research report - london school of hygiene &...
TRANSCRIPT

Page
1
Formative Research to inform design of a behaviour change
intervention for the “F” and “E” of the SAFE strategy in
Oromia, Ethiopia
RESEARCH REPORT
Principal Investigators
UK: Ms. Katie Greenland
Research Fellow in Hygiene Behaviour
Environmental Health Group
London School of Hygiene & Tropical Medicine
Keppel Street, WC1E 7HT
Ethiopia: Dr. Wondu Alemayehu
Berhan Public Health and Eye Care Consultancy, Ethiopia
& Technical Advisor to The Fred Hollows Foundation Ethiopia
Co-Investigators
Ms. Sian White
Dr. Adam Biran
Environmental Health Group, LSHTM
Dr. Matthew Burton
Mr Esmael Habtamu Ali
Trachoma Group / International Centre for Eye Health
LSHTM
Dr. Zelalem Haabtamu
Mr. Damtew Yadeta
Oromia Regional Health Bureaau
Mr. Nazif Jemal
Mr. Ahmed Abajobir
Mr. Berhanu Bero
Mr. Amanuel Atomsa
The Fred Hollows Foundation Ethiopia
Dr Aida Abashawl
Berhan Public Health and Eye Care Consultancy, Ethiopia
Funded by: The Fred Hollows Foundation

Page
2
Executive Summary Background
Globally, evidence around the “F” and “E” components of the SAFE strategy – which consists of Surgery, Antibiotics,
Face washing and Environmental change – is lacking, which in turn has limited the effective design of trachoma
elimination programs in countries like Ethiopia. The formative research reported on in this study was conducted to
identify, and explore the determinants of a range of behaviours and hygiene practices that are potentially associated
with increased risk of trachoma in a trachoma hyper-endemic area of the Oromia Region of Ethiopia. The following
behaviours were explored: defecation and stool disposal practices; general water use; personal hygiene behaviours,
including handwashing, face washing and face wiping; laundry practices; sleeping arrangements; and solid waste
disposal practices.
Specific research questions
What are the current practices pertaining to water collection and priorities for use; personal hygiene i.e. face
washing and wiping, handwashing and bathing; defecation and stool disposal; animal husbandry and faeces
disposal; garbage disposal; fly control; sleeping arrangements; and laundry?
Who carries out these behaviours, where, and using what?
How do the social, physical and biological environment influence water use, personal and other hygiene
practices, sanitation practices and sleeping arrangements?
How important are knowledge of trachoma, rational decisions, different motives and cues in driving each of
the behaviours of interest?
Are potential intervention strategies acceptable to the community and considered feasible?
Methods
Methods included direct observation in households with young children, semi-structured interviews with caregivers
of young children, focus groups with mothers of children under three years-of-age, grandmothers and fathers to
explore the behaviours, solutions and community perceptions and interviews with key stakeholders within
community and district structures. Data were collected over two weeks in January 2016. Ten households, from five
different Kebele’s (communities) were purposively selected to take part in direct observation. At the end of each
observation caregivers from these families were interviewed. A total of five focus group discussions (FGDs) took
place, one in each Kebele. Lastly, stakeholder interviews were conducted and four individuals, a Kebele leader, a
School teacher in a school with a Fred Hollows Foundation Trachoma Club, a Health Extension Worker and a District
Level Government worker involved in trachoma elimination. Findings were thematically analysed by behaviour. A
theoretical framework of the determinants of behaviour was used to help guide the data analysis and interpretation
process.
Results
A range of sub-optimal hygiene practices were documented in these communities. However, there were also many
positive hygiene practices or practices that, although sub-optimal, made sense given the constraints of the setting.
Sanitation infrastructure in these Kebeles was observed to be poor. Only three of the five communities
studied had latrines, but they had been poorly constructed following advice by Health Extension Workers,
had been built under the threat of a fine and were not in high demand. The latrines in the school that was
visited and the health centre were well-constructed but there was a lot of faeces in and around the latrine
buildings. It was acceptable for young children to defecate within the home and compound. Open defecation
was still a normative and accepted practice and faeces were not buried after defecation. Human faeces were
observed within many compounds and faeces were around the holes of the latrines creating a suitable
breeding environment for Musca sorbens flies even in communities with latrines.
Flies were common in all communities and were frequently seen on faces (mainly children’s) and on animals.
Animals were kept in close proximity to humans, either within the compound or even within the sleeping
quarters of a house.

Page
3
Faces were observed to be washed as part of a routine on a daily basis and occasionally in response to a cue
(food or dirt on the face). Faces were not dried after washing, but Vaseline was commonly put on faces once
dry. Differences between face washing among family members were observed, with not all faces washed in a
household and some washed with soap and some without. Any family member could assist another while
they washed, although mothers tended to care for the youngest children. School children were reportedly
judged negatively if their faces were unclean.
Faces of young children were rarely wiped, even when the child had visible eye or nasal discharge. Hands or
clothing were used for wiping but hands were not washed afterwards and it was not considered necessary to
use soap to remove discharge.
Full body bathing was frequent for babies (a priority) and weekly for school children, but adults bathed
infrequently (less than once a month) and women lacked privacy to bathe at home. Water availability also
constrained the frequency of bathing.
Flies were particularly prevalent on animals and faces, but did not appear to be attracted to garbage (which
was largely inert) or drying / dry cow dung. Flies are thought to be attracted to milk and cattle.
People slept closely together and shared pillows and blankets, although older children often sleep apart
from their parents and young siblings. Mattresses, skins, blankets and pillows were available in insufficient
quantities to allow each individual to have separate bedding. Sleeping patterns alter following the birth of a
child or when there are visitors.
Laundry was done infrequently with the exception of the clothing of babies. Some items of bedding were
washed at the river, again on an infrequent basis (perhaps monthly or less) as too much water is required to
wash bedding at home. Laundry is time consuming and inconvenient.
Discussion
Possible solutions for each of the sub-optimal practices identified are explored. There are multiple potential routes
by which trachoma can be spread and it is unknown which of these is the most important. However, it is possible to
consider the biological plausibility and feasibility of intervening in different areas. For instance, it may be less
relevant to focus efforts on encouraging more frequent laundry of bedding - which requires a lot of water and time
and may not interrupt transmission - than to invest time in sanitation promotion to establish an open defecation
free environment and to encourage safe disposal of all human faeces in latrines with drop-hole covers. School
sanitation should not be neglected. Given the source of infection on a person is nasal and ocular discharge,
encouraging new habits to develop for face washing so that the faces of all household members are washed with
soap on multiple occasions throughout the day should be a priority. It may be possible to encourage face washing
before bed and complement this initiative with promotion of separate pillows for each household member. It is also
worth exploring how to make nasal and ocular discharge appear more disgusting to try to trigger appropriate action
(e.g. wiping and handwashing) in response to this visible cue. Promotion of bathing shelters may also encourage
more frequent bathing and thus face washing, although it would be important to understand how water scarcity at
other times of behaviour would affect this and other hygiene practices. A number of context-specific behaviour
change techniques for each of these strategies are proposed and warrant further development through behaviour
trials and piloting of concepts.
Following this research, key next steps include a) a review meeting to explore the findings and potential
opportunities for intervention in more depth b) replication of some of these study methods in another setting with a
high trachoma burden, in ‘cold spot’ locations with low trachoma prevalence, and in the same setting at harvest /
rainy season (when hygiene behaviours are substantially compromised) c) behaviour trials and/or concept
development of feasible interventions, bearing in mind the fact that a campaign with a limited number of messages
is more likely to be successful. Although not the main focus of this research, a number of potential touchpoints were
identified that could be exploited in a future campaign.

Page
4
Contents Executive Summary ..................................................................................................................................................... 2
BACKGROUND ............................................................................................................................................................ 7
Situation in Ethiopia (and Oromia) .......................................................................................................................... 8
Study rationale ........................................................................................................................................................ 8
Conceptual framework ............................................................................................................................................ 8
Overall Aim ................................................................................................................................................................. 9
Specific Objectives and Research Questions ................................................................................................................ 9
METHODS ................................................................................................................................................................. 10
Study design and setting ....................................................................................................................................... 10
Study population ................................................................................................................................................... 10
Data collection ...................................................................................................................................................... 10
Observation and interviews ............................................................................................................................... 11
Focus group discussions .................................................................................................................................... 11
Stakeholder interviews ...................................................................................................................................... 11
Data handling and analysis .................................................................................................................................... 11
Ethics and consenting............................................................................................................................................ 12
Training ................................................................................................................................................................. 12
RESULTS .................................................................................................................................................................... 13
Reporting framework ............................................................................................................................................ 13
Setting and participants ........................................................................................................................................ 13
1. Water ................................................................................................................................................................ 14
Availability ........................................................................................................................................................ 14
Use.................................................................................................................................................................... 15
Reuse ................................................................................................................................................................ 16
Factors affecting availability and use ................................................................................................................. 16
2. Cleanliness of faces ........................................................................................................................................... 16
Frequency of face washing and bathing ............................................................................................................. 16
3. Face wiping ....................................................................................................................................................... 19
4. Handwashing .................................................................................................................................................... 21
5. Sanitation .......................................................................................................................................................... 23
Toilet availability and sanitation promotion....................................................................................................... 23
Toilet type ......................................................................................................................................................... 23
Page
5
Toilet use/lack of use ........................................................................................................................................ 24
6. Animal faeces .................................................................................................................................................... 25
7. Garbage ............................................................................................................................................................ 27
Cleanliness of home environment ..................................................................................................................... 27
Garbage disposal ............................................................................................................................................... 27
8. Flies................................................................................................................................................................... 28
Presence of flies ................................................................................................................................................ 28
Factors influencing compound cleanliness............................................................................................................. 29
9. Sleeping arrangements ...................................................................................................................................... 30
Current practices ............................................................................................................................................... 30
Factors influencing current practices ................................................................................................................. 33
10. Laundry ........................................................................................................................................................... 34
Regularity of washing clothing ........................................................................................................................... 34
Regularity of washing bedding........................................................................................................................... 35
Community perceptions ............................................................................................................................................ 36
Trachoma and its control ...................................................................................................................................... 36
Perceived issues in the community........................................................................................................................ 37
Perceived role of men and women ........................................................................................................................ 37
Decision making in the household ......................................................................................................................... 37
Children and childhood manners ........................................................................................................................... 38
Treatment of guests .............................................................................................................................................. 38
Perceptions of an ideal mother ............................................................................................................................. 38
Gossip ................................................................................................................................................................... 39
Celebrities ............................................................................................................................................................. 39
Community structure and touchpoints ...................................................................................................................... 40
Holidays ................................................................................................................................................................ 42
DISCUSSION .............................................................................................................................................................. 43
Potential intervention strategies ............................................................................................................................... 43
Overview of solutions in relation to trachoma transmission .................................................................................. 43
Face washing solutions .......................................................................................................................................... 45
Hand washing solutions ........................................................................................................................................ 48
Sleeping and laundry solutions .............................................................................................................................. 49
Presence of flies (sanitation) solutions .................................................................................................................. 51

Page
6
Considerations for intervention design and delivery .................................................................................................. 52
Implications of current trachoma control .............................................................................................................. 52
Implications of community perceptions ................................................................................................................ 53
Implications of community structure and touchpoints........................................................................................... 53
Implications of context .......................................................................................................................................... 54
Limitations ................................................................................................................................................................ 54
Conclusions and recommended next steps................................................................................................................ 54
References ................................................................................................................................................................ 55
Appendices ............................................................................................................................................................... 56
A Research questions ............................................................................................................................................ 56
B Structured observation notes and pictures ......................................................................................................... 56
C Focus group discussion guides ............................................................................................................................ 56
Page
7
BACKGROUND
Trachoma, caused by the organism Chlamydia trachomatis, is the commonest cause of infectious blindness and
results in the loss of 1.3 million disability-adjusted life years [1]. The mechanism of transmission is not fully known,
but is thought to mainly include: 1) direct spread during play or sleep; 2) spread on fingers (after touching ocular and
nasal secretions); 3) indirect spread by fomites such as towels; 4) and spread by eye-seeking flies [2]. As trachoma
tends to cluster in villages and households, transmission is also thought to be associated with close, prolonged
contact [3]. Cases of active trachoma are a major source of infection, and the highest bacterial loads are usually
found in pre-school age children, particularly those under 1 year-of-age [4].
The Global Elimination of Trachoma 2020 (GET 2020) initiative was set up with the goal of eliminating blinding
trachoma by 2020 through implementation of the SAFE strategy. SAFE entails: Surgery for the distorted upper eyelid;
Antibiotics to treat infection; Facial cleanliness and Environmental hygiene to reduce transmission. The “F” and “E”
components are challenging in areas prone to drought, and amongst pastoralist communities who migrate and have
poor access to water. Indeed, migration makes all aspects of the SAFE strategy challenging to deliver. In practice,
trachoma elimination methods have been biased towards ‘S’ and ‘A’ interventions. Azithromycin (Zithromax) has
been shown to be highly effective at clearing Chlamydial infection after only one dose [5]. Annual mass distribution
of antibiotic (MDA) with donated Zithromax is now being rolled out in communities demonstrated to be endemic for
trachoma. Surgery to correct the upper eye lid deformity is also effective at preventing vision loss, and in some
instances can improve vision: it certainly reduces the pain and discomfort from ingrowing eyelashes [6]. It is now
increasingly recognised that ultimate interruption of transmission requires “F” and “E” [2]; i.e. implementation of the
full SAFE strategy [3]. Delivery of “F” and “E” components present several challenges for practice. Their
implementation will require significant localised programming, resources and behaviour change. It is also likely to be
most difficult to achieve regular face washing and environmental hygiene in the settings in which trachoma thrives
(e.g. drought prone and water scarce area, amongst the poorest of the poor and amongst nomadic pastoralist
populations) [7].
One way trachoma is thought to spread is through eye-seeking flies, principally Musca sorbens, which are attracted
to, and feed on ocular and nasal secretions [8, 9]. Female Musca sorbens flies lay their eggs in waste and faeces.
They prefer human faeces, but also breed (with lower fitness, i.e. giving rise to smaller offspring) in the faeces of
other animals [10]. There is some evidence of the effectiveness in reducing fly populations from trials of insecticide
spraying and the use of pit latrines [11, 12]. Latrine access reduces trachoma [11], possibly because it removes faecal
matter from the environment so there is less faeces for flies to breed in. However, it is imperative that latrines are
hygienically used and that the faeces of all household members are disposed of in this latrine.
The evidence that face washing is important in interrupting transmission of trachoma comes from a limited number
of studies of varying quality [13, 14]. Outcomes are commonly measured by self-report. If social desirability bias
causes good face washing / facial cleanliness to be over-reported it would affect the apparent relationship between
face washing and risk of trachoma. An alternative measure, such as observation of whether or not a face is clean can
also be subjective: some have argued that certain indicators (presence of discharge and flies on the face) are better
than others (presence of dust and food) [15, 16]. It is also important to note that use of water for laundry and
hygiene purposes is directly related to the quantity of water available in the home [17], so face and clothes washing
is physically constrained in areas of extreme water scarcity.
Overcrowding, particularly while sleeping, is also considered a risk factor for transmission [18], but the evidence is
largely historical i.e. from the USA and UK [19] and may be confounded by poverty and larger households having a
greater number of young children [2]. Reducing overcrowding is not considered in the SAFE strategy, but it may have
been overlooked as a behavioural risk factor.
As the transmission dynamics of trachoma are not well understood there continues to be scientific debate about the
evidence-base for “F” and “E” interventions [20]. However, a recent systematic review (based on the findings of 11
of 15 meta-analyses) concluded that there is strong evidence that water, sanitation and hygiene interventions can

Page
8
reduce the odds of trachoma, particularly through face washing and improving sanitation access [14]. This review
considered evidence for the impact of water (distance; source; access; quantity for washing and total quantity,
sanitation (access; use; type; maintenance; education) and hygiene (face cleanliness; frequency of face washing;
ocular/ nasal discharge; soap use; hygiene education; towel use; bathing frequency; nose wiping and towel sharing)
on trachoma. As there is no single route of transmission and the contribution of different routes to transmission is
likely to vary in different settings, it is recognised that context-specific “F” and “E” interventions need to be
developed that are tailored to the potential risk factors for transmission in a specific setting.
Situation in Ethiopia (and Oromia) Ethiopia has the highest burden of trachoma globally with an estimated 1.2 million people affected with trachoma
trichiasis (TT) [21] and 76% of the population living in trachoma endemic areas [22]. Among its 90 million inhabitants
more than 80% live arid, rural areas and almost 40% of the nation’s population survive on less than a dollar a day
[23]. Water scarcity is a major challenge in Ethiopia, with many individuals having to travel a significant distance to
collect water and almost 50% of the population not having access to safe water [24]. Improved sanitation coverage is
also low nationally (27%) [24]. These environmental and living conditions create the ideal situation for trachoma to
prevail. Studies have estimated the prevalence of active trachoma (measured among children 1-9 years old) to be
40%, although this was found to be up to four-fold higher in rural areas [25]. The national prevalence of TT
(measured in those 15 years and older) is estimated to be over 3%, amounting to 1.3 million people [25]. Data from
the Global Trachoma Mapping Project-GTMP (from 2012 to 2014) suggest 78 million people are at risk of trachoma.
Like other nations, Ethiopia is working towards eliminating trachoma by 2020. The country began implementing the
SAFE strategy as part of national policy in 2003. Specifically this has included the provision of improved trichiasis
surgery, the mass administration of azithromycin, and the distribution of public health messages by radio, video, and
printed materials [26]. To date the evidence around the “F” and “E” components remains uncertain. Studies
undertaken in Ethiopia suggest that even though people were widely exposed to the health education messages,
there was little change in their behavioural practice as a consequence [26]. To date there has been little targeted
formative research to understand the factors that drive the hygiene and sanitation related behaviours that are likely
to be associated with trachoma transmission in this context and as such this has been a limitation for the effective
design of sustainable trachoma interventions.
Study rationale Globally, evidence around the “F” and “E” components of the SAFE strategy is lacking, which in turn has limited the
effective design of trachoma elimination programs in countries like Ethiopia. Knowledge of trachoma and its
transmission pathways has also been found to be insufficient to lead to sustained behaviour change. The absence of
a solid evidence base around these personal hygiene and environmental risk factors is likely to significantly impede
progress towards the GET target of 2020. This research adopted an exploratory approach in order to understand the
array of sub-optimal hygiene and sanitation behaviours that may contribute to trachoma transmission in rural
settings where water is scarce, sanitation is low and resources are minimal.
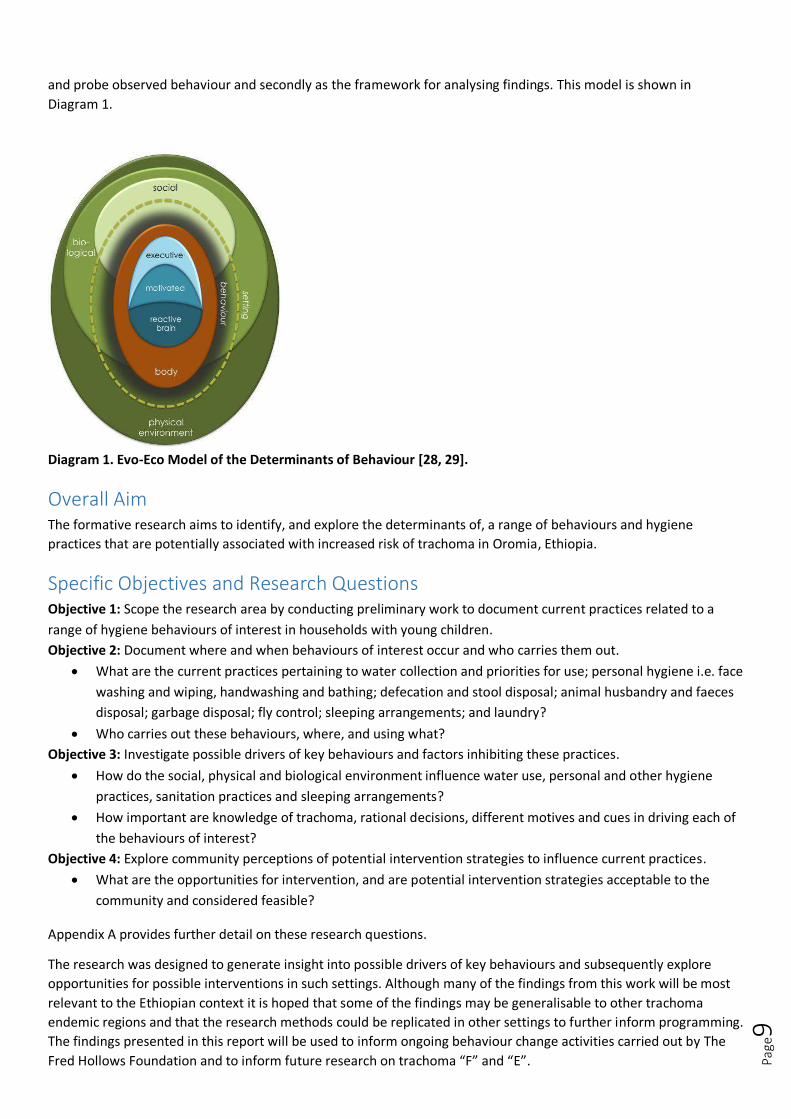
Conceptual framework This formative research was informed by Behaviour Centred Design (BCD) Approach. The approach sets out a theory
for the determinants of behaviour as well as a process for how to use these determinants to design behaviour
change interventions. The approach was developed by researchers at LSHTM (http://ehg.lshtm.ac.uk/behavior-
centred-design/) and has been applied to a range of public health issues in low and middle income settings. The BCD
approach is deemed appropriate for this study because it acknowledges that much of hygiene and sanitation
behaviour is not reliant on increasing health knowledge (which has been found to be high in most settings [27]) but
rather that it can be influenced by emotional drivers of behaviour. In the formative research stage the theory draws
on evolutionary and environmental psychology as well as best marketing practice to explore critical domains of
behaviour including cognitive processes, behavioural practice and the way individuals interact with their social and
physical environments. The Evo-Eco Model of the Determinants of Behaviour was used as a starting point to explore
Page
9
and probe observed behaviour and secondly as the framework for analysing findings. This model is shown in
Diagram 1.
Diagram 1. Evo-Eco Model of the Determinants of Behaviour [28, 29].
Overall Aim The formative research aims to identify, and explore the determinants of, a range of behaviours and hygiene
practices that are potentially associated with increased risk of trachoma in Oromia, Ethiopia.
Specific Objectives and Research Questions Objective 1: Scope the research area by conducting preliminary work to document current practices related to a
range of hygiene behaviours of interest in households with young children.
Objective 2: Document where and when behaviours of interest occur and who carries them out.
What are the current practices pertaining to water collection and priorities for use; personal hygiene i.e. face
washing and wiping, handwashing and bathing; defecation and stool disposal; animal husbandry and faeces
disposal; garbage disposal; fly control; sleeping arrangements; and laundry?
Who carries out these behaviours, where, and using what?
Objective 3: Investigate possible drivers of key behaviours and factors inhibiting these practices.
How do the social, physical and biological environment influence water use, personal and other hygiene
practices, sanitation practices and sleeping arrangements?
How important are knowledge of trachoma, rational decisions, different motives and cues in driving each of
the behaviours of interest?
Objective 4: Explore community perceptions of potential intervention strategies to influence current practices.
What are the opportunities for intervention, and are potential intervention strategies acceptable to the
community and considered feasible?
Appendix A provides further detail on these research questions.
The research was designed to generate insight into possible drivers of key behaviours and subsequently explore
opportunities for possible interventions in such settings. Although many of the findings from this work will be most
relevant to the Ethiopian context it is hoped that some of the findings may be generalisable to other trachoma
endemic regions and that the research methods could be replicated in other settings to further inform programming.
The findings presented in this report will be used to inform ongoing behaviour change activities carried out by The
Fred Hollows Foundation and to inform future research on trachoma “F” and “E”.

Page
10
METHODS Study design and setting A formative research study was carried out in the North Shewa Zone in Oromia. Fred Hollows Foundation Ethiopia is
currently working in this region. Data were collected from five communities in an area with high prevalence of active
trachoma near Gerbe Guracha, rural town with an active trachoma prevalence (TF) of 49.9% in children 1-9 years of
age (result of Global Trachoma Mapping Project in Oromia conducted 2012-2014); a rate which is much higher than
the cut-off level of TF 10% set to determine public health significance at district level warranting an immediate 5-
year implementation of SAFE. Study communities were selected on the advice of the NTD Focal Person working at
the District Government level. Communities were purposively selected to reflect variations in geography, sanitation
coverage and access to water.
Study population The study was targeted to investigate practices in households with young children. Wherever possible, a caregiver
with a child below three years-of-age was selected as they are most at risk of active trachoma and the actions of
their caregivers are key contributors to their high-risk status. Where possible selected households also had older,
school-going children. This was done to observe interactions between siblings as this is thought to also be key for
trachoma transmission. In some villages households with a household member with trichiasis were selected. The
socio-economic status of the households was also considered at the time of selection to ensure the sample
represented a diverse range of lifestyles in these communities.
Data collection There are challenges in investigating privately-conducted and sensitive hygiene behaviours. Qualitative research
methods were selected for this study with the aim of creating an in-depth understanding of actual practices in
different settings rather than conducting a representative quantitative survey. The latter would have generated large
amounts of data based on self-reported practices which rarely reflect actual behaviour. The methods used are
summarised in Table 1 and subsequently described in turn. In all communities the Kebele leader was first
approached for permission to conduct the study.
Table 1. Summary of methods used to investigate the research questions.
Objective Research questions Method Quantity Details
1,2,3 Obj 2: What are the current practices pertaining to water collection and priorities for use; personal hygiene i.e. face washing and wiping, handwashing and bathing; defecation and stool disposal; animal husbandry and faeces disposal; garbage disposal; fly control; sleeping arrangements; and laundry? Obj 2: Who carries out these behaviours, where, and using what? Obj 3: How do the social, physical and biological environment influence water use, personal and other hygiene practices, sanitation practices and sleeping arrangements? Obj 3: How important are knowledge of trachoma, rational decisions, different motives and cues in driving each of the behaviours of interest? Obj 4: Are potential intervention strategies acceptable to the community and considered feasible?
Household observations
10 Five different communities HHs with (ideally) a child under 3 years-of-age
2,3 Interviews with caregivers
10 Following observation
2,3,4 Focus group discussions
5 Mothers of children under 3: Sleeping arrangements and laundry Face washing and bathing Garbage, flies, sanitation and handwashing Grandmothers on perceptions of blindness, trachoma, disgust Fathers on community structure, touch points, roles of men and women and decision-making and trachoma knowledge
4 Key informant interviews
4 Health Extension Worker School Teacher in a School with a Trachoma Club Kebele Leader NTD Focal Person (District level Government)

Page
11
Observation and interviews Households with at least one child under 9 years of age, and preferably under 3 years-of-age were identified through
discussion with the Health Extension Worker in the study communities and through a random walk through the
village. Two non-neighbouring households were selected in each community. Eligible households were identified on
the morning of the study to prevent caregivers from cleaning their homes and otherwise altering their natural
environment in preparation for this visit.
On the first day of data collection, the observation was unstructured and lasted for the majority of the day (from
dawn until 3pm). Thereafter a shorter observation period was selected (dawn until midday) to allow for other
activities to be conducted in the afternoon when less activity was observed in the households. As many behaviours
and aspects of daily life were studied, notes were taken on all activities conducted during the observation period.
Data were collected on the following activities of interest for trachoma elimination: water availability; defecation
and stool disposal; waste disposal; presence of flies; location of animals; sleeping patterns; personal hygiene, and
water use behaviours including hand washing, face washing (and wiping), bathing and domestic activities. Photos
were used to capture behaviour in context, and video was taken to help understand sequences of behaviour.
Following observation, female primary caregivers in each household were interviewed to aid understanding of the
observed behaviour and to explore potential determinants of key behaviours. At the end of these interviews a brief
survey was conducted to record basic socio-demographic information, sanitation facilities and the cleanliness of the
environment.
Participants were given a compact mirror, some soap and some coffee to compensate them for their time.
Focus group discussions
The first focus group discussions were held after four households had been observed so that the content of the focus
groups could be adapted to reflect issues that had come up during the observations. The focus groups were designed
to further explore drivers of behaviour, explore perceived norms and to discuss potential opportunities for change
and intervention strategies. Focus groups were held with similar individuals (age and gender) and the size was kept
small (approximately 5-6 individuals per group) to encourage active participation. Three focus groups were held with
mothers of children under three, each exploring different behaviours and potential solutions (see topic guides in
Appendix C). Focus groups were also held with grandmothers and with male heads-of-household to explore
knowledge on trachoma and other perceptions and normative practices in the community. Each focus group
involved interactive activities and props to help keep attention and engage participants (most of whom were
illiterate). Participants were provided with refreshments and snacks.
Stakeholder interviews
On the final day of data collection select key stakeholders were interviewed to help fill in gaps surrounding identified
practices, community structures, and control strategies.
Data handling and analysis A debrief meeting was held at the end of each day of field work to discuss observations and revise topic guides for
interviews and focus groups for the next day. Data from the observations were recorded in field notes (Appendix B).
Data from focus group discussions and individual interviews were voice-recorded and transcribed. Simultaneous
translations were also provided during field work by the local field workers and the field coordinator so that
interviews could effectively probe on participant responses. Socio-economic demographics and water and sanitation
facilities from each of the participating households were entered into an MS Excel spreadsheet and summarised.
Data were thematically analysed by behaviour, following the six-step method put forward by Braun and Clarke [30].
Behaviour Centred Design (BCD) theory was used as a framework to help guide the data analysis and interpretation
process. BCD presents a model of behavioural determinants which can be used as a checklist [31] to evaluate the
influence of factors in the brain, body and environment on the target behaviours. This framework was used as a
deductive ‘top down’ coding system [32] for the thematic analysis. Examples of quotes and observations were

Page
12
selected to exemplify each theme. Note that a limited number of quotations have been selected due to the low
quality of the transcription.
Ethics and consenting The research protocol was approved in Ethiopia by the Oromia Regional Health Bureau research ethics review board
and by the London School of Hygiene and Tropical Medicine Ethics Committee.
Information sheets and consent forms were prepared in English and Afaan Oromoo and were explained verbally to
participants in either Afan Oromoo or Amharic as necessary. Informed written consent was obtained for each
individual household member aged 18 years or over. Informed written consent of the parent or guardian was
obtained for all household members aged less than 18 years. Informed written assent was also obtained for all
household members aged 7 – 17 years. For householders aged 14-17 years this was on the basis of the same
information provided for written consent (i.e. they also signed the informed consent form). A simplified version of
this form was provided for householders aged 7-14 years. Consent was almost always given by a witnessed thumb
print from the participant. It was not always possible to identify a literate witness. No names or household identifiers
were recorded.
Consent forms for group discussions explained the rules of the discussion and confidentially. This information was
also explained verbally.
An additional part of the consent form was used to seek permission for the use of photos and videos and with
regards to how these images and footage could be used. Verbal permission was also sought again prior to the taking
of the first images or footage.
Training Two young, female field workers / translators were selected to assist with the field work following interviews with
short-listed individuals provided by Berhan Consulting. They were oriented on the study before it started and trained
on the methods as they worked alongside the LSHTM researchers. The study was facilitated by a FHF Ethiopia staff
member (Nazif Jemal) who worked with the District Government NTD Focal person and with Health Extension
Workers in each community to help recruit households and set up focus groups and interviews.

Page
13
RESULTS Reporting framework Objective 1 (orientation) is not reported on separately. The results pertaining to Objectives 2, 3 and 4 are presented
for each behaviour in turn. Current practices are described and factors influencing these practices are summarised
according to what was discovered about the potential determinants of behaviour. Other relevant factors, such as
community perceptions of trachoma, are presented and potential intervention strategies to address each behaviour
are then discussed.
Data were collected during the period from Wednesday 13th January to Friday 22nd January, 2016.
Setting and participants The study area was rural, with some communities inaccessible by road. The study area was on the border of Oromia
and Amhara, resulting in both Oromeefa or Amharic being spoken by participants in this study. All participants were
Christian in this study, with the majority following the Coptic Orthodox religion which dominates this area. All
households kept animals within their compound and had land for farming. Compounds were clearly demarcated
with fences and had a variety of set-ups which typically included one or more houses where people slept and other
building(s) where animals were kept (Figure 1). This household set-up makes it quite difficult to observe what your
neighbours are doing. However, people do socialise over the fence if they are close enough and neighbours come
visiting to ask for some embers to start their fire, to borrow food and household items and to drink coffee, the main
social pastime.
Figure 1. Study setting: rural, well-kept compounds.
Some kitchens were located in separate buildings and others were in the main living / sleeping hut and poorly
ventilated (Figure 2). Animals were also brought into the main living areas / kitchens at night.
Figure 2. Kitchen in a separate building where animals were also kept at night.
Communities differed with respect to power supply and latrine coverage (Table 2). All participants were married
(one polygynously), illiterate, and used cow dung and wood for fuel. The majority of homes had soap.

Page
14
Table 2. Characteristics of households and caregivers participating in the household observation and interviews
Community A Community B Community C Community D Community E
HH ID 1 2 3 4 5 6 7 8 9 10
HH size 9 5 5 4 8 8 7 7 9 6
No. children 5-17 yrs 3 2 3 1 4 5 3 4 4 2
No. children <5 yrs 0 1 0 1 2 1 0 1 2 1
Estimated vol. water person-1 day-1
19L 15L 15L 19L 8L 9L 17L 6L 8L 13L
Latrine No No No Yes (not in use) Yes Yes Yes Yes No No
Human faeces in compound
Yes Yes Yes No No No Yes Yes No (?) Yes
Soap Yes No (just dishes) Yes Yes Yes Yes Yes No Yes Yes
Education level None None (?) None None None Some 1° None None None None
Radio No Yes No No Yes No Yes No No Yes
Electricity Yes (just
light, rarely power)
Yes No No Yes Yes Yes (just light, rarely power)
No No No
Mobile Yes Yes No Yes Yes Yes (2) Yes Yes Yes Yes (3)
Animals Cows,
chickens 2 Cows, 2 donkeys 4 Cows, chickens
2 donkeys; 60 chickens; 30 goats; 2 ox; 1
cow
1 bull, 1 donkey, chickens
2 cows, 3 sheep, 2 donkeys
4 cows, 2 calves, 2
donkeys, 6 sheep and chickens
1 ox, 1 donkey, 6
sheep, chickens
4 cows, 2 calves, 9 sheep,
chickens
4 cows, 2 donkeys, 4
sheep 2 chickens
Location of animals Alongside*
house Alongside house Alongside house Alongside house
Alongside house
Alongside house
Inside kitchen (except cattle)
Alongside house
Calves & sheep inside
house
Alongside house
* Alongside house = adjacent to the home in another shelter.
1. Water
Availability Even in the same village, where households under observation were a few minutes apart, different sources of water
were often chosen. Decisions about where to source water from were made based on availability of alternative
options, cost, reliability of the water flow, time spent queuing and distance from the home. Water is often collected
from more than one source (Figure 3). For example, one household paid for water monthly (2 Birr), but they also
obtained water at additional cost (0.25 Birr per jerry can) from an alternative source that is further away but more
reliable. Although water points were rarely more than 15 minutes’ walk away, water collection could easily take
upwards of an hour, due to the need to queue and, often, low water pressure at the taps / pump. Water points were
reported to be shared by 30 households but in practice appeared to be used by more than this.
In one household a male child used a donkey to collect water, while in another an 18-year-old male collected water.
However, in general female family members were responsible for water collection.
Figure 3. Example of main sources of water in the study communities
Rivers / unprotected springs (e.g. HH8) Water points could be close by but were often associated with very long queue (e.g. HH5)

Page
15
Only three of the 10 households transferred water to other containers for storage. Even in these households, water
was still primarily used directly from the jerry cans it had been collected in. All water that has been collected tends
to be used during the course of the day, with little water remaining in a household overnight. Consequently, water
collection is one of the first activities of the day. Reported information on water collection, coupled with observed
water collection data, suggests that between 6 and 19 litres of water were available for use per person per day. The
amount of water collected did not appear to increase greatly in households with more people and livestock. Water is
used on domestic activities as well as for drinking and sanitary and hygiene-related tasks. As households also had
livestock, the amount of water available should be considered to be somewhat less than this. Lack of water was not
reported to be a significant problem in this season. Householders were seen to undertake activities which were
reportedly restricted when less water is available (e.g. laundry). Nevertheless, observations revealed that water was
used quite conservatively (particularly for dishwashing and laundry). People were also chastised for wasting water.
Use
The main use of water – other than personal hygiene (see face washing section) and drinking – was for cooking-
related activities. If a household cannot get enough water, cooking is the first priority. During observation all
households were seen to use water for cooking and washing dishes. Dish washing was done carefully: items were
washed as needed and using little water (water was poured from one cup or pot into another). Soap and rags were
sometimes used. The bucket and items used to prepare enjera (staple food) were carefully washed as well.
Other uses of water were, in order of the number of households they were observed in:
Giving animals water (n=6)
Making coffee and cleaning coffee cups and pots (n=5)
Relaying the floor with cow dung and water (n=5)
Washing clothes (n=3)
Watering banana plants (n=2)
Re-laying the floor of the houses with cow dung took quite a lot of water (e.g. 20-30L) as did washing clothing (35L in
the household that washed many items). Additional water is collected on days when laundry is done from home,
although because laundry takes a lot of water it is often done from the river instead (see laundry section for more
detail).
Hands were not always washed immediately after working with cow dung. Often when they were washed it was with
water and no soap. As the jerry can is used throughout this process, dung is often on the mouth of the container
(Figure 4) and hence jerry cans were observed to be thoroughly rinsed at water points.
Figure 4. Re-laying the floor of a house with cow dung.
Coffee ceremonies took place in half of the households during the observation period. Making coffee requires water
to wash the beans, to clean the coffee pot, cups and coffee table (sometimes more than once) and to make the
coffee itself. Making coffee also takes considerable time – well over an hour - from start to finish, as beans are

Page
16
roasted and ground each time coffee is made. This was the one activity where family did not appear to skimp on the
amount of water used.
Reuse
Water given to animals is often reused from washing dishes or even bathing. Sometimes this water is soapy,
although in focus groups participants were adamant that soapy water cannot be given to animals.
It was even remarked that it is “forbidden” to reuse bath water for other people, and the only observed reuse of
water from bathing involved washing baby clothing in the water that had just been used to bathe that baby.
Factors affecting availability and use
The quantity of water available and therefore the activities which are conducted was reported to vary according to:
Season (which also affects the water source and the time spent collecting water, as well as the quantity
collected)
Presence of guests
Occurrence of celebrations and other special events
The need to do laundry
The number of people and animals in a household at a given time point
During celebration days additional water is required for cooking more food, washing clothing, bathing, and – most
importantly – preparing alcohol.
2. Cleanliness of faces
Frequency of face washing and bathing
Infants and babies
Parents treat the personal hygiene of children under 2 quite differently to children 3 and up. Among this lower age
group, children are rarely put down, they are normally bathed every morning and night and have their faces washed
or wiped as needed during the day. Children of this age are normally bathed inside the house with cold water. Faces
were washed thoroughly in all bathing episodes observed. Children are normally wrapped in large cotton wraps or
more modern baby blankets and dried. Towels were not used at all. In some families, mothers were observed to use
vaseline on the baby’s skin after bathing.
Figure 5. Mothers giving their babies a full bath in the morning inside the house. The mother on the left does not
use soap during bathing. The picture in the middle shows a mother thoroughly cleaning her child’s eyes while
bathing. The picture on the right shows a mother applying vaseline to her baby’s face, older children do the same.
Page
17
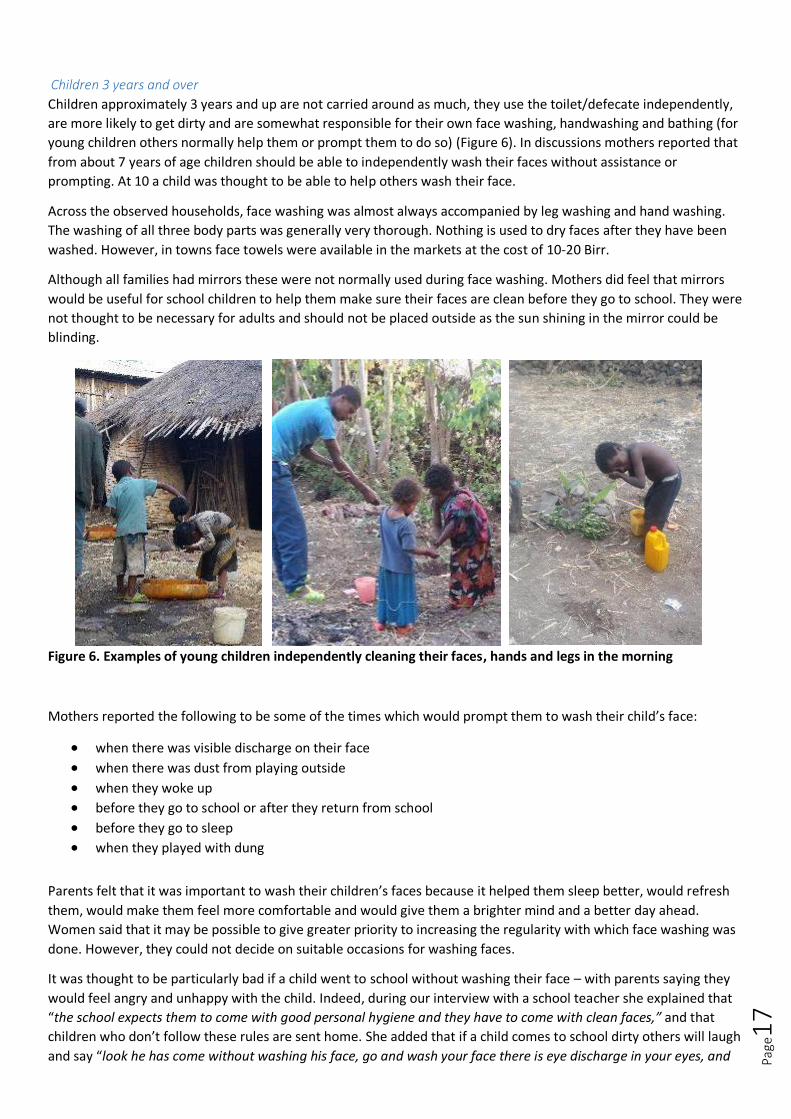
Children 3 years and over
Children approximately 3 years and up are not carried around as much, they use the toilet/defecate independently,
are more likely to get dirty and are somewhat responsible for their own face washing, handwashing and bathing (for
young children others normally help them or prompt them to do so) (Figure 6). In discussions mothers reported that
from about 7 years of age children should be able to independently wash their faces without assistance or
prompting. At 10 a child was thought to be able to help others wash their face.
Across the observed households, face washing was almost always accompanied by leg washing and hand washing.
The washing of all three body parts was generally very thorough. Nothing is used to dry faces after they have been
washed. However, in towns face towels were available in the markets at the cost of 10-20 Birr.
Although all families had mirrors these were not normally used during face washing. Mothers did feel that mirrors
would be useful for school children to help them make sure their faces are clean before they go to school. They were
not thought to be necessary for adults and should not be placed outside as the sun shining in the mirror could be
blinding.
Figure 6. Examples of young children independently cleaning their faces, hands and legs in the morning
Mothers reported the following to be some of the times which would prompt them to wash their child’s face:
when there was visible discharge on their face
when there was dust from playing outside
when they woke up before they go to school or after they return from school
before they go to sleep when they played with dung
Parents felt that it was important to wash their children’s faces because it helped them sleep better, would refresh
them, would make them feel more comfortable and would give them a brighter mind and a better day ahead.
Women said that it may be possible to give greater priority to increasing the regularity with which face washing was
done. However, they could not decide on suitable occasions for washing faces.
It was thought to be particularly bad if a child went to school without washing their face – with parents saying they
would feel angry and unhappy with the child. Indeed, during our interview with a school teacher she explained that
“the school expects them to come with good personal hygiene and they have to come with clean faces,” and that
children who don’t follow these rules are sent home. She added that if a child comes to school dirty others will laugh
and say “look he has come without washing his face, go and wash your face there is eye discharge in your eyes, and
Page
18
that kinds of thing.” Some mothers felt that if other parents noticed that their child had a dirty face they might say
that they were a bad mother or gossip about them. They explained that they would not like their own child to play
with a child with a dirty face as it attracted flies and their child could get diseases from them. The NTD
representative at the district level explained that despite their work establishing trachoma clubs at schools, they had
faced challenges translating knowledge on face washing into practice:
“Generally the students know [to wash faces]. There are some good things, but in the rural area we are
not doing very well in increasing facial cleanliness, because they are so busy…. we can give health
education… we are doing that, but we lack the action that is the problem, that is what we have to
target”.
The importance of being clean for school was also cited as the rationale for why school age children were reported
to always take a full bath at least once a week. For older children and adolescents bathing happens outside, within
the compound using cold water or in the river if the child is still quite young or if they are male.
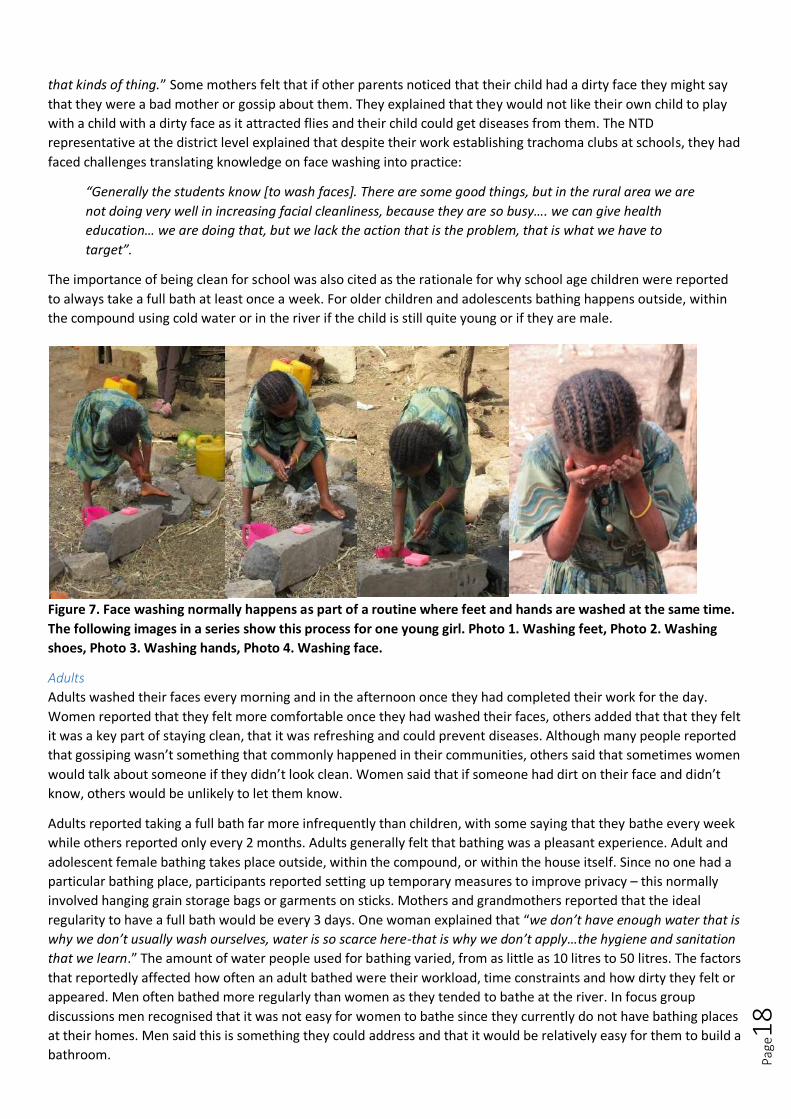
Figure 7. Face washing normally happens as part of a routine where feet and hands are washed at the same time.
The following images in a series show this process for one young girl. Photo 1. Washing feet, Photo 2. Washing
shoes, Photo 3. Washing hands, Photo 4. Washing face.
Adults
Adults washed their faces every morning and in the afternoon once they had completed their work for the day.
Women reported that they felt more comfortable once they had washed their faces, others added that that they felt
it was a key part of staying clean, that it was refreshing and could prevent diseases. Although many people reported
that gossiping wasn’t something that commonly happened in their communities, others said that sometimes women
would talk about someone if they didn’t look clean. Women said that if someone had dirt on their face and didn’t
know, others would be unlikely to let them know.
Adults reported taking a full bath far more infrequently than children, with some saying that they bathe every week
while others reported only every 2 months. Adults generally felt that bathing was a pleasant experience. Adult and
adolescent female bathing takes place outside, within the compound, or within the house itself. Since no one had a
particular bathing place, participants reported setting up temporary measures to improve privacy – this normally
involved hanging grain storage bags or garments on sticks. Mothers and grandmothers reported that the ideal
regularity to have a full bath would be every 3 days. One woman explained that “we don’t have enough water that is
why we don’t usually wash ourselves, water is so scarce here-that is why we don’t apply…the hygiene and sanitation
that we learn.” The amount of water people used for bathing varied, from as little as 10 litres to 50 litres. The factors
that reportedly affected how often an adult bathed were their workload, time constraints and how dirty they felt or
appeared. Men often bathed more regularly than women as they tended to bathe at the river. In focus group
discussions men recognised that it was not easy for women to bathe since they currently do not have bathing places
at their homes. Men said this is something they could address and that it would be relatively easy for them to build a
bathroom.

Page
19
Soap use
All but one of the families used soap to bathe their young children. Older children were always observed to use soap
for washing their hands, feet and faces. Sometimes younger children (eg under 12 years) were observed to not use
soap or only use soap to wash their hair, hands and faces. In discussions mothers reported that sometimes the
purpose of washing their child’s face was just to refresh them and in these cases soap was not used. Generally the
soap that was used for face washing and bathing was shared among the whole family. However, in one family almost
all individuals had their own soap while in another there was one soap demarcated for the baby while the rest of the
family shared one bar. Mostly families had special bathing soaps that they used. There were two families which were
observed to use liquid soap or shampoo for bathing.
Water use
Mothers did not perceive face washing to use a lot of water. However, in one house we did observe a mother
discipline her children for using too much water in cleaning their faces, hands and feet. Mothers reported that the
lack of water never created a barrier for face washing as water was prioritised for this purpose.
Face washing was always done so that the water just fell on the ground (as opposed to into a container). In general
people felt that water you had washed your face with was dirty and could spread disease, therefore it should not be
reused. We did not observe any cases of face washing water being reused.
3. Face wiping Mothers (or other family members that share a role in caring for children), wipe their child’s faces relatively
infrequently. That is to say that children are often left with discharge on their faces for a long period of time before it
is cleaned. This suggests that the presence of discharge alone is not normally sufficient to trigger the desired face
cleaning behaviour. In total only 3 cases of face wiping were observed. Of those observed, mothers either used a
child’s garment (one that was not being worn) or used their fingers. Mothers said they would only use their fingers
to wipe the child if they were clean (eg not when they are out in the field). In focus groups mothers reported that if
their children are with them in the field then sometimes they would use the bottom of their dresses to wipe the
child’s face.
Despite this, nasal and eye discharge is seen as something that is disgusting. In a focus group discussion we asked
participants to rank the following things according to how disgusting they were: Cow dung, blood, nasal discharge,
eye discharge, dirty bath water, dirt under nails, rotting meat and human faeces. This ranking is shown in Figure 8.
Participants said that rotting meat, human faeces and blood were more disgusting than nasal and eye discharge.
Nasal discharge was considered more disgusting than eye discharge. Both nasal and eye discharged were grouped
together in the middle of the disgust spectrum along with blood, dirty bath water and dirt under nails. When we
asked about this grouping of things participants explained that all of the things in the middle could easily be washed
clean with water.
Dirty bath
water
Dirt under
nails
Blood
Eye discharge
Nasal
discharge
Rotting
meat
Cow dung Human faeces
Things that can easily be
washed clean with
water.
Most
disgusting
Least
disgusting
Page
20
Figure 8. Ranking of things according to their level of disgust
During some of the focus group discussions we gave mothers disposable face wipes to try. Mothers appeared to like
them. They were surprised by how much dirt was removed by the wipes and they found them refreshing. They said
that they would feel comfortable throwing them away after just one use and would be willing to pay 10-20 Birr for a
small container (about 2 months worth) of face wipes. It is unlikely that locally available face wipes are
biodegradable.
Mothers were familiar with the tippy tap design. This was suggested as something that could aid in face washing and
reduce the amount of water used. Mothers did not appear to think that this would make a big difference to face
washing practice, possibly because they weren’t very concerned about how much water it uses in the first place.
Mothers reported that it would be difficult to keep soap outside as they thought it would be taken by birds.
Determinants of bathing practices and face washing described in the text are shown in Tables 3 and 4, respectively
according to the categories of the Evo-Eco Model.
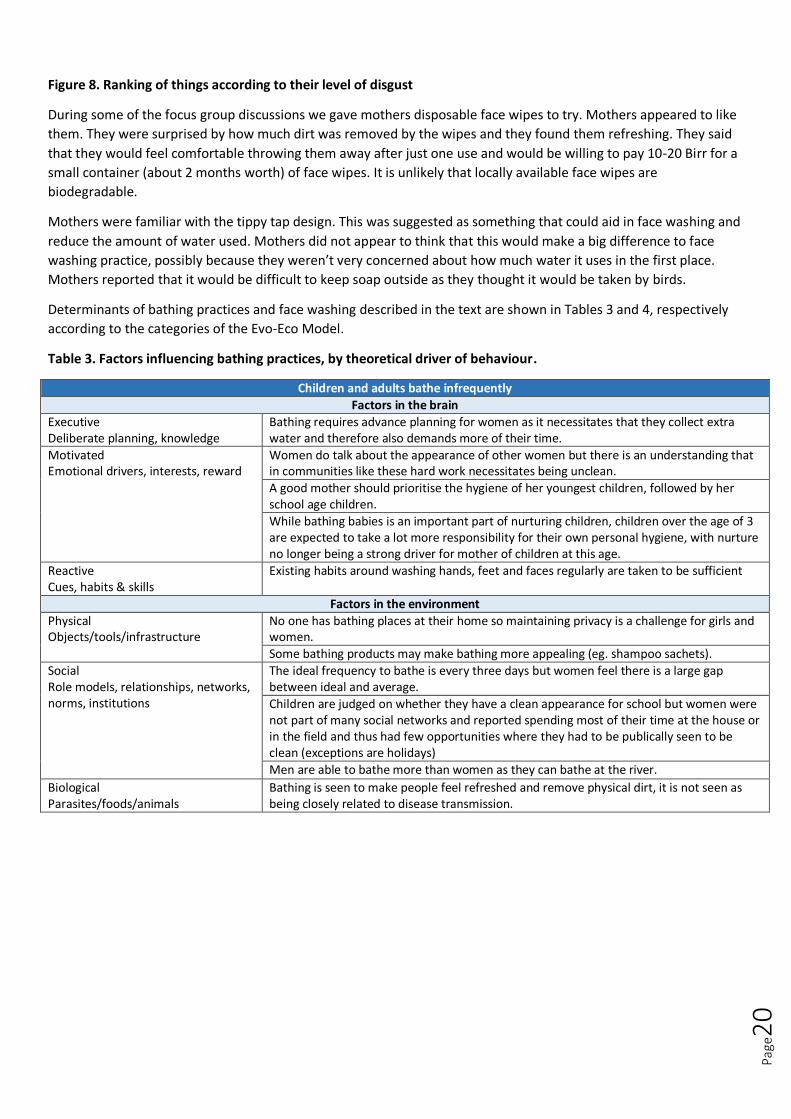
Table 3. Factors influencing bathing practices, by theoretical driver of behaviour.
Children and adults bathe infrequently
Factors in the brain
Executive Deliberate planning, knowledge
Bathing requires advance planning for women as it necessitates that they collect extra water and therefore also demands more of their time.
Motivated Emotional drivers, interests, reward
Women do talk about the appearance of other women but there is an understanding that in communities like these hard work necessitates being unclean.
A good mother should prioritise the hygiene of her youngest children, followed by her school age children.
While bathing babies is an important part of nurturing children, children over the age of 3 are expected to take a lot more responsibility for their own personal hygiene, with nurture no longer being a strong driver for mother of children at this age.
Reactive Cues, habits & skills
Existing habits around washing hands, feet and faces regularly are taken to be sufficient
Factors in the environment
Physical Objects/tools/infrastructure
No one has bathing places at their home so maintaining privacy is a challenge for girls and women.
Some bathing products may make bathing more appealing (eg. shampoo sachets).
Social Role models, relationships, networks, norms, institutions
The ideal frequency to bathe is every three days but women feel there is a large gap between ideal and average.
Children are judged on whether they have a clean appearance for school but women were not part of many social networks and reported spending most of their time at the house or in the field and thus had few opportunities where they had to be publically seen to be clean (exceptions are holidays)
Men are able to bathe more than women as they can bathe at the river.
Biological Parasites/foods/animals
Bathing is seen to make people feel refreshed and remove physical dirt, it is not seen as being closely related to disease transmission.

Page
21
Table 4. Factors influencing facial cleanliness, by theoretical driver of behaviour.
Children’s faces are not washed or wiped regularly
Factors in the brain
Executive Deliberate planning, knowledge
People associated unclean faces with disease transmission.
Water is prioritised for face washing
Motivated Emotional drivers, interests, reward
Washing a child’s face is seen as refreshing and can make children more comfortable and ‘give them a brighter mind’.
Reactive Cues, habits & skills
The presence of discharge, sniffing or sneezing do not act as cues for family members to wipe or wash a child’s face. The presence of food or other dirt on faces often does cue the target behaviour.
Face washing is done as a part of daily routines rather in response to cues and is often done in conjunction with hand and feet washing.
The presence of a lot of flies does sometimes act as a cue for washing or wiping a child’s face.
Factors in the environment
Physical Objects/tools/infrastructure
No special objects are used for face washing or wiping. The same water container and soap that is used for feet and handwashing is used for face washing.
Mothers wipe children’s faces with either an item of the child’s clothing, their own clothing or their hands. But feel that none of these items are suitably clean for the task.
Social Role models, relationships, networks, norms, institutions
Face washing and wiping is currently done by mothers. However, siblings spend a lot of time caring for young children and are in a good position to aid with face wiping or washing.
A well-mannered child is seen as one who is able to manage their own personal hygiene.
Face washing is something that family members often help each other with. Eg. a daughter may pour water for her father or siblings may pour water for each other.
Biological Parasites/foods/animals
People feel that dirty faces attract flies and worry that flies landing on faces can spread disease. Face washing is therefore seen to reduce flies. Faces of young children are washed to remove food or other physical dirt, but not discharge.
4. Handwashing Handwashing is almost always done outside the house. Normally people use an area with a few stones to rest the
soap and water on. Women reported that handwashing should also take place at the following times: early in the
morning when you wake up, after cleaning the house, when eating (unclear if this meant before or after), when
cooking, after touching things that are perceived to be dirty and after cleaning up animal faeces. Washing hands with
soap was considered important whenever you have something that is sticky or difficult to remove from hands.
No handwashing was observed after wiping a child’s face. However, mothers reported that they knew that they
should wash hands with soap after wiping a child’s face in order to be truly clean. One woman explained this point:
“we usually wipe by our hands and put [the discharge they wiped from the child’s face] on the ground, because we
are in rural area but is not enough to be clean.”
Handwashing commonly precedes face washing. One woman was observed to always wash her child’s hands after
eating and then wash their faces. She explained that this was because they had spices and oils from eating on their
faces.

Page
22
Figure 9. Left - A mother washes her child’s hands before eating, Centre – a woman requests a neighbour to pour
water for her after returning from defecation, Right – a mother washes her hands with water only after re-laying
the floor with cow dung.
Table 5. Factors influencing handwashing practices, by theoretical driver of behaviour.
Hands are not washed after wiping discharge from a child’s face
Factors in the brain
Executive Deliberate planning, knowledge
Women know the ideal behaviour but have accepted that this is not attainable for people like them.
The trigger for the behaviour (the presence of discharge) is either constant or hard to predict.
Motivated Emotional drivers, interests, reward
Discharge is something that is disgusting but the discharge from a mothers own child is likely to be less disgusting to them.
Mothers tend to wipe or clean a child’s face when they see the presence of flies. This action seems to be borne out of a nurture motive and therefore it is possible their own hygiene is deprioritised.
Reactive Cues, habits & skills
If discharge is either constant or can occur at irregular intervals it is likely that mothers will often be busy doing other things and not be able to easily wash hands.
Mothers may on occasion wipe their child’s face subconsciously.
Factors in the environment
Physical Objects/tools/infrastructure
When they are in the field no water or soap are available.
Social Role models, relationships, networks, norms, institutions
Handwashing after face wiping is not a norm and is not socially noticed.
Parents and siblings are highly affectionate and often coming into contact with discharge on faces of young children.
Biological Parasites/foods/animals
Discharge was something that did not necessarily require soap use to be removed.
Page
23
5. Sanitation
Toilet availability and sanitation promotion Five households in three of the 5 Kebeles we visited had latrines. In the Kebeles where toilets were present people
informed us that the health extension workers had told them they must build toilets. They were also threatened that
if they were found defecating in the open they would be fined.
Health workers reportedly receive training on how to build toilets and this forms one of their major roles in
communities. However, they have 16 other health programs to deliver and often have limited capacity to visit all
households in their catchment area. Health workers do not appear to promote sanitation for reasons other than
health. A Kebele leader in one community explained that health workers told their community “that using toilet can
protect us from 8 communicable diseases.” The NTD Focal person also said that toilets were promoted by telling
people the health benefits. He also explained that the district was trying to deliver a Community-Led Total Sanitation
(CLTS)-style program “there is some program related to Trachoma ODF, at the District level by the support of FHF we
give training to HEWs and other health workers on how to trigger, post trigger, but that training is not working
properly.”
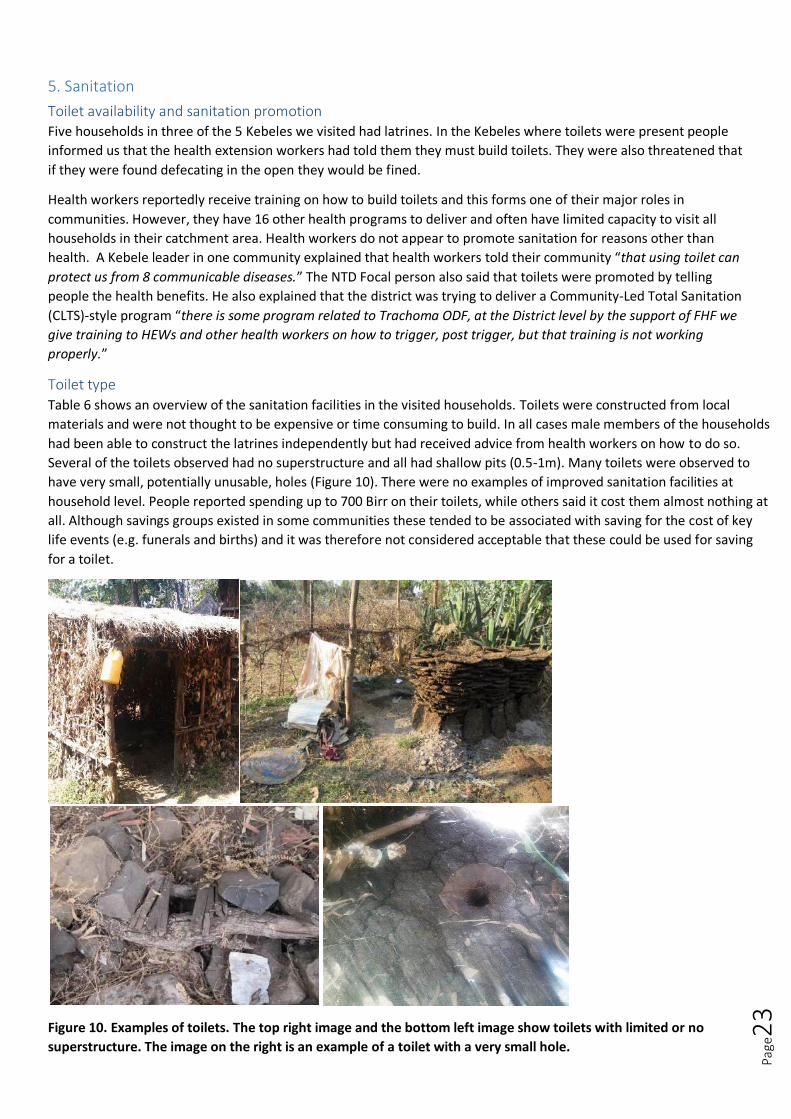
Toilet type
Table 6 shows an overview of the sanitation facilities in the visited households. Toilets were constructed from local
materials and were not thought to be expensive or time consuming to build. In all cases male members of the households
had been able to construct the latrines independently but had received advice from health workers on how to do so.
Several of the toilets observed had no superstructure and all had shallow pits (0.5-1m). Many toilets were observed to
have very small, potentially unusable, holes (Figure 10). There were no examples of improved sanitation facilities at
household level. People reported spending up to 700 Birr on their toilets, while others said it cost them almost nothing at
all. Although savings groups existed in some communities these tended to be associated with saving for the cost of key
life events (e.g. funerals and births) and it was therefore not considered acceptable that these could be used for saving
for a toilet.
Figure 10. Examples of toilets. The top right image and the bottom left image show toilets with limited or no
superstructure. The image on the right is an example of a toilet with a very small hole.

Page
24
Table 6. Sanitation facilities in the study households.
Household Number
Toilet present
Visible faeces in compound
Disposal of child faeces
Drop hole cover
Pit depth Size of hole Superstructure Likelihood toilet is used regularly
1 No Yes Unknown N/A N/A N/A N/A N/A
2 No Yes Inside compound with adult faeces
N/A N/A N/A N/A N/A
3 No Yes Left wherever it is N/A N/A N/A N/A N/A
4 Yes No Carried outside compound
No Shallow Ok None Moderate
5 Yes No Reportedly thrown in latrine
No Shallow Narrow & awkward
3 walls and a roof of straw, no door, faces the compound
Strong (but faeces around hole)
6 Yes No Unknown No Shallow Small Partial walls, including one which is a cow dung pile
Strong
7 Yes Yes Defecate outside compound and left in situ
No Shallow Very small 3 walls and a roof of straw, no door, outside compound
Moderate – was outside the compound in direction of defecation but hard to tell as so clean and hole so small
8 Yes Yes Left wherever it is No Shallow Ok None Poor (and no faeces seen)
9 No No Infants defecate in clothes which are ‘thrown away’
N/A N/A N/A N/A N/A
10 No Yes Swept up and disposed of in rubbish pile
N/A N/A N/A N/A N/A
VIP style latrines were present at the health centre and the school. However, in both cases the toilets were found to be
very poorly cared for with a lot of faeces around the hole and outside the toilet facility. No water or soap was available at
these locations.
Figure 11. The toilets at the school were not kept clean. To the right is supposed to be the handwashing place yet
there is no water and it is dirtied with human faeces.
Toilet use/lack of use
In some instances where there were toilets at household level, human faeces was still observed within the
compound (Table 6), indicating that toilets were not regularly used. Furthermore, faeces was found around the hole
in several of the toilets that were in use.

Page
25
The benefits of toilets were described as the following: they improve health, they provide privacy, they are easier (as
faeces is all in one place) and reduce smell within the compound and they are associated with people who are
modern and educated. In contrast others reported that the benefits of opening defecation were that you could use
the faeces for compost others and that toilets smelt worse than defecating in the open. Children were also reported
to prefer open defecation.
People tend to defecate first thing in the morning, when it is not fully light. When people go for open defecation
they take water with them in a container and collect leaves to wipe. Nothing is done to cover the faeces. However
women did report that this was something that would be acceptable to change saying that people could easily bury
their faeces with their hands. Hands are rinsed with the water near to the place of defecation. In some cases it was
observed that in addition to this hands were washed with soap upon returning to the house.
In focus groups mothers described that in cases where a family did not have a toilet, different family members would
defecate in different locations (Figure 12). In general adult men and women as well as teenagers were reported to
defecate outside the compound in a nearby field. Men and women would not normally go to the same nearby field
to defecate and often the places where they go rotate. It was reported to be acceptable for children under 5 to
defecate anywhere inside the compound. For children under two it was acceptable for them to defecate inside the
home. In both cases mothers should then move the faeces and put it outside the compound. Based on observation
child faeces was left for some hours before eventually being swept up and placed in the rubbish pile. In other
households it was clearly not swept up or moved at all. Human faeces and animal faeces are viewed in completely
different lights. Even though animal faeces may be all around a compound (Figure 13), it is not acceptable for an
adult to defecate indiscriminately within the compound.
Figure 12. Mock outline of a compound used during the focus group discussions to better understand where
people of different ages and genders open defecate
6. Animal faeces In all households animals were kept close to the house and consequently there was always a lot of animal faeces in
the compound. Animal faeces were also inside homes and kitchens in the households where animals were kept
inside overnight. Animal faeces were understood to be categorically different to human faeces as it served a useful
purpose (e.g., cow dung was used for fuel and re-laying the floor – see Water use section). Cow dung was gathered
up each morning for these purposes, but no action was observed to be taken to actively remove other animal dung

Page
26
from the compound other than general sweeping of the surroundings. During a focus group one woman even said
that because of this functionality “cow dung is not disgusting, it is pleasant even”. In contrast when asked about
human faeces the response from the same group of women was “wuuuuh! It is disgusting”.
Figure 13. The image below highlights the amount of faeces present in one compound. Animal faeces is highly
present and acceptable. Child faeces may be in the environment, but adult faeces should not be in the open.
Table 7. Factors influencing sanitation practices, by theoretical driver of behaviour.
Poor sanitation demand and toilet use
Factors in the brain
Executive Deliberate planning, knowledge
Toilets were only promoted as something beneficial to health and there is little knowledge of other benefits.
People were forced to build them rather than toilets being desirable
Motivated Emotional drivers, interests, reward
Some people said toilets were modern but this is not necessarily something people aspire to be.
Seen to be as comfortable and convenient to defecate in the open (people often go not too far from the house)
Although there are supposed to be fines for open defecating these are not enforced
Reactive Cues, habits & skills
People defecate when it is dark so privacy is not an issue
Toilets are often built without superstructures so there is less of a visible reminder about where people should defecate
Factors in the environment
Physical Objects/tools/infrastructure
Toilets are poorly designed and likely to collapse
Toilets are poorly cleaned with faeces often present, so they are not nice places to be
Social Role models, relationships, networks, norms, institutions
Toilets at health centres and schools are poorly maintained so these do not inspire people to have toilets or use them well.
Open defecation is still seen as a cultural and social norm and not frowned upon.
Biological Parasites/foods/animals
There is a lot of animal faeces in the environment
Human faeces is disgusting but still tolerated as a normal part of the environment
Faeces was not seen as the predominant reason for the presence of flies (rather they were seen to be most attracted to milk)

Page
27
7. Garbage
Cleanliness of home environment People’s homes were almost all well-ordered, with pegs and shelves built into the home in a purposeful way. Every
item had a clear place within the home, and on the whole, compounds were also organised and fenced off. Most had
one or more purpose-built structure to house grain and animals. The contrast in the cleanliness of the home
environment in HHs 7 & 8 - which both had family members reportedly suffering from TT – was notable (Figure 14).
Figure 14. The cleanliness of the home environment was noticeably worse in some households
Homes and compounds are swept several times a day. When asked what items they actively throw out / away, focus
group participants listed the following items:
Animal dung
Garbage that are cleaned from houses like papers
Dirty water
Children’s faeces
Action taken with these items is discussed in turn based on what was observed in the households.
Garbage disposal
Ash from the fire is moved to the edge of the compound or outside it. Sweepings from the home and compound are
put elsewhere, usually in one location or in several discrete piles at a distance from the home or outside the
compound perimeter (Figure 15). According to focus group participants, garbage should be disposed of at some
distance (15 to 18 steps demonstrated during an enactment) from the house and in particular away from the kitchen
to avoid smell, flies and young children touching it; in the households we observed, garbage was generally closer
than this to the house.
In one household, child stool was seen to be swept up when the compound was swept (so perhaps not deliberately
moved) and transferred to the same rubbish pile. Dirty water from cooking and cleaning was not always discarded in
one place, but was often added to the rubbish pile.
HH1 & HH2 were markedly more wealthy than other homes
Inside HH8. It was not very clean and children all had noticeable coughs. Some children had gone to live with other relatives for financial reasons.
Most homes had cupboards made from mud in the same way (HH3)
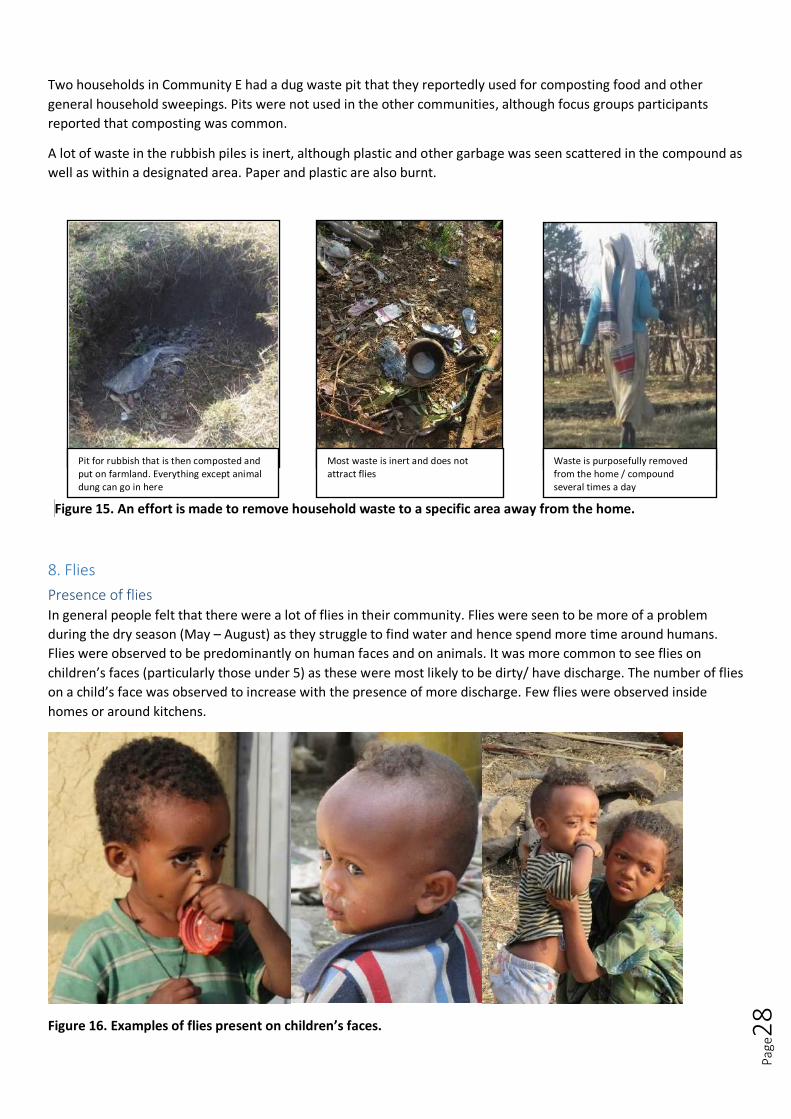
Page
28
Two households in Community E had a dug waste pit that they reportedly used for composting food and other
general household sweepings. Pits were not used in the other communities, although focus groups participants
reported that composting was common.
A lot of waste in the rubbish piles is inert, although plastic and other garbage was seen scattered in the compound as
well as within a designated area. Paper and plastic are also burnt.
Figure 15. An effort is made to remove household waste to a specific area away from the home.
8. Flies
Presence of flies In general people felt that there were a lot of flies in their community. Flies were seen to be more of a problem
during the dry season (May – August) as they struggle to find water and hence spend more time around humans.
Flies were observed to be predominantly on human faces and on animals. It was more common to see flies on
children’s faces (particularly those under 5) as these were most likely to be dirty/ have discharge. The number of flies
on a child’s face was observed to increase with the presence of more discharge. Few flies were observed inside
homes or around kitchens.
Figure 16. Examples of flies present on children’s faces.
Pit for rubbish that is then composted and put on farmland. Everything except animal dung can go in here
Most waste is inert and does not attract flies
Waste is purposefully removed from the home / compound several times a day

Page
29
Flies were observed to be predominantly active after about 9am when it began to get hot.
There was some disagreement between participants about whether flies are more numerous in the dry season or
the rainy season. Other than differences caused by the weather, the presence of flies was linked by participants to
dirt:
“Flies do not land on a clean thing, on a clean faces, so we have to clean our environment.” (Male
Focus Group Participant)
People felt that flies were attracted to fresh milk/milking (many people felt this was the only thing that attracted
flies), cattle, uncovered food (although generally we observed very vigilant food covering), when children get dirty,
open wounds, mud, children’s faeces, dead animals, the latrine and other places where there is a bad smell.
Interestingly, animal faeces, whether dry or fresh did not attract flies (Figure 17). As the garbage piles were largely
dry waste they did not appear to attract flies either.
Figure 17. Cow dung is present in all homes in large quantities but was not swarming with flies.
Factors influencing compound cleanliness From a trachoma perspective, the cleanliness of the home and environment is important because of flies. The
association between flies in the environment and behaviours related to these items is considered in Table 8.
Table 8. Factors affecting the presence of flies in the home environment
Flies are found in the home environment
Factors in the brain
Executive Incense / smoke is deliberately burnt to reduce flies in the home
Deliberate planning, knowledge
Knowledge of the role of flies in disease transmission (including trachoma) is relatively high, although not everyone is aware of how you can reduce flies or believes that you are able to do so
Motivated Items that smell bad are removed from the immediate home environment. Faeces recognised to draw flies Dirty children and faces thought to draw flies Flies in the environment are not particularly seen to be a nuisance, but flies on people, and especially children, are bothersome: "I don’t feel good when flies land on my child’s face"
Emotional drivers, interests, reward
Reactive Habitual sweeping of the house and compound occurs several times a day and can remove faeces and other waste from the immediate environment Cues, habits & skills
Factors in the environment
Physical Vaseline is put on children's faces to repel flies but could actually attract them Waste can be put in pits but this is not a widespread practice (Community E only). People dispose of waste multiple times a day so practically, although not next to the living quarters, this place is not far from the home
Objects / tools, infrastructure
Social Health Extension Workers advise people on actions that can be taken to reduce flies in the home Role models, relationships,
networks, norms, institutions
Biological Human and animal faeces is widespread in the home environment. Even when there are latrines there is faeces surrounding them, providing a breeding environment for Musca sorbens. Parasites/foods/animals
Cattle, milk and dead animals are thought to attract flies

Page
30
Participants were reasonably knowledgeable about the problems brought by flies:
“They cause lots of diseases because they land on faeces and come home and land on our faces and foods.” (HH3)
Some people knew that they transmitted trachoma, however others believed flies to be vectors for HIV and other
diseases.
Participants did not actively swot flies away from their children’s faces either, even when they were breastfeeding.
However, they said that when flies landed on their face it made them feel dirty, it irritated them and made them feel
uncomfortable (Box 1). Vaseline is believed to help prevent flies from landing on the face.
Parents reported being worried about seeing children with flies on their faces and said that this would prompt them
to wash the child’s face. People felt that the numbers of flies could be reduced by improving personal hygiene
through things such as face washing and environmental hygiene, including burning or burying rubbish regularly.
People also thought pesticides could be used to control flies. Locally people also burnt certain hinds of wood in their
homes which apparently creates smoke which repels flies. Other people felt that there was nothing humans could do
to reduce the number of flies as it was determined by external factors in the environment.
Health Extension Workers report actively promoting covering food, preparing a hole for compost and collecting cow
dung in one place and allowing it to dry to reduce flies; covering food, washing dishes, and disposing of waste –
sometimes in pits - are existing practices to some extent. Cattle and other animals are present in every compound
and nothing is done to reduce flies on animals.
9. Sleeping arrangements
Current practices (Extended) families in the ten observed households slept in clusters. There was some variation, but generally young
children were with their mother or both parents, and older children and sometimes men slept apart (Figure 18). The
polygamous family (HH4) slept in two different arrangements depending on whether or not the Head of Household
was home. The place used for sleeping was sometimes a bedroom and sometimes the main living space that was
also shared with animals.
Box 1. Mothers say flies on their children bother them, but little was seen to be done to remove flies from children’s faces Researcher: How do they feel when flies land on their face? Women: It feels uncomfortable and also brings dirt on our faces. Researcher: Does it feel any different when the flies are on your children’s faces? Women: It feels the same, I don’t feel good when flies land on my child’s face. Researcher: Is there anything you can do to stop flies coming their faces? Women: I should wash the baby and oil with Vaseline. Researcher: What does the Vaseline do? Women: They don’t like to land on it.

Page
31
Key
G Grandmother G Grandfather U Uncle
M Mother F Father
room / house Girl (5 yrs +) Boy (5 yrs +)
Young girl (<5 yrs) Young boy (<5 yrs)
HH1 HH2 15
F M 5 G G 13 6 15 Mat
Bed Bed Mat Bed
House 1 18 20
Mattress M F 1
House 2 Bed
HH3 no particular order HH4 Or 8 M
M 7 9 11 F Cot with mattress - outside Bed 1 8 1
Mat behind curtain M F
HH5 HH6
17 F M 1 3 7 8 10 7 13 16
Bed Bed Mattress M F 1 18
Building 1 Building 2 (mother wouldn't show this, description only) Bed
HH7 HH8 F 15 10
G G 12 15 M 8 F 5 8
Bed Mattress Mat Bed Mattress
House 1 House 2
M 3
Mattress
HH9 M 4 F 5 HH10
G 3 7 8 Mattress
Mattress Mats 2 12
16 M F U 14 18
Bed Mat
House 1 House 2
Figure 18. Schematic of sleeping arrangements of all individuals in the ten observed households.
Beds were of three types: some were raised on a wooden frame, while others were straw mattresses or woven mats
that were placed on the floor and covered with goat skins, lastly some people only slept on goat skins. Raised beds
tended to be used by either adult males, both parents or parents and their youngest children. Everyone else slept on
straw mattresses, woven mats or goat skins. Blankets were shared except for some older children who slept in the
same space but used their ‘own’ covers. In focus groups some people reported that they covered mattresses with
sheets as well, however no sheets were seen in the households we observed. Pillows as we know them are not
commonly used, but old garments or bags of grain may be bundled up to support the head. These can be placed
directly under the head or beneath the mattress inside an empty grain sack. According to focus group discussion
participants, young children do not expressly need to be given a pillow, but they may share a pillow if they are in the
same bed. Figure 19 shows a number of the items of bedding observed.
Figure 19. Beds, mattresses, bedding and pillows in use in the study households.
Figure 19. Beds, mattresses, bedding and pillows in use in the study households.
In focus groups with mothers we explored normative sleeping patterns. Participants were introduced to a
hypothetical family consisting of a mother and father and their 3 children aged 18 (son), 13 (daughter) and 2 (son).
An aerial house plan was drawn and they were asked to discuss where each family member should sleep and who
should have their own sheet. There was a relatively high level of consensus among participants that the youngest
Cot bed where father sleeps on a goat skin outside the house (HH3)
Straw mattress covered with a mat (and goat skins which had
been taken to the fields). Old clothes are used as a pillow (HH9)
Five people sleep under one blanket (HH8)

Page
32
child should sleep together with the parents in the bedroom under one blanket, and the other children should sleep
in the living space with separate blankets if two were available (Figure 20). It was considered impossible for children
to ‘top and tail’ (that is so to say that one child would lay so that their head would be next to the other child’s feet)
as they would kick each other and quarrel. The same participants felt that children above 5 years-of-age should get
their own blanket if the economic situation of the family allows this, but there was no agreement on an age when a
child should have a pillow. Participants seemed open to the idea of giving children their own pillows, again, if it was
affordable. Participants were asked whether blankets are used to cover heads while sleeping. Differing practices
were reported regarding this with many indicating that it may happen sub-consciously.
Figure 20. Typical sleeping arrangement of a family illustrating where people sleep and who might share a blanket
according to participants from a focus group.
Almost immediately after families woke up in the morning they made their beds and / or tidied away the skins, mats
and blankets that had been used for sleeping. People were observed bundling all bedding into a pile on the bed or
somewhere within the home, while some households aired bedding outside.
Visitors
Focus group participants differed in their opinions of where a visiting male relative should sleep (Box 2). This visitor
would also be given a separate sheet / blanket to use that is normally reserved for special occasions and is not in
general use. This is done out of respect for the guest. These sheets cannot be given to other household members, for
example, to avoid children sharing bedding. This is further explored in the section on the treatment of guests.
Cost of Bedding
Commonly found items of bedding were located easily in the local markets. The costs of these items is shown in
Table 9. As a comparator, all households owned plastic coffee tables worth 60 Birr, a bar of soap costs 6 Birr, and 25L
jerry cans cost 40 Birr.
Box 2. Conversation during the focus group regarding where a male visitor would sleep.
Mother: “He sleeps alone just next to the children but not together with the children.”
Second Mother: “I would leave the bed for the uncle and sleep with my children and he sleeps
with my husband.”
Researcher: “Which one generally is more common do they think, for the uncle to be in the
salon or to be in the bedroom?”
Mothers: “More common is for the uncle to sleep with a father in the bedroom and for the
mother to sleep with children.”

Page
33
Table 9. Cost of common bedding materials
STRAW MATTRESS = 120 Birr MATTRESS = 1400 Birr (1.5m) PILLOWS = 90 Birr
(Not seen in households)
RICE SACKS (stuffed & used as pillows) = 6 Birr BLANKETS = 250-300 Birr SHEETS = 90 Birr
Factors influencing current practices Table 10. Factors influencing current sleeping practices, by theoretical driver of behaviour.
Parents and young children sleep close together
Beds, mattresses, blankets and pillows are shared
Factors in the brain
Executive People sleeping in a bed / mattress may have a ‘spot’. Children can sleep anywhere: “there is no formula, children move here and there in the night.”
Differing opinions on whether a child 'needs' their own blanket and at what age they need a pillow Deliberate planning,
knowledge
Motivated Young children can cry in the night and need to be near the mother It is cold at night
Stuffed rice sacks and old garments are not considered to be uncomfortable as a pillow Some households choose to air their bedding
Emotional drivers, interests, reward
Reactive Unless a bed or mattress is used, there does not seem to be a set 'place' where people sleep
Presence of a guest cues provision of a new, clean sheet or blanket Cues, habits & skills
Factors in the environment
Physical Householders share existing beds / mattresses / goat skins which brings them close together
Households do not have sufficient bedding to allocate items to all individuals Cost of bedding prevents purchase of more sheets and blankets
Objects / tools, infrastructure
Social Presence of a guest / polygamous husband changes sleeping
patterns Birth of a new child can change sleeping patterns
Most household items are shared, although blankets can be used by specific individuals Guests are given sheets that are otherwise reserved for special occasions out of respect
Role models, relationships, networks, norms, institutions
Biological Animals often share the same living space (highlighting the lack of additional structures that can be used for sleeping in) Presence of bed bugs in bedding can alter sleeping patterns
Parasites/foods/animals

Page
34
10. Laundry Laundry was often reported to be done on a weekend. Some houses reported doing laundry at their home while
others did it at nearby rivers. The river was often used for large amounts of laundry, adult clothes and bedding while
smaller loads, in particular the washing of baby clothes, were done at home. Laundry is seen as taxing in terms of
water use, soap use and time. Very limited amounts of water were observed to be used when washing clothes at the
house. Yet participants reported that often when they were doing laundry at home it would often mean collecting
50-75 extra litres of water. At some points during the year people said it was not possible for them to collect this
amount of extra water and hence laundry became less frequent.
There were three occasions where laundry was observed during observation. In two cases this involved just the
washing of baby clothes. In one case we observed a woman doing a full load of laundry in preparation for Timkat
celebrations. This took her 1.5 hours.
Figure 21. Woman doing a full load of washing in the home
Regularity of washing clothing
To reduce the burden of laundry, different types of clothes are washed at different frequencies. The clothing of
young children (under 2) is seen as the biggest priority and is washed daily. Some women also said that washing their
husband’s clothes was a priority. One woman explained that she prioritises her clothes and the baby’s because “the
baby always makes her clothes dirty.” School age children wash their clothes and uniforms weekly as it is thought
that it is important for them to look clean and smart at school. Adult clothes were often washed less frequently
ranging from every three days for to every 2 months. Adults have work clothes and clothes for special occasions with
the latter being washed only as needed. Women reported wearing a set of work clothes only for 2 or three days
however observation suggests it may commonly be longer. Women said that it would be difficult to increase the
regularity with which they washed clothes but thought it was possible to do laundry every 3 days in some seasons.
Women reported that it was acceptable for younger girls or even their husbands to assist with laundry if it was
necessary to increase the frequency with which it was done.
Figure 22. Examples of clothes washing done at home. In general, this includes just a few items of babies clothing.

Page
35
Regularity of washing bedding
Sheets are considered the priority among items of bedding and are washed on average every 2 weeks, while
blankets are washed every month or two months. Because of the size of sheets and blankets they are normally
washed at the river. Women reported that when guests visit their houses they always wash the sheets immediately
after. Some people reported that animal skins (which are placed on top of the mattress for sleeping) are also washed
at the same regularity as blankets but others said they could not be washed (more likely). Pillow cases (made from
grain sacks) and mattresses are generally not washed but are commonly placed outside in the sunlight to air on a
daily basis. Some mothers were open to the idea of washing pillow cases more regularly because they felt it would
use less water.
Figure 23. An example of bedding being placed outside to air
Table 11. Factors influencing laundry practices, by theoretical driver of behaviour.
Laundry is washed infrequently
Factors in the brain
Executive Deliberate planning, knowledge
Water is limited so laundry is strategically prioritised. Mothers are taught during pregnancy classes that it is important to regularly wash their baby’s clothes
Motivated Emotional drivers, interests, reward
Participants said they enjoyed the feeling of fresh bedding. Doing large loads of laundry is seen as time consuming and inconvenient.
Reactive Cues, habits & skills
Laundry is done on the basis of being physically dirty.
Factors in the environment
Physical Objects/tools/infrastructure
Laundry is difficult and is done on rocks or grain sacks in the home or has to be carried a long distance to the river. The availability of water often leads to laundry compromises. People did not have laundry baskets or things used only for laundry. Pillows are made out of the same fabric as mattresses and therefore like mattresses are not washed. Pillows are placed under the sheets/animal skins and therefore not something that needs to be washed. People use only one set of bedding and so when it is washed it has to be used again straight away.
Social Role models, relationships, networks, norms, institutions
Children must be seen to be clean at school or this might cause embarrassment for themselves and their families. The ideal frequency to wash clothes is every three days but women feel there is a large gap between ideal and average. Children are judged on whether they have a clean appearance for school but women were not part of many social networks and reported spending most of their time at the house or in the field and thus had few opportunities where they had to be publically seen to be clean (exceptions are holidays)
Biological Parasites/foods/animals
Clothes and bedding are not seen as something that could transmit germs.
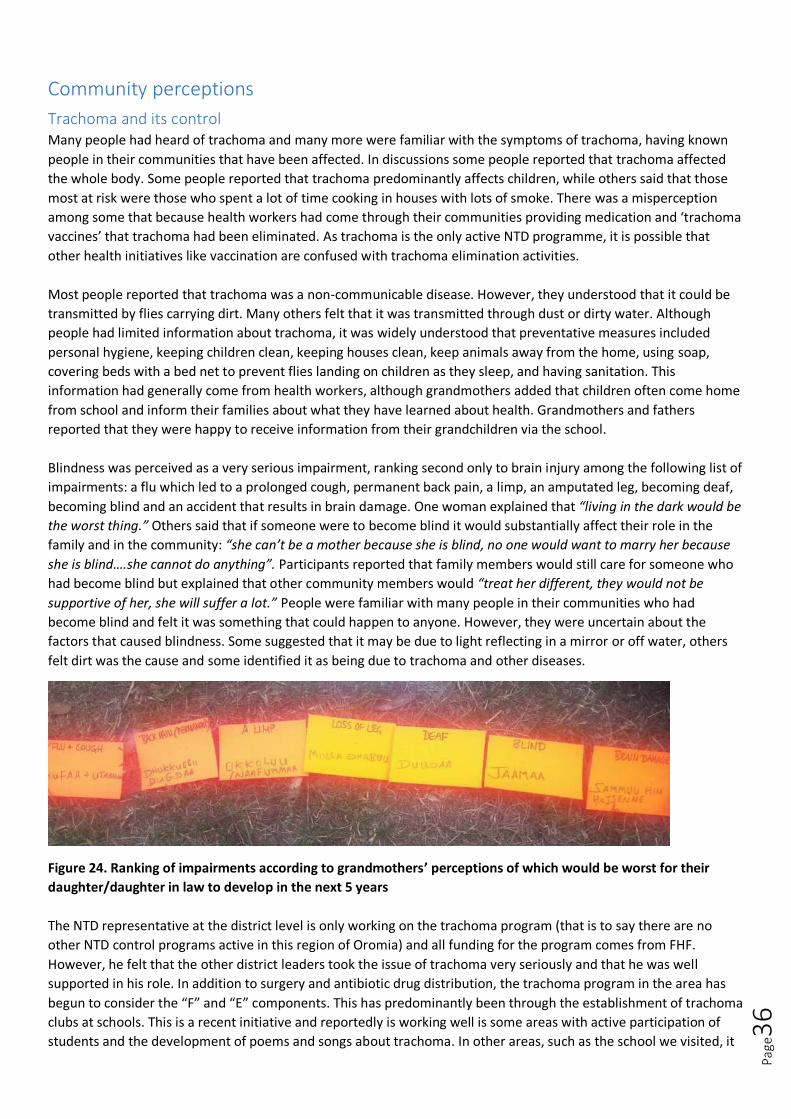
Page
36
Community perceptions
Trachoma and its control Many people had heard of trachoma and many more were familiar with the symptoms of trachoma, having known
people in their communities that have been affected. In discussions some people reported that trachoma affected
the whole body. Some people reported that trachoma predominantly affects children, while others said that those
most at risk were those who spent a lot of time cooking in houses with lots of smoke. There was a misperception
among some that because health workers had come through their communities providing medication and ‘trachoma
vaccines’ that trachoma had been eliminated. As trachoma is the only active NTD programme, it is possible that
other health initiatives like vaccination are confused with trachoma elimination activities.
Most people reported that trachoma was a non-communicable disease. However, they understood that it could be
transmitted by flies carrying dirt. Many others felt that it was transmitted through dust or dirty water. Although
people had limited information about trachoma, it was widely understood that preventative measures included
personal hygiene, keeping children clean, keeping houses clean, keep animals away from the home, using soap,
covering beds with a bed net to prevent flies landing on children as they sleep, and having sanitation. This
information had generally come from health workers, although grandmothers added that children often come home
from school and inform their families about what they have learned about health. Grandmothers and fathers
reported that they were happy to receive information from their grandchildren via the school.
Blindness was perceived as a very serious impairment, ranking second only to brain injury among the following list of
impairments: a flu which led to a prolonged cough, permanent back pain, a limp, an amputated leg, becoming deaf,
becoming blind and an accident that results in brain damage. One woman explained that “living in the dark would be
the worst thing.” Others said that if someone were to become blind it would substantially affect their role in the
family and in the community: “she can’t be a mother because she is blind, no one would want to marry her because
she is blind….she cannot do anything”. Participants reported that family members would still care for someone who
had become blind but explained that other community members would “treat her different, they would not be
supportive of her, she will suffer a lot.” People were familiar with many people in their communities who had
become blind and felt it was something that could happen to anyone. However, they were uncertain about the
factors that caused blindness. Some suggested that it may be due to light reflecting in a mirror or off water, others
felt dirt was the cause and some identified it as being due to trachoma and other diseases.
Figure 24. Ranking of impairments according to grandmothers’ perceptions of which would be worst for their
daughter/daughter in law to develop in the next 5 years
The NTD representative at the district level is only working on the trachoma program (that is to say there are no
other NTD control programs active in this region of Oromia) and all funding for the program comes from FHF.
However, he felt that the other district leaders took the issue of trachoma very seriously and that he was well
supported in his role. In addition to surgery and antibiotic drug distribution, the trachoma program in the area has
begun to consider the “F” and “E” components. This has predominantly been through the establishment of trachoma
clubs at schools. This is a recent initiative and reportedly is working well is some areas with active participation of
students and the development of poems and songs about trachoma. In other areas, such as the school we visited, it
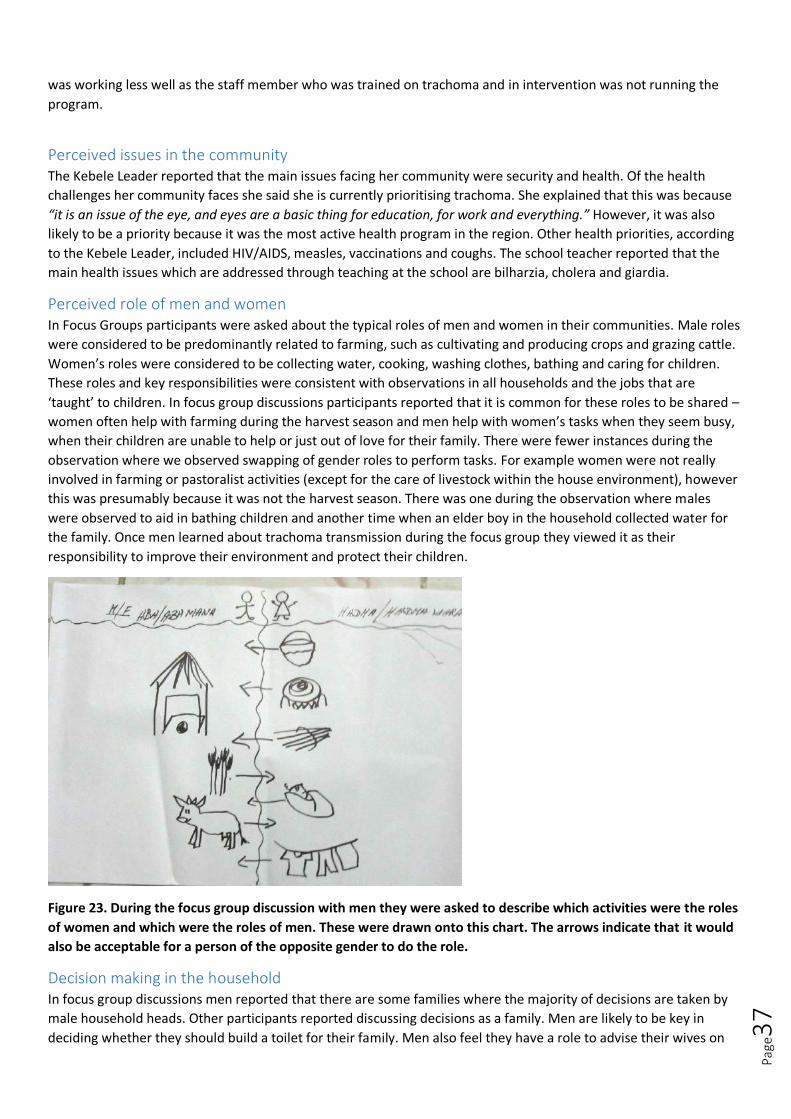
Page
37
was working less well as the staff member who was trained on trachoma and in intervention was not running the
program.
Perceived issues in the community The Kebele Leader reported that the main issues facing her community were security and health. Of the health
challenges her community faces she said she is currently prioritising trachoma. She explained that this was because
“it is an issue of the eye, and eyes are a basic thing for education, for work and everything.” However, it was also
likely to be a priority because it was the most active health program in the region. Other health priorities, according
to the Kebele Leader, included HIV/AIDS, measles, vaccinations and coughs. The school teacher reported that the
main health issues which are addressed through teaching at the school are bilharzia, cholera and giardia.
Perceived role of men and women In Focus Groups participants were asked about the typical roles of men and women in their communities. Male roles
were considered to be predominantly related to farming, such as cultivating and producing crops and grazing cattle.
Women’s roles were considered to be collecting water, cooking, washing clothes, bathing and caring for children.
These roles and key responsibilities were consistent with observations in all households and the jobs that are
‘taught’ to children. In focus group discussions participants reported that it is common for these roles to be shared –
women often help with farming during the harvest season and men help with women’s tasks when they seem busy,
when their children are unable to help or just out of love for their family. There were fewer instances during the
observation where we observed swapping of gender roles to perform tasks. For example women were not really
involved in farming or pastoralist activities (except for the care of livestock within the house environment), however
this was presumably because it was not the harvest season. There was one during the observation where males
were observed to aid in bathing children and another time when an elder boy in the household collected water for
the family. Once men learned about trachoma transmission during the focus group they viewed it as their
responsibility to improve their environment and protect their children.
Figure 23. During the focus group discussion with men they were asked to describe which activities were the roles
of women and which were the roles of men. These were drawn onto this chart. The arrows indicate that it would
also be acceptable for a person of the opposite gender to do the role.
Decision making in the household In focus group discussions men reported that there are some families where the majority of decisions are taken by
male household heads. Other participants reported discussing decisions as a family. Men are likely to be key in
deciding whether they should build a toilet for their family. Men also feel they have a role to advise their wives on

Page
38
how to best care for their children. Women do normally have access to some money and it is considered normal for
women to buy soap for the family and other products for the children without permission from her husband.
Children and childhood manners During individual interviews we asked how people would view a well manner child. Responses included that a well-
mannered child should obey their parents and elders in the community, they should collect water, help with
household chores, not quarrel with other children, pursue their education and contribute to their family (often
financially as they get older). Well-mannered children should also speak slowly, and dress somewhat traditionally. In
contrast a poorly-behaved child is one that insults others, is disrespectful and uses bad language.
Interestingly many people felt that there was little that parents could do to shape the nature of their child’s
behaviour and their personality as people perceived personality to be determined at birth.
Children were observed to contribute actively to the household. Children were observed to assist their mothers with
cooking, collecting water, cleaning the house, helping younger siblings to bathe/wash faces and hands and helping to
re-lay the floor. From the age of about 7 children took on significant caregiving roles for their younger siblings and
had a high level of physical interactions with them (frequently carrying them around, hugging them and kissing
them).
Figure 24. Left and middle show older siblings caring for younger siblings. Right shows a young girl collecting water
for the family.
Treatment of guests Guests are considered very important and highly respected. In focus group discussions participants explained that
special arrangements are made when a guest visits someone’s house. This includes the special preparation of certain
types of food and drink, cleaning the house and the preparation of a place for them to sleep. As a sign of respect
guests should always be given separate sheets to the rest of the family and the sheets should always be washed
after they leave. These sheets are not used by the family. One woman explained that she would be worried if a guest
arrived at her house and she had not had time to prepare: “it worries us very much, we have to clean our houses, we
have to prepare where he should sleep, we go and buy drinks, then cook food until he drinks, and if the guest is from
very far away and respectful one, we even buy sheep and slaughter for the guest.”
Perceptions of an ideal mother In focus group discussions we asked grandmothers to describe the ideal mother. As a visual aid we drew a stick
figure and got the participants to add elements to the figure to make her the ideal mother. From this discussion it
emerged that an ideal women is perceived to be of slim to medium build, her face should be narrow, her lips small
and she should be beautiful. Her hair should be quite long and she should comb it and put butter through it
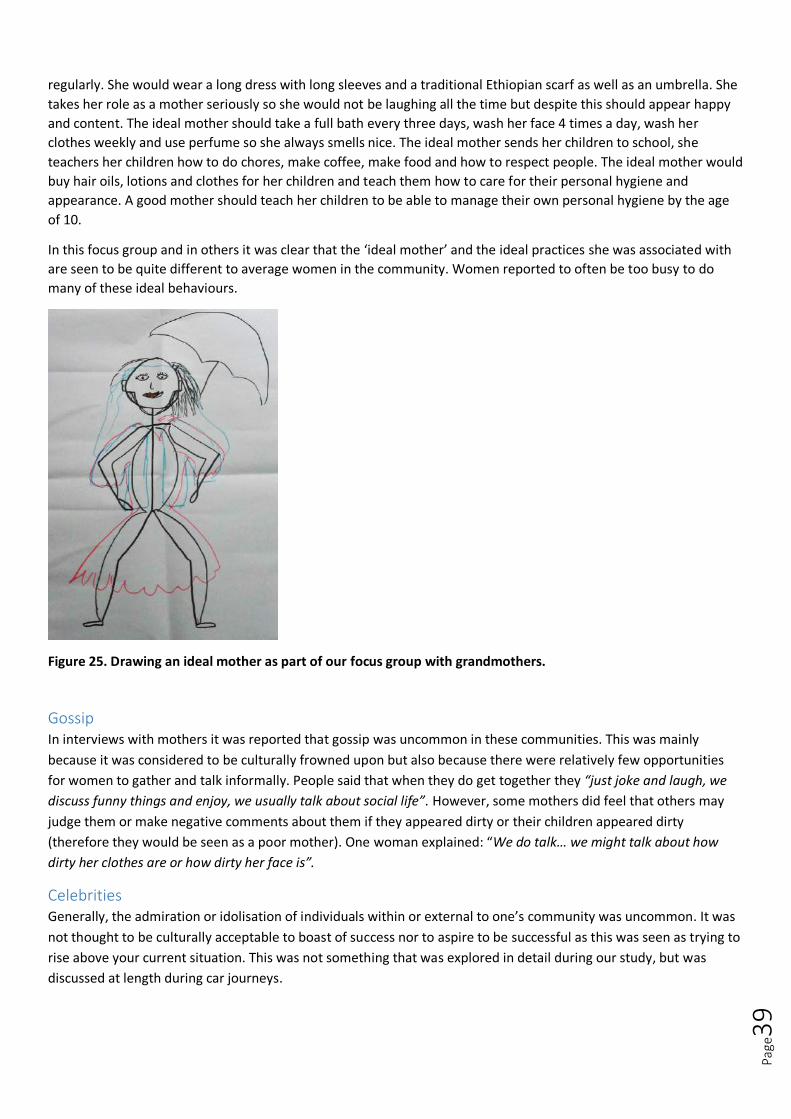
Page
39
regularly. She would wear a long dress with long sleeves and a traditional Ethiopian scarf as well as an umbrella. She
takes her role as a mother seriously so she would not be laughing all the time but despite this should appear happy
and content. The ideal mother should take a full bath every three days, wash her face 4 times a day, wash her
clothes weekly and use perfume so she always smells nice. The ideal mother sends her children to school, she
teachers her children how to do chores, make coffee, make food and how to respect people. The ideal mother would
buy hair oils, lotions and clothes for her children and teach them how to care for their personal hygiene and
appearance. A good mother should teach her children to be able to manage their own personal hygiene by the age
of 10.
In this focus group and in others it was clear that the ‘ideal mother’ and the ideal practices she was associated with
are seen to be quite different to average women in the community. Women reported to often be too busy to do
many of these ideal behaviours.
Figure 25. Drawing an ideal mother as part of our focus group with grandmothers.
Gossip In interviews with mothers it was reported that gossip was uncommon in these communities. This was mainly
because it was considered to be culturally frowned upon but also because there were relatively few opportunities
for women to gather and talk informally. People said that when they do get together they “just joke and laugh, we
discuss funny things and enjoy, we usually talk about social life”. However, some mothers did feel that others may
judge them or make negative comments about them if they appeared dirty or their children appeared dirty
(therefore they would be seen as a poor mother). One woman explained: “We do talk… we might talk about how
dirty her clothes are or how dirty her face is”.
Celebrities Generally, the admiration or idolisation of individuals within or external to one’s community was uncommon. It was
not thought to be culturally acceptable to boast of success nor to aspire to be successful as this was seen as trying to
rise above your current situation. This was not something that was explored in detail during our study, but was
discussed at length during car journeys.
Page
40
Community structure and touchpoints This study operated at the Kebele (community/ward) level which represents that lowest administrative unit in
Ethiopia, falling underneath the Woreda (district). Each Kebele has roughly 2000-5000 people and is led by a Kebele
leader. The Kebele leader is an elected position that sits for a term that can go beyond 20 years if they are popular.
Kebele leaders can be removed from their role if they are not acting according to the community’s wishes. The
Kebele, nor the Kebele Leader, does not have any formal financial mechanisms independent of the district it sits
within. The kebele leader interviewed in this study (who happened to be female) explained that when something
needs to be done in the community, everyone comes together to generate the funds. The kebele leader is supported
by a broader administrative cabinet including a deputy leader and ‘militias’ who are the people who report to the
district and enforce law. There are 8 other key leaders in a kebele, each of whom looks after a different issue. These
include the health extension worker for health issues, the school principle on education matters and the agricultural
extension worker for farming. Within the Kebele there are administrative groupings called Goti which are groups of
up to 30 households headed by elected representatives also. Community labour and contributions tend to be
organised through these groups.
In addition to the above hierarchy in the Kebele, each individual over the age of 18 also participates in a one-to-five
group. These are literally groups of 5 individuals (men and women have separate groups), with one leader who acts
as a go-between between local leaders and the rest of their group. These groups act as the principle way for
information to be disseminated in the community and for feedback to reach the village leader. The groups meet
amongst themselves almost every week and the representatives from each group meet with the village leadership
three times a week too. District administrations also use these networks to deliver information. Leaders of each one-
to-five groups are elected based on their reputation and work in the community. All community members over the
age of 18 are a part of such groups. People reported that trachoma was something that had been discussed in their
one-to-five groups in the past. Community meetings are also held once a month. The whole community are invited
to these and tend to discuss issues of key importance such as security and development. The kebele leader we
interviewed said that in her community trachoma was something that had been discussed at these large meetings in
the past.
According to the Kebele leader we spoke to, there were few external health or development programs which were
delivered at a Kebele level. The Kebele leader explained that sometimes representatives from the district would
attend the community meetings to talk to the community about particular issues. She also explained that the school
does educational programs, however these appear to be driven by the national curriculum rather than health or
development programs which use the school as a mode of delivery. According to the Kebele leader there were no
formal sanitation programs in the communities, only the ongoing sanitation promotion work done by the health
extension workers. This was somewhat at odds with what we heard from district representatives who mentioned
there was an ODF plan for the area and they were beginning to roll out CLTS.

Page
41
Information also reaches these communities via radio or television. Some of the houses where we did observation
had radios. None had TVs. Both are still relatively uncommon in these rural areas. Reportedly it is mainly young
educated men who watch TV when they travel to a larger town. Apparently it is common for these people to then
return to the community and share news about what they watched on TV. People’s favourite TV programs and Radio
programs are sports coverage and political or economic programs.
Figure 27. Mapping structures and touch points in the community.
There are various other social, financial and skills-based groups in the communities where we were working. These
included:
Eddir – social insurance groups that meet weekly. People contribute money primarily for things like funerals
and other life events. At the meetings they discuss community issues also. Men and women have separate
savings groups. Women tend to save for things such as childbirth.
Debo- a system where neighbours work together in rotation to ensure everyone’s fields are farmed.
Women’s associations and saving groups – these were different from Eddir and tended to be for saving
money to establish small business initiatives. Generally these groups were established informally among
female friendship groups.
WASH committees – WASH committees maintain the water points in the community and are also
responsible for locking the water points at certain points during the day.
Pregnant mothers’ groups – These are established in connection to the health centre and coordinated by the
health workers. These meet monthly and provide information about infant care (eg. feeding, breastfeeding
and food hygiene). One of the things they actively promote is to wash young children on a daily basis.
Church - Most people attend church on Sundays and there are some groups associated with the church who
meet at other times.
Zeker – This is an informal social structure associated with the Orthodox Christian church. Women form
small groups of friends and on one set day a month one woman’s friends come to her house for bread and
coffee. On other set days in the month she will go to the houses of the other members of her group for
bread and coffee.

Page
42
Coffee drinking – coffee ceremonies are common in this part of Ethiopia and it is not uncommon for families
to invite their neighbours to join them for a coffee and some food on an almost daily basis.
Local bars – In most communities there are a few people who produce traditional alcohol to sell. In the
evenings and particularly on weekends the homes of these local alcohol producers become mini bars where
people socialise and come together.
School events - Sometimes the school run sporting events or drama performances which general members
of the community attend.
Holidays The main holidays are Christmas, New Year, Easter and Epiphany. On these days it is common for people to spend
additional time on their appearance and on the cleanliness of their home. For example, people reported that on such
days clothes are always washed and all family members would have a full bath. The floors of the house are often re-
laid for these occasions too.

Page
43
DISCUSSION
Potential intervention strategies
Overview of solutions in relation to trachoma transmission This research explored sub-optimal hygiene behaviours associated with known trachoma transmission pathways. As
documented we found a range of sub-optimal practices. However, we also observed a lot of positive hygiene
practices or practices that, although sub-optimal, made sense given the constraints of the setting. From the outset
we knew that it was unlikely that this research would identify one clear course of action that would dramatically
reduce trachoma prevalence. As Figure 25 illustrates this was based on an understanding that trachoma can pass
from one eye to the next through three principle means: flies, fingers and fomites (which in this case is likely to be
predominantly bedding or clothing). Intervening on any one transmission route would be likely to only reduce
trachoma proportionately.
Figure 25. Trachoma basic transmission diagram
However, in thinking about solutions it is important not to treat all transmission routes as equal as the behaviours
that contribute to each transmission route are in some cases more numerous. For example, if we were to aim to
reduce flies in the environment, we would have to look at all the factors that increase the current presence of flies in
this setting. This is likely to require a) the removal of all animal and human faeces (including child faeces) from the
open environments near houses, b) the movement of livestock further away from houses, c) creating a demand for
sanitation and improving toilet use and d) the effective management of garbage. An intervention unrelated to
behaviour may also consider the value of large-scale fumigation to literally reduce the fly population. An intervention
which only builds toilets, for example, is likely to be insufficient to achieve a substantial reduction in trachoma
transmission if the other factors are not addressed. However, in order to deliver a behaviour change intervention it
may not be feasible to intervene on all sub-optimal practices.
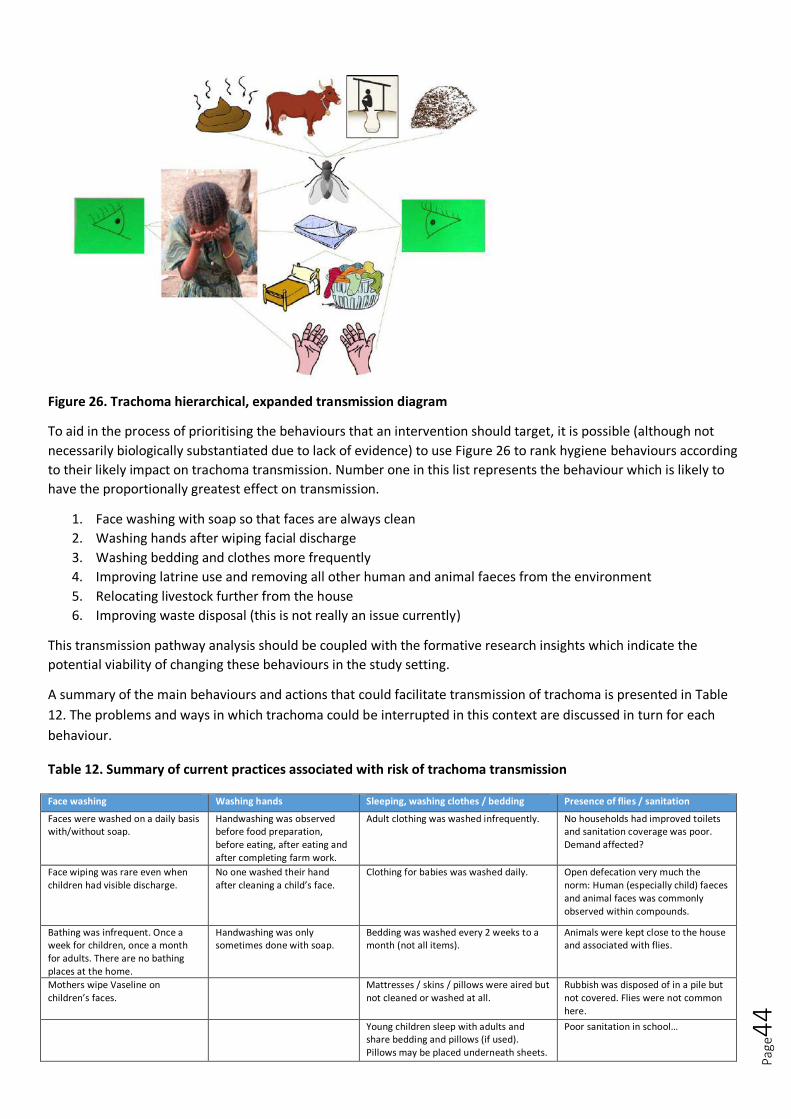
Page
44
Figure 26. Trachoma hierarchical, expanded transmission diagram
To aid in the process of prioritising the behaviours that an intervention should target, it is possible (although not
necessarily biologically substantiated due to lack of evidence) to use Figure 26 to rank hygiene behaviours according
to their likely impact on trachoma transmission. Number one in this list represents the behaviour which is likely to
have the proportionally greatest effect on transmission.
1. Face washing with soap so that faces are always clean
2. Washing hands after wiping facial discharge
3. Washing bedding and clothes more frequently
4. Improving latrine use and removing all other human and animal faeces from the environment
5. Relocating livestock further from the house
6. Improving waste disposal (this is not really an issue currently)
This transmission pathway analysis should be coupled with the formative research insights which indicate the
potential viability of changing these behaviours in the study setting.
A summary of the main behaviours and actions that could facilitate transmission of trachoma is presented in Table
12. The problems and ways in which trachoma could be interrupted in this context are discussed in turn for each
behaviour.
Table 12. Summary of current practices associated with risk of trachoma transmission
Face washing Washing hands Sleeping, washing clothes / bedding Presence of flies / sanitation
Faces were washed on a daily basis with/without soap.
Handwashing was observed before food preparation, before eating, after eating and after completing farm work.
Adult clothing was washed infrequently. No households had improved toilets and sanitation coverage was poor. Demand affected?
Face wiping was rare even when children had visible discharge.
No one washed their hand after cleaning a child’s face.
Clothing for babies was washed daily. Open defecation very much the norm: Human (especially child) faeces and animal faces was commonly observed within compounds.
Bathing was infrequent. Once a week for children, once a month for adults. There are no bathing places at the home.
Handwashing was only sometimes done with soap.
Bedding was washed every 2 weeks to a month (not all items).
Animals were kept close to the house and associated with flies.
Mothers wipe Vaseline on children’s faces.
Mattresses / skins / pillows were aired but not cleaned or washed at all.
Rubbish was disposed of in a pile but not covered. Flies were not common here.
Young children sleep with adults and share bedding and pillows (if used). Pillows may be placed underneath sheets.
Poor sanitation in school…

Page
45
Face washing solutions
Problem 1. Faces of children were often dirty.
Behaviour task and context:
The faces of children under two were generally washed with soap two to four times per day (at least in the morning
and at night). Children over the age of two did not have their facial cleanliness monitored as closely by their mother.
In this older age group it was seen to be the child’s responsibility (with support from older siblings) to clean their
face. Despite this most children washed their face (sometimes with soap, sometimes not with soap) twice a day,
once in the morning and once at night. Although faces are cleaned first thing or before school and before sleeping
there is still a long period during the day when faces are not washed. This means that discharge tends to build up on
the faces of young children as the day progresses. For the purposes of trachoma transmission we would like all
family members to wash faces more regularly throughout the day. We would also like family members to support
each other to ensure this is done routinely, but also specifically when discharge is observed.
Opportunities for change:
1. Add occasions for face washing by building on existing routines/ ritualise face washing.
When we asked mothers about the potential of adding extra face washing times to their daily routine they agreed
that this would be possible but struggled to agree on what times would be appropriate. Times that could be
considered include before or after eating, before breastfeeding, after collecting water (since then there is plenty of
water available), or any time hands are washed. We also observed that there are several ritualised aspects of
everyday life in Ethiopia. Perhaps the best example of this are coffee ceremonies. It may be possible to add face
washing to these rituals or create a new ritual around face washing.
Feasibility: strong. Behaviour trial: possible (this should include trialling face washing at different times in the day)
2. Make discharge more disgusting/visible
Eye and nasal discharge was reported to be disgusting according to the disgust ranking exercise we did in Focus
groups. However, in practice it was not disgusting enough for it to be a trigger for face washing or wiping. A
behaviour change intervention may strive to increase the level of disgust associated with discharge in order to illicit
the desired behavioural response.
Feasibility: strong. Behaviour trial: no but pre-testing of intervention design concepts should be done.
3. Make face washing more enjoyable or comforting
Currently face washing is a routine behaviour, performed only at certain times of day. It is seen as refreshing and
associated with positive outcomes such as feeling brighter for school. In order to get face washing performed more
frequently a behaviour change intervention may seek to make the process more enjoyable or rewarding or increase
the perceived comfort associated with face washing.
Feasibility: moderate. Behaviour trial: no, but pre-testing of intervention design concepts should be done.
4. Make it a priority for all family members to have washed their faces.
Currently mothers prioritise the facial cleanliness of their very young children (those under 2 years) who receive
twice daily baths and often have their faces washed at other times during the day as well. Slightly older children
(eg:3-7 years of age) are important for the transmission of trachoma yet are expected to be semi-independent in
relation to their face washing practices and are not subject to the same pressure to look clean for school. A
behaviour change intervention might target the prioritisation of face washing among this age group specifically.
Feasibility: strong. Behaviour trial: possible.

Page
46
Problem 2. Face wiping was rare even when children had visible discharge
Behaviour task and context:
Faces were rarely observed to be wiped even when they had visible discharge. On a few occasions mothers were
observed to wipe their child’s face with either an item of the child’s clothes or their hands. In focus groups mothers
also reported sometimes wiping their child’s face with the inside of their dress. Mothers explained that they were
reluctant to wipe their child’s faces because they often did not have anything clean to wipe a child’s face with. This is
seen to be a particular challenge during the harvest season when young children often accompany parents to their
fields. In these circumstances there is no soap or water available for washing faces and clothes and hands are too
dirty to wipe faces. For the purpose of trachoma transmission we would prefer that faces are washed whenever
there is visible discharge but understand that this is not always feasible. Regular wiping with a clean product that it is
not reused should be promoted.
Opportunities for change:
1. Introduce a face wipe product
In focus groups with mothers we gave them samples of face wipes to try. Mothers liked the face wipes, reporting
that they made them feel refreshed, they were also impressed with the amount of dirt they visibly removed.
Mothers said they would happily use them on both their faces and the faes of their children. Mothers understood
that they face wipes could only be used once and then had to be discarded but found this acceptable. Mothers also
understood that face wipes like this would cost money and said that they would be willing to spend 20 Birr on
roughly 2 months’ worth of face wipes. Mothers said that if the face wipes came in a small container they could
easily wrap this up in the scarf they tie around their waste so that it would be easily available when in the field.
Feasibility: moderate. Behaviour trial: possible.
Problem 3. Faces were not always washed with soap
Behaviour task and context:
Faces were observed to not always be washed with soap. Even within one household, where soap was available, it
was common to see some family members wash their faces thoroughly with soap while others used only water. For
the purposes of trachoma transmission, we want to increase the use of soap when face washing.
Opportunities for change:
1. Create a face washing stand where soap and water can be kept.
As described previously participants were somewhat familiar with tippy taps but no one was observed to have a
handwashing or face washing station at their house. In focus groups mothers did not seem that keen about building
a place where faces could be washed. They felt that mirrors may be useful for helping young children to wash faces
but generally that mirrors were not something that should be kept outside at a face washing station as they would
not be used by adults and the reflection of the sun in the mirrors might hurt people’s eyes.
Feasibility: poor. Behaviour trial: possible (trials of different kinds of designs may be effective).
Problem 4. Although faces are washed during bathing, bathing happens infrequently due to lack of bathrooms and
water scarcity
Behaviour task and context:
Faces are washed thoroughly during bathing with water and soap. However, for women particularly, bathing is
irregular, often happening just once every two months. One of the factors that contributes to this is that there are
no places for women to bathe in privacy at their homes. A secondary facor is that women perceive bathing to
Page
47
consume a lot of water (water which is both scare and time consuming to collect). It would be beneficial if
bathrooms were constructed within people’s compounds as this is likely to encourage all members of the family to
bathe more frequently. Secondly it would be beneficial to design bathrooms with devices to reduce the amount of
water used. Having said this, it is uncertain whether increasing bathing frequency will significantly impact
transmission of trachoma.
Opportunities for change:
1. Promote the creation of bathrooms so it is more convenient and nicer for women to bathe.
Men recognised that it is not easy for their wives and daughters to bathe at home as there is no place for this. They
said it would be quite possible for them to construct a bathroom, they explained how it might look and the kinds of
materials they would use. Like the construction of toilets, the potential construction of bathrooms was not
something that was thought to require money.
Feasibility: strong. Behaviour trial: possible
2. Create shower like infrastructure to minimise water waste while bathing.
There are a range of simple shower designs that can reduce the amount of water wasted while showering. Many of
these involve a bucket or cloth bag with small holes in the base to allow only a small amount of water to come out at
a time. This idea was not explored in depth with participants so there may be additional local shower designs which
are preferred.
Feasibility: strong. Behaviour trial: possible.
Problem 5. Mothers put Vaseline on children’s faces after washing which may attract flies.
Behaviour task and context:
Vaseline was observed to be present in almost all households we observed. Commonly after bathing a baby or after
washing a child’s face Vaseline would be rubbed over the face or in some cases the whole body. In focus groups
mothers reported that Vaseline was an effective way of reducing flies or preventing them from landing on their
child’s face. It is thought that Vaseline may actually have the reverse effect, although it keeps faces looking clean and
shiny it is moist and this is likely to attract flies. For the purposes of trachoma transmission it may therefore be
beneficial to reduce Vaseline use.
Opportunities for change:
1. Reduce Vaseline use.
Vaseline use could be reduced wither through complete cessation of the product and the associated behaviour or
replacement of the project with a differ type of moisturiser that is absorbed more readily into the skin.
Feasibility: poor (belief around the benefits of Vaseline may be difficult to counter).
Behaviour trial: possible. There are two options for this 1) start with a simple test to see whether flies are attracted
to Vaseline (eg by leaving a pot in the sun) 2) do a behaviour trial where mothers stop using Vaseline or try another
product instead.
Page
48
Hand washing solutions
Problem 1. No one washes their hand after cleaning a child’s face.
Behavioural task and context:
Make handwashing after wiping a new HW moment.
There is an existing culture of handwashing. However handwashing moments were currently limited to the
following: 1) before food preparation, 2) before eating, 3) after eating and 4) after completing farm work. For the
purposes of trachoma transmission we want mothers, as well as older siblings and others who care for young
children, to always wash their hands with soap after cleaning a child’s face.
Possible approaches for changing behaviour:
1. Encourage disgust at discharge and therefore the need to clean it by washing hands.
Facial discharge is already considered disgusting. Simultaneously, however, it is seen as normal and a biological
product that attracts no dramatic action from caregivers. A behaviour change intervention could increase the sense
of disgust associated with the visible presence of discharge. This emotional response aim to influence performance
and adoption of the target behaviour. In the long term the biological cue of discharge should lead to a reactive
response of handwashing post wiping.
Feasibility: strong. Behaviour trial: no, but pre-testing of intervention design concepts should be done.
2. Build handwashing after contact with facial discharge into routines or create a ritual out of it.
Among children under 5, the presence of facial discharge is either constant or unpredictable (some days worse,
some times of day worse). Since the cue for the target behaviour is unpredictable then building it into a routine or
creating a ritual around it is unlikely to be feasible.
Feasibility: poor. Behaviour trial: no.
Problem 2. Handwashing not always done with soap.
Behavioural task and context:
Most, but not all, families have at least one bar of soap available in their house. Although people reported that they
felt they should use soap for all key handwashing occasions, it was observed that in practice it was only used by
some people and on some occasions. In general soap use was part of face, feet and hand cleaning routine each
morning (and sometimes in the evening) and was considered somewhat ritualised before and after eating (in that
the process was associated with manners and status). For the purposes of trachoma transmission we want mothers,
as well as older siblings and others who care for young children, to always wash their hands with soap after cleaning
a child’s face. However in practice it may be easier to ensure that all people always use at all key handwashing times,
on the assumption that after wiping discharge is one of these times.
Opportunities for change:
1. Make handwashing with soap easy and observable by creating a place for hand washing place where soap
and water can be stored.
Participants were somewhat familiar with tippy taps but no one was observed to have a handwashing station at their
house. In focus groups mothers did not seem that keen about building a handwashing station. They felt that animals
may steal the soap and drink the water if it was permanently positioned outside and that if you placed the soap and
water out of the reach of animals it would also be out of the reach of children. Houses are clearly demarcated spaces
Page
49
in which only close family members reside. The creation of a handwashing stand in this setting is unlikely to make
the behaviour more observable or socially judged.
Feasibility: poor. Behaviour trial: possible.
Sleeping and laundry solutions
Problem 1. (Adult) clothing is washed infrequently
Behavioural task and context:
Get all households to wash adult and child clothing regularly.
People currently wash baby clothing and other small items on a daily basis / regularly. If chlamydia bacteria cannot
survive for long on clothing, as currently believed, clothing would need to be washed daily if transmission from these
fomites is to be interrupted. This is very difficult to achieve in practice given that laundry is not done very often at
this time of year because of the amount of water and effort involved, and this is not even the time when water is at
its most scarce.
Possible approaches for changing behaviour:
1. Promote regular laundry of all adult and child clothing
An intervention could attempt to change perceptions about dirty clothing and thus hope to drive action to clean
clothes more regularly, but mothers were already aware that clothing is dirty so this may not prompt any changes
unless the important physical barriers that prevent frequent clothes washing are addressed. In the absence of a
water supply intervention that gives people household water connection it seems unlikely that people would be able
to change their behaviour even if they wished to do so.
Feasibility: poor. Behaviour trial: no.
2. Promote regular laundry of specific items of adult and child clothing
Assuming that it is not feasible to launder all items of clothing, it is relevant to consider washing small items that
may be more likely to be contaminated with chlamydia. This could include any scarves or other items that are used
to wipe children’s faces (even though it is rare it still occurs when in the field and occasionally at other times). While
baby clothing is washed daily, the clothing of slightly older children (particularly in the 3-7 year old age range) is not
washed. Extending daily washing practices to include children of this age group (who are most at risk of active
trachoma) may be possible and potentially relevant for control.
Feasibility: moderate. Behaviour trial: worth doing to try to understand which items people are willing and able to
wash.
Problem 2. Bedding is washed infrequently, while mattresses, skins and pillows may not be washed at all.
Behavioural task and context:
Get all households to wash or air items of bedding that come into contact with the face more regularly.
People currently wash blankets and sheets (if they have them) very infrequently and other items such as mattresses,
skins and old garments used as pillows may not be washed at all. Large items are unlikely to be washed more
regularly, and even if they were, this would not impact on trachoma transmission. The only interventions that are
worth considering are those that can remove chlamydia from the sleep environment on a daily basis.
Possible approaches for changing behaviour:
Page
50
1. Promote use of pillow sacks which can be washed or wiped on a daily basis
Most households put something under the head when sleeping. Although this is not always considered necessary for
children, they often sleep together with their parents when very young. Old garments are bundled together and it
might be feasible to encourage families to place the clothes into a rice sack or cloth pillow that could then be easily
washed or wiped on a daily basis. A trigger such as nurture could be used to persuade mothers that what is placed
next to their child’s head at night matters. It may also be feasible to discourage parents from covering a child’s head
at night with a blanket that is not going to be washed (although it may be more relevant to encourage face washing
at night if heads are covered with blankets).
Feasibility: moderate (and perhaps more beneficial if the main effort is focussed on ensuring faces are clean before
bed). Behaviour trial: yes. Many different options are possible and it is worth trialling some of them (e.g. put
garments in a cloth bag and wash the bag, put garments in rice sacks and wipe the sacks). Further exploration of
where pillows are placed in relation to sheets (over or under) is also necessary. Product development could also be
considered to explore other materials that would be easy to wipe clean but which would feel comfortable to sleep
on.
2. Encourage daily airing of all bedding in the sun
This is already practiced for some items in some households and could be quite easily promoted if it is considered a
viable intervention (i.e. if UV exposure kills chlamydia).
Feasibility: good. Behaviour trial: yes, to see which items should be aired and understand the acceptability of this.
The biological plausibility of this should also be explored in such a trial.
Problem 3. Young children sleep with adults and share bedding and pillows.
Behavioural task and context:
This behaviour is common and there are a number of barriers to changing it (issues of cost, cold weather, space in
the home, etc). Ideally, people would sleep further apart and use separate items of bedding that are ‘theirs’.
Possible approaches for changing behaviour:
1. Promote different sleeping arrangements for young children
It is unlikely that this can be changed for very young children who are kept near the mother for warmth and in case
they cry in the night.
Feasibility: poor. Behaviour trial: no.
2. Promote use of separate blankets and pillows
It may be possible to encourage clusters of individuals who sleep together to use separate pillows if separate
blankets cannot be afforded. This may reduce direct transmission at night from one person to another. As heads are
often covered with blankets at night, as described for problem 2, this may not reduce risk of transmission, but it is
unlikely that covering the head can be changed, as even if it is not done deliberately, it may occur during the night.
In some households all belongings are shared, including items of bedding. Encouraging individual ownership of
pillows, even if there are insufficient blankets to go around, may not make any different to transmission if chlamydia
does not survive on bedding from one night to the next.
Feasibility: moderate. Behaviour trial: yes. In addition to promoting use of pillows that can be cleaned, it could be
worth trialling use of separate pillows.

Page
51
Presence of flies (sanitation) solutions
Problem 1. No households had improved toilets and sanitation coverage was poor.
Behavioural task and context:
Achieve safe disposal of all human faeces in homes.
Sanitation coverage is low and existing latrines are poorly constructed under duress. Faeces and flies are found
there. Young children defecate in the compound and faeces is not always moved. It is also acceptable for adults to
defecate within the compound or in nearby fields. Faeces is not covered. The close proximity of open defecation
sites and poorly constructed and unhygienic latrines mean that the current environment is ideal for the breeding of
Musca sorbens flies.
Possible approaches for changing behaviour:
1. Sanitation promotion (demand creation) using emotional drivers of behaviour
Latrines are constructed to avoid fines. Promotion currently involves telling people about the health benefits of
having a latrine. There is considerable work to be done to reverse the poor work which has already taken place.
Uptake and use of latrines (including for disposal of all faeces) could be driven through development of an
intervention that using emotional drivers of behaviour.
Feasibility: good in areas without sanitation coverage, unknown in areas where latrines exist and are not used.
Behaviour trial: further work would need to be done to develop and pre-test appropriate intervention materials to
drive latrine construction, and ultimately use.
2. Sanitation promotion through CLTS
It is unclear exactly where and how CLTS is being rolled out in this area, but there is the potential to use the CLTS
model to drive uptake of sanitation.
Feasibility: good if the programme and resources exist in this area. Behaviour trial: the existing model can be used,
although it may be worth additional work to encourage covering of faeces if there are insufficient resources for a full
sanitation promotion intervention at present (we appreciate the disadvantage of such a strategy from the
perspective of diarrhoea and other NTD control).
Problem 2. Flies are found in the home environment, in particular in association with animals.
Behavioural task and context:
Create a fly free home and compound environment
Flies are not a big problem inside the homes, and they are mainly drawn to humans and animals in the environment.
There is a lot of waste scattered within compounds and placed in specific places, none of which are far enough away
to keep flies away from the compound. However, waste is predominantly dry and did not seem to attract flies. This
does not seem to be a big problem that needs addressing.
Possible approaches for changing behaviour:
1. Reduce flies around animals
It is unlikely that anything can be done here, as animals are kept close to the home for security and every household
has animals.
Feasibility: poor. Behaviour trial: no.
Page
52
2. Promote clean compounds as well as houses
Houses are well-kept. Elsewhere, an intervention designed to change the entire kitchen set-up succeeded in
improving food hygiene practices. It could be worth exploring whether a similar type of makeover is possible in
people’s homes here, in particular in the compounds.
Feasibility: moderate. Behaviour trial: would be worth studying further to think how the environment could be
changed and what impact this could potentially have on trachoma transmission, and thinking about whether fly
traps would be beneficial.
Problem 3. School sanitation is unhygienic
Behavioural task and context:
Create clean latrines in public areas e.g. those used by students during school hours and at health facilities
In the school and health facilities that was visited the latrines had been well-constructed by there was no soap and
water available and faeces and flies were everywhere in the surrounding environment. The current latrines are
exceedingly unpleasant. As well as a potential fly breeding ground, these latrines are likely to be a focus for
transmission for many faecal-oral diseases. If children are taught about trachoma in trachoma clubs at school, the
poor status of the existing sanitation could undermine any other programme activities. Toilets at schools should be
of a high standard so that they are in some ways ‘aspirational’ and may drive sanitation uptake in the home.
Furthermore, health centres should set an example for the community and this should be an achievable goal.
Possible approaches for changing behaviour
1. Use ‘nudges’ to encourage desired behaviour
Robert Dreibelbis and colleagues have successfully increased handwashing with soap behaviour in schools using
environmental stimuli to act as cues and aid habit formation [33].
Feasibility: good if water is available. Behaviour trial: yes, but would require some investment to trial this properly
in a school
2. Create a ‘toilet task force’ to keep toilets clean
This study did not explore school sanitation in any depth, so it is unknown whether other schools lack suitable
facilities, or whether the existing facilities are unhygienically managed (as in this study). In the Dreibelbis study, the
school caretaker voluntarily filled up the water tank for handwashing and children happily commented when the
water was low. A system would need to be established to ensure latrines were kept clean and well maintained.
Feasibility: moderate, dependent on individuals. Behaviour trial: yes, although more work in schools is needed first.
Considerations for intervention design and delivery
Implications of current trachoma elimination activities Although knowledge on trachoma is still poor in these communities this does not necessarily mean that an
effort to increase face washing and improve environmental hygiene should focus on increasing knowledge
on trachoma. Adoption of these practices could be achieved through behaviour drivers only.
Work on the “F” and “E” components may present an opportunity to collaborate and pool the resources,
skills and reach of other government and NGO partners. This is a particularly plausible option for tackling
sanitation demand.
While schools present an opportunity to lead by example (eg. improved sanitation, soap and water access)
and positively reinforce key behaviours (eg. face washing, handwashing, and clean general appearance
Page
53
associated with clothes washing) an intervention targeted only at schools is unlikely to substantially effect
transmission. This is partly because you are only reaching older children who are the ones going to school
but also because the key behaviours need to occur in the household and involve all family members. Having
said this, older children can be useful agents of change (e.g. grandmothers and fathers reported that they
enjoyed learning from student-age children in their households) and are still involved in the care of younger
siblings.
Implications of community perceptions The community leadership and key structures such as schools already feel that health is one of the most
important issues for their community. Trachoma is also seen to be a leading health issue in these areas. This
provides a helpful building block for future programs.
Any intervention to control trachoma is likely to have to target the whole family. This is because women are
primarily responsible for activities and behaviours that are associated with Trachoma transmission. Children
are highly involved in caring for their younger siblings and also sleep in close proximity to each other. Lastly
husbands are likely to be key because they may make decisions for the households, control most of the
money and be critical for the construction of latrines or bathrooms.
Interventions may have to be sensitive to the cultural perceptions of what determines behaviour (ie. that it
is determined at birth).
There may be an opportunity to capitalise on the fact that guests receive special treatment since this has
specific implications for bedding and cleanliness. Perhaps it is possible for people to maintain this level of
cleanliness by heightening the emotion associated with feeling underprepared for when an unexpected
guest arrives.
Behaviour change interventions that hinge on concepts such as gossip or social judgement (affiliation
motive), celebrity culture or role models (status motive) and the ideal mother character (nurture motive),
may not work so well in these communities since these concepts are less salient, culturally acceptable or in
the case of the ideal mother, it is seen as being distant to everyday realities. That is not to say that using the
affiliation, status and nurture motives in new novel ways might not be effective.
All households had a mirror, almost always hung on a hook or kept in a cubby hole. People were aware of
their appearance and men, women and children were observed to look in the mirrors, although mirrors were
said not to be kept outside because of the sunlight, so use of mirrors in face washing stations may not be
acceptable.
Implications of community structure and touchpoints Communities in this area are quite highly structured at an administrative level. However, many of these
structures are historically linked to oppression and the enforcement of law so associating trachoma with
them may carry some risk.
One-to-five groups appear to be the structure which is most likely to reach all members of the community.
It is quite possible that the pregnant mothers’ groups could be used as an opportunity to influence
behaviour. It is likely that current practices around the daily bathing for young children, have been
influenced by health workers speaking to mothers about this in this setting.
The fact that holidays are associated with a heightened need for purity could provide an opportunity to build
on this belief. For example, it could be suggested that every Sunday is a kind of holiday and so all of these
practices normally done on special occasions should also be done every week.
It would be interesting to do further exploration of the savings and loan structures in the community.
Currently people felt that these groups could not be used for saving money to build a toilet. Partially this was
also because the felt there were not many costs associated with building a toilet. However, if there were to
be an effective sanitation program that effectively drove up demand for improved latrines there would be a
greater cost incurred at a household level. Saving for this through a group structure can help support
everyone to build toilets and apply pressure on those who are slow to adopt.

Page
54
In these communities women tended to spend the majority of their day around the home. To some extent
women do interact socially while at the water point, during Zeker and other coffee ceremonies, but generally
there are few opportunities to get dressed up or be seen to be clean and smart. The absence of these social
events is likely to result in reduced social judgement and a de-prioritisation, by mothers, of their own
hygiene practices. This is something a behaviour change program may seek to change. It might be possible to
instil a new ritual of face washing around coffee drinking.
Homes are quite far apart and separated by fences, which makes it hard to observe the behaviour of
neighbours, adding to the argument that social judgement is unlikely to change behaviour here.
Implications of context Literacy is very low, and caregivers of children under-five had not had any schooling so materials should be
appropriate for this situation.
Ethiopia is striving to achieve universal access to sanitation by 2018. This goal is measured using an indicator
for coverage, but (hygienic) use is not tracked. There is less incentive to ensure sanitation programmes are
well-designed and to assess behaviour change so this would need to be addressed.
People are very house proud and have many decorations, even when they are poor; it may be possible to
encourage similar behaviour in relation to the compound environment.
Limitations It is important to recognise that this is a formative research report and, while rich in descriptive data, a small number
of communities and households were studied. Although we cannot say that saturation has been achieved with this
sample, the study paints a good picture of patterns of behaviour. Further, as the communities included were
purposively selected to reflect differences in accessibility, sanitation coverage and levels of trachoma, these
households and communities do not represent the whole of Oromia region and findings have to be interpreted with
caution.
It was not possible to conduct observations late in the evening to observe actual face washing and other practices at
this time of day. Reactivity due to the presence of a Western observer is possible, although households were
consented on the day of observation and did not have the opportunity to clean the environment before the start of
observation. As events of interest were seen to be carried out by young children it is less likely that their behaviour
has been influenced by the presence of an observer. Socio-economic status and education level have been
associated with increased reactivity, further suggesting that much of what has been observed was ‘real’ behaviour.
As water availability and climate vary throughout the year it is possible that the findings would have been very
different if the study had been conducted at a different time.
Conclusions and recommended next steps This piece of formative research provides information on the current practices related to behaviours of potential
importance in trachoma transmission. A number of opportunities for behaviour change are suggested and discussed
in the context of the potential to interrupt transmission. The feasibility and potential impact of these solutions varies
as there are multiple potential routes by which trachoma can be spread and it is unknown which of these is the most
important. It may be less relevant to focus efforts on encouraging more frequent laundry of bedding than to invest
time in sanitation promotion to establish an open defecation free environment and to encourage safe disposal of all
human faeces in latrines with drop-hole covers. School sanitation should not be neglected. Given the source of
infection on a person is nasal and ocular discharge, encouraging new habits to develop for face washing so that the
faces of all household members are washed with soap on multiple occasions throughout the day should be a priority.
It may be possible to encourage face washing before bed and complement this initiative with promotion of separate
pillows for each household member. It is also worth exploring how to make nasal and ocular discharge appear more

Page
55
disgusting to try to trigger appropriate action (e.g. wiping and handwashing) in response to this visible cue.
Promotion of bathing shelters may also encourage more frequent bathing and thus face washing, although it would
be important to understand how water scarcity at other times of behaviour would affect this and other hygiene
practices. A number of context-specific behaviour change techniques for each of these strategies are proposed and
warrant further development through behaviour trials and piloting of concepts.
The following next steps are worth considering in light of the study findings:
Additional formative work in i) a different location and ii) at a different time of year
Evaluation of the ongoing Fred Hollows Foundation - Ethiopia activities in Schools with a view to modifying the Trachoma Clubs and improving sanitation facilities
Review of CLTS / sanitation programmes in Fred Hollows Foundation - Ethiopia areas
Workshop to review findings and agree priorities for behaviour change in the form of a “Creative Brief” that summarises the behaviour gaps and sets out the behavioural tasks
Behaviour trials to assess acceptability and feasibility of some potential intervention strategies
Microbiology to understand the role of clothing and bedding in transmission (?)
References 1. Resnikoff, S., et al., Global data on visual impairment in the year 2002. Bull World Health Organ, 2004.
82(11): p. 844-51. 2. Emerson, P.M., et al., Review of the evidence base for the “F” and “E” components of the SAFE strategy for
trachoma control. Trop Med Int Health, 2000. 5(8): p. 515-27. 3. Hu, V.H., et al., Epidemiology and control of trachoma: systematic review. Trop Med Int Health, 2010. 15(6):
p. 673-91. 4. Dolin, P.J., et al., Trachoma in The Gambia. Br J Ophthalmol, 1998. 82(8): p. 930-3. 5. Evans, J.R. and A.W. Solomon, Antibiotics for trachoma. Cochrane Database Syst Rev, 2011(3): p. CD001860. 6. Yorston, D., et al., Interventions for trachoma trichiasis. Cochrane Database Syst Rev, 2006(3): p. CD004008. 7. Rabiu, M.M., N. Muhammed, and S. Isiyaku, Challenges of trachoma control: an assessment of the situation
in northern Nigeria. Middle East Afr J Ophthalmol, 2011. 18(2): p. 115-22. 8. Emerson, P.M., et al., Transmission ecology of the fly Musca sorbens, a putative vector of trachoma. Trans R
Soc Trop Med Hyg, 2000. 94(1): p. 28-32. 9. Taye, A., et al., Seasonal and altitudinal variations in fly density and their association with the occurrence of
trachoma, in the Gurage zone of central Ethiopia. Ann Trop Med Parasitol, 2007. 101(5): p. 441-8. 10. Emerson, P.M., et al., Human and other faeces as breeding media of the trachoma vector Musca sorbens.
Med Vet Entomol, 2001. 15(3): p. 314-20. 11. Emerson, P.M., et al., Role of flies and provision of latrines in trachoma control: cluster-randomised
controlled trial. Lancet, 2004. 363(9415): p. 1093-8. 12. Rabiu, M., et al., Environmental sanitary interventions for preventing active trachoma. Cochrane Database
Syst Rev, 2012. 2: p. CD004003. 13. Ejere, H.O., M.B. Alhassan, and M. Rabiu, Face washing promotion for preventing active trachoma. Cochrane
Database Syst Rev, 2012. 4: p. CD003659. 14. Stocks, M.E., et al., Effect of water, sanitation, and hygiene on the prevention of trachoma: a systematic
review and meta-analysis. PLoS Med, 2014. 11(2): p. e1001605. 15. Harding-Esch, E.M., et al., Risk factors for active trachoma in The Gambia. Trans R Soc Trop Med Hyg, 2008.
102(12): p. 1255-62. 16. Zack, R., et al., Issues in defining and measuring facial cleanliness for national trachoma control programs.
Trans R Soc Trop Med Hyg, 2008. 102(5): p. 426-31. 17. Cairncross, S. and R. Feachem, Environmental Health Engineering in the Tropics. An Introductory Text. (2nd
ed.) Chichester: John Wiley & Sons. 4-7. 1993. 18. Sahlu, T. and C. Larson, The prevalence and environmental risk factors for moderate and severe trachoma in
southern Ethiopia. J Trop Med Hyg, 1992. 95(1): p. 36-41.

Page
56
19. H., T., Trachoma. A blinding scourge from the Bronze Age to the Twenty-first century. Pub. Center for Eye Research, Australia., 2008.
20. Mabey, D., Reader Comment: No good evidence to support water, sanitation or hygiene interventions for the control of trachoma. PLoS Med, 2014. Available: http://www.plosmedicine.org/annotation/listThread.action?root=80008. Accessed June 2015.
21. Centre, T.C. Ethiopia - Controlling Trachoma. 2015; Available from: http://www.cartercenter.org/countries/ethiopia-health-trachoma.html.
22. Trachoma Atlas. Ethiopia Country Profile. 2015; Available from: http://www.trachomaatlas.org/maps/ethiopia.
23. World Bank. Country Data: Ethiopia. 2015; Available from: http://data.worldbank.org/country/ethiopia. 24. Joint Monitoring Program - WHO/UNICEF, Ethiopia: estimates on the use of water sources and sanitation
facilities (1980 - 2012). 2014. 25. Yemane Berhane, et al., Prevalence of Trachoma in Ethiopia Ethiop.J.Health Dev. , 2007. 21 ((3) ). 26. Tansy Edwards, et al., Impact of Health Education on Active Trachoma in Hyperendemic Rural Communities in
Ethiopia. American Academy of Ophthalmology 2006. 27. Curtis, V., L.O. Danquah, and R.V. Aunger, Planned, motivated and habitual hygiene behaviour: an eleven
country review. Health education research, 2009. 24: p. 655-73. 28. Aunger, R. and V. Curtis, The Evo-Eco approach to behaviour change. Applied Evolutionary Anthropology, ed.
by David Lawson and Mhairi Gibson. Springer, pp. 271-295. Available http://www.hygienecentral.org.uk/pdf/aunger-curtis-the-evo-eco-approach.pdf. Accessed Apri 2014., 2014.
29. Aunger, R. and V. Curtis. A Guide to Behaviour Centred Design. 2015. 30. Braun, V. and V. Clarke, Using thematic analysis in psychology. Qualitative Research in Psychology, 2006.
3(2): p. pp. 77-101. 31. Biran, A., et al., Effect of a behaviour-change intervention on handwashing with soap in India (SuperAmma):
a cluster-randomised trial. Lancet, 2014. In print. 32. Hayes, N., Theory-led thematic analysis: social identification in small companies. In N. Hayes, in Doing
Qualitative Analysis in Psychology. Hove,. 1997, Psychology Press.: UK. 33. Dreibelbis, R., et al., Behavior Change without Behavior Change Communication: Nudging Handwashing
among Primary School Students in Bangladesh. Int J Environ Res Public Health, 2016. 13(1).
Appendices
A Research questions
B Structured observation notes and pictures
C Focus group discussion guides

APPENDIX A. OVERVIEW OF RESEARCH QUESTIONS AND METHODS
Topic Research Questions Method Detailed Notes
Water use
What are the current practices regarding water use for hygiene purposes (i.e. hand / face washing, bathing, and laundry)?
Unstructured observation for 2 days.
Semi-structured observation for 4 hours.
Asset inventory.
This will include going with HH members to water points to observe water use there, observing the types of water containers available, water storage and use throughout the day and the availability and use of soap and tissues or rags.
How much water is collected on average per family, per day and how is it prioritised?
Unstructured and Semi-structured observation.
In depth interviews with families following observations.
In depth interviews with primary caregivers and heads of household.
Assessed first by asking the participants how much water they collect for the family per day. Small cups will be used to visually represent this (ie 4 buckets would be represented by 4 cups). Given what they currently access they will be asked to explain how they prioritise the water. The research should then change the situation by adding or removing ‘buckets’ to see how water use priorities may shift when the family access more or less water than they do currently.
Who (and what) gets washed / wiped, by whom, where and when and using what?
If going to face wash when is this possible?
Unstructured observation for 2 days.
Semi-structured observation for 4 hours.
Asset inventory.
This will include identifying what materials and products are used for washing and wiping, whether they are used repeatedly and by different people.
How much water do people think is needed for face / hand washing?
In depth interviews with primary caregivers and heads of household.
Focus group discussions.
Identify commonly available local containers and ask participants to estimate first how much water they feel they should use to wash their face and then actually get them to try. Then ask how they think they could conserve water.
How socially important is it to be clean / have a clean face, and for children to be clean?
In depth interviews with families following observations.
In depth interviews with primary caregivers and heads of household.
Use images of people who look like they could be from the local area. They should have different levels of visible cleanliness and appearance. Participants should be asked to draw conclusions about the type of person in the picture, what their family is like, what their home environment is like.
How does it feel to be clean / have a clean / dirty face / and to wash hands? When during the day is this most important?
In depth interviews with families following observations.
In depth interviews with primary caregivers and heads of household.
Ask people to demonstrate how they would normally wash their hands or wash their face. Get them to describe how the feel immediately after.
Is sufficient water available for hygiene purposes throughout the day and how
Unstructured observation for 2 days. Document when water is collected, by whom, how many times per day and from where, and how long a round trip takes; how much water is available per HH member and how much water is available in the

does this vary at different times of year? Semi-structured observation for 4 hours.
Asset inventory.
In depth interviews with families following observations.
evening, early morning?
Is it acceptable to re-use water? Unstructured observation for 2 days.
Semi-structured observation for 4 hours.
In depth interviews with families following observations.
In depth interviews with primary caregivers and heads of household.
Focus group discussions.
Was any water re-use observed? How was it re-used, by whom and under what circumstances? Otherwise ask if this ever happens or if it would be acceptable for it to happen? Have participants heard of others in their community doing this and if so what do they think of these people?
Sanitation practices
What are the current sanitation and child stool disposal practices?
Unstructured observation for 2 days.
Semi-structured observation for 4 hours.
Asset inventory.
Identify type of latrine if latrine is present and who it is used by and whether it is always used. Document how child faeces is disposed. Document practices around open defecation (ie where it takes place and whether it is buried) or defecation outside of the home environment. Understand whether the HHs were exposed to CLTS triggering
What are people’s attitudes towards improved sanitation
In depth interviews with families following observations.
In depth interviews with primary caregivers and heads of household.
Focus group discussions.
How do people feel when they use a toilet, what are the smells/feelings/sensations/risks they associate with it. This may be done through free-listing using cards. These could then be used to explore how sanitation practices be modified or improved in simple acceptable ways
Flies
Are flies observed on people’s faces and is any action taken to remove them from faces or the surrounding environment, particularly when living near animals?
Unstructured observation for 2 days.
Semi-structured observation for 4 hours.
Asset inventory.
Document who flies are landing on and how this relates to observed hygiene practices, when are they most common and how do individuals or caregivers react to flies. Are there an devices which are used to get rid of flies or any attempts to keep flies out of certain areas.
How do people perceive flies and other insects?
Why do people think there are flies around?
In depth interviews with families following observations.
In depth interviews with primary caregivers and heads of household.
How do people feel when flies land on them? What words do people associate with flies.
Crowding and sleeping practices
Where and how closely are children and other family members currently sleeping?
Unstructured observation for 2 days.
Semi-structured observation for 4 hours.
Asset inventory.
Document bedding materials, whether these are shared or individual. Ask whether sleeping arrangements vary and what factors contribute to this, how frequently are bedding materials cleaned or washed?

In depth interviews with families following observations.
What opportunities are there to change sleeping practices to reduce trachoma transmission
In depth interviews with primary caregivers and heads of household.
Focus group discussions.
Are there certain cultural rules around sleeping arrangements? What would be the ideal sleeping arrangement? Would it be acceptable for sleeping practices to change? Would it be acceptable for children to have their own bedding which only they use? These questions can be explored through getting groups to draw out typical sleeping arrangements and then considering how to adjust them.
Laundry practices
How often is laundry done generally and does this always include washing things like often are towels, bedding, and cleaning rags washed
Unstructured observation for 2 days.
Semi-structured observation for 4 hours.
Asset inventory.
In depth interviews with families following observations.
Document or ask about laundry practices including frequency, how much water is used, type of soap used, who does it, where it is done/hung, what items are washed most frequently? How often are things like bedding, towels and cleaning rags washed.
How do people feel about having clean things? What drives their desire to do laundry?
In depth interviews with families following observations.
In depth interviews with primary caregivers and heads of household.
How do people feel when they use something clean for the first time? How do they feel in contrast when they have to use something dirty? What are the factors that enable or constrain their ability to do laundry? What things or experiences would make them think ‘oh I really have to do the laundry now’?
Use images of people who look like they could be from the local area. They should have different levels of visible cleanliness and appearance. Participants should be asked to draw conclusions about the type of person in the picture, what their family is like, what their home environment is like.
Direct contact
In what other ways do adults contact children and do children contact each other / play?
Unstructured observation for 2 days.
Semi-structured observation for 4 hours.
Document interactions between children in the home and between adults and children in the home. Other than playing, what forms of direct contact exist?
Religion
How does religion influence hygiene practices?
In depth interviews with families following observations.
In depth interviews with primary caregivers and heads of household.
Does your religion guide you on what you should or should not do in relation to any of the key target behaviours?
Touch points
What communication channels exist to reach people in this area? What are all the social and community structures that exist and any other potential ‘touch points’ that future community interventions could utilise?
In depth interviews with families following observations.
In depth interviews with primary caregivers and heads of household.
The researchers should work with the participants to use a visual mapping process for identifying channels. Particularly explore schools and structures as a way of reaching children and in turn families.
Manners Are local understandings of manners associated with some or all of the hygiene and sanitation practices that may contribute to trachoma transmission?
In depth interviews with primary caregivers and heads of household.
Ask how would you describe a well-mannered child? What lessons do you try to teach your child about how to behave? Is it embarrassing if others see you doing or not doing X behaviour? What kinds of things do people normally gossip about in your community?
Would others laugh at you if they saw you doing or not doing X behaviour? Use card piling to associate the

sub-optimal hygiene and sanitation behaviours with manners.
Ideal roles of men, women and children
Are any of the hygiene and sanitation practices that may contribute to trachoma transmission associated with aspirational ideals of ideal mothers/father/children?
In depth interviews with primary caregivers and heads of household.
Can you describe the characteristics of an ideal wife/mother in your community? Can you describe the characteristics of an ideal husband/father in your community? Can you describe the characteristics of an ideal child in your community? How would you describe your community to others? What makes a good community? How far are all of the ideals to the norm in their community (ie the way they actually view others and their community)
Ownership and hoarding
Are household things related to hygiene and sanitation owned (ie used by only one person) or shared
Unstructured observation for 2 days.
Semi-structured observation for 4 hours.
Asset inventory.
In depth interviews with families following observations.
Document practices in regards to who uses soap/s, face cloths and bedding and whether these are shared? Are there other household items that are only able to be used by one person – what are these and why are they different from other things?
How is ownership perceived and what opportunities are there to change the way products are used and owned?
In depth interviews with primary caregivers and heads of household.
Focus group discussions.
What socio-cultural ideas are associated with sharing things or independent use of things? Present FGD groups with potential ideas for individual ownership of hygiene related products (ie individual face cloths) and get feedback on whether these are likely to be feasible and acceptable.
Motives Are motives such as comfort, attract, nurture, and status are likely to be associated with the behaviours of interest?
In depth interviews with primary caregivers and heads of household.
Focus group discussions.
Ask what times of the day do you feel most content/happy/proud of with yourself?
Use images of people who look like they could be from the local area. They should have different levels of visible cleanliness and appearance. Participants should be asked to draw conclusions about the type of person in the picture, what their family is like, what their home environment is like. Using these ask participants rank the characters according to different criteria such as which character they think they are most like, who they would most like to be, who they think is most attractive, who they think is most influential and who looks like the best mother?
Get participants to trial some of the target behaviours and explain how they feel immediately after. This may include washing their face using a mirror, the difference between washing their face with and without soap, using a face wipe etc.
Perceptions of blindness
What are the perceived social costs and consequences of blindness?
In depth interviews with primary caregivers and heads of household.
Ask people to imagine that someone in their family loses their sight. How would this change their role in the family, the things they do, the way they contribute to the community and the way they are viewed. Do they know people who are blind? How would they describe those people? Is blindness seen as something that is natural/avoidable/treatable? Explore the extent to which fear and discomfort in the future may motivate current behaviour.
Commodities What commodities are available in the local area? What commodities are commonly bought by most HHs
In depth interviews with families following observations.
In depth interviews with primary caregivers and heads of household.
Focus group discussions.
Ask people to free list all the things available in the local shop/market. Ask them which items they usually buy and which items they think other people usually buy. Explore who buys the other ‘non-normal’ items. Invite FGD participants to trial certain products related to the behaviours and ask about whether they would be likely to purchase such good if they were available and how much they would pay for them (and example of this may be mirrors or face wipes)
Page
61
APPENDIX B. UNSTRUCTURED OBSERVATION NOTES FROM
OBSERVATION IN 10 HOUSEHOLDS IN 5 COMMUNITIES
COMMUNITY A: HOUSEHOLD 1
Friday 15th January
Household Composition: Grandparents living with 13yr and 6 yr old girl and 20yr and 18 yr old boy + second house
with 1 son and his wife and their 5 yr old son.
General Observations / Comments:
Note: grandmother declined to have photos used for the report
Women are from home collecting water when we arrive and Head of Household gives consent. Women are
consented when they return with water. Children are washing faces with soap when we arrive so this is
definitely not for our benefit.
Defecation is open and usually close to the compound / within it but not in the main living space
HH doesn’t lack water, collect 5 jerry cans per day
They seem quite wealthy. They have electricity (light only) but say it usually doesn’t work. They have a
mirror on the wall at the inside entrance of the HH. They have shower gel and liquid soap and a lot of bar
soap.
Lots of face washing seen and soap used – hair and face are washed twice with soap which seems a little
excessive.
Lots of flies and animal faeces in compound; lots of kids sitting around together and playing – how to change
the presence of flies?!
Men / boys and kids generally sitting around. The grandfather was quite busy.
Not seen any face wiping at all today. Some kids snotty and sneezing but no action taken.
Flies on faces of some kids
Kids interact a lot, adults are also quite tactile with the kids but not the grandparents.
Coffee ceremony – incense is burned and two cups of coffee are drunk
The daughter-in-law was more ‘modern’ than the grandmother
No items are owned just by one person, everything can be used by everyone; blankets for sleeping are
shared
Events undertaken during observation period:
Time Activity
07:45 As we arrived we saw 13yr old girl and 18yr old boy washing legs, feet, arms and face with soap in a bucket outside the house while dressed for school
07:50 Boy and girl left for school directly as we arrived
07:58 5yr girl and 6yr boy washed hair with soap – spent a long time doing this, lots of lather. One urinated. No soap used on face
08:00 Father left to the field behind the house 08:10 Daughter-in-law returned with water on her back (25L) and leaves in her hand
08:14 Daughter-in-law agrees to participate – gives her chilld an egg from chicken coup and goes in house to feed the chicks
08:15 6 yr old brings out a hand mirror and uses it to apply Vaseline (?) to hair
08:22 G’mother returns home with water (25L) and leaves – agrees to participate
08:28 We go with G’mother & DIL back to water point to collect second jerry can she had filled and left at the WP
08:38 Arrival at water point

Page
62
08:50 Reach the house – we have 20L of water this time.
08:55 DIL returns with water
08:56 G’mother clears ashes from the fire
09:00 DIL lights fire (brazier) with a match
09:05 Both women sweep
09:14 DIL washes hands in small bucket after cleaning house
09:16 G’mother washes hands and arms with just water in a bucket
09:17 DIL starts cooking on brazier
09:18 G’mother washes face with water
09:20 G’mother puts pot on stove to boil water for wat – uses straw for firewood
09:30 6 yr girl returns with firewood. Cows are walking through the compound and they drink soapy water from the bowl where everyone bathed. Cows are given more water in this bowl too
09:34 5yr boy eats inside the house; DIL is still cooking more food as her husband is coming later
10:18 After a quiet period DIL washes scarves in bowl using liquid soap (27 birr); they also have shower gel and this is shown to us (17 birr)
10:25 Child drinks
10:28 G’father returns with hay
10:32 DIL cleans the floor with dung using her hands and water (not seen what she did after)
10:36 G’mother adds pesticide to their large store of grain
10:45 We are called to eat with the DIL, her husband and brother (we shared our food with theirs) – everyone rinsed hands before and washed with soap after eating
11:00 DIL cleaned the dishes, washing one into another – no soap (?)
11:06 G’mother sorted out grains inside the house
11:18 DIL leaves house to visit sister
11:28 G’mother started up the fire in a separate building with a stove just for njera
11:45 She is making njera on the hot plate – the DIL returns and leaves to the shop to get sugar
12:00 DIL returns
12:08 DIL starts making coffee by cleaning the beans
12:26 Child 5yrs boy eats mango; DIL washes cups for coffee (water only) 12:27 Girl 6yrs takes a cup of water and washes her face in compound
12:29 DIL pounds the coffee beans
12:33 Girl 13yrs returns from school
12:34 Girl 6 yrs and then G’father and 13yr girl eat in the other house – hands washed with water before – not seem after
12:49 5 yr boy given a bath with soap – twice and very thoroughly – by his father who scrubs him and uncle who pours the water. He said do it twice to clean properly
12:59 5 yr old boy sits cuddled up with father
1:19 Coffee is ready
1:30 DIL washes coffee cups (one into the other using the same water and her hands) and bouls water for more coffee
1:38 G’mother left – didn’t say where to
2:00 G’mother returns with leaf for njera
2:11 More coffee is prepared and then washed in the same way by the DIL
2:14 G’mother prepares njera with the leaves to separate each one
2:16 Women both sort dried leaves
2:19 Kids play ball together
2:23 DIL peals onion and washes dishes (again with water only) and cooks until 3pm when stop
2:30 G’mother sieves teef (until 3pm when stop) 3:05 5yr old boy eats again
Selection of photos from observation in this household:

Page
63
Child washing hair (with soap) with aid of a sibling
View of compound
Water
point
Mother
washes
scarves and hangs them out using little water and liquid soap
(only house seen with soap like this)

Page
64
Child given a full bath with excessive soap (washed
twice) by father and uncle
COMMUNITY A: HH2
General notes:
The family had three children, a 15 yr old boy (not present during observation), a 13 year old girl and a 1.5
year old boy. The father left to go to the fields and graze cattle as was therefore absent for most of the
observation. The 13 year old attended school during part of the observation.
The family shared the compound with the husband’s brother’s family.
The family were preparing for the funeral of the father’s mother.
The family had one building which was divided into 3 rooms. The kitchen was outside behind the house and
animals were kept alongside the house.
The family had 3 25L jerry cans which were full of water in the morning. Two of these were kept in the house
and one was kept on the porch. At least 6 other 10L Gerry cans were observed in the house.
The family had 2 cows and two donkeys.
There was no toilet at the house. All family members defecated in the compound behind the houses. Human
and animal faeces was observable in the compound and was uncovered.
Flies were observed to be on the faces of young children – often more than 5 flies on the face at one time.
Those with more observable discharge had more flies.
Few flies were observed to be on the cow dung. Almost no flies were observed to be inside the house or
around the kitchen.
There was a high level of interaction and physical contact between neighbours and children. Older children
take a dominant role in caring for younger children.
The waterpoint was an Afridev pump and was located 12 minutes walk away. There was no queue to get
water. The pump area was walled with branches and is only open at certain times of the day.
Food was very well covered with lids and plastic bags.
The family had functioning electricity, a radio and a mobile phone.
The family has no bar soap. They have powdered soap which is used for laundry and occasionally for dishes.
This is kept in a bottle in the kitchen.
They use 3 gerry cans of water to undertake their normal daily activities.
Time Observed action 7:55am Observation starts. All family members are awake. Daughter leaves for school. Mother washes dishes and prepares
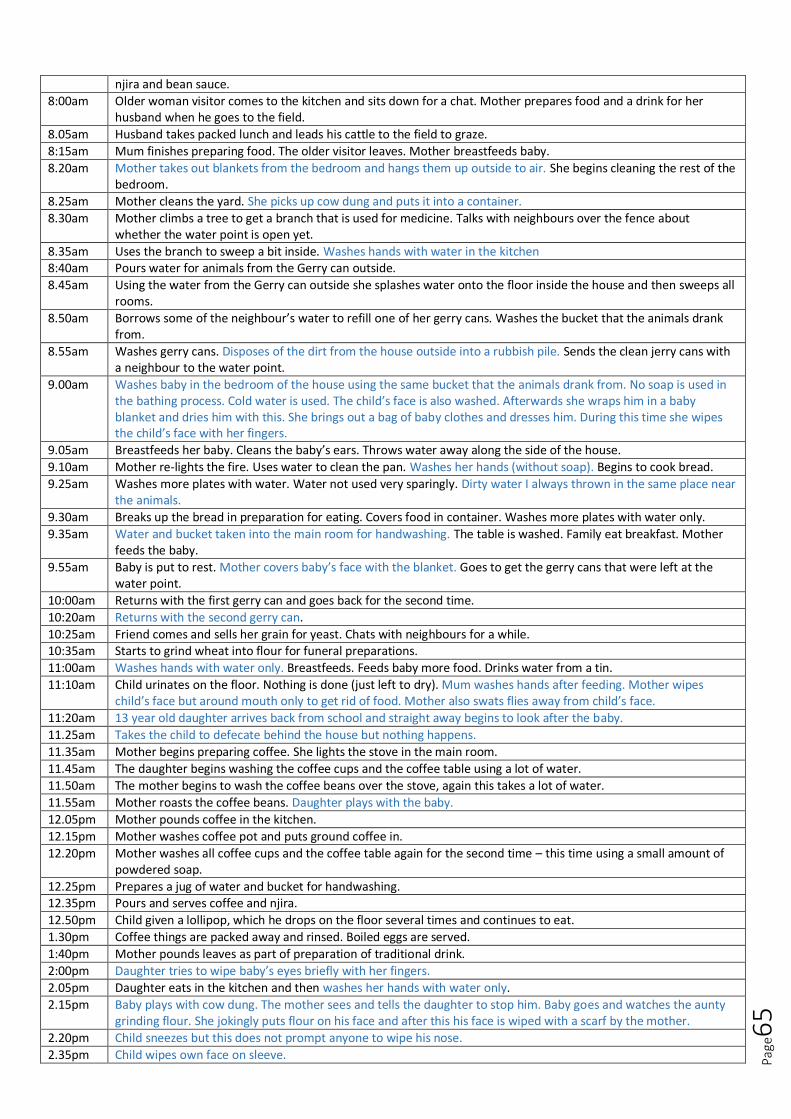
Page
65
njira and bean sauce.
8:00am Older woman visitor comes to the kitchen and sits down for a chat. Mother prepares food and a drink for her husband when he goes to the field.
8.05am Husband takes packed lunch and leads his cattle to the field to graze.
8:15am Mum finishes preparing food. The older visitor leaves. Mother breastfeeds baby.
8.20am Mother takes out blankets from the bedroom and hangs them up outside to air. She begins cleaning the rest of the bedroom.
8.25am Mother cleans the yard. She picks up cow dung and puts it into a container.
8.30am Mother climbs a tree to get a branch that is used for medicine. Talks with neighbours over the fence about whether the water point is open yet.
8.35am Uses the branch to sweep a bit inside. Washes hands with water in the kitchen 8:40am Pours water for animals from the Gerry can outside.
8.45am Using the water from the Gerry can outside she splashes water onto the floor inside the house and then sweeps all rooms.
8.50am Borrows some of the neighbour’s water to refill one of her gerry cans. Washes the bucket that the animals drank from.
8.55am Washes gerry cans. Disposes of the dirt from the house outside into a rubbish pile. Sends the clean jerry cans with a neighbour to the water point.
9.00am Washes baby in the bedroom of the house using the same bucket that the animals drank from. No soap is used in the bathing process. Cold water is used. The child’s face is also washed. Afterwards she wraps him in a baby blanket and dries him with this. She brings out a bag of baby clothes and dresses him. During this time she wipes the child’s face with her fingers.
9.05am Breastfeeds her baby. Cleans the baby’s ears. Throws water away along the side of the house.
9.10am Mother re-lights the fire. Uses water to clean the pan. Washes her hands (without soap). Begins to cook bread.
9.25am Washes more plates with water. Water not used very sparingly. Dirty water I always thrown in the same place near the animals.
9.30am Breaks up the bread in preparation for eating. Covers food in container. Washes more plates with water only.
9.35am Water and bucket taken into the main room for handwashing. The table is washed. Family eat breakfast. Mother feeds the baby.
9.55am Baby is put to rest. Mother covers baby’s face with the blanket. Goes to get the gerry cans that were left at the water point.
10:00am Returns with the first gerry can and goes back for the second time.
10:20am Returns with the second gerry can.
10:25am Friend comes and sells her grain for yeast. Chats with neighbours for a while. 10:35am Starts to grind wheat into flour for funeral preparations.
11:00am Washes hands with water only. Breastfeeds. Feeds baby more food. Drinks water from a tin.
11:10am Child urinates on the floor. Nothing is done (just left to dry). Mum washes hands after feeding. Mother wipes child’s face but around mouth only to get rid of food. Mother also swats flies away from child’s face.
11:20am 13 year old daughter arrives back from school and straight away begins to look after the baby.
11.25am Takes the child to defecate behind the house but nothing happens.
11.35am Mother begins preparing coffee. She lights the stove in the main room.
11.45am The daughter begins washing the coffee cups and the coffee table using a lot of water.
11.50am The mother begins to wash the coffee beans over the stove, again this takes a lot of water.
11.55am Mother roasts the coffee beans. Daughter plays with the baby.
12.05pm Mother pounds coffee in the kitchen.
12.15pm Mother washes coffee pot and puts ground coffee in.
12.20pm Mother washes all coffee cups and the coffee table again for the second time – this time using a small amount of powdered soap.
12.25pm Prepares a jug of water and bucket for handwashing. 12.35pm Pours and serves coffee and njira.
12.50pm Child given a lollipop, which he drops on the floor several times and continues to eat.
1.30pm Coffee things are packed away and rinsed. Boiled eggs are served.
1:40pm Mother pounds leaves as part of preparation of traditional drink.
2:00pm Daughter tries to wipe baby’s eyes briefly with her fingers.
2.05pm Daughter eats in the kitchen and then washes her hands with water only.
2.15pm Baby plays with cow dung. The mother sees and tells the daughter to stop him. Baby goes and watches the aunty grinding flour. She jokingly puts flour on his face and after this his face is wiped with a scarf by the mother.
2.20pm Child sneezes but this does not prompt anyone to wipe his nose.
2.35pm Child wipes own face on sleeve.
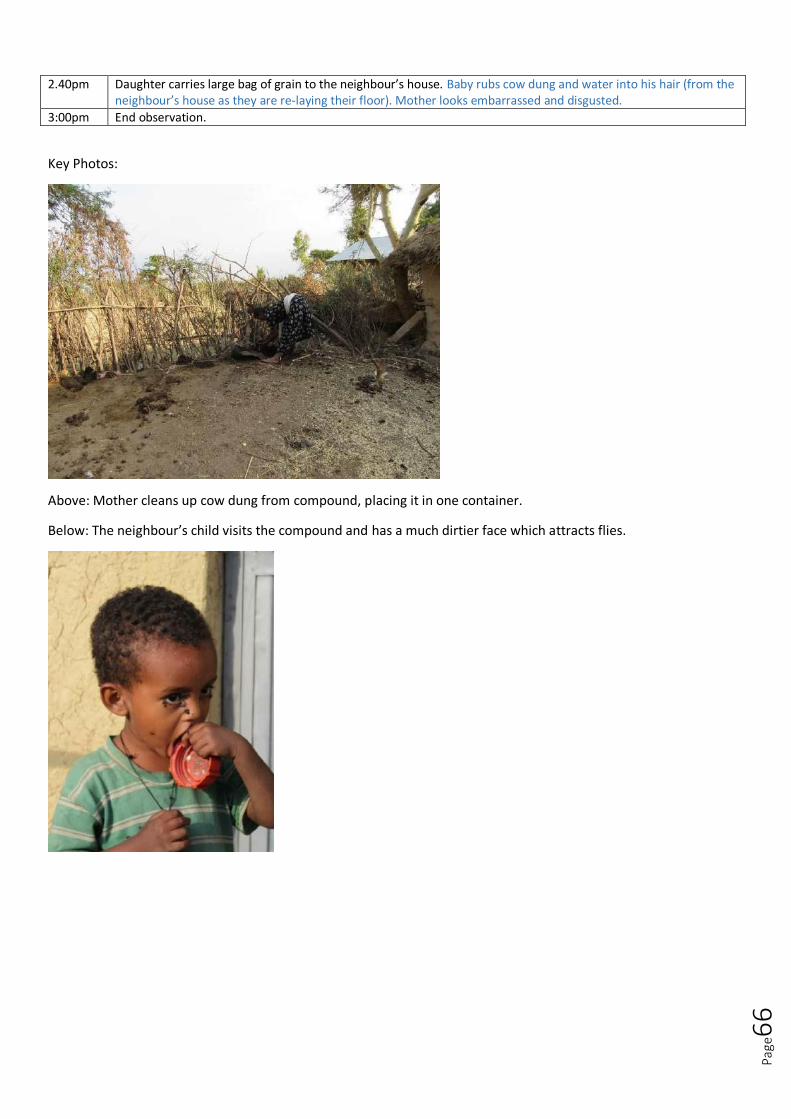
Page
66
2.40pm Daughter carries large bag of grain to the neighbour’s house. Baby rubs cow dung and water into his hair (from the neighbour’s house as they are re-laying their floor). Mother looks embarrassed and disgusted.
3:00pm End observation.
Key Photos:
Above: Mother cleans up cow dung from compound, placing it in one container.
Below: The neighbour’s child visits the compound and has a much dirtier face which attracts flies.
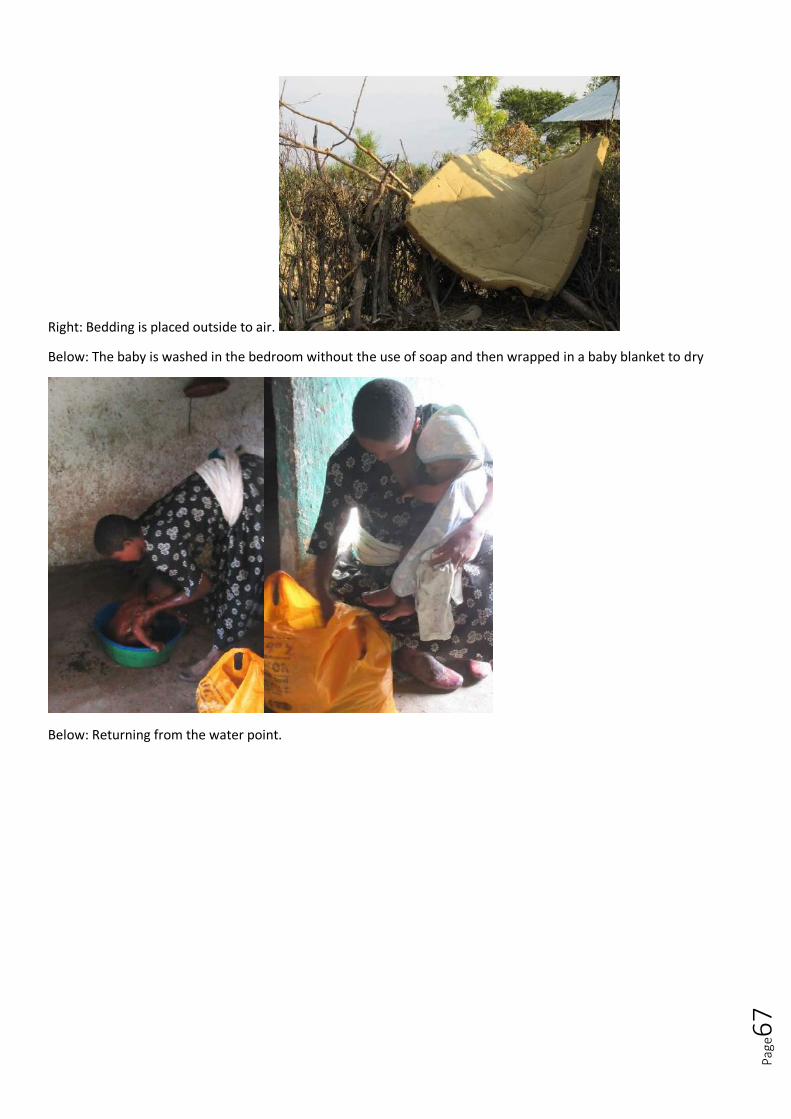
Page
67
Right: Bedding is placed outside to air.
Below: The baby is washed in the bedroom without the use of soap and then wrapped in a baby blanket to dry
Below: Returning from the water point.
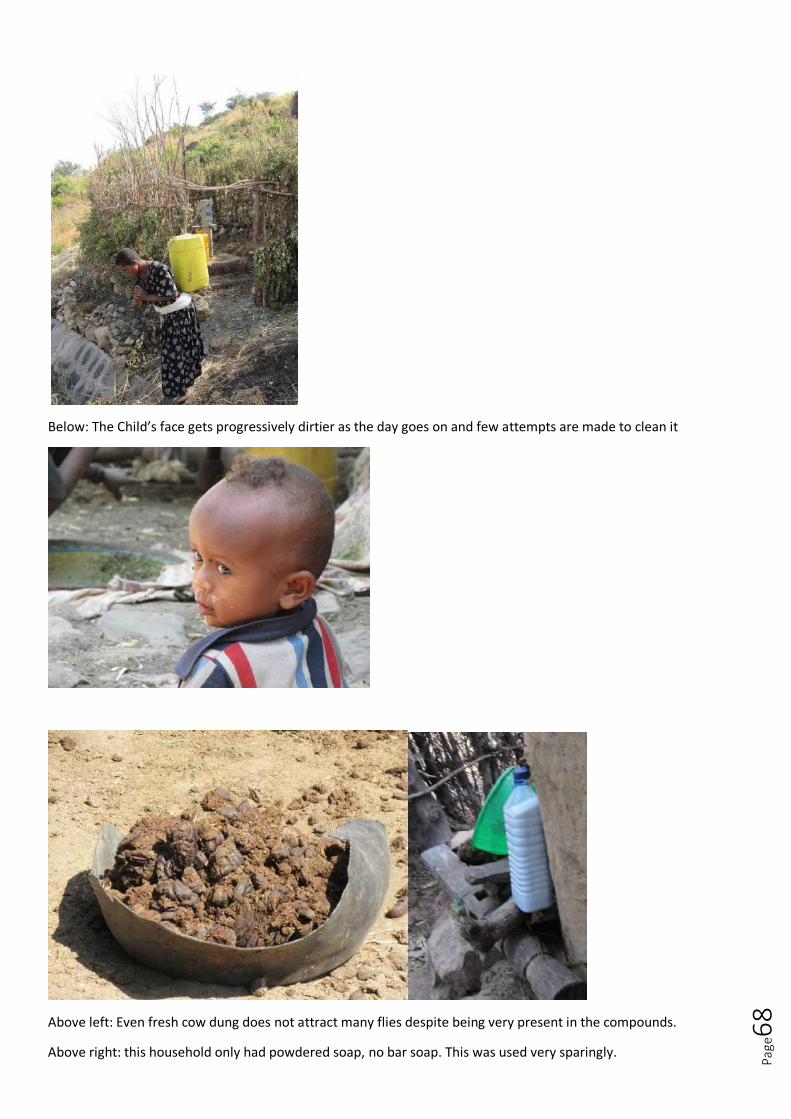
Page
68
Below: The Child’s face gets progressively dirtier as the day goes on and few attempts are made to clean it
Above left: Even fresh cow dung does not attract many flies despite being very present in the compounds.
Above right: this household only had powdered soap, no bar soap. This was used very sparingly.

Page
69
Below: Older children play a dominant role in caring for younger children.
COMMUNITY B: HH3
Saturday 16th January
Household composition: Mother and father, father is much older as the mother married at 9 yrs of age. Girls of
11yrs, 9yrs & 7yrs, Girl of 20yrs with 5 day old baby (we only see her once and don’t see the baby at all as they are
kept behind the cloth in the sleeping room).
General Observations / Comments:
Village is more rural than yesterday.
Household is much poorer than yesterday, they just have one house and sleeping area is behind a curtain
not in a separate room. They all sleep together except the father. They sleep on animal skins. Sleeping area
not seen as baby mother and new baby are in there.
Open defecation

Page
70
Water – the HH has one jerry can of 20L full of water at start of observation (the 9rl old girl has collected it
before we arrived); 20L is collected during observation + a few 3L jerry cans (roughly 50L water). Water is not
stored as we have seen yesterday and in other HH’s – it is used directly from jerry cans.
Fuel for the fire is dung which is stacked next to the house. They also use stalks (not wood) from maize field
(all has been harvested). There are no flies here.
Animal faeces is scattered throughout the compound
Faces are not dried (or bodies) after washing so use of cloths /towels that need washing is not an issue
Events undertaken during observation period:
Time Activity
07:50 Start observation
07:55 Mother puts water in pot on stove inside the house to boil water for the baby for a bath
08:00 Mother went next door to drink coffee with a neighbour
08:08 Mother was found behind the hut squatting – embarrassed to have stumbled upon her. She was using water – possible defecation? Checked later and human faeces was found behind the hut
08:10 Mother unties cattle and children lead them out to the fields. She puts wood on the fire
08:15 Girl 9yrs washes arms and face with soap behind the house using a cup. Her legs are still very dusty.
08:15 Mother sweeps the house and 7yr old throws the sweepings outside within the compound. Baby is crying.
08:20 Baby mother leave house and goes to field next to compound. Girl 7yrs accompanies her carrying soap and water. Baby mother defecates and washes but can’t see exactly what she washes. 7yr old returns to house to take her more water. Baby mother returns and removes the soap from within the scarf tied around her waist and goes back behind the sleeping curtain – we don’t see her again.
08:26 Mother washes dishes with just water and her hands and cleans a bucket for njera
08:30 Mother brings out njera jug to the outside fire and njera dish and starts making njera.
08:33 Girl 7yrs pours water from 3L jerry can in to a bowl and puts soap outside on ground and proceeds to wash hair with soap and then face, arms, feet and legs (the latter without soap). She pulls her top back on without drying herself in anyway
08:39 Baby mother says she is washing baby behind the curtain
08:45 Father is smoking a pipe inside and coughing a lot as he does so. Mother continues making njera and child 7yrs sits with her and eats it as she makes it. Other children are sitting around.
08:51 Girl 11yrs returns with water (20L) on her back and 2x3L containers of water in her hands which she fetched from water point (hadn’t seen her leave so must be quite close)
08:56 Girl 9yrs returns with stalks from field for firewood
09:01 Girl 11yrs washes bowl inside house with water and hands and starts sieving flour
09:04 The father is brought njera with horse bean wat to eat. The 11yr old girl joins him.
09:05 Mother washes hands in house with water
09:12 Girls 7yrs and 9yrs eat together inside (no HW). 7yr old rinses hands in bowl after eating and drinks
09:20 Mother stirs porridge for the mother of the baby and gives it to her
09:32 Mother is still making njera outside. A visitor comes to greet the father and sits inside for a while and the two men leave with an axe.
09:31 Young girl comes to take embers from the fire
09:36 Neighbour comes to greet the mother of the baby and give gifts
All is very quiet in the house for a while. 11yr old girl wipes eyes with fingers
10:16 Mother comes inside and continues cooking on the inside stove (3 stone). Very smoky inside house.
We are brought water from the water point to drink as she said her water is river water.
10:24 11yr old starts washing dishes and mother takes over. Washing with very little bit of soap and water in a bowl using little water to wash from dish to dish.
10:30 Cows come back on their own and are shooed away again
10:57 Everyone sitting around a lot until the end of observation – 9yr old girl brings firewood for inside the house. Decide to stop observation and do interview as nothing is happening.
Selection of photos from observation in this household:
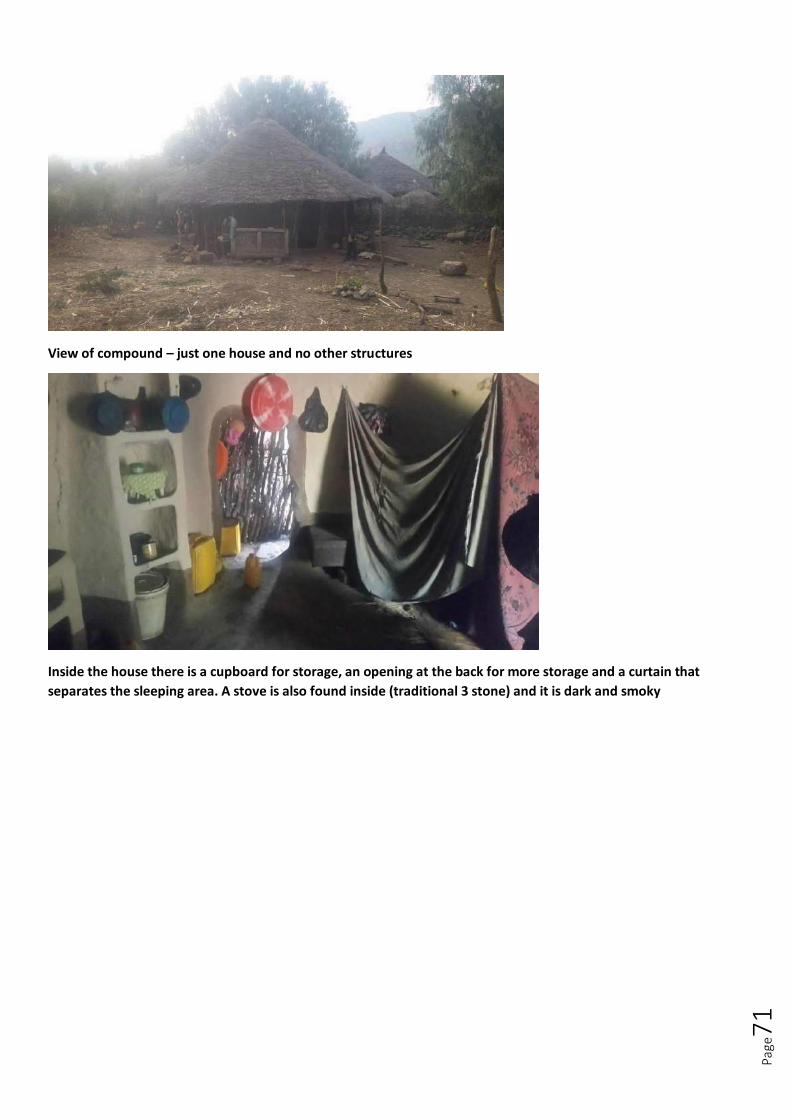
Page
71
View of compound – just one house and no other structures
Inside the house there is a cupboard for storage, an opening at the back for more storage and a curtain that
separates the sleeping area. A stove is also found inside (traditional 3 stone) and it is dark and smoky
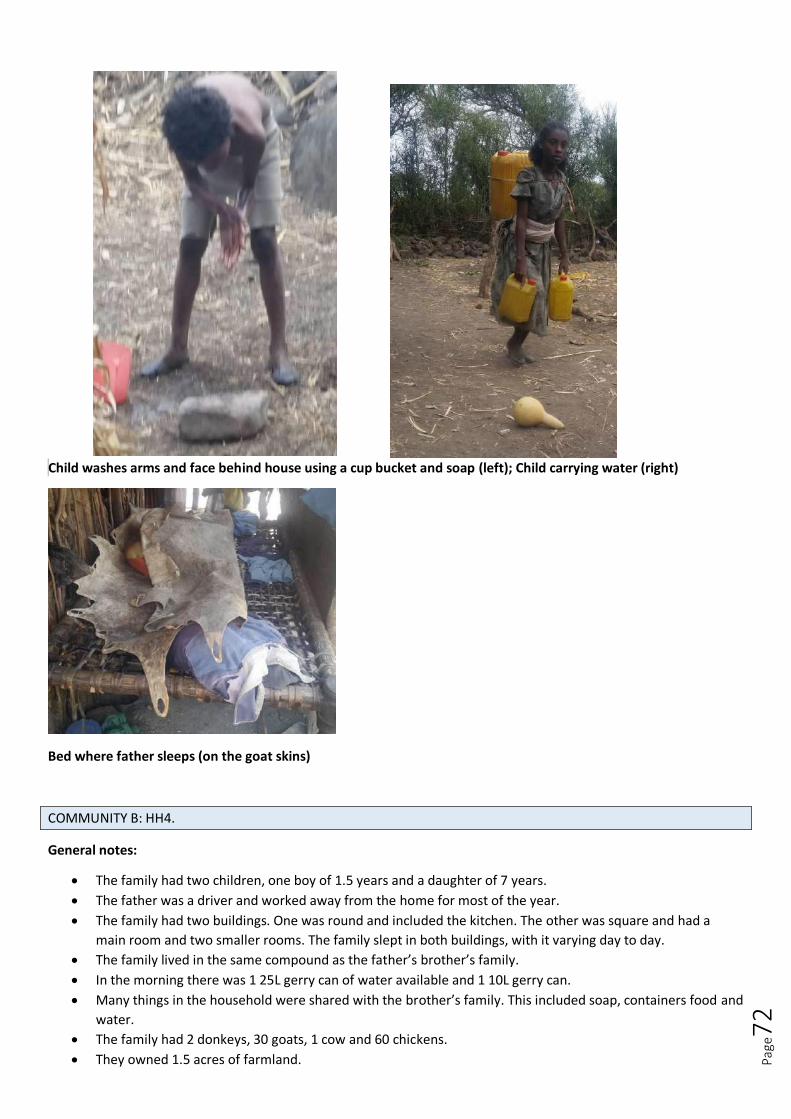
Page
72
Child washes arms and face behind house using a cup bucket and soap (left); Child carrying water (right)
Bed where father sleeps (on the goat skins)
COMMUNITY B: HH4.
General notes:
The family had two children, one boy of 1.5 years and a daughter of 7 years.
The father was a driver and worked away from the home for most of the year.
The family had two buildings. One was round and included the kitchen. The other was square and had a
main room and two smaller rooms. The family slept in both buildings, with it varying day to day.
The family lived in the same compound as the father’s brother’s family.
In the morning there was 1 25L gerry can of water available and 1 10L gerry can.
Many things in the household were shared with the brother’s family. This included soap, containers food and
water.
The family had 2 donkeys, 30 goats, 1 cow and 60 chickens.
They owned 1.5 acres of farmland.

Page
73
They had a mobile but no functioning electricity.
They had a toilet which seemed to be used most of the time (no faeces present around compound) but the
toilet had no superstructure.
The mother was celebrating Zecker at her house the day we visited. This is a religious process where a group
of friends meet monthly at each other’s house to share coffee and bread.
The family had only bar soap available x 2.
The family use 3 jerry cans of water to do their normal daily activities.
Time Observed activity
8:00am Start observation. Mother goes to fetch water. Children playing outside the house.
8:15am Mother returns with 20L of water. Breastfeeds baby. Wipes child’s nose with a piece of his clothing which was beside her.
8:20am Mother instructs daughter to clear up the house. Child moves bed sheets from the round house where they had slept that night to the square house and lay them across the bed.
8.25am Mattress is moved out of the way and mother sweeps the round house.
8.30am Daughter brings cow dung from the neighbouring field and places it inside the house. Her hands were not immediately washed.
8.40am Mother warms water over the fire and uses some of this it wash pots. Uses part of a plastic bag to scrub pots. No soap used. She rises her hands in the dirty water from the dishes. Throws dirty water outside into a container alongside the house so that it can be drunk by the animals.
8.45am Uses the rest of the warm water to wash the baby with soap. The mother took the soap from her waist band. The baby was washed in the same container that the daughter used for collecting cow dung. Face and hair are washed but without a lot of lather. Mother specifically wipes nose. Wraps the baby in a cloth and puts cream all over his body. In total only about 1L of water was used in bathing. This water was then thrown outside with the dishwater, for the animals.
8:55am Dirty baby clothes are hung up. Mother begins to cook. She washes each plate only as it is needed. She cuts an onion.
9.10am Daughter washes legs and shoes outside. Uses soap and about 1/2L of water.
9.15am Mother washes hands with water only and then feeds baby.
9.20am Daughter washes face and hands with soap and wipes some water through her hair. A further 1/2L water is used for this.
9.25am Daughter puts cream on her hands. Mum gives baby water to drink. Mum goes to collect wood from neighbouring field.
9.30am Girl gives soap to the neighbouring household.
9.35am The neighbours use the soap to wash some of their clothes, shoes and then the aunty has a full bath in the compound. Throughout the water and soap is used sparingly.
9:40am Children play with each other on the mattress inside while mother continues to prepare food. Goats are led to drink from the water that was thrown away.
9:50am Mother goes and cleans up the other house.
9.55am Mother breastfeeds and does not wipe nose despite being snotty.
10.00am Fresh water from the gerry can given to goats.
10.10am The mother rinses her hands. The family eat together and the mother feeds the baby. 10.25am Mother starts re-laying the floor by mixing water with the cow dung that was brought into the house
earlier. 6L of water are used in the process.
10.45am Mother sweeps the other house and then re-lays the floor in that house too.
11.15am Mother runs out of cow dung and water and so does not complete the porch. She washes her hands with soap and then her face and chest, legs and shoes. Cleans the soap afterwards.
11.30am Observation concludes.
Key Photos:
Below: Flies present on the faces of children from early in the morning. The daughter was again observed to
take a primary role in playing with and looking after the baby.

Page
74
Below: There was a specific place for rubbish within the compound but most of this was dry and did not
attract flies.
Below: The family had a toilet which appeared to be used but it did not have a superstructure (although they
reported that it previously did). Child faeces was disposed of outside the compound rather than in the toilet.

Page
75
Above: Dirty water from dishes and bathing the baby is stored and given to the animals.
Below left: Child is bathed with soap. However there is minimal lather and water is used sparingly.
Below right: after washing her legs, shoes and hands the sughter washes her face with soap.

Page
76
Below left: The mother re-lays the floor with cow dung and water.
Below right: The mother washes her legs, shoes, hands, chest and face with water and soap.

Page
77
COMMUNITY C: HH5.
Saturday 16th January
Household composition: Mother and father (father is a tailor). 17yr old boy, girls of 8yrs, 7yrs, 3yrs and 1 yr.
General Observations / Comments:
Main room of the house is a bar. Behind a curtain they have a store and a lot of activities of the day were
conducted there and couldn’t be easily observed
Father had a sewing machine and was busy making clothes in one building. They had several other buildings
and beds with mattresses could be seen
Village is quite rural
They have electricity (light only) and a mobile phone is seen charging.
The health post is nearby
The main house is quite dirty
They have a latrine but there is a lot of faeces near the hole. Health extension worker told them to build it so
father built it.
There is a lot of garbage everywhere in this compound, scattered as well as in one place
Not too many flies but they are sometimes on the kids faces, particularly the snotty 3 yr old and a
neighbour’s child who is often in the compound and has flies on the face and nasal and eye discharge (little
is done to clean the 3yr old’s nose)
Water – HH has 25L water outside the house when we arrive and 20L empty when we arrive (water is
collected in this). A further 20L jerry can is in the queue at the water point as well. Mother had collected the
25L jerry can before we arrived and will get the other one from water point in the afternoon.
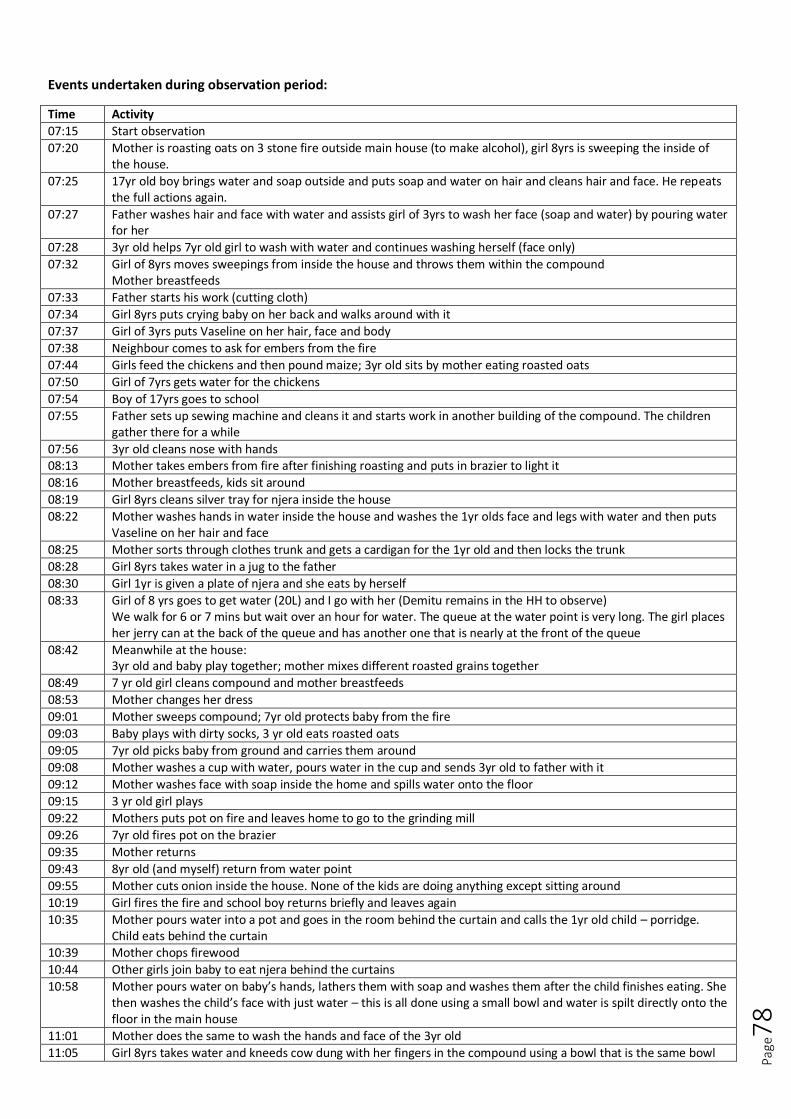
Page
78
Events undertaken during observation period:
Time Activity
07:15 Start observation
07:20 Mother is roasting oats on 3 stone fire outside main house (to make alcohol), girl 8yrs is sweeping the inside of the house.
07:25 17yr old boy brings water and soap outside and puts soap and water on hair and cleans hair and face. He repeats the full actions again.
07:27 Father washes hair and face with water and assists girl of 3yrs to wash her face (soap and water) by pouring water for her
07:28 3yr old helps 7yr old girl to wash with water and continues washing herself (face only)
07:32 Girl of 8yrs moves sweepings from inside the house and throws them within the compound Mother breastfeeds
07:33 Father starts his work (cutting cloth)
07:34 Girl 8yrs puts crying baby on her back and walks around with it
07:37 Girl of 3yrs puts Vaseline on her hair, face and body
07:38 Neighbour comes to ask for embers from the fire
07:44 Girls feed the chickens and then pound maize; 3yr old sits by mother eating roasted oats
07:50 Girl of 7yrs gets water for the chickens
07:54 Boy of 17yrs goes to school
07:55 Father sets up sewing machine and cleans it and starts work in another building of the compound. The children gather there for a while
07:56 3yr old cleans nose with hands 08:13 Mother takes embers from fire after finishing roasting and puts in brazier to light it
08:16 Mother breastfeeds, kids sit around
08:19 Girl 8yrs cleans silver tray for njera inside the house
08:22 Mother washes hands in water inside the house and washes the 1yr olds face and legs with water and then puts Vaseline on her hair and face
08:25 Mother sorts through clothes trunk and gets a cardigan for the 1yr old and then locks the trunk
08:28 Girl 8yrs takes water in a jug to the father
08:30 Girl 1yr is given a plate of njera and she eats by herself
08:33 Girl of 8 yrs goes to get water (20L) and I go with her (Demitu remains in the HH to observe) We walk for 6 or 7 mins but wait over an hour for water. The queue at the water point is very long. The girl places her jerry can at the back of the queue and has another one that is nearly at the front of the queue
08:42 Meanwhile at the house: 3yr old and baby play together; mother mixes different roasted grains together
08:49 7 yr old girl cleans compound and mother breastfeeds
08:53 Mother changes her dress
09:01 Mother sweeps compound; 7yr old protects baby from the fire
09:03 Baby plays with dirty socks, 3 yr old eats roasted oats
09:05 7yr old picks baby from ground and carries them around
09:08 Mother washes a cup with water, pours water in the cup and sends 3yr old to father with it
09:12 Mother washes face with soap inside the home and spills water onto the floor
09:15 3 yr old girl plays
09:22 Mothers puts pot on fire and leaves home to go to the grinding mill
09:26 7yr old fires pot on the brazier
09:35 Mother returns
09:43 8yr old (and myself) return from water point
09:55 Mother cuts onion inside the house. None of the kids are doing anything except sitting around
10:19 Girl fires the fire and school boy returns briefly and leaves again
10:35 Mother pours water into a pot and goes in the room behind the curtain and calls the 1yr old child – porridge. Child eats behind the curtain
10:39 Mother chops firewood
10:44 Other girls join baby to eat njera behind the curtains
10:58 Mother pours water on baby’s hands, lathers them with soap and washes them after the child finishes eating. She then washes the child’s face with just water – this is all done using a small bowl and water is spilt directly onto the floor in the main house
11:01 Mother does the same to wash the hands and face of the 3yr old
11:05 Girl 8yrs takes water and kneeds cow dung with her fingers in the compound using a bowl that is the same bowl
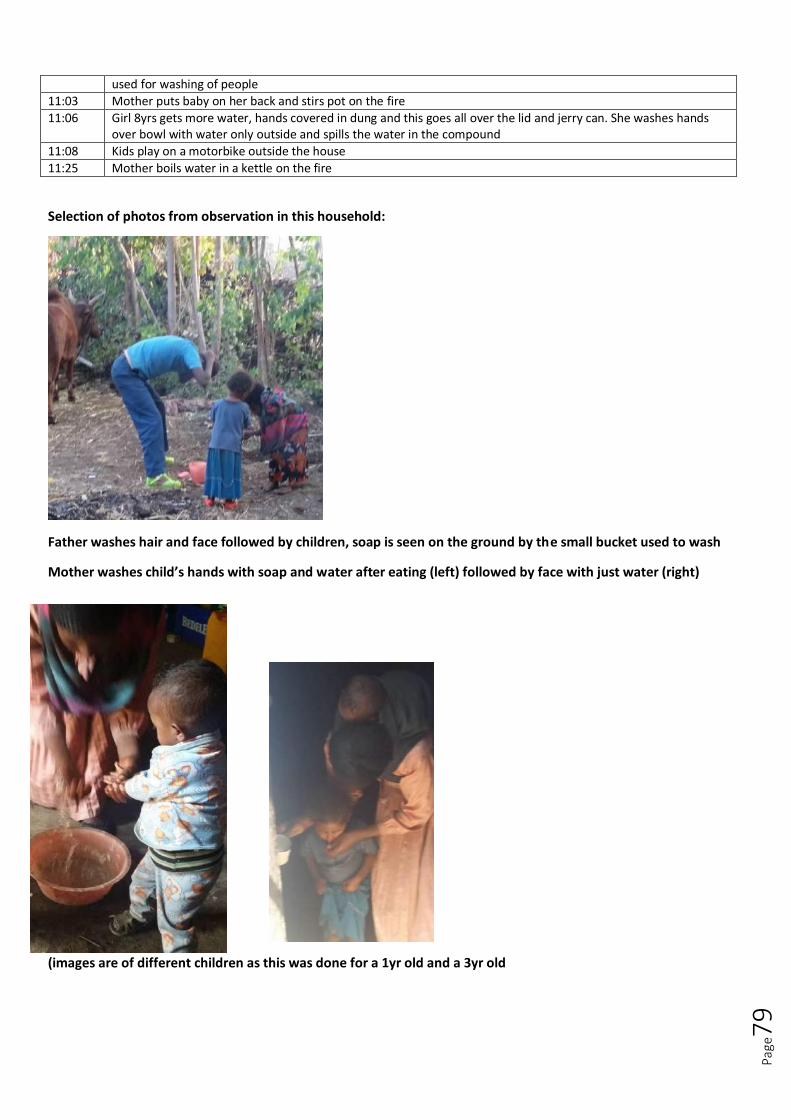
Page
79
used for washing of people
11:03 Mother puts baby on her back and stirs pot on the fire
11:06 Girl 8yrs gets more water, hands covered in dung and this goes all over the lid and jerry can. She washes hands over bowl with water only outside and spills the water in the compound
11:08 Kids play on a motorbike outside the house
11:25 Mother boils water in a kettle on the fire
Selection of photos from observation in this household:
Father washes hair and face followed by children, soap is seen on the ground by the small bucket used to wash
Mother washes child’s hands with soap and water after eating (left) followed by face with just water (right)
(images are of different children as this was done for a 1yr old and a 3yr old

Page
80
Queue for the water point
Basic latrine with small hole and lots of faeces surrounding the hole
COMMUNITY C: HH6.
General notes:
The family had a daughter of 18, a daughter of 16, a daughter of 13, a son of 10, a daughter of 7 and a son of
5 months.
The husband of the family was the Kebele leader and had two wives. This was the house of his second wife.
On average he spent 2 nights there a week.
The mother had been married previously and her eldest thee children are from that marriage.

Page
81
The house includes two buildings. One square building with two rooms and another round building which
includes the kitchen.
The elder 3 girls sleep in the building where the kitchen is and the rest of the family sleep in the square
buildings.
The family have cows, sheep, donkeys and a puppy.
The family have functional electricity and a mobile phone.
The family have several bars of soap and one that is used only for the baby. They also have lots of beauty
products such as Vaseline and other creams, combs and mirrors.
Each child has a backpack hanging up with their own belongings in it.
The family have a lot of different buckets, containers and flasks.
The family have a toilet which appears to be used but has a low superstructure with no roof. The pit is only
about 1m deep.
At the beginning of the day the family had 1.5 25L gerry cans of water available.
In both buildings the family sleep on a mattress filled with straw. On top of this is laid animal skins. Under
the animal skins they fill a rice sack with old clothes and use this as a pillow.
Use incense sticks in the house to make it smell nice – particularly while making coffee.
They use 3 gerry cans of water to undertake their normal daily activities.
Time Observed activities
7.20am Observation starts. Younger children just waking up. All children (except the 5 month old and 13 year old) go outside to wash. 16 year old uses soap to wash hands, legs and face. 7 and 10 year olds help each other (by pouring water) to wash hands and faces only but no soap is used. Nothing is used for drying. Mother washes some pots and heats water. Dirty water is given to the cows in a bowl.
7.30am 13 year old sweeps house. Mother washes coffee pots and cups. Children get changed. The 7year old plays with the baby.
7.40am 16 year old spends a lot of time grooming, brushing her hair and rubbing different creams onto her face, legs, hands and hair. 13 year old throws rubbish into a pile at the front of the house.
7.45am 13 year old tends to the fire and prepares breakfast. 16 year old tidies the kitchen area and folds the bed covers. Mother makes coffee.
7.50am 13 year old takes blankets out of the main house and puts them outside to air. 16 year old uses the toilet. No handwashing observed
7.55am Mother and the 13 year old bathe the baby inside the house using soap and some warm water. The babies face is also washed. The baby is wrapped in a special baby blanket. The 18 year old washes her feet hands and face outside with soap.
8.00am Soapy water from the baby’s bath put outside and the dirty baby clothes are placed inside it. Mother rubs cream on the baby’s whole body. The 7 year old and 10 year old come over and also use the cream to moisturise their faces and hands. Mother puts clean clothes on the baby. There is quite a lot of wiping of the baby’s face with fingers during this process. The 10 year old boy goes out to urinate in the corner of the compound (not toilet).
8.05am Mother and 13 year old rinse the plates and the water is tipped outside on the rubbish pile. 16 year old goes to school.
8.10am The 18, 7 and 10 year old eat in the kitchen. The mother breastfeeds the baby. The 13 year old serves the mother food and helps her to wash her hands (without soap).
8.15am Children finish eating and rinse plates. 18 year old goes to school. 7 year old shakes some garments that were inside the house outside. 10 year old eats raw chickpeas. Mother drinks coffee.
8:25am Visitor arrives and he also has coffee. 8:30am Mother discards old milk near kitchen so that puppy can drink it. Mother then sterilises the bottle with boiling
water and washes the flask with soap and a rice sack rag.
8.40am Mother instructs the 10 year old to dig a hole near the kitchen for the puppy to lie in.
8.45am Mother milks cow.
8.50am Mother boils the fresh milk, mixing it with water.
9.00am 13 year old eats in the bedroom of the main house. Washes her hands (no soap) after.
9.10am 13 year old prepares onion and throws peel in dirty dish water. She then throws this on the rubbish pile outside.
9:20am Mum strains hot milk and pours it into a flask.
9.30am Mother cooks onions and spices. Dirty water and milk thrown away and given to puppy.
9.35am 13 year old goes to water point to get 25L water.
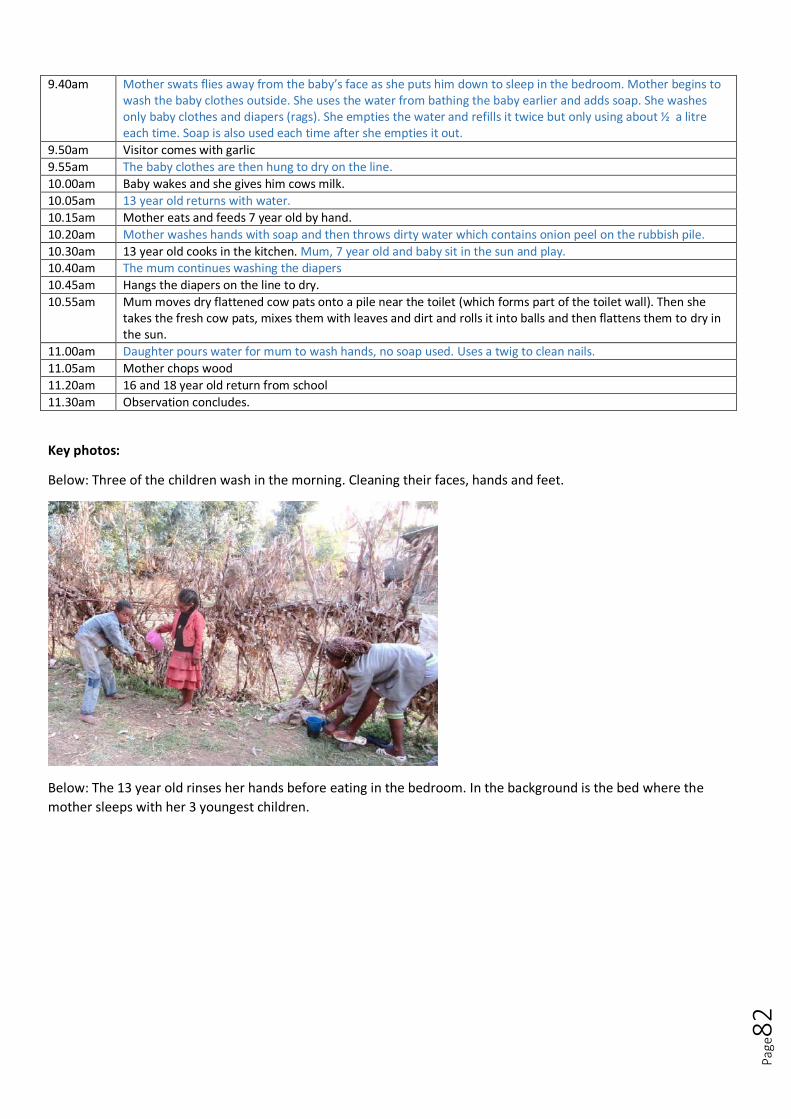
Page
82
9.40am Mother swats flies away from the baby’s face as she puts him down to sleep in the bedroom. Mother begins to wash the baby clothes outside. She uses the water from bathing the baby earlier and adds soap. She washes only baby clothes and diapers (rags). She empties the water and refills it twice but only using about ½ a litre each time. Soap is also used each time after she empties it out.
9.50am Visitor comes with garlic
9.55am The baby clothes are then hung to dry on the line.
10.00am Baby wakes and she gives him cows milk.
10.05am 13 year old returns with water.
10.15am Mother eats and feeds 7 year old by hand.
10.20am Mother washes hands with soap and then throws dirty water which contains onion peel on the rubbish pile.
10.30am 13 year old cooks in the kitchen. Mum, 7 year old and baby sit in the sun and play. 10.40am The mum continues washing the diapers
10.45am Hangs the diapers on the line to dry.
10.55am Mum moves dry flattened cow pats onto a pile near the toilet (which forms part of the toilet wall). Then she takes the fresh cow pats, mixes them with leaves and dirt and rolls it into balls and then flattens them to dry in the sun.
11.00am Daughter pours water for mum to wash hands, no soap used. Uses a twig to clean nails.
11.05am Mother chops wood
11.20am 16 and 18 year old return from school
11.30am Observation concludes.
Key photos:
Below: Three of the children wash in the morning. Cleaning their faces, hands and feet.
Below: The 13 year old rinses her hands before eating in the bedroom. In the background is the bed where the
mother sleeps with her 3 youngest children.
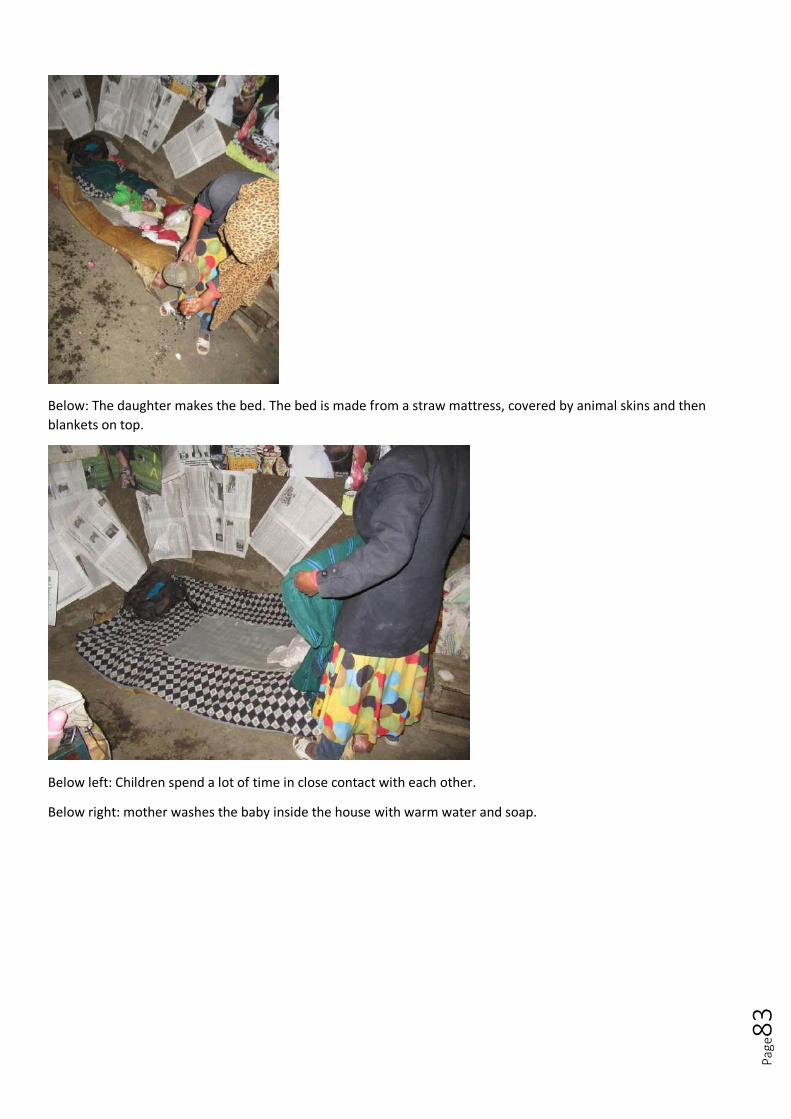
Page
83
Below: The daughter makes the bed. The bed is made from a straw mattress, covered by animal skins and then
blankets on top.
Below left: Children spend a lot of time in close contact with each other.
Below right: mother washes the baby inside the house with warm water and soap.

Page
84
Below: Mother applies Vaseline to baby’s face, while the other two children use the Vaseline to apply to their faces
and hands also.
Below: the toilet at the house had a shallow pit and only had a low superstructure (made from branches and cow
dung) without a roof.
Below: the presence of flies on a child’s face is often not addressed by mothers

Page
85
Below: food waste, such as onion peel is thrown out onto the rubbish pit with the dirty water from washing plates.
Below: Water is collected from an unprotected spring
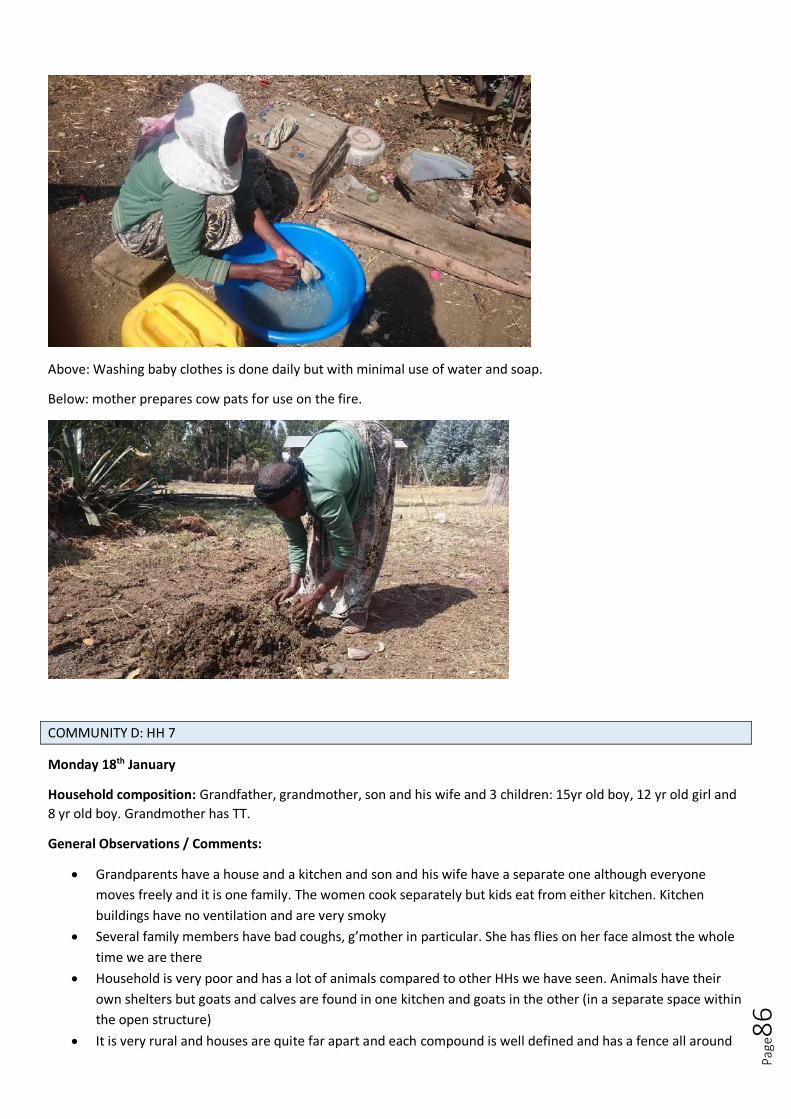
Page
86
Above: Washing baby clothes is done daily but with minimal use of water and soap.
Below: mother prepares cow pats for use on the fire.
COMMUNITY D: HH 7
Monday 18th January
Household composition: Grandfather, grandmother, son and his wife and 3 children: 15yr old boy, 12 yr old girl and
8 yr old boy. Grandmother has TT.
General Observations / Comments:
Grandparents have a house and a kitchen and son and his wife have a separate one although everyone
moves freely and it is one family. The women cook separately but kids eat from either kitchen. Kitchen
buildings have no ventilation and are very smoky
Several family members have bad coughs, g’mother in particular. She has flies on her face almost the whole
time we are there
Household is very poor and has a lot of animals compared to other HHs we have seen. Animals have their
own shelters but goats and calves are found in one kitchen and goats in the other (in a separate space within
the open structure)
It is very rural and houses are quite far apart and each compound is well defined and has a fence all around
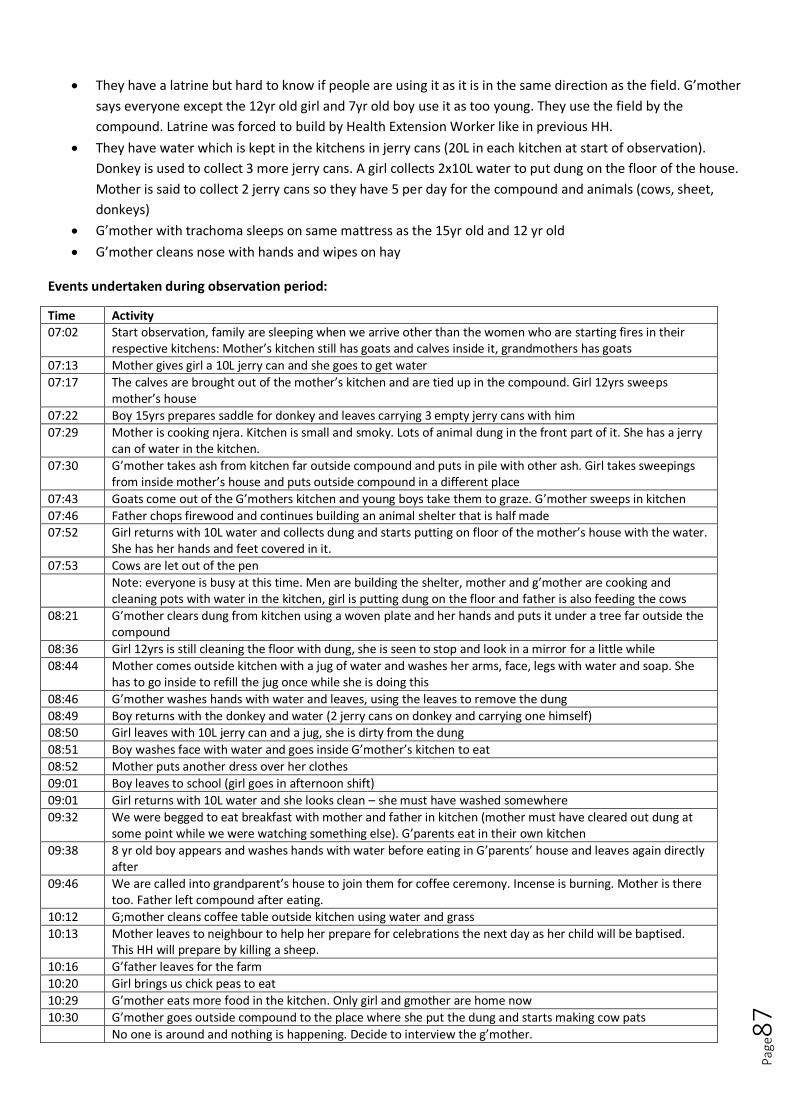
Page
87
They have a latrine but hard to know if people are using it as it is in the same direction as the field. G’mother
says everyone except the 12yr old girl and 7yr old boy use it as too young. They use the field by the
compound. Latrine was forced to build by Health Extension Worker like in previous HH.
They have water which is kept in the kitchens in jerry cans (20L in each kitchen at start of observation).
Donkey is used to collect 3 more jerry cans. A girl collects 2x10L water to put dung on the floor of the house.
Mother is said to collect 2 jerry cans so they have 5 per day for the compound and animals (cows, sheet,
donkeys)
G’mother with trachoma sleeps on same mattress as the 15yr old and 12 yr old
G’mother cleans nose with hands and wipes on hay
Events undertaken during observation period:
Time Activity 07:02 Start observation, family are sleeping when we arrive other than the women who are starting fires in their
respective kitchens: Mother’s kitchen still has goats and calves inside it, grandmothers has goats
07:13 Mother gives girl a 10L jerry can and she goes to get water
07:17 The calves are brought out of the mother’s kitchen and are tied up in the compound. Girl 12yrs sweeps mother’s house
07:22 Boy 15yrs prepares saddle for donkey and leaves carrying 3 empty jerry cans with him
07:29 Mother is cooking njera. Kitchen is small and smoky. Lots of animal dung in the front part of it. She has a jerry can of water in the kitchen.
07:30 G’mother takes ash from kitchen far outside compound and puts in pile with other ash. Girl takes sweepings from inside mother’s house and puts outside compound in a different place
07:43 Goats come out of the G’mothers kitchen and young boys take them to graze. G’mother sweeps in kitchen
07:46 Father chops firewood and continues building an animal shelter that is half made 07:52 Girl returns with 10L water and collects dung and starts putting on floor of the mother’s house with the water.
She has her hands and feet covered in it.
07:53 Cows are let out of the pen
Note: everyone is busy at this time. Men are building the shelter, mother and g’mother are cooking and cleaning pots with water in the kitchen, girl is putting dung on the floor and father is also feeding the cows
08:21 G’mother clears dung from kitchen using a woven plate and her hands and puts it under a tree far outside the compound
08:36 Girl 12yrs is still cleaning the floor with dung, she is seen to stop and look in a mirror for a little while
08:44 Mother comes outside kitchen with a jug of water and washes her arms, face, legs with water and soap. She has to go inside to refill the jug once while she is doing this
08:46 G’mother washes hands with water and leaves, using the leaves to remove the dung
08:49 Boy returns with the donkey and water (2 jerry cans on donkey and carrying one himself) 08:50 Girl leaves with 10L jerry can and a jug, she is dirty from the dung
08:51 Boy washes face with water and goes inside G’mother’s kitchen to eat
08:52 Mother puts another dress over her clothes
09:01 Boy leaves to school (girl goes in afternoon shift)
09:01 Girl returns with 10L water and she looks clean – she must have washed somewhere
09:32 We were begged to eat breakfast with mother and father in kitchen (mother must have cleared out dung at some point while we were watching something else). G’parents eat in their own kitchen
09:38 8 yr old boy appears and washes hands with water before eating in G’parents’ house and leaves again directly after
09:46 We are called into grandparent’s house to join them for coffee ceremony. Incense is burning. Mother is there too. Father left compound after eating.
10:12 G;mother cleans coffee table outside kitchen using water and grass
10:13 Mother leaves to neighbour to help her prepare for celebrations the next day as her child will be baptised. This HH will prepare by killing a sheep.
10:16 G’father leaves for the farm
10:20 Girl brings us chick peas to eat
10:29 G’mother eats more food in the kitchen. Only girl and gmother are home now
10:30 G’mother goes outside compound to the place where she put the dung and starts making cow pats
No one is around and nothing is happening. Decide to interview the g’mother.
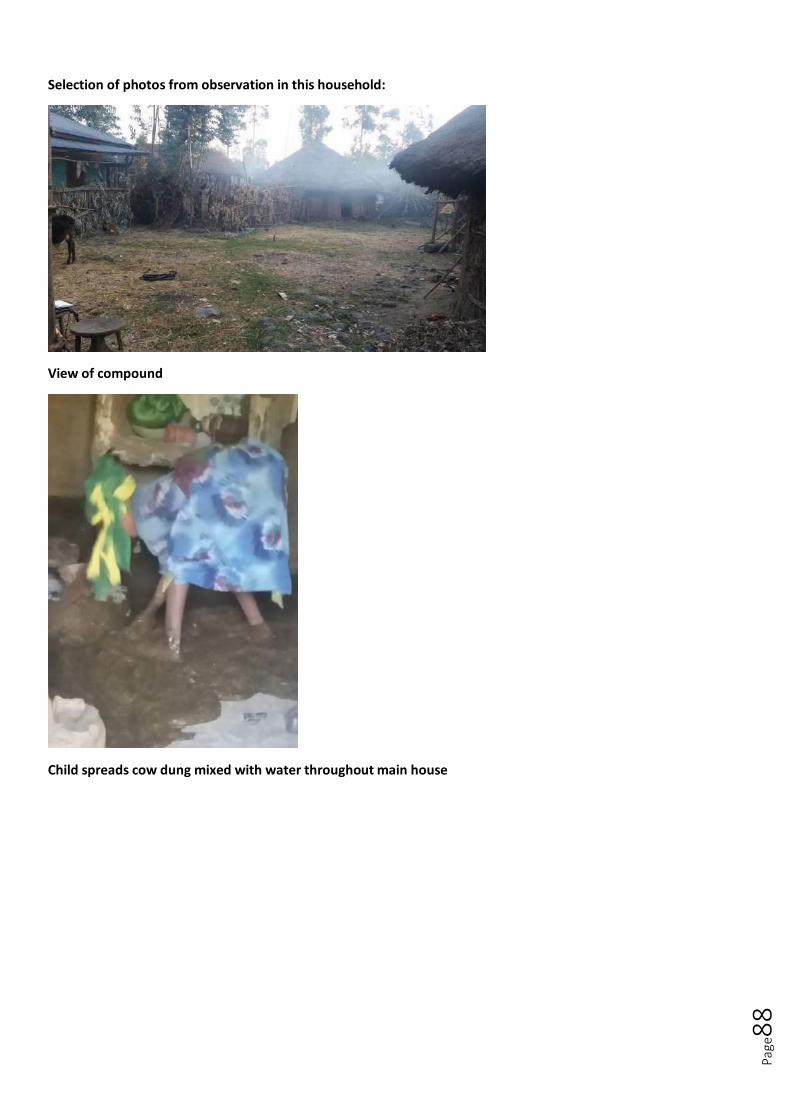
Page
88
Selection of photos from observation in this household:
View of compound
Child spreads cow dung mixed with water throughout main house

Page
89
Water fetched by school-age boy using a donkey
Latrine has a tiny hole but is clean and possibly unused

Page
90
Grandmother has TT and flies on her face
Grandmother and two children sleep together on this straw mattress which they cover with a mat and then goat
skins. They sleep under a blanket and use old clothes as a pillow

Page
91
COMMUNITY D: HH8.
General notes:
The family had 5 children present in the house. These were a boy of 15, a girl of 10, a girl of 8, a girl of 5 and
a boy of 3 years. The family had 3 other children (20, 18 and 13) who lived with relatives because they could
not afford to care for them.
The house consisted of two buildings. One which was primarily for the animals but which also served as a
secondary kitchen for njira preparation. The other main building was the primary kitchen and place where all
the family slept.
The family owned only one gerry can. In the morning less that ¼ of this gerry can was filled with water. The
family also had a traditional clay pot where they stored water later in the day. They owned two 10L gerry
cans which the children used to get water from the river (rather than the water point).
The family reported that they did not have much farmland. They had two cows, two donkeys, 6 sheep and
some chickens.
Children all had noticeable coughs
They had a toilet but this had a shallow pit and no superstructure. It was not always used and human faeces
was observed behind the house.
They had several rubbish piles around the house which they reported using for compost.
The family only had njira and spices for breakfast.
The family did not own soap.
The family did not own a coffee pot.
The father slept on an animal skin with 4 of the children under two blankets. The mother slept with the 3
year old on a mattress. Bags of grain were put under their heads for sleeping.
Mother appears to have active trachoma.
Relatively few flies around the house.
The 3 year old’s face was not wiped for the duration of the observation and attracted the most flies.
Time Observed activities
7.00am Observation begins. Whole family is only just getting up. Mother lights the fire. Dad takes the animals out of the other house. Mother takes the mattress outside to air. Dad gathers hay for the animals.
7.05am Mother begins to sweep house. Puts the rubbish behind the house. Father moves to the neighbouring field to continue working the hay.
7.15am Mum washes hands inside the house. The dirty water is collected into a container. No soap is used. The children are still huddled under a blanket, sitting on the animal skin.
7.20am Mother goes out to collect cow pats for the fire.
7.25am Dad calls the 15 year old son to help him (pour water) wash his face and hands with water only. The 15 year old then washes his own face and hands and picks the dirt out from under his nails. The father then goes inside the main house and uncovers the chickens. He takes some dried njira, mixes this with water and drops it on the floor to feed them.
7.30am Mother serves the father breakfast which is only njira and some spice powder. The 10 year old girl goes behind the house to defecate. No handwashing is observed afterwards.
7.35am 3 year old goes out to urinate in the bushes far from the house. 10 year old goes to get water with gerry can.
7.50am Reach the water point (afridev pump) and waits in line. While the daughter is waiting for water the mother cleans the cow dung up in the house where the animals are kept, 8 year old defecates behind house, and the children eat breakfast.
8.35am Begins to fill her gerry can.
9.00am 10 year old arrives back at the house but does not bring gerry can as she is too small to carry it. Mother is cooking njira for the next two days.
9:30am Washes plates with last remaining bit of water and lets the water fall onto the floor.
10.00am Daughter goes to the river with 2 10L gerry cans and fills these up.
10.10am Mother finishes cooking and rinses hands. Feeds some njira to chickens and gets changes into new clothes.
10.15am Mother walks to the water point to collect the gerry can. 10 year old returns from river with the water also.

Page
92
10.35am Mother returns from the water point. 10 year old daughter washes face with water from the river. The mother transfers some of the water from the gerry can into the traditional pot.
10.45am The daughter is told off by the mother for using a bowl that the dog had drunk from to transfer water from the gerry can into the other container.
10.55am Rinses all the dirty dishes in the house and the bucket that had the njira mixture in it. 10 year old pours 10L of water onto 3 banana trees in the garden.
11.00am Observation concludes.
Key Photos:
Above:
Above: Children huddled under the blanket in the morning. Blankets are normally washed less than monthly and in this case
were shared by more than 5 people nightly.
Below left: Mother washes her hands with water only and the dirty water is kept in a container in the house and then thrown
away. Below right: one of the daughters defecates behind the main house.
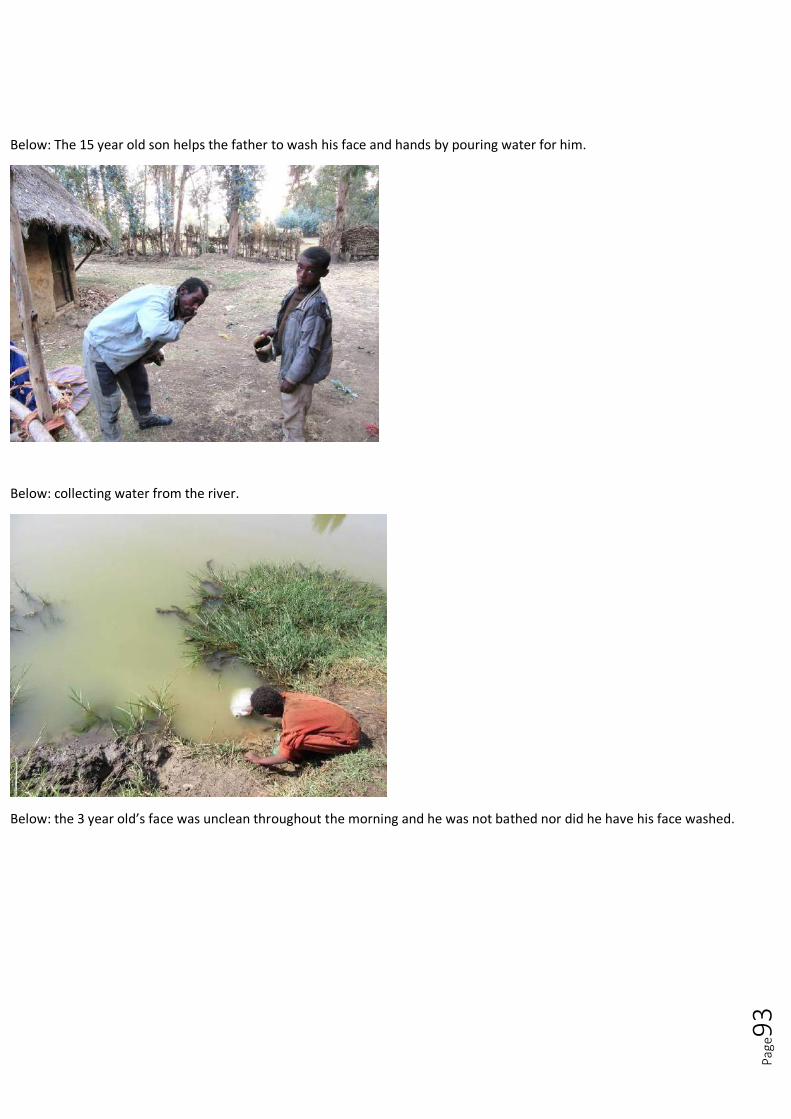
Page
93
Below: The 15 year old son helps the father to wash his face and hands by pouring water for him.
Below: collecting water from the river.
Below: the 3 year old’s face was unclean throughout the morning and he was not bathed nor did he have his face washed.

Page
94
Below: the 8 year old washes her face with river water.
Below: The toilet in the compound was not regularly used and lacked a superstructure.
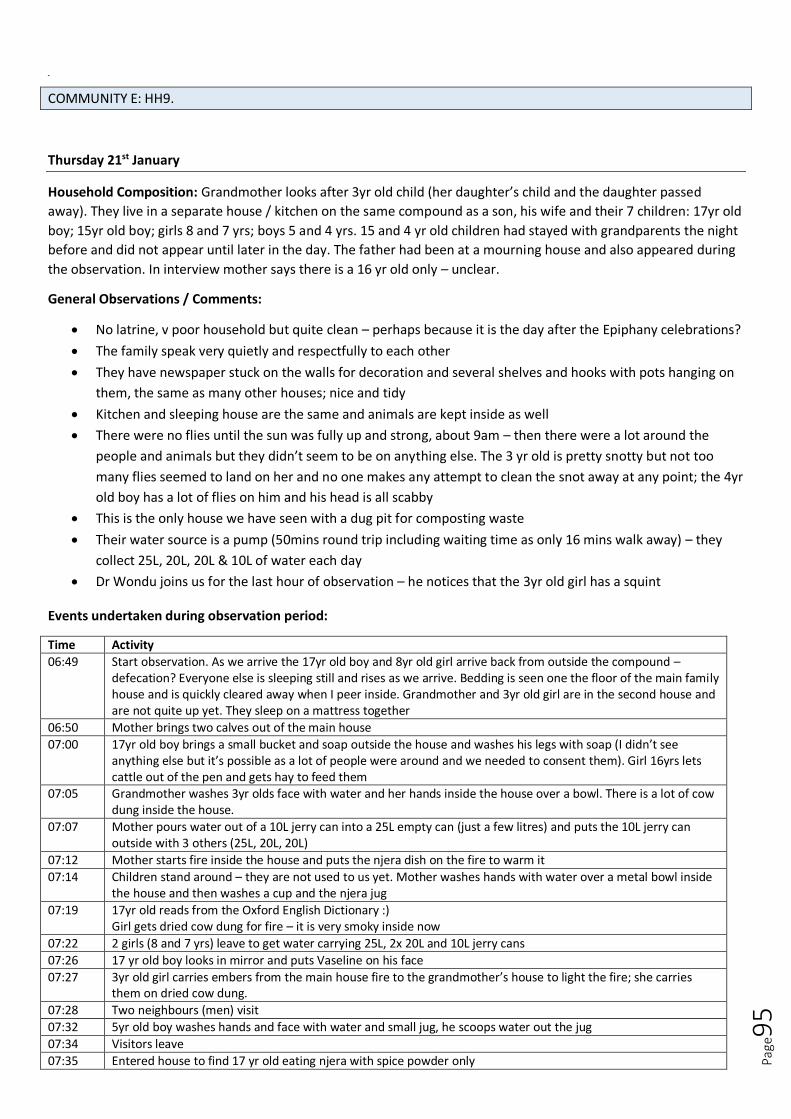
Page
95
Bel ow
COMMUNITY E: HH9.
Thursday 21st January
Household Composition: Grandmother looks after 3yr old child (her daughter’s child and the daughter passed
away). They live in a separate house / kitchen on the same compound as a son, his wife and their 7 children: 17yr old
boy; 15yr old boy; girls 8 and 7 yrs; boys 5 and 4 yrs. 15 and 4 yr old children had stayed with grandparents the night
before and did not appear until later in the day. The father had been at a mourning house and also appeared during
the observation. In interview mother says there is a 16 yr old only – unclear.
General Observations / Comments:
No latrine, v poor household but quite clean – perhaps because it is the day after the Epiphany celebrations?
The family speak very quietly and respectfully to each other
They have newspaper stuck on the walls for decoration and several shelves and hooks with pots hanging on
them, the same as many other houses; nice and tidy
Kitchen and sleeping house are the same and animals are kept inside as well
There were no flies until the sun was fully up and strong, about 9am – then there were a lot around the
people and animals but they didn’t seem to be on anything else. The 3 yr old is pretty snotty but not too
many flies seemed to land on her and no one makes any attempt to clean the snot away at any point; the 4yr
old boy has a lot of flies on him and his head is all scabby
This is the only house we have seen with a dug pit for composting waste
Their water source is a pump (50mins round trip including waiting time as only 16 mins walk away) – they
collect 25L, 20L, 20L & 10L of water each day
Dr Wondu joins us for the last hour of observation – he notices that the 3yr old girl has a squint
Events undertaken during observation period:
Time Activity
06:49 Start observation. As we arrive the 17yr old boy and 8yr old girl arrive back from outside the compound – defecation? Everyone else is sleeping still and rises as we arrive. Bedding is seen one the floor of the main family house and is quickly cleared away when I peer inside. Grandmother and 3yr old girl are in the second house and are not quite up yet. They sleep on a mattress together
06:50 Mother brings two calves out of the main house
07:00 17yr old boy brings a small bucket and soap outside the house and washes his legs with soap (I didn’t see anything else but it’s possible as a lot of people were around and we needed to consent them). Girl 16yrs lets cattle out of the pen and gets hay to feed them
07:05 Grandmother washes 3yr olds face with water and her hands inside the house over a bowl. There is a lot of cow dung inside the house.
07:07 Mother pours water out of a 10L jerry can into a 25L empty can (just a few litres) and puts the 10L jerry can outside with 3 others (25L, 20L, 20L)
07:12 Mother starts fire inside the house and puts the njera dish on the fire to warm it
07:14 Children stand around – they are not used to us yet. Mother washes hands with water over a metal bowl inside the house and then washes a cup and the njera jug
07:19 17yr old reads from the Oxford English Dictionary :) Girl gets dried cow dung for fire – it is very smoky inside now
07:22 2 girls (8 and 7 yrs) leave to get water carrying 25L, 2x 20L and 10L jerry cans
07:26 17 yr old boy looks in mirror and puts Vaseline on his face
07:27 3yr old girl carries embers from the main house fire to the grandmother’s house to light the fire; she carries them on dried cow dung.
07:28 Two neighbours (men) visit
07:32 5yr old boy washes hands and face with water and small jug, he scoops water out the jug
07:34 Visitors leave
07:35 Entered house to find 17 yr old eating njera with spice powder only

Page
96
07:39 3yr old eats grain from the floor of the main house
07:40 5yr old boy lets the sheep out of the pen inside the main house and he spends a lot of the morning chasing the cattle and sheep away from the road and hay stack
07:49 17yr old boy washes a bowl with water
07:52 Girl 3yrs eat some bread. 17yr old boy goes to school
08:12 The girls return from collecting water with 2 jerry cans (20L and 10L)
08:15 8 yr old girl walks to field and returns with chick peas for us to eat. She rinses them (to remove the burn from the outside)
08:21 Girl takes clothes and bowl outside
08:23 Girl 8 yrs takes bucket outside and cleans it in a bowl with water using a rag she tears of old clothing
08:30 Girl 8yrs gets out a basket she is weaving and sits doing it looking at us – she is doing it for effect and puts it away quickly
08:31 Mother takes sweeping and goes outside and throws them in a pit at edge of compound
08:32 Grandmother has made coffee and we are called to drink it. Mother brings us bread to eat (left from celebration day)
08:45 Girl puts Vaseline on herself and the 3yr old girl’s face and hair.
08:32 Girl 8 yrs combs her hair
09:01 Mother starts doing the laundry using a 20L jerry can of water. She pours a little water onto a rice sack, scrubs the clothes and soaps them with bar soap. There are a lot of suds. She rinses each item in turn and uses water to clean the rice sack from soap suds as she goes.
09:18 Father arrives from a mourning house. He leaves straight away.
09:38 Mother hangs up first batch of washing to dry. Grandmother and 3yr old are sitting around. A neighbour comes to visit
09:44 Girl returns from the water point with another 20L jerry can and gives to mother who is still washing clothes. She and the 3yr old leave the compound (defecation?)
10:04 Father returns
10:20 Father washes his hair and face and upper body with soap and water from a jug behind the house
10:27 Mother has finished laundry – she used about 35L of water. She gives the father more water for washing himself and he washes his legs with water only
10:47 Father eats njera
10:54 Mother is cooking again and washing dishes
10:54 Boy 15yrs arrives with boy 4yrs – they had spent the night at grandparents.
11:00 The kids who had left the compound all come back
11:09 Boy 4yrs washes hands with water while girl 7yr pours and then they reverse. They wash over a bowl and then eat together inside the house.
11:10 Father leaves to the church
11:16 3yr old joins them to eat without washing hands. 8yr old girl comes a couple of mins later and washes hands with water before eating.
11:30 Stopped observation to do interview as mother needs to go to the water point and then to the church
Selection of photos from observation in this household:

Page
97
The compound: two houses with kitchens (one with a pen for sheep) and calves sleeping inside and one pen for
the cattle (half obscured behind the left hand house)
Grandmother washes 3yr olds face with water shortly after waking
The number of jerry cans of water collected each day
Straw bed used by the grandmother and 3yr old; everyone except the father sleep on the floor on a woven mat in
the other house

Page
98
Pit for rubbish – it is then composted and put on the farmland. Everything except animal dung can go in here
Mother washes the clothes on a rice sack using bar soap and 35L of water
Page
99
Clothes line showing the number and type of clothing washed with 35L of water
COMMUNITY E: HH10
General notes:
The family have 4 children, a boy of 18, a boy of 14, a girl of 12 and a girl of 2.
The house included two buildings, one main house where everyone slept and one round house which served
as the kitchen and where the animals were kept at night.
The day we visited the family had had their uncle stay overnight in their house.
The family were celebrating Timkat and were also preparing for a funeral meaning that practices were
slightly different from normal.
The father of the family sells eggs from the village to Addis Ababa and was only at home briefly for the
holiday.
The family had three mobiles but not electricity.
The family had 2 cows, 2 donkeys, and 6 sheep that were mainly in the yard while we were there.
In the morning the family had 1.5 25L gerry cans of water available. They had 3 25L gerry cans in total
The waterpoint was an afridev pump and no queue was observed on either of the two occasions they visited
it. There was also a river nearby which was used for bathing and laundry.
The family had several bars of soap as well as small packets of shampoo.
The elder two boys slept in one bed with the uncle and the mother, father and two younger children slept in
one bed.
Although few flies were observed generally in the compound a lot of flies were observed on the animals.
There was no toilet at the household and open defecation was observed.
There was a rubbish pit at the house which had more moist waste than at other households. The rubbish
area was far from the house.
Time Observed activities
7.00am Observation starts. Everyone waking up. Cows and donkeys are let out of hut. 14 year old gathers the dung from inside the hut and puts it in a basket
7.05am Mum roasts coffee
7.10am 14 year old sweeps the inside of the house and puts it in a small container which he then takes to the back of the house and throws on the rubbish pile. 12 year old lets out the sheep. Mum boils the water. Boy 14 then washes his hands, hair and face with liquid soap/shampoo from a small packet.
7.15am 18 year old pounds coffee. 12 year old does more sweeping of the hut where the animals were. 14 year old washes his legs without using any soap. He dries face and hair by shaking them vigorously. 2 year old defecates right behind the house with the animals/kitchen in it. No handwashing is observed and no covering of the faeces is observed.
7.20am Mum prepares coffee, lighting the oven and washing the coffee pot. 14 year old gets changed into his school uniform. Mum wipes her own face with the 2 year old’s garment.
7.25am 14 year old and 2 year old eat njira and spice in the main house. 18 year takes a plastic bag full of his clothes and hangs several of his clothes out on the fence in the sun to air. Dad feeds hay to the cows in the yard.
7.30am 18 year old brings large box of eggs outside to the porch. 12 year old girl washes her hands, initially without soap. She then begins to wash her face and adds bar soap (small slither). Blows nose with fingers in the process. Dad pours water for the 2 year old who asked to wash her hands. No soap is used.
7.35am A mixture of warm and cold water is used to wash the coffee cups. Father gives the 14 year old money and then the boy goes to school. 2 year old hangs out with the father on the lawn near the cows.
7.40am Mother and father carry the mattress outside down by the side of the house to air. The 2 year old puts a shoe in her mouth and the father says not to.
7.45am 12 year old throws some more rubbish from the household alongside the house, on the porch. The mother and father take a blanket and hang it across the doorway between the two rooms in the house. Mother washes hands with a larger bar of body soap (brand ‘giv’). The daughter pours water for her. The mother then washes her face with water only.
7.50am 2 year old tries to wash the shoes in the gerry can. She is told this is wrong and the remaining water is used to water the banana plants. Father also washes hands with ‘giv’ soap while the 12 year old pours water. He

Page
100
washes his face with soap and rinses his mouth, using his fingers to rub his teeth.
7.55am Mother lights incense. Father is served Njira and spice. Mother pours and serves him coffee.
8.00am Mother wipes 2 year old’s face with fingers. 18 year old and 12 year old also eat. 18 year old gives food to 2 year old.
8.20am 2 year old is encouraged to serve the njira to the rest of her family and pick up the empty coffee cups.
8.30am Mother washes coffee cups and some other dishes with hot water. Dad goes to field.
8.35am Mother throws dirty water into a container in the yard for the cattle to drink. The uncle washes his face and hands with liquid soap/shampoo. 12 year old pours. He sits on a stool while washing. He uses more water than others to wash.
8.40am 18 year old goes for water. The uncle grooms his hair in the mirror.
8.45am Mother begins to re-lay the floor inside the main house. The 12 year old helps, firstly by pouring water and then by spreading it around.
8.50am 18 year old returns with gerry can full of water. The walk is about 10 minutes and there was no queue at the waterpoint.
9.05am They finish relaying the floor in the house and on the porch. 18 year old pours water for the mother to wash her hands. No soap used.
9.10am Mother washes a cup, tin and plate with water and re-lights the fire. Daughter washes hands with water only (no one pours for her). She then pours water for the uncle to wash his hands.
9.15am Daughter starts to wash her feet but stops to collect rest of fresh cow dung from the yard. Mother sweeps rest of the porch and garden around the house.
9.20am Mother sweeps up child’s faeces from earlier (now dried). 12 year old goes to the back of the house, near the rubbish pits with the cow dung and begins mixing it with dirt to be made into cow pats. By this time the 2 year old has been eating raw chickpeas and has a snotty nose.
9.25am Mother splashes some water outside where she is sweeping and sweeps rubbish into basket. The rubbish, including the human faeces, is then added to the rubbish pile. The mother then collects some of the dry cow pats and moves them to the front of the house where there is a large pile. The 2 year old attempts to assist her mother and elder sister carry the dry cow pats to the front of the house.
9.40am 12 year old washes hands and then also rinses the gerry can. Neither the mum nor daughter wash their feet after laying the cow dung inside the house. Mother tends to fire.
9.45am Daughter and then mother sharpen knife on a stone outside. Mother washes chopping board and begins to prepare an onion.
9.50am Mother washes plates with water.
10.05am 18 year old washes hair with packet soap/shampoo. Then washes faces with soap and uses only water to wash his legs. 12 year old gives hay to the cows.
10.10am Dad shaves at the rear of the house. The 12 year old holds the mirror for him. The 18 year old gets changed.
10.15am 18 year old takes dirty water out for the cattle. Mother chops wood.
10.20am Mother tends to fire – using a mixture of wood and cow pats for fuel. Daughter washes plates. Mother criticises 18 year old and uncle for using so much water to bathe.
10.30am 18 year old goes to the water point
10.36am Arrive at the water point and fill gerry can right away as there is no queue.
10.45am Returns with water to the house. Father gets changed and ready for church as there is a funeral.
10.55 Mother serves the family bread and the traditional drink (taleh) to the family. Incense is lit and then father says a prayer since to mark Timkat.
Key Photos:
Below: the father took a lead role in the parenting of the youngest child.

Page
101
Below: The uncle grooms himself in the mirro after washing.
Below: the mother sweeps up the child’s dry faeces and deposits it in the rubbish pit at the rear of the house.
Below left: The 2 year old daughter copies her mother as she moves the dry cow dung to the front of the house.
Below right: Although there is a lot of animal faeces around, both the wet and dry dung do not attract many flies.

Page
102
Below left: The rubbish pile which is far from the house.
Below right: The 2 year old was observed to defecate right behind the house
Above: Clothes are hung out to dry before they are worn later in the day.
Below: The 14 year old uses liquid shampoo to wash his hair and the remaining soap to wash his face and hands.

Page
103

Page
104
APPENDIX C. FOCUS GROUP DISCUSSION GUIDES
Focus Group Discussion 1 with mothers of young children
Covering behaviours related to sleeping and laundry
1. Introductions of researchers and participants individually. 2. Explain the purpose of the focus group – to understand more about the daily lives of people in this
community. Explain that it will be a discussion with several interactive activities. Ask participants if they feel comfortable participating and sharing their opinions and ideas. If yes ask them if it is also ok to film and take photos during the focus group. Explain that nothing they say will be directly attributed to them but rather reported anonymously. If all agree get them to sign a consent form.
3. Explain that in a discussion like this it is helpful to have some ground rules. Suggest that these should be: a. Whatever is said during the discussion should not be discussed outside this group with others in the
village. b. Treat the opinions of others with respect as there is no right answer to what we ask and all opinions
are valuable. c. Put your hand in the air when you wish to speak and do not speak over others. d. If you don't understand something please ask us to clarify. e. If you feel uncomfortable, please let us know.
4. Explain that we have been in their community now for several days and that we have learned that some of
the activities that they do on a day to day basis include, sleeping, bathing, doing laundry, washing their faces,
cooking njira, going to the toilet, and sweeping and clearing rubbish. For each action place down a card with
a drawing of the activity. Get agreement that these are things that people in this community do in their day
to day lives. Explain that today we mainly want to discuss sleeping patterns and laundry.
5. Now we would like to introduce you to an imaginary family. The family includes a mother and a father (show
cut out figurines) a baby boy who is 2 years old, a girl who is 5 years old, a girl who is `3 years old and a boy
who is 18 years old. We would like you to imagine that they are a normal family living in a normal house in
this community.
6. Can you help us to draw a picture of a normal house in this community (draw from an arial view).
7. Now let’s place each family member into the house showing where they would sleep.
8. What would these people use to cover themselves while sleeping?
9. What would they put under their head while sleeping, if anything?
10. Who would share blankets/sheets/ pillows with who? Is there anyone who can’t share with someone else?
11. Now I want you to imagine that their uncle comes to visit and stays the night. Where would he sleep?
12. Having someone come to visit is one example of something that may cause sleeping arrangements to
change. Are there any other reasons sleeping arrangements change?
13. How often do people around here wash their sheets/blankets? As we have travelled in your community
some people have told us every 3 days while others have said 2 months, what factors determine this
variation? Probe on:
Dirtiness
Time pressure
Available water
Seasonality
Soap availability
Distance to water.
14. Do people wash pillows often (if used)?

Page
105
15. How does it feel when sheets have been cleaned? Do people notice the difference?
16. When are other clothes washed? Where and with what?
17. We would like you to help us list the different types of clothes people have. For example we have seen baby
clothes. As each is listed write/draw them on separate cards. Probe for categories such as:
Clothes by gender
Work clothes vs special occasion clothes
Clothes for specific activities like school uniforms.
18. When the list is created ask about how often each category of clothes is washed and why.
19. What if they had a big pile of washing to be done but were unable to do it all that day. Rank the cards in
order of priority.
20. What factors may limit their ability to wash clothes frequently?
21. Has anyone heard of trachoma? If so get them to explain it to the group.
22. If not has anyone heard of a disease that causes blindness or people’s eyelashes to turn in?
23. Explain a little about trachoma. Trachoma is a result of eye infections that happen as a child and lead to
blindness in adults. The disease can move from one person’s eye to another. The reason we have been
talking about bedding and laundry today is because if a person has trachoma it can be transferred onto the
bedding and then be transferred to another person’s eye if they are sharing that bedding. (Use transmission
cards to demonstrate this). Now we would like your help to see if there is anything to do with sleeping or
laundry that we could change in this community so that we could reduce the spread of trachoma.
24. So if we look at where our family were sleeping is there any way we can change the way people sleep?
25. Could more space be created between where people lie?
26. Could people sleep head to toe?
27. Would it be acceptable/affordable for everyone to have their own blanket, including children?
28. How could pillows be different so that they could be washed more?
29. Could the pillow be made from a fabric that could be whipped daily (eg a rice sack stiffed with clothes)?
30. What solutions might there be to making sure bedding is washed regularly?
31. How frequently do you think you could feasibly be able to wash the bedding?
32. If you had little water available how can you still wash the bedding?
33. If you had little time available (such as during harvest season) how could you still wash the bedding?
34. Would it be affordable to always have one set of clean sheets?
35. Would you be willing to only prioritise washing the pillow more regularly?
36. How would you feel if your child came home from school and said that they felt that the sheets were dirty
and they should be washed?
37. How would you feel if your child came home from school and asked for their own blanket/pillow?
38. If we think about trachoma, infection form one child’s eye to another could also occur through clothing or
material that is used to wipe a child’s face. This is most likely to be the child’s own clothes or the mother’s
clothes. Can you think of any way that washing children’s cloths and the scarves/wraps that mother’s wear
could be given priority (for example over the husband’s clothes)?
39. Could anyone else in the family help do the washing if you didn’t have time?
40. Can you suggest any other ideas that could enable clothes to be washed more frequently?

Page
106
Focus Group Discussion 2 with mothers of young children
COVERING BEHAVIOURS RELATED TO FACE WASHING AND BATHING
INTRODUCTIONS & CONSENTING
FACE WASHING
1. Family scenario cards – introduce participants to the family and ask for each person:
a. When in the day would they face wash? (Write the times on post it notes underneath each person)
b. How does this vary by season?
c. Why do they face wash at these times?
d. When don’t they do this?
e. Who needs help or reminding?
f. What is used to wash the face (e.g.) soap, when is soap not necessary when washing the face?
g. Does the face need to be dried and what would be used?
2. How does it feel when you’ve washed your face?
3. If you return from the field and cannot wash your face because there is no water then how does it feel?
Would anyone say anything?
4. If your child had to go to school with a dirty face then how does it feel? Would anyone say anything about
you as a mother?
5. Are there any benefits to face washing (other than the things said in response to qu 3)
6. Would you be happy for your child to play with a child with a dirty face?
7. If you are in the field with your 2yr old and their face is dirty what would you do to clean it?
a. Prompt: talk about wiping the face with hands and clothing
BATHING
1. Return to the family scenario. Ask:
a. When would each of these people wash their whole body (write on post it notes)
b. What do they use and where do they wash?
c. How does this vary by season?
2. What might prevent you from bathing as regularly as you like?
a. Prompt for following if they don’t emerge: privacy, time, water
TRACHOMA
1. Has anyone heard of trachoma – what is it?
2. If not: has anyone heard of an eye disease where the eye lashes can turn inwards and you can go blind? Do
you know anyone like this?
3. Use cards to explain how trachoma spreads from the eyes of one person to the eyes of another person and
explain the role of facewashing and issues with flies using the cards and why we have been talking about
these behaviours / issues.
4. Ask the group to help you think now about ways to stop trachoma spreading
SOLUTIONS: FACE WASHING

Page
107
1. Explain again that facewashing can reduce flies on the face and bathing is also important because faces are
washed. We’d like to discuss how we can increase the frequency of facewashing.
2. What would make it easier / more convenient to wash faces more regularly?
3. What would make it easier / more convenient to bathe more regularly?
4. If we want to increase the frequency of face washing what additional times of day could faces be washed?
(Use the family scenarios and remind the of the post it notes with the times that faces are currently washed)
5. Would you have enough water if your child came home from school and said they need to wash their face at
these additional times?
6. How could we reduce the amount of water used for face washing?
a. Can water be captured and reused? Is this done? What can water be reused for? What about soapy
water?
7. Who has a mirror? Have you ever looked in a mirror to see if your face is clean?
8. Would this be a useful aid for face washing if it was kept near where faces are washed?
9. Show them the water bottle with the stick in it and explain a tippy tap and how it works – would this be
useful?
10. Show the drawing of a possible facewashing station which uses little water, has a mirror, and has soap kept
there – what do they think about this?
11. Kids get snotty a lot, what age child can be taught to clean a snotty face? What age can they assist a younger
child?
12. Get everyone to try a face wipe and as how it feels.
a. Explain that you have to buy them and throw them away after using – ask if anyone things they
would buy face wipes? At what cost?
13. Drying a face after washing can stop flies landing on it. If you had a cloth/ towel or something only used to
dry the face of one child would that be feasible financially / practically (e.g. could you wash it regularly and
would you use it?) Note: scrapped this question as they don’t dry faces
Thank participants, ask if there are any questions and close focus group.

Page
108
Focus Group Discussion 3 with mothers of young children
COVERING BEHAVIOURS RELATED TO GARBAGE, FLIES, SANITATION & HANDWASHING WITH SOAP
INTRODUCTIONS & CONSENTING
1. Mention that we have been observing their lives and have observed the following activities taking place:
sweeping, fetching water, going to the toilet, bathing washing faces and hands, making njera etc. Tell the
behaviours we will focus on in this focus group.
GARBAGE
1. What type of things get thrown away? How often?
2. Show map of a compound and explain it. Ask the participants to imagine this is their home and ask them
where they would dispose of rubbish in this compound. Mark it on the map.
a. Ask someone to walk away from the group with rubbish and ask the group to decide when the
rubbish is far enough away from the house (if the group is the house).
b. Do you do anything to the garbage to help to dispose of it?
c. Does vegetable waste get thrown in the same place?
d. Is it also OK to leave waste anywhere within the compound?
FLIES
1. Do you feel that there are a lot of flies in this community at the moment?
2. Does the amount of flies change at different times of year?
3. What might be the cause of flies in the community?
4. What can you do to reduce flies? Inside and outside the home?
a. If it doesn’t come up: do you use incense or something similar?
5. How do you feel when flies land on your face / your children’s faces?
a. Is there anything you can do to stop this?
6. If your child is snotty and you wipe it with your hand is this enough to be clean? (i.e do hands need washing
– how dirty is snot)
7. Can flies cause any problems?
SANITATION
1. Where do people in this community go to defecate
2. Show the family cards and use the map of the compound to ask questions about the defecation practice of
this family. Note: this community had latrines so asked them to imagine the time before the last 5 years or so
when they didn’t have a latrine.
a. Where would each person defecate?
b. Where else can they defecate?
c. What happens with child faeces?

Page
109
d. What would you do if X person defecated in X spot?
3. Say that we are not from here, imagine that this person was visiting your house and needed to defecate
a. Where would she go (use a family card to indicate on the compound map
b. Ask the group the following questions and act out their responses:
i. What does she take with her?
ii. What does she do when she gets there (I.e.to see if they cover faeces)
iii. What does she do when she’s finished?
4. If no one was here to ask when she had to defecate and she decided to go ‘here’ (point to a place within the
compound) because she saw a lot of animal faeces there would that be OK?
5. Why is human faeces different from animal faeces?
6. Does anyone in this community have a latrine? Note: this community all had latrines so had to adapt
questions.
7. What are the good things about latrine? Bad things?
8. When do parents stop accompanying a child to the latrine?
HANDWASHING
1. Earlier you said (if they say it) that hands need to be washed after the latrine. When else do hands need to
be washed?
a. Which of these times needs soap?
2. Do you have a specific place for washing hands or does it depend on the activity?
3. Children often have dirty faces as we have discussed – is it too much for a mother to wash her hands each
time she wipes a child’s face with her hands?
TRACHOMA
1. Has anyone heard of trachoma – what is it?
2. If not: has anyone heard of an eye disease where the eye lashes can turn inwards and you can go blind? Do
you know anyone like this?
3. Use cards to explain how trachoma spreads from the eyes of one person to the eyes of another person and
explain the role of the behaviours we have been discussing.
4. Ask the group to help you think now about ways to stop trachoma spreading
SOLUTIONS – GARBAGE
1. Could you increase how often you dispose of garbage? What is reasonable Note: not asked as everyone
disposed of garbage every day multiple times
SOLUTIONS – SANITATION (note – most questions not relevant as they have latrines in this community)
1. If note said: if you dig a hole, defecate and cover it so flies cannot get to it how would you dig this hole?
2. Would it be possible to put child faeces where the rest of the faeces goes (if relevant based on discussion)
3. Do you want a toilet? Why (not relevant as everyone has a latrine here)
4. Do you know anyone who can build a toilet?
5. If you ask your husband to build a toilet what would he say?
6. How much does it cost? How do you afford this? Can you use savings groups to save for latrines?
7. Would you feel more content / proud / respected if you had a latrine? (Changed during discussion to ask
how they feel now they have a latrine).
8. Thank participants, ask if there are any questions and close focus group.
Page
110
FOCUS GROUP DISCUSSION WITH GRANDMOTHERS OF YOUNG CHILDREN
Covering Beliefs, attitudes and cultural practices
41. Introductions of researchers and participants individually. 42. Explain the purpose of the FGD – to understand more about the daily lives of people in this community.
Explain that it will be a discussion with several interactive activities. Ask participants if they feel comfortable participating and sharing their opinions and ideas. If yes ask them if it is also ok to film and take photos during the focus group. Explain that nothing they say will be directly attributed to them but rather reported anonymously. If all agree get them to sign a consent form.
43. Explain that in a discussion like this it is helpful to have some ground rules. Suggest that these should be: f. Whatever is said during the discussion should not be discussed outside this group with others in the
village. g. Treat the opinions of others with respect as there is no right answer to what we ask and all opinions
are valuable. h. Put your hand in the air when you wish to speak and do not speak over others. i. If you don't understand something please ask us to clarify. j. If you feel uncomfortable, please let us know.
44. Explain that during this discussion we will be covering a lot of different topics.
-------------------------------
45. Explain that we have been guests in the community for a few days. We want to learn more about how they
normally treat guests in this community and how you would welcome a guest to your home. Probe on:
a. Things you would do when a guest arrives
b. Food and eating
c. Sleeping arrangements if the guest stays overnight
d. What would happen if a guest arrived unexpectedly? What kinds of things would they be worried
that they didn’t have change to prepare?
-------------------------------
46. Now we would like to know your attitudes towards some things. Use cards to explain each thing one by one.
The following separate cards are presented: cow dung, human faeces, blood, dirt under finger nails, snot,
eye discharge, vomit and rotting meat. Ask participants to rank these things from not so disgusting to most
disgusting. Discuss why the cards are placed where they are.
-------------------------------
47. We want you to imagine that your daughter or daughter in law acquires an illness in the next 5 years. Show a
card for each of the following flu and cough, a limp, deaf, blind, loss of a leg, brain injury and back pain.
Page
111
Make sure the understanding of each is clear. Ask the participants to rank the cards from least bad to most
severe illness.
48. How would their daughter’s role as a mother change if she became blind?
49. Would her family change the way they treat her?
50. Would the community change the way they treat her?
51. Is becoming blind something that you think could happen to a member of your family?
52. If someone becomes blind what do you think could be the causes?
53. Have you ever heard of trachoma? If yes, what do you know about it? If no, have your seen anyone who is
effected by a disease that causes blindness and eyelashes to curl in?
54. Do you know how you get trachoma?
55. Do you know how you can prevent getting trachoma?
----------------------------
56. We would like you to help us draw a picture of a good mother. Here is a sketch of a stick figure which we will
add to based on what you describe. Probe for:
a. What would her body look like?
b. What would her facial expression be?
c. What would her hair be like?
d. What would she wear?
e. What would she carry?
f. What would her personal hygiene be like?
g. How would she behave?
h. What lessons would she teach her children?
i. How would she help her children maintain their personal hygiene?
j. At what age would a good mother expect her children to look after their own personal hygiene?
-------------------------------
57. We have learned that your big celebrations are Epiphany, Easter, New Year, Mascal and Christmas. During
any of these celebrations do you do anything different with your clothes?
58. During these celebrations do you do anything different to your house?
59. Do you need to be cleaner than normal for these celebrations? How?
--------------------------------
60. Often when we have wanted to wash our hands in your community someone has offered to pour water for
us. Yet when we offer to pour water for them to wash their hands they often decline. Why is this?
61. What other ways are there in this community to show respect?
--------------------------------
62. At what times during the day/ or after what activities do you feel most:
a. Happy
b. Content
c. Proud or pleased with something you have done?
Page
112
---------------------------------
Focus Group Discussion 5 WITH FATHERS
Covering Community Structure, Roles of men and women and decision-making
INTRODUCTIONS & CONSENTING
1. Explain that we want to understand their community structure and social groups, roles of men and women
and how decisions are made
TOUCHPOINTS
1. Can you tell me about all of the groups that you have in your community and where you spend your time?
Who is involved? What topics if relevant? Frequency of meeting?
DRAW a touchpoint map in front of them as they talk
a. Prompt:
i. Sports groups
ii. Music
iii. Water groups
iv. Anything for men, women or kids
v. Church
vi. Health / clinic related
vii. Kabele meetings and related activities
viii. Events with other kabeles
2. We know that you have a kabele leader. Does he make all of the decisions or are there structures in place to
help him?
MEDIA & PROGRAMS
3. How else do you get information?
a. Prompt for TV – who watches and where
b. radio – shows and channels
c. print – does anyone read?
4. Have any health or education programmes been run in your kabele?
a. Ask them to describe and probe based on what comes up about who was targeted and how they
were delivered
ROLES OF MEN & WOMEN
5. Use A3 paper for men and women. Ask: Can you tell us about the activities and jobs that a man and his wife
would do in their homes and with their families?
a. Probe on: key behaviours (bathing, face washing, water collection, laundry and construction)
b. Which roles can be done by a man or woman?
6. Building: what is the last thing that you built? How did you decide what to use, where did you get materials?
Cost?
7. Who makes decision within the household and about what?
a. What do women decide on?

Page
113
b. Probe on building and products - can a woman ask a man to build something? Can she chose to buy
products like perfume and soap? Does a wife have money to buy these things as and when she
chooses?
ROLE OF MEN IN RAISING CHILDREN
8. What lessons should a good mother teach to her children?
a. Do men ever get involved in teaching children these things?
b. Have you ever asked your wife to do something for the children that she hasn’t done before or did
differently to how you would like?
TRACHOMA
9. Who has heard of trachoma? What is it?
10. If they don’t know ask who has heard of a disease where eyelashes turn in and you go blind
11. Do they know anyone who has that?
12. What do you know about how you get trachoma?
13. What can you do to prevent it?
14. Where did they hear this info (if they know anything)?
a. Have their kids ever brought health info home from school? Has anything they have ever said
influenced their actions?
POSSIBLE SOLUTIONS
1. We are interested in how to prevent trachoma in communities like this.
Flies
1. Tell them how it spreads if they don’t know using the eye cards and start with flies
2. Do they do anything to control flies in their homes? Probe
3. Ask the if they could catch flies in a glass with sugar and whether it could work and where you would put the
glass
Facewashing
1. Use eye cards to explain importance of face washing for trachoma control
2. Sometimes it is difficult to wash children’s faces regularly because water and soap may not be readily
available or the child’s face is dirty so often. Do you have any suggestions for how we can get children’s faces
clean often?
3. Give each man a face wipe. Would they buy them? Who would use them? What would they pay? Could their
wife buy if they chose to?
Bathing
1. Do you think it is always easy for your teenage daughters and wives to bathe?
a. Probe on privacy
2. Does anyone have a bathroom in this community?
3. If you had one what would it be built from and what would be inside? Ask them to draw it?
4. If your wife said she would like a bathroom what factors would prevent you from building one
5. Is it possible to keep soap outside? Problems? Solutions?
Thank participants, ask if there are any questions and close focus group.