renal replacement therapy for intoxications timothy e. bunchman pediatric nephrology &...
TRANSCRIPT

Renal Replacement Therapy for Intoxications
Timothy E. Bunchman Timothy E. Bunchman
Pediatric Nephrology & TransplantationPediatric Nephrology & Transplantation
DeVos Children’s HospitalDeVos Children’s Hospital
Grand Rapids, MIGrand Rapids, MI
(thanks to Pat Brophy for his help and (thanks to Pat Brophy for his help and some slides) some slides)

Before we get going remember
Looking at therapeutic medications or Looking at therapeutic medications or intoxications there is an intoxications there is an Absorption process Absorption process
&& An elimination/metabolism processAn elimination/metabolism process

What is unique to Pediatric Intoxications? Vehicle in which the medication was Vehicle in which the medication was
delivereddelivered Metabolism of drug Metabolism of drug Volume of distributionVolume of distribution Variable size of the childVariable size of the child

Vehicle in which drug was administered
Oral liquid/mucosal absorptionOral liquid/mucosal absorption Rapid absorption fixed metabolismRapid absorption fixed metabolism
Short acting pill formShort acting pill form Slower absorption, fix metabolismSlower absorption, fix metabolism
Long acting pill formLong acting pill form Slowest absorption, fix metabolismSlowest absorption, fix metabolism

Drug absorption in a child
0
10
20
30
40
50
60
0 2 4 6 12
liquidshort acting pilllong acting pill

CSA metabolism varies with Age
0
100
200
300
400
500
600
700
0 2 4 8 12 24
adultchildinfant

Intoxications
2.2 million reported 2.2 million reported poisonings (1998) poisonings (1998)
• 67% in pediatrics67% in pediatrics
• Approximately 0.05% Approximately 0.05% required extracorporeal required extracorporeal elimination elimination

Kearns, G. L. et. al. N Engl J Med 2003;349:1157-1167
Developmental Changes in Physiologic Factors That Influence Drug Disposition in Infants, Children, and Adolescents

PHARMOCOKINETIC COMPARTMENTS
kidneybloodPeripheralliverGI TractDistribution Re-distribution
INPUT
ELIMINATION
A. J ör res 02/2001A. J ör res 02/2001
Factors affecting clearance
Delivery of drug to hemofilterDelivery of drug to hemofilter Blood flow, volume of distribution Blood flow, volume of distribution
(Vd)(Vd) Drugs unique ultrafiltration propertiesDrugs unique ultrafiltration properties Mol. Wt., Chemical structure, drug-Mol. Wt., Chemical structure, drug-
membrane interaction, protein membrane interaction, protein bindingbinding
Ultrafiltration rateUltrafiltration rate
Protein bindingProtein binding
Golper TA et al, Int J Art Organs, 1985

Extracorporeal MethodsExtracorporeal Methods• Peritoneal DialysisPeritoneal Dialysis• HemodialysisHemodialysis• HemofiltrationHemofiltration• Charcoal hemoperfusionCharcoal hemoperfusion
– No longer needed (historical No longer needed (historical perspective)perspective)
• HD followed by HFHD followed by HF

INDICATIONSINDICATIONS
>48 hrs on vent>48 hrs on vent ARFARF Impaired metabolismImpaired metabolism high probability of high probability of
significant significant morbidity/mortalitymorbidity/mortality
progressive clinical progressive clinical deterioration deterioration
INDICATIONSINDICATIONS severe intoxication severe intoxication
with abnormal vital with abnormal vital signs signs
complications of complications of coma coma
prolonged coma prolonged coma intoxication with an intoxication with an
extractable drugextractable drug

PERITONEAL DIALYSISPERITONEAL DIALYSIS 1st done in 1934 for 2 anuric patients after 1st done in 1934 for 2 anuric patients after
sublimate poisoning sublimate poisoning (Balzs et al; Wien Klin Wschr 1934;47:851 )(Balzs et al; Wien Klin Wschr 1934;47:851 )
Allows diffusion of toxins across peritoneal Allows diffusion of toxins across peritoneal membrane from mesenteric capillaries into membrane from mesenteric capillaries into dialysis solution within the peritoneal cavitydialysis solution within the peritoneal cavity
limited use in poisoning (clears drugs with low limited use in poisoning (clears drugs with low Mwt., Small Vd, minimal protein binding & those Mwt., Small Vd, minimal protein binding & those that are water soluble) that are water soluble) alcohols, NaCl intoxications, salicylatesalcohols, NaCl intoxications, salicylates

HEMODIALYSISHEMODIALYSIS optimal drug characteristics for removal:optimal drug characteristics for removal:
relative molecular mass < 500 relative molecular mass < 500 water solublewater solublesmall Vd (< 1 L/Kg)small Vd (< 1 L/Kg)minimal plasma protein bindingminimal plasma protein bindingsingle compartment kineticssingle compartment kinetics low endogenous clearance (< 4ml/Kg/min)low endogenous clearance (< 4ml/Kg/min)
– (Pond, SM - Med J Australia 1991; 154: (Pond, SM - Med J Australia 1991; 154: 617-622)617-622)

Hemodialysis: Nl vs High Flux
Normal is a smaller pore size (12 Kda) and Normal is a smaller pore size (12 Kda) and dialysate runs at ~ 30 l/hrdialysate runs at ~ 30 l/hr
High flux is larger pore size (up to 50 Kda) High flux is larger pore size (up to 50 Kda) and runs dialysate at ~ 50 l/hrand runs dialysate at ~ 50 l/hr

Hemofiltration use for intoxications (primary or tandem) Hemofiltration allows for continuous Hemofiltration allows for continuous
therapy at bedside 24 hrs a daytherapy at bedside 24 hrs a day Can be Convective (CVVH), Diffusive Can be Convective (CVVH), Diffusive
(CVVHD), or combination (CVVHD)(CVVHD), or combination (CVVHD) CVVHD does not add significantly to what CVVHD does not add significantly to what
can be done with maximizing CVVH or can be done with maximizing CVVH or CVVHD aloneCVVHD alone

A. J ör res 02/2001A. J ör res 02/2001
Filtration vs. Dialysis
Filtration:Clearance by
convection
Dependent on UFR and
sieving coefficient
Dialysis:Clearance by diffusion
Dependent on concentration
gradient

CVVH/CAVHCVVH/CAVH Convective clearanceConvective clearance Replacement SolutionsReplacement Solutions
Physiologic sterile Physiologic sterile solution that is either solution that is either infused pre filter or infused pre filter or post filter that post filter that infused at a set rate infused at a set rate (Qr)(Qr)
CAVH/CVVH: Convective Clearance

CAVHD/CVVHDDiffusive Clearance
CVVHD/CAVHDCVVHD/CAVHD Diffusive clearanceDiffusive clearance DialysateDialysate
Physiologic sterile Physiologic sterile solution that is infused solution that is infused countercurrent to the countercurrent to the blood flow rate (Qd)blood flow rate (Qd)

Sieving Coefficients
Solute (MW) Convective Coefficient Diffusion Coefficient
Urea (60) 1.01 ± 0.05 1.01 ± 0.07
Creatinine (113) 1.00 ± 0.09 1.01 ± 0.06
Uric Acid (168) 1.01 ± 0.04 0.97 ± 0.04*
Vancomycin (1448) 0.84 ± 0.10 0.74 ± 0.04**
Cytokines (large) adsorbed minimal clearance
*P<0.05 **P<0.01

Dialysis Dose
0123456789
10W
eek
ly s
tdK
t/V
0.3 0.5 0.7 0.9 1.1 1.3 1.5
eKt/V each dialysis
234567
No. of D
ays/week
EDDEDD
35ml/kg35ml/kg
45ml/kg45ml/kg
20ml/kg20ml/kg
Adapted from Gotch et al. Kidney Int 2000;58:S3-18Adapted from Gotch et al. Kidney Int 2000;58:S3-18
CRRTCRRT
PD

So for any clearance moment to moment High (flux) efficiency HD > standard HD > High (flux) efficiency HD > standard HD >
CVVH > CVVHD > PDCVVH > CVVHD > PD Thought process of acute RRT needs to Thought process of acute RRT needs to
ensure that pt does not become ensure that pt does not become hypophosphatemic, hypokalemic, etchypophosphatemic, hypokalemic, etc Electrolyte components can be added to Electrolyte components can be added to
the dialysate “bath”the dialysate “bath”

Intoxicants amenable to HemodialysisIntoxicants amenable to Hemodialysis alcoholsalcohols
ethylene glycolethylene glycolMethanolMethanol
• (beware that one does not clear the rescue (beware that one does not clear the rescue drug)drug)
vancomycin (high flux)vancomycin (high flux) Highly protein bound seizure drugsHighly protein bound seizure drugs lithiumlithium salicylatessalicylates

A good Friday night
Teens deciding that beer was to expensive Teens deciding that beer was to expensive so they went for anti-freeze insteadso they went for anti-freeze instead
Had metabolic acidosis and osmolar gapHad metabolic acidosis and osmolar gap Before use of (fomepizol) treated with IV Before use of (fomepizol) treated with IV
alcohol and dialysis (may clear rescue drug)alcohol and dialysis (may clear rescue drug) Alcohols are in general small molecular wt Alcohols are in general small molecular wt
poorly protein boundpoorly protein bound

Ethylene Glycol IntoxicationRx with (std) Hemodialysis
0
100
200
300
400
500
600
700
800
900
0 2 4 6
Pt 1Pt 2
Duration of Rx (hrs)
Mg/
ml
(> 3
0 m
g/m
l tox
ic)

A bad Friday night
If a little vancomycin is good a lot is betterIf a little vancomycin is good a lot is better Historically thought to be poorly dialyzable Historically thought to be poorly dialyzable
but with High efficient membrane clears but with High efficient membrane clears easilyeasily
Senario is in children with reduction in Senario is in children with reduction in GFR dosed based upon nl GFRGFR dosed based upon nl GFR
Has a 2 compartment distributionHas a 2 compartment distribution

Vancomycin clearance High efficiency dialysis membrane
0
50
100
150
200
250
0 3 12 15 27 30
Pt 1Pt 2
Time of therapy
Van
c le
vel
(m
ic/d
l)
Rx Rx Rx
Rebound Rebound
A fun Friday night
Highly protein bound anti-seizure meds Highly protein bound anti-seizure meds thought to be only cleared by CHPthought to be only cleared by CHP
CHP is where one removes blood from the CHP is where one removes blood from the pt, filters thru a charcoal filter, goes to a pt, filters thru a charcoal filter, goes to a dialysate membrane back to the ptdialysate membrane back to the pt
Problem with CHP, large extracorporeal Problem with CHP, large extracorporeal circuit, cold, hypocalcemic, coagulopathic..circuit, cold, hypocalcemic, coagulopathic..
essentially “they get ugly”essentially “they get ugly”

0
5
10
15
20
25
30
35
0 5 10 15 20 25 30 35 40
CBZ level(nl < 12;76%proteinbound))
High flux hemodialysis for Tegretol Intoxication
HD Rx
Hrs from time of ingestion
Mic
/ml
2 compartment rebound

Tandem therapies: prevention of the rebound If one has a rapid generation rate or a large If one has a rapid generation rate or a large
volume of distribution consider tandem volume of distribution consider tandem therapiestherapies
HD for rapid removal followed by HF for HD for rapid removal followed by HF for prevention of the reboundprevention of the rebound
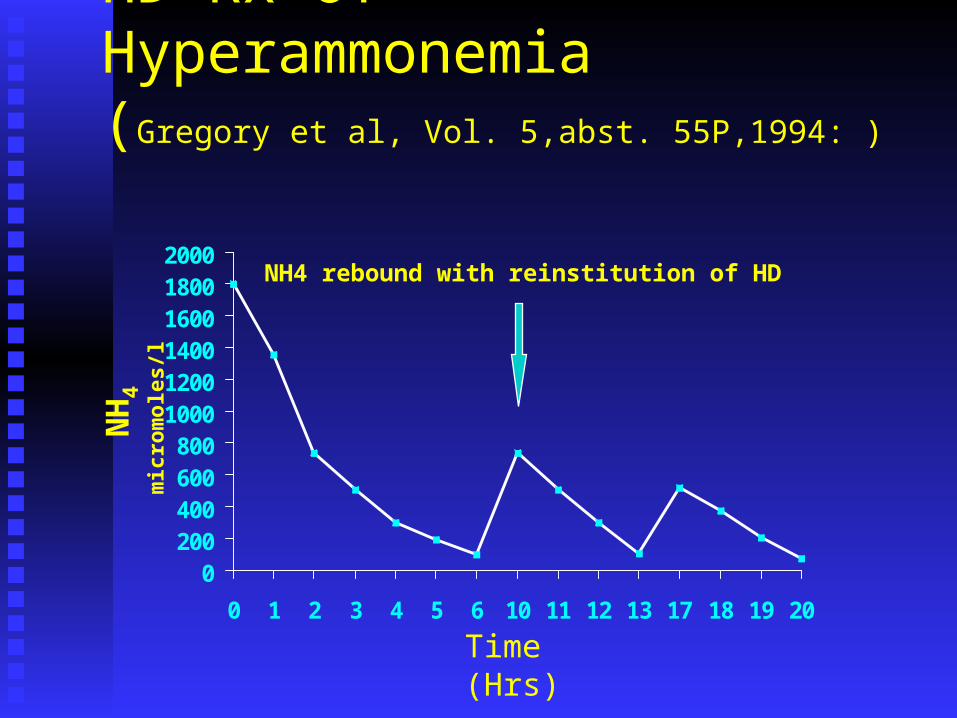
HD Rx of Hyperammonemia(Gregory et al, Vol. 5,abst. 55P,1994: )
0200400600800
100012001400160018002000
0 1 2 3 4 5 6 10 11 12 13 17 18 19 20
N
H4
mic
rom
oles
/l
Time(Hrs)
NH4 rebound with reinstitution of HD

HD to CRRT(prevention of the rebound)
0
200
400
600
800
1000
1200
0 1 2 3 4 5 10 11 17
Time (Hrs)
N
H4
mic
rom
oles
/L Transition from HD to CVVHD

Tandem TherapiesHD to HF
0
1
2
3
4
5
6Pt #1Pt #2
Hours
Li
mEq/ L
CVVHD following HD for Lithium poisoning
HD started
CVVHD started CT-190 (HD)Multiflo-60both patientsBFR-pt #1 200 ml/minHD & CVVHD -pt # 2 325 ml/minHD & 200 ml/min
CVVHDPO4 Based dialysate at
2L/1.73m2/hr
Li Therapeutic range0.5-1.5 mEq/L

Summary
RRT can be an adjunct to normal RRT can be an adjunct to normal elimination of drug or a substitution of drug elimination of drug or a substitution of drug removal (with concomitant ARF)removal (with concomitant ARF)
RRT therapies are safe RRT therapies are safe RRT machines are “pediatric friendly”RRT machines are “pediatric friendly” HF HD > HF > CVVH > CVVHD HF HD > HF > CVVH > CVVHD No role for PDNo role for PD

Summary
Tandem therapies allow for rapid and Tandem therapies allow for rapid and sustaining removal of drugs with prevention sustaining removal of drugs with prevention of rebound…of rebound…
Vascular access already in placeVascular access already in place Early consideration of RRT Early consideration of RRT

Conclusion
…………..if you can measure it, ..if you can measure it, we can clear it…we can clear it…