report final eng 17.08 - world health...
TRANSCRIPT
UNFPA Country Office/Mongolia, UN House, 12 United Nations Street, Ulaanbaatar
Tel: + (976) 11-323365, + (976) 11-353501
J O I N T U N F PA / W H O M I S S O N I N C O L L A B O R AT I O N W I T H T H E M I N I S T RY O F
H E A LT H T O R E V I E W T H E C U R R E N T S TAT U S O F AC C E S S T O A C O R E S E T O F
C R I T I C A L , L I F E - S AV I N G M AT E R N A L / R E P RO D U C T I V E H E A LT H M E D I C I N E S
I N M O N G O L I A
1 8 J U N E – 0 3 J U LY 2 0 0 9
U N F P A / M O N G O L I A

2
T A B L E O F C O N T E N T S
Page
Acknowledgements 3 Executive Summary 4 Chapter 1. Context and Background 9 Chapter 2. Key Findings and Action Recommendations
1. Need and Demand 10 2. Essential Medicine List 11 3. Availability of Critical RH Medicines 12 4. Standard Treatment Guidelines/Protocols 15 5. Rational Use of Critical RH Medicines 17 6. Quality Assurance 17 7. Storage 19 8. Procurement and Supply Chain Management 20 9. Costs 22 10. Coordination/Integration 24
Chapter 3. Conclusion and Recommendations 27
Annexes
A. Terms of Reference 28 B. Mission Schedule 31 C. List of People Met 35 D. Key Documents Reviewed 39 E. Checklists (Health Facility; Medical Stores/Pharmacies;
Product Specific; Procurement) 40 F. List of Acronyms 49 G. Map of Mongolia 51 H. Organizational Structure of MOH 52 I. List of People Attended/Participated in Final Debriefing Session 53

3
ACKNOWLEDGEMENTS
The Mission Team would like to express its gratitude to Dr. J. Tsolmon, Vice Minister of Health, Ms. Ch. Munkhdelger, Head of Division for Medicine and Medical Devices, Dr. Ts. Sodnompil, Director of Department of Health, GIA of MOH, Mr. Gunibazar, Vice Director, the State General Inspection Agency and Heads of Departments of Health of Ulaanbaatar, Bulgan, Khentii, Orkhon aimags. Also our gratitude to all those dedicated staff members serving the peoples in Mongolia in the hospitals, other health facilities, pharmacies and stores, private sector representatives, professional associations and the communities that we have visited during this mission The team would also like to acknowledge the assistance of other developmental partners, especially WHO Geneva and Country Office in Mongolia; UNICEF, Mongolia office, JICWELS, ADB, MSI, MFWA and other civil society organizations in Mongolia whose ideas; experience, inputs and reports were valuable to this mission (Detailed lists in Annex: C). Special thanks are also extended to the UNFPA Mongolia Country Office Representative Mr. Jose Ferraris and other staff for the assistance in organizing this mission; colleagues from the UNFPA Asia Pacific Regional Office in Bangkok and Commodity Security Branch (CSB) in New York for their technical support and encouragement. Without the support and contribution of the aforementioned groups, agencies, and individuals, this report would not have been possible. Team Members: Dr. Kabir U Ahmed, UNFPA, New York Dr. Anna Ridge, WHO, Geneva Dr.Buyanjargal Ya, MOH, Mongolia Ms. Amarjargal Ch, MOH, Mongolia Dr. Govind Salik, WHO, Mongolia Dr. Tsevelmaa B, UNFPA, Mongolia Dr.Enkhjargal Kh, UNFPA, Mongolia Mr. Kang Nam Il, Population Centre, DPRK Dr. Altantuya D, State Inspectorate Agency Dr. Kim Kwang Jin, Population Centre, DPRK Dr.Yanjinsuren D, Lecturer, HSUM Dr. Daariimaa Kh, Lecturer, HSUM Ms. Enkhmaa Ts, UNFPA, Mongolia Dr. Bold A, National Consultant, UNFPA
4
Executive Summary
In an effort to improve access to quality essential Reproductive Health (RH) medicines and medical devices, WHO, UNFPA and partners in the Reproductive Health Supply Coalition (RHSC) are engaged in a series of activities aimed at promoting harmonized global standards and technical assistance. These include developing guidance on sourcing good quality suppliers and products, building procurement capacity in resource-limited countries, and removing barriers to the appropriate use of these products. A well-functioning supply chain capable of selecting, forecasting, quantifying, financing, procuring, and delivering the medicines and related medical devices and consumables needed is a critical element in all efforts to improve the health and well-being of mothers and children in developing countries. Delivering goods alone is not sufficient to ensure better outcomes for those who benefit from RH programmes. RH Commodity Security (RHCS) is essential to meeting the target of universal access to reproductive health by 2015, as called for by the International Conference on Population and Development and the Millennium Development Goals. The purpose of this mission was to present a “snapshot” of the current status of access to medicines for Maternal and Newborn Health Care and Reproductive Health, which are not routinely monitored. The findings of this mission are intended to supplement the findings of other on-going studies and studies planned for the very near future. The six critical RH medicines chosen for the study were Oxytocin injection, Ergometrine injection, Magnesium Sulphate injection and three antibiotics, Ampicillin injection, Gentamicin injection and Metronidazole injection. These medicines were chosen because they are the WHO recommended medicines for the prevention and management of three major causes of Maternal Mortality:
• Haemorrhage (Oxytocin, Ergometrine injections) • Eclampsia, pre-eclampsia (Magnesium Sulphate injection) • Maternal/Neonatal Sepsis (Ampicillin, Gentamicin and Metronidazole injections)
The main objectives of the mission were to conduct a pragmatic exploratory study to:
1. Obtain a snapshot of the current status of access, supply and rational use of selected life saving maternal/RH medicines
2. To guide Institutional support and capacity building in the areas RH commodities security. 3. Suggest action recommendations for consideration by MOH and Key Stakeholders for improving
accessibility, availability, procurement, rational use and quality issues of selected life saving maternal/RH medicines
Information required for the study was obtained through document reviews, key informant interviews, and selected site visits for the purposes of tracking the need, demand and supply of the six products (tracer medicines) through the supply system to the point of use. Field visits were conducted in Ulaanbaatar, Bulgan, Khentii, and Orkhon aimags (and selected soums). LIMITATIONS and STRENGTHS OF THE STUDY This is a rapid assessment exercise which aims to provide a snapshot of the current situation in Mongolia regarding the availability and use of the selected sample of life saving RH medicines in a pragmatic sample of health facilities and pharmacies in a number of provinces in Mongolia. The aimags were selected purposively considering transport, human capacity and the time constraints of the assessment and also because they have not been included in recent/previous RH assessments. Therefore, a limitation of the assessment is that the findings may not be generalizable to health facilities and pharmacies throughout Mongolia. However, the strengths of the assessment are that it can be completed in a short time frame; it is relatively inexpensive; the findings can supplement and/or validate other similar on-going or planned studies; it can enable wider stakeholder involvement in collaboration with the MoH and the findings can be used for further raising awareness among key stakeholders.
5
The full terms of reference for this assessment exercise can be found in Annex A. Key Issues Identified and Suggested Action Recommendations Issues Identified with the EML:
• Ergometrine not currently listed in EML • Metronidazole injection listed in Section 6.4 Antiprotozoal Drugs and not in Section 6.2.2 Other
antibacterials • Hydralazine is not included in the Mongolian EML • Salbutamol injection 50 mcg is listed in Section 22.2 Antioxytocics
Action recommendations for EML: The MoH through its Department of Pharmacy and the Department of Health establish a working group/focal point to:
• Consult with Obstetric and Gynaecology experts and professional organizations to review need to add Ergometrine to the EML at the next meeting to revise and up-date the EML
• Take the necessary actions to add Metronidazole injection to Section 6.2.2 Other antibacterials during the current ongoing revision of the EML and obtain the required official approval and disseminate the revised EML through approved channels
• Consult with Obstetric and Gynaecology experts and professional organizations to determine whether there is a need to include hydralazine on the EML and then prepare the necessary documentation and authorizations for implementing the recommendation.
• Take the necessary actions to replace Salbutamol injection with Nifedipine 10mg immediate release capsules in the next revision of the EML
Issues Identified with the Availability:
• Overstocks of ergometrine in some visited sites • Occasional stock outs of some selected medicines (from 1 week to 2 months) such as oxytocin, (mainly
in UB City) metronidazole (in rural areas because of high cost), and ampicillin ( because of excessive demand and poor forecasting) were observed in some visited sites.
• There was no standardised guidelines for estimation of medicines Action recommendations for increasing availability:
• Capacity building on estimation/forecasting at all levels through the development and application of standardised estimation and forecasting tools and relevant training and supervision
• MoH should systematically scale up the LMIS that had been initiated and supported by UNFPA by establishing a clear mechanism for its institutionalisation using an official working group approach.
Issues Identified with the availability and use of STGs/Algorithms/Protocols :
• Guidelines currently available in health facilities date from 2000-2003. May be out of date when compared with the current evidence based practice recommended by WHO
• No nationally endorsed standardized treatment algorithms displayed in or near delivery room because of lack of these officially approved algorithms. There was evidence that several vertical initiatives had been undertaken by health professionals for making treatment algorithms available in or near the delivery ward, but there was no consistency in the type and source of the information displayed. Examples included photocopies of pages from an obstetric textbook describing the use of Oxytocin for induction of labour and a A4 size poster detailing the different dosage regimens for Magnesium Sulphate, depending on the strength of solution (50% or 25%), for the treatment of pre-eclampsia/eclampsia, which had been provided by the Maternal and Child Health Research Centre. However, this was only found in one Soum Hospital.

6
• WHO guidelines were not adapted to reflect the locally available strengths of magnesium sulphate
Action recommendations for STGs/Protocols:
• Review, revise and adapt the current handbooks and guidelines approved for Mongolia to be in-line the latest WHO materials and update the Mongolian versions accordingly
• Develop standardized nationally endorsed posters of the treatment algorithms for prevention and treatment of PPH; treatment of pre-eclampsia and eclampsia and management of maternal sepsis and neonatal sepsis for display in facilities which provide delivery services and set up a mechanism for these posters to be widely distributed in sufficient numbers to the facilities at all levels
• Set up a mechanisms for regular future revisions of guidelines that should include treatment regimens based on the use of 25% solution of magnesium sulphate in line with revised treatment algorithms
Issues Identified with the Rational Use:
• Critical knowledge practice gap exists regarding the appropriate use of oxytocin and magnesium sulphate in some selected sites visited, but was not generalised.
• These selected tracer medicines can be bought from private pharmacies without prescriptions • Magnesium sulphate injection is being sold to outpatients for the treatment of hypertension. Magnesium
sulphate is an anticonvulsant, not an antihypertensive medication. Irrational use of this medicine. Need to investigate why it is being used as an outpatient treatment for hypertension.
Action recommendations for Rational Use:
• Provision of in-service training to practitioners to effectively use the guidelines and standards for the use of Oxytocin 10 IU as a routine and essential part of AMTSL
• Ensure the application of the guidelines and recommended standard dose of continuous MgSO4 solution in accordance with the approved treatment algorithms and supportive in-service training.
• Good prescription and dispensing practice should be strengthened with the support of the Department of Health and the Hospital Drug and Therapeutic Committees (DTC) through the provision of on-going in-service training
Issues Identified with the Registration and Quality Assurance:
• One unregistered brand of calcium gluconate (Novosibchem Pharma, Russia) was found to be in use in 3 of the surveyed health facilities that included an aimag general hospital (1) and FGPs (2)
• One unregistered brand of magnesium sulphate (Vero Pharm, Russia) was found to be in use at one of the surveyed Soum Hospital
Action recommendations for Registration and Quality Assurance:
• The State General Inspection Agency in collaboration with the Department of Health should investigate the unregistered calcium gluconate and magnesium sulphate products and take appropriate measures and develop a framework approach for dealing with counterfeit and unregistered drugs
Issues Identified with the Storage:
• There was widespread inappropriate storage of Oxytocin in most of the visited Facilities/pharmacies. • It was also found at the same survey sites the manufacturer’s instructions for all these tracer medicines
were only in English or in Russian.
7
Action recommendations for Storage:
• MoH to demand that all procurement contracts include storage instructions and drug inserts in Mongolian as an essential condition for selection during the tendering process. MoH should also demand that approval of the registration of the drugs be conditional on commitment by the drug manufacturer/supplier to provide storage instructions and drug inserts in Mongolian.
• MoH review the current storage facilities and conditions at the central and local level facilities and then revise and update the standards for storage of drugs and other medical supplies.
Issues Identified with the Procurement and Supply Chain Management:
• Most of the oxytocin and all of the ergometrine is currently provided and funded by UNFPA • A variety of approaches (all within the procurement law) were employed by the various surveyed
facilities. These were 1) bulk procurement through an aimag tendering process, 2) direct procurement from the wholesalers or 3) through the Revolving Drug Fund mechanisms.
• Inadequate capacity for estimation/forecasting RH essential medicines in terms of estimation and forecasting methods used, knowledge and skills of the staff doing the forecasting/estimation, unavailability of standardised forms/checklists with their associated guidelines and procedures for doing estimations and forecasting requirements and weak or non functioning DTCs.
Action recommendations for Procurement and Supply Chain Management:
• The government should also examine a variety of sustainable mechanisms for procurement, storage and distribution of all RH essential medicines, with special emphasis on oxytocin and ergometrine and select the one suitable for implementation in Mongolia using the findings of the in-depth study referred to earlier that is integrated with an expanded national LMIS also mentioned above.
• Further in-depth study of different supply methods for Soum Hospital for all essential medicines to identify the essential components that would constitute a most efficient and cost-effective supply system.
• Forecasting capability should be strengthened and integrated with the institutionalised LMIS, as mentioned earlier.
Issues Identified with the Costs:
• Health Facilities have to contend with very wide variation in cost when procuring these tracer and other medicines
• Metronidazole injection is very expensive especially in the rural areas (950-2500 tugrik; US $ 0.679-1.786).
• The Drug Registration Process does not include a price ceiling conditionality Action recommendations for the Costs:
• Government to obtain a commitment by drug manufacturers, importers, wholesalers and, where applicable, retailers to adhere to a price ceiling and drug pricing policies and lists of the government as an essential conditionality and prerequisite for the registration of all RH essential drugs and all medicines on the EML
• Government (MoH and MoF) should establish a permanent mechanism for developing, periodically reviewing and revising and enforcing, with adequate sanctions, a price list for all medicines on the EML that is integrated with the national.
8
Issues Identified with the Coordination/Integration:
• Co-ordination and harmonisation of project activities in the country related to LMIS and the regulation,
inspection, provision and use of essential RH and other medicines along with MCH and RH activities between different organizations and partners is currently quite weak.
• Inadequate participation of private sector and domestic NGO partners in initiatives/projects undertaken by the MoH in the area of reproductive health, such as training workshops, seminars and capacity development activities
Action recommendations for Coordination/Integration:
• Promote a more integrated approach for planning, implementation and monitoring of RH interventions through the use of the established MoH aid coordination mechanisms including setting up of working group and/or focal point n the MoH
• Increase participation of private and domestic NGO partners in future initiatives/projects by MoH in the area of reproductive health, including training activities and capacity building by mandating representation on the strengthened coordination mechanisms mentioned earlier and through mandatory participation of selected partner staff and stakeholder representatives, using mutually accepted selection criteria.

9
Chapter 1. Context and Background With a population of 2.6 million people on an area of 1,566,460 square kilometers, Mongolia has a vast, sparsely populated territory and four seasons alternate with a harsh continental climate. 60.6% of population lives in urban areas and 39.4% lives in rural areas. Population of Mongolia is continuing to rapidly change both in terms of its geographical distribution and urbanization. 8 provinces of the country have their population actually decreased over period of 15 years from 1990 to 2005; while on overall, population of the country grew from 2.1 million to 2.5 million over the same period. In 2008, Mongolia’s population reached 2.684 million. At the same time, population of Ulaanbaatar doubled from 586 thousands to 994 thousands in 2006. This number doesn’t include a large number of migrants who seldom register (unofficially the capital’s population is estimated to be near 1.2-1.5 million people). Exactly, 32.6 percent of the population are children under the age of 15, and 28.3 percent are women of 15-49 years of age. Average life expectancy is 66.5 years of age for Mongolians, where women’s average life expectancy is 70.2, and men’s 63.1. (NSO, Annual report, 2008)
Mongolia is divided into 21 aimags, 338 soums and UB city divided into 9 districts and 132 khoroos. Urban migration has resulted in the growth of Ulaanbaatar City’s population. While high-risk pregnancies are increasingly being referred from the soum to the aimag and from the aimag to the capital city, childbirths have risen in the aimags and the capital city, and aimag joint hospitals and maternity hospitals in Ulaanbaatar are unable to sustain the load. For instance, the number of women giving birth in Ulaanbaatar rose by 23.0 percent compared to 10 years ago, while the number of beds in maternity units decreased by 22 percent. Natural disasters and harsh weather conditions cause herders to migrate to different areas miss the obligation to register with the local government, and, among them, many poor and disadvantaged people are not able to receive reproductive health services. About 83.3 percent of maternal mortality cases are herders and unemployed women, and the average distance between their home and the hospital was 61.8 km. (Why did women die? ADB, MCHRC, 2006) Health services in Mongolia from primary to tertiary level are organized as follows: bagh, soum or family clinic, aimag or district, and specialized hospitals or centers. Out of the 2,100 health institutions operating nationwide, there are 15 specialized hospitals and centers, 3 regional diagnosis and treatment centers, 27 aimag and district general hospitals, 6 rural hospitals, 321 inter-soum and soum hospitals, 228 family practitioner units, and 299 maternity waiting homes, as well as 1063 private clinics. (Health statistics, 2008) Maternal Service Delivery: Management of the maternal and newborn health services At primary level or family, village and soum clinics, general practitioners are responsible for the health of reproductive age women, antenatal care for low risk pregnant women and postpartum care after uncomplicated deliveries, family planning services, and for identifying and referral of women with high risk pregnancies and complications. The primary care providers should also care and treat patients according to specialist instructions and provide home visits to postpartum women and newborn. During these home visits, family or soum doctors check women and newborn health and provide necessary management. Secondary level health services include district health centers and hospitals, and aimag and city general hospitals. Aimag and Ulaanbaatar city health departments provide policy development, planning and management of local health services. They are responsible for the structure of services, coordination and distribution of the resources, and monitoring and supervision of the general hospitals, soum, village and family clinics, bagh service delivery points on its administrative territory. Tertiary level health services include national centers and hospitals provide specialized medical care in UB and referral services for rural populations. They also responsible for research and some of them act as teaching hospitals under Ministry of Health.
10
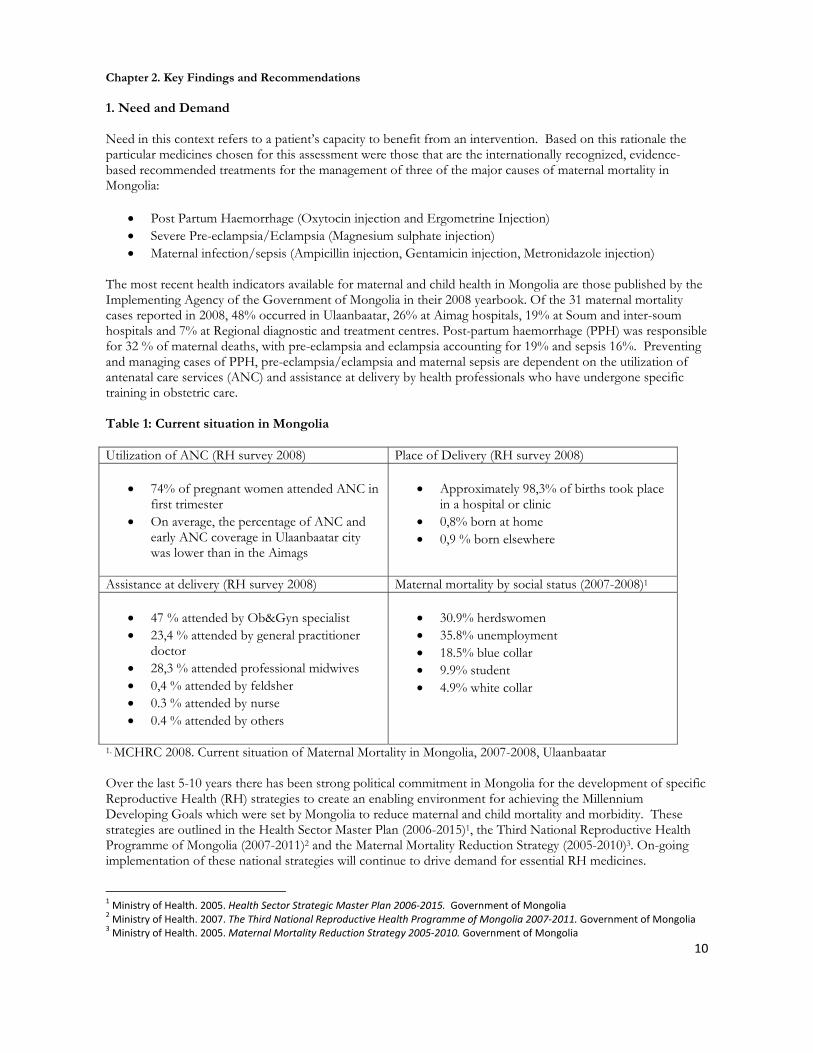
Chapter 2. Key Findings and Recommendations 1. Need and Demand Need in this context refers to a patient’s capacity to benefit from an intervention. Based on this rationale the particular medicines chosen for this assessment were those that are the internationally recognized, evidence-based recommended treatments for the management of three of the major causes of maternal mortality in Mongolia:
• Post Partum Haemorrhage (Oxytocin injection and Ergometrine Injection) • Severe Pre-eclampsia/Eclampsia (Magnesium sulphate injection) • Maternal infection/sepsis (Ampicillin injection, Gentamicin injection, Metronidazole injection)
The most recent health indicators available for maternal and child health in Mongolia are those published by the Implementing Agency of the Government of Mongolia in their 2008 yearbook. Of the 31 maternal mortality cases reported in 2008, 48% occurred in Ulaanbaatar, 26% at Aimag hospitals, 19% at Soum and inter-soum hospitals and 7% at Regional diagnostic and treatment centres. Post-partum haemorrhage (PPH) was responsible for 32 % of maternal deaths, with pre-eclampsia and eclampsia accounting for 19% and sepsis 16%. Preventing and managing cases of PPH, pre-eclampsia/eclampsia and maternal sepsis are dependent on the utilization of antenatal care services (ANC) and assistance at delivery by health professionals who have undergone specific training in obstetric care. Table 1: Current situation in Mongolia Utilization of ANC (RH survey 2008) Place of Delivery (RH survey 2008)
• 74% of pregnant women attended ANC in
first trimester • On average, the percentage of ANC and
early ANC coverage in Ulaanbaatar city was lower than in the Aimags
• Approximately 98,3% of births took place
in a hospital or clinic • 0,8% born at home • 0,9 % born elsewhere
Assistance at delivery (RH survey 2008) Maternal mortality by social status (2007-2008)1
• 47 % attended by Ob&Gyn specialist • 23,4 % attended by general practitioner
doctor • 28,3 % attended professional midwives • 0,4 % attended by feldsher • 0.3 % attended by nurse • 0.4 % attended by others
• 30.9% herdswomen • 35.8% unemployment • 18.5% blue collar • 9.9% student • 4.9% white collar
1. MCHRC 2008. Current situation of Maternal Mortality in Mongolia, 2007-2008, Ulaanbaatar Over the last 5-10 years there has been strong political commitment in Mongolia for the development of specific Reproductive Health (RH) strategies to create an enabling environment for achieving the Millennium Developing Goals which were set by Mongolia to reduce maternal and child mortality and morbidity. These strategies are outlined in the Health Sector Master Plan (2006-2015)1, the Third National Reproductive Health Programme of Mongolia (2007-2011)2 and the Maternal Mortality Reduction Strategy (2005-2010)3. On-going implementation of these national strategies will continue to drive demand for essential RH medicines.
1 Ministry of Health. 2005. Health Sector Strategic Master Plan 2006‐2015. Government of Mongolia 2 Ministry of Health. 2007. The Third National Reproductive Health Programme of Mongolia 2007‐2011. Government of Mongolia 3 Ministry of Health. 2005. Maternal Mortality Reduction Strategy 2005‐2010. Government of Mongolia
11
Key strategies which directly impact on the demand for essential RH medicines in Mongolia are:
• To improve quality and accessibility to RH services by hastening the introduction of international standards and evidence-based practices
• To increased accessibility, equity and availability of RH and safe motherhood services for the remote, migrant and disadvantaged groups of women
• To create conditions necessary for providing emergency care to mothers and children in remote, peripheral areas
Demand is also being driven by the implementation of guidelines for the management of pregnancy related complications. In 2001, the Ministry of Health translated and printed 2000 copies of the Integrated Management of Pregnancy and Childbirth (IMPAC)4 guideline, which were disseminated nationwide. Between 2001 and 2004 specific training for all Obstetric and Gynaecology Soum doctors in 16 provinces was provided (there are still 5 provinces which have yet to receive training) and in 2003-2004 the guidelines were included in the revised undergraduate and residency training curriculum. The Pregnancy, Childbirth, Postpartum and Neonatal Care5 (PCPNC) guideline was first introduced in 2003 for midwives. In 2007 the Mongolian version was up-dated following the publication of a second edition of the WHO PCPNC guidelines. At this time training on PCPNC for Soum midwives in selected provinces was organized. At the same time the midwife curriculum was revised to include the PCPNC guideline. Mongolia follows pro-natalist policies and as a result the birth rate is increasing. The following social benefits included in the number of policy documents including Law of Mongolian Development Fund, Law on Subsidies for Mother and Child and Monetary Allowances for Child, Mother and Family. These include:
• Newborn child payment 100,000 tugrik (one off payment) • Child Money Program 3000 tugrik/month, plus 25,000 tugrik/quarter • Maternity leave benefit 70% salary if employed; 20,000 tugrik/month if unemployed for 4 months • Mother’s Medal One off payments of 50, 000 tugrik for having 4 children and 100,000 tugrik for having
≥ 8 children In the last two years, the number of births increased, from 47,376 in 2006 to 63,087 in 2008. This was an increase of 33%. An increasing birth rate will naturally lead to an increase demand for essential RH medicines. 2. Essential Medicines List (EML) The National Essential Drug List provides an indication of which medicines should be available at the different levels of healthcare facilities in Mongolian. MoH facilities are encouraged to use the EML to inform purchasing decisions. However, purchase is not restricted to medicines on the EML. The current version of the Mongolian EML was last revised in 2005. There are plans to revise the EDL later this year. Currently Oxytocin, Magnesium Sulphate and Gentamicin are listed in the EML for use in Soum hospitals and above. Calcium gluconate and Ampicillin are listed for use at all levels of health care including the Feldsher posts. Metronidazole injection is currently listed in section 6.4 Antiprozoal Drugs for use at Aimag Hospitals, Clinical Hospitals and Specialized Centres. Only Metronidazole tablets are listed in Section 6.2.2 Other antibacterials. Ergometrine is not currently listed in the EML. Whilst reviewing the current Mongolian National EML it was noted that there are some WHO recommended essential medicines for Reproductive Health that are not listed. It was noted that hydralazine is not included in the Mongolian EML 2005. In the WHO Model List of Essential Medicines hydralazine is listed for the acute management of severe pregnancy
4 World Health Organization. 2000. Integrated Management of Pregnancy and Childbirth. Managing Complications in Pregnancy and Childbirth. A guide for midwives and doctors. Geneva: World Health Organization 5 World Health Organization. 2006. Pregnancy, childbirth, postpartum and newborn care: a guide for essential practice. 2nd ed. Geneva: World Health Organization
12
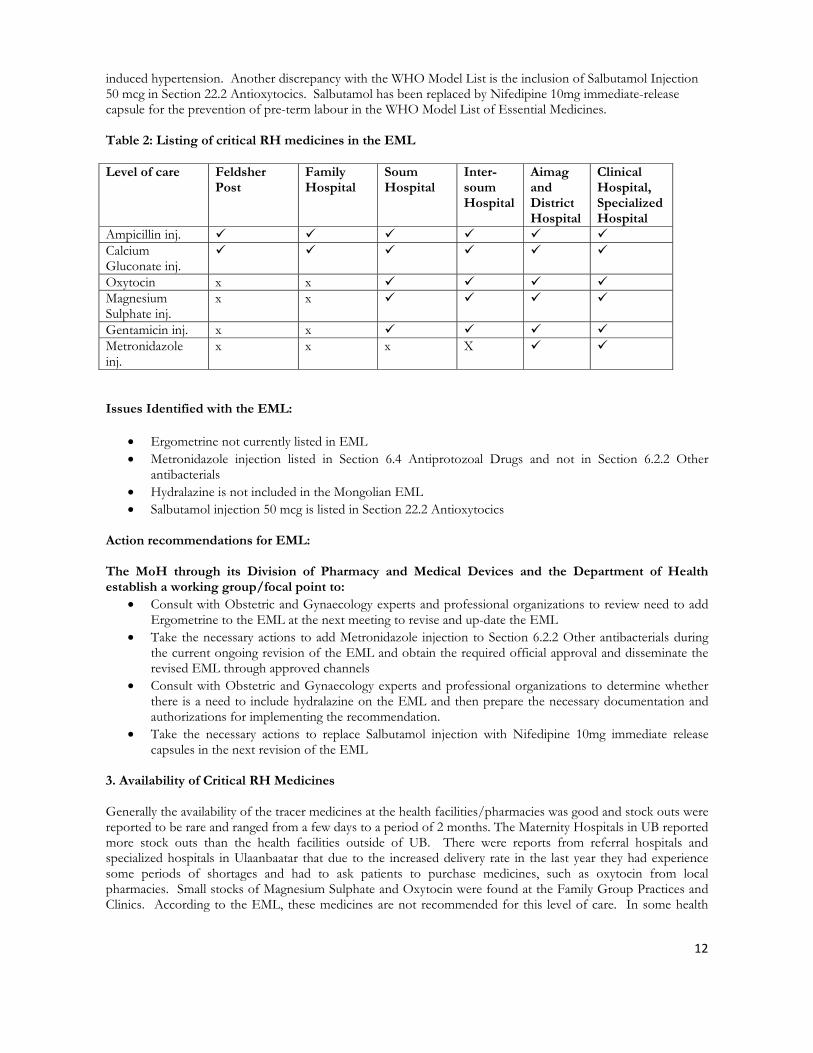
induced hypertension. Another discrepancy with the WHO Model List is the inclusion of Salbutamol Injection 50 mcg in Section 22.2 Antioxytocics. Salbutamol has been replaced by Nifedipine 10mg immediate-release capsule for the prevention of pre-term labour in the WHO Model List of Essential Medicines. Table 2: Listing of critical RH medicines in the EML Level of care Feldsher
Post Family Hospital
Soum Hospital
Inter-soum Hospital
Aimag and District Hospital
Clinical Hospital, Specialized Hospital
Ampicillin inj. Calcium Gluconate inj.
Oxytocin x x Magnesium Sulphate inj.
x x
Gentamicin inj. x x Metronidazole inj.
x x x X
Issues Identified with the EML:
• Ergometrine not currently listed in EML • Metronidazole injection listed in Section 6.4 Antiprotozoal Drugs and not in Section 6.2.2 Other
antibacterials • Hydralazine is not included in the Mongolian EML • Salbutamol injection 50 mcg is listed in Section 22.2 Antioxytocics
Action recommendations for EML: The MoH through its Division of Pharmacy and Medical Devices and the Department of Health establish a working group/focal point to:
• Consult with Obstetric and Gynaecology experts and professional organizations to review need to add Ergometrine to the EML at the next meeting to revise and up-date the EML
• Take the necessary actions to add Metronidazole injection to Section 6.2.2 Other antibacterials during the current ongoing revision of the EML and obtain the required official approval and disseminate the revised EML through approved channels
• Consult with Obstetric and Gynaecology experts and professional organizations to determine whether there is a need to include hydralazine on the EML and then prepare the necessary documentation and authorizations for implementing the recommendation.
• Take the necessary actions to replace Salbutamol injection with Nifedipine 10mg immediate release capsules in the next revision of the EML
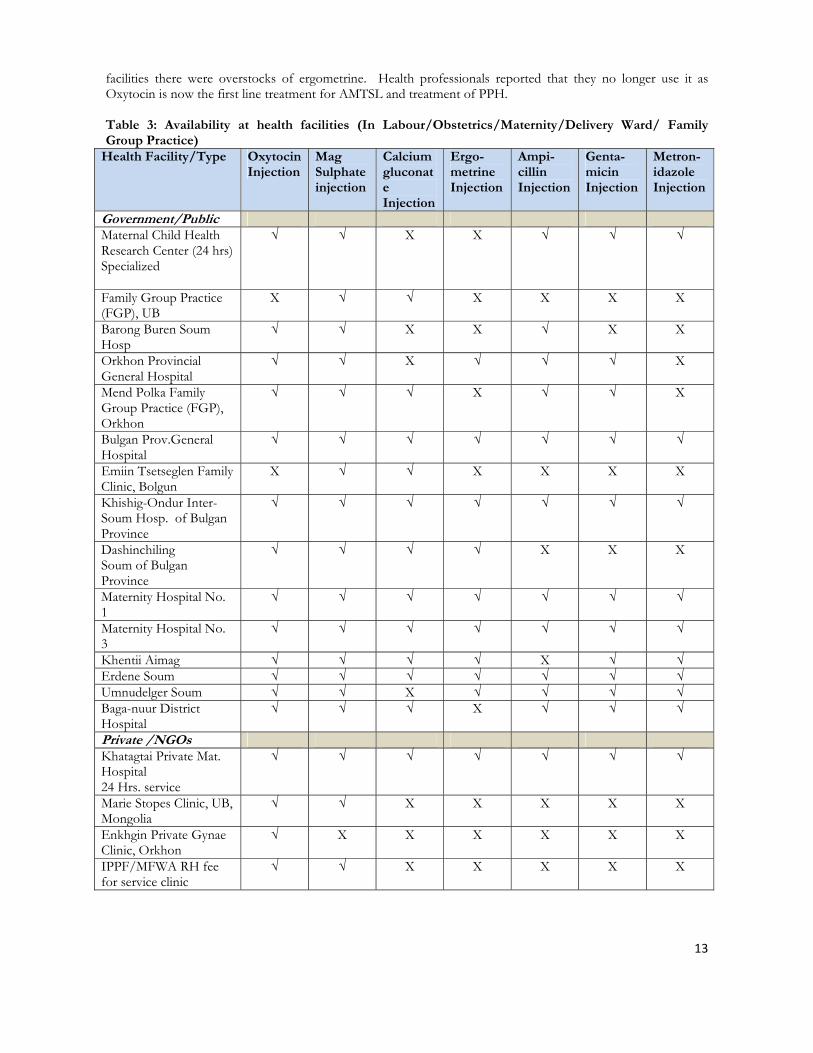
3. Availability of Critical RH Medicines Generally the availability of the tracer medicines at the health facilities/pharmacies was good and stock outs were reported to be rare and ranged from a few days to a period of 2 months. The Maternity Hospitals in UB reported more stock outs than the health facilities outside of UB. There were reports from referral hospitals and specialized hospitals in Ulaanbaatar that due to the increased delivery rate in the last year they had experience some periods of shortages and had to ask patients to purchase medicines, such as oxytocin from local pharmacies. Small stocks of Magnesium Sulphate and Oxytocin were found at the Family Group Practices and Clinics. According to the EML, these medicines are not recommended for this level of care. In some health
13
facilities there were overstocks of ergometrine. Health professionals reported that they no longer use it as Oxytocin is now the first line treatment for AMTSL and treatment of PPH. Table 3: Availability at health facilities (In Labour/Obstetrics/Maternity/Delivery Ward/ Family Group Practice)
Health Facility/Type Oxytocin Injection
Mag Sulphate injection
Calcium gluconate Injection
Ergo- metrine Injection
Ampi- cillin Injection
Genta- micin Injection
Metron-idazole Injection
Government/Public Maternal Child Health Research Center (24 hrs) Specialized
√ √ X X
√ √ √
Family Group Practice (FGP), UB
X √ √ X
X X X
Barong Buren Soum Hosp
√ √ X X √ X X
Orkhon Provincial General Hospital
√ √ X √ √ √ X
Mend Polka Family Group Practice (FGP), Orkhon
√ √ √ X √ √ X
Bulgan Prov.General Hospital
√ √ √ √ √ √ √
Emiin Tsetseglen Family Clinic, Bolgun
X √ √ X X X X
Khishig-Ondur Inter- Soum Hosp. of Bulgan Province
√ √ √ √ √ √ √
Dashinchiling Soum of Bulgan Province
√ √ √ √ X X X
Maternity Hospital No. 1
√ √ √ √ √ √ √
Maternity Hospital No. 3
√ √ √ √ √ √ √
Khentii Aimag √ √ √ √ X √ √ Erdene Soum √ √ √ √ √ √ √ Umnudelger Soum √ √ X √ √ √ √ Baga-nuur District Hospital
√ √ √ X √ √ √
Private /NGOs Khatagtai Private Mat. Hospital 24 Hrs. service
√ √ √ √
√ √ √
Marie Stopes Clinic, UB, Mongolia
√ √ X X X X X
Enkhgin Private Gynae Clinic, Orkhon
√ X X X X X X
IPPF/MFWA RH fee for service clinic
√ √ X X X X X
14
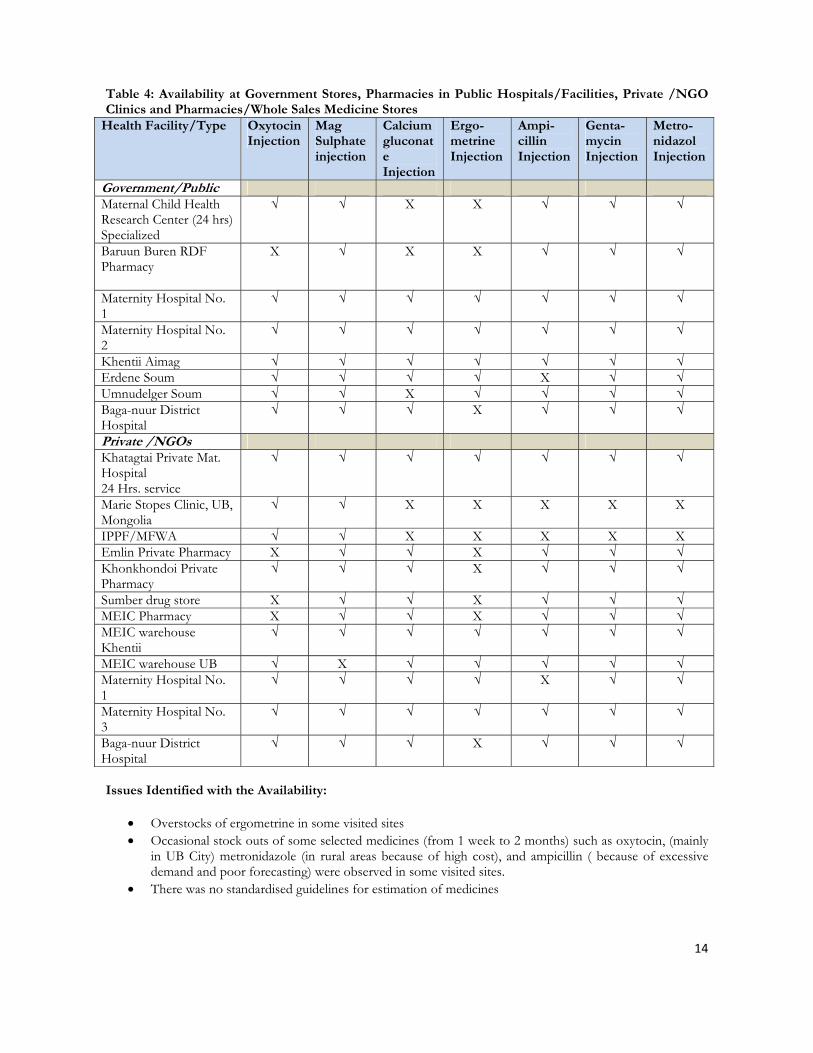
Table 4: Availability at Government Stores, Pharmacies in Public Hospitals/Facilities, Private /NGO Clinics and Pharmacies/Whole Sales Medicine Stores
Health Facility/Type Oxytocin Injection
Mag Sulphate injection
Calcium gluconate Injection
Ergo- metrine Injection
Ampi- cillin Injection
Genta- mycin Injection
Metro-nidazol Injection
Government/Public Maternal Child Health Research Center (24 hrs) Specialized
√ √ X X
√ √ √
Baruun Buren RDF Pharmacy
X √ X X √ √ √
Maternity Hospital No. 1
√ √ √ √ √ √ √
Maternity Hospital No. 2
√ √ √ √ √ √ √
Khentii Aimag √ √ √ √ √ √ √ Erdene Soum √ √ √ √ X √ √ Umnudelger Soum √ √ X √ √ √ √ Baga-nuur District Hospital
√ √ √ X √ √ √
Private /NGOs Khatagtai Private Mat. Hospital 24 Hrs. service
√ √ √ √
√ √ √
Marie Stopes Clinic, UB, Mongolia
√ √ X X X X X
IPPF/MFWA √ √ X X X X X Emlin Private Pharmacy X √ √ X √ √ √ Khonkhondoi Private Pharmacy
√ √ √ X √ √ √
Sumber drug store X √ √ X √ √ √ MEIC Pharmacy X √ √ X √ √ √ MEIC warehouse Khentii
√ √ √ √ √ √ √
MEIC warehouse UB √ X √ √ √ √ √ Maternity Hospital No. 1
√ √ √ √ X √ √
Maternity Hospital No. 3
√ √ √ √ √ √ √
Baga-nuur District Hospital
√ √ √ X √ √ √
Issues Identified with the Availability:
• Overstocks of ergometrine in some visited sites • Occasional stock outs of some selected medicines (from 1 week to 2 months) such as oxytocin, (mainly
in UB City) metronidazole (in rural areas because of high cost), and ampicillin ( because of excessive demand and poor forecasting) were observed in some visited sites.
• There was no standardised guidelines for estimation of medicines

15
Action recommendations for increasing availability:
• Capacity building on estimation/forecasting at all levels through the development and application of standardised estimation and forecasting tools and relevant training and supervision
• MoH should systematically scale up the LMIS that had been initiated and supported by UNFPA by establishing a clear mechanism for its institutionalisation using an official working group approach.
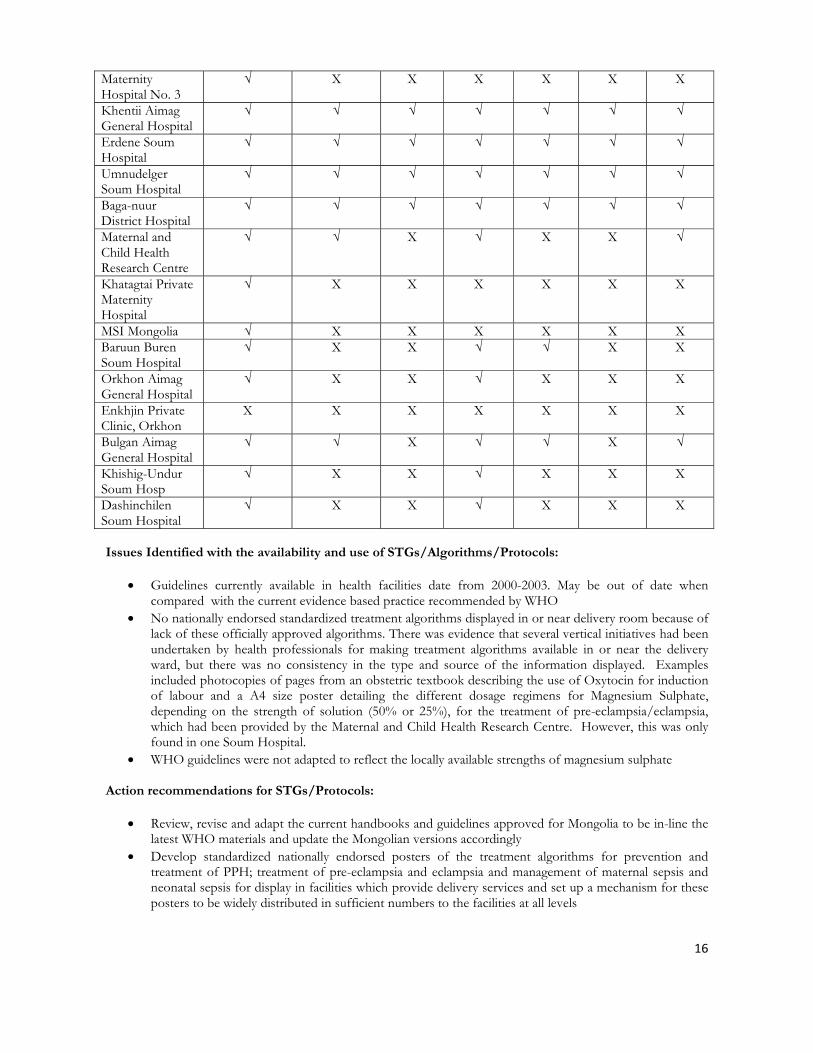
4. Standard Treatment Guidelines (STGs) and Protocols On the day of the assessment visit the availability of treatment guidelines/protocols and educational materials for prevention and treatment of PPH, management of pre-eclampsia/eclampsia and maternal and neonatal sepsis at the lower levels of hospital care was generally greater than at the more specialized centres. Overall, 7 different types of guideline were found at the health facilities visited. Usually the copies of the guidelines were found in the ObGyn doctor’s office or the midwives office/desk at the facility. However, in a few cases the guidelines were only found in the hospital director’s office. None of the guidelines observed were more recent than 2003. In most health facilities there was evidence of training materials for Emergency Obstetric Care and Behavior Change Communication and Information, Education and Communication training materials. All of the available guidelines and training materials were in Mongolian and had been developed in partnership between the MoH, WHO, UNFPA and professional associations. All the treatment regimens for MgSO4 described in the currently available guidelines for the management of pre-eclampsia and eclampsia were based on a 50% solution of MgSO4 and did not include a regimen for the 25% solution of MgSO4, which is the strength that is widely available in Mongolia. There is currently no 50% MgSO4 solution registered in Mongolia. No nationally endorsed standard treatment algorithms for the prevention and treatment of PPH or for the treatment of severe pre-eclampsia and eclampsia were found on display in any of the obstetric care delivery points. There was evidence that several vertical initiatives had been undertaken by health professionals for making treatment guidelines available in the delivery ward for all members of staff. Examples included photocopies of pages from an obstetric textbook describing the use of Oxytocin for induction of labour and a A4 size poster detailing the different dosage regimens for Magnesium Sulphate depending on the strength of solution (50% or 25%) for the treatment of pre-eclampsia/eclampsia in one Soum Hospital, which had been provided by the Maternal and Child Health Research Centre. Table 5: Availability of guidelines at Health Facilities
Availability of Guidelines at Health Facility
Managing complications in pregnancy and childbirth 2001
Management of high risk pregnancies 2003
RHSCH Vol. 1 Infection Prevn
2000
RHSCH Vol. 2 Obstetrics 2000
RHSCH Vol. 3 Family Planning 2000
RHSCH Vol. 4 Sexually Trans. Dx 2000
Obstetric care and services 2003
Organizations involved in guideline development and publication
MoH, WHO, MFOG
MoH, WHO, UNFPA, MCHRC
MoH, UNFPA, WHO, AVSC Int. MFOG
MoH, UNFPA, WHO, AVSC Int. MFOG
MoH, UNFPA, WHO, AVSC Int. MFOG
MoH, UNFPA, WHO, AVSC Int. MFOG
MoH, UNFPA, WHO, MCHRC
Name of Health Facility
Maternity Hospital No. 1
X X X √ X X X
16
Maternity Hospital No. 3
√ X X X X X X
Khentii Aimag General Hospital
√ √ √ √ √ √ √
Erdene Soum Hospital
√ √ √ √ √ √ √
Umnudelger Soum Hospital
√ √ √ √ √ √ √
Baga-nuur District Hospital
√ √ √ √ √ √ √
Maternal and Child Health Research Centre
√ √ X √ X X √
Khatagtai Private Maternity Hospital
√ X X X X X X
MSI Mongolia √ X X X X X X Baruun Buren Soum Hospital
√ X X √ √ X X
Orkhon Aimag General Hospital
√ X X √ X X X
Enkhjin Private Clinic, Orkhon
X X X X X X X
Bulgan Aimag General Hospital
√ √ X √ √ X √
Khishig-Undur Soum Hosp
√ X X √ X X X
Dashinchilen Soum Hospital
√ X X √ X X X
Issues Identified with the availability and use of STGs/Algorithms/Protocols:
• Guidelines currently available in health facilities date from 2000-2003. May be out of date when compared with the current evidence based practice recommended by WHO
• No nationally endorsed standardized treatment algorithms displayed in or near delivery room because of lack of these officially approved algorithms. There was evidence that several vertical initiatives had been undertaken by health professionals for making treatment algorithms available in or near the delivery ward, but there was no consistency in the type and source of the information displayed. Examples included photocopies of pages from an obstetric textbook describing the use of Oxytocin for induction of labour and a A4 size poster detailing the different dosage regimens for Magnesium Sulphate, depending on the strength of solution (50% or 25%), for the treatment of pre-eclampsia/eclampsia, which had been provided by the Maternal and Child Health Research Centre. However, this was only found in one Soum Hospital.
• WHO guidelines were not adapted to reflect the locally available strengths of magnesium sulphate
Action recommendations for STGs/Protocols:
• Review, revise and adapt the current handbooks and guidelines approved for Mongolia to be in-line the latest WHO materials and update the Mongolian versions accordingly
• Develop standardized nationally endorsed posters of the treatment algorithms for prevention and treatment of PPH; treatment of pre-eclampsia and eclampsia and management of maternal sepsis and neonatal sepsis for display in facilities which provide delivery services and set up a mechanism for these posters to be widely distributed in sufficient numbers to the facilities at all levels

17
• Set up a mechanisms for regular future revisions of guidelines that should include treatment regimens based on the use of 25% solution of magnesium sulphate in line with revised treatment algorithms
5. Rational Use of Critical RH Medicines The practices of healthcare providers and their use of life-saving RH medicines should be informed by the guidelines set by the WHO-MOH.and regulated with the policies set down by law-makers and legislators. Rational use was assessed by undertaking interviews with health professionals (Ob/Gyn doctors, midwives and nurses working on the delivery ward) and reviewing available patient records. Generally the level of knowledge for the indication, dose and contraindications for the tracer medicines was high and deemed appropriate for the level of expertise and responsibility of the health professionals interviewed. There were a few inconsistencies regarding the continuous dose of MgSO4 for the management of pre-eclampsia, with the timing of the maintenance doses ranging from 4 to 12 hourly. Knowledge of the need to use Oxytocin 10 IU for every delivery as part of the Active Management of the Third Stage of Labour was high, but there were some reports that not all patients were being given Oxytocin 10 IU e.g. only for those deemed high risk for PPH and in one facility it was reported that only 5 IU was being administered in order to save drug supplies. The patient record keeping was of a high standard and it was possible to determine how the diagnosis was made and track the management of the patient. There was evidence that the use of Oxytocin 10 IU for the active management of the third stage of labour was being undertaken, although it was found that in some facilities only 5 IU was being administered to patients as part of the AMTSL. Magnesium sulphate maintenance dose was not being given every 4 hours. The study medicines could be bought from private pharmacies without prescription. It was reported that IV antibiotics were often sold to patients without prescriptions. A review of prescriptions at these pharmacies showed that there was no standardized official prescription form. Some prescriptions were unsigned pieces of paper with just the name of a medicine written on them. Magnesium sulphate injection was being sold to outpatients as a treatment for hypertension. Issues Identified with the Rational Use:
• Critical knowledge practice gap exists regarding the appropriate use of oxytocin and magnesium sulphate in some selected sites visited, but was not generalised.
• These selected tracer medicines can be bought from private pharmacies without prescriptions • Magnesium sulphate injection is being sold to outpatients for the treatment of hypertension. Magnesium
sulphate is an anticonvulsant, not an antihypertensive medication. Irrational use of this medicine. Need to investigate why it is being used as an outpatient treatment for hypertension.
Action recommendations for Rational Use:
• Provision of in-service training to practitioners to effectively use the guidelines and standards for the use of Oxytocin 10 IU as a routine and essential part of AMTSL
• Ensure the application of the guidelines and recommended standard dose of continuous MgSO4 solution in accordance with the approved treatment algorithms and supportive in-service training.
• Good prescription and dispensing practice should be strengthened with the support of the Department of Health and the Hospital Drug and Therapeutic Committees (DTC) through the provision of on-going in-service training
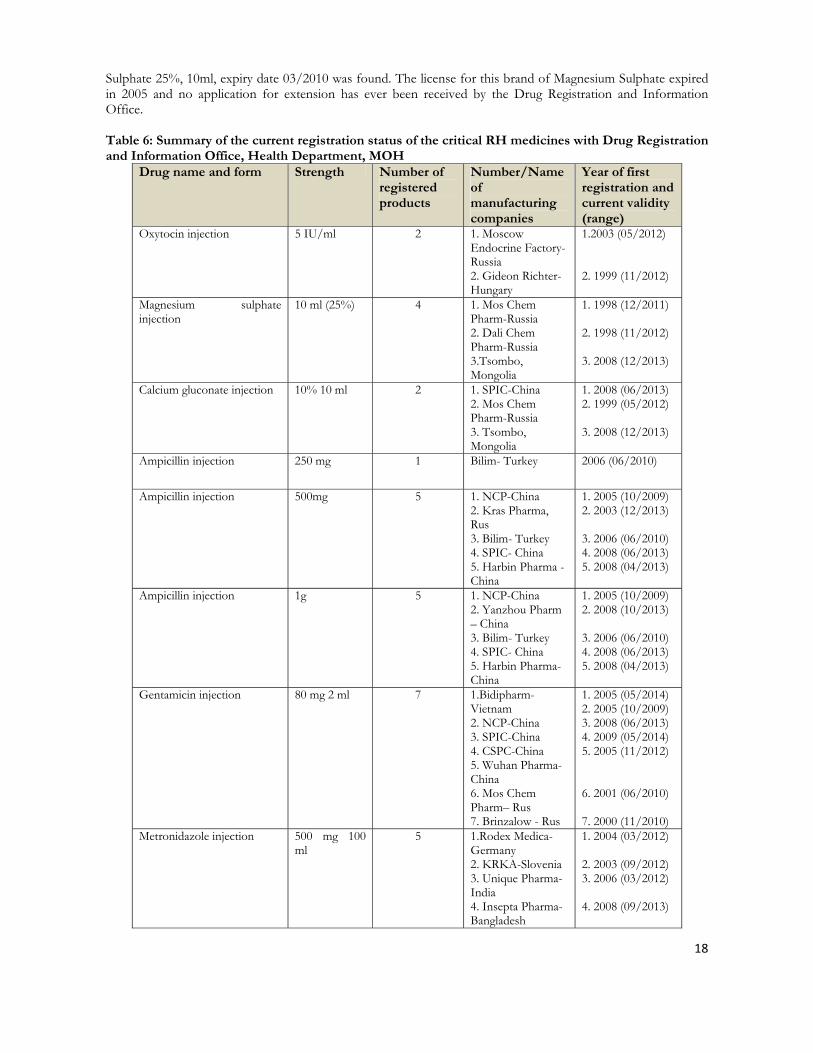
6. Registration and Quality Assurance During field visits, the team found 230 ampoules of one calcium gluconate brand, 10%, 10 ml from Russia (Novosibrisk Pharma) in the Orkhon General Hospital Pharmacy with expiration in December 2009. Also there is another brand of calcium gluconate found in few health facilities (Bulgan Provincial General Hospital, Emiin Tsetseglen Family Clinic- Bulgan, and Mend Polka Family Group Practice-Orkhon) which was labeled as ‘TMH’ but did not have a manufacturer’s name or country of origin on the ampoule. The original packaging was not available, so no further information about this brand could be elicited regarding the origins of this product. At the Erdene Soum Hospital, 47 ampoules of an unregistered Russian brand (Vero Pharma) of Magnesium
18
Sulphate 25%, 10ml, expiry date 03/2010 was found. The license for this brand of Magnesium Sulphate expired in 2005 and no application for extension has ever been received by the Drug Registration and Information Office. Table 6: Summary of the current registration status of the critical RH medicines with Drug Registration and Information Office, Health Department, MOH
Drug name and form Strength Number of registered products
Number/Name of manufacturing companies
Year of first registration and current validity (range)
Oxytocin injection 5 IU/ml 2 1. Moscow Endocrine Factory- Russia 2. Gideon Richter-Hungary
1.2003 (05/2012) 2. 1999 (11/2012)
Magnesium sulphate injection
10 ml (25%) 4 1. Mos Chem Pharm-Russia 2. Dali Chem Pharm-Russia 3.Tsombo, Mongolia
1. 1998 (12/2011) 2. 1998 (11/2012) 3. 2008 (12/2013)
Calcium gluconate injection 10% 10 ml 2 1. SPIC-China 2. Mos Chem Pharm-Russia 3. Tsombo, Mongolia
1. 2008 (06/2013) 2. 1999 (05/2012) 3. 2008 (12/2013)
Ampicillin injection 250 mg 1 Bilim- Turkey 2006 (06/2010)
Ampicillin injection 500mg 5 1. NCP-China 2. Kras Pharma, Rus 3. Bilim- Turkey 4. SPIC- China 5. Harbin Pharma - China
1. 2005 (10/2009) 2. 2003 (12/2013) 3. 2006 (06/2010) 4. 2008 (06/2013) 5. 2008 (04/2013)
Ampicillin injection 1g 5 1. NCP-China2. Yanzhou Pharm – China 3. Bilim- Turkey 4. SPIC- China 5. Harbin Pharma- China
1. 2005 (10/2009)2. 2008 (10/2013) 3. 2006 (06/2010) 4. 2008 (06/2013) 5. 2008 (04/2013)
Gentamicin injection 80 mg 2 ml 7 1.Bidipharm-Vietnam 2. NCP-China 3. SPIC-China 4. CSPC-China 5. Wuhan Pharma-China 6. Mos Chem Pharm– Rus 7. Brinzalow - Rus
1. 2005 (05/2014)2. 2005 (10/2009) 3. 2008 (06/2013) 4. 2009 (05/2014) 5. 2005 (11/2012) 6. 2001 (06/2010) 7. 2000 (11/2010)
Metronidazole injection 500 mg 100 ml
5 1.Rodex Medica-Germany 2. KRKA-Slovenia 3. Unique Pharma-India 4. Insepta Pharma-Bangladesh
1. 2004 (03/2012) 2. 2003 (09/2012) 3. 2006 (03/2012) 4. 2008 (09/2013)
19
5. SPIC-China 5. 2008 (06/2013)
Issues Identified with the Registration and Quality Assurance:
• One unregistered brand of calcium gluconate (Novosibchem Pharma, Russia) was found to be in use in 3 of the surveyed health facilities that included an aimag general hospital (1) and FGPs (2)
• One unregistered brand of magnesium sulphate (Vero Pharm, Russia) was found to be in use at one of the surveyed Soum Hospital
Action recommendations for Registration and Quality Assurance:
• The State General Inspection Agency in collaboration with the Department of Health should investigate the unregistered calcium gluconate and magnesium sulphate products and take appropriate measures and develop a framework approach for dealing with counterfeit and unregistered drugs
7. Storage (of Tracer Drugs) Medicines are securely stored, and storage conditions of medicines are generally well controlled. It was found that all the facilities had enough space with shelves. Most of the facilities visited were relatively clean and in good order in spite of heavy workload, but the temperature is always dependent on ambient temperature. Potential attention should be given to future storage condition for Oxytocin or provision of appropriate Oxytocin. Most of the facilities are using Oxytocin which is not required for specific storage condition, a few of them visited have kept the Oxytocin at ambient temperature that should have been stored below 2-8.This means that there has been a certain possibility that the other facilities must have kept in that wrong way due to little knowledge on special requirement for storage condition for Oxytocin.The team could find no evidence that cold chain maintenance was ensured throughout the supply system. Therefore it might be the best and cost effective option to purchase and provide appropriate Oxytocin (storage condition; below 25) for the cold chain. Issues Identified with the Storage:
• There was widespread inappropriate storage of Oxytocin in most of the visited Facilities/pharmacies. • It was also found at the same survey sites the manufacturer’s instructions for all these tracer medicines
were only in English or in Russian. Action recommendations for Storage:
• MoH to demand that all procurement contracts include storage instructions and drug inserts in Mongolian as an essential condition for selection during the tendering process. MoH should also demand that approval of the registration of the drugs be conditional on commitment by the drug manufacturer/supplier to provide storage instructions and drug inserts in Mongolian.
• MoH review the current storage facilities and conditions at the central and local level facilities and then revise and update the standards for storage of drugs and other medical supplies.

20
8. Procurement and Supply Chain Management Drug supply system in Mongolia is fully privatized and the procurement is also decentralized. Before 1991 all procurement and supply chain management was centralized. The hospitals purchase pharmaceuticals through an open tendering process. The implementation of the tendering process is based on the new procurement law. Under this law, the procurement is divided into several rules depending on the size of the tender. Currently, every Aimag manages their own procurement and supplies of medicines independently through tendering. Ulaanbaatar city carries out a tender for all of its district hospitals. The larger National hospitals (centrally located secondary, tertiary and specialized hospitals in Ulaanbaatar and 3 specialized provincial level hospitals known as regional diagnostic centers) manage their own procurement and supplies of medicines and medical devices independently through open tendering process. The smaller hospitals are clustered together in a combined tender. Apparently at the Soum levels there are different options of procurement: mostly through the Revolving Drug Fund (RDF) mechanisms; or alternatively either integrated into the Aimag tendering process, or direct procurement by individual soum or a mixed of these processes. About 30% of 330 soum hospitals do not have facility, transportation and cold chain equipments to maintain quality of drug and medical devices at the required level of standard. Soums don’t have human and technical capacity to make proper estimation, procurement, inventory, storage and warehousing and distribution of drug and medical devices at acceptable level of quality. Pharmaceutical sector is one of the first in Mongolia that was privatized. There are 38 drug manufacturers, 136 drug wholesale agencies, 1026 pharmacies work in the area of producing and procuring drug and medical supplies including RH commodities. Mongolia imports 75-80% of its required drugs and medical supplies and produces the rest domestically. Since 1992 UNFPA has been providing about 90% of total contraceptives spending. Also UNFPA has been providing almost all (90%) of Oxytocin and perhaps 100% of Ergometrine injections (except that the team found only one private clinic who has been brining/importing a small amount of Ergometrine injections). Although, Government spends considerable amount of funding for medical care related with pregnancy and delivery, funding for RH commodities is not included as a separate line item in the state budget. Supply of drugs, medical devices and equipments for essential obstetric and infant care is below 20% in rural areas, which contributes to the relatively higher maternal and infant deaths and inadequate quality of care. (National strategy on RH commodity security, 2009) National RH Commodity Security Strategy 2009-2013
A Memorandum of Understanding between MOH and UNFPA signed in 2007 outlines series of mutual commitments and serves as a basis for initiatives in the sustainable RH commodity security in the longer-term basis. And eventually Mongolia was selected as a Stream 1 country for the UNFPA’s Global Programme to enhance RHCS. As a result of effective advocacy efforts special article on “increasing government resources to secure RH commodity needs of herders and the poor” was included into the Mid-Term Development Framework of Mongolia for 2009-2011 and approved by the government of Mongolia. Also as it was mentioned under target/indicator 1.1.1, the Government allocated for the first time US$ 50,000 (85 m Mongolia Tug) for RH commodities including contraceptives in 2009 state budget. Consequently the National RHCS Strategy and Plan of Action was developed and endorsed in April 2009 and it has 3 main objectives covering areas of improving legal and regulatory mechanisms for RH commodity supply, the establishment of system at all levels for RH commodity procurement, building national capacity, creating reliable financial sources and improving accessibility of RH commodities to meet population needs and demands.

21
Logistics Management Information System (LMIS and CHANNEL) In 2002 LMIS was introduced for central and provincial levels. In 2007 UNFPA developed an integrated RH HMIS and LMIS software to be implemented as a pilot project. Piloting of the UNFPA’s software for RH commodities at soum level was initiated in three focus aimags (Bayan-Ulgii, Khovd and Uvs) with prior training and logistics support. Evaluation of the pilot intervention in selected soums was undertaken in the same year and was deemed to be successful. It was subsequently expanded to two other aimags (Gobi-Altai, Khuvsgul) in 2008. So these whole pilot LMIS interventions included all the areas related to development of software, capacity building (training of staff involved) and provisions of required logistics support. In addition, from early 2008 steps taken to introduce the UNFPA global CHANNEL software at the 21 aimags and 9 districts under Ulaanbaatar for monitoring procurement and supply of RH commodities. For this CHANNEL has already been translated into Mongolian, training conducted at the central level for the respective RH coordinators UNFPA CO focal points. From April 2009, the UNFPA IT specialist started working to introduce CHANNEL as a web based LMIS (which was shared in the Regional Workshop in Bangkok in May, 2009). Now UNFPA is working closely with MOH, in consultation with the UNFPA HQ (Commodity Security Branch), for implementation (by the 4th quarter of 2009) and follow up. BOX 1: Excerpts from the assessment team National Level Questionnaire for RH Medicine Procurement (from MOH)
Describe the public sector procurement process for essential medicines, including following information: Who buys? Who supplies? Level of healthcare distribution.
According to the law of Tender, which was renewed in 2006, every government organization should purchase goods, supplies and consultancy services through bidding altough the specific type of procurement depends on the amount of the allocated budget. In purchasing drugs, diagnostic reagents, and medical devices, each hospital has to establish a bidding committee to evaluate and select the suppliers. Furthermore, according to the above mentioned law, all tertiary and secondary level hospitals are required to purchase the essential medicines for the year by bidding /open tendering/. In each aimag, soum level’s needed essential medicines are purchased through centralized tenders organized by the aimag’s Health department. Annualy about 40 drug and pharmaceutical supply tender processes are organized / 10 tertiary hospitals’; 12 secondary hospitals’; 9 centralized, aimag and soum hospitals’/. Nationally, out of all 150 pharmaceutical wholesalers approximatelly 60 participate in tendering processes and about 15 pharmaceutical wholesalers supply more than 70 percent of all drugs purchased through tenders.
Issues Identified with the Procurement and Supply Chain Management:
• Most of the oxytocin and all of the ergometrine is currently provided and funded by UNFPA • A variety of approaches (all within the procurement law) were employed by the various surveyed
facilities. These were 1) bulk procurement through an aimag tendering process, 2) direct procurement from the wholesalers or 3) through the Revolving Drug Fund mechanisms.
• Inadequate capacity for estimation/forecasting RH essential medicines in terms of estimation and forecasting methods used, knowledge and skills of the staff doing the forecasting/estimation, unavailability of standardised forms/checklists with their associated guidelines and procedures for doing estimations and forecasting requirements and weak or non functioning DTCs.
Action recommendations for Procurement and Supply Chain Management:
• The government should also examine a variety of sustainable mechanisms for procurement, storage and distribution of all RH essential medicines, with special emphasis on oxytocin and ergometrine and select the one suitable for implementation in Mongolia using the findings of the in-depth study referred to earlier that is integrated with an expanded national LMIS also mentioned above.
22
• Further in-depth study of different supply methods for Soum Hospital for all essential medicines to identify the essential components that would constitute a most efficient and cost-effective supply system.
• Forecasting capability should be strengthened and integrated with the institutionalised LMIS, as mentioned earlier.
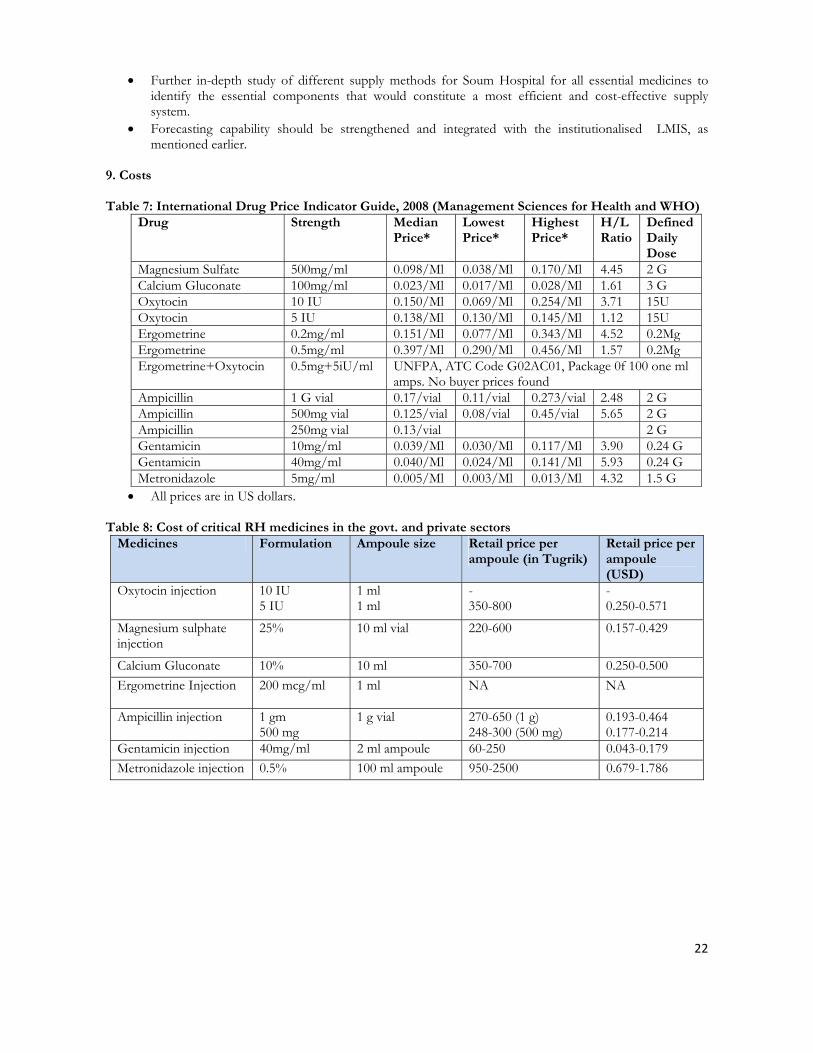
9. Costs Table 7: International Drug Price Indicator Guide, 2008 (Management Sciences for Health and WHO)
Drug Strength Median Price*
Lowest Price*
Highest Price*
H/L Ratio
Defined Daily Dose
Magnesium Sulfate 500mg/ml 0.098/Ml 0.038/Ml 0.170/Ml 4.45 2 G Calcium Gluconate 100mg/ml 0.023/Ml 0.017/Ml 0.028/Ml 1.61 3 G Oxytocin 10 IU 0.150/Ml 0.069/Ml 0.254/Ml 3.71 15U Oxytocin 5 IU 0.138/Ml 0.130/Ml 0.145/Ml 1.12 15U Ergometrine 0.2mg/ml 0.151/Ml 0.077/Ml 0.343/Ml 4.52 0.2Mg Ergometrine 0.5mg/ml 0.397/Ml 0.290/Ml 0.456/Ml 1.57 0.2Mg Ergometrine+Oxytocin 0.5mg+5iU/ml UNFPA, ATC Code G02AC01, Package 0f 100 one ml
amps. No buyer prices found Ampicillin 1 G vial 0.17/vial 0.11/vial 0.273/vial 2.48 2 G Ampicillin 500mg vial 0.125/vial 0.08/vial 0.45/vial 5.65 2 G Ampicillin 250mg vial 0.13/vial 2 G Gentamicin 10mg/ml 0.039/Ml 0.030/Ml 0.117/Ml 3.90 0.24 G Gentamicin 40mg/ml 0.040/Ml 0.024/Ml 0.141/Ml 5.93 0.24 G Metronidazole 5mg/ml 0.005/Ml 0.003/Ml 0.013/Ml 4.32 1.5 G
• All prices are in US dollars. Table 8: Cost of critical RH medicines in the govt. and private sectors
Medicines Formulation Ampoule size Retail price per ampoule (in Tugrik)
Retail price per ampoule (USD)
Oxytocin injection 10 IU 5 IU
1 ml 1 ml
- 350-800
- 0.250-0.571
Magnesium sulphate injection
25%
10 ml vial 220-600
0.157-0.429
Calcium Gluconate 10% 10 ml 350-700 0.250-0.500 Ergometrine Injection 200 mcg/ml
1 ml NA
NA
Ampicillin injection 1 gm 500 mg
1 g vial 270-650 (1 g) 248-300 (500 mg)
0.193-0.464 0.177-0.214
Gentamicin injection 40mg/ml 2 ml ampoule 60-250 0.043-0.179 Metronidazole injection 0.5% 100 ml ampoule 950-2500 0.679-1.786

23
Table 9: Cost to the patient of the WHO recommended treatment regimens based on retail prices identified during the field visit
Medication Formulation Indication Recommended treatment regimen
Number of ampoules required
Total cost to patient (Tugrik)
Total cost in USD*
Magnesium Sulphate injection
25% in 10 ml ampoule
Severe Pre-eclampsia / Eclampsia
Loading dose 4g IV+ 10g IM Maintenance dose: 5g IM every 4 hours for 24 hours
18 2700-10800
2.83-7.71
Oxytocin 10 IU in 1ml ampoule 5 IU in 1 ml ampoule
Prevention of PPH
10 IU immediately after birth of baby
1 (10 IU)2(5 IU)
NFS 700-1600
NFS 0.50-1.15
Treatment of PPH
10 IU IM followed by IV infusion, up to maximum 40 IU
5 (10 IU)10(5 IU)
NFS 3500-8000
NFS 2.50-5.71
Ergometrine 200 mcg in 1 ml ampoule
Treatment of PPH if heavy bleeding persists after use of Oxytocin
200 mcg IM/IV slowly. Repeat 200 mcg after 15 minutes if heavy bleeding persists.
2 NFS Only donated by UNFPA
Ampicillin Injection
1 g 500mg
First line of treatment for maternal sepsis
First dose 2 g IM/IV. Then 1g IV/IM every 6 hours- for 5 days maximum
21 if 1 g 42 if 500 mg
5670 -13,650 10416 - 12,600
4.05-9.75 7.44 - 9.00
Gentamicin Injection
40 mg/ml, 2 ml ampoule
Severe abdominal pain; dangerous fever/very severe febrile disease; complicated abortion, uterine and fetal infection
80 mg IM every 8 hours (give until the woman is fever free for 48hrs)- max 5 days
15 900-3750 0.65-2.68
24
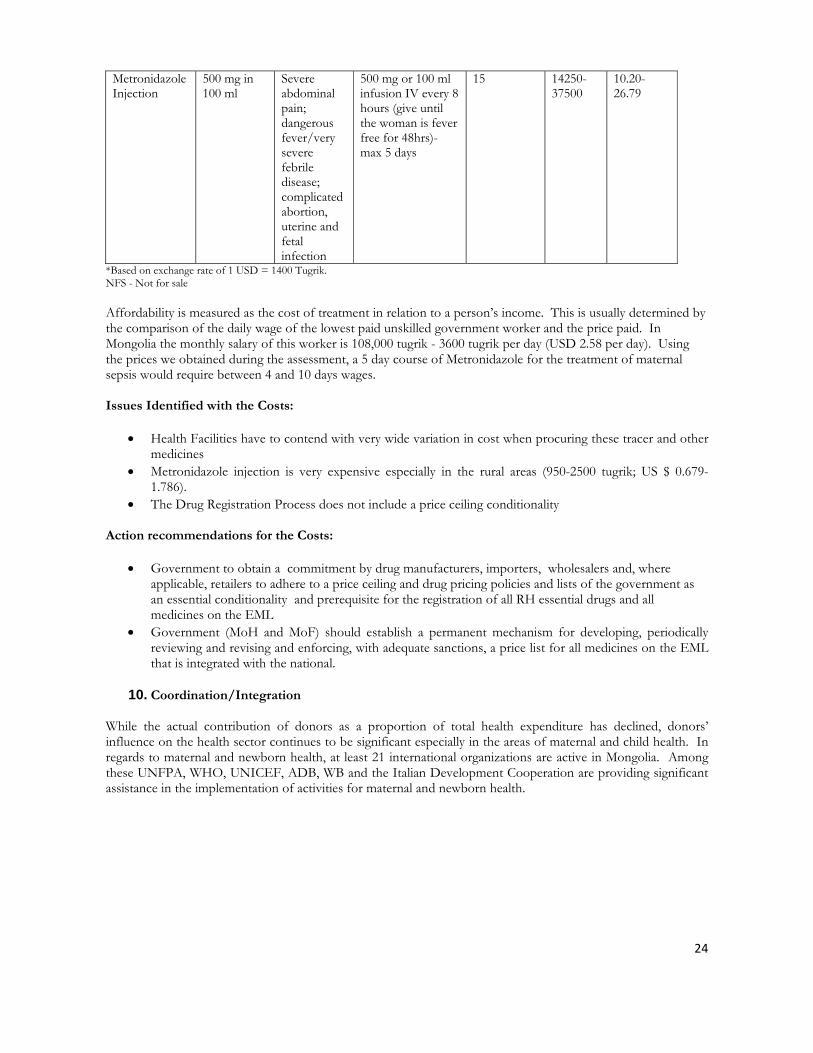
Metronidazole Injection
500 mg in 100 ml
Severe abdominal pain; dangerous fever/very severe febrile disease; complicated abortion, uterine and fetal infection
500 mg or 100 ml infusion IV every 8 hours (give until the woman is fever free for 48hrs)- max 5 days
15 14250-37500
10.20-26.79
*Based on exchange rate of 1 USD = 1400 Tugrik. NFS - Not for sale Affordability is measured as the cost of treatment in relation to a person’s income. This is usually determined by the comparison of the daily wage of the lowest paid unskilled government worker and the price paid. In Mongolia the monthly salary of this worker is 108,000 tugrik - 3600 tugrik per day (USD 2.58 per day). Using the prices we obtained during the assessment, a 5 day course of Metronidazole for the treatment of maternal sepsis would require between 4 and 10 days wages. Issues Identified with the Costs:
• Health Facilities have to contend with very wide variation in cost when procuring these tracer and other medicines
• Metronidazole injection is very expensive especially in the rural areas (950-2500 tugrik; US $ 0.679-1.786).
• The Drug Registration Process does not include a price ceiling conditionality Action recommendations for the Costs:
• Government to obtain a commitment by drug manufacturers, importers, wholesalers and, where applicable, retailers to adhere to a price ceiling and drug pricing policies and lists of the government as an essential conditionality and prerequisite for the registration of all RH essential drugs and all medicines on the EML
• Government (MoH and MoF) should establish a permanent mechanism for developing, periodically reviewing and revising and enforcing, with adequate sanctions, a price list for all medicines on the EML that is integrated with the national.
10. Coordination/Integration While the actual contribution of donors as a proportion of total health expenditure has declined, donors’ influence on the health sector continues to be significant especially in the areas of maternal and child health. In regards to maternal and newborn health, at least 21 international organizations are active in Mongolia. Among these UNFPA, WHO, UNICEF, ADB, WB and the Italian Development Cooperation are providing significant assistance in the implementation of activities for maternal and newborn health.

25
Organizations active in Maternal and Newborn Health in Mongolia FP, family planning; AC, antenatal care; SBA, skilled birth attendance, B-Em, basic emergency obstetric and newborn care; C-Em, comprehensive obstetric and newborn care; PP, post-partum; NC, newborn care; MNN, maternal and neonatal nutrition; WASH, Water Sanitation Hygiene
MNH-related activities
FP AC SBA B-Em C-Em PP NC MNN WASH
Asian Development Bank – X X X X X – X –
Italian Development Cooperation in China and Mongolia
– X X X X X X X –
Mongolian Federation of Obstetrics & Gynaecology
X X X – X – – – –
United Nations Population Fund X X X X X X X X X
United Nations International Children's Fund
X X X X X X X X X
World Bank X X – X X X – X X
World Health Organization X X X X X X X X X
Adapted from “Mongolia: External Partners’ Assistance Matrix.” 2008 by World Bank
The Health Sector Strategic Master Plan (HSSMP) is a medium-term policy framework for 2006-2015 which represents the Ministry of Health’s first comprehensive documentation of its future health sector directions. It incorporates the Mongolian government’s commitment to the MDGs and health sector reform using a Sector Wide Approach.
In May 2009, MoH established Council on Coordination of Foreign Aid and Loan in the Health Sector chaired by Vice Minister of Health (Minister’s Order 141 of 2009). This body represented by heads of international partners active in the health sector including UN agencies.
UN Joint program on Maternal and Newborn Health
In 2008, current UN agency activities were mapped according to the WHO-UNFPA-UNICEF-World Bank Joint Country Support for Accelerated Implementation of Maternal and Newborn Continuum of Care core components and the UNDAF. Through this mapping exercise, opportunities for increased joint support and impact were identified. Following this exercise, in order to improve coordination of international aid in the health sector, the UN organizations jointly developed and have been implementing a harmonized programme
26
approach since Feb 2009 in the form of the UN Joint Programme on Maternal and Newborn Health in Mongolia.
Despite these efforts by the UN agencies to pool resources and technical expertise and the MoHs recent effort towards having better coordination at national level, there is still a need to strengthen coordination and communication between the different partners. During the assessment, stakeholders especially from private sector and NGO community expressed their interest to improve partnerships between public and private through increased involvement of private institutions and professional associations in the policy development, monitoring and evaluation, regulation, as well as implementation efforts.
Issues Identified with the Coordination/Integration:
• Co-ordination and harmonisation of project activities in the country related to LMIS and the regulation,
inspection, provision and use of essential RH and other medicines along with MCH and RH activities between different organizations and partners is currently quite weak.
• Inadequate participation of private sector and domestic NGO partners in initiatives/projects undertaken by the MoH in the area of reproductive health, such as training workshops, seminars and capacity development activities
Action recommendations for Coordination/Integration:
• Promote a more integrated approach for planning, implementation and monitoring of RH interventions through the use of the established MoH aid coordination mechanisms including setting up of working group and/or focal point n the MoH
• Increase participation of private and domestic NGO partners in future initiatives/projects by MoH in the area of reproductive health, including training activities and capacity building by mandating representation on the strengthened coordination mechanisms mentioned earlier and through mandatory participation of selected partner staff and stakeholder representatives, using mutually accepted selection criteria.

27
Chapter 3. Conclusion and Recommendations
This assessment report presents a “snapshot” of the current status of access to and rational use of selected maternal health tracer drugs, which are not routinely monitored. The six selected critical medicines chosen for the study were Oxytocin injection, Ergometrine injection, Magnesium sulphate injection and three antibiotics, Ampicillin injection, Gentamicin injection and Metronidazole injection. These medicines were chosen because they are the WHO recommended medicines for the prevention and treatment of three major causes of Maternal Mortality: Haemorrhage, Eclampsia/eclampsia and Maternal/Neonatal Sepsis. Demand for these medicines in Mongolia has being increasing by the implementation of the specific Reproductive Health (RH) strategies to improve quality and accessibility to RH services and the implementation of international standards and evidence-based practices for the management of pregnancy and child birth related complication. The assessment findings show that generally the availability of these tracer medicines at the health facilities/pharmacies was good and stock outs were reported rare. Oxytocin, Magnesium Sulphate, Gentamicin, Calcium gluconate and Ampicillin and Metronidazole are listed in the Mongolian EML (2005). The different types of treatment guidelines/protocols and educational materials date from 2000-2003 were found at the health facilities visited. The level of knowledge for the tracer medicines was high. Also key issues were identified by the assessment with the EML, availability, rational use of these medicines as well as supply chain management which are listed in the Executive Summary in detail. In conclusion, we would like to highlight following major action recommendations to improve the availability, accessibility and rational use of essential RH medicines.
• Forecasting capability should be strengthened at all levels through the development and application of standardized tools and relevant training and supervision and integrate with the institutionalized LMIS.
• Systematically strengthen and scale up national LMIS by establishing a clear mechanism for its institutionalization at all levels and provide in-service training.
• Further in-depth study on procurement, storage and distribution of all RH essential medicines, with special emphasis on oxytocin and ergometrine should be undertaken to identify the essential components of efficient and cost-effective supply management system which is most suitable for Mongolia.
• Review, revise and adapt the current handbooks and guidelines according to the latest WHO materials in collaboration and professional societies and training institutions and provide in-service training to practitioners and develop standardized nationally endorsed posters for the treatment algorithms for PPH, pre-eclampsia and eclampsia and management of sepsis.
• The Ministry of Health, through its Pharmacology Department and the Department of Health Drug Registration Unit consult with the experts and professional organizations to review need to add Ergometrine and Hydralazine to the EML, also establish a framework for systematically investigating the availability and use of unregistered life saving RH medicines.
• Promote a more integrated approach for planning, implementation and monitoring of RH interventions through the use of the established MoH aid coordination mechanisms including setting up of working group and/or focal point n the MoH and increase participation of private and domestic NGO partners in the area of reproductive health.
28
ANNEXES Annex A. Terms of Reference
TERMS OF REFERENCE
Review of current status in access to a core set of critical Life-saving RH Medicines in Mongolia
UNFPA AND WHO JOINT INITIATIVE
In an effort to improve access to quality essential reproductive health (RH) medicines and medical devices, WHO, UNFPA and partners are engaged in a series of activities aimed at promoting harmonized global standards and technical assistance, developing guidance on sourcing good quality suppliers and products, building procurement capacity in resource-limited countries, and removing barriers in the appropriate use of these products. These efforts are complementary to the objectives of the UNFPA Global Programme to Enhance Reproductive Health Commodity Security, launched in November 2006. In 2007, Mongolia is selected one of first nine countries to receive support from the Global RHCS Programme. The Global RHCS Programme is designed to ensure that Reproductive Health commodity needs are met consistently and reliably for all who need them, and to facilitate linkages between programmes and partners to enhance the capacity of national stakeholders to improve systems for RH commodity supply, quality of care, demand and access to products and services.
A well-functioning supply chain capable of selecting, forecasting, quantifying, financing, procuring, and delivering the medicines and related medical devices and consumables needed is a critical element in all efforts to improve the health and well-being of mothers and children in developing countries.
The UNFPA Global Programme to Enhance Reproductive Health Commodity Security6 was created to provide a structure for moving beyond ad hoc responses to stock outs of essential RH products towards more predictable, planned and sustainable country-driven approaches for securing essential supplies and ensuring their use. Focused at the needs of countries, this programme is intended to create a process that will galvanise, institutionalise and coordinate national efforts to produce the following results:
• Reproductive health commodity needs met consistently and reliably for all who need them; • Strong linkages between RHCS and national RH and HIV/AIDS programmes and policies; • Enhanced capacity of national stakeholders and improved systems [particularly for RH commodity
supply, quality of care, demand and access]; • Mainstreaming of RHCS through gradual increases in government-controlled funding to finance
capacity and system enhancement and planned commodity provision; • Increased national ownership and management of all aspects of RHCS.
Within the broad framework of enhancing RHCS, UNFPA, in collaboration with WHO and partners, plans to assess the accessibility of some critical RH medicines in some selected countries and assessing their utilization patterns and rational use. There are anecdotal evidences that some of these medicines are not available in many facilities and/or they are not properly used and stored. The nine countries, identified as stream 1 countries, by
6 See: UNFPA Global Programme to Enhance Reproductive Health Commodity Security [2007-2011] http://www.unfpa.org/news/news.cfm?ID=881
29
the UNFPA Global Programme, including Mongolia, are selected for the initial assessment of critical RH medicines to be undertaken in 2009. The broad objectives of the assessment are:
• To obtain a snapshot of the current status of access to, quality and rational utilization of selected critical essential medicines for RH, especially those not routinely monitored through other mechanisms.
• To guide Institutional support and capacity building in the areas RH commodities security. • To develop core recommendations for country level coordination of supply strategies, quality assurance,
appropriate use of medicines and medical devices and pharmaceutical policy matters. More specific objectives are:
• Take stock of logistics and information systems of the selected medicines. • Review the functionality of supporting systems up to consumption of the end user. • Obtain a snapshot of the current availability, access to, and rational utilization of selected life-saving RH
drugs those not routinely monitored. • Review the mandate, current function and potential role of relevant departments and institutions to
manage supplies and logistics of RH commodities • Summarize the current status to guide Institutional support and capacity building in the areas RH
commodities security. • To develop core recommendations for country level coordination of supply strategies, quality assurance,
appropriate use of targeted medicines and policy matter
The targeted critical life-saving RH medicines
A small basket of tracer medicines not monitored routinely was selected as indicators to identify gaps in information. The tracer medicines ideally will include those indicated for prevention and management of anaemia, post-partum haemorrhage, obstructed labour, unsafe abortion and infection, namely:
Oxytocin, Ergometrine, Magnesium Sulfate, Calcium Gluconate, Ampicillin, Gentamycine and Metronidazole
These medicines are life-saving for maternal health and their unavailability, poor quality, and improper use can directly result in devastating consequences for the user.
30
Approach and Methodology
UNFPA and WHO jointly developed a generic approach for the review of life-saving RH medicines and utilized for the assessment in other countries that will be as basic tool for the proposed assessment. The generic approach will be adapted to the country specific context. Assessment methodology will include document reviews, key informants interviews, and selected site visits for purposes of tracking the need, demand and supply of selected critical live-saving RH medicines from entry into the system to the site of use. Assessment Team
As a first step, UNFPA and WHO propose MOH to nominate specialists to represent MOH and other relevant authorities in the assessment team with following competencies: 1 supply chain specialist (alternatively procurement specialist) from pharmaceutical division of MOH, 1 RH/Maternal Health program specialist from MOH, 1 clinical obstetrician from the professional association and 1 drug quality assurance specialist from National Professional/Drug Inspectorate Authority. UNFPA and WHO also propose that a joint fact-finding mission team undertake country visit to Mongolia to assist to national team in conducting the assessment at national and sub-national level. In addition, a national consultant will be contracted for one month to document the current status of access to essential RH medicines will be part of the assessment team. One program specialist from each UNFPA and WHO also will work as assessment team members. UNFPA will support one assessment team member from MOH and UNFPA CO focal point to participate in the same assessment/attachment training in Philippines. PROPOSED TIMELINES: Set up a national assessment team: May, 2009 Participation of MOH/UNFPA CO representative in Philippine assessment 17-30 May Recruitment of national consultant 2 June-3 July Document review and preparation for the assessment May-June UNFPA WHO joint mission 17 June-3 July Assessment and selected site visits 17 June-3 July Consolidation of results and writing assessment report July-August Next steps/dissemination assessment findings September-October

31
Annex B. Mission Schedule
Schedule UNFPA WHO Joint Mission to review Critical Maternal Life-Saving Medicines Ulaanbaatar, MONGOLIA 17 June-04 July, 2009 Team 1. Team 2.Dr. Kabir Ahmed, UNFPA HQ ( Team Leader) Dr. Anna Ridge, WHO Geneva Dr. Buyanjargal.Ya, MOH Dr. Govind Salik, WHO, Mongolia
Ms. Amarjargal Ch, MOH Dr. Tsevelmaa.B, UNFPA Mongolia
Dr. Enkhjargal Khorloo, UNFPA MongoliaDr. Altantuya.D. State Inspectorate Agency
Mr. Kang Nam, Population Center, DPRK Mr. Kim Kwang Jin, Population Center, DPRK
Dr. Yanjinsuren, Lecturer of HSUM
Dr. Bold A, National Consultant Dariimaa, Lecturer of HSUM
Date/Time Particulars Venue Responsible Person
Team 1 Team 2 Wednesday, 17 June 09.30 am OM224
Airport Pick up Mr. Kang Nam and Kim Kwang, DPRK and check in Ulaanbaatar Hotel
Chingges Khaan Airport
Driver UNFPA
10.40 pm. KE Airport Pick up Dr. Kabir UNFPA, HQ and check in Ulaanbaatar Hotel
Driver UNFPA
Thursday, 18 June 8.45 am Hotel Pick up and proceeds to UNFPA Mongolia CO Driver 9.00-9.30 Meeting with UNFPA OIC UNFPA CO 9.30-10.00 UNFPA CO All Staff Meeting UNFPA CO 10.30 – 12.30 Joint Mission Team Work
• Planning • Review the assessment tool • Documentary review
UNFPA CO A. Bold
1.00-2.00 Lunch break 2.30 – 5.30 Team work continues UNFPA CO A. Bold 5.45 Back to Hotel Driver Program for Friday, 19 June TBC Pick up Dr. Anna Ridge, WHO and check in Ulaanbaatar
Hotel Chingges Khaan Airport
Driver WHO
9.45 am Hotel pick up and proceeds to MOH Driver 10.00– 11.00 Combined meeting chaired by Vice Minister of Health
(Heads of Departments of Medical Services and Public Health Policy Implementation Coordination, OICs, Representatives of UNFPA, WHO, UNICEF, HSMP IMU)
MOH
Ch. Amarjargal, MOH
11.00-12.30 Individual meetings with technical staff of MOH 11.00-11.30 meeting with Ya.Byanjargal, OIC, MoH 11.30-12.00 meeting with HSMP team 12.00-12.30 any additional meeting will be determined in the morning
MOH Ch. Amarjargal, MOH A.Bold Buyanjargal
1.00-2.00 Lunch meeting with Head of ObGyne Department, HSUM (Prof.Jav, Kabir, Anna, Kang Nam Ill, Kim Kwong Jin, Enkhjargal, Bold)
A.Bold, Enkhmaa
2.30– 3.30
Meeting with Head and OICs of Division for Medicine and Medical Devices Policy, MOH and Chief and officials of Drug Registration and Information Division, the Health Agency under MOH
MOH
Ch. Amarjargal, MOH
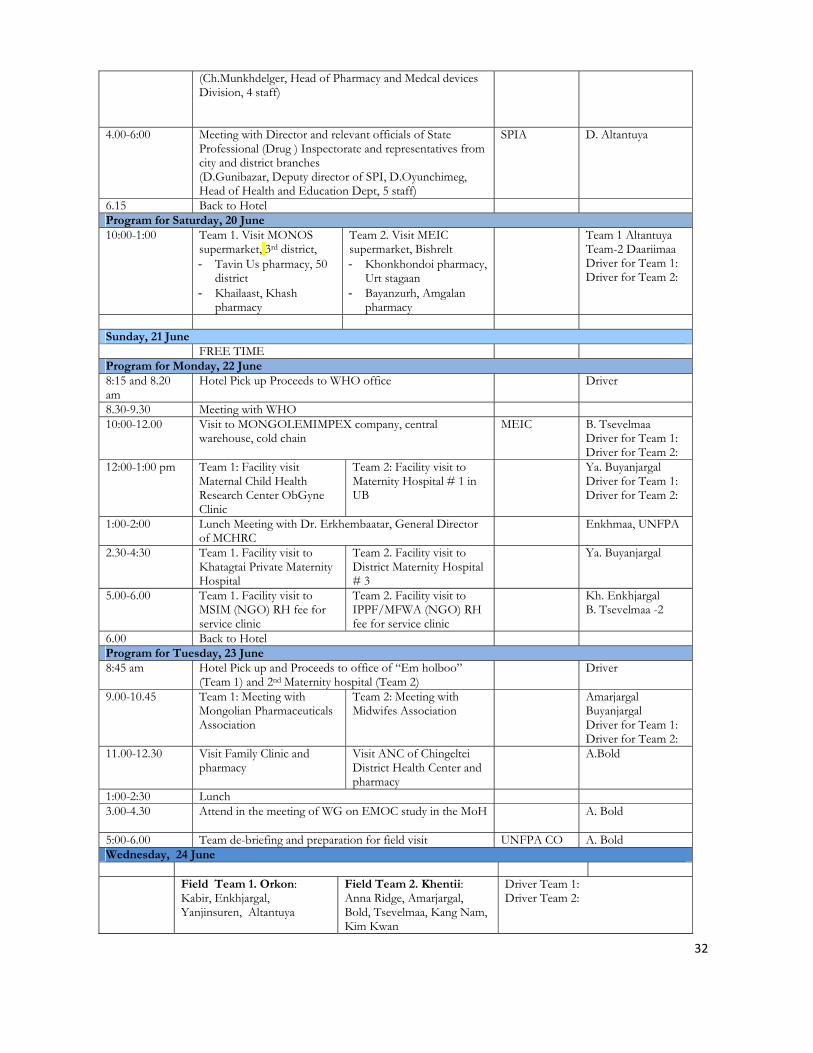
32
(Ch.Munkhdelger, Head of Pharmacy and Medcal devices Division, 4 staff)
4.00-6:00 Meeting with Director and relevant officials of State Professional (Drug ) Inspectorate and representatives from city and district branches (D.Gunibazar, Deputy director of SPI, D.Oyunchimeg, Head of Health and Education Dept, 5 staff)
SPIA D. Altantuya
6.15 Back to Hotel Program for Saturday, 20 June 10:00-1:00 Team 1. Visit MONOS
supermarket, 3rd district, - Tavin Us pharmacy, 50
district - Khailaast, Khash
pharmacy
Team 2. Visit MEIC supermarket, Bishrelt - Khonkhondoi pharmacy,
Urt stagaan - Bayanzurh, Amgalan
pharmacy
Team 1 Altantuya Team-2 Daariimaa Driver for Team 1: Driver for Team 2:
Sunday, 21 June FREE TIME Program for Monday, 22 June 8:15 and 8.20 am
Hotel Pick up Proceeds to WHO office Driver
8.30-9.30 Meeting with WHO 10:00-12.00 Visit to MONGOLEMIMPEX company, central
warehouse, cold chain
MEIC B. Tsevelmaa Driver for Team 1: Driver for Team 2:
12:00-1:00 pm Team 1: Facility visit Maternal Child Health Research Center ObGyne Clinic
Team 2: Facility visit to Maternity Hospital # 1 in UB
Ya. Buyanjargal Driver for Team 1: Driver for Team 2:
1:00-2:00 Lunch Meeting with Dr. Erkhembaatar, General Director of MCHRC
Enkhmaa, UNFPA
2.30-4:30 Team 1. Facility visit to Khatagtai Private Maternity Hospital
Team 2. Facility visit to District Maternity Hospital # 3
Ya. Buyanjargal
5.00-6.00 Team 1. Facility visit to MSIM (NGO) RH fee for service clinic
Team 2. Facility visit to IPPF/MFWA (NGO) RH fee for service clinic
Kh. Enkhjargal B. Tsevelmaa -2
6.00 Back to Hotel Program for Tuesday, 23 June 8:45 am Hotel Pick up and Proceeds to office of “Em holboo”
(Team 1) and 2nd Maternity hospital (Team 2) Driver
9.00-10.45 Team 1: Meeting with Mongolian Pharmaceuticals Association
Team 2: Meeting with Midwifes Association
Amarjargal Buyanjargal Driver for Team 1: Driver for Team 2:
11.00-12.30 Visit Family Clinic and pharmacy
Visit ANC of Chingeltei District Health Center and pharmacy
A.Bold
1:00-2:30 Lunch 3.00-4.30 Attend in the meeting of WG on EMOC study in the MoH
A. Bold
5:00-6.00 Team de-briefing and preparation for field visit UNFPA CO A. Bold Wednesday, 24 June Field Team 1. Orkon:
Kabir, Enkhjargal, Yanjinsuren, Altantuya
Field Team 2. Khentii: Anna Ridge, Amarjargal, Bold, Tsevelmaa, Kang Nam, Kim Kwan
Driver Team 1: Driver Team 2:
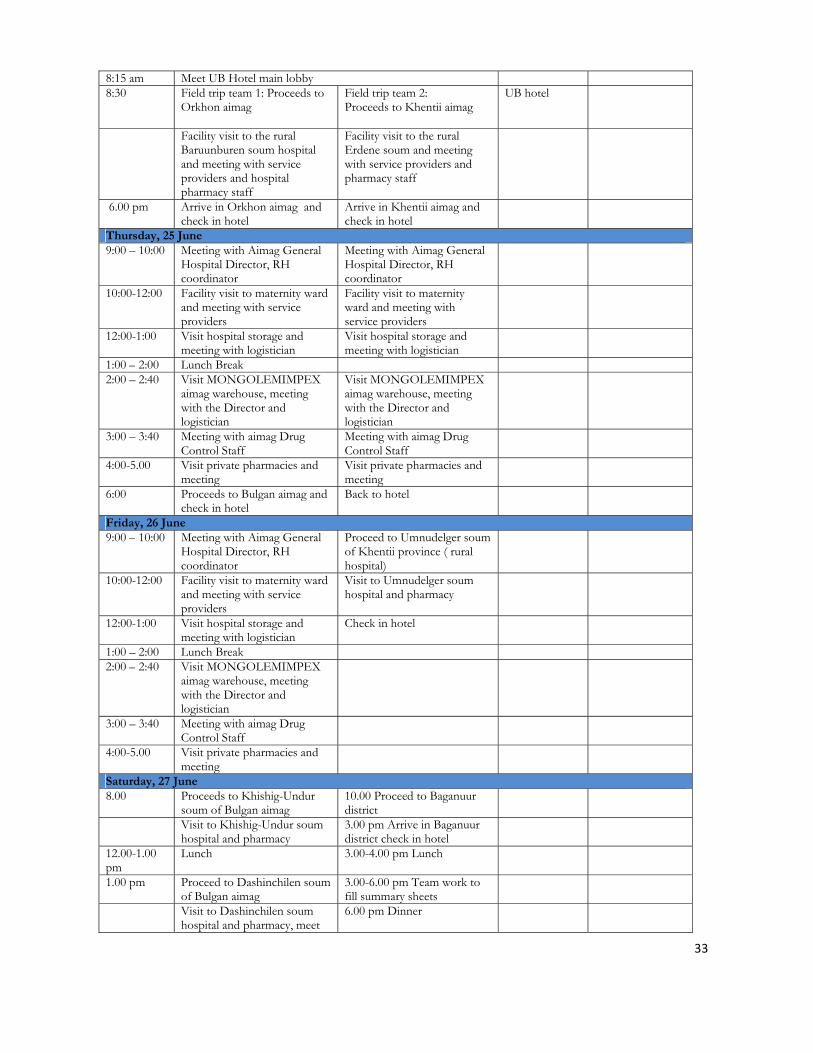
33
8:15 am Meet UB Hotel main lobby 8:30 Field trip team 1: Proceeds to
Orkhon aimag
Field trip team 2: Proceeds to Khentii aimag
UB hotel
Facility visit to the rural Baruunburen soum hospital and meeting with service providers and hospital pharmacy staff
Facility visit to the rural Erdene soum and meeting with service providers and pharmacy staff
6.00 pm Arrive in Orkhon aimag and check in hotel
Arrive in Khentii aimag and check in hotel
Thursday, 25 June 9:00 – 10:00 Meeting with Aimag General
Hospital Director, RH coordinator
Meeting with Aimag General Hospital Director, RH coordinator
10:00-12:00 Facility visit to maternity ward and meeting with service providers
Facility visit to maternity ward and meeting with service providers
12:00-1:00 Visit hospital storage and meeting with logistician
Visit hospital storage and meeting with logistician
1:00 – 2:00 Lunch Break 2:00 – 2:40 Visit MONGOLEMIMPEX
aimag warehouse, meeting with the Director and logistician
Visit MONGOLEMIMPEX aimag warehouse, meeting with the Director and logistician
3:00 – 3:40 Meeting with aimag Drug Control Staff
Meeting with aimag Drug Control Staff
4:00-5.00 Visit private pharmacies and meeting
Visit private pharmacies and meeting
6:00 Proceeds to Bulgan aimag and check in hotel
Back to hotel
Friday, 26 June 9:00 – 10:00 Meeting with Aimag General
Hospital Director, RH coordinator
Proceed to Umnudelger soum of Khentii province ( rural hospital)
10:00-12:00 Facility visit to maternity ward and meeting with service providers
Visit to Umnudelger soum hospital and pharmacy
12:00-1:00 Visit hospital storage and meeting with logistician
Check in hotel
1:00 – 2:00 Lunch Break 2:00 – 2:40 Visit MONGOLEMIMPEX
aimag warehouse, meeting with the Director and logistician
3:00 – 3:40 Meeting with aimag Drug Control Staff
4:00-5.00 Visit private pharmacies and meeting
Saturday, 27 June 8.00 Proceeds to Khishig-Undur
soum of Bulgan aimag 10.00 Proceed to Baganuur district
Visit to Khishig-Undur soum hospital and pharmacy
3.00 pm Arrive in Baganuur district check in hotel
12.00-1.00 pm
Lunch 3.00-4.00 pm Lunch
1.00 pm Proceed to Dashinchilen soum of Bulgan aimag
3.00-6.00 pm Team work to fill summary sheets
Visit to Dashinchilen soum hospital and pharmacy, meet
6.00 pm Dinner
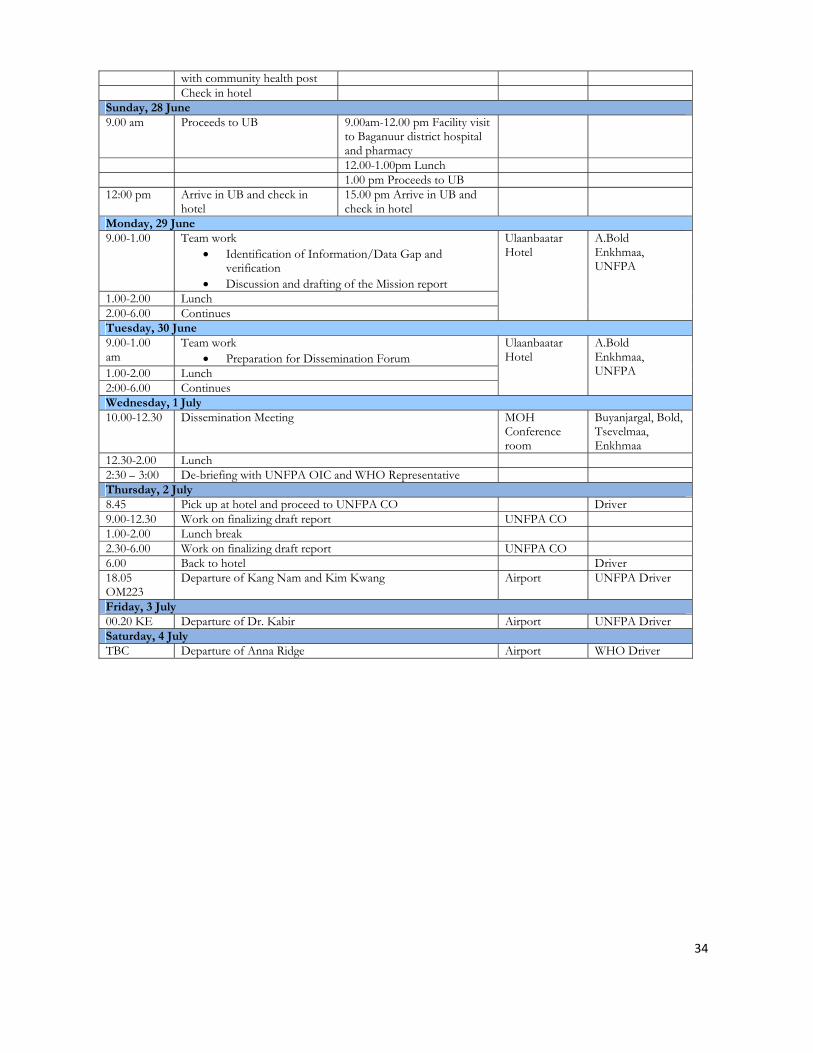
34
with community health post Check in hotel Sunday, 28 June 9.00 am Proceeds to UB 9.00am-12.00 pm Facility visit
to Baganuur district hospital and pharmacy
12.00-1.00pm Lunch 1.00 pm Proceeds to UB 12:00 pm Arrive in UB and check in
hotel 15.00 pm Arrive in UB and check in hotel
Monday, 29 June 9.00-1.00 Team work
• Identification of Information/Data Gap and verification
• Discussion and drafting of the Mission report
Ulaanbaatar Hotel
A.Bold Enkhmaa, UNFPA
1.00-2.00 Lunch 2.00-6.00 Continues Tuesday, 30 June 9.00-1.00 am
Team work • Preparation for Dissemination Forum
Ulaanbaatar Hotel
A.Bold Enkhmaa, UNFPA 1.00-2.00 Lunch
2:00-6.00 Continues Wednesday, 1 July 10.00-12.30 Dissemination Meeting MOH
Conference room
Buyanjargal, Bold, Tsevelmaa, Enkhmaa
12.30-2.00 Lunch 2:30 – 3:00 De-briefing with UNFPA OIC and WHO Representative Thursday, 2 July 8.45 Pick up at hotel and proceed to UNFPA CO Driver 9.00-12.30 Work on finalizing draft report UNFPA CO 1.00-2.00 Lunch break 2.30-6.00 Work on finalizing draft report UNFPA CO 6.00 Back to hotel Driver 18.05 OM223
Departure of Kang Nam and Kim Kwang Airport UNFPA Driver
Friday, 3 July 00.20 KE Departure of Dr. Kabir Airport UNFPA DriverSaturday, 4 July TBC Departure of Anna Ridge Airport WHO Driver
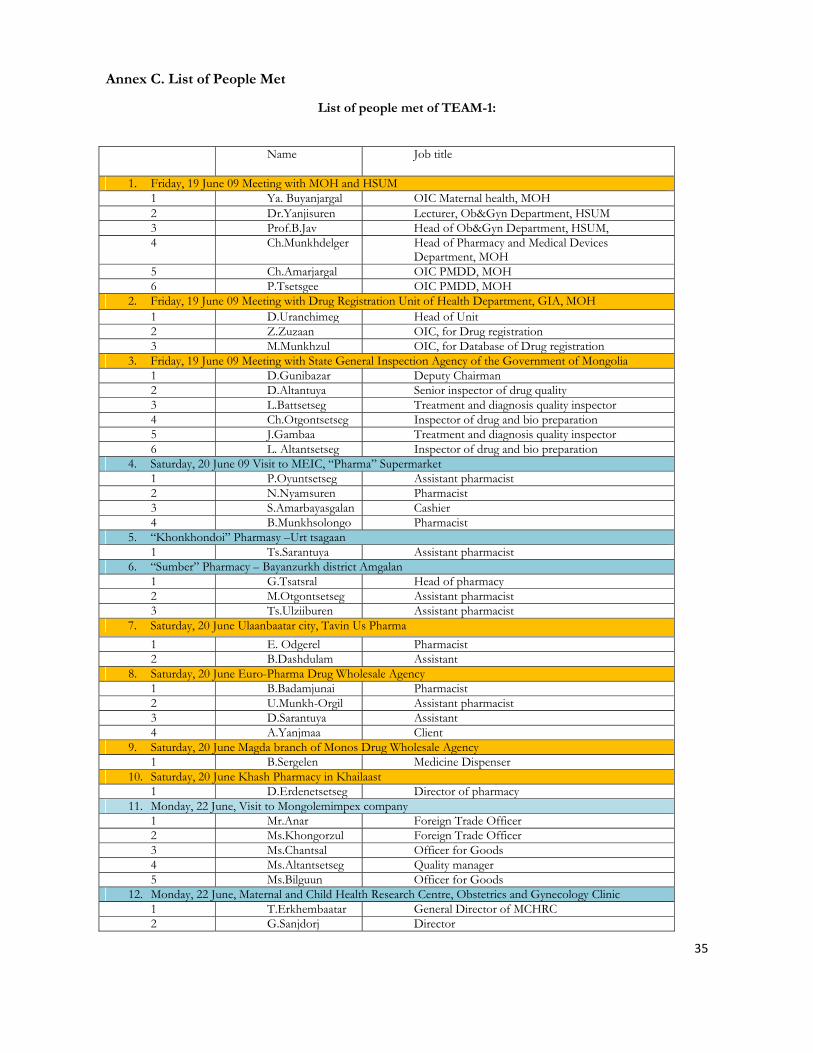
35
Annex C. List of People Met
List of people met of TEAM-1:
Name Job title
1. Friday, 19 June 09 Meeting with MOH and HSUM1 Ya. Buyanjargal OIC Maternal health, MOH 2 Dr.Yanjisuren Lecturer, Ob&Gyn Department, HSUM 3 Prof.B.Jav Head of Ob&Gyn Department, HSUM, 4 Ch.Munkhdelger Head of Pharmacy and Medical Devices
Department, MOH 5 Ch.Amarjargal OIC PMDD, MOH 6 P.Tsetsgee OIC PMDD, MOH
2. Friday, 19 June 09 Meeting with Drug Registration Unit of Health Department, GIA, MOH 1 D.Uranchimeg Head of Unit2 Z.Zuzaan OIC, for Drug registration 3 M.Munkhzul OIC, for Database of Drug registration
3. Friday, 19 June 09 Meeting with State General Inspection Agency of the Government of Mongolia 1 D.Gunibazar Deputy Chairman 2 D.Altantuya Senior inspector of drug quality 3 L.Battsetseg Treatment and diagnosis quality inspector 4 Ch.Otgontsetseg Inspector of drug and bio preparation 5 J.Gambaa Treatment and diagnosis quality inspector 6 L. Altantsetseg Inspector of drug and bio preparation
4. Saturday, 20 June 09 Visit to MEIC, “Pharma” Supermarket 1 P.Oyuntsetseg Assistant pharmacist 2 N.Nyamsuren Pharmacist3 S.Amarbayasgalan Cashier 4 B.Munkhsolongo Pharmacist
5. “Khonkhondoi” Pharmasy –Urt tsagaan1 Ts.Sarantuya Assistant pharmacist
6. “Sumber” Pharmacy – Bayanzurkh district Amgalan 1 G.Tsatsral Head of pharmacy 2 M.Otgontsetseg Assistant pharmacist3 Ts.Ulziiburen Assistant pharmacist
7. Saturday, 20 June Ulaanbaatar city, Tavin Us Pharma 1 E. Odgerel Pharmacist 2 B.Dashdulam Assistant
8. Saturday, 20 June Euro-Pharma Drug Wholesale Agency 1 B.Badamjunai Pharmacist2 U.Munkh-Orgil Assistant pharmacist 3 D.Sarantuya Assistant4 A.Yanjmaa Client
9. Saturday, 20 June Magda branch of Monos Drug Wholesale Agency 1 B.Sergelen Medicine Dispenser
10. Saturday, 20 June Khash Pharmacy in Khailaast 1 D.Erdenetsetseg Director of pharmacy
11. Monday, 22 June, Visit to Mongolemimpex company 1 Mr.Anar Foreign Trade Officer 2 Ms.Khongorzul Foreign Trade Officer3 Ms.Chantsal Officer for Goods 4 Ms.Altantsetseg Quality manager5 Ms.Bilguun Officer for Goods
12. Monday, 22 June, Maternal and Child Health Research Centre, Obstetrics and Gynecology Clinic 1 T.Erkhembaatar General Director of MCHRC2 G.Sanjdorj Director

36
3 S.Bayasgalan Quality manager4 Ts.Solongo Pharmacist 5 S.Amarmandakh Advisor Doctor of Reanimation Department 6 B.Tsedenkhorloo Advisor Doctor of 1st Maternity Ward 7 L.Chuluunbadam Midwife of 1st Maternity Ward 8 Kh.Baldanjav Director of Hospital Pharmacy9 D.Ganchimeg Medicine Dispenser
7. Monday, 22 June, Ach Pharm Trade pharmacy1 S.Altantuya Medicine Dispenser
8. Monday, 22 June, Khatagtai Private Maternity Hospital 1 A.Otgonbold Advisor Doctor 2 D.Ichinkhorloo Director3 L.Ayurzana Anesthesiologist 4 Kh.Daariimaa Ob&Gyn doctor
9. Monday, 22 June, Marie Stops NGO Clinic 1 E.Bolormaa Manager2 I.Oyumaa Nurse 3 T.Davaajav Ob&Gyn doctor 4 S.Unurmaa Ob&Gyn doctor5 Ts.Erdenebat Project manager
10. Tuesday, 23 June, United Association of Pharmacies of Mongolia1 O.Damba Executive director
11. Wednesday, 24 June, Visit to Baruunburen soum hospital of Selenge aimag 1 N.Otgonsuren Hospital director2 S.Battur Midwife
12. Thursday, 25 June, Visit to Orkhon aimag Health Department1 G.Gankhuyag Head of Department 2 Dr.Enkhjargal Officer for training and IEC 3 U.Delgermaa RH Coordinator4 Ms.Oyunchimeg Officer for Medicine
13. Thursday, 25 June, Visit to Orkhon aimag General Hospital1 L.Ganbold Advisor doctor of Ob&Gyn Department 2 Dr.Erdenebulgan Head of Ob&Gyn Department3 Dr.Darisuren Ob&Gyn doctor of 2nd Maternity ward 4 S.Lkhagvasuren Ob&Gyn doctor of 2nd Maternity ward 5 Ts.Tuya Midwife of 1st Maternity ward6 D.Uyanga Neonatologist 7 Sh.Bayarmaa Director of Pharmacy8 B.Baasanbat Pharmacist
14. Thursday, 25 June, Visit to Orkhon Medicine Supply Co LTD 1 Sh.Jiidee Director2 P.Baterdene General pharmacist 3 B.Oyunzul Director of pharmacy
15. Thursday, 25 June, Visit to Mednbulag FGP of Orkhon aimag 1 D.Oyunsaikhan Director of FGP 2 T.Enkhtuya Family doctor
16. Thursday, 25 June, Visit to Enkhjin clinic 1 Dr.Buyan-Ulzii Ob&Gyn doctor
17. Thursday, 25 June, Visit to Orkhon branch of Monos Pharm Trade company 1 Yu. Narantuya Director2 J.Tsetsgee Sale person of supermarket
18. Thursday, 25 June, Visit to State Inspection Department of Orkhon aimag 1 B.Buyantsogt Head of Department for health, education, food,
animal husbandry and manufacture inspections 2 D.Erdenetungalag Inspector for diagnosis and treatment quality
inspection 3 Yo.Erdenechimeg Inspector for medicine and bio-preparation quality
inspection
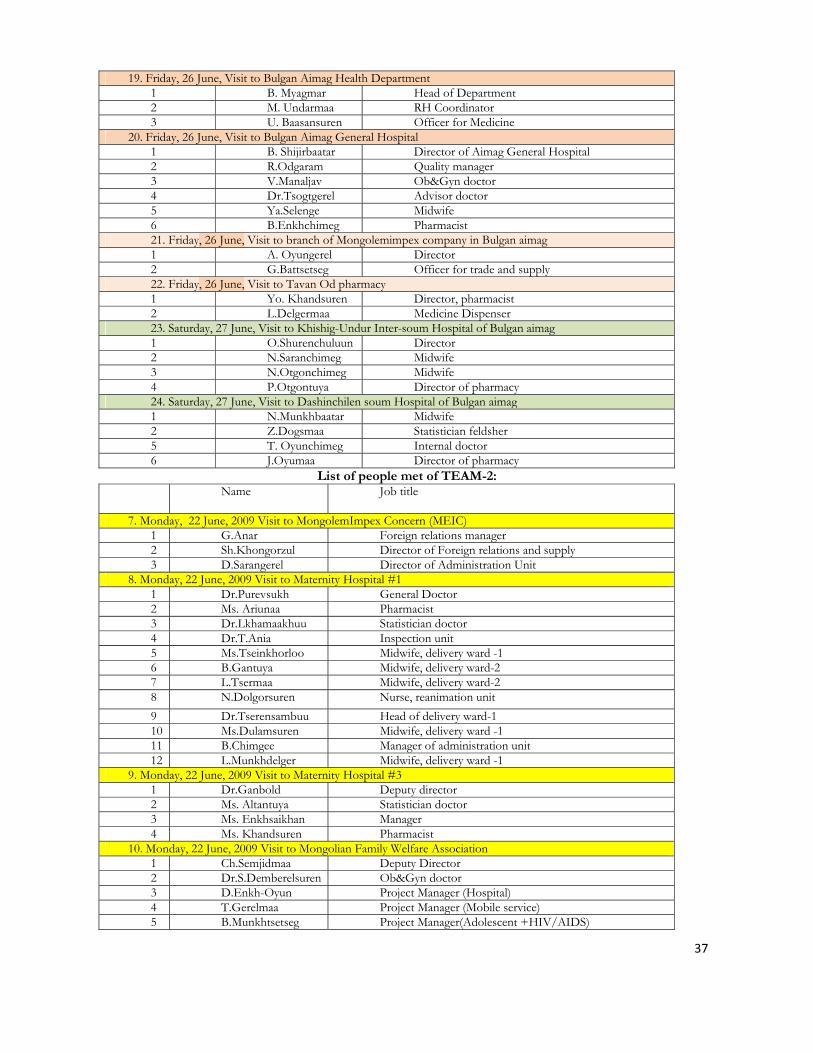
37
19. Friday, 26 June, Visit to Bulgan Aimag Health Department1 B. Myagmar Head of Department 2 M. Undarmaa RH Coordinator 3 U. Baasansuren Officer for Medicine
20. Friday, 26 June, Visit to Bulgan Aimag General Hospital 1 B. Shijirbaatar Director of Aimag General Hospital 2 R.Odgaram Quality manager 3 V.Manaljav Ob&Gyn doctor4 Dr.Tsogtgerel Advisor doctor 5 Ya.Selenge Midwife 6 B.Enkhchimeg Pharmacist 21. Friday, 26 June, Visit to branch of Mongolemimpex company in Bulgan aimag 1 A. Oyungerel Director2 G.Battsetseg Officer for trade and supply 22. Friday, 26 June, Visit to Tavan Od pharmacy 1 Yo. Khandsuren Director, pharmacist2 L.Delgermaa Medicine Dispenser 23. Saturday, 27 June, Visit to Khishig-Undur Inter-soum Hospital of Bulgan aimag1 O.Shurenchuluun Director 2 N.Saranchimeg Midwife 3 N.Otgonchimeg Midwife4 P.Otgontuya Director of pharmacy 24. Saturday, 27 June, Visit to Dashinchilen soum Hospital of Bulgan aimag1 N.Munkhbaatar Midwife 2 Z.Dogsmaa Statistician feldsher5 T. Oyunchimeg Internal doctor 6 J.Oyumaa Director of pharmacy
List of people met of TEAM-2: Name Job title
7. Monday, 22 June, 2009 Visit to MongolemImpex Concern (MEIC) 1 G.Anar Foreign relations manager 2 Sh.Khongorzul Director of Foreign relations and supply 3 D.Sarangerel Director of Administration Unit
8. Monday, 22 June, 2009 Visit to Maternity Hospital #11 Dr.Purevsukh General Doctor 2 Ms. Ariunaa Pharmacist 3 Dr.Lkhamaakhuu Statistician doctor 4 Dr.T.Ania Inspection unit 5 Ms.Tseinkhorloo Midwife, delivery ward -16 B.Gantuya Midwife, delivery ward-2 7 L.Tsermaa Midwife, delivery ward-28 N.Dolgorsuren Nurse, reanimation unit9 Dr.Tserensambuu Head of delivery ward-110 Ms.Dulamsuren Midwife, delivery ward -1 11 B.Chimgee Manager of administration unit12 L.Munkhdelger Midwife, delivery ward -1
9. Monday, 22 June, 2009 Visit to Maternity Hospital #31 Dr.Ganbold Deputy director2 Ms. Altantuya Statistician doctor 3 Ms. Enkhsaikhan Manager4 Ms. Khandsuren Pharmacist
10. Monday, 22 June, 2009 Visit to Mongolian Family Welfare Association1 Ch.Semjidmaa Deputy Director 2 Dr.S.Demberelsuren Ob&Gyn doctor 3 D.Enkh-Oyun Project Manager (Hospital)4 T.Gerelmaa Project Manager (Mobile service) 5 B.Munkhtsetseg Project Manager(Adolescent +HIV/AIDS)

38
6 G.Munkhzul Finance Manager7 Mr.Zolbayar IEC officer 8 Ms.Narantsetseg Pharmacist (part time) 9 Ms.Tsetsegmaa Midwife10 Ms.Ganchimeg Nurse 11 Ms.Dulamjav Assistant12 J.Batbold Driver
11. Tuesday, 23 June, 2009 Meeting with Mongolian Midwifes Association1 S. Davaasuren Midwife, Maternity Hospital #22 Ms.Ichinkhorloo Midwife, Maternity Hospital #1 3 Ms.Alinch bish Midwife, Maternity Hospital #24 Ms.Oyungerel Midwife, Maternity Hospital #1
12. Tuesday, 23 June, 2009 Visit to ANC of Chingeltei District Health Alliance and Pharmacy 1 D.Nemekhbat Director of Outpatient Department 2 B.Ulambayar Foreign relation manager 3 Dr.Ariumaa Ob&Gyn doctor4 Dr.Dorjkhand Ob&Gyn doctor 13. Wednesday, 24 June, 2009 Visit to Erdene soum hospital of Tuv aimag1 D. Badamkhand Director, General doctor 2 D.Narantsetseg Midwife 3 Ts.Tserenkhand Nurse4 Ts.Ulzii Nurse Thursday, 25 June, Visit to Khentii Aimag General Hospital1 T.Bolormaa Director of Aimag Health Department 2 T.Urnaa Deputy Director AHD3 N.Ariunaa Advisor doctor 4 J.Kherlentsetseg Quality manager of Treatment 5 Ts. Amgalanbuyan Ob&Gyn doctor6 T.Ouynbileg Head of Ob&Gyn department 7 Kh.Mandakh Neonatologist8 D.Purevdorj Ob&Gyn doctor 9 Ts.Jadambaa Midwife (RH) 10 Ch.Enkh-Amgalan Ob&Gyn doctor11 D.Munkhchimeg Officer of AHD Friday, 26 June, Visit to Umnudelger soum hospital of Khentii aimag1 D.Munguntsatsral Director 2 J.Atartuya Ob&Gyn doctor3 D.Ichinnorov Midwife4 Dr.Javsanragchaa Pediatrician 5 B. Uugantstseg Officer of Public HealthSunday, 28 June, Baganuur District Hospital of UB city 1 T.Budmaa Head of Ob&Gyn department2 N.Selengesuljee Neonatologist 3 B.Bumaa Senior nurse 4 D.Shinebayar General practitioner 5 J.Narantsetseg Midwife 6 D.Altanzagas Midwife7 D.Sarantuya Midwife 8 T.Altanzul Midwife 9 D.Enkhtuya Nurse 10 P. Battsetseg Nurse 11 Kh.Narantsetseg Nurse12 B.Bayarsaikhan Nurse 13 P. Erdenetsetseg Nurse14 D.Ouyntuya Nurse15 B.Lkhagva Nurse 16 Dr.Badamtsetseg General practitioner

39
Annex D. Key Documents Reviewed
1. Annual report, NSO, 2008 2. Assessment of medicines regulatory system, Mission Report, Mr Jun Yoshida, Technical Officer, Mr
EshetuWondemagegnehu, Technical Officer and Focal PersonWHO Headquarters, Ulaanbaatar, Mongolia, June 2005
3. Clinical guidelines, ADB, 2005 4. Diagnosis and treatment of newborns, WHO 5. Ensuring drug accessibility, quality and safety, presented by Ms T. Gandhi, Minister of Health at the 5th
Conference of the National Drug Policy. 6. Essential and Complementary Package of Services, MoH, Mongolia, 2004 7. Integrated Management of Pregnancy and Childbirth Pregnancy, Childbirth, Postpartum and Newborn Care: A
guide for essential practice, World Health Organization, Geneva, 2006 8. Implementation of Clinical Pharmacy Curriculum in the Health Sciences University of Mongolia, , Mission
Report, Dr Syed Azhar Syed Sulaiman, WHO Consultant, Ulaanbaatar, Mongolia, September 2005 9. Good Manufacturing Practices (GMP), Mission Report, Mr Alain Kupferman
WHO Consultant, Ulaanbaatar, Mongolia, July 2007 10. Guideline for pregnancy, delivery, postnatal and neonatal care, WHO, 2002 11. Government Policy on Drugs, State Great Khural Resolution No. 68 of 2002 12. Health Sector Strategic Master Plan, Implementation Framework, 2006-2010, MoH, Mongolia 13. Health Indicators, 2008, MoH, Mongolia 14. Law of Mongolia on Health, 1998 15. Law of Mongolia on Medicines and Medical Devices, 1998 16. Management of pregnancy and delivery complications, UNFPA, WHO, 2001 17. Maternal mortality reduction strategy, 2005-2010 18. Mid-term Review of UNFPA’s 4th Country Programme of Assistance for Mongolia, 2007-2011, May 2009 19. Mongolia Pharmaceutical Sector Assessment Report, Ministry of Health, December 2004; 20. National RH Commodity Security Strategy 2009-2013, MoH, Mongolia, 2009
21. Order of the Minister of Health Mongolia: Approval of the revised rules for drug registration, 7 July 2003, No.177;
22. Protocol of inspection; 23. Revised Drug Law (draft); 24. Rule for issuing import license for medicines and medical equipment (Appendix of the degree 296 of the
Minister of Health, 13 December 2002) 25. Rules of the National Drug Council (Appendix 2 to the Government Resolution 121 of 1998); 26. Rules and operational procedures for inspection 2003 (Order of the Minister of Inspection); 27. The Introduction of the State Specialized Inspection Agency, Regulatory Agency of the Government of
Mongolia; 28. Third National Reproductive Health Programme, 2007-2011 29. The Fifth List of National Essential Drugs, 2005 30. United Nations Joint Programme on Maternal and Newborn Health in Mongolia, 2009-2011 31. 1 World Health Organization. 2000. Integrated Management of Pregnancy and Childbirth. Managing Complications in
Pregnancy and Childbirth. A guide for midwives and doctors. Geneva: World Health Organization 32. 1 World Health Organization. 2006. Pregnancy, childbirth, postpartum and newborn care: a guide for essential practice. 2nd ed.
Geneva: World Health Organization 33. Why did women die?, ADB, MCHRC, 2006

40
Annex E. Checklists (Health Facility; Medical Stores/Pharmacies; National Level questionnaire for RH Medicine Procurement, Product Specific Survey)
REPRODUCTIVE HEALTH COMMODITIES SURVEY ( Health Facility Survey )
Country: City: Date of survey:
Name of health facility
Data collector name: Contact email:
Health facility type:
SPECIALIZED HOSPITAL SOUM HOSPITAL Maternity Ward
DISTRICTHOSPITAL PRIVATE CLINIC Obs and Gynae ward
AIMAG HOSPITAL Labour ward Neonatal unit
Other (specify)…………………………………………………………………………..
1. Assessing level of need and demand Estimated workload of facility Number in last year
(June 2008 - June 2009) Comment on how numbers were verified
(Records reviewed or verbal report) Pregnant women attending for ANC at facility
Women who deliver at facility
Number of cases of pre-eclampsia in last year
Number of cases of eclampsia in last year
Number of cases of PPH in last year
Number of cases of maternal sepsis/severe infections in last year
Number of cases of neonatal sepsis/severe infections in last year
• Does the facility provide 24 hour care? Yes No • Is the facility a designated provider of emergency obstetric care? Yes No
Please indicate the total number of healthcare workers currently employed for the management of obstetric and neonatal care in the health facility:
Current members of staff Total number Staff on duty at time of visit Obstetrician General Doctor Medical officer Midwife Staff Nurse Healthcare assistant Other (please specify)
2. Availability of treatment guidelines/protocols/training manual
a) Copy of Essential Medicine List available and year of publication:
Yes No
Year of publication:_______________
b) Copy of Standard Treatment Guideline available and year of publication:
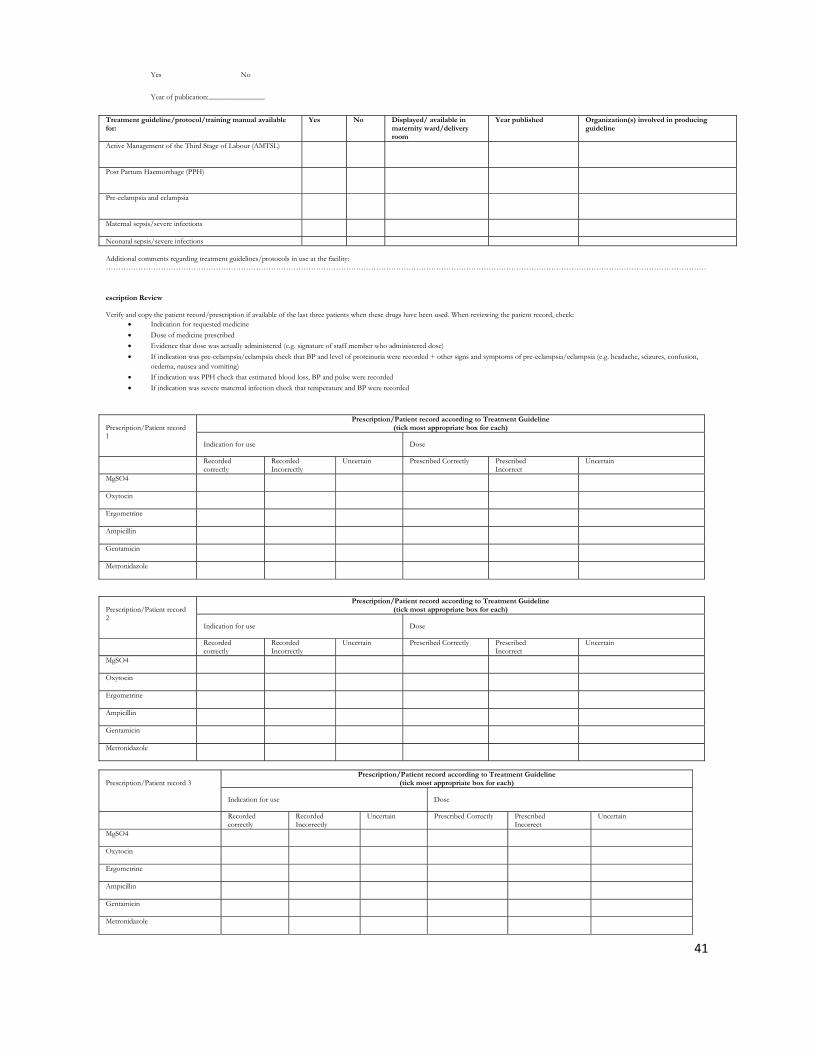
41
Yes No
Year of publication:_______________
Treatment guideline/protocol/training manual available for:
Yes No Displayed/ available in maternity ward/delivery room
Year published Organization(s) involved in producing guideline
Active Management of the Third Stage of Labour (AMTSL)
Post Partum Haemorrhage (PPH)
Pre-eclampsia and eclampsia
Maternal sepsis/severe infections
Neonatal sepsis/severe infections Additional comments regarding treatment guidelines/protocols in use at the facility: ……………………………………………………………………………………………………………………………………………………………………………………………………………………
escription Review Verify and copy the patient record/prescription if available of the last three patients when these drugs have been used. When reviewing the patient record, check:
• Indication for requested medicine • Dose of medicine prescribed • Evidence that dose was actually administered (e.g. signature of staff member who administered dose) • If indication was pre-eclampsia/eclampsia check that BP and level of proteinuria were recorded + other signs and symptoms of pre-eclampsia/eclampsia (e.g. headache, seizures, confusion,
oedema, nausea and vomiting) • If indication was PPH check that estimated blood loss, BP and pulse were recorded • If indication was severe maternal infection check that temperature and BP were recorded
Prescription/Patient record 1
Prescription/Patient record according to Treatment Guideline (tick most appropriate box for each)
Indication for use Dose
Recorded correctly
Recorded Incorrectly
Uncertain Prescribed Correctly PrescribedIncorrect
Uncertain
MgSO4
Oxytocin
Ergometrine
Ampicillin
Gentamicin
Metronidazole
Prescription/Patient record 2
Prescription/Patient record according to Treatment Guideline (tick most appropriate box for each)
Indication for use Dose
Recorded correctly
Recorded Incorrectly
Uncertain Prescribed Correctly PrescribedIncorrect
Uncertain
MgSO4
Oxytocin
Ergometrine
Ampicillin
Gentamicin
Metronidazole
Prescription/Patient record 3
Prescription/Patient record according to Treatment Guideline (tick most appropriate box for each)
Indication for use Dose
Recorded correctly
Recorded Incorrectly
Uncertain Prescribed Correctly PrescribedIncorrect
Uncertain
MgSO4
Oxytocin
Ergometrine
Ampicillin
Gentamicin
Metronidazole
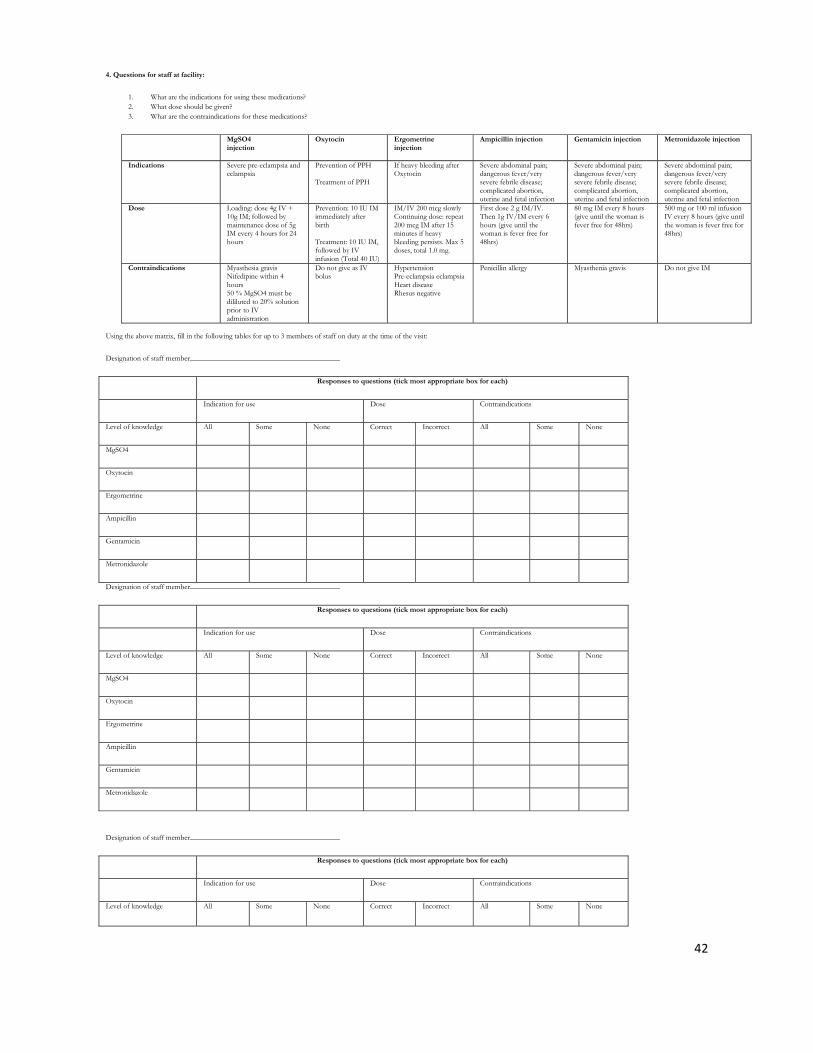
42
4. Questions for staff at facility:
1. What are the indications for using these medications? 2. What dose should be given? 3. What are the contraindications for these medications?
MgSO4 injection
Oxytocin Ergometrineinjection
Ampicillin injection Gentamicin injection Metronidazole injection
Indications Severe pre-eclampsia and eclampsia
Prevention of PPH Treatment of PPH
If heavy bleeding after Oxytocin
Severe abdominal pain; dangerous fever/very severe febrile disease; complicated abortion, uterine and fetal infection
Severe abdominal pain; dangerous fever/very severe febrile disease; complicated abortion, uterine and fetal infection
Severe abdominal pain; dangerous fever/very severe febrile disease; complicated abortion, uterine and fetal infection
Dose Loading: dose 4g IV + 10g IM; followed by maintenance dose of 5g IM every 4 hours for 24 hours
Prevention: 10 IU IM immediately after birth Treatment: 10 IU IM, followed by IV infusion (Total 40 IU)
IM/IV 200 mcg slowlyContinuing dose: repeat 200 mcg IM after 15 minutes if heavy bleeding persists. Max 5 doses, total 1.0 mg.
First dose 2 g IM/IV. Then 1g IV/IM every 6 hours (give until the woman is fever free for 48hrs)
80 mg IM every 8 hours (give until the woman is fever free for 48hrs)
500 mg or 100 ml infusion IV every 8 hours (give until the woman is fever free for 48hrs)
Contraindications Myasthesia gravis Nifedipine within 4 hours 50 % MgSO4 must be dililuted to 20% solution prior to IV administration
Do not give as IV bolus
HypertensionPre-eclampsia eclampsia Heart disease Rhesus negative
Penicillin allergy
Myasthenia gravis Do not give IM
Using the above matrix, fill in the following tables for up to 3 members of staff on duty at the time of the visit:
Designation of staff member________________________________________
Responses to questions (tick most appropriate box for each)
Indication for use Dose Contraindications
Level of knowledge All Some None Correct Incorrect All Some None
MgSO4
Oxytocin
Ergometrine
Ampicillin
Gentamicin
Metronidazole
Designation of staff member________________________________________
Responses to questions (tick most appropriate box for each)
Indication for use Dose Contraindications
Level of knowledge All Some None Correct Incorrect All Some None
MgSO4
Oxytocin
Ergometrine
Ampicillin
Gentamicin
Metronidazole
Designation of staff member________________________________________
Responses to questions (tick most appropriate box for each)
Indication for use Dose Contraindications
Level of knowledge All Some None Correct Incorrect All Some None
43
MgSO4
Oxytocin
Ergometrine
Ampicillin
Gentamicin
Metronidazole
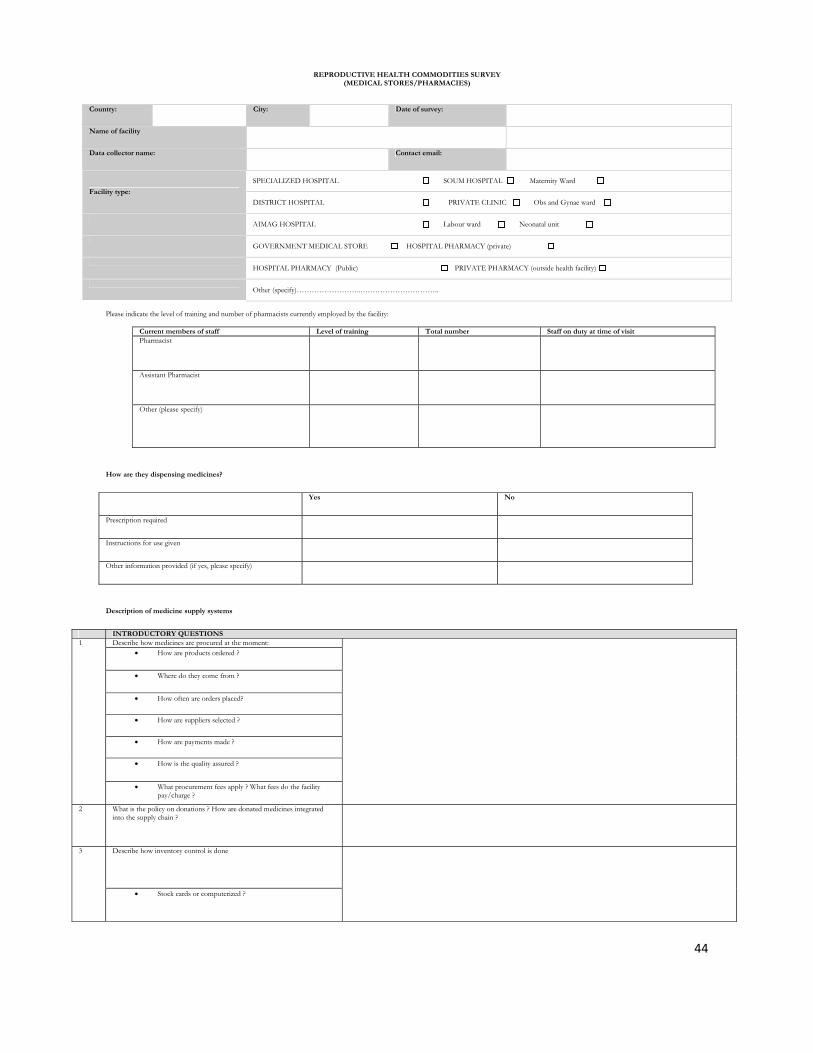
44
REPRODUCTIVE HEALTH COMMODITIES SURVEY (MEDICAL STORES/PHARMACIES)
Country: City: Date of survey:
Name of facility
Data collector name: Contact email:
Facility type:
SPECIALIZED HOSPITAL SOUM HOSPITAL Maternity Ward
DISTRICT HOSPITAL PRIVATE CLINIC Obs and Gynae ward
AIMAG HOSPITAL Labour ward Neonatal unit
GOVERNMENT MEDICAL STORE HOSPITAL PHARMACY (private)
HOSPITAL PHARMACY (Public) PRIVATE PHARMACY (outside health facility)
Other (specify)……………………..…………………………..
Please indicate the level of training and number of pharmacists currently employed by the facility:
Current members of staff Level of training Total number Staff on duty at time of visit Pharmacist
Assistant Pharmacist
Other (please specify)
How are they dispensing medicines?
Yes No
Prescription required
Instructions for use given
Other information provided (if yes, please specify)
Description of medicine supply systems
INTRODUCTORY QUESTIONS 1 Describe how medicines are procured at the moment:
• How are products ordered ?
• Where do they come from ?
• How often are orders placed?
• How are suppliers selected ?
• How are payments made ?
• How is the quality assured ?
• What procurement fees apply ? What fees do the facility pay/charge ?
2 What is the policy on donations ? How are donated medicines integrated into the supply chain ?
3 Describe how inventory control is done
• Stock cards or computerized ?
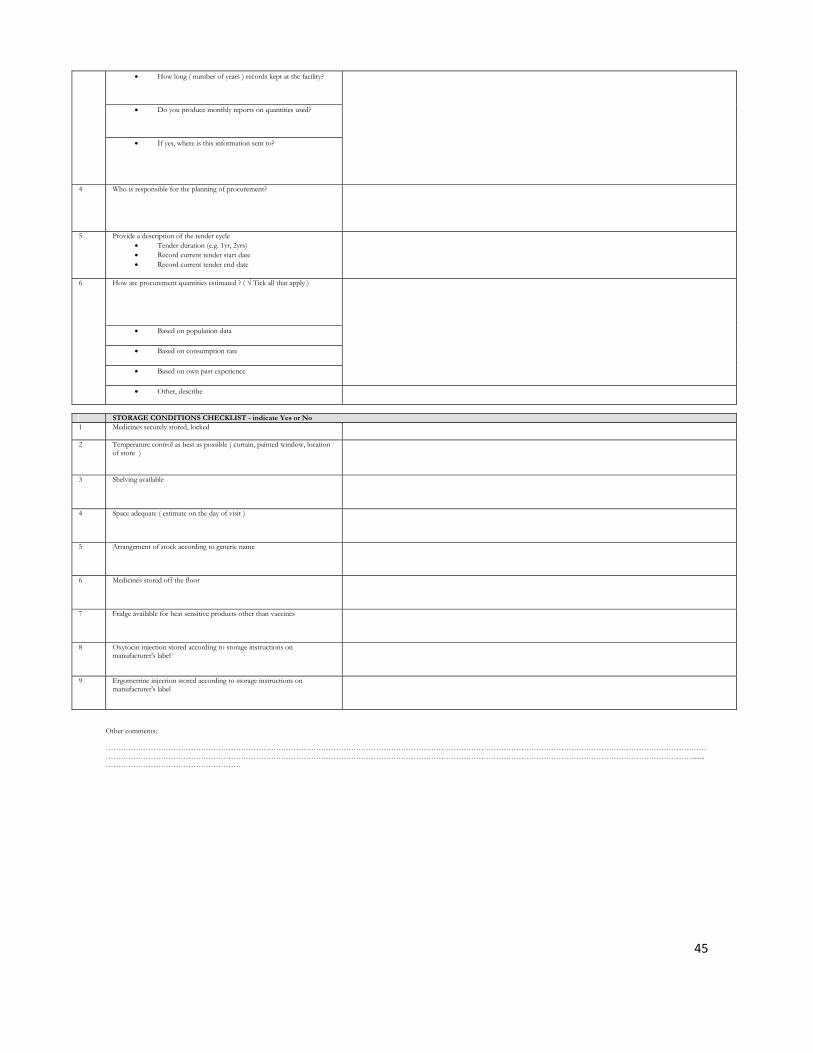
45
• How long ( number of years ) records kept at the facility?
• Do you produce monthly reports on quantities used?
• If yes, where is this information sent to?
4 Who is responsible for the planning of procurement?
5 Provide a description of the tender cycle • Tender duration (e.g. 1yr, 2yrs) • Record current tender start date • Record current tender end date
6 How are procurement quantities estimated ? ( √ Tick all that apply )
• Based on population data
• Based on consumption rate
• Based on own past experience
• Other, describe
STORAGE CONDITIONS CHECKLIST - indicate Yes or No 1 Medicines securely stored, locked
2 Temperature control as best as possible ( curtain, painted window, location
of store )
3 Shelving available
4 Space adequate ( estimate on the day of visit )
5 Arrangement of stock according to generic name
6 Medicines stored off the floor
7 Fridge available for heat sensitive products other than vaccines
8 Oxytocin injection stored according to storage instructions on manufacturer's label
9 Ergometrine injection stored according to storage instructions on manufacturer's label
Other comments: ……………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………........………………………………………………
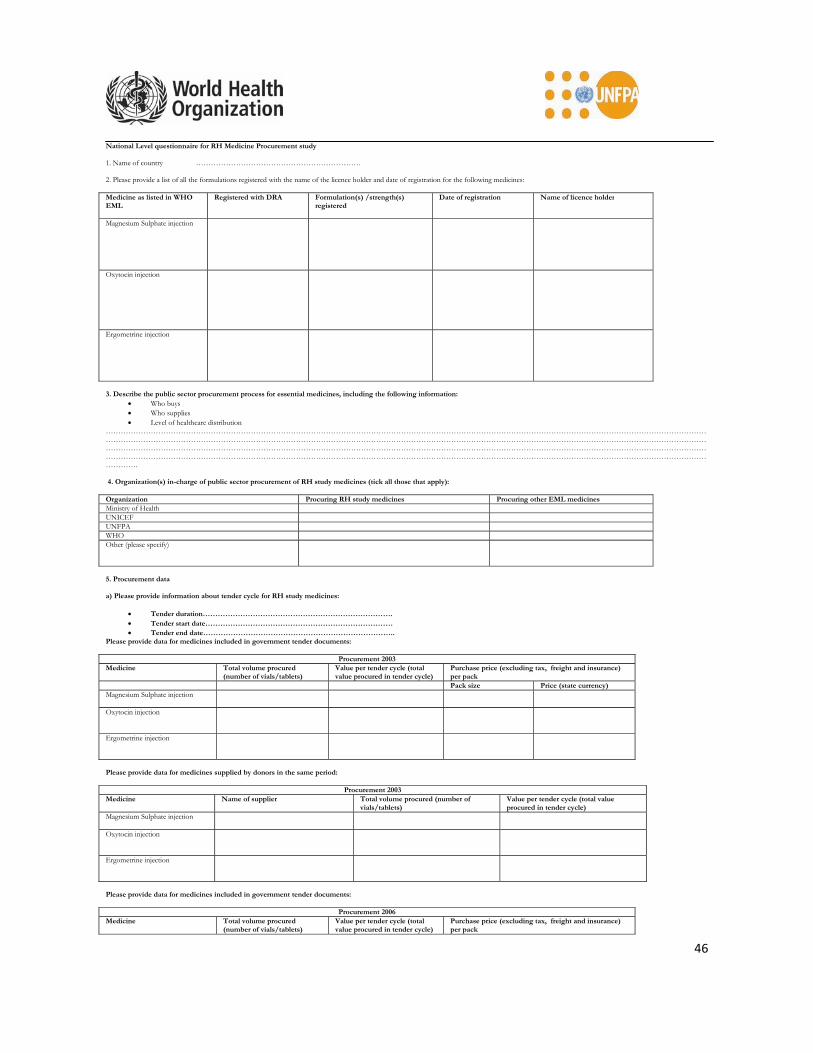
46
National Level questionnaire for RH Medicine Procurement study 1. Name of country ………………………………………………………… 2. Please provide a list of all the formulations registered with the name of the licence holder and date of registration for the following medicines: Medicine as listed in WHO EML
Registered with DRA Formulation(s) /strength(s) registered
Date of registration Name of licence holder
Magnesium Sulphate injection
Oxytocin injection
Ergometrine injection
3. Describe the public sector procurement process for essential medicines, including the following information:
• Who buys • Who supplies • Level of healthcare distribution
………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………. 4. Organization(s) in-charge of public sector procurement of RH study medicines (tick all those that apply): Organization Procuring RH study medicines Procuring other EML medicines Ministry of Health UNICEF UNFPA WHO Other (please specify)
5. Procurement data a) Please provide information about tender cycle for RH study medicines:
• Tender duration…………………………………………………………………. • Tender start date………………………………………………………………… • Tender end date…………………………………………………………………..
Please provide data for medicines included in government tender documents:
Procurement 2003Medicine Total volume procured
(number of vials/tablets) Value per tender cycle (total value procured in tender cycle)
Purchase price (excluding tax, freight and insurance) per pack
Pack size Price (state currency) Magnesium Sulphate injection
Oxytocin injection
Ergometrine injection
Please provide data for medicines supplied by donors in the same period:
Procurement 2003Medicine Name of supplier Total volume procured (number of
vials/tablets) Value per tender cycle (total value procured in tender cycle)
Magnesium Sulphate injection
Oxytocin injection
Ergometrine injection
Please provide data for medicines included in government tender documents:
Procurement 2006Medicine Total volume procured
(number of vials/tablets) Value per tender cycle (total value procured in tender cycle)
Purchase price (excluding tax, freight and insurance) per pack
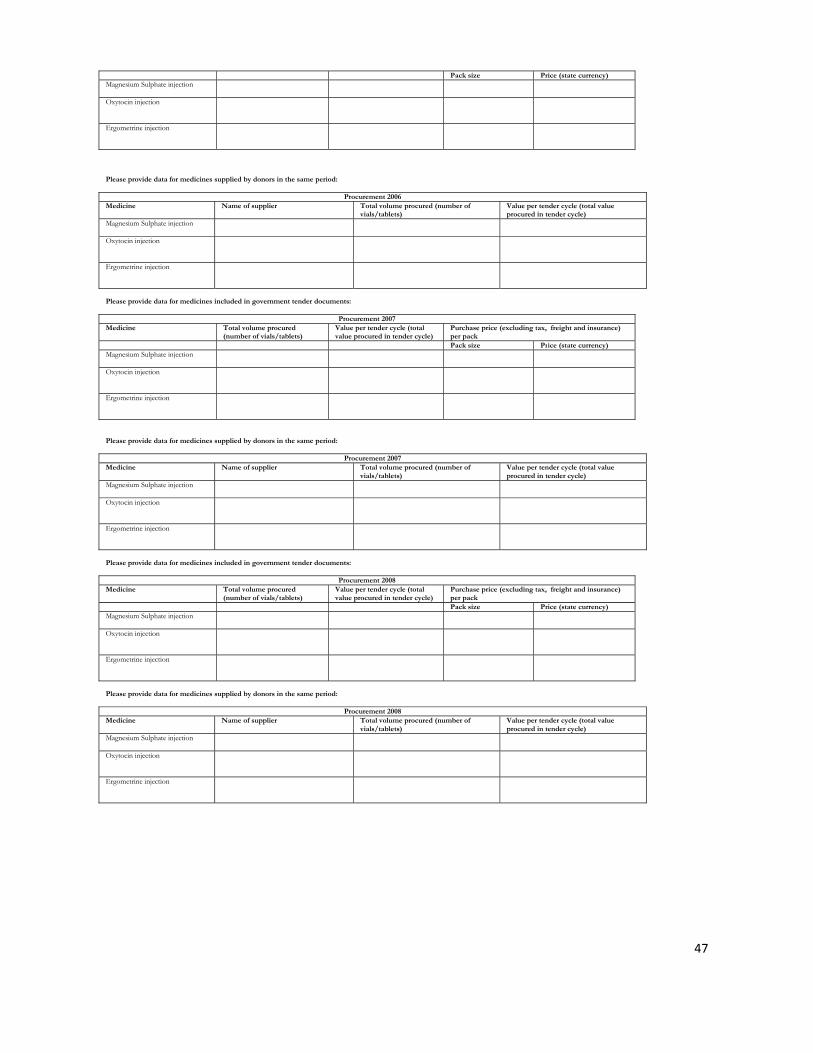
47
Pack size Price (state currency) Magnesium Sulphate injection
Oxytocin injection
Ergometrine injection
Please provide data for medicines supplied by donors in the same period:
Procurement 2006Medicine Name of supplier Total volume procured (number of
vials/tablets) Value per tender cycle (total value procured in tender cycle)
Magnesium Sulphate injection
Oxytocin injection
Ergometrine injection
Please provide data for medicines included in government tender documents:
Procurement 2007Medicine Total volume procured
(number of vials/tablets) Value per tender cycle (total value procured in tender cycle)
Purchase price (excluding tax, freight and insurance) per pack
Pack size Price (state currency) Magnesium Sulphate injection
Oxytocin injection
Ergometrine injection
Please provide data for medicines supplied by donors in the same period:
Procurement 2007Medicine Name of supplier Total volume procured (number of
vials/tablets) Value per tender cycle (total value procured in tender cycle)
Magnesium Sulphate injection
Oxytocin injection
Ergometrine injection
Please provide data for medicines included in government tender documents:
Procurement 2008Medicine Total volume procured
(number of vials/tablets) Value per tender cycle (total value procured in tender cycle)
Purchase price (excluding tax, freight and insurance) per pack
Pack size Price (state currency) Magnesium Sulphate injection
Oxytocin injection
Ergometrine injection
Please provide data for medicines supplied by donors in the same period:
Procurement 2008Medicine Name of supplier Total volume procured (number of
vials/tablets) Value per tender cycle (total value procured in tender cycle)
Magnesium Sulphate injection
Oxytocin injection
Ergometrine injection

48
REPRODUCTIVE HEALTH COMMODITIES SURVEY ( Facility Survey - Product Specific )
Country: City: Date of survey:
Name of facility
Data collector name: Contact email:
Facility type:
SPECIALIZED HOSPITAL SOUM HOSPITAL Maternity Ward
DISTRICT HOSPITAL PRIVATE CLINIC Obs and Gynae ward
AIMAG HOSPITAL Labour ward Neonatal unit
GOVERNMENT MEDICAL STORE HOSPITAL PHARMACY (private)
HOSPITAL PHARMACY (Public) PRIVATE PHARMACY (outside health facility)
Other (specify)……………………..…………………………..
PRODUCT SPECIFIC QUESTIONS Magnesium
Sulphate injection
Calcium Gluconate injection
Oxytocin injection
Ergometrine injection
Ampicillin injection
Gentamicin injection
Metronidazole injection
1 Supplier of product on shelf ( manufacturer )**
2 Strength of product on shelf (mg) 3 Volume of product on shelf (ml/vial) 4 Number of vials / tablets per pack (pack size) 5 Expiration date of product on the shelf 6 Total number of packs on the shelf on day of
visit
7 Total number of vials procured
a • In 2008
b • In 2007
c • In 2006
d • In 2003
8 Value procured (state currency procured in) a • Last 12 months
b • Last 3 years
9 Are there problems with expired stock a • Number of expired vials/tablets
on day of visit
b • Number of expired vials/tablets in last 12 months
10 Number of days out of stock a • Last 3 months
b • Last 12 months 11 Purchase price as per invoice, excl freight,
insurance
12 How much will patient pay today (per vial / tablet or capsule) ?
13 How often are stocks checked by a higher authority? (record date of last stock check and name/designation of higher authority)
• Every 6 months • Once a year • Never • Other
**All supplier/manufacturer names of the individual medicines available on the day of the visit should be recorded, including expiration date and cost of the product

49
Annex F. List of Acronyms
UNFPA United Nation’s Fund for Population Activities
RH Reproductive Health
MOH Ministry of Health,
MSI Marie Stops International Mongolia
CO Country Office
HQ Headquarter
AVSC Int The Association for Voluntary Surgical Contraception International
HMIS Health Management Information System
USD United States Dollar
GIA Government Implementation Agency
FGP Family Group Practices
MEIC Mongolemimpex Concern
MFOG Mongolian Federation of Obstetrics and Gynecology Doctors
IV Intravenus
IM Intramuscular
ADB Asian Development Bank
WB World Bank
WHO World Health Organization
UNICEF The United Nations Children's Fund
JICWELS Japan International Corporation of Welfare Services,
MFWA Mongolian Family Welfare Association
UB Ulaanbaatar IPPF International Planned Parenthood Federation RDF Revolving Drug Fund NFS Not for sale UNDAF United Nations Development Assistance Framework RHCS Reproductive Health Commodity Security
HSUM Health Sciences University of Mongolia
OIC Officer in Charge
EML Essential Medicines List
IU International Unit

50
AMTSL Active Management of Third Stage of Labour
DTC Drug and Therapeutic Committee
MoF Ministry of Finance
LMIS Logistics Management Information System
MCH Maternal and Child Health
NSO National Statistics Office
PPH Post-partum Haemorrhage
NGO Non Governmental Organizaion
HSMP Health Sector Master Plan
ANC Antenatal care
STGs Standard Treatment Guidelines
Ob&Gyn Obstetrics and Gynecology
MCHRC Maternal and Child Health Research Centre
PCPNC The Pregnancy, Childbirth, Postpartum and Neonatal Care
DPRK Democratic People’s Republic of Korea
IMPAC Integrated Management of Pregnancy and Childbirth
WG Working group
EmOC Basic Emergency Obstetric Care

51
Annex G. Map of Mongolia
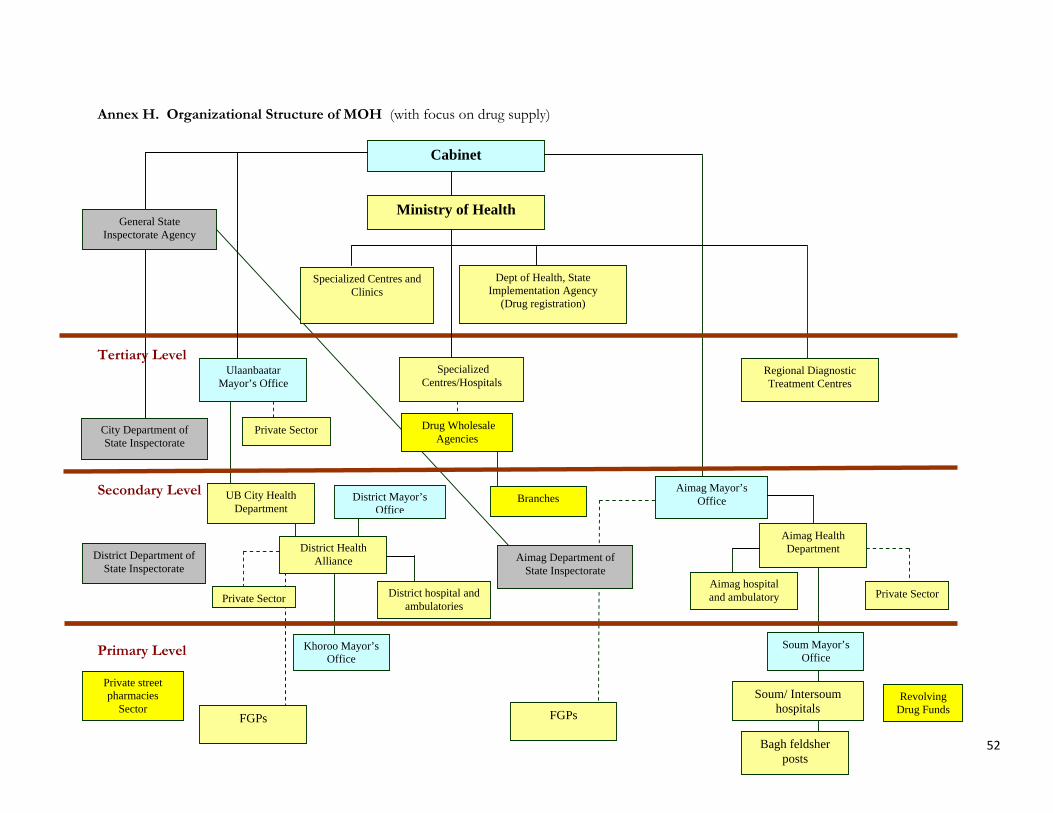
Annex H. Organizational Structure of MOH (with focus on drug supply)
Tertiary Level Secondary Level Primary Level
Dept of Health, State Implementation Agency
(Drug registration)
District Department of State Inspectorate
Aimag Department of State Inspectorate
Private street pharmacies
Sector Revolving
Drug Funds
Specialized Centres and Clinics
Drug Wholesale Agencies
Branches Aimag Mayor’s
Office District Mayor’s Office
District hospital and ambulatories
Khoroo Mayor’s Office
Soum Mayor’s Office
District Health Alliance
Aimag Health Department
UB City Health Department
Private Sector
Specialized Centres/Hospitals
Ulaanbaatar Mayor’s Office
Bagh feldsher posts
Soum/ Intersoum hospitals
Aimag hospital and ambulatory
FGPs
Private Sector
Regional Diagnostic Treatment Centres
Private Sector
Cabinet
Ministry of Health General State
Inspectorate Agency
City Department of State Inspectorate
FGPs
52

Annex I. List of People Attended/Participated in Dissemination Meeting
29 June 2009, MoH, Meeting Hall
# Name and Organization Position Ministry of Health
1 S.Tugsdelger Head of Public Health Policy Implementation Department2 Ch.Munkhdelger Head of Medicine and Medical Devices Division 3 Ya.Amarjargal Deputy Head of Medical Services Policy Implementation
Department 4 G. Tsetsegdari OIC, Public Health Policy Implementation Department 5 Z.Zuzaan OIC, for Drug registration, GIA, Health Department, MoH 6 M.Munkhzul OIC, for Database of Drug registration, GIA, Health
Department, MoH 7 Т. Erkhembaatar Director, MCHRC, MoH 8 S. Purevsukh Director, 1st Maternity Hospital9 D. Bat-Ochir Director, 3rd Maternity Hospital
International partners 10 Jose Ferraris OIC for Resident Representative, UNFPA 11 Wiwat Rojanapithayakorn Resident Representative, WHO 12 Yameen Mazumder UNICEF13 V. Surenchimeg UNICEF 14 Kabir Ahmed Team Leader, UNFPA HQ 15 Anna Ridge Team member, WHO, Geneva16 S. Navchaa Deputy Representative, UNFPA, Mongolia 17 Kh. Enkhjargal Program Officer, UNFPA, Mongolia18 B. Shinetugs RH consultant, , UNFPA, Mongolia 19 Ts. Enkhmaa Program Assistant20 D. Enkhchimeg Translator, UNFPA, Mongolia21 B. Tsedmaa Project Coordinator, UNFPA, Mongolia 22 D.Jargalsaikhan Director SHSDP, ADB
Associations and NGOs 23 O.Damba Executive Director, Em Association24 S. Davaasuren Executive Director, Mongolian Midwifes Association 25 B.Jav Board Member, MFOG 26 О.Bayanjargal Board Member, MFOG27 B.Bolormaa Executive Director, Mongolemimpex Concern 28 D.Bolormaa Project manager, MSI 29 А.Otgonbold Advisor doctor, Kharagtai Private Maternity Hospital
Team members 30 Ya.Buyanjargal OIC, Team member, Medical services Policy Implementation
Department 31 Ch. Amarjargal OIC, Team member, Medicine and Medical Devices Division 32 Kim Kwong Jin Team member, DPRK33 Kang Nam Team member, DPRK34 А.Bold Team member, UNFPA National consultant 35 B. Tsevelmaa Team member, UNFPA RH project staff 36 D.Altantuya Team member, Central Professional Inspectorate Agency 37 D.Yanjinsuren Team member, Lecturer of HSUM38 Kh. Daariimaa Team member, Lecturer of HSUM
53