research | training | policy | practice the legacy of the war on poverty’s health programs for...
TRANSCRIPT
Research | Training | Policy | Practice
The Legacy of the War on Poverty’s Health Programs for Non-Elderly Adults and Children
Barbara (Bobbi) WolfeJune 12, 2012

Major Components of the War on Poverty’s Health programs
• Medicaid– Expanded to Children's Health Insurance
Program
• Neighborhood Health Centers– National Health Service Corp added to
attract providers
Pre War on Poverty
• Public sector – – public hospitals, military health care,
Public funding for medical research, school health programs, programs to promote maternal and infant health, worker’s comp for health
–~one percent of GDP
• Private insurance covered < 30% of private health spending. Employers provide as cost of business so tax subsidized.
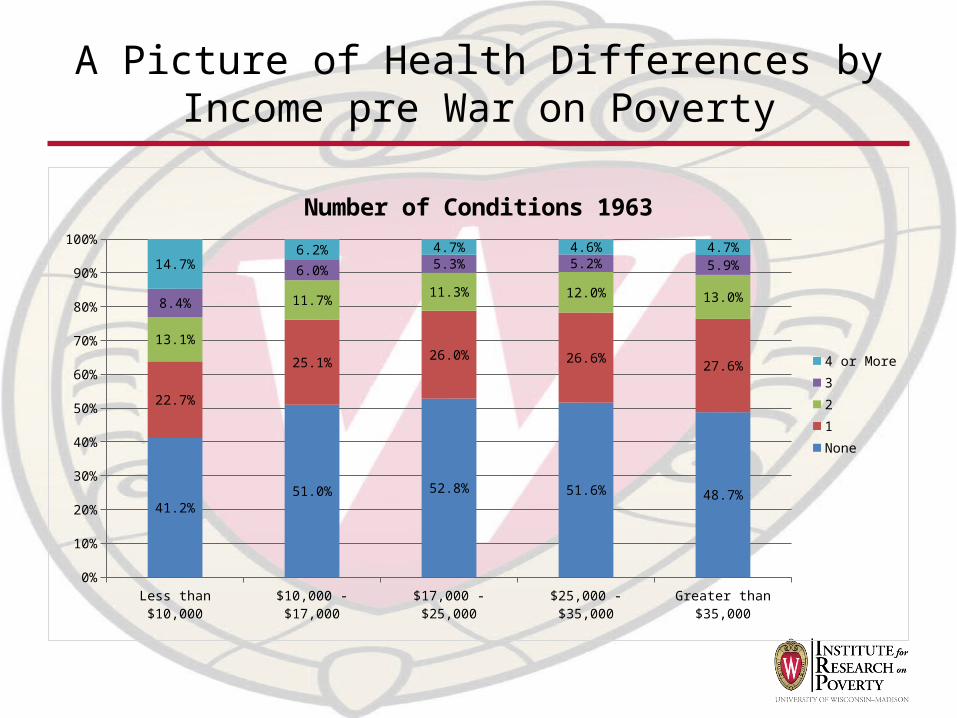
A Picture of Health Differences by Income pre War on Poverty
Less than $10,000 $10,000 - $17,000 $17,000 - $25,000 $25,000 - $35,000 Greater than $35,0000%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
41.2%51.0% 52.8% 51.6% 48.7%
22.7%
25.1%26.0% 26.6%
27.6%
13.1%
11.7%11.3% 12.0% 13.0%8.4%
6.0% 5.3% 5.2% 5.9%14.7%6.2% 4.7% 4.6% 4.7%
Number of Conditions 1963
4 or More321None

Medicaid• Became law in 1965; a Demand side program that provides
coverage to eligible persons• Joint federal-state program
– Federal – minimum benefit package; majority of financial resources (match based on average per capita income in state: range 50-83 percent.) Mandatory groups- single-parent family members, quickly expanded to pregnant women• Minimum benefits for children 1967, Early & Periodic Screening,
diagnostic and Treatment
– State – option to cover additional groups (medically needy) and services and set income-eligibility for mandatory groups (tied to AFDC eligibility).
– Major Eligibility Expansions: • 1986-pregnant women and infants with income <100% FPL as
state option; 1988 mandatory. 1989: expanded to cover up to 133% FPL. & up to age 6.
• 1990: All children to age 18 up to 100% FPL• 2010: ADA – all under 133% FPL
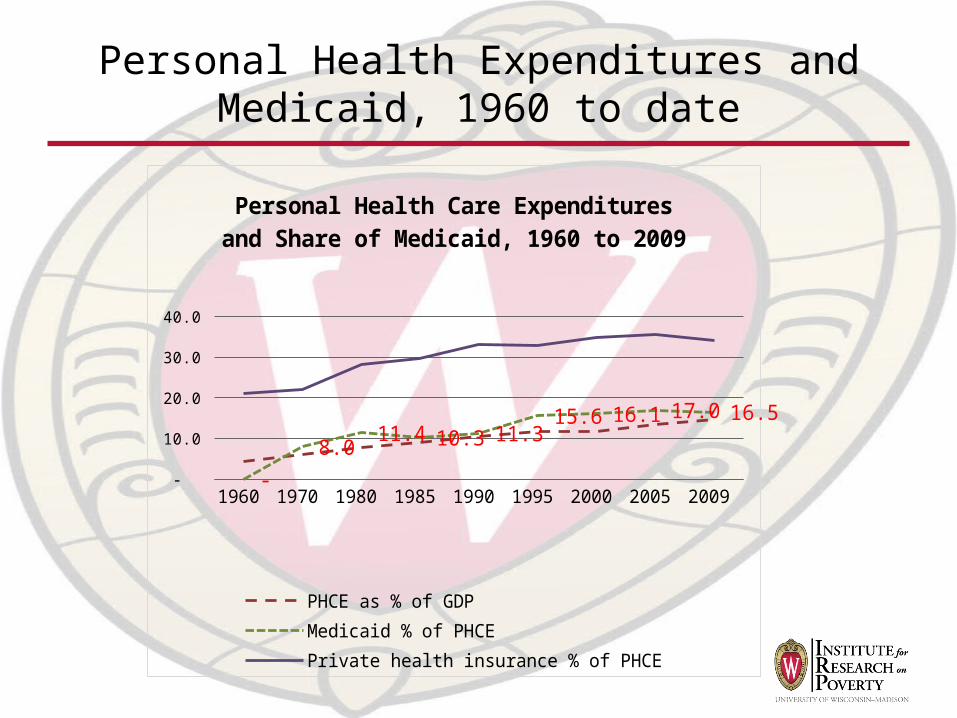
Personal Health Expenditures and Medicaid, 1960 to date
1960 1970 1980 1985 1990 1995 2000 2005 2009 -
5.0 10.0 15.0 20.0 25.0 30.0 35.0 40.0
-
8.0 11.4 10.3 11.3
15.6 16.1 17.0 16.5
Personal Health Care Expenditures and Share of Medicaid, 1960 to 2009
PHCE as % of GDPMedicaid % of PHCEPrivate health insurance % of PHCE
Core problems with Medicaid
– Zero-one nature re eligibility. “Notch”• Negative labor market incentive• Negative private coverage incentive
(increases uninsured) May change use of care in way that influences health
– Coverage varies by state: inequality– Crowd-out. – Low reimbursement especially for
specialists and oral health providers limits access
– Cost of program esp. to states

Evaluation tied to core issues
– Wisconsin Badgercare• Eligibility to 185% FPL, no asset test, family coverage• Premiums for higher income families• State subsidy for ESI for those eligible for BadgerCare (tied
to income)• outreach
– Outcomes: increased coverage. Evidence that bridged gap between public and private provision. Estimates of crowd out about 25%
– Medicaid Managed Care Program- (Kaestner, DuBay and Kenney)• evaluate effect of MMC on prenatal care usage and infant health.
• Find no tie to adequacy of prenatal care; or health outcomes.
– Community Care of NC (KFF study)• Medical home model-MDs, hospitals, county health & social
service agencies coordinate care. 24/7 access on call• Improved care and cost savings.
ACA –lessons from Experience of Medicaid
• Makes eligibility more uniform across states
• Raises importance of smooth transition from Medicaid to private coverage– Subsidy plan; administration and
implementation– Providers who participate
• Access – will providers participate? Reimbursement
• Medical or health homes to improve care for chronically ill

(State) Children’s Health Insurance Program
• 1997: SCHIP 2009: CHIP• Joint federal state program to expand
coverage beyond Medicaid to low income children. extensive leeway to states. – Coverage varies from 160% up to 400%
FPL.– Targeted on children but states have
option to expand to parents. – Federal government pays Medicaid rate
+ 15%
• Issues – low take-up rate, churning enrollment and crowd out.

Evaluation• Focus on Take-up rates and strategies to increase
(2009=84.8%)– Outreach– Simplify enrollment– Longer periods of eligibility
• Focus on Crowd-out and ways to reduce– Use of waiting periods; lock-outs– Premiums
• Improvements in coverage for children?– CPS data show drop in uninsured children < 250% FPL while
adults increase rate
• Improvements in access?– Greater utilization if have Medicaid/Chip but disparities
continue in quality, and access to specialty care including time to appointment
– Managed care networks not serve both Medicaid/CHIP and privates

Neighborhood Health Centers
• Concept: provide health and social services in poor and medically underserved areas and promote community empowerment. Established in 1965 as part of War on Poverty.
• Slow growth – perceived threat and only benefit those in geographical areas would be served (supply side approach that differed from private insurance.) – Early 19070s only ~ 100. Now 1,124 and under ACA expected to
double capacity– 2010 served 19.5 million – 93% < 200% FPL; 72% <FPL
• FQHC-1989 on– 90% federally qualified; – all can receive cost-based reimbursement from Medicaid and Medicare
(since 1989). – FQHC covered for malpractice. – Medicaid accounts for 37% of funding; federal grants 25%, state &
local grants 12%

CHC - evaluation
• Most compare CHC to other providers– Quality of care; access; disparities; cost-effectiveness– Mostly favorable
• Reduced infant mortality rate and low birth weight• More up to date on cancer screening than
comparable women• More pediatric patients have recommended
preventive care• Lower rate or ambulatory care sensitive
hospitalizations• Lower cost than comparable care—Medicaid covered
CHC patients lower hospitalizations rates and fewer annual hospital days

Issues-CHCs
• Current issue – insufficient funding to serve population– 1985-2006 real / ca appropriations steadily decreased
• Staffing – Funded vacancies esp. in rural areas
• Access to specialty services• Can they expand to meet expected increase in demand?

Measures of Success of These Programs-insurance coverage
• In 1965, >70% of population had hospital coverage; 67% surgical care but little else. >25% had no coverage. By 1970, 15% had no coverage*.
• Records of actual coverage only begin in 1982 (earlier count policies.)
1982
1983
1984
1986
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
0%5%
10%15%20%25%30%35%40%
34%33%31%33%32%34%
30%30%30%28%27%29%29%29%29%28%27%25%27%28%28%28%
26%28%30%29%
10%11%10%10%10%11%11%13%12%13%12%12%11%11%10%11%10%11%12%12%12%13%12%13%13%13%
Rate of Uninsured by Poverty, Whole Popu-lation,
1982-2010
Below the Poverty Line Above the Poverty Line

Indicator of success of Medicaid and S-CHIP on covering children
1982
1983
1984
1986
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
0%
5%
10%
15%
20%
25%
30%
35%
40%
34%
31%30%32%32%32%
27%
24%23%21%
20%20%22%
21%21%20%17%
15%15%16%16%16%13%
16%15%13%
11%11%10%10%10%
12%11%13%
11%13%
11%11%10% 9% 8% 9%
7% 7% 7% 7% 7%9% 8% 8% 7% 7%
Rate of Uninsured by Poverty, Children, 1982-2010
Below Poverty Line Above Poverty Line
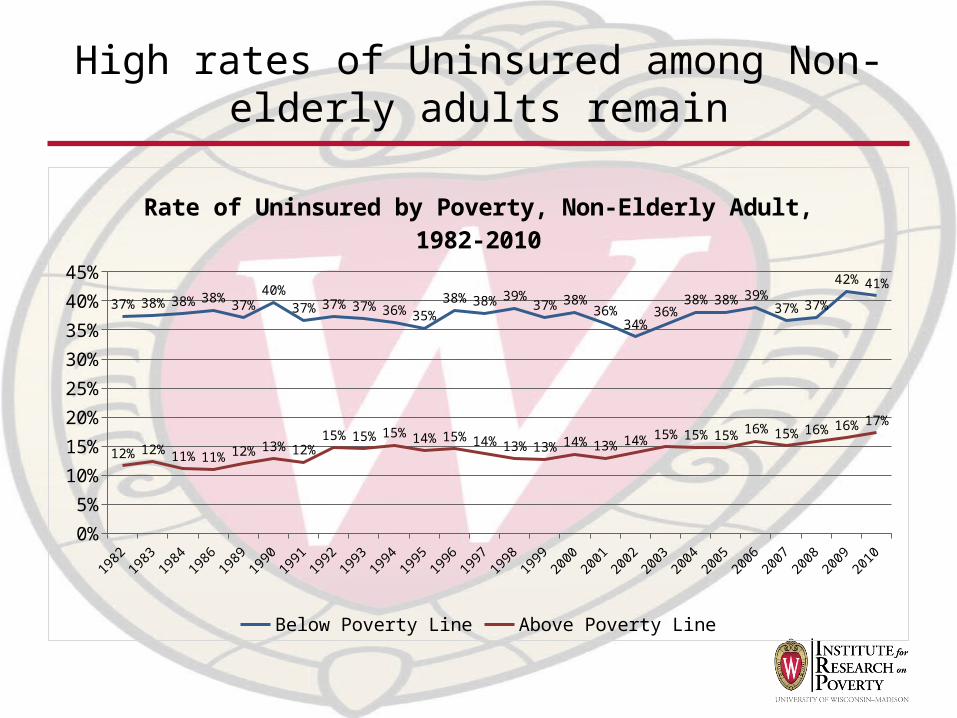
High rates of Uninsured among Non-elderly adults remain
1982
1983
1984
1986
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
37%38%38%38%37%
40%37%37%37%36%35%
38%38%39%37%38%
36%34%
36%38%38%39%
37%37%
42%41%
12%12%11%11%12%13%12%15%15%15%14%15%14%13%13%14%13%14%15%15%15%16%15%16%16%17%
Rate of Uninsured by Poverty, Non-Elderly Adult, 1982-2010
Below Poverty Line Above Poverty Line

Indicator of Success-utilization disparities
1963 1968 1973 1978 1983 1988 1992 199660%
65%
70%
75%
80%
85%
60%
69%
74%76%
74%
76%77%
78%
67%
70%
74% 75%74%
76%77%
78%
74%75%
76%77% 78%
79%
81%
83%
Visited a Doctor in the Last Year, 1963-1996
Low Income Middle IncomeHigh Income
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
2006
2008
2010
70%
72%
74%
76%
78%
80%
82%
84%
86%
88%
Visited a Doctor in the Last Year by Poverty Status,
1982-2010
Below the Poverty Line
Above the Poverty Line

Indicator of Success – infant mortality rates by race
1950 1960 1970 1980 1990 2000 20070
5
10
15
20
25
30
Twenty-Eight-Day Infant Mortality Rate by Race, 1950 to 2007
White infants Black infants
Final thoughts1. Bulk of evidence clearly suggests that the combination of
Medicaid/Chip/CHC /NHSC have increased health insurance coverage, access (as captured by utilization) to medical care for the poor and decreased gaps in health status.
2. ACA if enacted will extend these benefits though clearly major issues remain in terms of actual access to beneficial care
3. It is also clear that evaluations in this area are complicated; beyond asking limited questions (for ex., take-up, crowd out, costs of care, labor market incentives, infant mortality) the profession has not done well at understanding the full benefits of this set of programs
1. Endogeneity of take up of Medicaid and use of CHCs2. Inaccuracy of numerous measures of health and limited scope of
others (mortality, infant mortality)3. Long term nature of health and effectiveness of medical care. 4. Role of risk taking behaviors/knowledge/exposures with health
consequences5. Difficulty in conducting experiments that might deny coverage or
access to care.