relevance of wavefront aberrations of the human eye in corneal laser surgery
TRANSCRIPT

1615-1615/04/19/03-126 $ 30.00/0
Med. Laser Appl. 19: 126–135 (2004)Elsevier – Urban & Fischerhttp://www.elsevier.de/lasermed
Relevance of Wavefront Aberrations of the Human Eyein Corneal Laser Surgery
MICHAEL MROCHEN1,2, HANS PETER ISELI2, MAIK KAEMMERER3, PETER MIERDEL4, HANS-EBERHARD KRINKE4, and THEO SEILER2
1 Institute of Biomedical Engineering, Swiss Federal Institute of Technology, Zurich, Switzerland2 IROC – Institut für Refraktive und Ophthalmo-Chirurgie, Zurich, Switzerland3 Mikrolab GmbH, Fürth, Germany4 Technical University of Dresden, Department of Ophthalmology, Dresden, Germany
Submitted: July 2004 · Accepted: July 2004
Summary
The classical optical errors of the human eye – myopia, hyperopia, and astigmatism – are known to reduce the visu-al performance of the patient eye and can be corrected by means of glasses, contact lenses, or corneal laser surgery.However, the optic of each individual eye includes also imaging errors of higher order (wavefront aberrations oroptical aberrations) such as spherical aberration or coma like aberrations that can decrease the visual performance.In contrast to the classical optical errors, the wavefront aberrations of higher order can not be corrected by means ofglasses or contact lenses. However, modern laser systems used in corneal laser surgery possess the potential to cor-rect the optics of an individual eye for such higher order imaging errors. The correction of higher order aberrations improving imaging quality requires a precise knowledge of the rele-vance of such aberrations. Therefore, we performed a clinical trail to measure the higher order wavefront aberra-tions in a large population of 130 eyes that were scheduled for corneal laser surgery. The averaged human eye was found to be of good optical quality. On average all Zernike coefficient are statistical-ly not significant different from zero, except the vertical coma and the spherical aberration for 5 and 7 mm pupilsize. None of the individual eyes had ideal optical performance with an rms- wavefront error smaller than theMarechal criterion (diffraction limit). Fifty percent of the investigated eyes had significant optical aberrations atpupil sizes > 3.2 mm. This critical pupil size represents the smallest pupil diameter at which diffraction limit isachieved. A statistical cluster analysis demonstrates a significant increase of the rms-wavefront errors in the eyes ofpatients over 40 years old. In conclusion, the averaged human eye has a rather good optical quality exceeding the Marechal criterion (diffrac-tion limit) only by a factor of 2. However, none of the individual eyes achieved the optical quality of “averagedeye”. Thus, the human eye is in general designed to have an almost perfect optical performance, whereas the indi-vidual eye deviates significantly from this ideal imaging quality. Optical aberration become significant at a pupilindividual size above > 3.2 mm and as a consequence optical quality decreases drastically at larger pupil diametersas they occur under dimmed light conditions (mesopic vision). As the pupil diameter can be as large as 6 mm in di-ameter under such low light conditions, modern corneal laser surgery uses optical relevant treatment zones of6.0 mm or larger and, consequently, the corrections should include the higher order wavefront aberrations. Sur-geons and patients should be aware that the corrections of the higher order aberrations are not stable over time be-cause optical performance decreases also with age.
Key wordsOptical aberrations, wavefront sensing, Tscherning aberrometer, physiological optics, imaging errors of the human eye

Relevance of Wavefront Aberrations of the Human Eye in Corneal Laser Surgery 127
Introduction
The term “monochromatic optical aberrations” wascoined in the early 19th century and included at thattime all optical errors of the eye except the sphericalmyopic or hyperopic refractive error (34). In thistime, Hermann von Helmholtz described the optics ofthe eye to be imperfect and posed the question aboutthe quality of the retinal image that is projected bycornea and lens (13). At the end of the 19th century,Tscherning investigated the non-refractive errors of
the eye in more detail (33). Nevertheless, Helmholtzdescribed these higher order errors of minor impor-tance (13) in complete contrast to Tscherning (33) andGullstrand (11). Donders (7) defined and specifiedthe measurement and correction of ocular astigma-tism introducing the sphero-cylindrical error and,thus, reducing the “monochromatic optical aberra-tions” to higher order optical errors such as sphericalaberrations and coma.
In the second half of the last century several tech-niques to measure monochromatic aberrations of hu-
Fig. 1. Overview of Zernike polynomials up to the 4th radial order. Row number is polynomial order n, column number is sinusoidalfrequency f, table entry is the single-index k. To convert between k and the values of n and f, the following relationships can be used:
In the Zernike pyramid, the 1st radial order represents tilt /prismatic errors, the 2nd radial order represents defocus and astigmatism, the3rd radial order are coma-like aberrations and the 4th order include spherical aberration and higher order astigmatism.
n (n + 2) + fk = –––––––––––– .2

128 M. MROCHEN et al.
man eyes were developed. One of the first was thecrossed cylinder aberroscope introduced by Howlandand Howland for subjective measurements (14) andthe improved version for objective measurements in-troduced by Walsh and coworkers (3, 35). Artal andSantamaria (1, 29) developed a device to measure thepoint-spread function of the human eye and intro-duced methods to calculate the wavefront-aberrationsfrom such data. Liang et al (16, 17) presented the firstmeasurement of ocular aberrations using a Hartmann-Shack sensor in 1994 and He et al. (12) used a psy-chophysical procedure to measure wavefront aberra-tions. In 1997, Mierdel et al. (22) demonstrated theclinical use of an automated aberrometer based on theprinciples of Tscherning’s aberrometry (33). Wave-front analysis, however, never was a clinical issuemainly because there was no therapeutic approach tocorrect wavefront errors by optical means such asspectacles or contact lenses. This changed since theintroduction of aspheric excimer laser treatment ofthe cornea (30) and, more specifically, customizedablation (9, 24).
In technical optics, the quality of an optical systemis defined by the aberrations of the wavefront from itsideal plane or spherical shape (4). Anwar Gullstrand(11) established a complicated mathematical formal-ism to describe such wavefront aberrations that never
found acceptance in technical optics or clinical oph-thalmology. Zernike (32, 37) introduced a more prac-tical mathematical formalism using different polyno-mials to describe wavefront aberrations. This polyno-mials, still used in technical optics, are associatedwith special optical errors such as tilt, defocus, astig-matism of different orders, spherical aberrations,coma, and n-fold of the wavefront; see Figure 1. Theuse of Zernike polynomials allows decomposing thetotal wavefront error into subsets of such characteris-tic optical errors (Fig. 2). Wavefront aberrations arealways perpendicular to the light rays entering theeye, thus, it is possible to derive image quality of anindividual eye directly from the wavefront aberration.A quantitative measure of the optical imaging qualityis the rms-wavefront error (root-mean-square) of thewavefront deviation. An optical system is consideredgood if all Zernike coefficients are close to zero and,as a consequence, the rms-wavefront error is smallerthan 1/14 of the wavelength (Marechal criterion) (18,20) The pupil size at which the eye can be assumed tobe diffraction limited is called the critical pupil size.
The purpose of this study was to measure the opti-cal quality of the human eye in a population sched-uled for corneal laser surgery by means of an aber-rometer of the Tscherning-type and to investigate itsdependence on pupil size and age. The measured
Fig. 2. Zernike decomposition of wave-front aberrations. The total wavefront erroris a result of the sum of subsets of charac-teristic optical errors. In theory, an infinitenumber of Zernike polynomials can beused. However, in clinical routine the useof Zernike polynomials up to the 6th radialorder were found to be adequate.
Relevance of Wavefront Aberrations of the Human Eye in Corneal Laser Surgery 129
wavefront aberrations are discussed in terms ofZernike polynomials, the Marechal criterion, and crit-ical pupil sizes. The results are discussed with respectto their relevance in corneal laser surgery.
Material and methods
Study groupOne hundred and thirty eyes of 90 individuals wereenrolled in the study; bilateral measurements wereavailable in 40 persons. Subjects (eyes) were eligibleto be included in the study if (1) they were at least 18years of age, (2) were free of ocular diseases, (3) hada best-spectacle-corrected visual acuity of 20/20 orbetter, (4) the spherical equivalent of the refractionwas between – 8.0 D and + 2.0 D, (5) the manifest re-fractive cylinder was less than 3.0 D, and (6) wave-front analysis using the technique described belowwas available with a virtual pupil size of 7 mm (thedilated pupil was ≥7 mm in diameter). Demographicand refractive data of the study group are listed inTable 1.
ExaminationsThe clinical investigation of the individuals includedautorefractometry (Model 590, Zeiss-Humphrey, SanLeandro, California) and best-spectacle corrected vi-sual acuity (BCVA). After slit lamp inspection thepupils were dilated by 2 drops of tropicamide (Mydri-aticum Dispersa, Ciba Vision, Hettlingen, Germany)followed by a latency in a dark room until achievingmaximally dilated pupils which were necessary forthe following wavefront measurement.
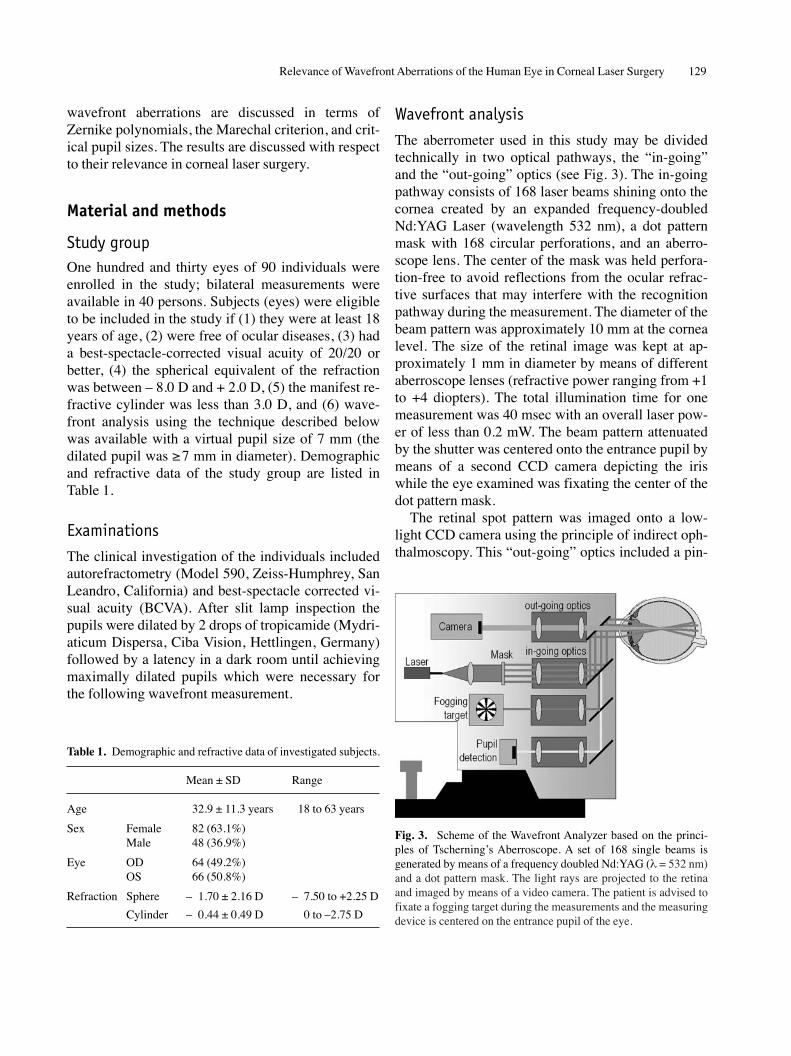
Wavefront analysisThe aberrometer used in this study may be dividedtechnically in two optical pathways, the “in-going”and the “out-going” optics (see Fig. 3). The in-goingpathway consists of 168 laser beams shining onto thecornea created by an expanded frequency-doubledNd:YAG Laser (wavelength 532 nm), a dot patternmask with 168 circular perforations, and an aberro-scope lens. The center of the mask was held perfora-tion-free to avoid reflections from the ocular refrac-tive surfaces that may interfere with the recognitionpathway during the measurement. The diameter of thebeam pattern was approximately 10 mm at the cornealevel. The size of the retinal image was kept at ap-proximately 1 mm in diameter by means of differentaberroscope lenses (refractive power ranging from +1to +4 diopters). The total illumination time for onemeasurement was 40 msec with an overall laser pow-er of less than 0.2 mW. The beam pattern attenuatedby the shutter was centered onto the entrance pupil bymeans of a second CCD camera depicting the iriswhile the eye examined was fixating the center of thedot pattern mask.
The retinal spot pattern was imaged onto a low-light CCD camera using the principle of indirect oph-thalmoscopy. This “out-going” optics included a pin-
Table 1. Demographic and refractive data of investigated subjects.
Mean ± SD Range
Age 32.9 ± 11.3 years 18 to 63 years
Sex Female 82 (63.1%)Male 48 (36.9%)
Eye OD 64 (49.2%)OS 66 (50.8%)
Refraction Sphere – 1.70 ± 2.16 D – 7.50 to +2.25 D
Cylinder – 0.44 ± 0.49 D 0 to –2.75 D
Fig. 3. Scheme of the Wavefront Analyzer based on the princi-ples of Tscherning’s Aberroscope. A set of 168 single beams isgenerated by means of a frequency doubled Nd:YAG (λ = 532 nm)and a dot pattern mask. The light rays are projected to the retinaand imaged by means of a video camera. The patient is advised tofixate a fogging target during the measurements and the measuringdevice is centered on the entrance pupil of the eye.

130 M. MROCHEN et al.
Fig. 4. Mean (± SD) higher order Zernike-coefficients of the investigated population(pupil size 5 and 7 mm; single-index-scheme,third to sixth order coefficients). Only verticalcoma C7 (p = 0.015) and spherical aberrationC12 (p = 0.01) were found to be significantlydifferent from zero. The small mean values(bars) compared to the large standard deviationdemonstrates that the “averaged” human eyehas only small higher order aberrations (meanvalues) but the higher order aberrations of mostof the individual eyes deviate significantlyfrom this “averaged” eye (standard deviation).
er order optical aberrations. With such a normaliza-tion factor, the contribution of the total wavefrontvariance by each term is given by the square of thecoefficient. Summing the squares of the coefficientsfor Zernike polynomial terms of a particular ordergives the contribution of that order to the variance.The normalization factors are calculated according tothe definition of the Zernike polynomials (4). As aquantitative measure of the optical aberrations theroot mean-square (rms) wavefront error Wrms was cal-culated by:
Wrms = √ S3 + S4 + S5 + S6 . (2)
The critical pupil size has been approximated byextrapolating linearly the rms-values calculated for7 mm and 5 mm pupil sizes to the value of theMarechal criterion. Here, the unit of the rms-value ismicrometer.
Zernike coefficients and wavefront errors werecompared statistically by means of the 2-tailed pairedt-test. Clinical variables were correlated with Zernikecoefficients and wavefront errors using parametricand nonparametric tests, and these correlations weretested for statistical significance, which was acceptedat p < 0.05.
Results
The mean and standard deviations of the Zernike-co-efficients from 3rd to 6th order averaged for all eyesare displayed in Figure 4. Nearly all Zernike-coeffi-
hole cropping the out-going pathway to a diameter ofless than 1 mm at the cornea level. The low-lightcamera was interfaced to a standard personal comput-er and the grabbed retinal dot pattern underwent im-age processing resulting in calculated centers of massof the retinal spots.
The ideal distortion-free (equal spaced) spot pat-tern was calculated based on the image magnificationof the Gullstrand’s reduced eye model, the previouslydetermined refraction, and the power of the usedaberroscope lens. From the deviations of the retinalspots from the distortion-free positions the actualwavefront was calculated in terms of Zernike-poly-nomials up to the 6th order for virtual pupil diametersof 5 mm and 7 mm.
Data analysisAs a quantitative measure of wavefront deviationfrom the ideal spherical form the total mean-squarewavefront error <W2> may be calculated by
where Cn are the Zernike-coefficients, Fn are normal-ization factors, S1 ... S6 are the sums of the wavefrontvariance for tilt, sphero-cylindrical and 3rd to 6th high-
1 2
– ∑ (CnFn)2r 2 + π n=1
<W2> =
<W2> = S1 + S2 + S3 + S4 + S5 + S6 (1)
1 5
– ∑ (CnFn)2r 4 + π n=3
1 9
– ∑ (CnFn)2r 6 +π n=6
1 14
– ∑ (CnFn)2r 8 + π n=10
1 20
– ∑ (CnFn)2r 10 + π n=15
1 27
– ∑ (CnFn)2r 12
π n=21+
=

Relevance of Wavefront Aberrations of the Human Eye in Corneal Laser Surgery 131
Fig. 5. Histogram of higher order rms-values interms of the Marechal-criterion of all investigat-ed eyes. For a 5 mm pupil the distribution isnearly Gaussian (p < 0.01), but not for 7 mmpupil size. No eye was found with an rms < 38 nm(Marachel-criterion for λ = 532 nm), so all eyesshowed significant aberrations. A: Marechal cri-terion; B: rms-value calculated from averagedZernike coefficients of higher order; C: meanvalue of the higher order rms of all eyes at 5 mmpupil size (0.138 ± 0.064 µm).
Fig. 6. Histogramm of the critical pupil sizeover all investigated eyes. At this pupil the eyefulfills the Marechal criterion and is aberration-free by definition (median 3.22 mm).
Fig. 7. Comparison between the mean rms-val-ues of the five age groups calculated only fromhigher-order aberrations (pupil size: 5 mm).The age groups I to III (age 18 to 40) revealedno statistically significant difference regardingthe rms-value but showed significantly smallerwavefront errors (p = 0.01) compared to groupIV and V (age 40 years and older).

132 M. MROCHEN et al.
cients had averages close to zero except C7 (verticalcoma) and C12 (spherical aberration) that were bothsignificantly different from zero. The statistical sig-nificance was found to be p = 0.015 (C7) and p = 0.01(C12) for a 5 mm pupil and p = 0.002 (C7) andp = 0.004 (C12) for a pupil diameter of 7 mm. On theother hand, the standard deviations were extraordi-narily higher than the averages by factors rangingfrom 5 to 42. This surprising inter-individual variabil-ity of higher order wavefront-errors is also evident inthe histogram of total wavefront error (Fig. 5). Here,the total rms-value for 5 mm pupils ranges from0.054 µm to 0.478 µm this range increased to0.137 µm to 1.324 µm in 7 mm-pupils. None of theeyes fulfilled the Marechal-criterion having an rms-wavefront error of less than λ/14 = 0.038 µm and thetotal rms-wavefront error calculated from the aver-aged Zernike coefficients was 2.1 times higher com-pared to λ/14. Only 8 out of 130 eyes of the studygroup showed a total rms-wavefront error smallerthan the total wavefront error calculated from theaveraged Zernike coefficients.
The pupil diameter accounting for a total wave-front error equal to the Marechal criterion is termedthe critical pupil diameter. Figure 6 shows the distri-bution of this critical pupil size over the investigatedeyes. The median of the critical pupil was found to be3.2 mm. Therefore, approximately 50% of normaleyes have a significant contribution of higher orderoptical aberrations at pupil diameter of more than3.2 mm.
Based on a cluster analysis the age groups listed inTable 2 were formed. Here, the age groups I to III(age 18 to 40) revealed no statistically significant dif-ference regarding the total rms-value but had signifi-cantly smaller total wavefront errors (p = 0.01) com-
pared to group IV and V (age 40 years and older) asdemonstrated in Figure 7. Analyzing the correlationsbetween age and each single Zernike coefficient (3nd
to 6th order) for 5 mm pupil sizes results in the follow-ing dependences: (1) 3rd order vertical coma C7 (R2 =–0.26, p < 0.001); (2) spherical aberration C12 (R2 =0.1, p = 0.003); (3) all other Zernike coefficients werefound to be not statistically significant correlated withage. In contrast, at 7 mm pupil size only 3rd order ver-tical coma was found to be significant related withage (R2 = –0.13, p < 0.001).
Discussion
The key finding of this paper is that the “average eye”has only minimal wavefront errors indicating that theconstruction of the human eye, in principle, providesexcellent optics exceeding the Marechal-criteriononly by a factor of 2.1 (see Fig. 4 and 5). However,such minimal aberrations are achieved in only 6% ofthe individual eyes examined in this study. We inter-pret this discrepancy by high variability of the refrac-tive surfaces of cornea and lens in each individualeye. Obviously the increase of wavefront aberrationswith age is due to age related lenticular changes lead-ing to further reduction in optical quality of the eye.More than 50% of the investigated eyes have signifi-cant higher order aberrations when their pupil size ex-ceeds 3.2 mm. Therefore, optical corrections based onsurgical procedures should include the higher orderimaging errors to achieve the best possible imagingquality of an individual eye.
Porter and coworkers (28) investigated the distri-bution of regular eye’s aberrations from 2nd to 5th
Zernike orders across a 5.7 mm pupil in 109 normalsubjects. They found, that 3rd to 5th order aberrationsaccount for about 7 % of the total imaging error in-cluding sphero-cylindrical errors. Castejon-Mochonand associates (6) reported wavefront aberrations of59 young subjects across a 5.0 mm pupil as well asWang and Koch (36) who investigated 532 eye of 306subjects. All three groups reported small “averaged”Zernike coefficients, but large intersubject variability.
The optical system of the eye consists of two mainoptical elements, the cornea and the lens. Althoughthe geometric shape of the anterior and posterior sur-faces of the cornea and lens are known to be aspheric
Table 2. Age groups of patients.
Group N Age (years)––––––––––––––––––––––––––––––––Range Mean ±SD
I 22 18 ... 22 20.0 1.6II 33 23 ... 30 25.2 1.9III 36 31 ... 40 35.6 2.2IV 22 41 ... 51 46.8 2.3V 17 52 ... 63 59.4 2.5

internal aberrations in younger and older eyes couldexplain the optical deterioration of the eye with age.
In summary, the “averaged” human provides goodoptical performance, while the wavefront aberrationsvary widely among subjects and they increase slightlywith age.
� Wellenfrontaberrationen des menschlichen�� Auges und deren Relevanz in der refraktiven�� Hornhautchirurgie
Die klassischen optischen Fehler des menschlichen Auges (Myo-pie, Hyperopie und Astigmatismus) sind für Ihren Einfluss aufdas Sehvermögen bekannt und lassen sich durch Brille, Kontakt-linse oder einen refraktiven Eingriffe korrigieren. Die optischenFehler des individuellen Auges beinhalten allerdings auch Abbil-dungsfehler höherer Ordnung, so genannte Wellenfrontaberratio-nen oder optische Aberrationen. Die bekanntesten Wellenfront-fehler sind Koma oder sphärische Aberration. Im Gegensatz zuden klassischen optischen Fehlern lassen sich solche optischenAberrationen nicht mit Brillengläsern oder Kontaktlinsen kor-rigieren. Demgegenüber haben moderne Lasersysteme für die re-fraktive Hornhautchirurgie das Potential, nicht nur die klassi-schen optischen Fehler, sondern auch die Optik des Auges durcheine Korrektur der optischen Aberrationen höherer Ordnung per-manent zu verbessern.Eine Korrektur der optischen Aberrationen durch einen chirurgi-schen Eingriff erfordert jedoch ein genaues Wissen über derenRelevanz. Im Rahmen einer klinischen Studie wurden die Wellen-frontfehler von 130 Augen von 90 Patienten gemessen. Das „mittlere“ menschliche Auge hat eine gute optische Qualität.Mit Ausnahme des vertikalen Koma und der sphärischen Aberra-tion zeigten alle gemittelten Zernike Koeffizienten keine sig-nifikante Abweichung von Null bei Pupillendurchmessern von 5und 7 mm. Jedoch fand sich kein individuelles Auge, welches dasIdeal der Beugungsbegrenzung erreichte. In allen Fällen war derrms-Wellenfrontfehler größer als das Marechal-Kriterium fürBeugungsbegrenzung. Fünfzig Prozent der untersuchten Augenhatten signifikante optische Aberrationen bei einem Pupillen-durchmesser von 3.2 mm oder größer. Dieser kritische Pupillen-durchmesser beschreibt den kleinsten Durchmesser, bei welchemdas individuelle Auge gerade noch Beugungsbegrenzung erreicht.Die statistische cluster Analyse zeigte eine signifikante Zunahmedes rms-Wellenfrontfehlers bei Patienten mit einem Alter über40 Jahre.Schlussfolgernd lässt sich sagen, dass das mittlere menschlicheAuge eine gute optische Qualität besitzt und das Marechal-Kri-terium (Beugungsbegrenzung) nur um einen Faktor 2 übersteigt.Es erreichten jedoch nur ca. 6% der untersuchten Augen einesolche optische Qualität. Somit ist das grundsätzliche Design desdurchschnittlichen menschlichen Auges als perfekte Optik an-gelegt, allerdings weicht das individuelle Auge von dieser idealenoptischen Abbildung ab. Optische Aberrationen spielen bereits abeinem Pupillendurchmesser von > 3,2 mm eine signifikante Rolleund somit reduziert sich das Sehvermögen bei größer werdender
Relevance of Wavefront Aberrations of the Human Eye in Corneal Laser Surgery 133
(8, 15). As a consequence, some of the higher orderaberrations that originate from the anterior front sur-face of the cornea might be compensated by intra-oc-ular structures.
Our group (26), among others, investigated suchcompensation mechanism. Main findings of thesestudies were that astigmatism and 3rd order opticalaberrations originate primarily from corneal shape er-rors in most of the investigated eyes. In contrast, 4th
order spherical aberrations as well as all other 4th to6th order aberrations do not correlate with the aberra-tions measured at the anterior surface of the cornea.This indicates that in a normal eye intraocular struc-tures may to a certain degree compensate for some ofthe higher order aberrations originated at the cornealfront surface. In particular, the lack of correlation be-tween corneal and total 4th order aberration might bedue to such an optical compensating mechanism.
Current laser surgery techniques aim to change theshape of the corneal front surface for correctingsphere, cylinder and also higher order aberrations ofthe eye. However, spherical aberration of the totalwavefront was found to be significantly higher in eyesafter corneal laser surgery (23, 25, 31). Especially,myopic corrections of more than –7.00 D demonstratethis effect (19) ignoring the balance between cornealand total wavefront aberrations by ablation profile cal-culation. Such ablation profiles will alter the naturaloptical balance of the eye. As a consequence, this maylead to a significant increase in total wavefront aberra-tions after a refractive procedure, if the intraocularstructures are not considered for the treatment plan-ning. Further research is required to avoid the annihi-lation of the natural optical balance between cornealand intra-ocular structures.
The amount of total aberrations in the eye increasesapproximately linearly with age (5, 10, 21, 27). Largeraberrations in the older eye produce a more degradedretinal image than in younger counterparts. Artal andassociates (2) analyzed the aberrations of the anteriorcornea and the internal optics (17 subjects) consideredas isolated systems. On the average, the aberrations ofthe cornea increase moderately with age. The aberra-tions of the internal surfaces showed a larger variabili-ty with a tendency to increase in middle-aged and old-er subjects. Neither ocular component itself appears toexplain the change in aberrations in the entire eye.Thus, only a different coupling between corneal and

Augenpupille z.B. bei Dämmerungssehen (mesopisches Sehen).Unter solchen schwachen Lichtbedingungen kann die Pupilleeinen Durchmesser von 6,0 mm oder mehr erreichen. Deshalbverwenden moderne Lasersysteme heute optische relevante Be-handlungszonen von 6.0 mm oder mehr und berücksichtigen dieoptischen Aberrationen höherer Ordnung. Sowohl Operateure alsauch Patienten sollten sich allerdings bewusst sein, dass sich dieoptischen Aberrationen mit dem Alter verändern und deshalb eineKorrektur zeitlich nicht stabil ist.
SchlüsselwörterOptische Aberrationen, Wellenfront Messungen, Tscherning Aberro-meter, physiologische Optik, Abbildungsfehler des menschlichenAuges
References
1. ARTAL P, SANTAMARIA J, BESCOS J: Retrieval of wave aberra-tion of human eyes from actual point-spread-function data. JOpt Soc Am 5/8: 1201–1206 (1988)
2. ARTAL P, BERRIO E, GUIRAO A, PIERS P: Contribution of thecornea and the internal surfaces to the change of ocular aber-rations with age. J Opt Soc Am A 19: 137–143 (2002)
3. ATCHISON DA, COLLINS MJ, WILDSOET CF, CHRISTENSEN J,WATERWORTH MD: Measurement of monochromatic ocularaberrations of human eyes as a function of accomodation bythe Howland aberroscope technique. Vision Res 35/3:313–323 (1995)
4. BORN M, WOLF E: Principles of optics. Oxford: PergamonPress (1987)
5. CALVER RI, COX MJ, ELLIOT DB: Effect of aging on themonochromatic aberrations of the human eye. J Opt Soc AmA 16(9): 2069–2078 (1999)
6. CASTEJON-MOCHON JF, LOPEZ-GIL N, BENITO A, ARTAL P:Ocular wave-front aberrations in a normal young population.Vision Res 42: 1611–1617 (2002)
7. DONDERS FC: Astigmatismus und cylindrische Glaeser. Ver-lag von Hermann Peters (1862)
8. FERNANDEZ V, MANNS F, ZIPPER S, SANDADI S, HAMAOUI M,TAHI H, HO A, PAREL J-M: Measurement of the topography ofhuman cadaver lenses using the PAR corneal topography sys-tem. SPIE Proceedings, Ophthalmic Technologies XI113–118 (2001)
9. GIBRALTER R, TROKEL SL: Correction of irregular astigma-tism with the excimer laser. Ophthalmology 101(7):1310–1314 (1994)
10. GUIRAO A, GONZALEZ C, REDONDO M, GERAGHTY E, NORRBY
S, ARTAL P: Average optical performance of the human eye asa function of age in a normal population. Invest Ophthal VisSci 40(1): 203–213 (1999)
11. GULLSTRAND A: Die Dioptrik des Auges, V. Die monochro-matischen Aberrationen des Auges. In: von Helmholtz H.Handbuch der Physiologischen Optik. 3rd edition, L. Voss,Leipzig 353–376 (1909)
12. HE JC, MARCOS S, WEBB RH, BURNS SA: Measurement ofthe wave-front aberration of the eye using a fast psychophysi-cal procedure. J Opt Soc Am 15/9: 2449–2456 (1998)
134 M. MROCHEN et al.
13. HELMHOLTZ H: Handbuch der physiologischen Optik.Leipzig, Leopold Voss 137–147 (1867)
14. HOWLAND HC, HOWLAND B: A subjective method for themeasurement of monochromatic aberrations of the humaneye. J Opt Soc Am 67/11: 1508–1518 (1977)
15. KIELY PM, SMITH G, CARNEY LG: The mean shape of the hu-man cornea. Optica Acta 29: 1027–1040 (1982)
16. LIANG J, WILLIAMS DR: Aberrations and retinal image qualityof the normal human eye. J Opt SocAm 14/11: 2873–2883(1997)
17. LIANG J, WILLIAMS DR, MILLER DT: Supernormal vision andhigh-resolution retinal imaging through adaptive optics. JOpt Soc Am 14: 2884–2892 (1997)
18. MAHAJAN VN: Aberration theory made simple – Part II. SPIEOptical Engineering press (1991)
19. MANNS F, HO A, PAREL J-M: Calculation of the primaryspherical aberration of an eye model using paraxial ray-trac-ing with matrix optics. SPIE Proceedings, Ophthalmic Tech-nologies XI 57–65 (2001)
20. MARECHAL A: Etude des effets combines de la diffraction etdes aberrations geometriques sur L’image d’un point lu-mineux. Revue d’optique 257–277 (1947)
21. MCLELLAN J, MARCOS S, BURNS SA: Age-Related Changesin Monochromatic Wave Aberrations of the Human Eye. In-vest Ophthal Vis Sci 42: 1390–1395 (2001)
22. MIERDEL P, WIEGAND W, KRINKE HE, KAEMMERER M, SEILER
T: Measuring device for determining monochromatic aberra-tion of the human eye. Ophthalmologe 6: 441–445 (1997)
23. MORENO-BARRIUSO N, MERAYO LLOVES J, MARCOS S,NAVARRO R, LLORENTE G, BARBERO S: Ocular Aberrationsbefore and after myopic corneal refractive surgery: LASIK-induced changes measured with Laser Ray Tracing. InvestOphthal Vis Sci 42: 1396–1403 (2001)
24. MROCHEN M, KAEMMERER M, SEILER T: Wavefront-guidedLaser in situ keratomileusis: Early results in three eyes. J Re-fract Surg 16: 116–121 (2000)
25. MROCHEN M, KAEMMERER M, SEILER T: Clinical results ofwavefront-guided LASIK at 3 months after surgery. JCataract Refract Surg 27: 201–207 (2001)
26. MROCHEN M, JANKOV M, BUEELER M, SEILER T: Correlationbetween corneal and total wavefront aberrations in myopiceyes. J Refract Surg 19: 104–112 (2003)
27. OSHIKA T, KLYCE SD, APPLEGATE RA, HOWLAND HC:Changes in corneal wavefront aberrations with aging. InvestOphthal Vis Sci 40(7): 1351–1355 (1999)
28. PORTER J, GUIRAO A, COX IG, WILLIAMS DR: Monochromaticaberrations of the human eye in a large population. J Opt SocAm A 1793–1803 (2001)
29. SANTAMARIA J, ARTAL P, BESCOS J: Determination of thepoint-spread function of human eyes using a hybrid optical-digital method. J Opt Soc Am 4/6: 1109–1114 (1987)
30. SEILER T, GENTH U, HOLSCHBACH A, DERSE MSO: Asphericphotorefractive keratectomy with excimer laser. RefractCorneal Surg 9: 166–172 (1993)
31. SEILER T, KAEMMERER M, MIERDEL P, KRINKE H-E: Ocular op-tical aberrations after photorefractive keratectomy for myopiaand myopic astigmatism. Arch Ophthalmol 118: 17–21 (2000)

Relevance of Wavefront Aberrations of the Human Eye in Corneal Laser Surgery 135
32. THIBOS LN, APPLEGATE RA, SCHWIEGERLING JT, WEBB R:Standards for Reporting the Optical Aberrations of Eyes. In:McRae S, Applegate RA, Krueger R: Cutomized Corneal Ab-lation. The Quest for Super Vision. SLACK Inc. Thorofare,NJ, 348–361 (2001)
33. TSCHERNING M: Die monochromatischen Aberrationen desmenschlichen Auges. Z Psychol Physiol Sinne 6: 456–471(1894)
34. VOLKMANN AW: Sehen. In: Wagner R. ed, Handwörterbuch derPhysiologie III. Vieweg und Sohn, Braunschweig, 289–293(1846)
35. WALSH G, CHARMAN WN, HOWLAND HC: Objective tech-nique for determination of monochromatic aberrations of thehuman eye. J Opt Soc Am 1/9: 987–992 (1984)
36. WANG LI, KOCH DD: Ocular higher-order aberrations in indi-viduals screened for refractive surgery. J Cataract RefractSurg 29: 1896–1903 (2003)
37. ZERNIKE F: Beugungstheorie des Schneidenverfahrens undseiner verbesserten Form der Phasenkontrastmethode. Physi-ca I 2: 689–704 (1934)
Correspondence address:Dr. Michael Mrochen, Institute of Biomedical Engineering, SwissFederal Institute of Technology, Gloriastrasse 35, CH-8092 Zurich,Switzerland;Tel.: ++41-1-632 4583; Fax: ++41-1-632 1193; e-mail: [email protected]