renal function with lvads
TRANSCRIPT

KIDNEYS VS LVADS:
CAN WE WORK
TOGETHERRenal Grand
Rounds
Ahad Lodhi
Disclosure:
• None of my financial holdings influence this presentation
directly or indirectly.

Outline:
• Problem & need
• Basic types of VADs (Ventricular assist devices)
• Preimplantation/Baseline renal function and outcomes
• Continuous flow VADs and renal function
• AKI post VAD
• Improvement in renal function post VAD
• RRT in VAD patient
• Modalities
• Access
• BP monitoring
• Pump speed, Flow, Pulsatility Index

Outline:
• Problem & need• Basic types of VADs (Ventricular assist devices)
• Peri-implantation/Baseline renal function and outcomes
• Continuous flow VADs and renal function
• AKI post VAD
• Improvement in renal function post VAD
• RRT in VAD patient
• Modalities
• Access
• BP monitoring
• Pump speed, Flow, Pulsatility Index
Problem:
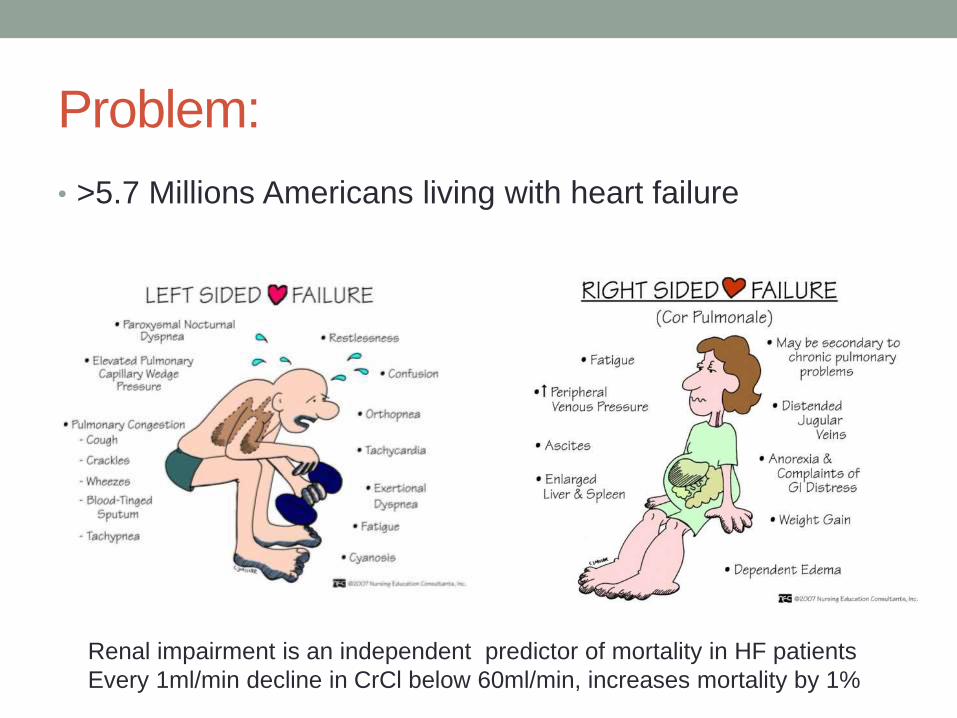
• >5.7 Millions Americans living with heart failure
Renal impairment is an independent predictor of mortality in HF patients
Every 1ml/min decline in CrCl below 60ml/min, increases mortality by 1%

Problem
44% CKD 3
14% CKD 4
7% CKD 5

Need for LVADs
• >50% mortality in advanced heart failure
• <3000 donors available per year
• LVADs provide improved survival in advance heart failure
• BTT (bridge to transplant) FDA approved
• DT (destination therapy) FDA approved
• BTR (bridge to recovery)
• Biventricular devices as BTT or BTR
• INERMACS (Interagency Registry for Mechanical
Assisted Circulatory Support)- 4311 LVADs June 2006-
Sept 2011 (1500/yr)

LVADs provide improved survival in
advance heart failure
• REMATCH Trial (2001): , 52% vs 25% at 1 yr
• Recent Trials (Starling et al 2011, Park et al 2012) survival
rates 73% DT and 85% BTT
Outline:
• Problem & need
• Basic types of VADs (Ventricular assist devices)
• Preimplantation/Baseline renal function and outcomes
• Continuous flow VADs and renal function
• AKI post VAD
• Improvement in renal function post VAD
• RRT in VAD patient• Modalities
• Access
• BP monitoring
• Pump speed, Flow, Pulsatility Index

Types
• Pulsatile devices (First Gen)
• Thoratec Paracorporeal, Thoratec implantable, Heartmate Vented
• Chambers filled with blood and pneumatic mechanism emptying
the chambers via one way valve
• Continuous Flow devices
• Newer
• Axial and centrifugal flow design
• HeartMate 2, Jarvik 2000, HeartWare
• Smaller, quiter, less thrombogenic, improved survival, less
arrhythmias, less Rt HF and Resp failure.
• 95% of all LVADs Jan 2010-June 2011 (INTERMACS)
4 min Videos (2+2)
• Heartware
• http://youtu.be/v8aIeoHXTMw
• HeartMate 2
• http://youtu.be/YBxDhUzSrsk
Outline:
• Problem & need
• Basic types of VADs (Ventricular assist devices)
• Preimplantation/Baseline renal function and outcomes
• Continuous flow VADs and renal function
• AKI post VAD
• Improvement in renal function post VAD
• RRT in VAD patient• Modalities
• Access
• BP monitoring
• Pump speed, Flow, Pulsatility Index

Preimplantation/Baseline renal function
and outcomes• Early studies with pulsatile flow associated high mortality
(75-100%) with preimplantation Renal dysfucntion.
• Recent with continuous flow:
• Sander et al, reported improved survival (1-3-6month) and
BTT rates when preimplantation gfr >60ml/min/1.73m2
• Yoshioka et al reported 30day, 90 day and 1 yr survivals
of 96%, 88% and 77% when Cr is <1.96 mg/dL
• Iwashima et all, suggest 2 week post-implantation gfr of
>82ml/min is stronger predictor of survival
• Intrinsic renal disease associated with worst outcomes.
Outline:
• Problem & need
• Basic types of VADs (Ventricular assist devices)
• Preimplantation/Baseline renal function and outcomes
• Continuous flow VADs and renal function
• AKI post VAD
• Improvement in renal function post VAD
• RRT in VAD patient• Modalities
• Access
• BP monitoring
• Pump speed, Flow, Pulsatility Index

Continuous flow VADs and renal function
• Still some pulsatility due to intrinsic LV function
• Increased diastolic pressure and decreased peak systolic
pressure and increased laminar flow, ? More stasis distal
to atherosclerotic lesions ? Cortical blood flow
• Animal studies : renal arterial smooth muscle hyperplasia,
peri-arterial inflammatory cells, Inc PRA, inc Ang 2 recp
and ACE.
• Hasin et al, Initial improvement in gfr (53-87) , later stable
or slow decline?
• Greater decline in renin & aldosterone levels with pulsatile
flow, long term implications?
Outline:
• Problem & need
• Basic types of VADs (Ventricular assist devices)
• Preimplantation/Baseline renal function and outcomes
• Continuous flow VADs and renal function
• AKI post VAD• Improvement in renal function post VAD
• RRT in VAD patient
• Modalities
• Access
• BP monitoring
• Pump speed, Flow, Pulsatility Index
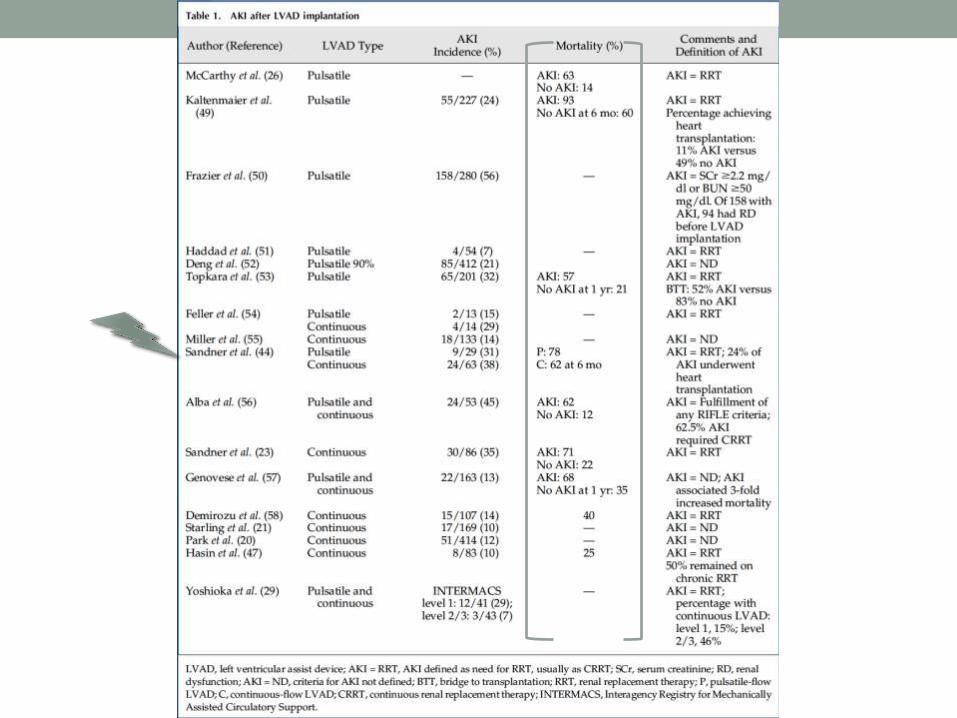
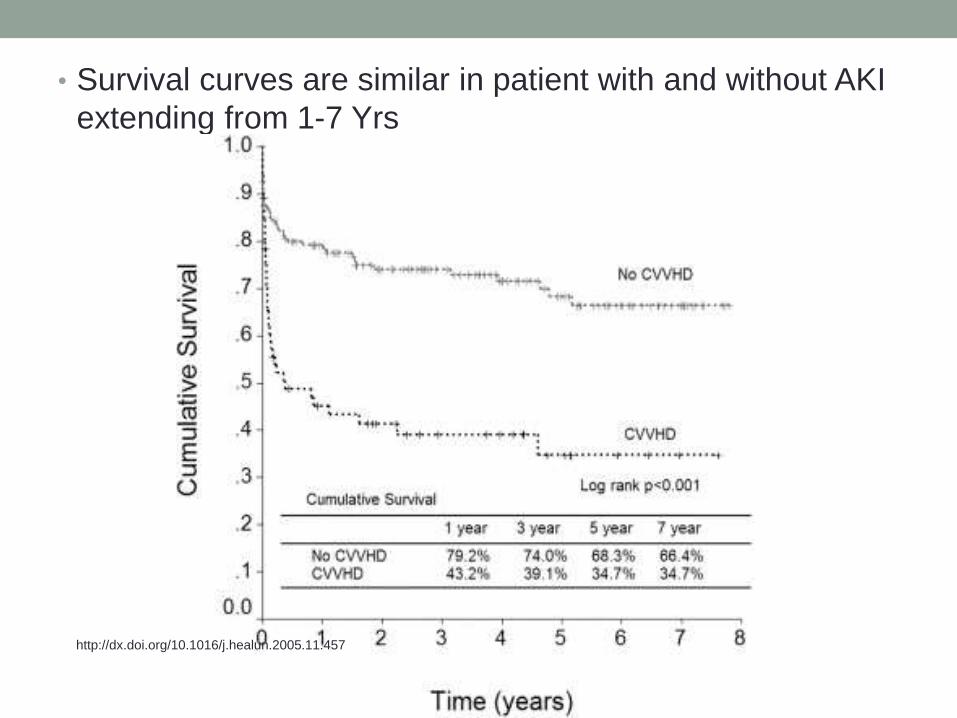
• Survival curves are similar in patient with and without AKI
extending from 1-7 Yrs
http://dx.doi.org/10.1016/j.healun.2005.11.457
Outline:
• Problem & need
• Basic types of VADs (Ventricular assist devices)
• Preimplantation/Baseline renal function and outcomes
• Continuous flow VADs and renal function
• AKI post VAD
• Improvement in renal function post VAD• RRT in VAD patient
• Modalities
• Access
• BP monitoring
• Pump speed, Flow, Pulsatility Index

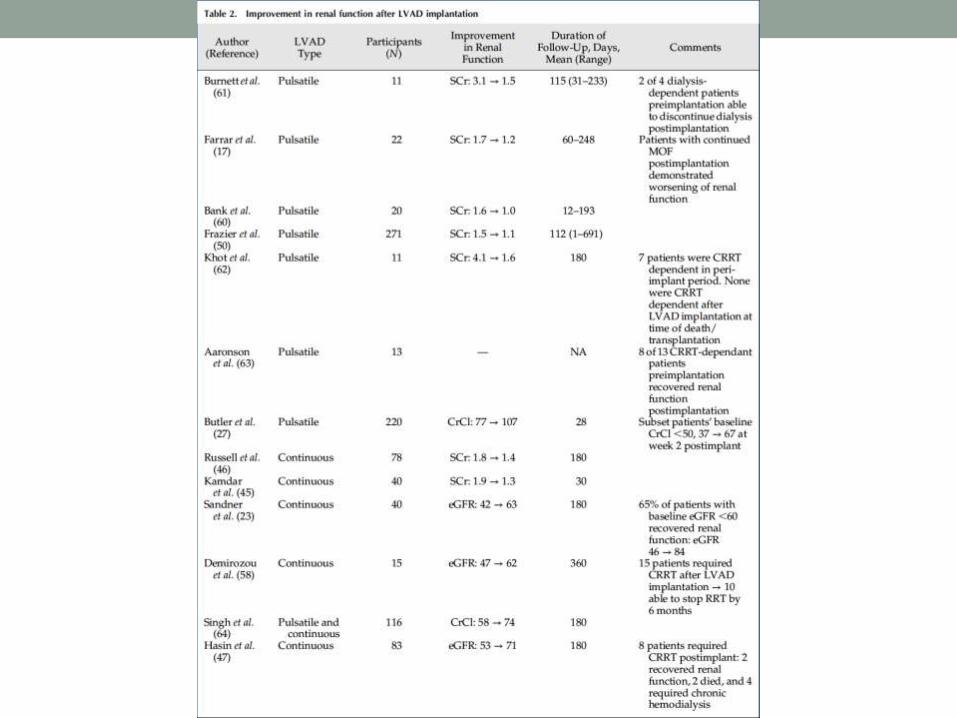
Improvement in renal function post VAD
• Due to? Improved flow, decrease congestion—dec
resistance, Dec activation of RAAS and sympathetic
systems.
• Improvement has been reported in upto 74% of patients
with baseline CKD…….how severe, acute or chronic
• Those who improve have better survival
• Patients who recover post-implant vs Pt without
dysfunction preimplant: no difference in survival curves, at
6 months, until transplanted and 1 yr post Txp.
• Patients with baseline chronic RD and diabetics are less
likely to recover significant renal function
Factors
• Pre-existing RD, various causes including HTN
• ongoing severe disease with MOF,
• residual damage from AKI,
• Renovascular Dz (atheroembolic)
• DM
• long standing low flow state
Effects Txp eligibility (can improve or worsen)
Use of CNIs
RRT IN LVAD PATIENTS
Modality:
• In acute settings: CRRT, once hemodynamically stable
can transition to IHD.
• PD:
• was not possible in older devices were large and were also
sometimes, implanted in peritoneal cavity or abd wall. Peritonitis
can be life threatening in this situation.
• Devices casuing hernia, bowel obs and erosion
• New devices can be implanted intra-pericardial or pre-peritoneal
• Gentle UF, less risk of bacteremia and device contamination and
it’s a home modality.
• Placing LVADs for in-center HD is a challenge in itself.

Vascular access
• All opinions and no Data:
• Suggest using ultrasound doppler to access patency in
both kind of AV access due to lack of pulsatile flow hence
lack of or poor bruit and thrill
• Most have suggested to use AV grafts as long as patient
is on LVAD.
• Does not need to mature and can be used very early, hence not
requiring catheter and risking bacteremia—pericardial and device
infection.
• AVFs need maturation , very poor maturation due to lack of
pulsatile flow.
• Usually less thrombosis as these patients are maintained on
systemic anticoagulation.

BP monitoring
• Difficult to use standard techniques and standard
automated devices (usually read if PP >15mmg,
oscillometric, significantly lower than arterial)
• Pulse Pressure in LVAD: Pump speed, native function,
Aortic valve stiffness, pre/afterloads.
• Doppler audible USG: Deflate the cuff, start of blood flow,
heard by Doppler, usually is the mean arterial BP
• High BP—increased afterload– retrograde flow through
valveless system—bad
• Optimal MAP 70-80mmHg
• Avoid –ve inotropes, first target RAAS

Pump Speed
• Rate of revolution, usually 8000 to 10000rpm
• Increase pump speed, incvacuum effect on left ventricle, faster and complete unloading & collapse of left V and even left atrium—not enough LVEDP to open aortic valve---Prolonged AV closure---stasis/Clot—also lead to coronary thrombosis
• Hemolysis, Platelet activation, septal shift to left with dec RVF
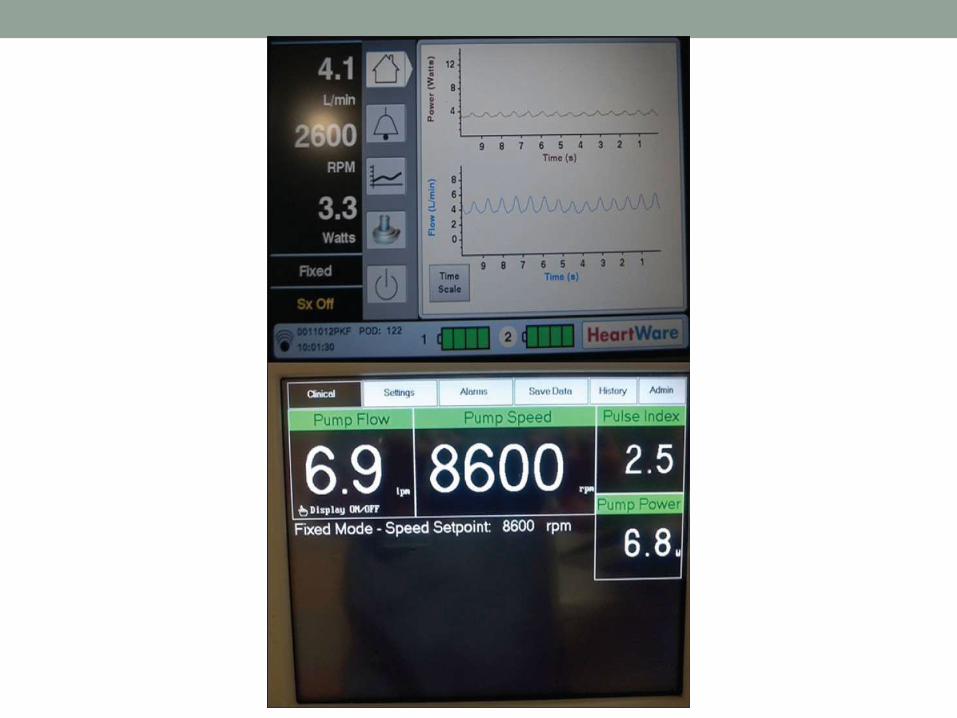
Pump Flow
• Flow 3-10L/min = cardiac output
• Derived from speed

Pulsatility Index
• Pulsatility of blood flow through the LVAD
• Depends on native LV function (contractility and flow)---
which depends on * preload & * pump speed.
• It can serve as an indicator for UF during CRRT.
• More UF, decrease preload, decreased PI, increase LVAD support
needed to maintain flow.
• It can be considered a surrogate marker for LVAD support
provided to maintain cardiac out put.
• Poor native LVF, decreased PI, increased LVAD support needed to
maintain flow and vice versa.
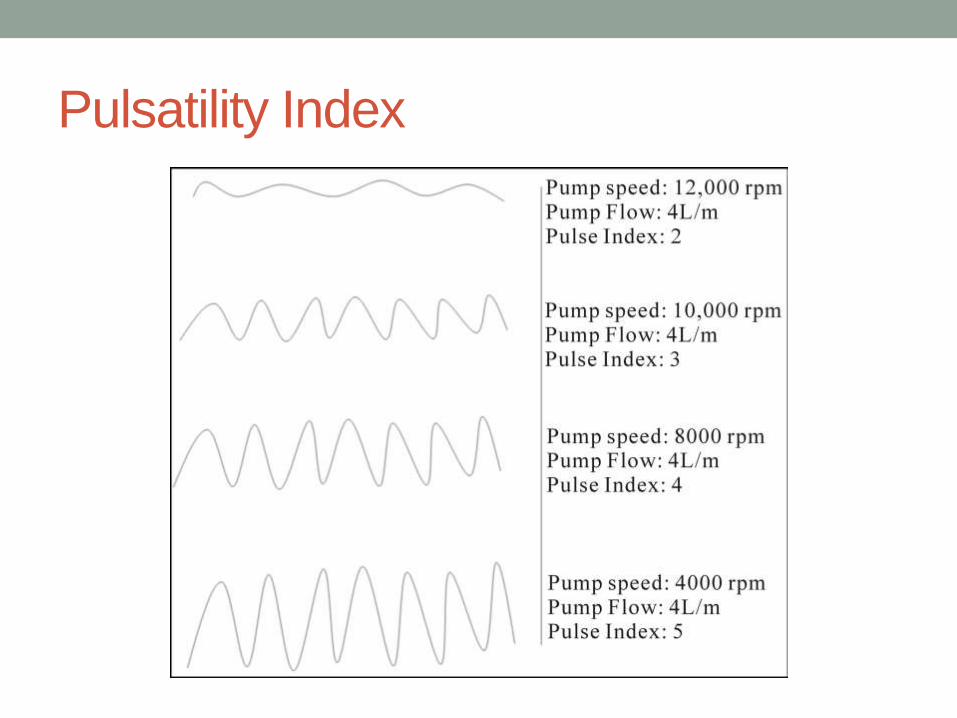
Pulsatility Index


Others
• Hemolysis/TMA
• Anticoagulation
• Bleeding.