reimbursement compliance auditing - leadingage new york complianc… · reimbursement compliance...
TRANSCRIPT
ZIMMET HEALTHCARE SERVICES GROUP, LLC 1
Reimbursement Compliance Auditing
1
May 21, 2013
Agenda
• Introduction to Compliance Auditing
• Auditing Principles and Structure
• Medicare / CMI Benchmarking and Audits: Identifying “Red Flags” in Your Claim Profile
• Getting to Know Your “Friendly” Third Party Auditors
• SNF Audit Trends
• Preparing Yourself for Audit
2
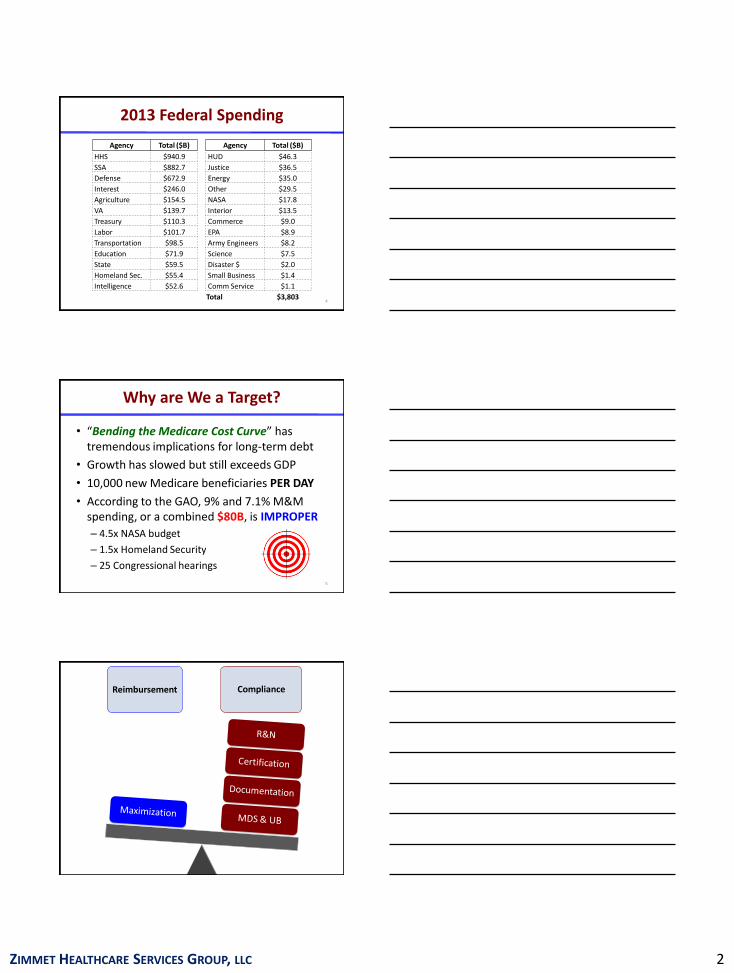
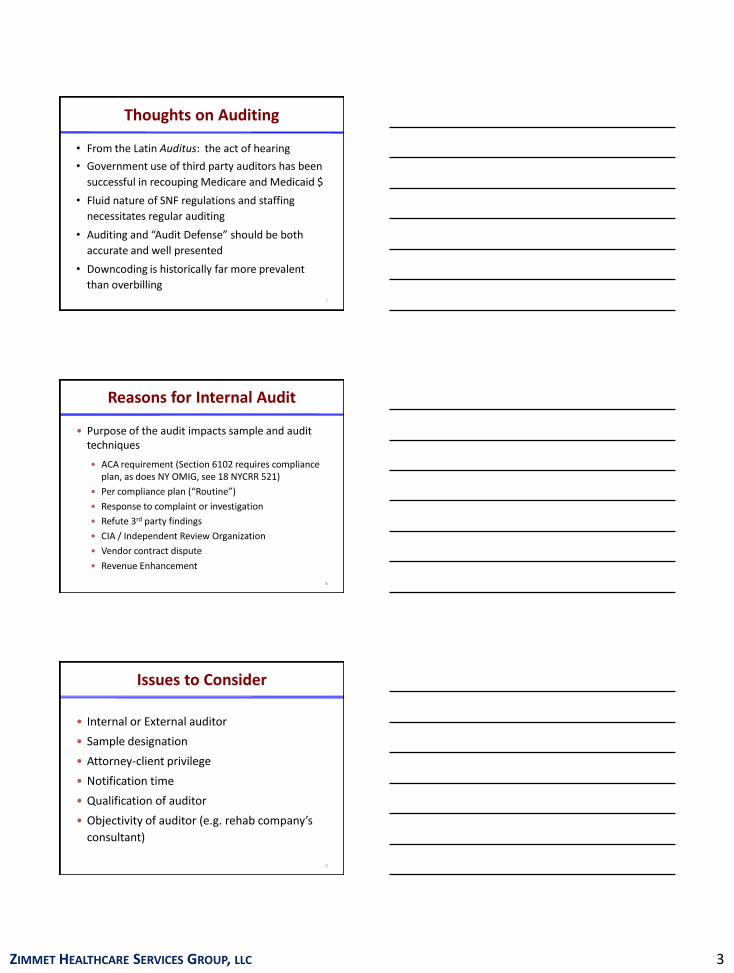
2013 Federal Spending
3
15%
11%
23%
18%
6%
33%Medicare
Medicaid
Social Security
Defense
Interest
Other
2013 Federal Spending = $3.8 Trillion
ZIMMET HEALTHCARE SERVICES GROUP, LLC 2
2013 Federal Spending
4
Agency Total ($B) Agency Total ($B)
HHS $940.9 HUD $46.3
SSA $882.7 Justice $36.5
Defense $672.9 Energy $35.0
Interest $246.0 Other $29.5
Agriculture $154.5 NASA $17.8
VA $139.7 Interior $13.5
Treasury $110.3 Commerce $9.0
Labor $101.7 EPA $8.9
Transportation $98.5 Army Engineers $8.2
Education $71.9 Science $7.5
State $59.5 Disaster $ $2.0
Homeland Sec. $55.4 Small Business $1.4
Intelligence $52.6 Comm Service $1.1
Total $3,803
Why are We a Target?
• “Bending the Medicare Cost Curve” has tremendous implications for long-term debt
• Growth has slowed but still exceeds GDP
• 10,000 new Medicare beneficiaries PER DAY
• According to the GAO, 9% and 7.1% M&M spending, or a combined $80B, is IMPROPER
– 4.5x NASA budget
– 1.5x Homeland Security
– 25 Congressional hearings
5
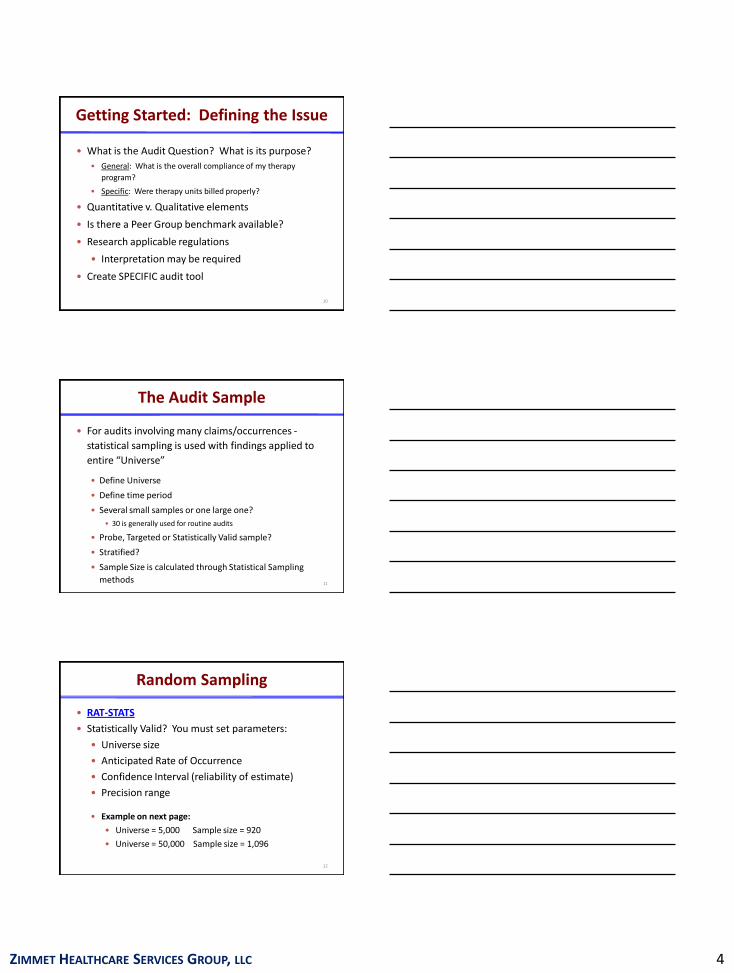
6
Reimbursement Compliance
ZIMMET HEALTHCARE SERVICES GROUP, LLC 3
Thoughts on Auditing
• From the Latin Auditus: the act of hearing
• Government use of third party auditors has been
successful in recouping Medicare and Medicaid $
• Fluid nature of SNF regulations and staffing
necessitates regular auditing
• Auditing and “Audit Defense” should be both
accurate and well presented
• Downcoding is historically far more prevalent
than overbilling7
Reasons for Internal Audit
• Purpose of the audit impacts sample and audit techniques
• ACA requirement (Section 6102 requires compliance plan, as does NY OMIG, see 18 NYCRR 521)
• Per compliance plan (“Routine”)
• Response to complaint or investigation
• Refute 3rd party findings
• CIA / Independent Review Organization
• Vendor contract dispute
• Revenue Enhancement
8
Issues to Consider
• Internal or External auditor
• Sample designation
• Attorney-client privilege
• Notification time
• Qualification of auditor
• Objectivity of auditor (e.g. rehab company’s
consultant)
9
ZIMMET HEALTHCARE SERVICES GROUP, LLC 4
Getting Started: Defining the Issue
• What is the Audit Question? What is its purpose?
• General: What is the overall compliance of my therapy
program?
• Specific: Were therapy units billed properly?
• Quantitative v. Qualitative elements
• Is there a Peer Group benchmark available?
• Research applicable regulations
• Interpretation may be required
• Create SPECIFIC audit tool
10
The Audit Sample
• For audits involving many claims/occurrences -
statistical sampling is used with findings applied to
entire “Universe”
• Define Universe
• Define time period
• Several small samples or one large one?
• 30 is generally used for routine audits
• Probe, Targeted or Statistically Valid sample?
• Stratified?
• Sample Size is calculated through Statistical Sampling
methods 11
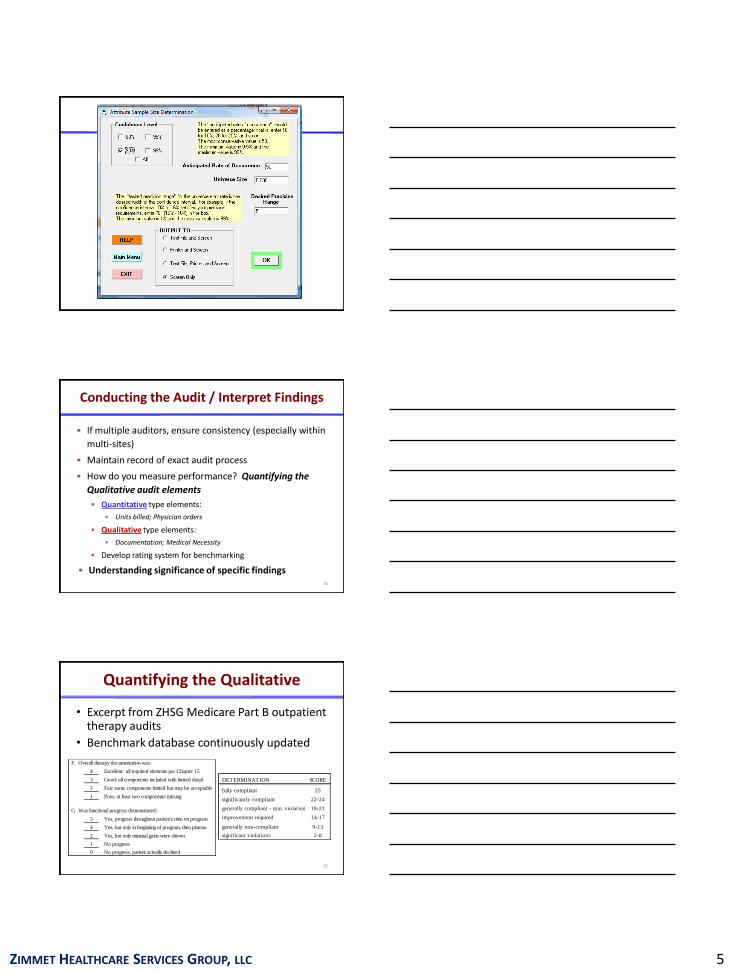
Random Sampling
• RAT-STATS
• Statistically Valid? You must set parameters:
• Universe size
• Anticipated Rate of Occurrence
• Confidence Interval (reliability of estimate)
• Precision range
• Example on next page:
• Universe = 5,000 Sample size = 920
• Universe = 50,000 Sample size = 1,096
12
ZIMMET HEALTHCARE SERVICES GROUP, LLC 5
Conducting the Audit / Interpret Findings
• If multiple auditors, ensure consistency (especially within
multi-sites)
• Maintain record of exact audit process
• How do you measure performance? Quantifying the
Qualitative audit elements
• Quantitative type elements:
• Units billed; Physician orders
• Qualitative type elements:
• Documentation; Medical Necessity
• Develop rating system for benchmarking
• Understanding significance of specific findings14
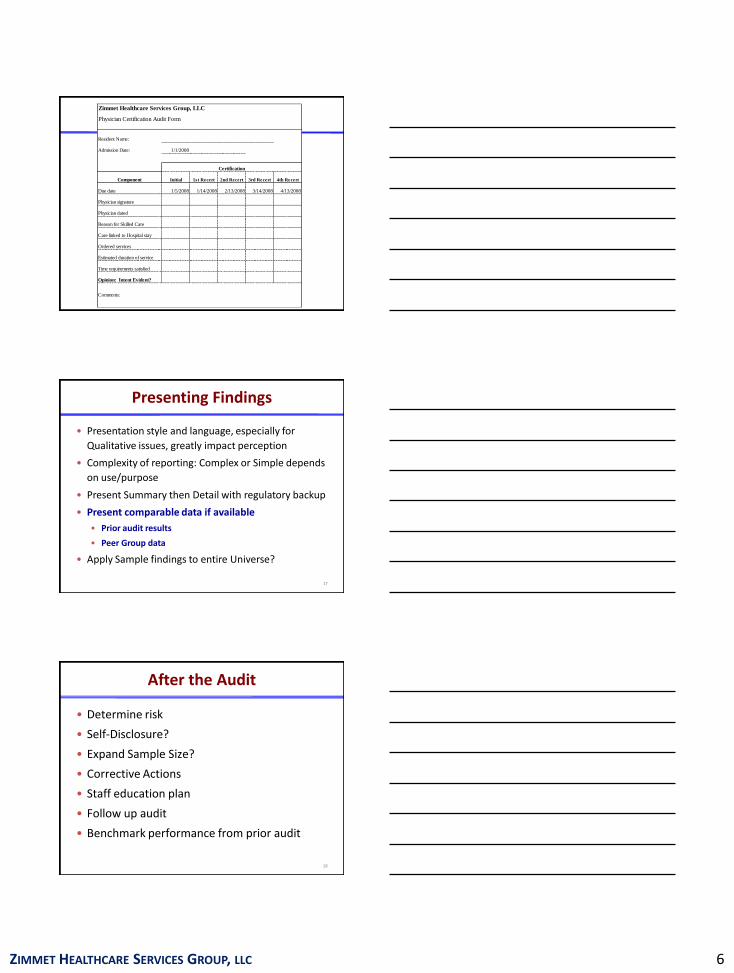
Quantifying the Qualitative
• Excerpt from ZHSG Medicare Part B outpatient therapy audits
• Benchmark database continuously updated
15
DETERMINATION SCORE
fully compliant 25
significantly compliant 22-24
generally compliant - min. violations 18-21
improvement required 14-17
generally non-compliant 9-13
significant violations 2-8
F. Overall therapy documentation was:
4 Excellent: all required elements per Chapter 15
3 Good: all components included with limited detail
2 Fair: some components limited but may be acceptable
1 Poor: at least two components missing
G. Was functional progress demonstrated:
5 Yes, progress throughout patient's time on program
4 Yes, but only in beginning of program, then plateau
2 Yes, but only minimal gains were shown
1 No progress
0 No progress, patient actually declined
ZIMMET HEALTHCARE SERVICES GROUP, LLC 6
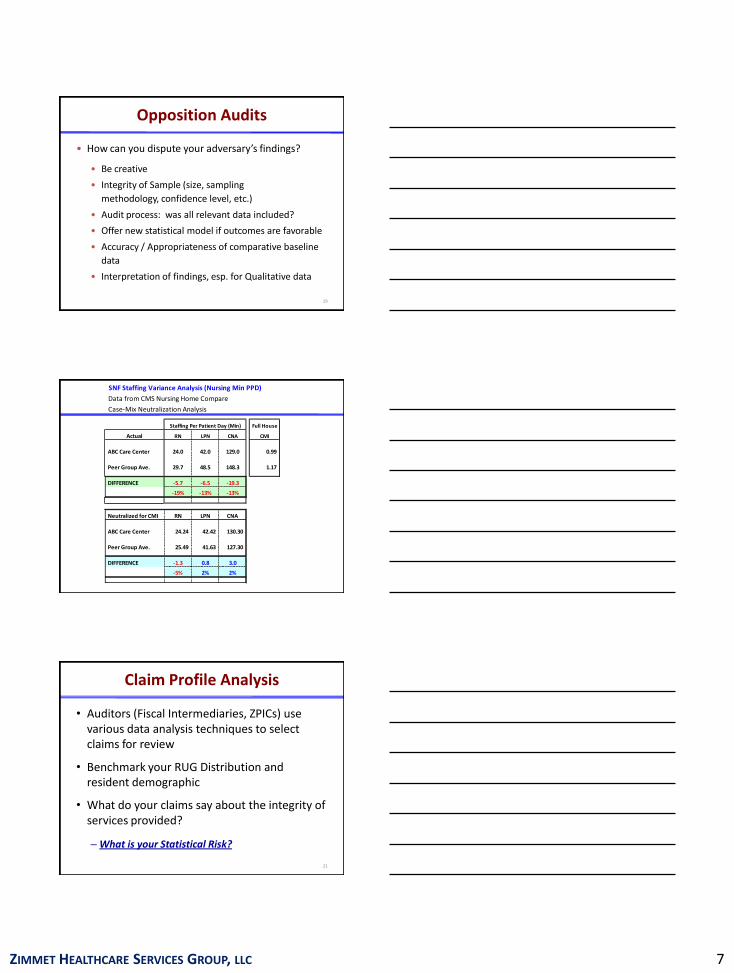
Zimmet Healthcare Services Group, LLC
Physician Certification Audit Form
Resident Name:
Admission Date: 1/1/2008
Certification
Component Initial 1st Recert 2nd Recert 3rd Recert 4th Recert
Due date 1/5/2008 1/14/2008 2/13/2008 3/14/2008 4/13/2008
Physician signature
Physician dated
Reason for Skilled Care
Care linked to Hospital stay
Ordered services
Estimated duration of service
Time requirements satisfied
Opinion: Intent Evident?
Comments:
Presenting Findings
• Presentation style and language, especially for
Qualitative issues, greatly impact perception
• Complexity of reporting: Complex or Simple depends
on use/purpose
• Present Summary then Detail with regulatory backup
• Present comparable data if available
• Prior audit results
• Peer Group data
• Apply Sample findings to entire Universe?
17
After the Audit
• Determine risk
• Self-Disclosure?
• Expand Sample Size?
• Corrective Actions
• Staff education plan
• Follow up audit
• Benchmark performance from prior audit
18
ZIMMET HEALTHCARE SERVICES GROUP, LLC 7
Opposition Audits
• How can you dispute your adversary’s findings?
• Be creative
• Integrity of Sample (size, sampling
methodology, confidence level, etc.)
• Audit process: was all relevant data included?
• Offer new statistical model if outcomes are favorable
• Accuracy / Appropriateness of comparative baseline
data
• Interpretation of findings, esp. for Qualitative data
19
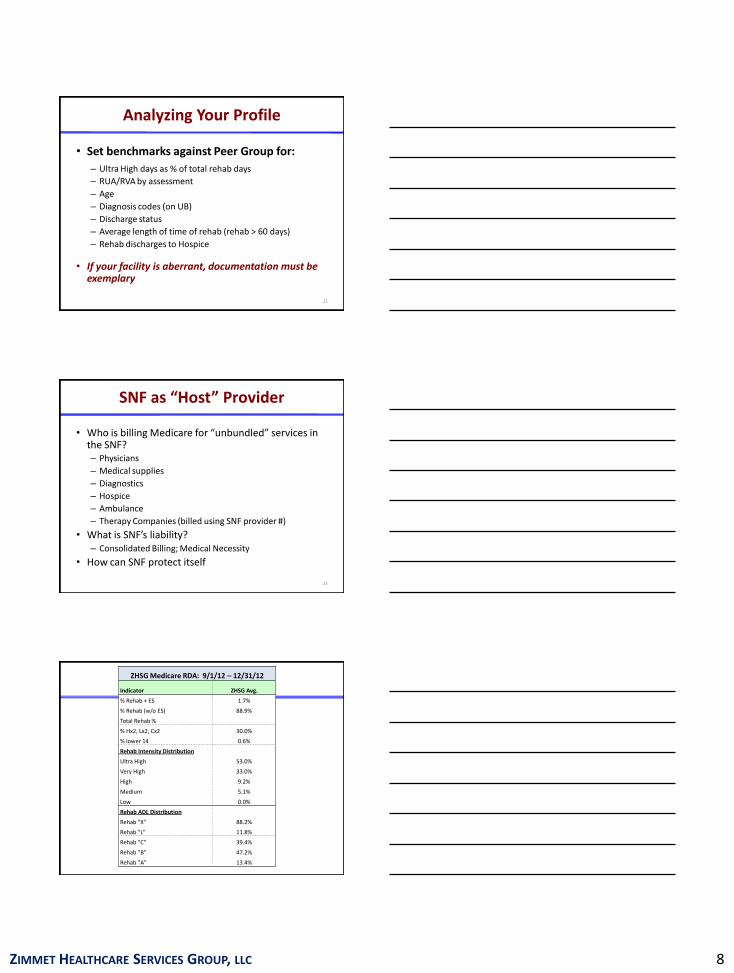
SNF Staffing Variance Analysis (Nursing Min PPD)
Data from CMS Nursing Home Compare
Case-Mix Neutralization Analysis
Full House
Actual RN LPN CNA CMI
ABC Care Center 24.0 42.0 129.0 0.99
Peer Group Ave. 29.7 48.5 148.3 1.17
DIFFERENCE -5.7 -6.5 -19.3
-19% -13% -13%
Neutralized for CMI RN LPN CNA
ABC Care Center 24.24 42.42 130.30
Peer Group Ave. 25.49 41.63 127.30
DIFFERENCE -1.3 0.8 3.0
-5% 2% 2%
Staffing Per Patient Day (Min)
Claim Profile Analysis
• Auditors (Fiscal Intermediaries, ZPICs) use various data analysis techniques to select claims for review
• Benchmark your RUG Distribution and resident demographic
• What do your claims say about the integrity of services provided?
– What is your Statistical Risk?
21
ZIMMET HEALTHCARE SERVICES GROUP, LLC 8
Analyzing Your Profile
• Set benchmarks against Peer Group for:
– Ultra High days as % of total rehab days
– RUA/RVA by assessment
– Age
– Diagnosis codes (on UB)
– Discharge status
– Average length of time of rehab (rehab > 60 days)
– Rehab discharges to Hospice
• If your facility is aberrant, documentation must be exemplary
22
SNF as “Host” Provider
• Who is billing Medicare for “unbundled” services in the SNF?– Physicians
– Medical supplies
– Diagnostics
– Hospice
– Ambulance
– Therapy Companies (billed using SNF provider #)
• What is SNF’s liability? – Consolidated Billing; Medical Necessity
• How can SNF protect itself
23
ZHSG Medicare RDA: 9/1/12 – 12/31/12
Indicator ZHSG Avg.
% Rehab + ES 1.7%
% Rehab (w/o ES) 88.9%
Total Rehab %
% Hx2, Lx2, Cx2 30.0%
% lower 14 0.6%
Rehab Intensity Distribution
Ultra High 53.0%
Very High 33.0%
High 9.2%
Medium 5.1%
Low 0.0%
Rehab ADL Distribution
Rehab "X" 88.2%
Rehab "L" 11.8%
Rehab "C" 39.4%
Rehab "B" 47.2%
Rehab "A" 13.4%
ZIMMET HEALTHCARE SERVICES GROUP, LLC 9
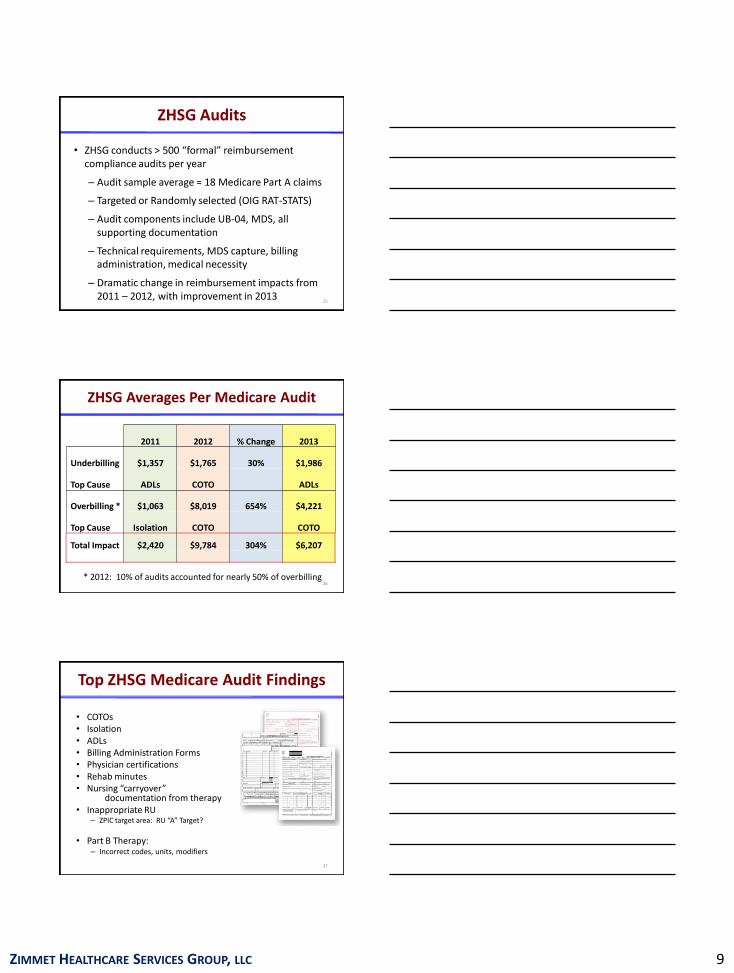
ZHSG Audits
• ZHSG conducts > 500 “formal” reimbursement compliance audits per year
– Audit sample average = 18 Medicare Part A claims
– Targeted or Randomly selected (OIG RAT-STATS)
– Audit components include UB-04, MDS, all supporting documentation
– Technical requirements, MDS capture, billing administration, medical necessity
– Dramatic change in reimbursement impacts from 2011 – 2012, with improvement in 2013
25
ZHSG Averages Per Medicare Audit
26* 2012: 10% of audits accounted for nearly 50% of overbilling
2011 2012 % Change 2013
Underbilling $1,357 $1,765 30% $1,986
Top Cause ADLs COTO ADLs
Overbilling * $1,063 $8,019 654% $4,221
Top Cause Isolation COTO COTO
Total Impact $2,420 $9,784 304% $6,207
Top ZHSG Medicare Audit Findings
• COTOs• Isolation• ADLs• Billing Administration Forms• Physician certifications• Rehab minutes• Nursing “carryover”
documentation from therapy• Inappropriate RU
– ZPIC target area: RU “A” Target?
• Part B Therapy: – Incorrect codes, units, modifiers
27
ZIMMET HEALTHCARE SERVICES GROUP, LLC 10
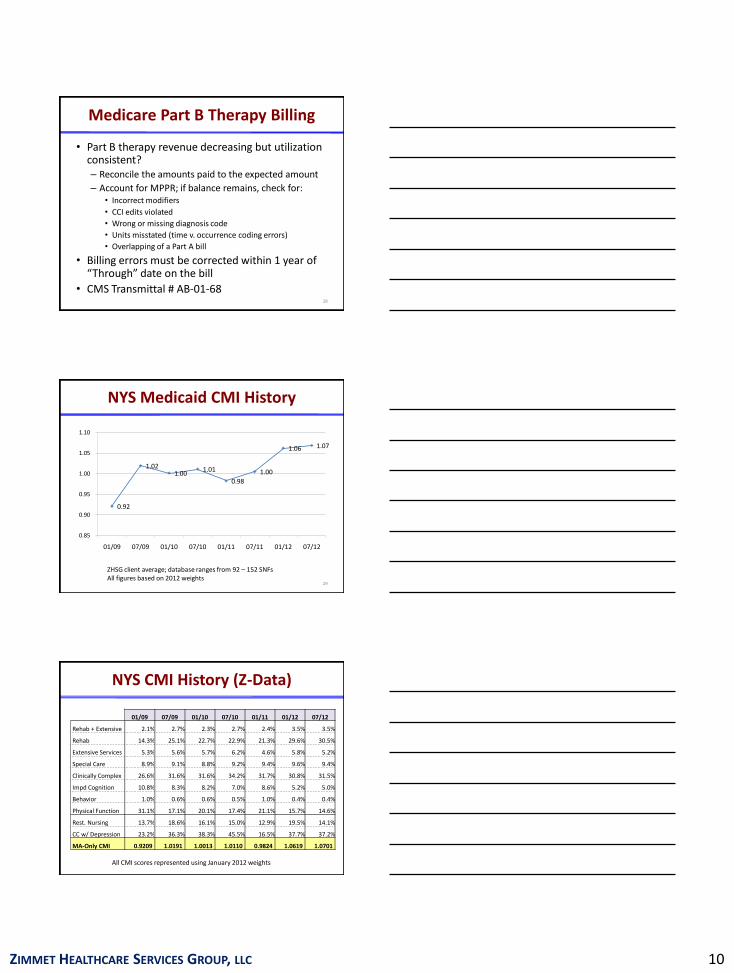
Medicare Part B Therapy Billing
• Part B therapy revenue decreasing but utilization consistent?– Reconcile the amounts paid to the expected amount
– Account for MPPR; if balance remains, check for:• Incorrect modifiers
• CCI edits violated
• Wrong or missing diagnosis code
• Units misstated (time v. occurrence coding errors)
• Overlapping of a Part A bill
• Billing errors must be corrected within 1 year of “Through” date on the bill
• CMS Transmittal # AB-01-6828
NYS Medicaid CMI History
29
ZHSG client average; database ranges from 92 – 152 SNFsAll figures based on 2012 weights
0.92
1.02 1.00
1.01
0.98
1.00
1.06 1.07
0.85
0.90
0.95
1.00
1.05
1.10
01/09 07/09 01/10 07/10 01/11 07/11 01/12 07/12
01/09 07/09 01/10 07/10 01/11 01/12 07/12
Rehab + Extensive 2.1% 2.7% 2.3% 2.7% 2.4% 3.5% 3.5%
Rehab 14.3% 25.1% 22.7% 22.9% 21.3% 29.6% 30.5%
Extensive Services 5.3% 5.6% 5.7% 6.2% 4.6% 5.8% 5.2%
Special Care 8.9% 9.1% 8.8% 9.2% 9.4% 9.6% 9.4%
Clinically Complex 26.6% 31.6% 31.6% 34.2% 31.7% 30.8% 31.5%
Impd Cognition 10.8% 8.3% 8.2% 7.0% 8.6% 5.2% 5.0%
Behavior 1.0% 0.6% 0.6% 0.5% 1.0% 0.4% 0.4%
Physical Function 31.1% 17.1% 20.1% 17.4% 21.1% 15.7% 14.6%
Rest. Nursing 13.7% 18.6% 16.1% 15.0% 12.9% 19.5% 14.1%
CC w/ Depression 23.2% 36.3% 38.3% 45.5% 16.5% 37.7% 37.2%
MA-Only CMI 0.9209 1.0191 1.0013 1.0110 0.9824 1.0619 1.0701
NYS CMI History (Z-Data)
All CMI scores represented using January 2012 weights
ZIMMET HEALTHCARE SERVICES GROUP, LLC 11
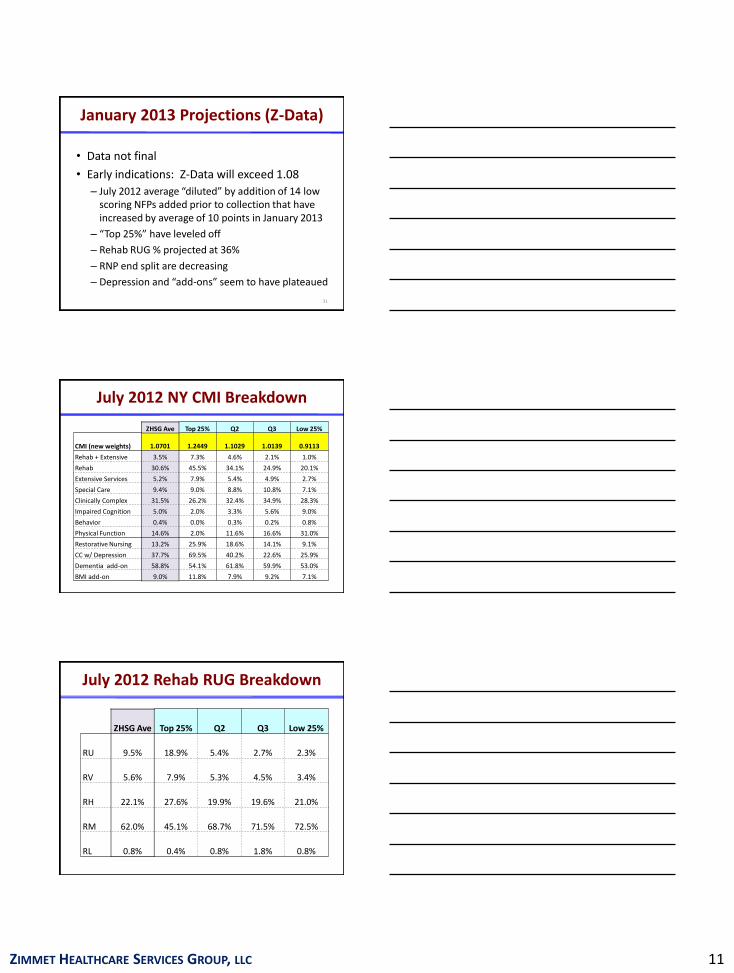
• Data not final
• Early indications: Z-Data will exceed 1.08
– July 2012 average “diluted” by addition of 14 low scoring NFPs added prior to collection that have increased by average of 10 points in January 2013
– “Top 25%” have leveled off
– Rehab RUG % projected at 36%
– RNP end split are decreasing
– Depression and “add-ons” seem to have plateaued
31
January 2013 Projections (Z-Data)
July 2012 NY CMI Breakdown
ZHSG Ave Top 25% Q2 Q3 Low 25%
CMI (new weights) 1.0701 1.2449 1.1029 1.0139 0.9113
Rehab + Extensive 3.5% 7.3% 4.6% 2.1% 1.0%
Rehab 30.6% 45.5% 34.1% 24.9% 20.1%
Extensive Services 5.2% 7.9% 5.4% 4.9% 2.7%
Special Care 9.4% 9.0% 8.8% 10.8% 7.1%
Clinically Complex 31.5% 26.2% 32.4% 34.9% 28.3%
Impaired Cognition 5.0% 2.0% 3.3% 5.6% 9.0%
Behavior 0.4% 0.0% 0.3% 0.2% 0.8%
Physical Function 14.6% 2.0% 11.6% 16.6% 31.0%
Restorative Nursing 13.2% 25.9% 18.6% 14.1% 9.1%
CC w/ Depression 37.7% 69.5% 40.2% 22.6% 25.9%
Dementia add-on 58.8% 54.1% 61.8% 59.9% 53.0%
BMI add-on 9.0% 11.8% 7.9% 9.2% 7.1%
July 2012 Rehab RUG Breakdown
ZHSG Ave Top 25% Q2 Q3 Low 25%
RU 9.5% 18.9% 5.4% 2.7% 2.3%
RV 5.6% 7.9% 5.3% 4.5% 3.4%
RH 22.1% 27.6% 19.9% 19.6% 21.0%
RM 62.0% 45.1% 68.7% 71.5% 72.5%
RL 0.8% 0.4% 0.8% 1.8% 0.8%
ZIMMET HEALTHCARE SERVICES GROUP, LLC 12
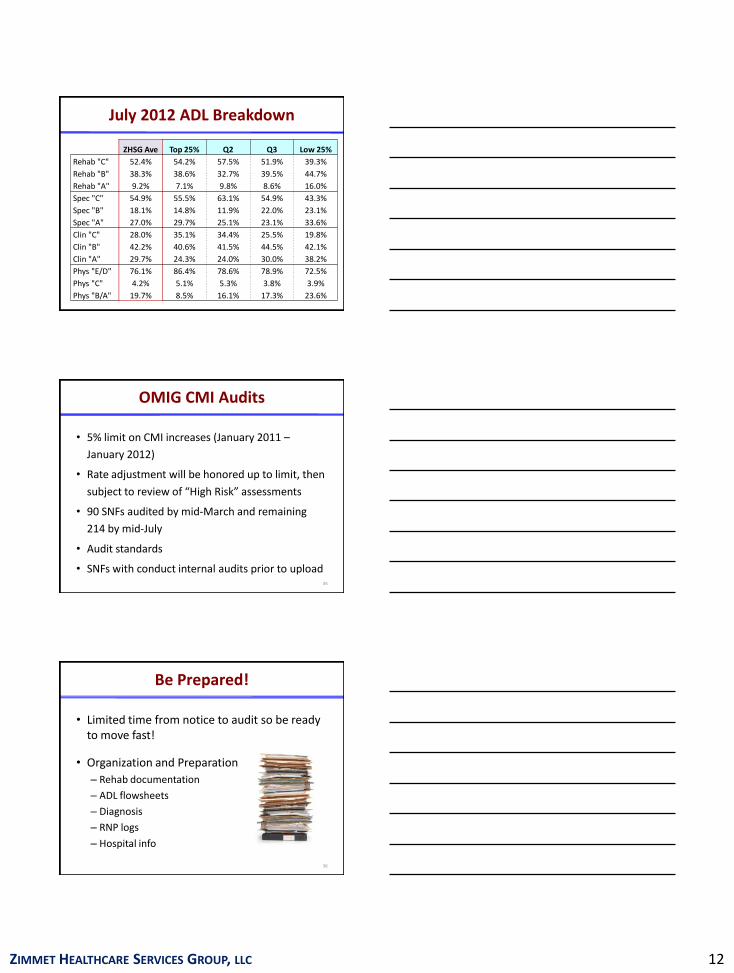
ZHSG Ave Top 25% Q2 Q3 Low 25%
Rehab "C" 52.4% 54.2% 57.5% 51.9% 39.3%
Rehab "B" 38.3% 38.6% 32.7% 39.5% 44.7%
Rehab "A" 9.2% 7.1% 9.8% 8.6% 16.0%
Spec "C" 54.9% 55.5% 63.1% 54.9% 43.3%
Spec "B" 18.1% 14.8% 11.9% 22.0% 23.1%
Spec "A" 27.0% 29.7% 25.1% 23.1% 33.6%
Clin "C" 28.0% 35.1% 34.4% 25.5% 19.8%
Clin "B" 42.2% 40.6% 41.5% 44.5% 42.1%
Clin "A" 29.7% 24.3% 24.0% 30.0% 38.2%
Phys "E/D" 76.1% 86.4% 78.6% 78.9% 72.5%
Phys "C" 4.2% 5.1% 5.3% 3.8% 3.9%
Phys "B/A" 19.7% 8.5% 16.1% 17.3% 23.6%
July 2012 ADL Breakdown
OMIG CMI Audits
• 5% limit on CMI increases (January 2011 –
January 2012)
• Rate adjustment will be honored up to limit, then
subject to review of “High Risk” assessments
• 90 SNFs audited by mid-March and remaining
214 by mid-July
• Audit standards
• SNFs with conduct internal audits prior to upload35
• Limited time from notice to audit so be ready to move fast!
• Organization and Preparation
– Rehab documentation
– ADL flowsheets
– Diagnosis
– RNP logs
– Hospital info
36
Be Prepared!
ZIMMET HEALTHCARE SERVICES GROUP, LLC 13
Medicaid CMI Audit Actions
• SNFs are required to have Compliance Plan including Reimbursement Auditing
• What happens if you find overstated CMI assessments?
– Structural issue with correcting assessments included in CMI collections - No limit to how far back we may go to correct an MDS, but once CMI is final, modifications will not impact scores
– NY providers: We have been in contact with the Bureau of Long Term Care Reimbursement (“BLTCR”) and OMIG to clarify this issue. BLTCR instructed us as follows:
• Follow the Federal MDS correction policy; and
• Send a letter to BLTCR and OMIG identifying particular MDS & error/mistake
37
Meet Your Auditors
• OMIG New York/MICs
• RACs
• ZPICs
• Fiscal Intermediaries/MACs
38
2012 Top Reasons for Medicare SNF Audits
• RUA on Any Assessment (FI/MAC, ZPIC)
• Disproportionate Number of RUB, RUC Days Compare to Peers (FI/MAC, ZPIC, DOJ)
• RU “anything” over 60 days (FI/MAC, ZPICs, DOJ)
• Excessive LOS Compared to Peers (FI/MACs)
• Disproportionate $ Paid to a Provider Compared to Peers (FI/MAC, ZPIC, OIG)
• Part B Therapy Claims with Ill-defined Diagnosis Codes (719.7, 728.9, 780.7, 290.0) (FI/MAC)
• Part B Therapy with CCI Modifier or Units Errors (RAC)
• Claims with 042 Diagnosis (FI/MAC)
ZIMMET HEALTHCARE SERVICES GROUP, LLC 14
OMIG in NY
• Spring 2013 brought a intensive round of Medicaid audits by the OMIG
– Reports from colleagues indicate the OMIG used a more gentle approach than other audit initiatives presently being conducted
• New audit staff on this first round
• Zimmet anticipates that additional audit efforts will be not be as unforgiving
MICs
What are Medicaid Integrity Contractors (MICs)?
• Private companies that conduct audit-related activities under contract to the Medicaid Integrity Group (MIG), which is charged by the U.S. Department of Health & Human Services with carrying out the Medicaid Integrity Program (MIP).
• There are three primary MICs:– 1) Review MICs analyze Medicaid claims data to
determine whether provider fraud, waste, or abuse has occurred or may have occurred;
– 2) Audit MICs audit provider claims and identify overpayments; and
– 3) Education MICs provide education to providers on payment integrity and quality-of-care
Medicare RACs in NY
• Performance Recovery (aka: Diversified Collection
Services, Inc.)– This RAC is based in Livermore, CA
• Website: www.performantrac.com or www.dcsrac.com
• Contact #: 1-888-201-0580
– Prior audit efforts in SNFs were based on automated claims data analysis
– 2013 brings “complex” review
• Medical records can be requested (ADRs) for both pre- and post-pay review
• RACs are allowed to go back 3 years from date of service
• Website lists SNF psych claims and high intensity RUGs as audit targets
– Beginning May 2013, this RAC will be responsible for all pre-pay Part B therapy services over the $3700 payment limitation
ZIMMET HEALTHCARE SERVICES GROUP, LLC 15
ADR Requests
• In April 2013 a new ADR limitation was set for RAC auditors
• Each limit is based on the provider’s Medicare claims volume from the previous calendar year
• In addition to a limit based on the Medicare claims volume, claim type will also factor into the limit. Recovery Auditors may select up to 75% of any claim type for review
• For SNFs, one additional documentation request represents a beneficiary’s entire episode of care– This includes medical records for all services rendered
from the date of admission to the final date of discharge.
RAC Prepay Review Demonstration
• Allows Medicare Recovery Auditors (RACs) to review claims before they are paid to ensure that the provider complied with all Medicare payment rules. The Ras are conducting prepayment reviews on certain types of claims that historically result in high rates of improper payments. These reviews will focus on seven states with high populations of fraud- and error-prone providers (FL, CA, MI, TX, NY, LA, IL)and four states with high claims volumes of short inpatient hospital stays (PA, OH, NC, MO) for a total of 11 states
• Demo will also help lower the error rate by preventing improper payments rather than the traditional "pay and chase" methods of looking for improper payments after they occur (began 9/1/12)
ZPICs
• Fraud and abuse arm of Medicare program
– Not a simple medical review to validate coverage and payment
– They are looking for reasons to deny claims and pursue fraud allegations
• 2012 saw increase in “on-site” audit visits by ZPIC s (FL, CA, LA, VA) although they are active in all states
ZIMMET HEALTHCARE SERVICES GROUP, LLC 16
ZPICs
• ZPICs stepped up audits activities in 2012, triggered by 2010 OIG report that Medicare overpayments were rampant
• ZPICs have “reason to believe” there are problems in your facility before they arrive at your door or send requests for records
– They know a LOT about you and are not on a random search for improper claims
• ZPICs have focused on Part A claims for therapy services (disproportionate RU RUG %) but no service is outside their authority to investigate
ZPIC Audit Findings
• Currently ZPICs are finding reasons to deny based on technical and clinical reasons which make your claims invalid (pre & post pay):– Incomplete or incorrectly signed and dated
CERTS, ORDERS, PLANS of CARE
– Missing treatment records, progress notes,
– Inadequate PLOF on therapy records (SNF cannot justify need for services)
– Medically unnecessary services or level of service provided
How Do ZPIC Auditors Differ?
• The primary mission of ZPICs is to identify fraud• No random audits• No specification regarding look-back periods• Can make unlimited document requests• Not paid on a contingency fee basis, although they do get
performance bonuses – De facto policy making???
• RACs must identify/correct improper payments, have some limits document requests and are paid on a contingency basis
• MACs educate providers, process and conduct billing, correct behaviors in need of change, prevent future inappropriate billing, and recover payments
Adapted from Reed Smith in Provider Long Term Care, July 2012
ZIMMET HEALTHCARE SERVICES GROUP, LLC 17
ZPIC Power
• Because of their “mission” to uncover fraud, ZPIC findings can result in immediate suspension of payment– Apply error rates on reviewed claims to your
entire claims submission file for recoupment
– Demand overpayments be refunded
– DME providers can lose their Accrediting Organization (AO) certification withdrawn
– Cases may be forwarded to the Department of Justice for resolution• Results in legal action, penalties and possible
incarceration
Fiscal Intermediaries/MACs
• FIs & MACs must continue their contractual commitment to CMS to do medical review to determine if claims are being paid appropriately
• DATA DRIVEN (based on claims already submitted) to determine WHAT will be reviewed– FIs and MACs can set whatever criteria they
believe is valid to run data statistics for targeting facilities and specific claim types
You’ve Been Notified!
• Carefully review the letter or the online notification to determine:– Who is asking?
– What do they want?
– When and Where must it be submitted?
• Assign staff for responsibility of “How” to comply– Gathering the clinical and financial records
– Organize record to “tell the story” with orders, certs and any other information to demonstrate appropriateness and accuracy of claim
– Make an exact copy of the record to retain at facility
– Consider clinical and/or legal assistance to review documentation prior to submission
– Submit with dated tracking number
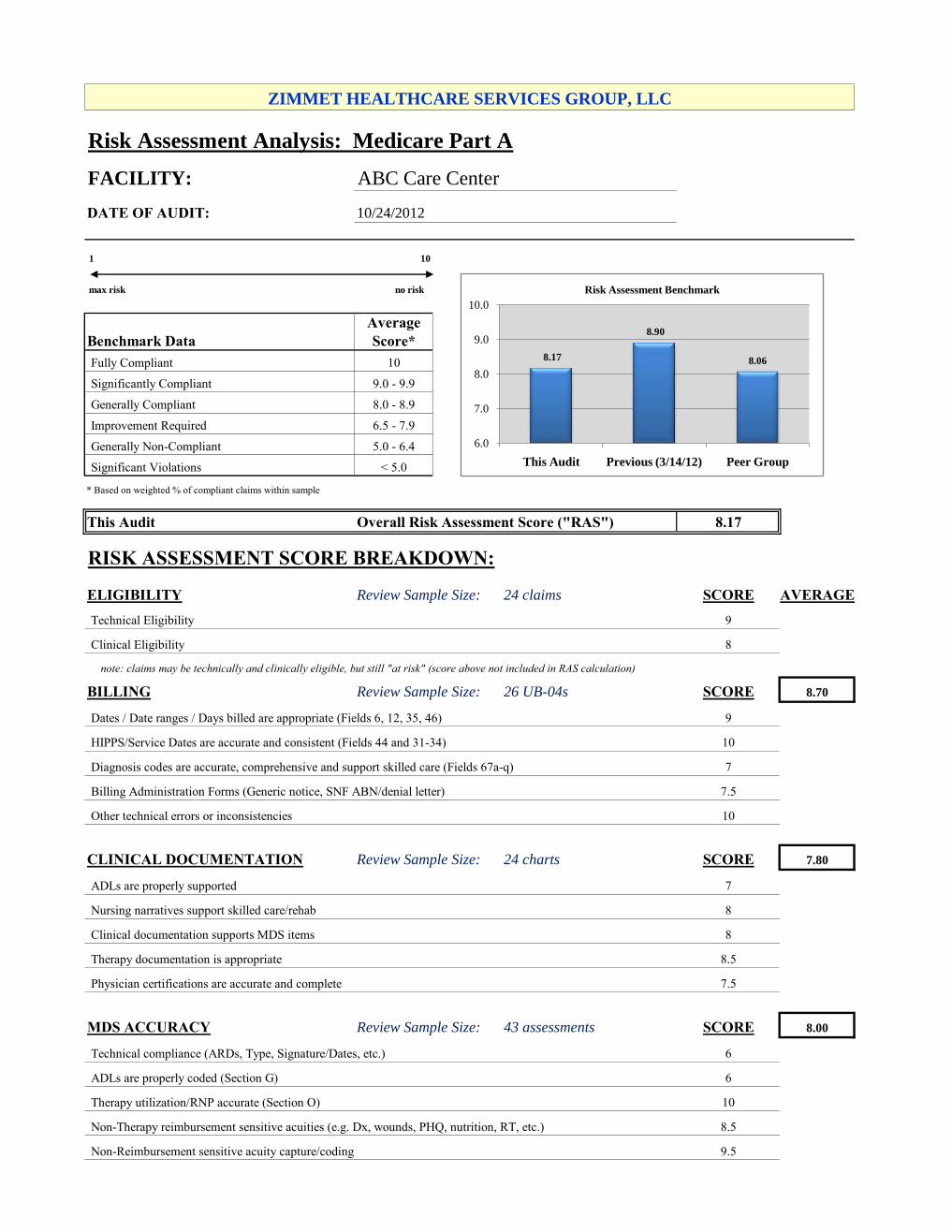
Risk Assessment Analysis: Medicare Part A
FACILITY: ABC Care Center
DATE OF AUDIT:
1 10
max risk no risk
Average
Benchmark Data Score*
Fully Compliant 10
Significantly Compliant 9.0 - 9.9
Generally Compliant 8.0 - 8.9
Improvement Required 6.5 - 7.9
Generally Non-Compliant 5.0 - 6.4
Significant Violations < 5.0
* Based on weighted % of compliant claims within sample
This Audit Overall Risk Assessment Score ("RAS") 8.17
RISK ASSESSMENT SCORE BREAKDOWN:
ELIGIBILITY Review Sample Size: 24 claims SCORE AVERAGE
Technical Eligibility 9
Clinical Eligibility 8
note: claims may be technically and clinically eligible, but still "at risk" (score above not included in RAS calculation)
BILLING Review Sample Size: 26 UB-04s SCORE 8.70
Dates / Date ranges / Days billed are appropriate (Fields 6, 12, 35, 46) 9
HIPPS/Service Dates are accurate and consistent (Fields 44 and 31-34) 10
Diagnosis codes are accurate, comprehensive and support skilled care (Fields 67a-q) 7
Billing Administration Forms (Generic notice, SNF ABN/denial letter) 7.5
Other technical errors or inconsistencies 10
CLINICAL DOCUMENTATION Review Sample Size: 24 charts SCORE 7.80
ADLs are properly supported 7
Nursing narratives support skilled care/rehab 8
Clinical documentation supports MDS items 8
Therapy documentation is appropriate 8.5
Physician certifications are accurate and complete 7.5
MDS ACCURACY Review Sample Size: 43 assessments SCORE 8.00
Technical compliance (ARDs, Type, Signature/Dates, etc.) 6
ADLs are properly coded (Section G) 6
Therapy utilization/RNP accurate (Section O) 10
Non-Therapy reimbursement sensitive acuities (e.g. Dx, wounds, PHQ, nutrition, RT, etc.) 8.5
Non-Reimbursement sensitive acuity capture/coding 9.5
10/24/2012
ZIMMET HEALTHCARE SERVICES GROUP, LLC
8.17
8.90
8.06
6.0
7.0
8.0
9.0
10.0
This Audit Previous (3/14/12) Peer Group
Risk Assessment Benchmark