Maternal, Diabetes
Actual Causes“Human Behavior”
Tobacco, Obesity, Diet, Inactivity, Alcohol, Motor Vehicle Accidents, etc.
Root Causes“The Human Condition”
Stress, Anger, Poverty, Economics, Education Levels, DepressionUnemployment, Broken Families, Environmental Factors, Loneliness,
Emptiness, Hopeless, Disconnectedness
Adapted from: National Civic League, Healthy Communities Conference 1994, Updated with Best Practices

“Before the pandemic, rural hospitals were struggling for survival. COVID-19 has put a spotlight on the fractures that already existed within rural communities in terms of their healthcare delivery.”
- Brock Slabach, Vice PresidentNational Rural Health Association


“Let’s remember that the suffering we experience as a nation does not fall evenly. In the days to come it will be especially important to care in practical ways for the elderly, the ill and the unemployed.”
– George W. Bush

Tolerating any disparity risks the legitimization of all disparities. This is expensive for all of us.

Addressing disparities requires careful strategy.

Elizabeth Teisberg, Founder, Value Institute for Health and Care
“Strategy requires reverse thinking. Start at your desired outcome and work backward.”

Achieving optimal health for rural Coloradans…

…requires monitoring outcomes…

…of deliberate and tactical interventions…

…fueled by training and partnerships…

…to achieve SMART goals…

…based on careful assessments…

…of reliable information.


CHA MissionSupport members through collaborative commitment to advance the health of their communities through affordable, accessible, high-quality health care
Rural Health VisionValue-driven systems, increased capacity, and innovative payment structures that optimize health and strengthen rural communities
Leverage Data to Inform System Development
and Interventions
Increase Leadership and Workforce Capacity
Improve Access to Excellent and Holistic Care
Strengthen Partnerships and Collaborations
CHA Rural Strategic Plan Summary2020-2022
Governance Capacity• Access to case-based learning• Trustee Recognition and
Accountability ProgramAdministrative Leadership Capacity• Academic partnerships• Two-year Rural leadership fellowship• Certification-based training• Access to case-based learningClinical/Technical Workforce Capacity• Access to rural Baldrige framework
• Develop outmigration and financial dashboards for rural hospitals
• Analyze and report on care migration and community health needs
• Develop baseline capacity dataset for rural organizations and communities
• Partner with academic institutions to conduct community health engagement surveys in four rural Colorado communities
• Introduce annual education program that prepares rural organizations and communities to recruit and retain high-quality primary care providers
• Initiate annual “fly-in” recruitment weekends to recruit clusters of primary care providers
• Develop statewide “air transportation highway” to increase access to specialty care for rural Coloradans
• Design private insurance framework to encourage value-based insurance design
• Collaborate with stakeholders to decrease redundancy and improve value
• Lead annual innovation trips to encourage collaboration and strategic alliances and foster innovation in healthcare delivery transformation

80% Capacity Building20% Policy
(Primary rural strategic focus is capacity building)

“We just don’t have a roadmap for what we’re currently experiencing - that in and of itself can bring up feelings of anxiety, loneliness, and fear. Not to mention the worry we feel about the health and safety of our parents, children, and loved ones and the financial security of so many families.”
– Michelle Obama


Sarahville Health Center
Mountain Plains Family Health Clinic

Rural Health Care Delivery System Assessment Tool

Common COVID-19 Challenges
Nine mini-chapters• Clinical care• Communication• Community• Cross-system collaboration• Space• Spending• Staffing• Statistics and surveillance• Supplies
Structured content
• Continuation of the case study
• Strategic thinking prompts
• Practical guidance• Pearls from your peers• Additional resources

MethodologyRapid review of the literature
oPeer-reviewed (PubMed, Google Scholar, MedRxiv)oGray literature (Google)
Key informant interviewso32 one-hour interviews, including 9 hospital
administrators, 5 governance members, 6 primary care clinicians, 5 rural public health professionals, and 7 patients and community members
Analysis of available resourcesoRural specificity; produced by a reputable organization;
frequently updated; dynamic information; easily navigable; highly applicable + practical advice

Remarkable Rural Innovation
Clinical care
• Expand provider-to-provider tele-health
• Tap into free education• Bring back the home
visit• Move as much care as
possible to patients’ cars
Communication
• Plan crisis communications in advance
• Host Facebook Live press conferences
• Film COVID-19 survivor videos
• Host standing, daily Zoom meetings across all levels

Remarkable Rural Innovation
Community• Give away prizes if
citizens caught caring• Establish a mutual aid
society or a community resource line
• Distribute lists of available public wi-fi
• Ask teachers to run programming to help health care workers
Cross-system Collaboration• Non-traditional Incident
Command (IC) teams focused on innovation
• Hospital infection control/PPE nursing home strike teams
• School/business partner-ships for contact tracing
• Independent providers staff alternate care sites

Remarkable Rural Innovation
Space• PPE donning + doffing
PPE and PVC stations w/ shower curtains and PVC pipe
• Alternate care sites: fairgrounds, community college, hockey rink
• Visiting specialist clinic becomes temporary respiratory clinic
Spending• Apply for everything, even
if you don’t think you qualify
• Devise new sources of revenue, i.e., screening for local businesses
• Engage volunteers or law enforcement to decrease lab courier fees

Remarkable Rural Innovation
Staffing• Redirect chronic care
managers and EMS to do community paramedicine
• Engage medical students to write grants, design alternate care sites, source tele-health platforms, etc.
• Repurpose staff for childcare centers
Statistics and Surveillance• Leverage relationships with
academic medical centers to get results faster to preserve PPE
• Employ known, native Spanish speakers to improve quality of contact tracing data
• Purchase Tableau subscription to share data easily with the public

Remarkable Rural Innovation
Supplies• Start an in-house PPE workshop w/ non-frontline
employees• Buy syringes now• Exploit all rural supply chains, i.e. paint, auto, vet,
agricultural, hardware stores• Re-use surgical tray blue wraps to extend life of N-
95s• Create portable PPE carts and appoint PPE czars

What would you do differently?
• Maintain stronger relationships w/ urban or academic facilities
• Frame guidance in terms of what one can do• Prioritize planning for the most vulnerable first• Explore a regional strategy for staff, supplies, and testing• Think infectious diseases in remodels, new construction• Incorporate rural philanthropy in the recovery phase• Cross-train staff at all times• Transition to multi-use PPE

How can an individual organization begin to develop strategies to address disparities in a post-COVID-19 world?

WHO
WHAT
WHERE
WHY
HOW
WHEN
OUTCOME NEEDS IMPROVEMENT?
ARE THE STAKEHOLDERS?
ARE OPPORTUNITIES TO SHARE?
ISN’T IT ALREADY HAPPENING?
DO WE MEASURE ITS SUCCESS?
DO WE EXPECT TO SEE PROGRESS?
THROUGH A HEALTH EQUITY LENS

Take what you’re already measuring and divide it by people group.
WHAT OUTCOME NEEDS IMPROVEMENT?
THROUGH A HEALTH EQUITY LENS
WHO ARE THE STAKEHOLDERS?
Think about all groups of people this outcome affects.
THROUGH A HEALTH EQUITY LENS
WHERE ARE OPPORTUNITIES TO SHARE?
Consider unlikely contributions from unlikely sources.
THROUGH A HEALTH EQUITY LENS

WHY ISN’T IT ALREADY HAPPENING?
Is it a capacity issue or a policy issue? Can it be "hacked” (retooled)?
THROUGH A HEALTH EQUITY LENS

HOW DO WE MEASURE ITS SUCCESS?
Ensure the impact is measurable.
THROUGH A HEALTH EQUITY LENS

Build out a specific timeline.
WHEN DO WE EXPECT TO SEE PROGRESS?
THROUGH A HEALTH EQUITY LENS

WHO
WHAT
WHERE
WHY
HOW
OUTCOME NEEDS IMPROVEMENT?
ARE THE STAKEHOLDERS?
ARE OPPORTUNITIES TO SHARE?
ISN’T IT ALREADY HAPPENING?
DO WE MEASURE ITS SUCCESS?
WHEN DO WE EXPECT TO SEE PROGRESS?
THROUGH A HEALTH EQUITY LENS

Phase 2What’s next?

“Fullerton Hospital: Board Governance in a Rural Community.”
Elizabeth Teisberg, PhD, Executive Director
Scott Wallace, JD, Associate Professor and Managing Director

“Kearny County Hospital: Improving Rural Maternal Health Care.”
Elizabeth Teisberg, PhD, Executive Director
Scott Wallace, JD, Associate Professor and Managing Director

“Value-based Health Care in the Shadow of a Pandemic.”
Bob Hansen, PhDProfessor of Business Administration

“Building Integration: The Merger of Conejos County Hospital and San Luis Valley Regional Medical Center to Create San Luis Valley Health
Clif Petty, PhDDean, Breech School of Business
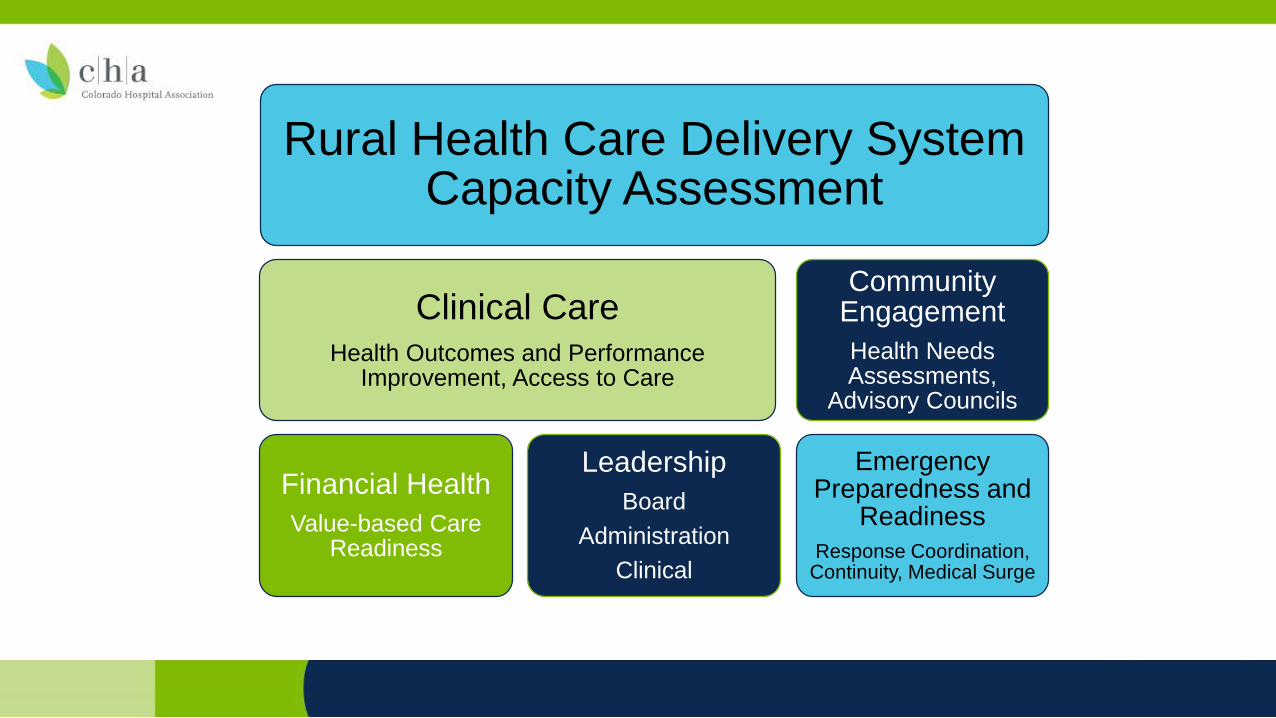
Rural Health Care Delivery System Capacity Assessment
Clinical CareHealth Outcomes and Performance
Improvement, Access to Care
Financial HealthValue-based Care
Readiness
LeadershipBoard
Administration Clinical
Community EngagementHealth Needs Assessments,
Advisory Councils
Emergency Preparedness and
ReadinessResponse Coordination,
Continuity, Medical Surge

Leadership Lessons from COVID-19
How do we align priorities?As leaders, we must each serve as a steady, guiding north star.
Why did it take a crisis to get there? COVID-19 highlighted and exploited the hairline fractures in our system.
Where are the solutions? As leaders, we must listen to the people most affected.
Is collaboration required or simply a best practice? People die if we don’t work together.

Why is this work so important?

A Final Thought:
Exhaustion is a silent thief of empathy.

Summary and Takeaways