report no. 6089-tu turkey health sector...
TRANSCRIPT

Report No. 6089-TU
TurkeyHealth Sector Review
September 1%!, 1986
Population, Health and Nutrition Department
FOR OFFICIAL USE ONLY
Document of the World Bank
This document has a restricted distribution and may be used by recipientsonly in the performance of their official duties. Its contents may not otherwisebe disclosed without World Bank authorization.
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

Tm~
(Annual Averages)
Value of UST Turkish Lira
1980 76.01981 111.21982 162.61983 225.51984 366.71985 542e0
FISCA4 TEAR
January 1 - December 31
NMI ACRORME USED IEN TEN REP=R
BAG-KJR - Social Insurance Agency of Merchants, Artisans andSelf Employed Professionals
GmS - Compulsory Medical ServiceGERF - Government Employees Retirement FundGDPHC - General Directorate for Primary Health CareGDMCHFP - General Directorate for Maternal and Child Health
and Family PlanningIHSS - Integrated Healths Services SchemeILO - International Labor OrganizationMCH - Maternal and Child HealthMOHSA - Ministry of Health and Social AssistanceMWRA - Married Women of Reproductive AgePHC - Primary Health CareSIO - Social Insurance OrganizationSIS - State Institute of StatisticsSPO ' State Planning OrganizationUNFPA - United Nations Fund for Population ActivitiesUNICEF - United Nations Children OrganizationWHO - World Health OrganizationYOK - Higher Education Council

FOR OFFICIUL USE ONLYT 9 R K x I
REALTR SECTOR RR11EV
TABIZ OF CoIIED
Page
EXECUTIVE SUNNARY ..... ............................... 5
I. HEALTH, NUTRITION AND FERTILITY STATUS
A. Sector Background ........................ ........ 10B .Health .........% * a. * ll *0*0.00s
C. Nutrition ......... 15D. Fertility ........ .. , 17E. Environmental Factors .............. ##.* ...... 19
II. SECTORAL POLICIES AND OBJECTIVES
A. Health ......** ....**, O#*** *******.....****, 21B. Nutrition ............ .......................... 23C. Population ** *** ***C** 9904 *9#940.......0**.00*...9 24
III. SECTORAL ORGANIZATION
A. The Ministry of Health and Social Assistance ..... 26B. The Medical Schools *,****************........... 29C. The Social Security System ....................... 30D. The Private Sector .............................. 36E. Management Systems and Issues ................... 39
IV. SECTORAL RESOURCES
A. Health Personnel ....... .............***. 44B. Health Facilities .** ............................ 49C. Health Costs and Financing ...................... 51D. Pharmaceuticals ..... 55
V. LAYING THE FOUNDATIONS OF A DEVELOPMENT STRATEGY 59
A. Improving Coordination of Sectoral Activities ... 61B. Strengthening Investment Planning ............... 61C. Focussing on Priority Areas in Primary Health Care 66D. Increasing Hospital Utilization ................. 67E. Adiusting Users Charges .......................... 73F. Strengthening Social Security's Financial Basis *. 76G. Outlining a Program of Applied Research ......... 80
This report vas prepared by Messrs. Louis G. Vassiliou, dt4)1 DeGeyndt, Dr. Jean Pillet (PHN), Dr. Jean Lecomte and Prof. Kamil Turan(Consultants), following a mission to Turkey in October 1985.
This document has a restricted distribution and may be used by recipients only in the performanceof their official duties. Its contents may not otherwise be disclosed without World Bank authorization.

-4-
LIST OF TABLES
1: Basic PHN Indicators for Turkey and Selected Countries2: Demographic Characteristics3: Evolution of Food Consumntion4: Consumption Levels by Regions, and Urban and Rural Areas5: New FP Acceptors by Method and Year in MDHSA Facilities6: New FP Acceptors by Method and Region in MORSA Facilities7: Distribution of Married Women Practicing Contraception by
Exposure Status8: Distribution of Female Contraceptive Users, by Method9: Health Pereonnel (Public and Private Sectors)10: Distribution of General Practitioners and Specialists11: Distribution of MORSA Personnel by Categories12: Evolution and Regional Distribution of Physicians13: Health Infrastructure (Public and Private Sectors)14: Hospitals and Beds by Type15: Hospitals and Beds, by Ownership16: Hospitals Under-Construction in October 198517: MOHSA and General Budget (1976-1984)18: Budget of Ministry of Health and Social Assistance19: Distribution of MOHSA Expenditure in 1984 and 198520: Public Investments in the Health Sector (1980-1986)21: Health Sector Investment Program22: Investment Program of MOHSA23: Fee Echedule for Selected MORSA Medical Services in 1985 and
Real Increase or Decrease Since 198124: Universal Old-Age and Disability Pension Scheme - Number of
Beneficiaries and Benefits Paid25: Social Insurance Organization: Contributors and Beneficiaries26: SIO: Total, Health and Maternity ContributionsZI: SIO: Annual Operating Expenditure on Health Facilities28: GERP: Beneficiaries and Benefits29: BAG-KUR - Contributors, Beneficiaries and Benefits30: Hospital Utilization Indicators by Provider31: Hospital Utilization Indicators by Type of Facility32: Hospital Infrastructure and Utilization by Province33: University Hospital Infrastructure and Utilization34: Expense per Patient Day and Per Bed for a Sample of Hospitals
GRAPHS
1: Contributions & Beneficiaries - Social Insurance Organization2: User Charges Funds
ORGANIZATIONAL CHARTS
1: Ministry of Realth and Social Assistance2: Provincial Health Services

-5-
T U RK I T
RBAL?T SECTOR RBVIlV
xRCUTIVI SUsmARY
Substantial improvements have been achieved in the health sectorover the past two decades and most Turkish indicators now compare favorablywith similar data for other middle-income countries. Nevertheless, strikinginequalities in health status, fertility levels, and access to basic healthcare still exist between Western and Eastern provinces, and between urbanand rural areas. Large segments of the population still suffer fromsurprisingly high infant and child mortality rates, persistent prevalence ofinfectious diseases, malnutrition, and relatively high levels of fertility.These are partially caused ane compounded by environmental problems ofpollution, sanitation and inadequate water supply, especially in periurbanareas. Future efforts should concentrate on measures to improve the healthstatus of lower income groups and residents of remote areas, to check thespread of infectious diseases, control common childhood diseases, and reducefertility among high risk women.
ii. Turkey's total population of 49 million is growing at an averagerate of 2.2X p.a. expected to fall to 1.9S for the 1980-2000 period.Improvements in the health status of the population are evidenced by a sharpincrease in life expectancy, now estimated at 63 years. Birth and deathrates declined substantially during the past two decades, to 31 and 9 perthousand, respectively. However, the infant mortality rate is still veryhigh, at 82 per thousand live births, and hides wide regional variations.Leading causes of infant mortality are perinatal complications, pneumonia,and diarrheal diseases; for child mortality, they are pneumonia, andinfectious diseases. Public health authorities recognize high priority tothree issues: the follow-up of the 1985 immunization campaign, the controlof tuberculosis, and the resurgence of malaria.
iii. The nation's food supplies provide a generous average of 3077calories per person/day. Between 1974 and 1982, daily per capita calorieintake increased from 2260 to 2400; but protein intake decreased from 85 to75 gr, while animal protein intake declined from 22.5 to 17.3 gr.Malnutrition remains the major contributing factor to child mortality; italso affects 35Z of pregnant women. But malnutrition does not appear ineasily identifiable pockets, groups or geographic regions. It appears to becorrelated with educational and cultural factors, and family and cookinghabits, rathet than income, food availability or distribution factors; thereis no evidence so far that recent declines in income levels have affectedthe nutritional status of the population. Nevertheless, malnutrition of
-6-
specific segments of the population and recent trends in consumptionpatterns call for close monitoring in coming years.
iv. Progress in contraception, rise in age of marriage, modernizinginfluences of education, urbanization and high levels of external migration,have led to a steady decline in the total fertility rate which now standsaround four. However, striking regional disparities persist; low fertilityrates and high levels of contraceptive prevalence in metropolitan areascoexist with high fertility rates in the rest of the country. The nationalcontraceptive prevalence rate is 34.1% for currently married women, and45.1% for women at risk. Yet, tFere is a large unmet need for familyplanning services, estimated at 2.2 million married women of reprodt.tiveage; it is illustrated by continuing high levels of induced abortions.Moreover, substantial gains in fertility reduction could be achieved througha shift to more effective methods.
v. In 1961, the Government introduced an Integrated Health ServiceScheme designed to unify under the same delivery system the servicesformerly provided by separate agencies. The ambitious goals set at thattime have not been met fully but the current Five Year Development Planreaffirmed Government's commitment to this policy; at the same time, itstated that access to family planning services should be improved; itsupported the expansion of the private sector, and encouraged thedevelopment of health insurance. However, except for some targets relatedto infrastructure, there are no quantified objectives in the Plan document.
vi. The health sector is notable for its complexity and lack ofcoordination between largely autonomous public and private organizations.There are more than thirty providers of health services in the publicsector: the Ministry of Health and Social Assistance, twenty one independentuniversity hospitals, the Social Insurance Organizatior, the Army, and otherministries and public organizations. Moreover, there is a very activeprivate sector which includes many foundations, religious groups and foreigncommunities which still operate their own facilities. Although tte Ministryof Health and Social Assistance is formally responsible for the design andimplementation of the country's health policy, its authority over theseservice providers remains rather limited.
vii. The country spends about 3.5% of its GNP on health, or some US$40per capita; this is less than most other middle income countries. Fiftyeight percent of these expenses are direct household outlays; most of publicexpenditures are channelled through the three major providers, i.e. theMinistry of Health (17%), the Social Insurance Organization (less than 12%)and university hospitals (about 8%). Annual investments in the publichealth sector as a whole decreased by almost 40% between 1982 and 1985although total public investments increased by 8% (in real terms). TheMinistry's budget alone declined by 13% in real terms Juring the 1976-84period, while total government expenditures were cut by 4%; it nowrepresents 3.1% of the general budget compared to 4.2% in 1978.
-7-
viii. Costs of outpatient and inpatient services are relatively low byinternational standards. Preventive care is provided free, but curativecare must be paid for, except by individuals recognized as indigents. Feesare higher in university hospitals than in public facilities; they are alsoadjusted regularly to keep pace with inflation. This is not the case forthe Ministry of Health where the last two adjustments were made in April1981 and January 1985.
ix. The Government is pursuing a determined poli.y to restructure andliberalize its economy and promote the privatization of activities which theprivate sector can handle more efficiently. However, while privatization inthe health field may be appropriate in some instances, this would not permitthe Government to extricate itself from the provision of health services orto reduce public health expenditures dramatically. We consider that theState should retain its fundamental responsibility in matters of preventivecare, containment of communicable diseases, provision of emergency servicesand ensuring access to basic health services by the poor. It is also in thenational interest to support programs to improve health and nutritionstandards, and to achieve fertility rates compatible with the country'sresources and development prospects. Finally, sustained public expendituresare needed to lay the foundations for a more efficient and equitable healthsystem.
X. The fundamental Government objective in the sector should be tostrengthen the effectiveness of the health care delivery system, with a viewto redressing existing inequalities in health status, fertility levels andaccess to basic health services, and further improving the overall status ofthe population. This can be achieved in spite of current stringent ecouomicand monetary policies. The strategy proposed to reach this objective isarticulated around six themes.
xi. First, the creation of a sectoral coordination mechanism should bea high priority. This could take the form of an interministerial HigherHealth Council, headed by the Prime Minister, with a permanent Secretasiatprovided by the Ministry of Health and Social Assistance. Its role would beto provide an appropriate forurt for in-depth discussion of availableoptions, advise the Government, and ensure coordination of sectoralinterventions.
xii. Second, the investment planning process must be improved. Basicinformation required by planners and policy makers is not readily available.No objective assessment can presently be made of the hospital constructionprogram. At the sectoral as well as the sub6ectoral level, insufficientattention is being paid to the justification of major projects and themonitoring of their implementation. There are presently 32 hospitals underconstruction; spreading limited funds over too many projects leads to majordelays before any of them can be completed. Furthermore, as civil worksabsorb the bulk of investments, there are few resources left to equip newfacilities, replace obsolete equipment, and purchase much needed vehicles.A crucial responsibility of the proposed Higher Health Council would be to

- 8 -
develop a consensus on sectoral investment priorities and on an optimalallocation of financial resources.
xiii. Pending the outcome of a critical evaluation of on-going andplanned projects. an immediate action program would include: (i) amoratorium on new hospital projects; (ii) an assessment of completion coats,operating expenses and manpower requirements of all on-going projects; (iii)the creation of an ad hoc technical group to scrutinize all on-goinghospital construction projects and, whenever appropriate. recommend scalingdown or abandoning altogether any project; (iv) delaying implementation ofprojects where sunk costs have not reached an agreed level; and (v) identifyareas for transferring funds freed by the above measures. paying particularattention to first level care in priority areas and target groups.
xiv. Third. better integration of services must be achieved, especiallyfor family planning and immunization. Effectiveness of primary health careservices at the outreach level is hampered by acute shortages of qualifiedmanpower, lack of vehicles and equipment. and insufficient supplies ofdrugs. Although implementation of the proposed program would requireadditional funds, the introduction of a cost recovery mechanism is notrecommended at this level.
xv. Fourth. increasing the utilization of existing hospital capacityis highly cost-effective and should receive highest priority. Conservativeestimates show that at least 20% more admissions could result from areduction in the average length of stay and a parallel increase in occupancyrates. This would necessitate a profound change in the philosophy ofhospital management, doctor's behavior. and structural reforms. But theproposed steps are realistic and include measures to improve: (i) thereferral system; (ii) the admission policy; (iii) hospital performance; (iv)bed utilization; and (v) to reorganize urban care. Such measures couldsignificantly reduce the need for new hospital construction.1
xvi. Fifth. the level and structure of the fee schedule applied inpublic facilities, for persons not recognized as indigents, must be adjustedto ensure proper and steady financing of health services. In a context ofhigh inflation. delaying adjustments of user charges results in asubstantial loss of revenue and wide fluctuations in hospital cash flow,which affects the quality of services and threatens the viability of thesystem. But frequent adjustments do not imply the setting up of an indexingmechanism. On the other hand, the whole structure of the fee scheduleapplied in public hospitals needs to be reexamined. The five year intervalbetween the last two adjustments has led to aberrations in charges leviedfor public services. On equity as well as social and economic grounds, itis fully justified to proceed with a gradual correction of existingdistortions.
1 The Government has already incorporated this recommendation among thepolicies of its current five year development plan.

-9-
xvii. Finally. strengthening the financial basis of the social securitysystem is a sine qua non to its survival. It still has considerable assetsestimated at US$1.5 billion although real rates of return on investments ofthe three major institutions were largely negative during the past decade;but its current deficit was estimated at US$1.8 billion in 1983. Thissituation resulted from a combination of factors which include legalconstraints. liberal lending policies to the members, generous benefits,conservative management and very high inflation rates. A major reform isunder consideration, which would extend health benefits to members of theSocial Insurance Agency for the Self-Employed and their dependents; at thesame time. an extended health insurance system is being proposed. In viewof the complexity and sensitivity of issues under discussion, only a widelyopen debate, based on an objective consideration of alternatives can lead toa national consensus on the future of the social security system, the natureand extent of its coverage, and tfe monetary implications of possibleoptions.
xviii. At a time when critical issues are being addressed and new avenuesexplored. and when decisions are called for which will radically affect thefuture of the sector, technical studies are needed to assist the Governmentin evaluating policy alternatives and their implications. - Priority areasfor research include disparities ia health and fertility indicators;hospital utilization; financing of health services; reform of the socialsecurity system; and national health insurance. Considerable expertise.which has so far not been tapped, already exists in the country. Butoutside consultants would also be useful to widen the perspective and takeadvantage of other countries' experience.
xix. Priority investment requirements for the sector are for: (i)design and implementation of primary health care interventions targeted tospecific areas and priority population groups; (ii) completion of highestpriority on-going projects. while deferring lower priority hospitalconstruction projects; (iii) equipping new facilities; (iv) launching aprogram for the gradual replacement of obsolete equipment; and (v) upgradingand expanding the Minist Irs fleet of vehicles. giving priority to outreachservices and supervision.
2 The Government has already incorporated this recommendation among thepolicies of its current five year development plan.

- 10 -
I. - =ALTR, NDTRTION AND )FUILITY STASMUS
A. Sector BEackgroimd
1. Turkey's total population of about 49 million, or 62 persons persquare kilometer, ranks it seventh in size among the middle-incomecountries, and first in the Bank's EMENA region. About 45% of thispokulation is urban (living in places of 20.000 persons or over). aproportion below the region's average; more than half the rural populationstill lives in communities of less than 1.000 inhabitants. The extensiveinternal migration of the last two decades. which originated largely fromthe northern and eastern provinces. has resulted in much higher densitiesand urbanization rates in the western part of the country. The rural-urbaninflow involved close to 3 million persons and contributed to thedeterioration of living conditions in "gecekondu" housing3 : by 1980. about65% of the population of Ankara lived in squatter settlements; thisproportion was 45% in Istanbul, 35% in Izmir. and between 20 and 40% in theother major cities. External migration, largely to West Germany. peaked inthe early 1970s at about 1.8 million. In 1977. more than 1 million Turkslived in West Germany, of which 40% were women and 36% children belowfifteen years of age; by the end of 1983, there were still more than 1million workers abroad; during that same year, more than 52.000 new migrantworkers left the country. mainly to Libya (23.000) and Saudi Arabia(20.000). The government continues to encourage emigration of its laborsurplus as these workers' remittances reached US$1.9 billion in 1984.
2. The first enumeration of the Turki h population took place in 1927and since 1935 censuses have been conducted regularly at five-yearintervals. Reliable vital statistics are maintained at the HacettepeInstitute of Population Studies in Ankara. In the 1960s. the natural rateof growth of Turkey's population averaged 2.5% p.a.; this rate declined to2.3% in the 1970s; emigration further reduced the overall rate of populationgrowth to 2.1% p.a. With the slowing down of external migration, the rateof growth of the resident population is now 2.22 p.a ; it is projected bythe World Bank at 1.9% p.a. for the 1980-2000 period ; this would yield a
3 Literally, "built in one night". These are housing built inviolation of the city plani without license. Housing standards aregenerally reasonable but these areas, at least initially. lack adequateinfrastructure and urban services.
4 The State Planning Organization's projections are based on a naturalrate of increase of 1.6% p.a. by the year 2000, derived from a crude birthrate of 22 and a crude death rate of 6 per thousand; this results in a totalpopulation of 66.9 million for that year (see "Country Report on PolicyObjectives and Measures Relevant to Population Trends of Turkey", StatePlanning Organization. June 1982).

- 11 -
total population of 65 millions by the end of the centory. The agingprocess of the population is illustrated by the proportion of children belowfifteen, which declined from 40.8% to 37.5% between 1973 and 1983.
3. Turkey compares favorably with Egypt and Iran, the other two mostpopulous countries of the region, on the selected indicators shown in Table1 (Tunisia, at the same level of per capita income, is also included in thetable). Life expectancy at birth is 61 years for males and 66 for females(compared to 49 and 52 years respectively in 1960); this is however belowSyrian and Jordanian levels. Mortality and fertility declined substantiallyduring the past two decades (40% and 262 respectively), although progresswas much slower for infant mortality. The crude death rate, which was 16per thousand in- 1960, now stands at 9 per thousand. The crude birth ratefell from 43 to 31 per thousand between 1960 and 1983, i.e. below theaverage for middle-income countries; however, it is still twice as high ascurrent rates in industrialized countries (14 per thousand on theaverage). The total fertility rate of 4.1 is again below the average formiddle-income countries, but substantially higher than in industrializedeconomies (1.7 in western countries and 2.3 in eastern European countries).
4. In recent years, improved productivity in agriculture, ruralmigration, and high rates of inflation which eroded real urban incomes, havesomewhat reduced income inequa'ities between rural and urban areas.Nevertheless, disparities between and within regions, and between the citiesand rural and periurban areas remain considerable and are apparent in allindicators. A good illustration is provided by literacy rates: nationalaverages were 75% for males and 48% for females in 1975, but 87% and 69%respectively in Istanbul province, and 35% and 8% in Hakkari province in theextreme southeast. In the early 1980s, per capita incomes were twice thenational average in the West, but less than haif the national average in theEast. These high disparities in terms of per capita incomes and educationallevels, as well as religious attitudes have direct bearing on health statusand demographic behavior.
3. Health
5. Improvements in the health status of the Turkish population areevidenced by the sharp increase in life expectancy. However, at 82 perthousand (184 in 1960), the infant mortality rate is substantially higherthan the rate recorded in industrialized countries (10-20 per thousand). In1975 for instance, 29% of all deaths reported at the provincial and districtlevel were of children under 1 year of age. Perinatal complications accountfor half of the reported cases of infant mortality; the second cause ofinfant deaths is pneumonia (181), followed by diarrheal diseases (8%), andother infectious diseases (5%), Regional variations are striking. In 1977for instance, while the overall infant mortality rate stood at 134 perthousand, it was 119 in urban areas, 146 in rural areas, 108 in the West,109 in the South, 151 in the Center, 141 in the North and 177 in the East of
- 12 -
the country. High infant mortality reflects, among other things, highfertility, low levels of brenatal care, improper delivery and feedingpractices, and environmental factors; they are also the consequ"nce ofunequal access to health services, often linked with the reluctance to usethem.
6. The child mortality rate (9 per thousand, compared to 47 in 1960)is just below the average for middle-income countries, but again much higherthan in industrialized countries (less than 1 per thousand). The majorcauses of child mortality are pneumonia, infectious diseases, accidents,diarrhea and malformations. These regiotered diagnoses point at theunderlying causes: incomplete immunizations, crowded housing, adverseenvironment, poor water supply and malnutrition. The high mortality bypneumonia and acute respiratory infections among infants and children callsfor increased attention, in health education programs, to the effects ofpassive smoking.
7. The causes of adult mortality are not well known as data refermainly to recorded cases in urban areas. Major causes of adult death arepneumonia, bronchitis, emphysema, asthma and malignant neoplasm. For thepopulation aged 45 and above, coronary diseases account for 40X of deaths;they are followed by malignant tumors (12%) and cerebrovascular diseases(8%); as many as 20X of cases are recordt.d as ill-defined, while the numberof coronary diseases is overestimated. At any rate, mortality bycardiovascular diseases, and the high incidence of lung cancer among adultmales are direct consequences of very high levels of tobacco consumption.Maternal mortality reflects inadequate obstetrical care, short intervalsbetween births, and high incidence of induced abortion.
8. Identified leading causes of infant morbidity are measles,diarrhea, intestinal infections and pneumonia, with malnutrition as acontributing factor. As regards adult morbidity, highest incidence refers toacute respiratory problems, diseases of genito-urinary system,gastroenteritis and diarrheal diseases. Some infectious and parasiticdiseases, such as plague, rabies, leprosy, trachoma and syphilis, have beenlargely controlled. Others, like hepatitis, typhoid, hydatidosis, areincreasing in spite of active control programs.
9. Public health authorities are presently concentrating theirefforts on three major problems: the follow-up of the immunization program;the control of tuberculosis; and the resurgence of malaria.
10. Until the end of 1985, is unixation coverage was extremely low.The only two compulsory vaccinations - against smallpox and typhoid - werediscontinued in 1981. No systematic immunization program was conducted byMOESA; the decision about vaccination was left entirely to the parents andonly the urban better educated who could bear the cost, had their childrenimmunized. In rural areas, the service was rarely available. In 1979 asample study showed that only 30% of the age group I to 5 w4s fullyimmunized against whooping cough, diphtheria, tetanus, measles,poliomyelitis and tuberculosis. More recent estimates by MOHSA on specific

- 13 -
disease coverage shoved 65% for tuberculosis, but 35% only for measles and32% for poliomyelitis, diphtheria, tetanus and whooping cougb. In fact,peripberal services lacked cold chain equipment, vehicles, trainedsupervisors end intersectoral support.
11. To face this critical situation, the government launcbed in 1985 anationwide "Expanded and Accelerated Immunization Program", witb the supportof the ministries of education, agriculture, industry, the private sectorand the ariy. The three-round campaign was also supported by UNICEF, WHO,bilateral donors and NGOs which, altogether, contributed over US$20 million.Four tillion doses of vaccine were produced by MOHSA and 16 million doseswere purchased or procured by donors. The campaign ended in December 1985;five million children were reached and full immunization could be as high as80%. Final costing of the operation and evaluation of immunity by bothserology and epidemiological data will permit a full assessment of this"expanded and accelerated" approach which has raised much interest in theinternational community. At any rate, MOHSA must now organize the follow-upof this operation; other campaigns at three or four year intervals areunlikely to succeed as popular support, intersectoral collaboration andforeign assistance would be difficult to mobilize. The solution lies in theintegration of immunizations into regular health services activities,especially now that the PHC system has benefited from the campaign in termsof know-how, vehicles, cold chain, and small equipment.
12. The second problem area is the control of tuberculosis. Incidenceof TB fell from 265 per 10,000 population in 1967 to 50 per 10,000 in 1978,but increased again slightly to 65 per 10,000 in 1983. Overcrowding, poorsanitation, and malnutrition linked to low incomes in periurban areas aremajor contributing factors; moreover, the high cost of treatment remainsinaccessible to large numbers of unemployed urban dwellers; these factorsare obviously beyond the control of the public health system. Although theapparent rapid decline as well as the resurgence are largely due to changesin the intensity of screening and case finding operations, the disease stillposes a serious threat: there were 130,000 registered cases in 1984 andprobably as many as 500,000 undetected cases. In spite of progress inambulatory treatments, 7,500 beds in general or chest hospitals are stilloccupied by TB patients. As at least 50% of births in rural areas are notattended by health personnel, increased BCG coverage could only be obtainedby strengthening the PHC system (i.e. the village midwife and healthcenters) and by intensifying screening and active case finding operations.The TB control program, with its 249 TB centers throughout the country, hasalready benefited from integration into PHC, but should be furtherstrengthened by additional facilities for massive bacterioscopy, forselective radiological control as well as provision of free drugs fortreatment of indigents.
13. Finally, a third concern of MOHSA is the resurgence of malariaduring the 1970s. Although Turkey was declared free of this disease in1970, large irrigation projects, particularly in Cukrova plain of Adanaprovince, and progressive reinfestation from the Syrian and Iraqi bordersswamplands, have reintroduced malaria in the country. Incidence rose

- 14 -
rapidly: 9,000 cases in 1975, 32,000 in 1976, and an epidemic of 115,500cases in 1977 led to a declaration of emergency and a call to WHO fortechnical assistance. Since then epidemics have been controlled butendemicity remains stable at 30,000 new cases per year. The complexmechanisms of the resurgence have been well analyzed: the impact ofagricultural and industrial development on the ecology; the movement of some600,000 seasonal and permanent migrant workers; and the resistance ofmosquitoes to usual insecticides. Malaria in South Eastern Turkey couldalso become a threat to tourism. It has caused international embarrassment,since infected migrant workers or truck drivers (about 40,000 trucks crossthe border every year) can spread the disease to Bulgaria, Yugoalavia, andeven Western Europe.
14. The Government has taken active steps to control the disease,earmarking 3X of MOHSA's budget for malaria control in 1985 (US$7.4million). The malaria program has been integrated with PHC, intensivespraying and screening are going on, amidst increasing resistance from thepopulation. For its part, the State Water Affairs Department (DSI) isactively pursuing drainage activities, including the costly maintenance ofextensive irrigation networks. To stop malaria transmission by 1989, fourinterventions have been designed:
- strengthen PEC programs, which cover control or surveillance inall infested or receptive areas, i.e. 37% of the country'spopulation;
- develop the mid-level management of malaria services, upgradingand strengthening the Adana Institute of Malariology to trainstaff at undergraduate and postgraduate levels, and perform as acoordinating center for malaria control and schistosomiasissurveillance;
- intensify drainage and spraying in the Cukrova region, incoordination with private industries and agricultural authorities;and finally
- complete, in 1986, the construction of nine pumping stations, tolower the ground water level of the Cukrova plain.
In addition, the Government is undertaking, with World Bank support, aproject for nation-wide improvement of drainage in irrigated areas.
15. MOHSA also fears infestation by schistosoma hematobium in existingand proposed large irrigation areas near the south-eastern borders.Nalacological surveillance has started and will have to increase asirrigation progresses.

- 15-
C. Nutrition
16. Turkey has always been a country of agricultural wealth, thereforenutrition was not considered a problem until demographic growth threatenedthe food balance. The nation's food supplies provide a generous 3077calories per person/day, the second highest among lower middle incomecountries. On the average, the population continues to be well fed,although actual consumption may have declined slightly in recent years.However, malnutrition of specific segments of population is a cause ofconcern.
17. The assessment of the nutritional status of the population isessentially based on the 1974 national survey carried out by HacettepeUniversity5. After 1976. small studies and surveys were carried out by theUniversity which also sponsored community programs, in Estimesgut. Cubuk andEswir for example, centered on mother and child malnutrition. In 1982. aSurvey on Food Consumption and Nutrition focussed on food availability (seeTable 3). New findings tend to confirm that malnutrition is correlated witheducational and cultural factors. and family and cooking habits, rather thanincome, food availability or distribution factors. All indicators are stillwell above minimum requirements, and the basic assumption is that recentdeclines in income levels have not. so far, affected the nutritional statusof the population; nevertheless, close monitoring of consumption will berequired over the coming years.
18. Between 1974 and 1982. daily per capita calorie intake increasedslightly from 2260 to 2400; but protein intake decreased from 85 to 75.3 gr.while animal protein intake declined from 22.5 to 17.3 gr. However, inspite of favorable national averages, malnutrition persist in some segmentsof the population. Malnutrition remains the major contributing factor tochild mortality: it is estimated that 20% of preschool children haveinadequate growth; 14% of school children are below expected weight for age,and 4% are under expected height for age. Other indicators of malnutritionamong children are riboflavin deficiency (6%). rickets (2%). and defectiveteeth (8%). Prevalence of weight deficiency is only 3% during the first 6months of life, but reaches 20% at 12 months (to remain at that level until2 years. and diminish slowly to 10% on the 5th year). The major causes ofinfant and child malnutrition are: insufficient breast feeding, as thecaloric and mineral content of milk becomes insufficient after the firstthree months of lactation; early weaning, combined with inadequatesupplementation, late introduction of solid supplements. inappropriate useof commercial formulas and limited use of the soy bean flour SEKMAMA
5 "Nutrition in Turkey" by T. 0. Koksal, Hacettepe University, Ankara,1977.
6 "Food Consumption and Ntarition in Turkey" by H. Gencaga, TurkishDevelopment Research Foundation, Ankara. 1985.

- 16 -
distributed by MORSA; and frequency of communicable diseases combined withdiarrhea episodes.
19. Pregnant and lactating women are the second group affected bymalnutrition and in particular by anemia, which occurs among 35% of pregnantwomen. The usual causes - short birth spacing, high parity, diminishingconsumption of proteins - are aggravated by adverse cultural habits thatgive priority to the feeding of adult males over women and children. Femaleobesity is a growing problem - 38% suffer from moderate obesity, and 26%from severe obesity - due to over consumption of carbohydrates and fats anda sedentary life style.
20. Malriutrition does tot appear in easily identifiable pockets,groups or geographic regions. It is associated with several closely relatedfactors which include education, size of the family and family income. Thenewly urbanized population is probably the one that suffers most frommalnutrition as it is most affected by unemployment, low earnings, and neweating habits. As can be expected, severe calorie malnutrition isconcentrated in lower income groups and affects 252 of the families in thebottom 20% of households, against 8% in the top income bracket. In 40% ofthe families in the lowest income bracket, per capita daily consumption ofanimal proteins is less than 10 gr, against 3% for the highest income group.It is estimated that the proportion of income spent on food is 40% for lowincome urban households, and as high as 65% for low income rural households.So far, lower income groups have adapted to inflation by replacing highpriced foods by low cost ones of equal nutritional value. However, thelower consumption of animal proteins signals a possible deterioration ofconsumption patterns. Table 4 shows the major variations in consumptionpatterns in various parts of the country.
21. More detailed data would be needed to identify high risk groups inoperational terms, and design effective interventions. The Governmentsupports several educational programs in nutrition. Most public or privateenterprises operate free or subsidized cafeterias; this satisfies the needsof the family head, but tends to detract his attention from the family foodbasket. MOHSA conducts programs in five areas: breast feeding; weaning foodand supplementation; growth monitoring and clinical follow-up; subsidizationand distribution of iron supplemented cereal derivates to prevent anemia andiodized salt to prevent goiter; and nutrition education through MCH andHealth Centers as well as schools in association with the Ministry ofEducation.
22. The Government has no coiordinated policy on food and nutrition.The Ministry of Agriculture monitors food consumption through its Departmentof Food Affairs that was transferred from MOHSA. No agency is responsiblefor overseeing the development of food technology, industrial foodproduction, or marketing policies. The creation of an intersectoraladvisory body, between MORSA and the ministries responsible for agricultureand education seems appropriate.

- 17 -
D. Fertility
23. Progress in contraception, rise in age of marriage, modernizinginfluences of education, urbanization and high levels of external migrationhave led to steady declines in fertility. Overall indicators are comparableto those of other middle income countries. but hide striking regionaldisparities. Low fertility rates and high levels of contraceptiveprevalence in metropolitan areas coexist with high fertility rates in therest of the country. Cultural and religious factors are often an obstacleto rapid response to family planning programs. In rural and eastern areas,entrenched attitudes towards women mean that the majority are still regardedas second-class citizens, despite 50 years of universal suffrage; there aretwice as many illiterate women as illiterate men. In remote Anatolianvillages, girls are still frequently kept away from school; contraception isconsidered sinful; polygyny. although illegal, is still practiced in thecountryside; men whose wives are unable to produce a son marry again atreligious ceremonies not sanctioned by law; marriage still occurs at veryearly ages in rural areas; and a large number of children is viewed as ablessing to farming families. Turkey is a secular state and a Muslimcountry and, as such, has not remained indifferent to events which arepresently shaking the Islamic world. It is, of all Muslim countries, theone which has achieved the highest levels of female literacy andparticipation in economic activity. These are both essential determinantsfor continuing fertility reduction.
24. As early as 1963, MOHSA carried out a "Knowledge. Attitudes, andPractices" survey. with the assistance of the Population Council. whichdemonstrated that about 75% of I4WRA were in favor of family planning. In1983. MOHSA conducted a nation-wide fertility survey. but data processingwas delayed for financial reasons and the results will not be availablebefore mid-1986. The 1978 Fertility Survey revealed however manycharacteristics which have probably persisted; it showed that 50% of womenof reproductive age were using contraception; this result had beenchallenged and a prevalence rate of 38%. calculated in conventional terms,was found more realistic; this still placed Turkey in the second position inthe Region, after Tunisia. Formal education of women appears to be thestrongest determinant of fertility in Turkey. Universal marriage is also asignificant factor: in 1978. only 1% of women aged 35 had never been marriedand an equal proportion were divorced or separated. The estimated completedfertility of 6.3 was much higher than the average desired family size of 3;it also varied widely, from 8.8 in the East. to 5.7 in the West; urbanfertility was 5.0. compared to 7.3 in rural areas. Similarly, the total
7 Defined as the average number of live children ever born to evermarried women by the end of their reproductive years. or age 49.

- 18 -
fertility rate8 was 4.3 at the national level, but only 3.7 in urban areas.compared to 5.1 in rural areas; the difference was even greater between theWestern (2.9) and Eastern (6.3) parts of the country.
2 . Contraceptive prevalence rates cannot be derived from servicestatistics as there are no nationwide comprehensive data on contraceptiveuse, in MOHSA facilities, or in university hospitals. the SIO, privatepractitioners or pharmacies. In 1978. only 12% of users relied on modernmethods (IUD. pill, condom), while 44% favored inefficient natural methods;IUD was used in only 3% of cases. A more recent estimate of FP users in1984. made by MOHSA, showed a national prevalence rate of 32.6% for evermarried women, 34.1% for currently married women. and 45.1% for exposedwomen9 (see Table 7). During the same year, new female acceptorsrepresented 7.4% of the total 15-49 age group; this ratio was only 3.6% inthe East and 4.7% in the Southeast; on the other hand. the Southwest showedtwice as many new acceptors as the national average (see Table 6).
26. A large unmet need for family planning services persists. The1978 survey already showed that smaller families were generally desired. animportant indicator of future fertility trends. The average desired familysize of 3 children was half the completed size of 6.3. Overalls 57% of MWRAwanted no more children. This was also the case for 50% of MWRA with twoliving children (59% in the cities. against 40% in rural areas; 64% in theWest, against 31% in the East; 72% with secondary education or more, against39% for illiterates). Estimates made by MOHSA in 1984 indicate that, toreach the desired norm of 3 children per family, the number of protectedwomen should increase from 2.8 to 5.1 million; for the desirable norm of 2children per family to be achieved, the number of protected women should be6.5 million. If this unmet need were satisfied, the crude birth rate woulddrop to 14-21 per thousand, instead of the current 31 per thousand.
27. But the inadequacy of services and shortfalls in contraceptivessupply is best illustrated by continuing high levels of induced abortions.According to the 1978 Fertility Survey, the annual percentage of women ofchild bearing age who had an abortion increased from 14% to 17% between 1975and that year. Of the 1.3 million women who had induced abortions, 66% hadit after their last delivery. and abortion seemed to be aimed at preventingbirth of more children and terminating reproductive life rather than forbirth spacing. The proportion of induced abortions increased rapidly withage. i.e. from 6% of women aged 15-19. to 47% of women in the 40-44 agegroup. Because of early marriage and rapid attainment of reproductiveideals. induced abortions start rather early in reproductive life. In 1984
8 Defined as the average number of children that would be born alive toa woman during her lifetime. if she were to pass through all herchildbearing years conforming to prevailing age-specific fertility rates.
9 Exposed status was defined as women living with husband, not inpost-partum amenorrhea. not pregnant and not sterile.

- 19 -
however, only 20.590 abortions were officially performed nationwide inMOHSA. social security and university hospitals.
28. Ignorance of modern contraceptive methods in rural areas. andwidely used inefficient contraceptive methods provide another explanationfor the high rates of induced abortions. In 1978, 88% of ever married womenwere aware of contraceptive method(s); 81% of them knew of the pill and 68%of the IUD; however, 15% of all rural women knew of no method at all. About63% of the women in the 25-34 age group had used some contraceptive method:75% in the cities, but only 48% in rural areas; 78% in the West. but only40% in the East; 93% of those at the secondary school level, but only 47% ofthose illiterate. As for present use of contraception among women ofreproductive age, it is strongly correlated with the number of livingchildren, indicating the desire to space later births rather than delayingthe first ones. Tables 5. 6 and 8 provide evidence of the considerablegains in prevalence rates that can be expected through a shift from naturalmethods and condoms to more effective contraceptive methods.
e. Environmental Factors
29. Deteriorating environmental conditions have increased morbidityassociated with water and air borne diseases. In rural areas, mostcommunities do not have piped water and rely on wells, public fountains orsprings; during the summer dry season, streams and rivers often have to beused for human and animal cons.. ption as well as washing. Sewers rarelyexist, and liquid and solid waste disposal systems are primitive.
30. In urban areas, sewage collection and disposal constitute the mostsevere urban problem in terms of unmet needs, followed by garbage collectionand disposal, particularly in the peripheral areas10. Sewer systems existonly in the major cities and serve an estimated 4.4 million people, or 18%of the total urban population; entire sections of most urban areas haveunsanitary conditions which contribute to the spread of water bornediseases. In 1980, 69% of the urban population had house connections. 25%used public standpipes, but only 6% had serious difficulty in obtainingwater. However, of the 990 municipalities with more than 3,000 inhabitants,only 42% have a fully modernized water supply and distribution system.Although housing conditions have improved markedly. overcrowding stillaffects most urban areas; between 1970 and 1980. the average urban houseincreased from 2.3 to 2.86 rooms; at the same time, the average size ofurban households declined from 5.7 to 5.2 persons.
10 See "Turkey : Urban Sector Review", World Bank, October 1983 (P,vortNo 4631-TU)>

- 20 -
31. Rapid urbanization has further lowered the quality of environmentin large cities, as municipal resources are insufficient to cope withgrowing problems of vater shortages, sewage, garbage disposal, etc. This iscompounded by lack of zoning regulations regarding the creation of newindustries which also affects health conditions through air and waterpollution. Finally, high levels of occupational diseases and accidents aregenerated by rapid industrialization; these are even higher in smallerenterprises and family shops where unsafe and unhealthy working conditionsprevail. In 1982 for example, SI0 statistics show that, among the 2.2million insured workers who represent at best 15S of the employed laborforce, there were 146,000 cases of serious work-related accidents oroccupational diseases, resulting in 2,760 cases of permanent disability andmore than 1300 deaths.
32. Municipalities carry the entire burden for enforcement of foodquality control, with limited success because of scarce technical andfinancial resources. Moreover, as responsibility for design and supervisionof this activity is diluted under six different ministries, regulations inthis area are not seriously enforced.

- 21 -
I1. - SECTONAJ POLICIES AND OBJECIrUES
A. Wealth
33. As early as 1961, the Government established health goalsemphasizing integration of public health services (referred to as"socialization"), and increasing coverage in rural areas, includingcommunity health and MCH/family planning. The Iategrated Health ServiceSebeh (IHSS), was designed to unify under the same health care delivery-system the services formerly provided by separate agencies, and to changehealth financing laws in order to allow access to public services to allthose without bealth insurance. It provides basic medical care, integratedNC8/FP services, prevention and treatment of communicable diseases,environmental health care, school health services, health education, andcommunity development. Improved nutrition is expected from increasedproduction and better distribution of basic food items, but the IHSS is toimplement specific programs within MCH, especially for poor pre-schoolchildren in both urban and rural areas.
34. The IHSS operates at four levels, the first two providing primarycare services. At the first level, health posts serve an average of2,000-2,500 population. They are staffed with a village midwife who worksgenerally alone. She provides PHC and FP care, dispenses basic drugs andcontraceptives, and attends deliveries either at home or at her smallstation; in addition, the midwife is supposed to visit each householdmonthly, but lack of transportation makes this task impossible in sparselypopulated areas. There are only 14,000 village midwives for some 36,000villages. Each health post is visited at least once a week by a mobile teambased in the health center.
35. At the second level, the health center (RC) is the cornerstone ofthe system; it serves 10-20,000 persons in scattered areas, while large(urban) centers serve 20-50,000 persons; moreover, each health centersupervises at least 3 health posts through its mobile teams. Realt'. centersare modestly equipped, and have a staff of 7 to 10: one MD (generally a newgraduate serving his compulsory medical service), one public health nurse,several midwives, a secretary and a driver. HCs are responsible forambulatory medical care and preventive programs, i.e. inmmunizations, MCH,family planning, health education, control of communicable diseases,epidemiological surveillance, case finding for TB, malaria and cancer. Theyare also responsible for outreach visits to health houses, homes, schools,work sites, etc. However, the shortage of vehicles limits considerablyoutreach activities.
36. The third level consists of a local hospital with 50-100 beds,staffed with four specialists (surgeon, gynecologist, internist andpediatrician), one laboratory technician and one dentist; each localhospital serves 5-6 health centers. Finally, at the fourth level, the

- 22-
general regional hospital serves a population of 200-400,000 persons, as areferral facility for 20-40 health centers.
37. The ambitious goal set in 1963 was to extend the new system to thewhole country in fifteen years, in order to redress inequalities in coverageof basic services and in health status. However, the IHSS failed to achievethese objectives, for lack of thorough preparation and planning at theconceptual stage, insufficient financing, and lukewarm, political and popularsupport. The only formal basis for the system is still the 1961 Lawcreating it; but no technical foundation was ever designed to seL uprealistic objectives, determine a timetable, evaluate costs and identifysources of financing. Since 1978, UNICEF is assisting MOHSA in theimplementation of a Primary Health Care Project which includes components inimmunization, oral rehydration, nutrition, MCH/FP, water/sanitation,essential drugs, health management and research.
38. Health education is largely neglected in Turkey and no specificprogram is implemented in this area. However, MCH clinics cover someaspects of health education in their pre-natal, maternal and child careactivities, and primary school programs include some elementary healtheducation topics. Low levels of education among women constitute a majorconstraint to improving the health status of the population, in rural aswell as in newly settled periurban areas, a 1980 survey confirmed therelationship between higher levels of infant mortality and mothers' loweducational levels.
39. The Fifth Developmeut Plan (1985-1989) contained generalstatements reaffirming Government's commitment to "equal access to healthservices by all citizens", and to "health services for all, everywhere andequally", under a single authority. As regards family planning, it statedthat the national policy should be to provide families with "effectivemeasures responsive to the family sizes they desire, in accordance withtheir socio-economic levels". The Plan introduced two major policyorientations which are bound to affect future sector development: first,private establishments and hospitals received official support throughderegulation of fees charged in these facilities, and through contracts tobe passed between the public health sector and physicians in privatepractice; second, the transition to health insurance is to be made duringthis period; it is not clear however what this entails in practice.
40. But the Plan's objectives focus on institutional issues. Thereare no quantified targets, and no specific measures are recommended toimprove the health status of the population. Objectives include improvedaccessibility and efficiency of services; emphasis on preventive medicine;better utilization of existing capacity; improved cooperation between state,university and Social Security owned hospitals; the strengthening ofregional hospitals, to stem the flow of patients in major cities; theexpansion and improvement of maintenance services; and manpowerdevelopment. A national target of 2.6 beds for 1,000 population has beenset, but the Plan explicitly excludes the construction of new hospitals inprovinces with under-utilized capacity. Finally, the Plan excludes the

- 23 -
construction Qf large teaching hospitals, not cost-effective and difficultto manage,
B. Nutrition
41. For more than tuenty years, as evidenced by four DevelopmentPlans, self-sufficiency in food and improvement of the nutritional status ofthe population have been priority objectives; agricultural projects havebeen largely justified on these grounds, although target groups or fooditems whose increased availability would improve the nutritional status ofthe population were rarely identified. Nevertheless, for large segments ofthe population, food availability in terms of calories and proteins is belownutritional requirements. A small nutrition inte-vention program consistingof the distribution of high protein weaning food (SEKMAN&) is implementedjointly by MOHSA and the Turkish Dairy Corporation with UNICEF assistance.However, it is not replicable in a wider scale.
42. Until the early 1980s, wheat and flour were subsidized. However,provision of wheat at subsidized prices tended to create a dual flour marketrather than stabilize prices. As government subsidies were exclusivelychannelled through bakeries, they were largely confined to the three majormetropolitan areas. Rural households and poor urban dwellers who make ttaeirown bread were not reached; moreover, the system hardly benefited smallercities, especially in the Eastern Anatolia and Mediterranean regions wherecalorie malnutrition is most prevalent. A more effective mechanism is beingintroduced for stabilizing prices and aleviating shortages during off-seasonperiods, namely spot sales on the free market, particularly in EasternAnatolia and the Mediterranean regions.
43. In a longer-tern perspective, the Government has taken measures toencourage consumption of key commodities such as pulses, potatoes, vegetableoils and margarine. Pulse production hae been encouraged througb anintensive research/extension effort known as the Fallow Reduction Program.In addition, the Government has completely liberalized the importation ofvegetable oil seeds to reduce domestic prices of oil and promote theirconsumption. Efforts should also be made to reduce the price of sugar, asthe Turkish sugar beet industry is not competitive and local wholesale priceof sugar is about 70% above international price. As for the low per capitaconsumption of potatoes, it is only partly due to consumption habits: apolicy has been designed to reduce production costs through seedimprovement, extension work, increased output and promotional support.Finally, increased efforts should be made to assist livestock development onthe farm, and to increase productivity of village herds as an essentialmeans of improving rural diets. With UNICEF assistance, the Ministry ofAgriculture is implementing a Food and Nutrition Planning and PolicyProject, now in its third phase, in order to support government's efforts inimproving commodity planning and food marketing.

- 24 -
C. Population
44. After World War I. Turkey followed an active pronatalist policy,justified by high mortality rates and acute manpower shortages. The FirstFive Year Development Plan, published in 1963. was the first legal documentto recognize that tjr rate of population growth was affecting adverselyeconomic developmentl The 1965 Law on Population Planving reversed thepreviously ?ronatalist official position and legalized contraceptive usewith a view to slowing down labor force growth and increasing savings andinvestment. For the first time. free or low cost contraceptive services andinformation were made available to the population; abortion for medicalreasons was legalized, but sterilization was banned. However. theGovernment never supported incentives to encourage fertility reduction. andnever questioned existing tax allowances for families of up to fivechildren. Implementation of the 1965 law was rather slow, at least until1978. Nevertheless. "population planning" programs12 were established inMOHSA and in military and volunteer organizations.
45. The September 1980 Constitution, endorsed by referendum inNovember 1982. mentions for the first time in a legal document the term"family planning" which, following the ambiguous formulation of Article 41.is to be implemented "through education". The Fourth Plan's (1979-1983)ambitious goal13 was to lower the country's total fertility rate to thelevel of the most developed provinces, by the year 2000. This implied areduction of the total fertility rate to 2,7, of the crude birth rate to 22per thousand, and of the crude death rate to 6 per thousand; thecorresponding rate of natural increase would be 1.6Z p.a.
46. The May 1983 Law on Population Planning set forth the principlesof population planning, defined the terms termination of pregnancy,sterilization and emergency situation requiring medical intervention, andregulated matters concerning the procurement, manufacture and officialrecognition of contraceptive drugs and devices. Abortion under 10 weeks ofpregnancy was authorized for social or economic reasons; over 10 weeksabortion was authorized for medical reasons only; sterilization was nolonger subject to medical justification, and paramedical personnel wereauthorized to provide FP services, including IUD insertion. MOHSA was giventhe responsibility to coordinate all FP services delivered by the variousproaviders.
11 See "Population Policy of Turkey" (Environmental Problems Foundationof Turkey. Ankara, July 1983) for a presentation of the population issue ina historical perspective.
12 "Population planning" is the official term used in the country todesignate family planning activities.
13 See "Country Report on Policy Cbjectives and Measures Relevant toPopulation Trends in Turkey". State Planning Organization. June 1982.

- 25 -
47. Family planning services are part of the program implemented bythe General Directorate for Maternal and Child Health and Family Planning,which operates 600 clinics, 95 dispensaries and 20 independent facilities inperiurban areas. These activities complement FP services provided by theprimary health care program. IUD, pills and condoms are available, but useror post-partum follow-up is not organized, therefore no current data areavailable on contraceptive prevalence. SIO and university hospitals providethe full range of services. The Turkish Family Planning Association createdin 1963 has 19 branches providing supplies and education materials. Themilitary, the Turkish Development Foundation, labor unions, the RailwaysCorporation, the Post Office, and insurance schemes also implement their ownprograms. The private sector remains the main provider of services in urbanareas, but no information is available on its real coverage. In ruralareas, where full health coverage has not yet been achieved, absence ofservices, supplies and promotional activity is clearly reflected in higherparity levels, infant mortality and abortions.
48. In the field, responsibility for health education rests primarilyon the midwives who conduct individual and group sessions at the healthcenter, the health post or during home visits; a specialized team is incharge of specific target groups such as teachers or religious leaders.UNFPA currently supports a five year project to strengthen and integrateNCH/FP services in 17 Eastern provinces. It executes an education andservices project targeted at 150,000 workers in more than one hunuredindustrial plants; it also assists the Ministries of Education, ofInformation and of Interior in the training of educators, the production ofmaterials for adult education centers, the production of TV films, and theprocessing of the 1985 census. Over the last 10 years, UNFPA's assistanceamounted to about US$10 million. Other agencies supporting Turkey's familyplanning programs include the Pathfinder Fund (training of midwives,advisory services to labor unions, and direct support to several FP programsfor industrial workers); Family Planning International Assistance, JHPIEGO,INTRAR, the Turkish Family Planning Association and other non governmentorganizations. Substantial assistance in the population field contrastswith the limited support provided by the international community in otherareas, and social sectors in particular.

- 26 -
III. SICTORAL ORGANIZATION
49, The Turkish health sector is charecterized by an extremecomplexity. A large numtler of public, semi-public and private institutionsare engaged in the financint, and deIivery of health services. The publicsector, for instance, is not limited to the Ministry of Health and SocialAssistance (MOHSA). Medical schools. through their university hospitals,cover a substantial part of demand for health services. The SocialInsurance Organizatioa (SIO) not only operates its own hospitals: it alsopurchases services for its members from public and private facilities. TheArmy has a large network of facilities and covers the health needs of itsactive members, retirees and their dependents; very little is known aboutits operations. beyond the number of hospitals and related beds. Otherministries (Education. Youth and Sports). public organizations (Post andTelecommunications. Railways). and state economic enterprises still operatetheir hospitals. In addition to the very active private for-profit sector.there are many foundations and hospitals for religious groups and foreigncommunities. Most of health services are however supplied under threelargely autonomous systems: (i) the Ministry of Health and SocialAssistance. (ii) the Medical Schools and (iii) the Social Security System.While MOHSA is formally responsible for the design and implementation of thecountry's health policies, its authority over other health servicesproviders remains rather limited.
A. The Ministry of Health and Social Assistance (NoESA)
50. Historical evolution. The Ministry14 was created in 1920 to trainhealth personnel, establish and operate model hospitals and maternityclinics. control infectious diseases, and prepare policy proposals for thedevelopment of health care. Its major responsibility was seen as theprevention of epidemics and infectious diseases. Curative care was left tothe private sector and in this area. MORSA's responsibility was limited toissuing permits for the establishment of private clinics or hospitals.controlling the production and prices of medical supplies and drugs. andsupervising the activities of the pharmacies; the model hospitals were onlybuilt by the government to encourage private investment in medical care. Inthe field, MO0SA's departments conducted their own programs independently.with their own resources. The infectious diseases program was quitesuccessful in controlling malaria and tuberculosis and also to a largeextent trachoma and syphilis. In the big cities, an immunization programwas implemented, with the support -of the Red Crescent and the Child WelfareSociety. However, MOHSA was much less successful in promoting the
14 It is also frequently referred to as Ministry of Health and SocialWelfare.

- 27 -
development of the private sector as health personnel remained in shortsupply and concentrated in the three major cities; on the other hand, thecreation of model hospitals did not stimulate private investments, even inmajor cities, because of lack of know how and low demand.
51. Improving economic and social conditions, higher levels ofeducation, and rapid urbanization generated increasing demand for personalmedical services which could not be met by the private sector or by localgovernments. This led MOHSA to expand its provision of curative services.Considerable investments were made, but without a coherent plan or specificobjectives. This increased the gap in the quality of services and generalhealth status between urban and rural areas and between provinces. Thepersistent low quality standards and inefficiency of the system was alsolargely due to the shortage of qualified health personnel. In 1960, a smallgroup of doctors and members of Parliament designed a national system forthe "socialization" of health care, without any cooperation or support fromMOHSA. This Integrated Health Service Scheme was endorsed by the militarygovernment and ratified in 1961 by the Parliament.
52. Present organization. MOHSA assumes a regulatory and policyfunction and, through a national network of hospitals, clinics, healthcenters and dispensaries, provides preventive services as well as inpatientand outpatient curative care. MORSA also operates schools for the trainingof nurses, technicians and midwives. However, it has limited control overthe activities of the SIO which provides medical care for its members andtheir families, in its own hospitals. Similarly, MOHSA has practically noauthority over the medical schools which, in addition to providing graduateand post graduate training, operate large teaching hospitals which cover anincreasing share of the country's medical care. In the past, manyministries, local governments and state enterprises had their own hospitalsand dispensaries to serve their staff and their families. Most of thesefacilities have now been transferred to MORSA, with the exception of theones belonging to the Ministry of Defense; in 1983, this Ministry actuallycreated its own medical school. The Child Welfare Society, an oldcharitable organization helping needy children, was transformed in 1984 intoa state economic enterprise. Outside the public sector, the Red Crescentprovides emergency assistance and operates blood transfusion centers in themajor cities.
53. At the central level, the Minister is assisted- by an Under-Secretary and three Deputy Under-Secretaries (see Organizational Chart I).The Ministry includes six General Directorates and eight central units.General Directorates or units are subdivided into a large number ofservices. For instance, the General 'Directorate for Maternal and ChildHealth and FAmily Planning (DGMCHFP) has three Deputy General Directors,five departments, and 14 sections with a total staff of 98 persons. Inspite of the IRSS, vertical programs such as malaria eradication and TBcontrol have survived the creation of the General Directorate for PrimaryHealth Care (GlPHC). Moreover, two units still share responsibilities inmatters of MCH/FP: the GDMCHEFP, which oversees service delivery; and theGDPHC which carries out the program of integrated health services. The

- 28 -
General Directorate for Pharmaceuticals plays a very important role,described below in Section IV. Finally, the General Directorate ofFrontiers and Coasts is responsible for the implementation of allinternational health regulations and for the control of communicable andepidemic diseases at the borders.
54. At the provincial level (Organizational Chart II), the HealthDirector is the senior health official, formally responsible for thedelivery and coordination of all public health services. However, all fundscome from the capital city where all decisions relating to health personuel,their job descriptions and specific tasks are also made; only clerical andunskilled workers are hired locally but political and social pressure issuch that they enjoy nearly total job security. In reality, as budgetallocations for each entity are separate, each General Directorate in Ankaraoperates its own program t ough its provincial structure.
55. In the populatiou area, the GDMCHFP has three majorresponsibilities: design and implementation of education and trainingprograms for health personnel and the general public; coordination anddistribution of contraceptives to public health facilities; and research andevaluation of family planning activities. The Ministry of the Interior, isin charge of civil registration. The collection and analysis of basic data,including censuses, is the responsibility of the State Institute ofStatistics attached to the Office of the Prime Minister. The ScientificCommission of Population Planning, created in 1966 under the responsibilityof MOHSA, is in charge of controlling the" quality of the drugs and devicesto be used in family planning". Finally, the Inter-Ministerial PermanentSpecial Commission on Population Activities created in 1980 under the StatePlanning Organization advises the Government on population issues andmonitors and evaluates family planning programs.
56. Three major agencies supply MOHSA with contraceptives. FamilyPlanning International Assistance (FPIA) provides pills (2 millions cyclesin 1984-85), IUDs (200,000 in 1984), and condoms (10 millions to bedelivered in 1985-1986). UNFPA provides all the contraceptives (pill, IUD,condom) for the 17 Eastern provinces. Finally, the Pathfinder Fund suppliescontraceptives through several projects. The public sector neverexperienced shortages of contraceptives at the national level. However,storage and distribution problems sometimes result in temporary shortages atthe provincial level. As far as the private sector is concerned, fivecompanies import raw material, and produce locally eight brands of pills.Altogether, in 1984, 3,300,000 cycles of pills were produced locally, anamount sufficient to protect only 254,000 women during a year, i.e. 3% ofMA.
57. For matters related to information and education majorresponsibility rests with the General Directorate for Health Education.Nevertheless, in the population area, the GDMCHFP has retained control ofIEC interventions and operates a Communication Support Center created withUNFPA assistance. The Ministry of Education supports IEC activities in manyareas of direct interest to the PHN sector through its National Education

- 29 -
Board, the Institute of Nonformal Education, and the Popular EducationCenters. The Ministry of Agriculture, Forestry and Rural Affairs has some1,000 home economists extension workers in rural areas who could participatein health and population education programs.
S. The Nddical Schools
58. Medical Schools assume three functions in the public sector, asresearch institutions, training facilities for high level health personnel,and as direct providers of health services. As the country bas no formalmanpower planning or policy, the Universities and their Medical Schools makeindependent decisions regarding the number of students to be trained,duration and standards of education, curricula, etc. Overall policy andcoordination takes place through the Higher Education Council (YOK). Foryears, the three Medical Schools in Ankara and Istanbul practicedrestrictive policies and, in spite of government's pressure, limited thenumber of students in order to safeguard quality standards and physiciansiucomes; they also resisted the establishment of new medical schools innewly created provincial universities.
59. In the 1970s, acute shortages of medical personnel and increasingsocial demand for all types and levels of education eventually overcame theresistance of the medical establishment, and a very rapid expansion ofmedical schools took place. The training capacity increased from 4 medicalschools with a total enrolment of 900 students in 1964, to 8 schools with1600 students in 1974; by 1984, there were 22 medical schools with a totalenrolment of 5500 students. As was feared, this rapid expansion has beenaccompanied by a decline in academic standards, as most new schools do nothave sufficient teaching staff; moreover, many lack adequate teachinghospitals and two of them have no teaching hospital and use MORSAfacilities. In the past, medical schools had been criticized for theirrestrictive policies and their use of inappropriate curricula and standards,derived from industrialized countries; while there was some value in thiscriticism, the very rapid increase in enrollments, which will eventuallyresult in an oversupply of less qualified physicians, is obviously not thesolution to Turkey's health problems.
60. As services providers, university hospitals, especially the oldestones, play a very important role in supplying curative care; many of themactually serve more as medical than teaching facilities. Demand for theirservices is very high as it is believed that these are of higher quality,and this is largely true since they are more receptive to new knowledge andtechnology, and have more resources to invest in equipment and materials.However, like most Turkish hospitals, they are affected by inefficientmanagement, as they are directed by prestigious physicians, appointed forfour years, with limited training or interest in administrative matters.
- 30 -
C. The Social Security System
61. The origin of the social security system in Turkey -can be tracedto the XIIth century when foundations, with government support, alreadyprovided some coverage of health risks. Under the Ottoman Empire. as earlyas in the XIIIth century. a sort of crop-insurance scheme existed in theagricultural sector, while most trade guilds operated social and economicprotection funds; in Istanbul alone, in the XVIIth century. 1109 tradeguilds were registered, with about 126.000 membersl5. Foundations andsocial welfare institutions evolved into at least twelve large organizationssuch as the Military Pension Fund (established in 1866), the Civil ServantsPension Fund (1881). or the Sailors Pension Fund (1890). The first socialinsurance institution in compliance with international conventions wascreated in 1921 for the benefit of coal miners, and Turkey is now signatoryto most ILO Conventions regarding labor standards and social security. Thevarious funds and schemes were merged in 1945 (for industrial workers) and1950 (for civil servants); the system was subsequently expanded to coverself-employed and agricultural workers.
62. There is a perceptible trend within the system towards generalcoverage and standardization of benefits. Although they vary with theinstitution, benefits tend to be generous; moreover, built-in safeguardshave been relatively successful in protecting beneficiaries during thesetimes of high inflation. The present situation is characterized by thejuxtaposition of universal and occupational schemes, which includeshort-term as well as long-term insurance programs. These are:
- National Health service: free preventive care for the wholepopulation; paying curative services, but fees waived for indigents.
- Universal Old Age and Disability Pension scheme: financialsupport to some 700,000 needy individuals.
- Active civil servants: free medical care for 1.4 milliongovernment employees and their dependents.
- Government Employees Retirement Fund: pensions; freecurative care for more than 660.000 pensioners and their dependents.
- Social Insurance Organization: pensions; pre-paid curativecare for 12.8 million beneficiaries.
- Social Insurance Agency of Merchants. Artisans and Self-Employed Professionals: pensions; health benefits under considerationfor some 10 million persons.
- Private Funds: pensions; pre-paid curative care for about300,000 persons. with limited benefits for dependents.
15 Social Security Council: "Extending and Improving the Effectivenessof the Social Security System, and the Unification of Social SecurityInstitutions". Ankara, March 1983 (report in Turkish).

- 31 -
63. The-nationsl health service is a universal scheme which, under the1961 Act concerning the IRSS, guarantees each citizen free preventive careand family planning services. Curative services must be paid for, except byindividuals recognized as indigents.
64. The Universal 014-Age and Disability Pension Scheme, introduced in1976, provides a flat-rate old-age or invalidity pension to needyindividuals fulfilling given criteria. The scheme, administered by theGovernment Employees Retirement Fund, is fully financed by the state. Atthe end of 1984, it covered more than 713,000 pensioners, i.e. 565.000 oldpersons, 44,000 invalids, and 104,000 disabled individuals (see Table 24).Total financial outlays for that year amounted to TL23.6 billion (US$64.4million). The number of pensioners peaked in 1981 but is now back at the1979 level. Pensions have been substantially eroded by inflation and, on aper capita basis, decreased by 63% in real terms between 1979 and 1984.
65. Cash benefits are also awarded to families of draftees duringtheir National Military Service. The cost of this program is born by themunicipalities, and actual levels of benefits may vary.
66. As regards occupational schemes, a distinction has to be madebetween civil servants and other categories of workers. Among the former,the Turkish law recognizes active and passive civil servants, i.e. thosestill working and those who retired; as will be seen, both groups arecovered under a generous system which extends its long and short-termbenefits to relatives and survivors alike.
Active Civil Servants
67. Active civil servants, their spouses, dependant children andparents are fully covered in case of illness or maternity. These arebenefits "in kind" provided directly by the employer, i.e. the State, at nocost to the worker. No institution collects contributions or manages aspecidl fund as all related expenses are borne directly by the Department ofthe civil servant concerned. Health benefits include medical and laboratoryexaminations, admission to health facilities, drugs and medical suppliesduring treatment, transportation of the patient, dental treatment,prosthetic devices, eye glasses and hearing aids. During sick or maternityleave, civil servants continue to enjoy full pay. There are no statutoryrequirements or time limit to these benefits.
68. Since September 1983, minor restrictions have been introduced intothe system, such as a 10% charge for drugs for out-patient services; thesewill not affect the overall level of expenditures. Medical expenses areidentified in the budget of each public organization (Article 180); theyfluctuate, as shall be seen later in this report, with the level of feesdecided by the Government. In current prices, they represented US$33.6million in 1984, compared to US$53.6 million in 1981.

- 32 -
69. Finally, although there are no specific family benefits, a heatingallowance called social assistance benefit was introduced in 1977 for somecivil servants, then extended to the pensioners; this flat-rate cash benefitis now equivalent to 25% of the salary of a civil servant within themiddle-income biacket. Other benefits of lesser importance include anursing allowance, coverage of funeral expenses, and a marriage allowancecorresponding to two years of pension.
The Government lupioyees Retirement Fund
70. The Government Employees Retirement Fund (GERF) covers old-age,death, invalidity, employment injuries and occupational diseases for whitecollar workers in central government, local governments and state economicenterprises. In addition to these long-term insurance benefits, GERF alsoprovides short-term health and maternity benefits for its pensioners, theirdependents and their survivors. Medical care is obtained by contracting outservices to MOHSA facilities or university hospitals. The fund was createdin 1950, by merging all public institutions' pension schemes, with a view tostandardizing benefits and statutory requirements for all govt:nmentworkers. Financed by contributions from civil servants and the State asemployer, it is attached to the Ministry of Finance and Customs. In 1981,contributions were raised to 10% of basic salaries for employees and 18% forthe State.
71. Pensionable age for civil servants is generally 65 for males and60 for females; irrespective of age, a proportional pension can be claimedafter 25 years of contributions for males and 20 for females. Invalidityand survivors pensions are subject to some statutory requirements. Between1981 and 1984, the number of active members (i.e. civil servants and publicsector employees) declined slightly from 1,415,000 to 1,375,000; but theoverall number of passive members (i.e. various types of pensioners andtheir dependents) increased from 573,000 to almost 662,000.
The Social Insurance Organization
72. Under the Social Insurance Act of 1964, the Social InsuranceOrganization (STO) is a state economic enterprise providing short-termmedical and maternity benefits, employment related accident and occupationaldisease benefits, and long-term benefits in terms of old-age, disability andsurvivors pensions. These cover all employed persons, with the exception ofcivil servants (manual labor in the public sector is covered), the military,and domestic servants. Under the 1973 Social Insurance Law Relative toAgricultural Workers, the pernmanently employed in agriculture, with a workcontract, have become contributors, and beneficiaries, of SIO. The SIO,attached to the Ministry of Labor and Social Security, is a tripartiteorganization, i.e. its General Assembly is made up of representatives ofworkers, employers, and the government. Its Governing Body, with membersselected from the General Assembly, retains its tripartite nature. A

- 33 -
General Director, designated by the Government, is responsible for itsmanagement and the implementation of government policy.
73. The SIO covers all insurance programs except family andunemployment benefits. Pensions are paid to all insured persons whocontributed at least 5,000 days and are at least 55 years of age for malesand 50 for females, or have been insured for at least 25 years, or aredisabled and aged at least 50. The old-age pension is equal to 70% ofaverage annual earnings; reduced pensions are also payable at 55-50 yearsfor persons who have been insured for at least 15 years; those who retire atage 55-50 without being entitled to old-age pension receive lump-sumpayments equal to the total contributions paid by them or on their behalf.Disability pensions can be awarded to workers who contributed for at least1800 days; moreover, disability pensions as well as survivor's benefits arealso payable to spouses or dependents.
74. Medical coverage includes free diagnosis, therapy and drugs to theinsured person and pensioner and the direct members of their families.Sickness benefits cover the cost of treatment for six months, and can beextended for eighteen months. Dependents contribute 20% to the cost ofmedicines. When the contributor or the pensioner dies, the dependentsremain eligible for health benefIts. The SIO operates its own healthfacilities. Their number has increased with the number of contributors,especially after 1965 under the pressure of labor unions; 8IO now has atleast one general hospital in 44 of the 67 provinces. Since the 1982extension of coverage to agricultural workers, the SIO is confronted withthe problem of providing health care to rural areas.
75. The SIO also maintains contracts with private or publicinstitutions, generally for outpatient care, or for inpatient care in areaswhere it does not operate its own hospital. In the case of MOUSAfacilities, this constitutes an indirect subsidy, as current fees in publicfacilities are well below real operating costs of SIO hospitals. As themarginal cost to the recipient of health care is nil or negligible, onewould expect an over consumption of health services by SIO's 13 millionbeneficiaries. Yet, the number of physician contacts per insured per yearis only 1.4, compared with 3 to 4 in other middle income countries withcomparable systems; one reason could be that SI members frequently usepublic health services. Also surprising is the low rate of hospitaladmissions (48 per thousand beneficiaries against 70-80 in other middleincome countries). As no ready explanation is available for these lowutilization rates, the finding requires further investigation.
76. The SI0 covered more than 2.4 million insured workers in 1984,with a very large majority of males, and a substantial number of publicsector employees (see Table 25). If non-contributing members and dependentsqualifying for health benefits are added, the total number of personscovered by the SIO in 1984 was 12.8 million, or one fourth of the Turkishpopulation. While self-employed are covered under a separate system (seebelow), there is still a substantial proportion of the labor forceunaccounted for, especially in family businesees and cottage industries

- 34 -
which employ large numbers of unreported children and apprentices (the 1980census showed a 42% participation rate for children aged 12-14 and of 60%for children aged 14-16). Recent years show a disturbing trend: between1979 and 1984, the number of contributors increased by only 13%, but thetotal number of beneficiaries increased by 78%;- during the same period,total contributions declined by 6% in real terms (Tables 25 and 26).Health related benefits paid by SI0 in 1984 (i.e. direct expenses for healthservices, plus salaries compensation for temporary disability) amounted toTL98.6 billion (US$21 per beneficiary); this represented an increase of 5%in real terms, over 1983 disbursements.
77. The SI0 is financed by a set of premiums, covering each individualrisk, paid by the employee and the employer. Overall contributions are veryhigh and vary between 33.5 and 39% of total labor costs; for health alone,they correspond to 11% of salaries, 5% paid by the employee and 6% by theemployer. Contributions, over a minimum and up to a maximum wage, areadjusted periodically. There is no state contribution,. In 1981, they wereslightly increased to the following levels:
RATM OF COITEIBUTIOUS TO SOAS PEILCETAGE OF TOTAL WAGES
Workers Employers Total
- Illness 5 6 11- Maternity - 1 1- Accid. & Occup. dis. - 1.5-7 1.5-7- Retirement 9 11 20
- Total 14 19.5-25 33.5-39
78. All SIO resources are allocated to a Special Fund which operatedwith a net positive cash flow until 1980. Since that year, however, the SIOhad to borrow increasing amounts from the Central Bank to cover itsdeficit. This deficit has three main causes, two of which call for overduestructural adjustments. First, high rates of internal inflation haveobviously had a negative impact on SIO's financial situation as cost ofhealth services, and corresponding reimbursements, increased more rapidlythan premiums linked to salary levels. A second, more serious reason isemployers' lengthening delays in transferring accrued premiums to SIO: aboutTL73 billion in 1983 (US$324 million); a quarter of these overdue paymentsare employees contributions collected at the source. The economic recessionand the difficulties experienced by most enterprises explain to some extentthis situation, but these enterprises take advantage of inadequatecollection procedures to build their liquidities. The third cause of SIO'sfinancial problems is the rising proportion of beneficiaries compared tocontributing members: between 1973 and 1984, this ratio increased from 1/7to 1/2.5.

- 35 -
The Social Insurance Agency of Nerchants, Artisans and Self EmployedProfessionals
79. The Social Insurance Agency of Merchants, Artisans and SelfEmployed (BAG-KUR) was created in 1972 to provide coverage for the abovecategories, on a compulsory and contributory basis. The 1973 SocialInsurance Law Relative to Self-Employed Persons Active in Agricultureextended the same benefits to these workers. Moreover, any citizen notcovered by a social security institution, including housewives, can applyfor membership. The General Assembly and Governing Body make up the higheradministration of BAG-KUR, also attached to the Ministry of Labor and SocialSecurity; it is managed by a DULector General designated by the government.
80. The institution provides only long-term benefits; for healthcoverage, its members have to rely on private insurance or the universalscheme. It is financed only by individual contributions set at 20% of theincome level stated by the insured person; this rate, increased in 1981, issubstantially higher than in the past (13% in 1972 at the creation ofBAG-KUR, and 15% in 1979). Overdue payments were estimated at TL6 billionin 1982 (US$37 million). Benefits are comparable to the ones provided by5IO. The number of contributors is increasing regularly, from 1.2 millionin 1979, to 1.4 million in 1981 and 2.1 million in 1985 (see Table 29). Thetotal number of persons receiving monthly benefits increased more rapidly,from 136,000 in 1981, to 239,000 in 1985; more than 60% of beneficiaries arepensioners.
81. The Government has decided to include health benefits in theBAG-KUR package, and a bill to this effect is under consideration by theParliament. The new scheme would be compulsory but introduced gradually,starting with the major cities; its adoption would practically result in auniversal health insurance scheme. BAG-KUR would not set-up its ownnetwork, but purchase services from public facilities. Health benefitswould be comparable to those provided by SIO. As no employer contributioncan be expected, members would have to bear the full cost of the insurance;the proposed level of premiums, and their adequacy, are discussed below.
The Private Funds
82. When the various schemes were regrouped under the Social InsuranceOrganization, in 1964, some private funds retained their independence, foractuarial or political reasons. The law provides however that they mustensure minimum benefits to their members, comparable to the ones describedfor SIO.
83. There are about 26 funds for employees of banks, insurancecompanies, chambers of commerce and industry, and stock exchanges. They allcover old-age, invalidity and survivors risks; with the exception of fourfunds (where those risks are directly covered by the employer), they alsoprovide illness and maternity benefits. Beneficiaries include about 78,000contributors and their 152,000 depe nts, 13,000 pensioners and their

- 36 -
26.000 dependents, and about 4.000 survivors. Each fund is administered byan elected Governing Body. subject to financial supervision of the Ministryof Labor and Social Security.
84. Although they have the status of civil servants. primary schoolteachers have retained their Mutual Assistance Fund. For a small monthlyfee, the fund provides them with additional benefits. in terms of lump-sumpayments in cases of birth. retirement or death. Attached to the Ministryof Education, the fund is supervised by the Ministries of Finance andLabor.
85. Finally, the Coal Mine Workers Afssistance Fund, established in1921, still operates and provides additional benefits in kind and cash incases of illness. industrial accidents, and occupational diseases; the fundalso awards grants and scholarships. It is supervised by the Ministry ofLabor and Social Security.
D. The Private Sector
86. With 40S of its pbysicians working in private practice, Turkeyappears to have an important private sector. However, for most physiciang.this is a part time activity: since 1981. medical doctors working in thepublic sector have been authorized to maintain a private practice afterregular work hours. Some of them take advantage of this privilege in thecities, but all of them do in rural areas. The number of physicians workingexclusively in private practice is not known but is said to be small.Private physicians provide a substantial share of primary care (as much as40% of first contacts in rural areas); they also provide some ambulatorychronic care, but they rely almost entirely on public hospitals forinpatient services. In this set up. physicians must keep a hospitalappointment that ensures them hospitalization privileges, a sine qua non forsuccessful private practice. Overall, there are advantages to this dualsystem: the Government is spared part of the burden of outpatient care.while patients retain the right to choose their physician; quality of carecan be preserved as long as control mechanisms operate effectively.Basically, the Turkish medical practice resembles those in Europe or in theUnited States; the major difference lies in the fact that third party payors- insurance or social security - play a much smaller role in Turkeyl6.
87. About 90% of private physicians practice alone. while 7% work inpartnership of legs than four physicians, and less than 3% work in largegroups offering a wide scope of specialties. Less than 1% of nurses areself employed, but almost 4% of midwives have their own practice: 32% of
16 The SI0, the Army, the Government and some other public entitiesprovide health services in their own facilities and do not reimburse visitsto private practitioners.

- 37 -
technicians - especially physical therapists, opticians, dental and labtechnicians - prefer self-employment or have some partnership withphysicians or dentists.
88. Private hospitals represent only 4% of total beds in the country(see Table 15). The larger ones are in fact non profit institutions: 8hospitals. with 680 beds belong to foreign communities; 4 hospitals (320beds) are owned by philanthropic associations or foundations; and 5hospitals (930 beds) are owned by ethnic or religious minorities; most arelocated in the Istanbul metropolitan area and are gradually being absorbedby the public system. The other 93 private hospitals, totalling 2,770 beds,are owned by investors and operate for profit; of these, only 4 (560 bedsaltogether), located in the three largest cities, are modern facilities; the89 others are small, often underequipped, and run by the owner physician;they are located in capital cities of western provinces and sea sideresorts. Private hospitals serve two profitable markets, namely the richand the tourist population; they concentrate on short stay, low risk, andhighly lucrative types of care, mostly abdominal surgery and obstetrics, andhave little impact on the bulk of the population.
89. The Government intends to extend the role of the private sector,and the State Planning Organization is exploring various alternatives.Technically, the role of private physicians, as providers of ambulatorycare, in solo or group practice, could be easily expanded. It would requirenevertheless that SIO and other health insurance schemes agree to reimbursea fixed amount for visits to private physicians; this is the way mostEuropean Social Security Systems operate. This could increase substantiallyaccess to care; quality of services could also be improved; finally, thepatient's free choice of physician, an issue of great concern to the MedicalAssociation, would be respected.
90. Expanding the role of private hospitals, would raise at leastthree technical and financial issues:
- First, small inpatient facilities, with limited resources,cannot apply standards of modern medicine which requires costlyequipment and an array of expertise. Larger group operatedfacilities would be more acceptable on technical grounds andcertainly more cost effective.
- Second, private hospitals can be profitable only if they skiminpatient care and concentrate on short stay low risk admissions(simple or intermediate surgery and obstetrics), and leaving longstay, high risk, high cost admissions to public hospitals.Therefore, investments in private hospitals in provincial capitalswould not be made unless substantial incentives were offered.
- Third, at the overall sectoral policy level it is argued that,for the time being, global bed capacity should not be increased.In this context, the expansion of the private sector implies atransfer of public or SIO facilities, i.e. a "privatization" of

- 38 -
some public hospitals. In terms of size, type, condition andlocation existing facilities would rarely be attractive to privateinvestors.
91. The proposal also raises a more fundamental issue, as the lot of asubstantial segment of the population could be worsened in the process. Thebulk of the population would still not be able to pay for private hospitalcare, unless third party payors foot part of the bill. The State, GERF,group insurance schemes, large companies, etc., could be made to reimbursepart of private hospitalization costs. The SIO itself already finds itadvantageous to use private facilities in areas where it does not operateits own hospital; and it could divest itself of all its facilities topurchase services in the open market, as advocated in some circles.Basically, however, the success of any attempt to expand the private sectorwould be contingent upon the existence of a third party payor. Conceivably,this could take the form, either of a universal health insurance program, orof a catastrophic insurance targeted to a segment of the population.
92. The foundations of a universal health insurance schRee, ensuringcomprehensive benefits to all individuals, already exist in Turkey, with the1961 law on IHSS, and the 1976 law creating the Universal Old-Age andDisability Pension Scheme. What would be needed is a mechanism to collect,in addition to government's financing under the overall budget (indigents orunemployed would be unable to contribute), mandatory mea-s-testedcontributions from potential beneficiaries, not already covered by thesocial security system. This seems to be the current line of thinking, asillustrated by the proposal to extend health benefits to BAG-KUR membe-s.
93. Alternatively, a more limited option would consist in the creationof a catastrophic health insurance program designed to put a ceiling onindividual financial exposure arising from occasional or prolonged disease.Ideally, annual health related expenses of each individual or householdwould be limited to a proportion of their income, which could vary with itslevel. In a long term perspective, such a system could curtail excessiveutilization of public services. However, its effective operation would callfor close monitoring of both incomes and health expenditures.
94. The choice is not an easy one as it would have direct implicationsfor taxpayers, and raise the risk of confrontation with strongly vestedinterests. Any decision in this area is bound to affect wage earners of themodern sector, i.e. the organized - and unionized - part of the labor force.To diffuse politically sensitive issues, and enlist the support ofinstitutionalized leadership and the population at large, it would beindispensable to set-up an effective consultative mechanism. Only thencould it be expected to overcome the resistance of ocganized labor, andcontributors of the Social Insurance Organization, when :hey will be calledto subsidize at least part of the health benefits for agricultural workers,the self-employed or the cohorts of unemployed.

- 39 -
B. Msaagement Systems and Issues
95. MOHSA's present organizational structure is the outcome of a longhistorical evolution and pragmatic compromise. Formal lines of authority areunclear and the department's operations are further disrupted by each changeof government. The weaknesses of the civil service in the health sectorhave long been identified by national and external expertsl7, but reformshave been hampered by passive resistance or open opposition from officialsconcerned or special interest groups. For instance. high level managerialpositions are almost exclusively held by male physicians, while middle levelmanagement positions are filled by other health personnel such as dentists,women physicians, veterinarians. or experienced paramedicals; practicallynone received formal training in management or administration; they showmore interest, and concern, for professional and technical issues than formanagerial or organizational problems. The same report noted in 1980 that"The government medical establishment is isolated from the larger concernsof health care in Turkey and unchallenged in its thinking.. Few health careexperts exist outside the narrowly medical disciplines.. The medicallytrained official is the sole and unquestioned decision maker in the MOHSA..The managerial model and the style of command within the Ministry would seemto be based on the clinical model.. Subordinates and the public are to beadministered to, and doctors are to deal with one another as independent.professionally ethical colleagues".
96. The sector's effectiveness is also affected by personnelmamnaement issues. many of which are beyond MOHSA's control. As most publicagencies, MOHSA suffers from overstaffing at the central level and inadministrative positions. Government's past lenient recruitment policy.designed to absorb labor surplus. resulted in plethoric and oftenunproductive personnel. Some senior professionals and technicians are paidabove the civil service scale, and many health personnel receive specialhardship allowances; however, as government salaries cannot keep pace withinflation and with the private sector. private practice or second jobs tendto expand for medical and paramedical staff alike. Frequent changes ofsenior staff constitute a major disrupting factor; these are generallypolitical appointees, replaced by each new government, even when no changein policy is involved. The lengthy replacement process generatesconsiderable stress on the individuals concerned and their subordinates; adifferent ideological emphasis may be introduced; on-going programs mayloose momentum or be canceled altogether; new teams have to be set-up and gothrough the normal learning process, while disillusioned civil servants waitfor the next government. As officials relieved of office must stay on theministry's payroll with the same salary. they load the civil service withposts of advisers or consultants. expecting to be one day reinstated.
17 See "The Management of Primary Health Care in Turkey' by Dr. IrisKapil, UNICEF, Ankara. March 1980.

- 40 -
97. Another factor affecting MOHSA, as most government departments, isthe lack of promotion opportunities. The rating system reaults in more than100,000 fotms filled every year and stored by the Personnel Office but thesystem is not geared to rewarding, or sanctioning, actual performance.Senior positions are frequently filled through outside recruitment ratherthan internal promotion. Finally, the coexistence of traditional and modernvalues in orgauizational thinking and management styles creates frequentfrictions highly detrimental to the smooth operation of governmentinstitutions.
98. A striking fact is the weakxiess of MOHSA's informatio, system, dueto the absence, in the organizational structure, of a general directoratefor statistics responsible for centralization, processing, analysis andfeed-back of epidemiological and health related data. As this functioncannot be performed by the existing Research, Planning and CoordinationCouncil - a relatively small unit whose limited staff is largely absorbed bythe preparation and follow-up on the ministry's budget - each directorateproduces its own set of statistics. This results in more limited coverageand lower quality of current statistics (generally processed by hand),duplication of efforts and, in the final analysis, a weaker statisticalbasis for planning, management, monitoring and evaluation.
99. Health services umaagement. The country's historical evolutionhas created a highly centralized public administration, with minimaldelegation of authority to lower levels of operations. This hierarchicalapproach also applies to the health sector. Hospital managers, programmanagers and all university trained health staff are appointed by theMinister. MORSA and SIO regulations stipulate that the hospital managermust be a physician, and the Minister makes his selection among the hospitalspecialists. In larger hospitals, this individual tends to be one of themost prestigious specialists. Management experience or ability to manage isnot a consideration in the selection of managers. Intdeed, management isoften viewed as that part of the organization which deals with laundry,kitchen, power supply, housekeeping, bookkeeping, transportation, etc. Infact, this practicing clinical specialist who is the highest authority inthe hospital is called "head of the hospital". The term "hospital director"is used for the person in charge of logistics, called a business manager inother countries; hospital directors are graduates from the School of HealthAdministration. Another key management position is the director of nursingto which one accedes after ten years of nursing experience, but againwithout a requirement for management skills and experience. At any rate,the hospital or the health center only controls a small part of the budgetsince salaries are paid centrally and do not enter the hospital accountingsystem. The part of the budget under control of the hospital's businessmanager deals with current expenses, some medical equipment and furniture,and repairs. The 'head of the hospit-l" is rarely involved in budgetarymatters. Cost accounting is absent a.d cost per unit of service is notavailable.

- 41 -
100. Primary health care shares most of the difficulties of otherhealth services. These are compounded by acute manpower shortages inoutreach services. For instance, about two thirds of health posts are notproperly staffed. Although 85% of health centers are manned by an MD, thisis often an inexperienced, unmotivated, not properly supervised MDperformitg his or her compulsory medical service; many are actively involvedin private practice after bours and therefore neglect outreach activities.Incomplete integration of activities raises another set of problems. TB andmalaria services were only integrated in 1980, under the PEC Directorate,but the 126 1CR centers and 370 MNC stations are still under the authorityof the Directorate of MCH and continue to operate under separate management,technical supervision and recording systems. Without the MCR and FPcomponents, the activities of the 3,000 health centers are incomplete, whilesome 500 NCH facilities remain isolated from the main stream of health careand are underutilized.
101. Lack of vehicles affects dramatically the efficiency of outreachservices: most village midwives have to rely on occasional transportation(mopeds have been tried successfully in some regions); half of the healthcenters have no vehicles; two thirds of vehicles in use are over 15 years ofage. Medical equipment, especially in health centers, is insufficient orneeds modernization. Public facilities provide only very basic or emergencydrugs and deliver prescriptions for the rest; however, as there are nopharmacies in rural areas, people tend to bypass the first or second levels.Finally, as PRC services do not charge fees, they cannot supplement theirrecurrent budget allocations and frequent shortages of fuel, drugs orsupplies paralyze their activities.
102. Maintenance of buildings, equipment and vehicles is remarkable byany standard. Hospitals as well as smaller facilities are well maintained,by numerous and well qualified personnel; yet, many old facilities, oftenover 80 years old, need extensive repair and remodeling that are well beyondthe limited regular maintenance budgets. Cleaning is scrupulously carriedout by in-house staff; some large hospitals have started contracting forcleaning with private companies, but it is too early to evaluate theirservices. Maintenance of equipment and vehicles is highly efficient. SomeX-ray equipment is over 20 years old, and still operating; 83% of thevehicles in services are over 15 years. Hospitals' mechanical andelectrical engineers are backed up by seven well equipped and well staffedRegional Maintenance Centers that carry out, with more ingenuity thanresources, impressive repairs that would not be undertaken in less cost-conscious countries. Sophisticated equipment is sometimes maintained withthe assistance of universities, in particular the Middle East TechnologicalUniversity. In spite of a very rational management of physical resources,the decline in real terms of maintenance budgets generates an increasingback-log of overdue operations. As at least 202 of facilities and equipmentare already totally obsolete, investment budgets must weigh carefullyexpansion of the system versus its modernization.
- 42 -
103. COustruCtion uanagemt follows rigid procedures. All projectproposals are subject to SPO approval before any funds can be appropriatedby the Ministry of Finance; the law applies to all public institutions,including the SIO. Responsibility for construction then passes to theMinistry of Public Works (ZIPW) which follows standard bidding regulations toaward the contracts to private contractors; this ministry will retain fullsupervision responsibility. Upon completion of construction, the healthfacility will be handed over to its owner, for commissioning and operation.These procedures have two weaknesses. First, the modest salaries for PPWstaff do not permit recruitment and retention of highly qualified architectsand engineers; this staff has limited expertise in design and inconstruction supervision of health facilities which partially explainsinefficient design of oversized and dysfunctional buildings; this willeventually result in higher operating costs. Second, management practicesresult in excessive delays, with hospitals taking 10 years or more to becompleted. The delays, which often work to the benefit of contractors, mayhave one or more of the following causes: the contractor underbids to winthe contract award and subsequently negotiates for additional funds afterconstruction has started; appropriated funds are not necessarily allocatedand construction programs are based on appropriated moneys; and higher thananticipated inflation rates result in the renegotiation of the contractswith frequent work stoppages.
104. Design parameters also have a crucial importance. It is customaryin Turkey to provide housing for staff, usually nurses, on the grounds ofhealth facilities. This practice greatly increases the surface requirementsfor all constructions of health posts and health centers. All healthcenters include 476 m2 for housing; this results in an extraordinarily hightotal gross building space of 813, 791, and 646 m2 respectively, for a cityarea, a district or a village. Similarly, a health post requires 120m2 which is at least 50% above usual standards. This is only partiallyoffset by relatively low construction costs (US$120 to 130 per m2 in October1985 for health centers and health posts, excluding equipment).
105. In the case of hospitals, the space required for staff bousing isrelatively smaller (less than 5% of the total gross space). But designparameters are not uniform and show remarkably wide variations. Thestandard 50 bed district hospital is sized at 5,027 gross m2, or 100 m2 perbed which is double internationally accepted standards; for a 100 bedhospital, this decreases to 80 m2, which is still too high. A 475 bedhospital (400 general care and 75 maternity beds) requires 22,386 grossm2 or an acceptable 47 m2 per bed, even including 682 m2 for nursequarters. The 1,000 bed MOHSA hospital in Izmir opened in 1982 has 117,000m2 of gross space or 117 m2 per bed which is extremely high even for ateaching hospital. Hospital construction cost was about US$ 150 per m2 inOctober 1985. The practice of building hospitals of over 1,000 beds shouldbe reconsidered as such large facilities have been proven to be lessefficient to operate.

- 43 -
106. Design parameters for future university hospitals have been set bythe Higher Education Council at a quite modest level. Gross space for a 600bed university hospital will be 40,000 m2 and double this amount for a 1,200bed facility. This translates into 67 m2 per bed, a relatively low averagefor a university hospital which requires classrooms, conference halls, morecirculation space, and more space between beds to accommodate students andprofessors; space standards for university hospitals are usually between 80and 100 m2 per bed.

- 44 -
IV. - SUCTODAL DUSOUR
A. Realth Personnel
107. In 1983, Turkey had more than 32,000 physicien, of which almost19,000 were specialists (see Table 9); there were in addition, about 6,800dentists and 11,400 pharmacists, all heavily concentrated in urbanareas. The national average of one physician for 1,400 persons comparedfavorably with other countries at the same income levels; however, thisratio concealed wide variations, ranging from 1/602 to 1/6334 (see Table12). On the other hand, the oversupply of specialists explains the high rateof vacancies in generalists positions in public hospitals, as well as thedifficulty faced by MOSA in extending health coverage in the provinces.The system's effectiveness is also affected by the imbalance between thenumbers of higher level and paramedical personnel, as the number of nursesis in the same range as the number of doctors.
108. The uneven distribution of high level health personnel isdocumented by some 1980 statistics. For example, 67% of the doctors wereworking in the cities of Ankara, Istanbul or Izair, an average of one doctorper 495, 585, and 733 persons respectively; in other provinces and in ruralareas, the ratio varied between 1/2500 and 1/14000. The distributionbetween public and private sectors is uncertain as physicians employed bythe public sector are authorized since 1981 to work part-time as privatepractitioners. In 1980 about 55% of the specialists were in the privatesector; 16% were on HORSA's payroll; 12% worked for the SIO; 11% for themedical schools; and the rest for other ministries and local authorities.As regards general practitioners, only 19% were included in the privatesector; 34% were working for MOHSA, 31% for the medical schools, 10% for theSIO and the rest for other ministries and local authorities.
109. The country has about 59,000 paramedical., or about one per 826population. Nurses and nurse aides are largely concentrated in hospitals,while most of the 14,000 trained midwives are assigned to rural areas.There are also some 12,000 health officers and technicians responsible forhealth education and environmental bealth; they are often involved indelivery of health services in the absence of physicians or nurses.Although there are enough nurses in hospitals, the quality of care,especially in smaller public facilities, remains low. The slow rate ofrecruitment for midwives and technicians has been a limiting factor in ruralareas. The future supply of midwives, who are the traditional basis forrural health care, has beeu further affected by the decision to close thevocational junior high schools for village midwives.
110. Nurses and midwives are employed almost exclusively by the publicsector; only 4% of the midwives but 34% of the technicians work for theprivate sector. Nurses seem more evenly distributed between regions andsectors, and reflect the existing infrastructure; in 1980, 74% were on

- 45 -
MOHSA's payroll, 12% worked for the SIO, 11% for the medical schools, andthe rest for other ministries of local authorities. The rapid increase inthe number of graduates at all levels was not aceompanied by parallelprogress in the quality of training; as regards nurses, this is aggravatedby, and further contributes to, deteriorating morale, insufficientmotivation, low salaries, and generally negative attitude of nurses towardstheir profession.
Ill. figher education and training of health personnel is provided byuniversities and specialized institutions. Until 1984, when nominal feeswere introduced at the higher level, public education in Turkey was free.Medical education lasts six years; post-graduate specialization requiresfour additional years in a teaching hospital or one of the large generalhospitals. SiDce 1981, medical graduates must serve two years in publichealth facilities. The country has 22 medical schools, 8 schools ofdentistry, 7 schools of pharmacy and five nursing schools attached to theuniversities. These universities also operate schools of higher educationwhere they train health personnel in specialized fields, such asphysiotherapy, rehabilitation, health administration, health technology, andnutrition. Finally, MORSA operates two schools of higher education for morespecialized personnel: the School of Social Work, and the Institute ofHealth Education.
112. The "hospital director" or business manager is a graduate of theSchool of Health Administration, transferred by MOHSA in 1982 to HacettepeUniversity in Ankara. The School is a four year post-secondary educationprogram; it has currently about 500 students in the regular license program,15 students at the master's level and 5 doctoral students. It accepts about100 students per year which is the number fixed by the Higher EducationCouncil. There is clearly an oversupply of graduates as many must find jobsin other sectors; a maximum enrollmeut of about 50 students per year wouldsatisfy the needs of the sector. A graduate will typically start a careerin the logistical services of a hospital and after ten years experience maybecome the "hospital director". The profession of health administration haslittle prestige as does public administration in general.
113. Paramedical training lasts four years after completion of thefirst cycle of secondary education; it is provided in MOHSA's vocationalschools for nurses, midwives and health technicians. Moreover, nurses aidesare trained in practical courses given in hospitals, vhile healthtechnicians (X-rays, laboratories, anesthesia) receive on-the-job training.The midwife is the backbone of the rural health care system since she isoften the only resource at the village level; but there are less than 14,000midwives for the 36,000 villages. The replacement of vocational schools forlower level village-midwives by training institutions for higher levelnurse-midwives has worsened the staffing problems of peripheral services.The Vth Plan has set a target of 10,500 additional nurse-midwives by 1990,but this type of personnel may find it difficult to adapt to a life longcareer in rural areas.

- 46-
114. As regards manpower development, four areas call for priorityattention, namely: the implications of a growing supply of health personnel,especially at the higher level; the compulsory medical service; the conceptof family physician; and training in public health and health management.The grovinag supply of health personnel has influenced the 1985-1990 ManpowerDevelopment Plan prepared by the Higher Education Council: it projects adramatic increase in higher education graduates, from 348,000 to 526,000 peryear. The REC also identified current shortages and set targets for somecategories of personnel, in the heaith sector in particular. These arepresented below.
BIGER EDUCATION CO CIocS PROJCTIONS OFMNNPORE I IN E T EALTh SSCOBR
1984 1990Exist in Needed Target
Nurses & midwives 62,000 75,500 112,000Technicians 15,000 15,900 26,600Dentist 7,800 8,700 12,900Pharmacists 12,000 12,000 12,000Physicians 33,600 37,800 56,200
TOTAL: 130,400 149,900 219,700
115. The method used, which adds up estimated vacancies with projectednorms, tends to overestimate actual requirements. Except for pharmacists,all categories of personnel would be substantially increased, by 68% for thesector as a whole; this "demand' for bealth personnel is expected to leveloff after five years. In quantitative terms, the existing system couldtrain the "needed" personnel. However, this increase in staff would bedifficult to absorb in such a short period. Moreover, it would be hard tojustify as long as the real issues related to the quality of training havenot been addressed. In more specific terms, even if only half theadditional supply were to be oriented towards the public sector (a ratherconservative estimate under current conditions), absorption of so many highlevel staff would require substantial increases in recurrent budgets. Theimplications of a rapidly growing supply of health personnel on the publicsector's development prospect warrant a more in-depth analysis than the oneprepared for the current five-year plan.
116. Issues related to the training of physicians preseutly dominatethe manpower debate. Medical education in Turkey has been for many years anexample of innovative development. Modern Turkey had adopted the Westernmodel of medicine and, for decades, a few medical schools turned out limitednumbers of graduates with solid scientific qualifications. In the early1960s, to balance the expansion of clinical services and hospital-basedteaching, and strengthen social and preventive medicine, the innovativeHacettepe medical school established Community-based teaching programs which

- 47 -
were to become blueprints of the future health system. However, during the1970's, demographic growth, increased health consciousness, extension ofcoverage to rural areas, and the development of higher technology increasedthe demand for physicians. As a result, the number of medical schools wasgradually raised to 22. Since 1981, in compliance with Governmentobjectives, these schools have substantially increased their intake and2,500 graduates are expected annually to meet YOK's objective of 56,200physicians in 1989.
117. This trend raises serious concerns among many medical educatorswho fear a further deterioration in education standards, as medical schoolshave neither the necessary faculty nor adequate operating budgets. First,training in basic sciences is likely to suffer most from the rapid increasein enrollments combined with budget restrictions affecting labs andeletronic equipment; this could result in a cohort of second rate doctors,as experience in many countries has shown that physicians never recuperatedeficiencies in basic science training. Second, clinical training wouldalso be affected by the deterioration of the student-instructor or student-bed ratios; however, this problem could be somewhat alleviated by increasingthe use of MORSA facilities as teaching hospitals. Finally, as regardspublic health training, rapidly increasing enrollments make it all the moredifficult to strengthen and expand training in such areas as epidemiology,sociology and demography, health administration, and community practice.
118. Since 1981, new graduates have to serve two years of CoupulsoryMedical Service (CMS) in public facilities; this does not exempt malephysicians from the sixteen-months compulsory military service. Thismeasure was introduced as a compensation, as medical education is stillpractically free (only nominal fees are levied since 1983). The experiencehas been so far very positive, but the foundations of the system must now beconsolidated. In general, young doctors have shown dedication and haveestablished good rapport with the population; the CMS is proving vital tothe health system in rural areas as primary health care consultations havedoubled in four years. The second batch of 3,000 doctors completed theirservice at the end of 1985, and the program is now being evaluated. Some ofits drawbacks have been identified already: lack of supervision and medicalguidance, absence of career opportunities, isolation, lack of vehicles foroutreach activities and limited contact with peripheral facilities andstaff. To improve training opportunities for these young graduates, MORSAenvisages splitting the CMS in two parts: one year of supervised service inhospitals (as an additional year of rotating internship) and one year inperipheral health centers. The evaluation will also include an estimationof needs for additional equipment and vehicles; it is also expected to dealwith the issue of improved incentives and working conditions.
119. The trend towards specialization (over 60% of Turkish physiciansare specialists) has created a shortage in general practitioners in front-line services; this is exacerbated by the inappropriate clinical training ofgeneral practitioners. To fill this gap the concept of Family Pbysician hasbeen put forward and has found strong supporters within MOHSA. A newspecialty in Family Practice, close to the US model, would be opened in the

- 48 -
universities, to train clinicians with a community orientation, to servemainly in the public sector. Post graduate training would last three years,i.e. one year of practice followed by two years of formal education. Theywould serve in intermediate and small facilities, as well as in urbanpolyclinics. Acting as team leaders for ambulatory care, they would referto, and coordinate as needed the activities of other specialists. Tofacilitate the transition and encourage students to enter the new system,incentives would be adopted; these could include the validation of one yearof CMS as the year of practice, an adequate salary upon certification andimproved career opportunities in the public sector.
120. The introduction of the Family Physician would influence thepattern of future outpatient services, and create a constituency of strongsupporters of "medicalization" of public health services. Therefore, it isessential to carefully assess the implications and potential drawbacks ofthe proposed reform, especially as the impact of this experience introducedin the USA less than ten years ago has not yet been fully analyzed. TheFamily Physician could rapidly supersede the general practitioner with theimmediate result of an extension of all medical studies by two or threeyears. This would have obvious implications on the cost of medicaltraining. Moreover, as shown by the US and Latin American experience, thiscould raise average costs of medical care, not only for the basicconsultation, but also by generating additional demand for moresophisticated and expensive services. In this context, it should berecalled that most European countries, because of the resistance of tIedicalAssociations, responded to the same issue by advocatirg improved training ofgeneral practitioners who have retained control of the first level ofmedical care.
121. Until 1965, training in public health was carried out at postgraduate level at a central School of Public Health; it was later onintroduced in the undergraduate curriculum of Medical Schools together withconmunity practice. The change has proved very positive as all physiciansnow receive basic training in preventive medicine. However, in the move,the country lost a valuable tool for training epidemiologists, public healthand tropical diseases specialists, general and hospital administrators; thisgap was only partly filled with the opening in 1982 of a special program forhospital directors in Hacettepe University. At the lower level, the RefikSaydan Institute of Hygiene, in Ankara, carries out inservice training forparamedical personnel, through periodic ad hoc courses for TB, malaria, orpharmacy technicians.
122. Post graduate training in public health is presently obtainedthrough overseas scholarships. Considering current needs, the organizationof a national program would be fully justified. An interestitngspecialization in public health is under consideration: a three year postgraduate training with a core of internal medicine, obstetrics. gynecology,pediatrics and infectology, and majors in epidemiology, primary health care,occupational or military medicine. As for the Family Physician the trainingobjective is a combination of clinical and public health skills, in thiscase with emphasis in public health.

- 49 -
B. Healtb Facilities
123. The number of facilities providing outpatient care is not vellknown as private practitioners cover a considerable, albeit not welldocumented, share of outpatient services, and all bospitals also provideoutpatient care. For its part, MOHSA operates an extensive network of about10,400 facilities consisting of 300 government physician's offices,2400 dispensaries and health units, 7100 health posts, and 500 MCH centersand stations. In addition, there are more than 8600 privately ownedpharmacies. The Fifth Plan's objective was to build 720 additional healthcenters, and 4215 smaller facilities by 1989.
Hospital lufrastructure
124. In 1984, the country had 730 health facilities for inpatient care,with a total of 115,600 beds (see Tables 13 through 16 and 30 through 34).Most of these beds belong to the three major care providers, namely MOHSA(52%), the SlO (15%) and the Universities (12%); the remaining isdistributed among the Ministry of Defense (13%), State Economic Enterprises,other ministries, large municipalities, minority and religious groups, andthe private for-profit sector (2.4% only). Special purpose hospitals andinstitutions are gradually disappearing through merger with largerfacilities, while smaller inpatient facilities are being closed altogether.Overall, Turkey has 2.4 beds per 1,000 population, a relatively favorableratio compared with other middle-income countries (Jordan, 1.9; Tunisia,2.1; Colombia and Ecuador, 1.8). But this capacity is not fully used as"staffed" beds represent only 87.5% of the total ("approved" beds). Thisdrops to 2.1 the real bed/population ratio. The unused capacity is causedby lack of staff and/or equipment, but also by the use of the space fornurse residences; it is normal for nurses to live on hospital grounds, but anumber of facilities did not include nurse quarters in their buildingplans. There are wide geographical differences in the bed/population ratio(4.4 in Istanbul, against 0.3 in Agri and Hakkari provinces).
125. There are 451 WOES hospitals in the country, with 60,500 beds,including more than 100 health centers; this total also includes 35 longterm facilities with some 13,600 beds. Most of MOUSA constructions werebuilt in the 1950s; some date from the first years of the Republic. Old aswell as more recent hospitals are always spacious, solidly built andremarkably maintained. In keeping with the concepts of the 1950s, directservice areas such as halls, corridors, waiting rooms, wards and nursingstations, are generally sized liberally, allowing for additional capacitywhen needed. Conversely, support areas such as X-rays, labs, offices,laundry, kitchen, etc., are barely sufficient. There is a marked deficit ininternal communications space, as well as elevators for materials, staff orpublic. Finally, most emergency and outpatient departments have becomeinsufficient to meet the needs of growing urban populations.

- 50 -
126. Equipment of public hospitals is modest and generally aging.Hostelry equipment such as beds and other furniture is sturdy. Diagnosticmedical equipment such as radiography. scintigraphy. echography. laboratorymay be adequate for routine secondary care testing, but is ofteninsufficient or outdated for tertiary care; shortage of high performanceequipment, such as fast X-ray processors and multianalyzers. slows down bedturnover. Therapeutic equipment in operating rooms and intensive orintermediate care units is generally sufficient but specialized equipment islacking or is of lov quality in radiotherapy. rehabilitation therapy andprosthetics units. Finally. equipment for kitchen. laundry. sterilization,power and water systems is. as a rule, contemporary to the construction ofthe hospital and has been kept operational through exceptionally goodmaintenance. in spite of its diversity due to age and lack ofstandardization. A carefully planned re-equipment and modernization ofservices would be a highly cost-effective investment by improving thequality of care and increasing the overall productivity of the system.
127. Staffing is adequate but sometimes excessive in smaller hospitalswith low utilization rates. Managerial and administrative staff are rarelyproperly trained, but medical personnel are competent and recruited amongthe best. Nursing staff is efficient and highly disciplined. Ancillarypersonnel is abundant. Overall. staffing does not raise any constraints inhospitals operations, although low salaries scales affect morale andperformance, especially at the middle and lower levels.
128. The SIO operates 77 short-stay hospitals with more than 17.700bedsl8. SIO hospitals are generally more recent and better equipped; theirstaff are better paid than civil servants, with a marked difference at themid-level. All but three of these hospitals have more than 100 beds.Overall, 302 of admissions are in obstetrics; few complex and hightechnology procedures are performed, as these cases are referred to MOHSA oruniversity hospitals. SIO's clients are mostly urban-based and the fivecities with the highest number of hospital discharges are: Istanbul(131.600). Izmir (63,700). Ankara (38.100), Zonguldak (31,600). and Bursa(28,900). These five cities account for half of SIO's hospitalizations.
129. The 20 universities operate 21 university hospitals (two inIstanbul University). with 13,800 beds; there is also one military medicalschool. Table 33 lists the university hospitals attached to these medicalschools together with utilization statistics derived from the MOHSA datasource book for 1984. No information is available on the military medicalschool hospital, and Edirne University is not listed with a universityhospital. Sixty percent of the beds are located in four universityhospitals: two in Istanbul, one in Ankara and one in Izmir, and they accountfor 50% of all admissions. University hospitals in Turkey do not only treat
18 The 1984 SIO activities report lists a total of 18,314 beds; this is3% higher than the MOHSA data source, and may be due to the inclusion ofbeds in some dispensaries.
- 51 -
the more severe cases. as is often the case in developed countries, butreceive a mix of patients.
Hospital Utilization
130. For the sector as a whole, the average of 48 ad&isiaon perthousand population is relatively low by international standards19. Formiddle income countries this ratio is in the 70-90 range. One fourth ofinpatients are treated in SIO facilities. and about 10% of hospitaladmissions for SIO beneficiaries are contracted out to other providers inthe public or private sector. Overall, the admission rate for this insuredpopulation is. coincidentally, also 48 per thousand. This is a surprisinglylow rate for a population with full medical insurance coverage. as uninsuredpatients treated by MORSA have similar utilization rates.
131. Occupancy rates vary widely. but are gonerally low. In 1984, forthe three major providers, they were 54% (MOHSA and Universities), and 67%(SIO)20. Larger, older and well established facilities tend to have higheroccupancy rates. In the case of MOHSA average low occupancy can bepartially explained by the existence of 103 health centers with beds (15%average occupancy), and by the fact that more than half of its hospitalshave 100 or less beds; smaller facilities tend to have lower occupancyrates. typically around 50-60%. University hospitals show large variationsranging from a low of 37% to a high of 75%,
132. Average lengtbs of stay (ALOS) are generally high, and variationsare quite marked for all providers. MOHSA and SIO hospitals. which accountfor 85% of all hospitalizations, have an ALOS of 7.1 and 7.7 respectively.In University hospitals, ALOS are in the 6.7-13.8 range, with an average of10.2 days. The national average is 7.6 for all hospital stays but drops to6.4 if only acute care short-stay hospitals. which account for 97% of alladmissions. are considered.
C. Health Cooto Sn Financing
133. Scanty data are a major obstacle to a comprehensive analysis ofcost and financing of services in the sector. Only rough estimates can bemade of households expenditures on health and there is no direct access tocosts of services provided by privately owned facilities. No data arereadily available on medical expenditures of large private companies who
19 Hospital statistics used in this analysis exclude the 44 militaryfacilities with their 15.100 beds for wbich no utilization information couldbe obtained.
20 The SIO reported a 71% occupancy rate in 1984.
- 52 -
often provide additional health benefits to their employees. Information onthe cost of services in SIO facilities is not collected systematically. andthe real level of health expenditures by the social security system is notwell known. The situation is only slightly better in the public sector, atleast as regards expenditures. which nevertheless tend to be equated withcosts of service delivery. Only the major university hospitals gatherrelevant data but these are not published and no systematic analysis isconducted. even at the individual facility level.
134. No attention seems to be paid to the cost of outpatient core. Inpublic health facilities. this cost is extremely low and could easily becalculated for dispensaries and health centers where expenditures consistalmost exclusively of salaries (only emergency drugs and supplies areavailable in limited quantities). Estimates would be more difficult to makefor hospitals where outpatient services are manned by the same personnel anduse the same equipment and laboratories. These daily clinics attract aconsiderable number of patients: the ratio of visits to admissions in publichospitals is almost 14 to 1 (see Tables 32 and 33). This excessive burdenon hospitals affects their effectiveness. as discussed below, but alsogenerates higher operating costs by encouraging use of sophisticated andexpensive services, not always justified for simple out patient care.
135. In SO hospitals, consultations are prepaid by beneficiaries. InUniversity hospitals. fees vary with the institution and the type ofservice. and are substantially higher than in public hospitals. As forMOESA facilities, the charge for outpatient visits was set at TL100 from1981 through the end of 198421; physical examination charges were set atTL1000. These fees were raised to TL500 and TL2500 respectively in thebeginning of 1985; in real terms. this represented a 46% increase in chargesfor outpatient visits. but a 27% decrease in charges for physicalexaminations (see Table 23).
136. Neither the SIO. nor any University or MOHSA hospital provide dataon their costs of inpatient care. An analysis of expenses per patient day.and per bed, was conducted by the mission for a sample of MOHSA hospitals(see Table 34). It confirmed the wide spread between daily expenses perbed. and per patient, a direct reflection of the nature of the institutionand variations in occupancy rates. It showed that in 1984 the average costper patient day was in the range of TL3-11,000 in general hospitals (US$8-29). about TL6,000 in teaching hospitals, and twice as much in the mostspecialized facilities. These very low costs for a middle income countrywere confirmed by spot checks in other public facilities. The study alsorevealed that personnel expenditures represent more than 70% of expenses ingeneral hospitals, against 40-50% in teaching hospitals and around 40% inspecialized institutions. User fees cover only 5-12% of total expenses ingeneral hospitals. 13-19Z in teaching hospitals, and as much as 30-35% ivspecialized surgery facilities.
21 This corresponded to US$0.90 and US$0.27 at the 1981 and 1984exchange rates.

- 53 -
137. Cost recovery in the public sector is only partial and adjustmentshardly keep pace with inflation. Table 23 presents the fee schedule appliedin NOH&A facilities for inpatient and outpatient care; it is of specialinterest as it compares fees applied since January 1985 (under a currentinflation rate of more than 40% p.a.). with the ones which prevailed fromApril 1981 through December 1984. The very structure of the schedule isquestionable as it does not reflect the relative cost of each service or thereal level of expenses incurred. More disquieting is the fact that. in realterms, fees were raised for most outpatient services (to TL500 or almostUS$1 for a simple visit). but reduced (often substantially) for inpatientcare. Although it may be justifiable, on social grounds, to cut by 56% thecharge for use of intensive care units. it seems more difficult to explain a42% ..eduction in charges for "deluxe" accommodation in public hospitals (51%in the case of private rooms).
138. Overall. cost recovery in the 206 MOHSA hospitals authorized tolevy user fees amounted to TL6.3 billion in 1984 (US$17 million), i.e. lessthan 8% of the ministry's recurrent budget. In real terms. this representedmore than twice the amount collected in 1980. but a reduction of 10%compared to 1981, after the previous fee adjustment. Chart I illustratesthe erosion of annual resources, and the swing generated by the 1981adjustment in selected hospitals. It is not possible at this stage toassess the impact of the 1985 revision of the fee schedule.
139. Total health expenditures represent about 3.5% of the country'sGNP; this ratio is below the 42 or more found in other middle incomecounti-ies or in Latin America. Total health expenditures exceeded TL407billion in 198322; this corresponded to almost TL8.600 per capita (US$38).Private expenditures amount to 58% of the total; this estimate is derivedfrom the last household expenditures survey which showed that, in 1978/79,2.8% of private income was spent on health related services. Another sourceindicates that in 1974. household expenditures on health absorbed 4.8% ofavailable incomes in rural areas, against 3.3% in urban areas; the lowerratio for the cities was explained by easier access to free public services.Since 1982. total public investments have been declining in real terms (seeTable 20). They also declined in relative terms. i.e. as a proportion oftotal public investments. Between 1982 and 1985. annual investments in thepublic health sector were reduced by almost 40%, although total publicinvestments increased by 8%. As a consequence, the share of health in totalpublic investments has fallen from 2% in 1982. to 1.1% in 1985.
22 This figure does not include outlays from the Miaistry of Defence.or private investments, which may amount to 5% of public investments.
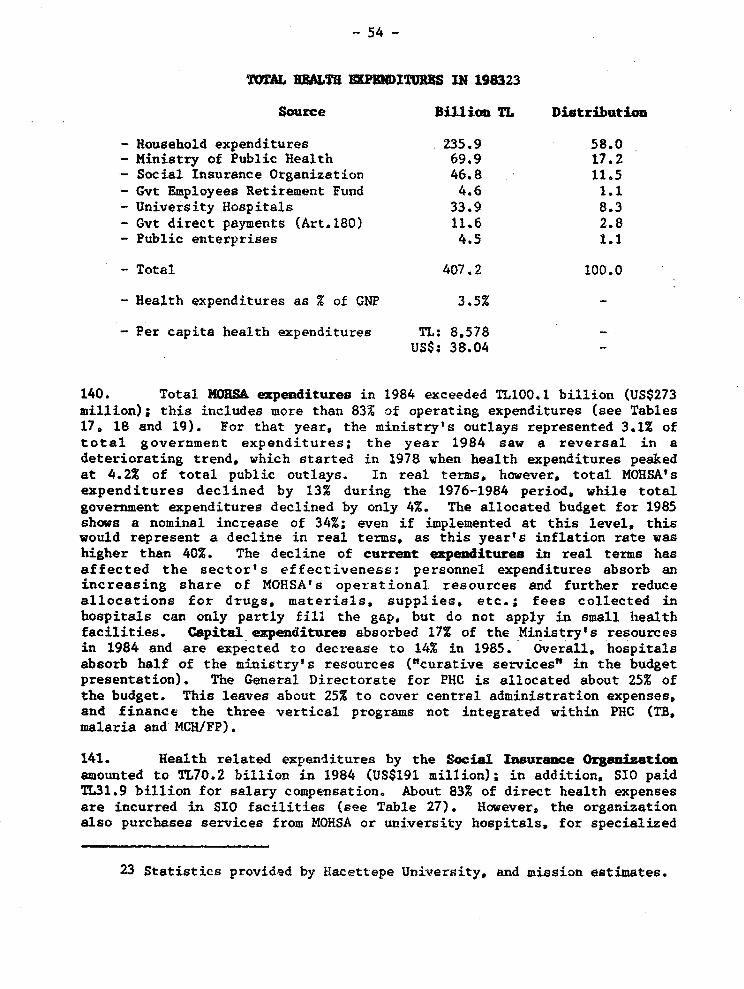
- 54 -
TOTAL U8ALTU KPEEDITURES IN 198323
Source Billion TL Distribution
- Household expenditures 235,9 58.0- Ministry of Public Health 69.9 17.2- Social Insurance Organization 46.8 11.5- Gvt Employees Retirement Fund 4.6 1.1- University Hospitals 33.9 8.3- Gvt direct payments (Art.180) 11.6 2.8- Public enterprises 4.5 1.1
- Total 407.2 100.0
- Health expenditures as % of GNP 3.5% -
- Per capita health expenditures TL; 8.578 -
US$: 38.04
140. Total NORSA expenditures in 1984 exceeded TL100.1 billion (US$273million); this includes more than 83% of operating expenditures (see Tables17. 18 and 19). For that year, the ministry's outlays represented 3.1% oftotal government expenditures; the year 1984 saw a reversal in adeteriorating trend. which started in 1978 when health expenditures peakedat 4.2% of total public outlays. In real terms, however, total MOHSA'sexpenditures declined by 13% during the 1976-1984 period. while totalgovernment expenditures declined by only 4%. The allocated budget for 1985shows a nominal increase of 34%; even if implemented at this level, thiswould represent a decline in real terms. as this year's inflation rate washigher than 40%. The decline of current expenditures in real terms hasaffected the sector's effectiveness: personnel expenditures absorb anincreasing share of MOHSA's operational resources and further reduceallocations for drugs, materials, supplies. etc.; fees collected inhospitals can only partly fill the gap, but do not apply in small hlealthfacilities. Capital ezpenditures absorbed 17% of the Ministry's resourcesin 1984 and are expected to decrease to 14% in 1985. Overall. hospitalsabsorb half of the ministry's resources ("curative services" in the budgetpresentation). The General Directorate for PHC is allocated about 25% ofthe budget. This leaves about 25% to cover central administration expenses,and finance the three vertical programs not integrated within PHC (TB,malaria and MCH/FP).
141. Health related expenditures by the Social Insurance Organizationamounted to TL70.2 billion in 1984 (US$191 million); in addition. SIO paidTL31.9 billion for salary compensation. About 83% of direct health expensesare incurred in SIO facilities (see Table 27). However. the organizationalso purchases services from MOHSA or university hospitals, for specialized
23 Statistics provided by lzacettepe UniNtersity, and mission estimates.

- 55 -
treatment or in areas where it does not operate its own facility: theserepresented 12% of total expenses in 1984. Finally. investments absorbedabout 5% of annual expenses. The health branch of the SIO still shows apositive balance as contributions for health and maternity represented 184%of outlays in 1984 and 195% in 1983. However, the deteriorating trend isevidenced by the decline in real terms of health and maternity contributions(see Table 26).
142. Annual health benefits paid by the Government Employees RetiremeAntFund have more than doubled in real terms since 1979 although the number ofbeneficiaries increased by only 30% (see Table 28). They amounted to TL7.?billion in 1984 (US$19.6 million) and consisted mainly of drugs (59%),hospital expenses (22%), and dental treatments (17%). The budget of eachministry and public institution includes an earmarked provision forreimbursement of medical expenses incurred by active civil servants; thisappears in Article 180. In 1984, these public expenditures for healthamounted to TL12.3 billion (US$33.5 million), compared to TL11.6 billion in1983.
143. Health expenditures of University Hospitals are significant andrepresent more than 8% of the total. or about half tMOHSA's expenditures.The estimate for 1983 was TL33.9 billion (US$150 million). including TL8.3billion for investments24. But the real level of these expenditures is notwell know as the budget of each university hospital is part of the budget ofthe medical school which, in turn, is included in the larger budget of theuniversity. Moreover, fees play a very important role in universityhospitals which are free to determine their level and adjust them regularlyto keep pace with inflation; in addition. donations from individuals andcontributions from charitable institutions are not negligible. Fees anddonations amount to substantial resources but information on their amountsis not readily accessible; in the case of the two facilities operated by theUniversity of Istanbul, they are said to be of the same magnitude as thebudget appropriations. In more general terms, it seems that in universityhospitals, fees account for at least as much as regular salaries inphysicians incomes. This practice is not authorized in MOHSA hospitals.
D. Pharwaceuticals
144. The foundations of a modern pharmaceutical industry were laid in1928 with the first law that regulated imports and sales of drugs. andencouraged local and foreign investment in this sector. Large investmentswere made in the mid-1950s. including by some multinational corporations.The itdustry now includes 86 establishments, five of which belong to the
24 Prof. M. Tokat, Hacettepe University.

- 56 -
public sector25. Of the 81 private companies. 7 are foreign-owned; 16 ofthe private plants produce raw materials as well as drugs. This is arelatively modern and capital-intensive industry representing almost 25,000jobs; it exports drugs to industrialized countries and technology todeveloping countries. The 10 largest producers, which include 5 of theforeign companies, account for more than 66X of output. Although MOHSAproduces a substantial share of its vaccines needs. it does not operate adrugs production unit.
145. Total production. by manufacturers prices. peaked in 1982 atUS$427 million but fell to US$317 million in 1984. It is largely based onimported raw materials (US$121 million in 1984). which reduce substantiallyimports of drugs (less than US$3 million). The local industry produces 1810different drugs, under more than 3500 dosage forms; this includes 3.3million cycles of contraceptive pills. marketed under 8 names. and producedby five companies. Most large public hospitals have a laboratory for galenicstandard preparations. The local industry also produces an increasing lineof medical and surgical supplies and small appliances. Overall. about 9.000drugs are registered in Turkey, but only 2.500 are in the market as many areoutdated, or have been replaced by new lines of products.
146. The Refik Saydan Institute of Public Health produces vaccines,serum and biological reagents. Vaccine production includes BOG. DPT,measles, polio and rabies, but covers only part of the needs of the country.For the immunization campaign, it supplied 25% of requirements. Some of thebacteriological techniques must be modernized and the virological ones mustbe expanded. Considering the country's population and potential savings inhard currencies. MOHSA envisages completing the vaccine production to becomeself-sufficient. The Institute of Public Health, under the Department ofPharmacy and Pharmaceutical Products, is responsible for quality control ofdrugs (registration and off-the-shelf testing), cosmetics, and narcotics.
147. Pharmaceuticals c _,ption is still relatively low. at US$7.60per capita in 1984. The Manufacturer's Association has calculated that, in1984, the ratio of drug consumption to GNP was 0.7% in Turkey, compared to1X in Switzerland and the United Kingdom, 1.2% in W. Germany and France. and1.9% in Japan. Consumption remains at minimal levels in public hospitalsand shortages are frequent in smallest facilities; as for out-patientfacilities, they only carry a minimum stock of emergency drugs, and patientsare expected to purchase their own drugs. This situation is in strongcontrast with conditions prevailing in university hospitals and SIOfacilities. This explains why drugs and medical supplies amounted to onlyTL6.8 billion in 1984 (US$18.5 million), or 8g of MOHSA's operating budget.In large MORSA hospitals. drugs and medical supplies represent 9-15S oftotal costs, being higher in specialized than in general hospitals; in50-bed district hospitals, they rarely exceed 5% of expenses. Information
25 Data in this section were provided by MOHSA's General Directoratefor Pharmaceuticals and the Pharmaceutical and Chemical ManufacturersAssociation
- 57 -
on drugs expenditures in university or SIO hospitals is not readilyavailable but it will be recalled that, overall, these represent 25% ofhealth expenditures of the SIO and 59% of GERF's.
148. The retail distribution of drugs to consumers goes either throughinstitutions as SIO, GERF and their consumers' cooperatives, or moregenerally through the large network of 8,000 retail pharmacies. However,since MORSA facilities do not provide medicines and small retail outlets arenot authorized to dispense drugs iu the absence of a pharmacist, ruralpopulations have limited access to basic drugs.
149. Turkey runs a large foreign trade deficit iu pharmaceuticals,which exceeded US$114 million in 1984, and US$75 million during the firstsemester of 1985. This is because, although it imports less than 1% of itsdrugs, it still imports two-thirds of the raw materials needed for itsindustry; in 1984, the country purchased abroad US$2.7 million of drugsagainst US$120.9 million of raw materials. Total exports cover only 13-16%of imports; they amounted to US$16.1 million in 1984, and US$12.6 millionduring the first semester of 1985. The tripling of exports of raw materialssince 1980 illustrates improving quality standards of the local industrywhich is now selling for instance acetylsalicilic acid and tetracycline toEurope and the USA. Pharmaceuticals are now sold to 19 foreign countries,including 7 industrialized eastern and western countries.
150. Strict quality controls are imposed on the pharmaceuticalindustry. Moreover, sales prices must be approved by NOHSA, while markupsare limited to 9% for wholesalers and 25% for retailers. Profits of thedrug manufacturer may not exceed 15% of the corporation's yearly revenuesor, for individual drugs, 20% of the product's yearly sales. Moreover,MOESA exerts leverage on local manufacturers through import licencing whichmay affect their production or pricing policies. It also oversees theactivities of the 8,600 private pharmacies scattered around the country.Updated regulations were introduced in January 1985 and, in anticipation,large investments were made during the last two years.
151. Turkey has not yet adopted a clear policy towards essential drugsor generics. The interpretation of "essential drugs", deviates from the WHOlist of precisely defined chemicals, to include drugs that are considereduseful. MORSA has not adopted standard drug lists nor standardizedtreatment protocols for hospitals or health centers, much less incentives toutilize essential drugs. Because of the pressure of advertising andmarketing, generics are almost unknown in the private sector, either to theprescriber or to the pharmacist. Similarly, only a few generics areutilized in MORSA, SIO or University Hospitals, where no Drug UtilizationReview committees have been set up to improve scientific quality oftreatment and reduce the costs of medicines. The Government shouldencourage changes in that direction.

- 58 -
152. Access to basic drugs26 is another area of concern f or MOHSA.Aside from a small supply of emergency or TB drugs, health centers andvillage midwives do not have medicines in stock; they write prescriptions.However, because the commercial drug outlets are very few in rural areas,actual access to drugs is often limited. The cost of drugs creates anotherconstraint. SIO and GERF secure co-payment for prescribed drugs (80% foractive affiliates and 90% for retirees and pensioners). However, indigentscannot afford to pay for prescriptions. The problem is more acute forchronic treatments such as diabetes. hypertension or arthritis, or in thecase of cancer chemotherapy; the latter, either as adjuvant or curativetherapy, costs an average of US$300 per treatment (excluding adriamycine andother expensive drugs) or 3 times the minimum monthly salary.
153. MOHSA has the overall responsibility to design and enforceregulations on manufacturing pra.tices and ensure high quality standardo; itcollaborates closely with WHO in this area. Its staff at the central levelincludes more than 80 professional pharmacists and there are 67 provincialunits of varying importance; MOHSA also operates the Central ControlLaboratory, staffed with 70 pharmacists. Quality control is an area ofgrowing concern for MOHSA. Until recently, industry had not felt the needto upgrade their production methods. Government's inability to controlquality, and therefore to enforce strict regulations especially on smallmanufacturers, left the door open to leniency. In 1984 however. to complywith internationally accepted standards and preserve the prestige of localproducts. Government and industry agreed to adhere to the Good ManufacturingPractices Code tGMP)D by November 1986. As a result, many companies areinvesting heavily to ccmply with GMPs, to avoid being absorbed by largermanufacturers or going out of business. To carry out its extended mission,MOHSA's Control Laboratory must be expanded. Its different units presentlyperform 3500 tests each year. This performance could be stretched to 4.000tests within acceptable safety margins, but the estimated 14.000 tests thatwill be needed by 1987 will require the expansion of laboratories,additional equipment, computerization of administrative procedures andrecords. and training of specialized staff. The total cost of thisoperation is estimated at US$750.000 and the Government is exploringalternatives for financing this expansion.
26 The deliberately loose denomination of "basic drugs" regroups some20 to 40 drugs that are either of domestic use and available withoutprescription (aspirin, vitamins, cold medicines. etc.). or drugs that areneeded for primary health care programs (oral rehydration salts.chloroquine. iron preparations. etc.).

- 59 -
V. lAYING 7 FOUNDMIONS OF L DEVELOlIiF T STIATEGY
154. Substantial improvements have been achieved in the health sectorover the past two decades and most Turkish indicators now compare favorablywith similar data for other middle-income countries. Nevertheless, strikinginequalities in health status, fertility levels and access to basic healthservices still exist between Western and Eastern provinces, and betweenurban and rural areas. Large segments of the population still suffer fromsurprisingly high infant and child mortality rates, persistent prevalence ofinfectious diseases, malnutrition, and relatively high levels of fertility.These are compounded by environmental factors, reflecting a low, and oftendeteriorating, quality of life, especially in periurban areas, brought aboutby nearly two decades of accelerated internal migration.
155. Efforts te improve the health status of lower income groups, tocheck the spread of infectious diseases such as tuberculosis and malaria,and to control the most frequent childhood diseases, have not achieved theexpected results. The IHSS has not yet succeeded in reducing inequalitiesin health status and access to basic health care. The integration ofservices has been retarded by vested interests, bureaucratic and politicalresistance, and the lack of financial support. This is best illustrated bythe low levels of immunization and contraceptive prevalence in rural areas.No routine program for childhood 4wmunization is implemented by the publicsector and, until the end of 1985, responsibility for vaccination seemed tohave been left to parental initiative, or at least to those parents whorecognize the need, have access to the service and can pay for it. There isstill a large unmet demand for family planning services, but the absence ofan explicit nationwide population program remains an obstacle to speedyprogress in coverage.
156. The present health status of the Turkish population has beenstrongly affected by extensive internal migration fueled by the rapidindustrialization of the 1970s, then by economic stagnation, decliningincomes and high levels of unemployment. However, this low health status isalso the outcome of organizational and managerial constraints, exacerbatedby declining financial resources, at a time when a very strong social demandfor improved public health services generates a continuing pressure forhigher levels of expenditures.
157. Under its current policy, the Government is determined torestructure and liberalize the economy and promote the privatization ofactivities which the private sector can handle more efficiently. Hovever,while privatization in the health field may be appropriate in someinstaries, this would not permit the Government to extricate itself from theprovision of health services, or to reduce dramatically public healthexpenditures. It is advocated in the following pages that even in thecontext of the legitimate objectives pursued by the Government, there arecompelling reasons for sustained high levels of public expenditures in thehealth sector. General arguments in favor of a public health sector are

- 60 -
well known: the State must retain its fundamental responsibility in mattersof preventive care, containment of communicable diseases, and emergencyservices; moreover, it must ensure access to basic health services to thepoor; finally it is in the national interest to maintain adequate health andnutrition standards, and to encourage the reduction of fertility rates tolevels compatible witb the country's resources and development prospects.
158. In the case of Turkey, more arguments militate in favor of acontinuing public presence in the health sector. First, on-going economicand fiscal constraints limit what the Government can do at present toimprove the incomes of the most vulnerable and disadvantaged groups; thesegroups therefore require particular attention to ensure adequate access tohealth services, at least until structural adjustments have started bearingfruit. Second, sustained public expenditures are needed to lay thefoundations of a more efficient, financially sound, public health sector,capable of providing quality services to all segments of the population, ata cost acceptable to the individual and the community at large.
159. Most Turkish data are within the range of international indicatorsfor middle income countries; indeed, many of these countries display muchworse indicators for mortality, life expectancy, calorie intake orfertility. Yet, one can be more demanding in the case of Turkey, because ofits long history, solidly entrenched traditions, abundant and qualifiedlabor force, and vast infrastructure. First, as mentioned repeatedly inthis report, national averages hide unacceptable disparities, most notablyregarding infant mortality and fertility rates, and access to basic healthservices. Second, Turkey has most of the resources needed to address itshealth problems successfully, provided the right steps are taken to overcomewell recognized obstacles, and agreement can be reached on an appropriatedevelopment strategy.
160. Consequently, the fundamental objective of the sector should be tostrengthen the effectiveness of the health care delivery system, with a viewto redressing existing inequalities in terms of health and nutritionalstatus, fertility, and access to basic health services, and furtherimproving the overall status of the population. Under current tightmonetary policy, the challenge confronting the Government would be toachieve this objective without major investments and/or substantialincreases in operating budgets; secondarily, it would appear feasible tomobilize additional resources by levying higher fees from users able, andwilling, to pay. The development strategy proposed to achieve thisobjective would revolve around seven themes, namely: (i) the creation of anappropriate coordination mechanism; (ii) the critical evaluation of the on-going and prospective sectoral investment program; (iii) the design andimplementation of a priority primary health care program targeted tospecific population groups; (iv) the improved utilization of existingfacilities; (v) the improved financing of bealth services through anadjustment of the user charges system, and (vi} the strengthening of socialsecurity's financial basis; this action program would be backed up by (vii)an applied research program, designed to pave the may for more fundamentaland long lasting interventions.

- 61 -
A. Improving Coordinotion of Sectoral Activities
161. The preceding pages have given ample evidence of the lack ofcoordination of sectoral policies and interventions between the mainproviders of health services. At a time when a restructuring of the economyis taking place, when crucial issues are being debated in the country andmajor reforms contemplated, the absence of a8 appropriate mechanism todiscuss the sector's development prospects and identify coherent proposals,is a dramatic gap which must be corrected without delay. The State PlanningOrganization, absorbed by many other tasks of a more general uature, cannotfulfill this technical and policy role. On the other band, the stronglycentralized system, which requires SPO's participation in most phases of theplanning process, is detrimental to the flexibility needed to adapt torapidly changing conditions. SPO's major functions are hampered byinvolvement in details at the project level. Only a coordinating body couldset the stage for an in-depth discussion of available options and provide amuch needed technical basis for future governmental decisions. Because ofthe multiplicity of agencies involved, such a coordinating body would needto take the form of an Interministerial Higber Health Council headed by thePrime Minister. Its Secretariat would be assured by the Ministry of Healthand Social Assistance, mandated by law to regulate and control all publichealth activities.
162. The Higher Health Council would be responsible for developingstandards, establishing priorities, and designing and coordinating theimplementation of a sectoral development strategy outlined below. It wouldalso commission a series of much needed studies on such topics as theimprovement of the utilization of existing facilities; the design of newcurricula for training of public health specialists and hospitaladministrators; the cost of inpatient and outpatient services in the varioustypes of facilities; effective ways of reducing regional disparities interms of coverage and quality of services; alternative ways of financinghealth service delivery; monitoring of sectoral recurrent and capitalexpenditures; etc. This program provides strong justification forstrengthening and upgrading the Research, Planning and Coordination Unit tothe General Directorate level.
B. Strengthening Investmet Planing
163. Improving the iuVestment planning process in the sector is longoverdue. The updated list of projects included in the Fifth Plan providesthree sets of financial information for each project: (i) its total cost,including in some cases the foreign exchange component; (ii) the cumulatedcapital expenditures through the end of the year; and (iii) the allocationof the Ministry of Finance for the current year, or rather the allocationrecommended by SPO. As far as the health sector is concerned, these dataare meaningless for three reasons:

- 62 -
- in the context of the high inflation characteristic of recentyears, sight has been lost of base costs of on-going projects;although these have been increasing regularly and oftensubstantially in real prices, the amounts mentioned in Plandocuments are not updated periodically; for example, the currentcost of the 1,110 bed hospital planned by the SIO in Izmircertainly exceeds TL7 billion, but is shown as TL4 billion in mostrecent SP0 documents;
- the cumulated investments for each on-going project aggregaterapidly depreciating moretary units of succeeding years over fiveto ten years periods; chey are actually provided only for bookkeeping purposes;
- the current year allocation for each project is also onlyindicative as it is not expected that the amount agreed upon withSP0 will actually be available; red tape and administrative delaysin releasing funds are general causes for, or means of, reducingpublic expenditures; moreover, each allocation is decreased by the1OZ value added tax; finally, the nominal allocation issubstantially eroded by the current 40Z inflation rate.
164. Moreover, the implications of these projects in terms ofadditional operating costs and manpower requirements are generallyoverlooked.
165. The SI0 Izmir hospital illustrates the uncertainty surroundingmany projects in the health sector, and more generally the planning processitself. In the 1986 update of the Plan document, it is presented as a1100-bed project launched in 1978; its total base cost is given as TL4billion; it is further mentioned that TL233 million have already been spentunder this project; finally the 1986 allocation to continue implementationis put at TLIOO million (less than US$200,000 at going rates). The realityseems to be quite different: first, local SI0 authorities refer to it as a600-bed facility; second, the actual cost of the construction alone willundoubtedly exceed TL7 billion (1985 prices); moreover, implementation is atthe very early stages and sunk costs are minimal; finally, in view of thetotal cost of the project, its priority status, and the rather limitedamounts spent so far, one may wonder what progress could be achieved with aTL100 million allocation expected to be eroded by some 30-40% by inflationand late appropriation.
166. Under prevailing conditions, it is understandable that technicalunits in charge of project monitoring would concentrate on current yearinvestments. But this has led to an implicit change in concepts. Sectoraldocuments updated by SPO have come to represent a list of annual capitalexpenditure proposals, ratber than projects to be implemented during a givenperiod to achieve the Plan's objectives. There is some merit to thisapproach when inflation runs at very high rates; however, crucial data havebeen lost iu the process as there is no readily available information oncurrent commitments at the project, sub-sector, or sector levels. It has

- 63 -
become urgent to f ill this gap and each organization Ohould, at the veryleast. regularly update its eatimtes of additional fincing required tocomplete every on-going project.
The Public Iavestmt Program
167. Table 20 presents the evolution and breakdown of publicinvestments in the health sector since 1980. In relative terms the sector'sshare in total public investments fell to 1.1%. from a maximum of 2% in1980. The decline in sectoral investments is largely due to the reductionin outlays from the consolidated budget which covers MORSA. all universityhospitals and the small capital expenses for health by other ministries; aparallel evolution can be noted in investments of state economicenterprises. which include the SI0. This decline was only partially offsetby increased capital expenditures by local administrations and, since 1984.by the financing of new equipment through publlc hospitals' revolving funds.The consolidated budget financed more than 95% of public investments in1980, but only 75.5% in 1985; during the same period, the share ofmunicipalities increased from 4.3% to 11.9%.
168. The Fifth Development Plan includes a list of 385 projects for thehealth sector27. As of the end of 1984. their total cost is indicated asTL133.2 billion and it is also mentioned that TL36.4 billion were spentthrough the end of 1984 for their implementation (see Table 21). The 1985allocation of TL36.2 billion of the Ministry of Finance (about US$72million) was distributed as follows: 1% for feasibility studies, 46% foron-going projects, and 53% for new projects. As mentioned above. the vaJueof these data is rather limited and the 1985 allocation will reach, at best,TL34.9 billion. Table 21 also presents the break-down of the programbetween MOHSA, university hospitals, the SIO, and the other institutionswhich constitute the health sector. Thes,e are reviewed in the followingparagraphs.
169. The 1985 investment prog-am of the Niaistry of Health and SocialAssistance, to which were allocated TL15.2 billion, is presented in Table22. For constructions, the priority given to completion of on-goingprojects is evident (TL7.1 billion, against TLO.9 billion for newprojects). The program also includes equipment. major upgrading and repairsof existing facilities, and replazement of about 10% of the ministry'svehicles. Another salient feature of MO}ISA's investment program is thelarge share of primary health care projects. which include 36 health centersand 109 health posts to be completed in 1985. and another 130 smallfacilities to be completed after 1985. This yearts allocation for primaryhealth care (TL4.1 billion) will absorb 52% of investments planned in civilworkC; this represents more than the 272 apparent ratio to total investmentsas PHC will receive part of funds earmarked for equipment, vehicles orrepairs. The investment program for curative services is centered on the
27 The 1986 update extended the list to 454 projects

- 64 -
completion of 8 hospitals (see Table 16); these add up to 1900 beds, i.e. a3% increase in MOHSA's present capacity.
170. The Higher Education Council (EEC) which oversees investments inUniversity 8ospitals also gives priority to completion of on-going projectsand has rejected all new project proposals since 1984. It has al6o scaleddown the size of many hospitals under construction and, with a view torationalizing future investments, has introduced new design standards forhospitals. The HEC does not keep updated records of base costs, or ofamounts needed to complete on-going projects; every year, it allocates toeach university its share of the funds obtained from the Ministry ofFinance, earmarking specific amounts for each project, including Uts. In1985, for instance, investment proposals from all universities amounted tosome TL70 billion; this was brought down to TL27 billion by the EEC, but theallocation from the Ministry of Finance was limited to TL25 billion, out ofwhich TL10.5 billion were earmarked for UHs. There are 109 health-relatedprojects for 20 universities but most resources are absorbed by the on-goingconstruction and equipment of 15 Uts, with a total of 10,850 beds. As somemedical schools now operate in MOHSA facilities which will be eventuallyreturned to the Ministry, the completion of this program Sill not result ina net addition of 10,850 beds to the present capacity of the medicalschools.
171. The Social Iasuramce Organisation received an allocation of TL3.7billion in 1985. It has revised its investment program which now consistsof two groups of projects. The first group represents 20 on-going projectswhich would require more than TL9.9 billion to be completed (in 1984prices); it includes 9 hospitals with a total of 3,700 beds, or anadditional capacity of 17%. The second group includes 15 new projects(mainly small health facilities) with an aggregate cost of TL5.5 billion(1984 prices).
An Immediate Action Program
172. In the 1970s and early 1980s, under strong pressure from theirconstituencies, MORSA, SIO, the Universities, as well as many otherorganizations started building large hospitals; some are alreadyoperational, but the on-going construction program includes 32 morehospitals, representing some 16,500 additional beds, with a very modestshare for MOHSA (see Table 16). Consequently, hospitals under constructionstill absorb the bulk of investments. On the other hand, low healthstandards, unequal coverage, and a very strong social demand for improvedpublic health services, fuels a continuing pressure for more hospitals.Moreover, because the number of admissions is relatively low and is certainto increase in coming years, it is argued in some circles that the nationalnetwork of hospitals must be rapidly expanded to accommodate future demand.Indeed, if all facilities under construction became fully operational by1990, the overall 14% increase in hospital capacity over five years wouldhardly affect the present bed to population ratio which would remain at 2.4per tbousand. As for the sector, it would be in a position to absorb

-65-
perhaps twice as much capital, assuming that financing is the only obstacleto a swift completion and that procurement and disbursement procedures areimproved. Nevertheless, there is significant underutilization of currentcapacity and opportunities exist to improve efficiency, which could freeresources from hospital construction for higher priority needs.
173. In spite of the considerable amounts involved, and the criticalcost implications of operating these new facilities, insufficient attentionis being paid to the justification of these projects, and the monitoring oftheir implementation. In the absence of an appropriate forum andcoordination mechanism, the SPO is not equipped to cope with the technicalnature of the issues involved, and the social and political pressuresgenerated by strongly vested interests. At present, no governmental agencyhas a clear view of the overall investment program, the adjustments whichcould be needed, and the longer term desirable orientations. The divisionof the decision making, financing and execution processes between a largenumber of independent institutions makes it all but impossible to safeguardthe higher interests of the sector. It would be the priority task of theproposed Higher Health Council to confront these issues and generate aconsensus on an optimal allocation of financial resources; this would likelyimply a redistribution between public organizations, between constructionand equipment, and between capital and recurrent expenditures.
174. An important reserve capacity already exists in most hospitals andthe following section will show that there is considerable room forimproving utilization of the existing infrastructure. In a shorter-termperspective and, pending the outcome of a more systematic approach tosectoral issues, the following measures would seem appropriate:
- enforce the moratorium on new hospital projects: this measure,introduced in 1984, is not followed with enough rigor; there areobviously cases when new projects may be justified, but theinterpretation of the concept of 'on-going project" seems tooliberal and extends to projects where sunk cost are marginal.
- conduct an objective evaluation of completion costs andadditional operating expenses and mampover requiremuts of everyon-going project;
- set-up a high level ad-hoc technical group, with the mandate toscrutinize the technical justification and architectural designsof all on-going hospital construction projects, taking intoaccount existing as well as planned facilities of allinstitutions, the geographical distribution of the population, andcurrent utilization patterns; this would include, whenappropriate, recommendations for scaling down or abandoningaltogether any project.
- unless specifically approved by the ad hoc group, delayimplenentation of all projects where sunk costs have not reached

- 66 -
an agreed level (25X would seem an acceptable ratio consideringthe slow pace of construction programs).
- identify priority -areas for transferring funds freed by theabove measures, such as accelerated completion of priorityhospitals, equipment, first level care in priority areas andtarget groups, operating expenditure, etc.
C. Focussing on Priority Areas in Primary Health Care
175. Incomplete integratiou of activities hampers the effectiveness ofoutreach services. While TB and malaria services were integrated in theGeneral Directorate for PRC (but not until 1980), the 600 MCH centers andstations are still under the authority of the General Directorate for MCH/FPand contin:-..; to operate under separate management, technical supervision andrecording systems. Some 9,000 health units are not providing enoughcoverage in MCH and FP, while most MCH facilities, isolated from the mainstream of health care, are underutilized.
176. High fertility rates in Eastern and Southern provinces, and inrural areas in general, have a direct bearing on the health status of thesepopulations; they are also incompatible with the country's developmentobjectives. Substantial gains can be expected in maternal, infant and childmortality rates from improved birth spacing and timing, and a reduction inthe total number of births. Therefore, in pursuing the objective of betterintegration of services, care should be exercised not to jeopardize theeffectiveness of on-going family plunuing activities; experience in manycountries has shown that, at least during the initial stages, integrationcan affect family planning services which require specific resources andmore specialized personnel. The considerable unmet need for family planningservices calls for an extension of population activities; it also calls foran improved mix in contraceptive methods.
177. Immunization should obviously rank high in MOHSA's priorities.The objective will be to capitalize on the success of the 1985 campaign toset up an effective system of continuing routine vaccinations; this wouldprevent the resurgence of the situation that had to be resolved through amassive, and costly, national immunization campaign.
178. As malontrition has been identified as a major contributing factorto child mortality, it too deserves special attention. Much of malnutritionappears to be the result of inappropriate practices that may be smenable tochange through education efforts. New social marketing techniques have beeneffectively used elsewhere to bring about change in behavior regardingdistribution of foods within the family, weaning foods, breastfeeding andfood hygiene. As public sector work in the field to date has not had thedesired impact, it may be worth exploring the possibility of involvingcommercial communications or marketing agencies in the nutrition education

- 67 -
efforts. Part of the nutrition problem is related to income levels,particularly in newly urbanized areas. Although the solution to thisproblem falls outside healtb services delivery, it is still a health issuefor wbich health authorities have an advocacy responsibility, and MOhSAshould encourage the formation of an intersectoral nutrition advisory bodywith the ministries responsible for agriculture and education.
179. While primary health care shares most of the problems of otherhealth services, these are compounded by acute shortages of qualifiedmanpower. For instance, about two thirds of health posts are not properlystaffed. Although 85% of health centers are headed by an MD, this is oftenan inexperienced, unmotivated, not properly supervised MD performing his orher compulsory medical service; many are actively involved in privatepractice after hours and therefore neglect outreach activities. Lack ofvehicles affects dramatically the efficiency of outreach ser-4ices: mostvillage midwives have to rely on occasional transportation (mopeds have beentried successfully in some regions); half of the health centers have novehicles; two thirds of vehicles in use are over 15 years of age. Medicalequipment, especially in health centers, is insufficient or obsolete.Public facilities provide only very basic or emergency drugs and deliverprescriptions for the rest; however, as there are no pharmacies in ruralareas, people tend to bypass the first or second levels. Because PHCservices do not charge fees, they cannot supplement their recurrent budgetallocations and frequent shortages of fuel, drugs or supplies paralyze theiractivities.
180. Implementation of the proposed program would obviously requireadditional funding to finance vehicles, equipment, drugs and other supplies,as well as the recruitment, training and higher mobility of healthpersonnel. The introduction of a cost recovery mechanism at this level isnot recommended, as it would raise very limited amounts, at an unacceptablesocial, political and administrative cost. In the present context ofstringent monetary policy, additional resources should preferably come froma shift of capital or recurrent funds within MORSA as well as other publichealth providers. The proposed Higher Health Council would have theauthority to present specific recommendations to the Government.
D. Increasing Hospital Utilization
181. A substantial rise in admissions (perhaps as much as 202) could beabsorbed by a reduction in the average length of stay and a parallelincrease in occupancy rates. This would necessitate a profound change inthe philosophy of hospital management, doctors' behavior, as well asstructural reforms; both raise real challenges in a sector characterized bylongstanding traditions and solidly vested economic, political, professionaland personal interests. This militates against the construction of newfacilities: for the immediate future, improviog the utilization of theezisting uetwork of public hospitals is bighly cost-effective and should be
68 -
the overriding priority for the sector. Most of the basic correctivemeasures to be taken have already been identified, and their introduction isoverdue. The following comments concern M.ORSA, because it operates 60% ofinpatieat facilities for which more detailed data are available; by andlarge they are also applicable to other services providers.
182. Admissions and occupancy rates are too lov, and average lengths ofstay are too high by international standards. Activating this unutilizedcapacity is an obvious, and highly cost-effective, objective which shouldreceive highest priority. MOHSA's thirty largest hospitals have a totaltheoretical capacity of 20,400 beds, only 80% of which (16,500) are active.Sote beds have been decommissioned for legitimate reasons (unsuitablepremises, use as nurse quarters, etc.), but in the majority of cases bedsare not activated because, over time, diagnostic and complementary servicescould not support the theoretical uumber of beds. Strengthening theseservices could increase by at least 10% the number of active beds, at arelatively low cost. Similarly, leaving aside small district hospitals forwhich bed occupancy is of secondary concern, large hospitals' bed occupancyrates, whicb are at best in the 60-70% range, could be brought at the 80-85%level with appropriate measures discussed below.
laproving the referral systen
183. Public hospitals managed by NORSA are the cornerstone and the mostvisible part of the health delivery system; they are the largest providersof health services all over the country and the facilities any citizen canturn to for regular or emergency care; they admit patients referred by otherproviders, including the S10 and university hospitals; ani -onsidering theirlimited financial resources and often obsolete equipment, they perform atacceptable quality standards, frequently higher than otber providers. Yet,they do not function as a network of facilities. Except for specializedinstitutions - chest, orthopedic, psychiatric and oncology hospitals - thatreceive selected patients, other facilities admit and treat any patient,from any origin. In theory, patients should seek primary care or first-contact care in health centers, dispensaries or, as it happens 50% of thetime, at a physician's private office; if the case requires furthertreatment or testing, it is referred to a District or State General Hospital(second level of care), and then only if necessary to a SpecializedHospital. In practice, patients seek care at the facility of their choice,regardless of geographic location or appropriateness; referrals are based ondoctors personal acquaintance or university affiliation. The result is anenormous flow of patients and relatives across the country. For example,38% of the patients of the Numune General Hospital in Ankara come from otherprovinces, including 10% from Istanbul; at the same time, 10% of thepatients in Istanbul's general hospitals come from Ankara. Patients fromthe East may travel to the West for simple treatments that could beperformed in the provinces. Patients affiliated to SIO, who normally shouldenter S10 facilities, frequently seek admission at MOUSA hospitals.

- 69 -
184. As normal geographic. technical or administrative rules areignored. workloads of the nervices cannot be forecast and activities cannotbe properly programmed. MOHSA has done little to remedy this situation: theclassifieetion of hospitale by levels of care is not implemented in practiceand abnormal referrals and bypasses are not detected and thereforesanctioned; hospitals are virtually independent on medical andadministrative matters; chiefs of medical departments have no formalrelationship with their counterparts at the same or higher echelons;similarly. they do not supervise practices in their discipline at lowerechelons. Administratively, hospitals are often too dependent on localauthorities to respond to other lines of command. Except for the chesthospitals which are linked to the central TB control unit. programmaticresponsibilities of hospitals - for instance in orthopedics. oncology.cardiology, etc. - are not clearly defined. The fact that hospitals haveneither outreach activities nor inputs into primary care keeps them furtheraway from the perception that they should operate in a system. Finally.within the hospital, the medical director is. as a rule, a clinician whoconcentrates on clinical activities and seldom sees the role of his hospitalin a wider perspective.
185. Referral procedures are not well codified and no guidelines seemto exist. The modest fee designed to deter non-referred patients is notenforced. Advance notice of referrals from one hospital to another, bycable or by phone, is exceptional. This occasionally places a strain onhospital operations and undermines primary care programs. Althoughimplementation of referral systems is a difficult undertaking in anycountry, initial steps enforced in Turkey would be sufficient to enhancedramatically the efficiency of the entire system.
mproving the admission policy
186. One major obstacle to improving hospital efficieicy is the currentadmission policy, resulting from the poor referral system as well asinadequate out-patient services. Major general hospitals aresdeliberatelyutilized. on a large scale, as outpatients clinics. This policy has theadvantage of facilitating access of the population to secondary and tertiarycare and bringing specialists in closer contact with primary care. However,it is a very inefficient instrument for outpatient consultation as well ashospitals admissions as it results in overcrowding at the tertiary level andin a considerable wastage of specialistst time and hospital resources.
187. An analysis of ten major hospitals28 showed. for example, that
28 The ten hospitals analyzed by the mission were: Numune and GeneralHospital (Ankara); Sisli Etfal, Haydarpa;a Numune, and Haseki (Istanbul);Ptaturk Derlet, and Cosuk (Izmir); Cukurova Numune. and Devlet (Adana); andNumune (Erzurum). They represented about 6,400 active beds. The overalladmissions to visits ratio was 5.0% ranging from 2.8% to 14.3%. The overall

- 70 -
Numune Hospital in Ankara receives an average of 2.400 outpatients perworking day. and more than 3,000 on Mondays; Haydarpaca hospital inIstanbul, with half the bed and staff capacity, receives about the samenumber of outpatients. Under such conditions of physical crowding andworkload pressure, quality of care is affected, regardless of thequalification of physicians and nursing staff. On the other hand, the ratioof admissions to outpatient visits is extremely low. varying from 2.81 to
14.21 and shows that outpatient departments act as general consultationfacilities. This misuse of specialist time and hospital resources (X-raysand laboratory notably) could only be justified if hospitals had idlecapacity; this is not the case. as evidenced by delays in pre-admissiontesting and subsequent inpatient testing. Under current conditions.outpatient departments are clearly diverted from their primary function. asdemonstrated by low bed occupancy rates. in spite of longer than optimallengths of stay. The "potential loss" in admissions - if bed occupancy wereto be raised to a conservative 85% - runs as high as 402 for the 10hospitals analyzed. -
188. One related aspect - the Pre-Admission Test (PAT) - is arelatively simple practice that saves bed capacity. At one major hospital.the average time for completing diagnostic testing of alreadv admittedpatient was estimated at 3 days (out of an average length of stay of 11days). Rapid PAT would require supplementing X-ray and lab equipment withrapid processing technology either in polyclinics (see below) or in thehospitals.
Improving Hospital Performance
189. Scheduling. Establishing weekly schedules of work for electivetreatments in the different services would ailow for better use of existingbed capacity. Weekly/monthly scheduling by clinical and surgicaldepartments would. in turn, lead to the scheduling of support activities.operating rooms, intensive care beds, special X-ray. physiotherapy,laboratory examinations. etc. Weekly/monthly scheduling generally meets theinterests of department chiefs, physicians and staff after an inductionperiod and appropriate training and guidance by medical directors.
190. The reallocation of excess capacity and removal of bottlenecks isanother cost-effective way of improving hospital performance. Ideally. allhospital services should optimize the use of their capacity so that the flowof patients, from admission to discharge, is not hampered by internal delaysand waiting lists. As a consequence of technological advances. the balancebetween services changes constantly but has not been reviewed lately in manypublic hospitals. Important bottlenecks exist in administrative sections.radiography, radiotherapy, laboratories, intensive care and coronary careunits, neonatal care, physical therapy; in all these services, new equipmentis needed. not only to improve quality of care. but also to increase the
occupancy rate was 60.5% (45-70% range).

- 71 -
increase the level of output. At the same time, some adjustments would bemade in areas with an excess capacity of beds, staff or equipment.
191. Quality control is minimal in MORSA hospitals. In other settings,instruments of quality control (peer review, medical audit, tissuecommittees, records audit, anatomopathology, etc.) bh.ve been developedprimarily to improve the quality of medical services. They have, moreover,contributed extensively to improving hospital organization, load and outputand have consistently worked to the physician's as well as the patient'sadvantage. In the case of Turkey, they would greatly improve utilization ofhospital capacity. In addition, joint medical/administrative staff meetingswould allow generalization of many innovative practices that individualphysicians have elready implemented in their immediate environment.
Increasing Bed Utilization
192. It should be stressed that improving bed "occupancy" is not a goalin itself: increased bed "utilization" is the real objective, if moreservices are to be provided with the existing infrastructure. It is notpossible to quantify, at this stage, the cumulative impact of improvedreferral, admissions and prograing, removal of bottlenecks, adoption ofmore flexible mechanisms, and introduction of quality controls and bettermanagement. A conservative estimate would bowever show at least a 20%increase in capacity within the existing premises.
193. Inefficient design and poor management practices are majorcontributing factors to low occupancy rates. Large rooms reduce flexibilityin assigning patients. Room assignments must consider male/female patients,infectious and non-infectious cases, and case severity. Repairs anddisinfection of large rooms put out of service a larger number of beds thanthe same activities performed in private or semi-private rooms. However,the most important weakness is poor management of patient turnover ("censusmanagement"). Bed management is under the control of clinical chiefs andnot of the hospital director. Thus clinical fiefdoms are created and excessdemand in one clinical subspecialty area cannot be compensated by empty bedsin another subspecialty. This practice creates about 20 small hospitalswithin a larger hospital and depresses the occupancy rates for lack offlexibility in room assignments. It should be a policy that hospital bedsare the property of the hospital and not of the chiefs of clinical services,and that all medical and surgical beds should be grouped under their generallabel without distinctions in subspecialties.
194. Average lengths of stay in MORSA as well as SIO hospitals (7.1 and7.7 days respectively) are too higb, because one out of eight admissions isin obstetrics which has an ALOS of less than three days. Universityhospitals have a ALOS of 10.2 days which in principle could be explained bya more complex case mix; detailed information on UHs is not available butfield visits and interviews tend to confirm that their case mix is similarto that of larger MOHSA hospitals. The major reason for long stays isinefficiency in management systems, i.e., admission and discharge planning,

- 72 -
logistics of clinical support systems, underutilization of facilities andequipment. Patients may be in the hospital for three to five days befor-treatment is begun, waiting for the results of laboratory tests orradiological examinations. Test results may be delayed for lack of suppliesor for shortage of technicians or for malfunctioning equipment. Operatingrooms are used primarily in the morning, and the use of specializedequipment is restricted by the availability of hours of technician time andof special supplies. For all three providers, ALOS could be reduced byabout two days with the introduction of more efficient procedures, and thiswould increase bed turnover rates.
Reorganizing Urban Care
195. A major issue confronting the government is the reorganization ofurban care for some 22 million persons, in order to achieve a viable mix ofall primary care providers, i.e. private doctors, MORSA, 8I0 and universityfacilities. In this context, MORSA started addressing the most pressingproblem, namely, the reduction of overcrowding of outpatient departments inlarge hospitals. To this effect, it is considering the creation of UrbanPolyclinics which would combine the resources, and missions, of Urban HealthCenters and Ambulatory Care Centers. As urban centers staffed with generalpractitioners, nurses and technicians, they would provide first contactcare, including integrated MCH/FP services, and cover at the same timepreventive activities, environmental health, school health and healtheducation. As ambulatory care centers, they would be organized as apolyclinic, with 12 to 15 specialties, serving between 300,000 and 400,000persons. The facility would provide secondary care to referred cases; itwould screen, check and orient patients referred for hospitalization andpossibly act as an admission office to hospitals. It would have enoughequipment to perform simple pre-admission tests.
196. Such polyclinics would.certainly relieve hospitals from thepressure of first contact visits, triage, pre-admission testing andtreatment. They would also free hospital X-ray and lab capacity for betterand faster in-patient care, and therefore contribute substantially to theimprovement of hospital productivity. However, their success would to agreat extent depend on good working relationships between specialists andhospital staff. Polyclinics could actually be staffed by hospitalspecialists taking turns, as is presently the case in outpatientdepartments, or by polyclinic specialists, associated or not with hospitals.
197. Urban polyclinics constitute an attractive alternative to hospitaloutpatient services which could improve health care delivery in urban areasand at the same time increase hospital productivity. However, the conceptis still at an early stage of development and some points would have to beclarified before a decision is made on their creation. First and foremost,it would be necessary to estimate the costs involved in urban landacquisition, construction, equipment, and operation. An analysis would alsobe required of the implications of the introduction of biomedical equipmentat this level of service,in terms of staffing, training, maintenance, etc.

- 73 -
198. Coordination with hospitals would be essential for polyclinics tofulfill their role; if not they would only constitute a new layer of urbanfacilities, and no progress would be achieved in regulating admissions andalleviating pressure on hospitals. At any rate, the smallest urban healthcenters presently in operation would still be needed and-their public healthfunctions would not be taken over by polyclinics; they would continue toprovide primary care to the poorest segments of the population. Indeed,their public health functions would have to be expanded rather thancurtailed; otherwise the present overcrowding of outpatient departmentswould simply be passed on to the polyclinics.
1. Adjusting User Charges
199. Patients are charged for services received in MOHSA facilities andUniversity hospitals. Medical schools are free to fix the level of theircharges, which must be approved by the Higher Education Council. Socialsecurity beneficiaries are not charged as health services are prepaidthrough their contributions and their employers'. An official fee scheduleexists for MOHSA and is updated periodically; In MOHSA facilities, theseuser charges supplement the funds received from the national budget.Revenues collected through user charges are pooled in a fund administered ineach hospital by independent bookkeeping staff who report only to theMinistry of Finance; 5X of funds received are transferred to the Treasury,another 10% is centralized for the benefit of other facilities which do notlevy fees. In university hospitals up to 50% of fees collected aredistributed among physicians as salary supplements; the balance is used forthe purchase of equipment, supplies and other small expenses. MOWSA may notuse this fund for salary supplements and the fund is only used for equipmentpurchases and operation or maintenance expenses approved by the Read of thehospital.
200. The share of revenues collected through direct billings in ahospital's total expenditures varies over time (see below) and betweenhospitals. MOHSA' teaching hospitals cover from 15 to 20% of theirexpenditures with user fees; specialized acute care hospitals about 30 to35%; and general hospitals less than 10%. One university hospital collectsas much as 50% of its budget from patients, either directly from individualsor th ough third party payors; others collect a lesser percentage, thoughusually more than large 14OFSA facilities.
201. Although some patients are exempt because recognized as indigents,most of them pay for services received in outpatient facilities as well ashospitals. In order to be considered medically indigent, the patient mustbring a certificate from the municipal administration certifying that he ispoor; the Read of the hospital (the medical director) then decides on thepaying status of the patient. No firm data are available about the numberof indigents served by the hospitals and health centers. One prestigiousUniversity hospital in Ankara is said to serve a maximum of 2% indigents.

- 74 -
The number of indigents receiving free care in MORSA facilities is probablyless than 10%.
202. There is some controversy in the country about the impact of feeson the accessibility of care to lover income groups, and the low rate ofhospital admissions is at least partly ascribed to user charges and theadministrative difficulties and dehumanizing practice of being declaredindigent. It is sometimes stated that fees often lead to postponement ofcare, which results at a later date in more expensive and more high risktreatment. Finally, those who advocate lower fees, or their eliminationaltogether, point to the income redistribution achieved through thismechanism. Yet, the practice has always been there and is accepted by thevast majority of the population. This is a considerable advantage comparedwith so many other countries where the absence of a cost recovery mechanism,and the procrastination at introducing user charges, makes it all butimpossible to redress the sector's finances and set the stage for viablelong term solutions. Nevertheless, what is urgently needed, is anevaluation of real outpatient and inpatient costs, by type of facility andnature of service. The introduction of cost accounting in publicfacilities, starting with the large hospitals, should receive high priority.
203. In the short run, two issues call for immediate decisions: first,the periodicity of the tariff updating and second, the restructuring of thetariff itself, to bring it more in line with the real cost of services. Ina longer term perspective, the Higher Health Council would be exiected toinitiate consultations on whether it is desirable - and feasible - to scalecharges according to recipients' ability to pay.
Adjusting the Fee Xevel
204. University hospitals apply higher fees than MHOSA, and also adjustthem frequently; no information on total receipts or their evolution overtime is directly accessible but neither does it seem to be an issue callingfor special attention. This is not the case for MORSA which is underconstant social and political pressure not to increase its fees; at currentlevels, the revenue generating potential of these fees is negligible. Asmentioned earlier and illustrated in Chart 1, delayed adjustments result inwide fluctuations in hospital cash flow, impossible to forecast. Theevolution of the past five years, presented below, shows the dramatic impactof the 1981 adjustment (+125X) and the erosion that followed (-101); it isstill too early to assess the outcome of the January 1985 adjustment, butthe depreciation of the local currency has been at least 40% during theyear.

- 75 -
Y38B COLLCT=D IN TMe W 2064ES BPITAZB(TL million)
Current 198Prices Prices lndes
1980 917 43 1001981 2 927 96 2251982 3 514 90 2121983 4 794 97 2271984 6 257 86 203
205. Without regard to the general issue of public financing of healthservices, frequent and regular adjustments of MORSA's fee schedule areinescapable. This does not imply the setting up of an indexing mechanismwhich would trigger automatic adjustments linked to inflation. What isneeded is the official recognition that, as long as inflation will remain athigh levels, the Government will be expected to adjust fees in order tosafeguard the quality of services and the longer term viability of thesystem.
Adjusting the Fees Structure
206. The whole structure of the fee schedule applied in MOESA hospitalsneeds to be reexamined. Irregular updating (five years between the last twoadjustments in a context of very high inflation rates) makes it all the moredifficult to confront unpopular decisions, and has led to the aberrationsdiscussed above. It will be recalled (see Table 23) that the January 1985adjustment resulted in a reduction in real terms of 42% (compared to April1981) of the daily rate for a "deluxe room" in public hospitals; at thatdate's exchange rate, this corresponded to US$9.23. At the same time, thecharge for a small dressing in outpatient facilities was increased by 193X,to US$1.85. Under present circumstances which entail increased hardship forlarge segments of the population, it would not be advisable to increasedramatically the tariff to reflect the real cost of all services; however,on social as well as economic grounds it would be fully justified to proceedto a gradual restructuring of this tariff. Revising pricing policy toreduce existing distortions, would at the same time improve equity. Asregards social security beneficiaries receiving services in MORSAfacilities, fees should be adjusted at least to the level of operating costsin SIO hospitals, in order to eliminate the indirect, and substantial,subsidy to SIO.
- 76 -
F. Strenagtheixg Social Security-s Fianciel Basis
207. The SIO, as vell as BAG-KUR and the GERF operate undercapitalization financing systems. Their resources are generated byindividual contributions and payroll deductions which have consistentlyincreased in recent years, to reacb the rate of 34.5Z for the SIO, 201 forBAG-KUR and 28S for GERP. Hovever, because of escalating costs and an 801level of collection of premiums, the system is confronted with a grovingdeficit estimated at TL400 billion in 1983 (US$1.8 billion), while legalreserves are not maintained at the required actuarial level.
208. The Plan states that welfare and social security services must beexpanded to larger segments of the population. At the same time theseinstitutions are expected to meet their commitments from their ownresources, while government subsidies would be terminated. To achieve theseseemingly contradictory objectives, it is proposed to strengthen thesystem's management, improve premium collection, eliminate expenditureswhich correspond to public transfers, and change the provisions governingearly retirement. However, the Plan only suggests that eligibility forretirement, for all agencies, be postponed to 55 years for men and 50 yearsfor women. It would certainly be preferable to extend to both sexes thesame limit of 60 years or, at least, generalize the 60-55 age limitsexisting in BAG-KUR.
209. The most important proposal put forward in the Plan is that allhealth care institutions of the Social Insurance Organization be turned overto KOUSA: 8IO would then purchase health services for its beneficiaries, inreturn for their financial contribution to the system. The outcome of thisproposal is not yet clear as it is likely to generate the resistance ofstrongly vested interests. At any rate, it emphasizes the need tostrengthen the financial foundations of the system.
Assets of Social Security Institutioua
210. The assets of the three major social security institutionsexceeded US$1.4 billion in 1984. A major proportion is kept in localbanks. Another substantial proportion of their assets is composed of housemortgages and personal loans to individual members: more than 202 for GERFand about the same ratio for 810 (in the "bonds and securities" category).As for outstanding contributions, they represent 16.5X of SIO's assets, andmore than 24S of BAG-KUR's.

- 77 -
ASS1WTS OF IWOR SOCIAL 5RCURI INSTITUTIONSA UDI DISTRIBUTION IN 1984 CZ)
GUI BiD BAG-KUR EIID8 TOTAL
- Bank deposits 59.4 30.0 66.7 - 40.0- Bonds & securities 15.6 26.0 2.4 32.2 21.1- Land & buildings 1.2 23.0 - 67.8 16.9- Outstanding contrib. - 16.5 24.1 - 12.8- Loans to members 20.7 - - - 5.0- Others 3.1 4.5 6.8 - 4.2
Total 100.0 100.0 100.0 100.0 100.0
TL Billion 131.2 334.0 60.1 20.0 545.3
US $ Million 357.8 910.7 163.9 54.4 1,486.8
Utilization of Assets
211. The resources of social insurance institutions. and theirutilization. are determined by law and controlled by the Ministry of Financeand Customs; only the private funds can freely manage their resources. Overthe years. and as in many other countries. the three major institutions havenot only been geared to the benefits of their members; they have alsolargely been used to the advantage of the State. Legal constraints, liberallending policies, generous benefits. conservative management and rapidinflation have limited the profitability of the system and endangered itslong term viability. In the early 1960s. with the introduction ofdevelopment planning, the operating surplus of social security institutionswas mobilized to finance public investments. In 1965 for example. it isestimated29 that investible funds of the SIO represented 27£ of totaldomestic savings and nearly 4% of GNP. These were largely used to financethe creation and expansion of state economic enterprises, through the newState Investment Bank.
212. The mechanism was rapidly diverted from its original objective, associal security funds were also used to finance current expenditures andcover operating deficits. Another illustration is provided by the mortgageloans made by the three social security institutions to their members.These have been instrumental in responding to a pressing social need bysupporting government's housing programs; however, the highly attractiveinterest rates did not benefit lowest income groups alone. By the end of
29 See S. Maruflu. "The Aim of the Social Welfare State and the SocialSecurity System" (in Turkish), Ankara. 197$.

- 78 -
1984, the SIO alone had made more than 229.000 such loans. As for BAG-KUR,by the end of 1983. it had made more than 8.900 mortgage loans against 3.700loans to small enterprises.
The Issue
213. From an economic as well as actuarial perspective. social andpolitical gains financed through social security funds have been achieved ata very high cost. Investment policies of the social security institutions,admittedly largely forced on them by government regulations, have resultedin impressive negative rates of return presented below. In a recent study.SP030 estimated that the accumulated actuarial deficits of SIO and BAG-KURby 1981 amounted to TL260 billion and TL63 billion respectively, in 1981prices (US$2.338 million, and US$567 million).
REAL RES OF REURN TO IWEWMWOF SOCIAL SBCRMM Z a)
GERF SIO BAG-KUR
1977 -17.8 -17.2 -15.81978 -45.0 -44.6 -43.01979 -72.5 -72.8 -71.71980 -79.2 -78.3 -74.51981 -34.4 -33.6 -18.6
214. Inflation as well as the freeze imposed by the government oninterest rates of bonds and securities were major causes for these negativerates of return. Another contributing factor was government imposedceilings on interest rates for all types of bank accounts. Moreover,investments in real estate under the rent-control system proved disastrousas rents could not keep pace with inflation, and hardly covered maintenancecosts of the buildings. Finally, personal and mortgage loans were anotheraberration which lasted almost two decades, although their financial impactwas contained by the limited size of the programs. Interests charged onthese loans, which had been set at three to four per cent in the 1960s. wereonly adjusted in the early 1980s. after inflation rates had reached thelevel of 80% p.a.
215. Actuarial deficits were also accelerated by reforms in socialsecurity legislation govetning old age pensions. Eligibility criteria weteeased so rapidly that, between 1965 and 1985. the number of persons drawing
30 State Planning Organization: "Fifth Five-Year Development PlanSpecial Expertise Committee. Report of the Sub-Committee on the Financingof the Social Security" (in Turkish). Ankara. February 1983.

- 79 -
invalidity pensions from GERF was multiplied by 4.7; during the same period.the number of old-age pensioners was multiplied by 35. The Social SecurityCouncil has calculated that. from 1970 to 1981. the average pensionable agedeclined from 57 to 51 years. As a result, the average duration of old-agepensions is now the highest in Europe3l: 19.4 years, against 8.8 in Ireland,9.0 in Switzerland. 13.9 in the Netherlands, 13.1 in France, and 13.0 inF.R. Germany.
216. The reform under consideration at BAG-KUR, to extend healthbenefits to all its members. would further strain the financial resources ofthis institution and, consequently, of the whole social security system.This is because an extremely low level of individual contributions iscontemplated by the proponents of the reform. In the proposal put forward tothe Parliament, Bag-Kur members would be required to increase by only 12%their present contributions in order to benefit from full health coveragefor themselves, their dependents and their survivors; benefits. andbeneficiaries, would actually be the same as for SI0. A separate healthfund would be created and, to build-up its reserves, no benefits would bedrawn during the first year of operation. For members at the lower incomelevel, the monthly contribution would be TL144 (US$0.27); for members at thetop of the scale, it would be TL1159 (US$2.14). These rates are clearlyinconsistent with the risk to be covered and, on the proposed basis,BAG-KUR's health fund is certain to run into substantial deficits. Undercurrent financial policies, this deficit could not be covered by thebudget. Having it supported by the SIO, for social and solidarity reasons,would obviously generate a strong resistance in this institution and rapidlyjeopardize its financial stability.
217. The foregoing discussion on social security's financial status hasemphasized the complexity and sensitivity of management and financing issuesin a system whose roots can be traced to the XIIth century. Today, thesocial security system is undoubtedly in a critical situation calling for areexamination of its foundations. raison dletre and benefits, at a timewhen, in spite (or because ?) of economic stringency. the Government isfaced with increasing pressure to expand the safety net to larger segmentsof the underprivileged population. Because too many interests are at stake,not necessarily selfish or prejudiced, this should be the object of a widelyopen debate aiming at a national consensus on the future of the socialsecurity system, the nature and extent of its coverage. and the monetaryimplications of possible alternatives. The proposed Higher Health Councilwould provide an adequate forum for the discussion of health related issuesand the implications of alternative proposals. The national debate wouldstand much to gain from a critical analysis of other mature social securitysystems in countries as the United Kingdom, Argentina, France, Canada, etc.Specialists from these countries should be called in to present the pros andcons of alternative systems and assist national experts in identifying the
31 Council of Europe. "Draft of the Final Activity Report. Committeeof Experts on Reducing Inequalities in Social Security Protection".SS-IP(82)

- 80 -
solution called for by specific local conditions. The International LaborOrganization, already associated in the implementation of various projectsin the country, could also provide valuable support to this undertaking.
G. Outlining a Program of Applied Research
218. In the process of analyzing the functioning of the health sectorand the major issues affecting its operations and development prospects.many gaps in basic information were identified. With a view to outlining asectoral program of applied research. these are presented below under fourthemes. namely: ti) primary health care; (ii) productivity of healthservices; (iii) health costs; and (iv) sector financing. The proposed HigherHealth Council would bear final responsibility for deciding which areasmerit further investigation. the organization of an applied research programand its timetable. commissioning the necessary studies. evaluating theirresults. and drawing the relevant conclusions and recommendations to bepresented to the Government.
Primary Health Care
219. There is a general agreement on the major weaknesses of theprimary health care system, and regional disparities in infant mortality.nutritional status and fertility are recognized. On the other hand, thefundamental principles laid down in the 1961 law that created the IntegratedHealth Services Scheme remain valid. as are the basic objectives set at thetime. What is still lacking is an outreach action program. with specificobjectives and timetables, and a detailed evaluation of resources needed.To design a realistic program and ensure effective collaboration of allparties concerned, provincial authorities would have to be closelyassociated at all stages. The initial step would however consist inassembling, and in many instances generating. the appropriate statisticalbasis which is presently missing32. This would include more operationaldata on fertility and nutrition in rural and eastern, which should be usedto develop specific, measurable program objectives, service deliverytargets, and a series of monitoring and evaluation tools.
Productivity of Health Services
220. Substantial productivity gains can be expected from a morerational use of existing public health facilities. The major flaws in thesystem were pointed out, and reference was made to corrective measures
32 The 1982 nutrition survey is based on a national sample of 1.480households. while the results of the 1983 fertility survey are notsignificant at the provincial level.

- 81 -
applied in otber countries. However, national specialists must take thelead in identifying their specific problems, and proposing effective andacceptable solutions.. This exercise is of paramount importance as it wouldset the stage for ar. objective discussion on the extension of the bospitalinfrastructure. Isolated and often competing initiatives must be replacedby a coordinated approach to sectoral investments. Moreover, trade-offsmust be recognized betw!en the construction of large facilities, and therevitalization, upgrading and equipment of district hospitals and healthcenters; improved rationalization of the former would be instrumental inreleasing the resources needed for outreach services.
Health Costs
221. The costs of public or private health services are not well known,and the analysis of this critical issue is hampered by the absence of asolid statistical base. Not much seems to be done beyond mere monitoring ofcapital and recurrent expenditures. Components of costs are practicallyignored. Improved management will be contingent upon a better appreciationof real costs of outpatient consultations, hospitalization, differentservices, drugs and supplies consumption, etc. In particular, these areessential to the adjustment of fees at a more realistic level.
sector Finci
222. Bacettepe University has initiated some work on overall healthexpenditures, but this does not seem to be the case in other institutions.Turkish universities have the resources needed to undertake basic studies inthis area. Yet, no attention seems to have been given to such topics as:expenditures differentials by income levels and residence; income elasticityof private health expenditures; price elasticity of demand for healthservices, with special reference to fees collected in public institutionsand their impact on utilization of services; etc.
223. The existing cost recovery mechanism deserves particularattention. Compared to most middle income countries, Turkey is in theenviable position of having collected fees for decades in its public healtbfacilities; the rate of recovery in recent years has been eroded severelybecause of high inflation rates, but its legitimacy is not questioned.Because it needs overhauling, now may be the appropriate time for an in-depth reform. The main justification of fees presently levied in publichospitals is to raise additional revenue for MORSA and to cover at leastpart of the cost of the service; but, as was shown, the gross yield is low(and declines very rapidly between adjustments), and the net yield isprobably much lower because of collection and administration costs.
224. However, fees can also be seen as a means of improving resourceallocation and access to basic care. Conceivably, a more realistic tarifffor inpatient care - with normal safeguards in favor of the poor - couldmake it possible to shift enough resources to provide for (virtually ) free
- 82 -
outpatient care. At any rate, many basic health programs must be providedfree because they benefit the whole community (vector control,immunization), or benefit the group rather than the patient (preventivecare, curative care for communicable diseases), or must be provided,irrespective of the ability or the willingness of the beneficiary to pay(emergencies, accidents). As regards other outpatient services in outreachfacilities, dispensaries or health centers, fees could be waived, not onlybecause of the frequent inability to pay and administrative costs involved,but also as a means of reducing pressure on higher levels of care, inparticular the outpatient clinics in the major hospitals.
225. Another issue alluded to in previous pages is the financing offuture sector development. Many options are being considered, notnecessarily compatible, at a time of rapidly changing economic environment.The Vth Plan advocated a transfer of SIO hospitals to MO0SA; the Ministryof Labor and Social Security is studying ways of strengthening the financialfoundation of the social security system; at the same time, however, it hasaccepted the principle of extending comparable health benefits to BAG-KURmembers, for what appears to be a token contribution; the Ministry ofFinance would favor a universal health insurance scheme; for their part,universities pursue imperturbaoly their own way. This situation obviouslycalls for an in-depth analysis of possible alternatives, conducted bynational experts, but drawing on international experience. Particularattention would need to be paid to the compatibility of a universal healthinsurance scheme with the existing social security system and its expansion;and to the risk of cost increases generated by any extended system of tbirdparty payment.

--- -----------------
0% P.,~QU~ 0
0%~~~%C
".4~~~~~~~~~~~~C
sr i con'
| ----- -------------------
g p] ~- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -* --co~
- - - - -~~-'-- - - - - - - - - - - - - - - -
g ~~~~~~ _ _________________
I|' A fl A ;Dt XiX lt 1k fl

TURKEY REALTH SECTOR REVIEW
Table 2: Demographic Characteristics(In thousands)
1972 1973 1974 17 1976 197 197$ 1979 100 1981 19M2 1983 194 Ii
?epatIo (md-year*scaage.) tl 37132 3872 39036 40078 40915 41768 42640 43330 44438 45446 46459 47471 46460
Iotat-urban distribution
ft ol 24393 24612 24813 23049 25236 2S410 25374 2572* 25563 2S599 A*063 260*2 24012Urban / 2739 13460 14223 15029 13679 16*38 17066 17604 1S373 19496 20396 21409 22398
a teture distributiam
Age& 0-14 years 15262 15316 13774 IUS3 16273 1649U 16715 16936 17162 17436 17634 17811 17974Age* 15-A4 yeas 20216 20852 21309 22211 22781 23369 23966 24546 25214 25935 27164 27611 2641Ages65 NW over 1652 1702 1733 1612 1861 1909 1957 2006 2062 2075 2061 2049 2045
196045 1965-70 1970-7S 1975-0 19s0-65
Crtde bithb rtte /2 41.5 40.1 35.0 32.2 30.6Crde death t te 1 13.3 13.3 10.6 10.0 9.0Rafaet rtality ate 13 180.0 133.0 120.0 110.0 43.2 1Life epctancy at bittb co
male 30.3 52.8 S6.3 36.3 60.0 Sla_ele 53.2 56.1 S9.4 62.8 5.51
Car rproduccion rate 2.9 2.7 2.S 2.2 1.9
/I Deried trm census data ot 1960. 1970. 1973 ad 1980 (As of July 1)./! Par tbousand of Population.3 1* -mr of intants bo die beore 1 yes o f age, per thousnd live birtbh in a given year.
Places over 20.000 ""Is are acceptd as urban
S0U1E6 State I.Wtitute of Statistics; 810.
(06621.p. 1)

- 85 -
TURKEY HEALTH SECTOR REVIEW
Table 3: Evolution of Food Consumption(1974 - 1982)
t IRACETTEPE SURVEY I TDRF SURVEYI t 1974 1 1982
I…I~~~~~~~~~~~~~~~~~~I I I IISample I I t
llouseholds covered 1 6,480 1 1,480IPersons covered 1 31,563 1 7,844 1lAverage family size 1 4.9 1 5.3- 1
I i I IlResults I I J
ITotal calories (p.c.tday 1 2,291 I 2,395 JITotal proteins (gr/p.c./day) I 85.0 1 75.3lAnimal protein (gr/p.c./day) I 22.5 | 17.3 I
IDaily consumption (grip.) I I II - Bread and cereals 1 493.0 1 544.8I - Dairy products 1 102.4 1 107.8I - Sugar and condiments 1 36.2 1 37.1 |I - Butter, fats and oil 1 37.9 1 32.8 1I - Eggs, meat and fish 64.4 J 52.9 I
- Potatoes and pulses I 41.9 J 71.4 1- Vegetables and fruit 1 510.5 J 272.5 1
Source: Food Consumption and Nutrition in Turkey, H. Gencaga,Turkish Development Research Foundation, Ankara, 1985.

- 86 -
TURKEY HEALTH SECTOR REVIEW
Table 4: Consumption Levels by Regions, and Urbanand Rural Areas (kg/personlyear) in 1982
-------------------------------------------------------------------
I I Regions I
I Coastal Regioun Cent. Anatolial East
I Rural Urban I Rural Urban tRural Urban I
f1. Wheat and wheat I I tI derivatives 1 208.3 174.4 I 254.0 193.8 1264.2 203.6 1
1 1 I I I1 2. Rice 1 5.2 10.9 1 5.2 9.5 1 6.1 9.7
1 3. Pulses I 11.5 14.3 1 11.4 10.2 1 4.3 11.2
1 4. Potatoes 1 15.5 17.8 1 20.4 22.1 1 37.9 22.2 1
1 5. Red Meat 1 8.3 25.5 1 3.1 18.0 1 3.7 20.4 1
1 6. Milk and other I I I II dairy products 1 88.3 90.6 1 133.7 98.7 1153.4 84.0 1
I 7. Eggs 1 2.2 4.6 1 2.9 5.3 | 0.9 2.3 1
1 8. Margarine and 1 18.4 23.3 I 9.6 16.5 1 3.3 9.4 1I liquid oils I 1 I II I I f I. 9. Sugar 1 13.0 12.6 1 9.7 10.8 | 20.1 14.8 |
i I I I I
Source: Food Consumption and Nutrition in Turkey, H. Gencaga,Turkish Developmeut Research Foundation, Ankara, 1985.

- 87 -
TLE 8EM1 SHWR REVM
Table 5: Total aber of ew EP Acceptors, byMethod and Year, in 1MSA Facilities
(1980-1984)
I N~WFPACEPI0S I
t IwDs (Pill I Cxa Total II () t(Z) 1 (Z) I (100)!
1980 I 34.8 I 37.9 I 27.3 I 235,90011981 I 30.9 140.1 1 28.9 1 307,800!1 198 1 27.0 1 37.6 I 35.3 1 402,70011983 1 27.4 1 34.7 I 37.8 1 588,600X1984 I 25.3 1 29.7 1 45.0 1 631,9001
Soce: MM
TWY HEAVI SEWR REVIEW
Table 6: Nse PP Acceptors by Methods and Reiomsin 1M Facilities (1984)
I I IE 1 NE FP AOCIORS I I~~I1I IP-- - - - PP I
- RIO15 I 15-49 1 IUD Pill I C0DdQM I Total I Acceptorsl
i I t I I I IINorth West I 1,804,500 1 33,105 1 34,285 1 66,673 1 134,063 I 7.4 1lSouth Wst I 1,067,900 1 22,784 1 46,175 1 70,600 1 139,559 1 13.1 1INorth I 1,393,300 1 17,266 1 27,522 1 39,256 I 84,044 4 6.0 1ICestrai 1 1,552,500 I 45,432 1 32,911 1 49,688 1 128,031 I 8.3 1ISouth 1 1,022,500 1 25,108 1 21,880 1 31,836 1 78,824 1 7.7 1lEast 1 943,600 1 9,792 1 11,151 1 12,914 1 33,857 1 3.6 13outh East 1 718,100 1 6,573 13,667 1 13,246 I 33,486 1 4.7
IOIAL I 8,502,400 1 16C,060 1 187,5911 284,21 1 631,864 1 7.4 I
Souce: Mi, and miSsicn estimtes

- 88 -
TLK IHALI~ SEDR KsV
Table 7: Distributio of Married Vme PtacticizgContraception by lasue Status (1984)
I I I Ptestly UsiEig Preva1ace IStatus I Total I Cotrceptio I Rate t
I
[Ever rried I 8,702,800 1 2,837,700 1 32.6 1
Ourently Nirried 1 8,330,900 1 2,837,700 1 34.1 1I I I I IIbpsed (1) 1 6,295,700 1 2,837,700 1 45.1 1
(1) Defined as livig wiith busband, not in post-partunaIworee, not pregmt, and not sterile.
Source: Dr. Tors - "Imerical Evaluation of D hic Needsin 1inke9. INe. Submitted to JIII ti lCouzil Neeting, April 1984.
Table 8: Distribution of Feale Coatraceptive Users,by Setbod (1984)
I i EIber of I Distribution 1
I I Users I (%) I . I I
IPill I 772,900 1 27.2 IIID I 395,700 D 14.0 1Cmm I 168,400 I 5.9W Witbirsl 992,200 D 35.0
tOter 1 508,500 t 17.9
I Total 1 2,837,700 1 100.0
Sonree: Dr. Tows - Sberical Evalustico of Dli erapbreeds in Zae. Memo. Subnitted to JI I 'aIntematimal Comuil Ieetisg, April 19Sf.

- - H6~~ ~ ~ ~ -l i--l t--
I E § i si fW
E-- - - - - - - - - -
i¢sSZU " E iE%ElMM E ffi~~~~~~~~~~~~~~~~~~~~~NJ: I F j]~~~~~~~~~~~~g S @,, £ W Q jt. I

- - - - - - --- - - - - - - --0% 1' @0. .' | I* %J1. ' - . 0
" 1 | f i - § X i [ | : I { f~i g---------------------- *--- --- i
-------------- ---------- ---
____ ___ ___ ___ ____ ___ _ _ _ ~ ff-
_ * W C M- _- WE M om g agEt w lSWMEs§t§§ ',Sga.%0~~~~~~
___________________________ ___ X~~~
0% CD § UIt. '@ ?.)#-§i P9
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ . _ _ _~~~~~~~~~~~~~~~~~'-

- 91 -
TUWEY UM11 SW= mEKI Page 1 of 2
Table 12: Evolutiom and Begional Distributim of Physicians(Public and Private Sectors)
I I 1979 190I 1981 1982 I 1983 11984 1
I 1 . .
ITst RE= (Ediux, Istbul, i I I I IIKirklreli, T ag) I I I I II -Physician 7973 I 8215 1 8669 1 8772 10579 110848I - Pbplatia per Physician 7151 7001 6791 695i 597 602!
lIIInd 1 N(Bolu, Kocaeli, I 1 I I I IISakarys, Zd*ulda) I I J ' I I II -Physicians 1 6431 6811 790 9051 906K 812!I - Poplatiom per Physican I 3947 3777 3318 1 2979 1 3058 1 3513 1II ( B e S I I I I I I IIIIIrd (Btlikesir, I I I I I IBICanakkale)I - Physicians 1 628 1666 1 684 1 775 1274 13911I - Popilation per Physicin 3780 13593 13557 1 3218 1 2005 1 18B4 II I . 1 I 1 I I IVth nMI(Aydin, Denizli, I I I I I IIir, Manisa, Nugla) I I I I I I II - Physicians 3071 3375 3360 3540 14217 4649 1I - Population per Physician 1 1478 1 1367 1 1394 1 1354 1 1162 1 1079!
lVth RM N (Afym, Bilecik, I I I I I IlEskiehir, Kutay, Usak) I I I 1 If -Physicians 1 589 1 634 f 666 1 864 1 845 1 8921
- Population per Physician I 3433 1 327 1 3078 1 2402 1 2483 1 2384 1I ~ ~I I I I i I I
IVIth UEIO (Antalya, 1 1 I t I IBluur, spert) 1 1 1 I I I I1 - aPhysicians 1 453 1537 1 495 1 612 1 62D1 683 1I - Populatimn per Physician 2938 1 2484 1 2729 1 2250 1 2260 1 2093 I
IVIIthRHIOC (Ankara, Cakri, I I I I I IIKastaumwuKirsehir, I I I I I IlINvehir Yogat) I I I I 1 1 1I -Physiciams 157451 5816 61771 6483 6526 6951 1I - Population per Physiciann 837 7851 746 1 720 1 725 1 691 1
IVIIIth RI (Rya, Nigde)- Physicians 258 I 281 1 303 1 440 1 615 I 6921
I - Popuiation per Physician 7934 1 7381 1 6934 4 468 I 3548 I 3215 1
l$bI I I I I I I IiOn%, BIEU, SiIp) I I 1 1 It - EPhysicia 522 553 642 872 19051 1248I -1Populatica per Phyiacian t 5510 5264 1 4581 1 3422 1 3343 1 2464 1
TIE 12A

| | X---------------------------------------r- --
# s fi fi K § . E E g. E g E 4 E 24 w K - i
w . >* *. $ "
t~~~~I i. I~ M E§ f ! E11t
- - - - - - - - - - --- - - - - - - - - - -
4.---- - ---- -------- -
1[ -R a E i S E W vW
-4 LII~~~~~~~~~~-4T
- ----------- -- --- -- --- -- --- a- S--g.I
iM~~~~~~~ § !l EW f X I
- - - - - - - - - - -- - - - - - - - - - - - - - - - - - --- - 9~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
SE S! iS MS §E lg !§ gW { x~~~-------- -- ----- - -- ------------ --s-s. Wa'
Et i @l ! §E Ms g w- - -- - - - ~- 'O%- - - - - - - - - - - - - -

- 93 -
TUM mant. Sam RlAEM
Table 13: Helth e(Public amd Private Sectors)
11979 1 1980 11981 11982 11983* 1
I I I I I I IIII P lBr l I I I 1 I Il-ospitals (nm- 532 536 1 544 1 530 I- 553 1
military) II I I1-BealthCeAters 1290 1 291 287 I 100 1 93 1I I I I t I II L I8221 827 8311 630 646 1
I w r w l E SIII U I I 1 I I I1-vt Physicias Office 1249 1 242 1 314 1 295 1 295 1
F-HealthPobas 16565 1 6594 1 6624 1 7044 1 7055 1
I-ma1tkhuits 11764 1 1827 I 1838 1 1955 1 1975 1
I-Dispeosariis 1 346 1 346 1 346 I 410 I 438 1i ~~~~I I I I I I
M-lM Cente sand 1194 1 190 I 190 I 190 184 1I DissLaiesl I I I I If
-EN statiws 1461 I 445 1 445 I 445 1 408I i I I I I II L 19579 1 9644 I 9757 110339 110355 1
I - IIII16174 1 6335 1 6914 I 7802 I 8599
I~~~ ~~ __ II
'Provisicnal figures
SOX=E: State Institute of Statistics

- - -- -- -- -- -- -- -- -- -- -- -- -- - -- -
If I; S Xtf ITXf.i
t g ~~~~~~- - - - - - - - - - - - - - - -
I : ffi ,; "[jF0i *1 F II*s g. * I- * !
I -- ---- ----------- -* F. H t 4
- - - - -- --I-I- - -- - - - - - - - - -
§ -.4§§

- ----- -- -- -- -- -- -- -- -- -- - -- -
r~- --------------------- -
-- -- --- - - - - - - - -
! X X X S~~~~I W '. e
"~~ N - . -X U
- B 1 -2 f l
&~~# - P P - -------- - Vi
* " ~~~~- v, i*0 I 4 X v

*----------- --------- -- Z----------------------
* II __ ___________. _______ I_ii). V S~~~~~~~
' .,ti4 ~ - --- - - -- - - - - - - -
---- --- - -- -rl - i-Fi-I--I-[i-1[-------- --- ---,--------- I------~----~-U
------- -----------------. ________ - I_
i IW I°ogoo gE gSsoog |W8f8°oolwB°°-|§1. M__ _______ _________________It gSSXE

I t * W------------ --
I I~~~ Z---- --- ------ --
-% 0~~I-
- - -- - - - - - - - - - - --3 J IJ - -1-
10.1~ ~ ~ ~~
- - -- - - - - - - - - .- ~ - -
o - -- - ---- -
- -- - -- - --
- - - - - - - - - -
- I. @
| 8 S* D u a E it |
fi ______________ __
I_ ________________________ _ .I
___ _______ __^___ -__.
£ a0 0
_ _ _ _ _ _ _ _ _ _ __

-- -- ------------------ -------
1EI. | [ q | [ {> i gg F
|, 8 - |t >_ $ _ 1
- - - - -- - - - - - - - - - - - - - - - - - - - - - - - - - - - - ---
-co o
- - - --- -- - - - -- 'a- -%- - -
X% %d %d 50 g o o 1~4t4 0 ¢) 0' %P" 5 8' - %Q0%~~~~~' Iz. " 4 Sl
-_-- - - - - - - - - - - - - - - - - - - - - - - - - - - - - -- -
__ _ __ _ _ I_ _ _ __ _ _ _ __ _ _ _ _. _0~~~~~~~~. W ~ "~~ i
_ _._ _ * _ _ _ _- _ _ _ _ _-__ _ _ -_ _ _- _ _- _ _ _ _ _ _ _ _ _ _ _ _ _

$> H H HIi -- -~~~~--- -- ---12P~~~~~~~~~~~~~~~~~~~~~~-
=; 1*.'-'(' IJ~t~)W:IVP 1 HO P I , _p
U 1E WA ! l@§fa;§ S W! 1W MmE3| 1! @ 0
* II *
-J 1 I 9 s ii o o I ? I Nt V , ;1 @
co w~ ~ i
I.Jt I1L~0 -'O% ( O" Vp
------------------------------- ----- - -
- -I11 &tgg l: " t -1 9 8M! ySll 1&"
________________________________ i

In ---- --
- In'f-.% --- ---
§ 11 iXEs AiZ A
i -4 u- , ---- e--
:lt --------------------- - -
I g 1 { m -* " sI i 0- _ __________
i A.M i MI } -E
e~~~ _~ ____________
( t :]i jXl 1 '2 3 02, I

IKE. --- - -- II[[ [II sX
9 . '.X" :
g-~~~ Va,_____ _____1I?S '. - I: I )d R
X w @ o 1o w w P U14 9 10XX ____ _ ___ __ __
# w S ° 18 g g ' 0%s-
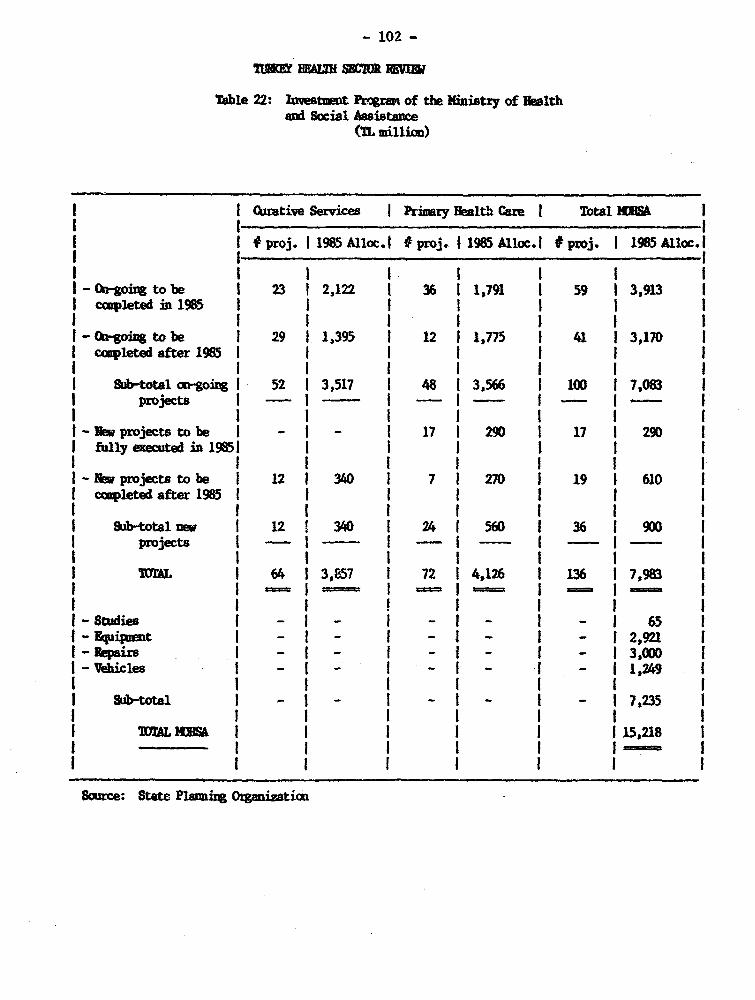
- 102 -
TO Hn SIMR JiRE
Table 22: IlvestmEt Prograu of tih Miistty of BEalthand Social Assistance
(TL mill)
1 (kirative Services Primry Health Car I Total IUlAL I
1 1 #proj. 1 1985 Alloc.i proj. 11985 Alloc.I poj. I 1985 11oc.II I . I
O- -going to be 1 23 1 2,122 1 36 1 1,791 1 59 I 3,913cplete n 1 1 1 1 1 1 1
Oa-(going to be 1 29 1 1,395 1 12 1 1,775 1 41 1 3,170eccupleted after 1985l
I cpe fe 9SI I I I I I II Sab-total -goiDgI 52 13,517 1 48 13,566 11 1 7,083 1I projects 1 -- I I I - I
I-N aprojects to be I -I - I 171 290 1 17 1 290 1I fully exeed in 19851 1 i I I I! I I I I I I II-R Mmprojects to be 1 12 1 340 1 7 1 270 1 19 1 610I ocletedafter1985 1 1 I I t I I I I I I I I
a1-totalnew 1 12 1 340 1 24 1 560 i 36 1 900 Iprojects 1 1 _ - -
I ~ 1U~AL I 64 13,857 1 72 14,126 1 136 17,983 1
I I _ I _ I _ I I -I-Studies I - - - I - I - 65 1
J-Egipznt I _ I _ I _ I _ I _ 12,921 1R-8epairs 1 - I - I - I - I - 13,000 1V-eicles I - I - I - I - I - 11,249 1
I Sb-total I -I- I -I - I - I7,235
TLM A I I I 115,218 1
I . I I I 1 1 o
Sice: State P1ami Orgnzticm

- 103 -
n IE I = R
Table 23: Fee Schedule For Selected NM Mdical Services in 1985and Real Increase or Decrease Since 1981
I I lsI1 ES* 1985 I REL I
I NNTICAL SICE I 1L I I 1 1$ I X)I. .. . , . ~~~~~~~~~~~~~~~I I
I I ~ I . 1 Ikstpaient Service
I .I I I I I visit 1 100 1 500 0 0.92 + 46
Pbysica 1auminatim I 1,000 I 2,500 1 4.61 - 27 1jiectiom 1 50 1 250 1 0.46 + 46 I
I ll DressiIg 100 1 1,000 1 1.85 I +193 1I lage Dressig 1 250 I 1,500 1 2.77 + 75 1
I atit serviI I I I I
I Itesive CaretUit I 5,000 1 7,500 1 13.84 -56 1I Deluxe Rom 1 2,500 I 5,000 1 9.23 1 - 42 1I Private Rcm l 1,500 1 2,500 1 4.61 1 - 51 1
Semi-Private oomI 1,000 1 1,500 i 2.77 1 - 56 1I hiltiple Bed Ron I 250 1 500 1 0.92 i - 42 1I Praubsurelncubstor ! 500 D 1,000 I 1.85 - 42 1
I inora Snery I 2,500 1 10,000 l 18.45 1 + 17IntermEdiate Sgery I 5,000 1 20,000 1 36.90 + 17 1
I Najor Surgery t 10,000 1 40,000 I 78.80 I + 17S Special Sugery I 20,000 1 60,000 I 110.70 1 -12
I I I I I II Spinal kestbesia 750 1 3,000 1 5.54 + 17
I NonlX-Rty 1 150 I 500 0 0.92 1 -3 3I BloodCellw Cwmt I 100 I 500 1 0.92 + 46 1
I~~ ~~ I 1 . . I
* Aplied frm April 15, 1981 Oxw& Decier 31, 1984.
S0IM: 3UA and missiaa esttes
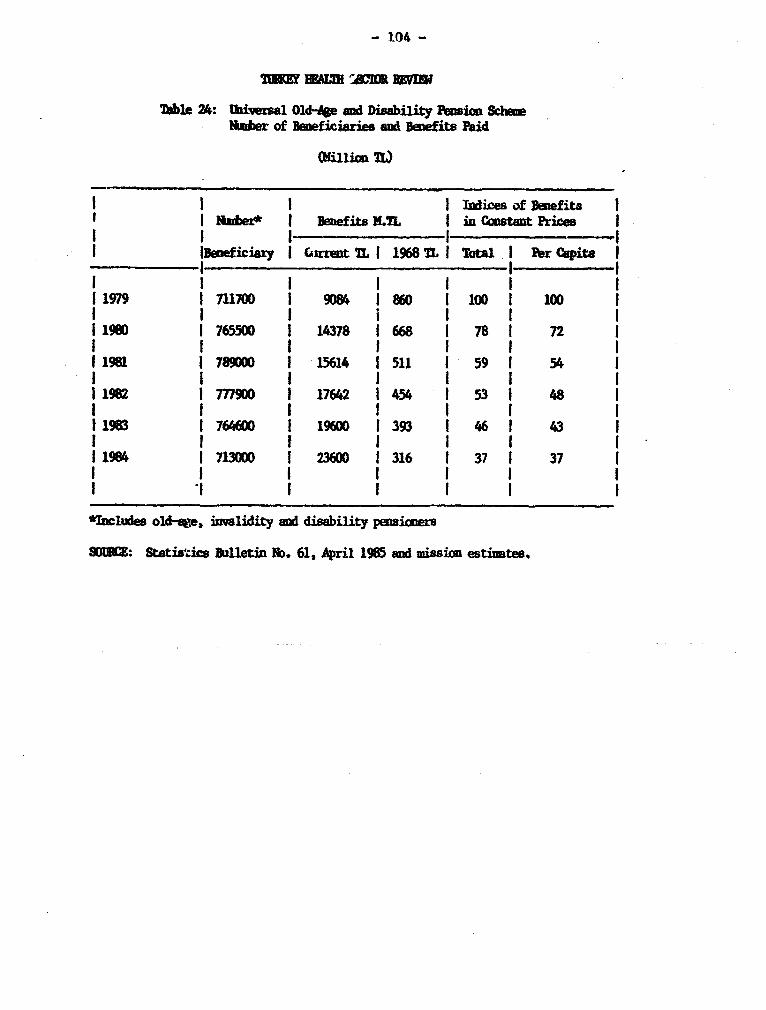
- 104 -
Table 24: Iaiversal Old*e and Disability Peusia SciemNRaber of BEe ciaries and Beeits Paid
Olilion t
t 1 I I lndices of Befita sI I aude~* 1 Isijbe 14efits I in Cinstant Prices II 1 I1 1 1
.Iueiciary I . zrent TL I 1968 IL I Total I er Cpita II .It
I i I I I 1 11979 1711100 1 9D84 1860 I100 IOD0 I ~I Im I o 6 o I 1 o I1980 1 765500 1 14378 I 668 1 78 1 72 1
I19#1 1789000 1 15614 1511 1 59 1 54 1I I I I I I I11982 Im900 1 17642 1 454 1 53 1 48 1I I I I I I I
193 1764600 l 19600 1393 1 46 43 1I I f I I I I 11984 713D 236 1 316 37 37
I| 1 1 I I t
*Iules old-%ge, 3nvality and disability pensioners
90132: Statiazics Bulletin ND. 61, April 1985 and mission esti,tes.

-- ----- -- ---- -- -- ---- - ----- -- ----- -- -------
fi~~~10 g o, !Q ! :ASg tsg B^
: - - --- ----------- I@ g R $I E 4 RJ I Ri
° III-- - -------------------------------
^~ ~~~~I i~~i j 1 ll *IIliiBi n 21Iiiij___H_____>_________g__________4________i_____ 4

- - - - - - - - - - - --
ve~~~~~~~~~~~~~.- I-- - - - - - -- -
-- - - - - - - - - -
- - - -- . - -- -
X~~~~~~~~~~~~~~~~ -- - - -; - - - - - - - - - - -
-------- --- -----------------
~~~~~~4 -4~~~~~~~~~~~~~~~-
'-I ~~!j I ..
°~~~~~~~~~~~~. .4 12a|48 ;fio0} g 0
M. _ __ _ _ _ _ __
_
-
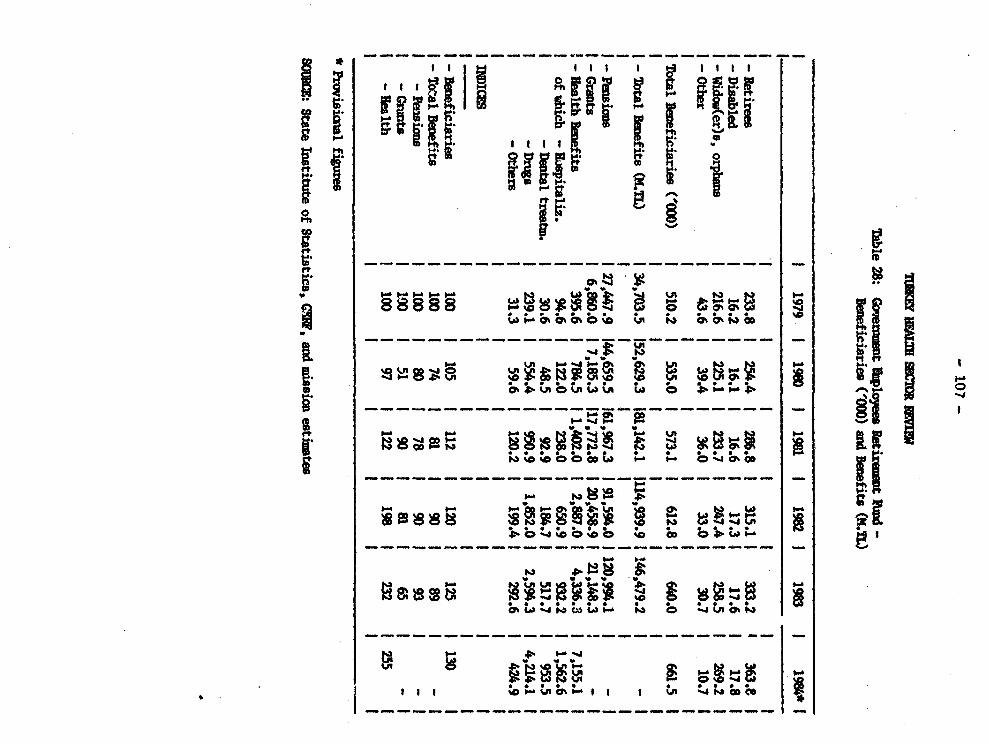
'1 W: , , , S X a W .C.
Zo' 00 ts'6b'tg~~~~~~z;-t ; i ILI LI ;4 6 z:
- - --- -| W oooow @ 9 coLX w b
i U.___________ _ L' .
{' oW>o>Wb W 'o S~~~~~~~_-* § g o*
i "89XF BEWbS! E S W§1C C JU @
Sg -soX I- II> %0.l'g I -.

- - - - - - - - - - - - - - - -
P-6 - ------- -4 -4 RMO
C4 co -----4 -
N - - -H--C -O -- 44
0 4
0 :N g R L
_- --------- -----O~~~~ ll A R n ne ;RSM,
-4 -4 Pe
a [IIw Weg S g ^s S S R gZ M Is I
*C41 ~ ~ ~ ~ ~ ~ ~ *I I I I - -
a _ _____________________ W

'I -. n------------- --
- -- - - - - - ~- - - - -- - - -
[j 1 1 i^ i6
w~~~~~ w .0.~~~~~~~~~~~~~~5B
ii~~~~~~~~~~~~~~. I | l- ° >4*,IS e 0 t |2 E i S oW CC) °°°oo a. 64 REigff iw t 8WX
~~s X. {g S
a-a - - .--..-. - - -- - ---
Oh t~IOh i Sg § | %s 4> eoicO so IQOhC,.ina 4 o
- ~ ~ ~ ~ ~ ~ ~ - --- --- -
- - - -~ O O h - - - - - - - - -
0,~ L. m ,o w I> t o*- - - - - -
6 5 0' 0~~~~~~~~~~~~~~~~~~~~~~~~~~~ 4 -.4
ft
S W 8fls S 8gag00 * *o~~~~~~~~~~~~~~~~~~~~ W W i01 _~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~- _
to~~~
---------- - - - - - - - - - - - - - - - - - -

- 110 -
lkble 32: Hospital Infrastz=ture and Utilization Pge 1 of 3by B.im and Provice (1984)
I ~ ~ . I I- I . 1 I 1, - II I I iA Z AM W I
I I BD6}8R m I gae I s 8 1AouSo m I II g EAND PMUAT I = D eM PM StY iVISITS/IPW1 I 1984 I PR. SM I MUM I (MS) Ova:UxATI PERM I
I REMI1 1 I 1 1 I I'Ilixkareli 1 291,7831 1.4 84.51 381 4.21 36.41 0.61Ediuie 1 375,964| 1.3| 80.41 361 5.31 49.21 0.6'IstgUbui l 5,601,228 1 4.4 1 85.2 1 68 1 12.4 1 61.5 1 1.1 1ibMdrnlg I 384,6411 1.91 94.81 43 1 7.2 1 46.9 1 0.5
Subtotal I 6,653,6161 4.01 85.41 641 11.81 60.51 1.0
lI I I .I , I . I _ I I ilKncaeli 1 672,4031 1.51 93.91 531 5.41 54.01 0.91IZougldak 1 1,024,2751 1.7 94.41 591 6.51 64.31 1.0IBolu 1 496,5361 1.9 1 91.5 1 47 1 8.1 1 59.4 1 0.611Sakarya I 579,7441 1.61 86.41 461 5.01 44.71 0.81
1 8ubtotal 1 2,772,9581 1.71 92.11 53 6.21 57.41 0.91I . I .-1 -1 - -.-- _ -I _-II FcIcIO 3 3 I I i I I I I13irsa t1,263,385 1 1.9 1 84.8 1 61 1 6.3 1 63.7 1 0.7 1ICavakkAle 1 403,983 1 1.1 1 94.3 1 33 1 4.6 1 39.5 1 0.41IBalikesir 1 889,105 1 1.9 1 100.6 1 61 1 6.1 1 51.2 1 0.81I I I I I I I I I
Subtotal 1 2,556,4731 1.81 91.71 571 6.11 56.1 1 0.71
I ~ GER 4 4 I I I I I I I1!4uiisa 1 981,423 1.81 87.61 421 7.31 51.31 0.71Ilunir 12,160,654 1 3.1 1 94.81 841 7.51 57.61 1.1IAydi 1 676,508 1 1.7 1 86.61 521 4.81 47.01 0.9IDwigli U 626,805 1 1.5 1 97.71 51 4.31 39.9 1 0.5 1lfi4a 1 459,5421 1.2 1 89.0 1 41 1 4.9 50.1 1 0.6 1
I Subtotal I 4,904,9321 1.8$ 93.21 45 1 7.5 1 56.4 1 u.61I I I -1 -ll _ -1 -_I - -1I
I REIms 1 I I I t I IIBilecik 1 152,586 1 0.8 1 100.0 1 22 1 5.1 1 37.4 1 0.31lEskiseir 571,518 1 2.6 1 93.31 901 5.31 53.01 1.0 IIlntahya 1 512,3861 1.9 98.01 581 6.71 56.9 0.71llUsk 1 256,7391 1.61 100.01 541 5.81 51.91 0.8tMyu 1 :607,5731 1.51 88.51 401 6.41 51.91 0.4
I Subtotal 1 2,100,8021 1.31 95.3i 401 5.81 53.81 0.5I I 1 -1 -I- -I -l -I
I~~~ I__ _ _ I ___ _ I 1___ I I__I_ _ _
TAZ32A

- 111 -
Table 32: lapite I e U tilizstion Pae 2 of 3by Regimo aui ne, 1key (1984)
I I I I I ' 1 1 1 1I I I S I IAYUA II I III REGOIIAND THUMI MS I PD I M1 I S IV /II 1WVUIZ I 1984 I CPC. I - I I ( S) u1wA1cT1 1m I
I BaM 6 t ! t I J IIlrta I 365,7421 4.6 1 88.6 1 941 10 .1 64.01 0.81
1adur 1 242,286 1 1.41 95.7 1 32 1 6.11 38.7 1 0.4 1lAntalya I 794,962 1 1.41 95.8 1 51 1 5.6 1 58.01 0.8 1
| § ~ ~ I I I I I I ISubtotal I 1,402,9901 2.3 91.9 1 59 I 10.01 71.7 1 0.7 1
I ~I .. I -I -1I -1 *--I -1 -1I i3iL0"7 7 1 1 I I I I5Kastmonu 1 458,154 1 2.6 1 86.3 1 48 1 7.7 1 45.5 1 0.5 IICsikiri 1 253,865 1 1.3 1 80.0 1 33 1 6.5 1 54.1 1 0.3 1WAMkars 1 3,010,203 1 3.9 1 89.4 1 32 1 9.6 1 61.4 1 1.2 1Irsr3ebir 1 244,691 1 0.7 1 87.4 1 35 1 3.4 5 52.4 1 0.2 1IYO,1at I 506,621 1 0.9 1 103.8 1 25 1 4.7 1 33.91 0.3 1INeusehir I 261,110 1 1.1 1 56.9 1 34 1 3.3 1 48.2 1 0.3 1I I I I I I I I 1
Subtotal I 4,734,6441 3.01 88.71 651 8.81 58.51 0.91I~~ ~ ~ I. S _I I -I _ -l -1 l_
I RiGICN8 1 1 1 1 1 1 11Ianya I 1,642,438 1 1.4 1 96.5 1 26 1 4.8 1 42.4 1 0.3 1lNigde I 540,357 1 0.6 1 101.1 1 29 1 4.7 1 53.3 1 0.4 1
Subtotal 1 2,182,7951 0.8 97.51 27 1 4.8 1 44.8 1 0.3 1I I I - l - -_ -l - -lI1 RFriON9 9 1 1 I 1 1lSamum I 1,067,163 1 1.6 1 84.2 1 49 1 7.2 1 68.5 1 0.6 1ISinop 1 280,979 1 0.9 1 85.8 1 31 1 5.3 1 53.2 1 0.3 1ICOrDn I 586,894 1 1.3 1 90.4 1 44 1 6.3 1 60.9 1 0.4 1mbmRyB I 351,609 1 1.3 1 88.0 1 37 1 5.2 1 45.6 1 0.3 1
lo,du I 741,373 1 1.3 I n.6 1 35 1 5.6 1 54.9 1 0.4 I
I Sbtotal 1 3,028,018 1.41 82.91 421 6.4 60.7 1 0.4 1
I 1 -5R--1 1 111- I -Iftdst I 638,510 1 1.0 1 9.4 1 37 1 4.9 1 47.0 1 0.4 1ISivas I 756,360 1 1.8 1 91.5 1 42 1 6.8 1 46.0 1 0.6 1IKayseri 1 837,6511 1.6 99.91 57 1 5.3 1 49.4 1 0.6 1
1 Subtotal 12,232,521 1.6 1 96.4 1 48 1 5.5 1 47.6 1 0.6 1
1 795,8655 0.6 1 94.8 1 20 1 4.5 1 44.0 1 0.3 1bbIMan I 1,636,293 1 1.6 1 70.9 1 41 1 6.0 1 59.1 1 0.4 1IIcel 1 922Y330 1 1.2 1 91.1 1 42 1 5.2 5 52.3 1 0.8 IIGcaiantep I 862,844 1 1.5 1 98.2 1 72 1 4.4 1 57.6 1 0.6 1Iflatay 1 923,069 1.0 86.95 351 3.9 43.4 0.61I I I t I I I I I
Subtotal I 5,140,4011 1.35 83.9 1 42 1 5.0 1 53.9 1 0.5 1iTLI -I I- -I-I_ I_II _ _ _ _ _ I I l. I1 I !TAl 325

- 112 -
Table 32: loapital 1f UCtr _x Utilintics Page 3 of 3-by Regios and Pwrtnce (1984)
I I I I 1 1 ^ 3 3 II I I P I I 2a A1S_ I III iU2OAND IPOUATI TUS , MS I m IAI 1 I JT.SYI
I ROM n1 1984 t C. I sAFF I US_ 1 8M) IOCMAZCTl P3( I
I U= ~12311111 IGiream 489,153 1 1.5 1 106.1 1 45 1 7.6 1 58.0 1 0.4 1lTrabos 1 737,5711 2.3 1 71.8 1 53 1 6.3 1 54.7 1 0.6 tIRium 1 375,381 1.4 1 98.1 1 59 1 4.9 1 56.5 1 0.9 3bhrnvin 3 229,519 2.8 92.91 383 5.51 42.0 0.31
IQmabmosue 1 263,553 0.7 110.01 17 4.93 28.0 0.21
I subtotal 1 2,095,177 1.7 87.2 1 46 1 6.2 1 52.7 1 0.5 11 I I -I -I -I -[ -I -I RHM 13 1 1 3 3 3IliwlD I 238,897 0.5 81.71 121 4.71 38.8 0.3 1ITbrceli 1 153,723 1.03 77.4 271 6.5 61.73 0.5 tIllzig 1 453,5671 4.21 59.7 1 40 1 13.1 1 57.4 1 0.6 1lNaIatya I 623,151 1 1.4 1 99.2 | 27 1 8.0 1 41.4 1 0.6 1
1hdiyam~a 379,1791 0.7 90.9 261 4.5 48.3 0.23
1 9ubtotal 1 1,848,517 1.8 74.31 281 8.91 50.31 0.51
1 1 1 4 1 - - - -IDiyartukir 3 855,915! 2.4 88.01 453 7.3 41.9 0.71ISiirt 484,964 3 0.5 1 57.2 3 9 I 5.2 1 36.4 1 0.3 1
3. 590,7993 0.4 86.33 103 5.4 38.1 0.23ISanliurfa I 605,6793 1.0 82.73 15 5.13 24.7 0.33I I 3 1 3 I 3 I 33 abt.otai 32,537,357 1.3 84.23 23 6.6 38.11 0.4
I RE6c, 15 1 i~ - I 3 1 3 3huers 1 695,519 0.81 66.31 15 4.4 1 33.0 1 0.3 1ihgri I 389,9883 0.3 95.31 13 3.8 1 38.4 1 0.2 1IErz&rum 3 832,976 1 2.5 1 85.3 1 47 1 9.6 1 56.2 1 0.6 1Ilr,incan 1 280,9231 1.81 78.33 373 4.51 33.21 0.73
Subtots1 1 2,199,406 1.5 81.5 301 7.5 1 48.7 1 0.4 1
I RBEI0 16 I 1 1 1 3 1 1bHIa I 2323,110 1 0.6 I 80.0 1 23 6.2 1 42,8 1 0.2 1IBitlis 3 281,005 0.61 74.9 11l 4.8 30.3 0.23IVan I 519,6713 0.8 1 58.2 3 17 1 5.1 1 47.9 1 0.3 3NIfaksai I 173,930 0.3 91.71 121 6.31 67.7 0.1 1I I 1 I I f I 3 I 9ubtotal 3 1,297,7161 0.71 68.71 15 5.31 44.61 0.21
I MMA IML 047,688,323 2.01 87.53 46 7.91 56.9 0.51_ -2 _- - - -1 3 -I -
TAWZ 3~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~

- 113 -
TEMnAT W REV3
Table 33: Ilnidwrty Hospital Infrastracture and Utilization Statisti (1984)
I I I I A I I I I I 1 II I N 5 1 ISrAe IEI I Z I 1AUA1 100MIIN1ESY 1 wUmI A1 m Ms I Z I 2 I PATJISTY IRA IIDrAL IMS I s I (5) I APPVU 1A34UII MS I OIM8) I (2) I
I. ,_ _ _ _ _ _ _ _ _ _ _ I. __ __ _ .1 1__ _ I ,,,.___ I. __ __ _ I _ _ __ _
I -AlgARA- I I I 1 1 t 1 I II I i I I I I I I IlAakara 1 2,157 1,984 92.01 15.6 13.9 1 18.7 1 13.8 1 56.1 1Ibcettepe -Gem 1 8261 9011 109.1 1 6.0 1 10.8 1 10.3 1 9.8 1 68.1 I
P-ediatrits 350 1 322 1 92.0 1 2.5 1 3.6 1 4.1 1 11.61 75.5 1-Dist. GC I aS 1 51 51 100.01 0.41 1.1 1 0.41 3.6 1 45.0 1-Psychiatric 1 1201 -1 -I -1 -I -f -1 -
1Gzi - Trmtolo 2001 _ I _ I _I _ I IWlitar Hbspital I -I -I -I -I -I -I -I -It I I I I 1 1 I I
| - - ~ ~~I I 1 I I I I I II ~ ~ ~~I I I I I 1 I I
I%=r8 - we l 1 2,282 1 1,3281 58.2 16.6 1 8.3 1 8.3 1 10.2 1 36.9 1IsWtaul -Genera1* I 2,120 1 1,4701 69.3 1 15.4 13.8 1 14.9 1 11.0 1 60.2 1
-I_ R - I I I I I I I I I
IAeae -Cenera 1 1,8671 1,8531 99.31 13.5 1 14.2 1 13.8 1 9.9 1 44.2 119 Sept. - Geral 1 3011 2911 96.7 1 -I -I -I -I -I
I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~I cI I I I I I I I
lMa -General I 515 1 50 1 97.7 1 3.7 1 7.6 1 5.9 1 7.9 1 69.3 1Ihntaly -General I D001 143, 143.01 0.71 2.41 2.01 6.7 1 66.1 1r a-Gaieral 1 4271 -I -I -I -I -I -I -I
IDiyabuIcir -Geeral I 549 1 690 1 125.7 1 4.0 1 5.2 1 4.4 1 7.3 1 40.6 1l1ixne-G 1 1 -I -I -I - I - I - I - I - I - IIElazig -Gmeral 1 170 1 113 1 66.51 1.2 1 -I -I - I -IIEir.ebir -Geral | 200 1 191 1 95.5 1 1.5 1 2.0 1 1.5 1 7.8 1 47.3 1f|a1m -N ieal I 2001 1911 95.51 L51 6.81 6.91 7.81 47.3 1
bysei -Gal 1eral 2431 3161 130.01 1.81 3.91 3.61 9.41 67.5 1imam"a- Guera 1 4411 -I -i -I -I - I - IIlumm -Genral I 2691 1801 66.91 2.01 2.4 2.0 8.21 64.4 1ISiva -General 300I 2681 89.3 1 2.2 1 2.8 1 2.2 1 8.1 1 49.2 1lTrabzon -General 1 961 1221 127.11 0.7 1 1.1 1 1.1 1 9.9 1 52.0 1
I I I I f I r I I I_ ITffOAIL I 13,784!1 10.917 1 86.7 1 100.0I 100.0) 100.01 10.2 1 54'.4 1
* Total coobwies 2 vedical schools.** Total based on available infounation.
SOCEe: 1984 Hbspital Sbitistic8, MM!, hrkara, 1985.

Tm uHwi Sam r
Table 34: hpesR e per Patint Day ard Per Bed for a Smile of K Hepitals, 1984
* . w I .0i 1 ' .' /'II' -S
:Iber of : Occupancy :otal pEnses: Expense Per : Daily Expense : % of 1eis: 1es CoveredIHspital :Staffed Beds : Rate (2) :TL (OO's) : Patient Day Per Bd : For alaries: by User Fees :
: : A
:Tewehti lspitals: : : : :: Arksaa Itme : 1408 : 70.0 : 2,381,853 : 6,621 : 4,636 : 49.9 : 18.9: ADsra BEtanesi : 393 : 69.3 : 921,405 : 9,269: 6,422 49.8 : 13.3: Istanbul Sisli : 774 : 52.4 : 903,365 : 6,102 : 3,197 : 38.5 : 17.1
:Specislizsi Ebspitals: : : : : : : Ankars Cardio-yascular : 373 : 74.7 : 1,470,549 : 14,460 : 10,800 : 35.9 : 34.9
Istanbul Cardio-vascular : 169 : 73.8 : 653,847 : 14,363 : 10,600 : 40.6 : 29.5 ::Isparta orthOpedics 600 : 85.2 : 303,652 : 1,627 : 1,386 : 43.0 : 16.2 :: * : : : : A : : *
: pitals: : : : : :: Kutahya 390 : 56.7 :278,658 : 3,452: 1,956: 55.4 : 12.2: Antskya (Hatay) : 170 : 38.4 : 166,888 : 7,004: 2,690 : 71.9 : 11.2: Istanbul Yalova : 100 : 36.7 : 133,777 : 9,987: 3,666 : 62.1 : 12.6: Kirsehir : 98 : 67.0 : 182,166 : 7,601: 5,093 : 74.9 : 8.3: Aydin : 35 : 20.0 : 29,385 : 11,501: 2,301: 77.6 ^ 4.8: Coru Tkilip : 50 : 127.3 : 54,711 : 2,355 : 2,997 : 70.9 : 8.1: A : : : : : : :
* Average lergth of stay
S90CE: MEA and missuion eatimstes

Turkey: Contributions & Beneficicaries180 - Social Insurance Organization
I Beneficiaries
170 -
160 -
150 -
140 -
(D 130 -
c 120 -
Insured
100 Lu
go - \ / _ lTotal Contributions
so
s0 L f health Contributions
701979 1980 1981 1982 1983 1984
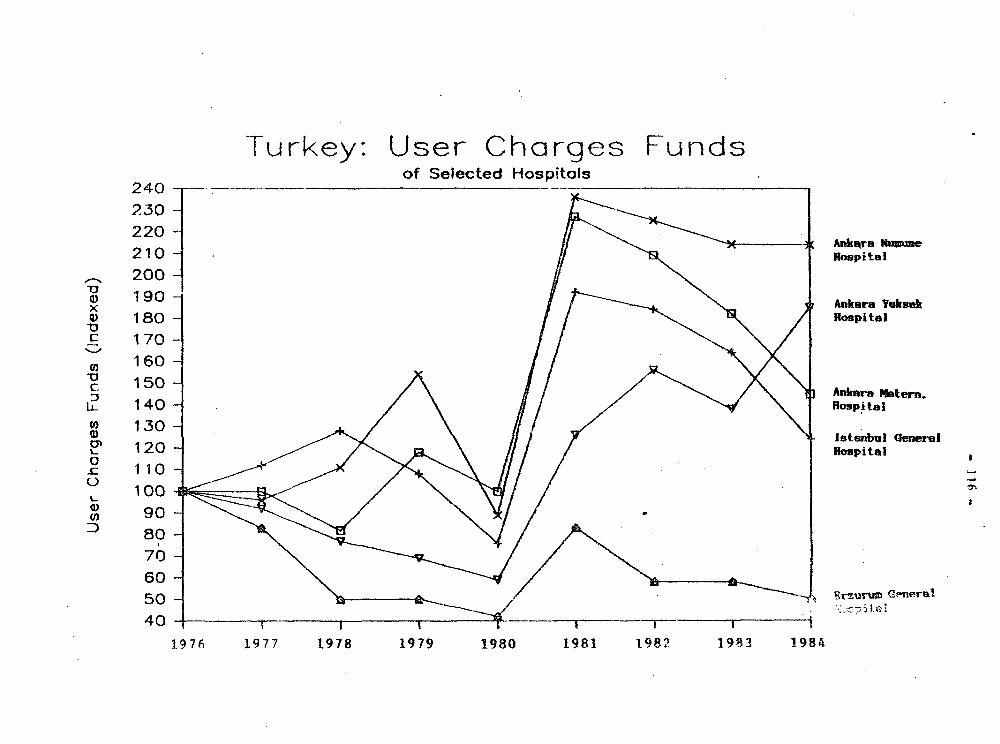
Turkey: User Charges Fundsof Selected Hospitals
240230e]220 - __
210 1 Hospital
2001190 Ankara Yaksek
0I) 180 Hospital170
150 i Ankara thtern.
23 140 - Hospital
1 30 - \~\
5,130 ~"IstanIm, General120 Hospital
1 191 00
9080766050 p G-rd
1.976 1977 t978 1979 1980 1981 1982 1983 1984
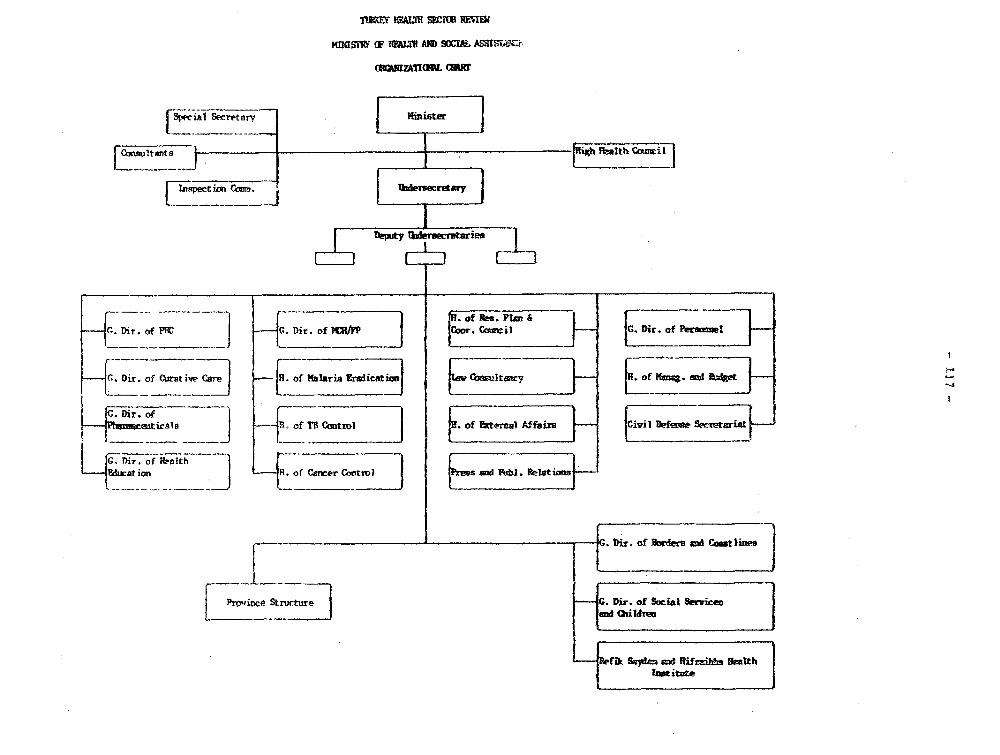
TOM' F&E SW" REW1
MSt- F FMV WiH AND S2tAL ASSISW:r,
(wnmzATraL cow
C LIjPes t ion i lt Ihfecre e
{ _ e~~~~~~~~~~~~~~e
of Res. pFim _4 . Dir. of PFI: J Dir, of .cmji V Dir, of h l }
.__________ [_ . __~~~~~ ~ ~ ~ ~~~~__________ __________
_ C;. 9ir, of (rstkw te jof Malaria Eraiicatwio tai It cy of ? a mxI tt
G. Dir, of . _t ,
XEdhrat ion _ R. of Cemcer Control a nd el t. Relstiom
__G. ir. of Uders aid CowtIin" j| Province Stnx:ture G. Dir. of Social servi|es
_. Q,ildU
(kSadf and ffif=zilf Smithl.otituZe
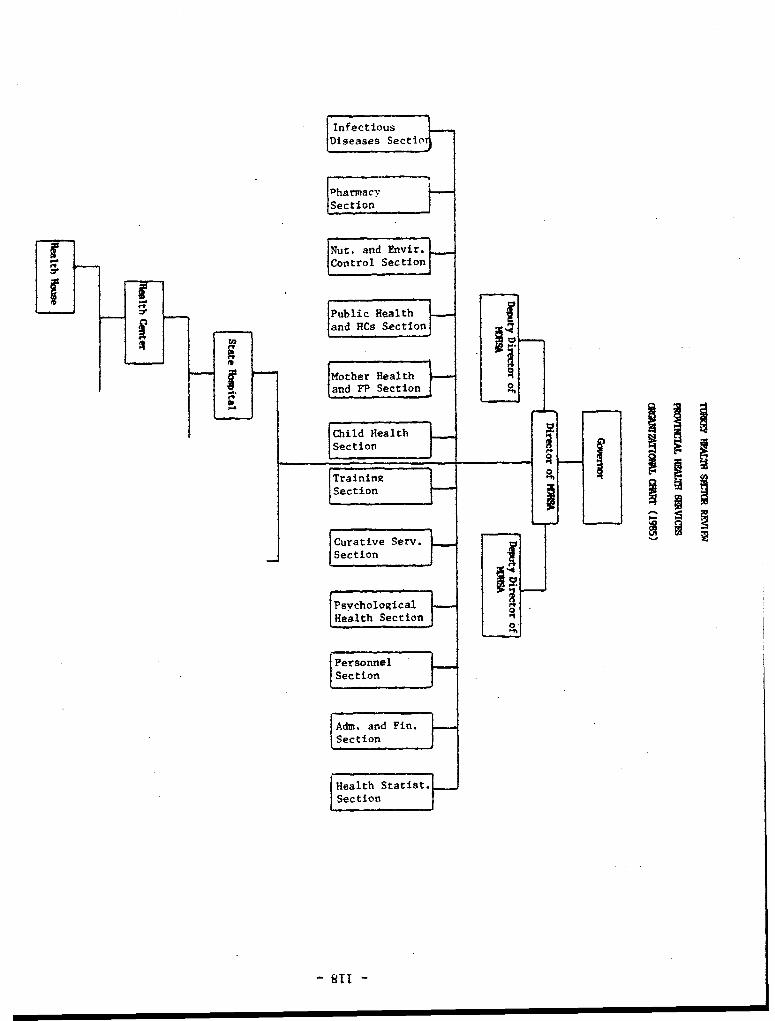
InfectiousDlseases Sectic l
PharmacySection
Nut. and Envir.Control Section
Public Healthand HCs SectionrA~~~~~5Mother Healthio4land FP Section
Child Health
Section
TraininR xSection
Curative ServSection
PsvchologicalHealth SectiOn
|PersonnelSection
Adm. and Fin.Section
Health Statist.Section
SllI -