resident – faculty advisor & mentorship systems brian v. reamy, md colonel(ret),usaf,mc...
TRANSCRIPT

Resident – Faculty Advisor & Mentorship Systems
Brian V. Reamy, MDColonel(ret),USAF,MC
Associate Dean for Faculty Professor of Family MedicineUniformed Services University

Introduction/Objectives
• Identify the different types of resident – faculty advisor & mentorship systems
• Explain the key developmental tasks of residents in training
• Identify positive and negative qualities in faculty advisors
• Describe the features of an “optimum” resident-faculty advisor system

Historical Context - 1982• Borus & Groves: “Training Supervision as a Separate Faculty
Role” Am J Psychiatry 1982;139(10):1339-42.

Historical Context
• “Training supervision is a longitudinal, nonclinically focused personal relationship between a faculty member and a resident for exploring the latter’s professional development. They … meet monthly over the 3-year residency.”
• “The training supervisor’s role is that of a non-evaluative senior colleague who orients and advises the resident and systematically reviews training progress and problems”

Who has a resident-faculty advisor system?
- How is it structured?- Who assigns residents?- Who makes changes when problems emerge?-Is it based on advising and evaluation or just advising?

Types of Advisor Systems
• Based on Clinical Care Teams• Self-selection • Proportional to faculty numbers
– Random assignment– Assigned by PG year group
• One faculty for each PG year group– Stay with year group thru residency program– Stay with their specific PG year group

Types: Clinical Care Teams
• Most common system• Example: 3 year PEDS Residency• 6-6-6 resident structure• 6 faculty + 1 PD + 1 Dept Chair
– Faculty physician + PG-3 + PG-2 + PG-1= care team– They cover each others patients during TDY’s/LV– This is also the academic advisor group

Types: Self-Selection
• Residents are told to select their advisor within 3 months of arrival– Can not select the PD– Rare in M.D. training– Common in Ph.D. programs

Types: Proportional
• If you have 24 residents and 8 faculty then each faculty member will get 3 advisees– Random/lottery or,– Each faculty takes one resident from each PGY or,– Assigned by PD based on research or clinical
interests, gender, request etc.

Types: Assigned to PG year groups
• Example: 3 year Internal Medicine Program• 8-8-8 resident complement; 16 faculty• One faculty (LTC Bezoar) has ALL PGY-1• One has ALL PGY-2…one has all PGY-3• 2 variations:
– LTC Bezoar stays with his year group x 3 years or,– LTC Bezoar is always the PG-1 faculty advisor
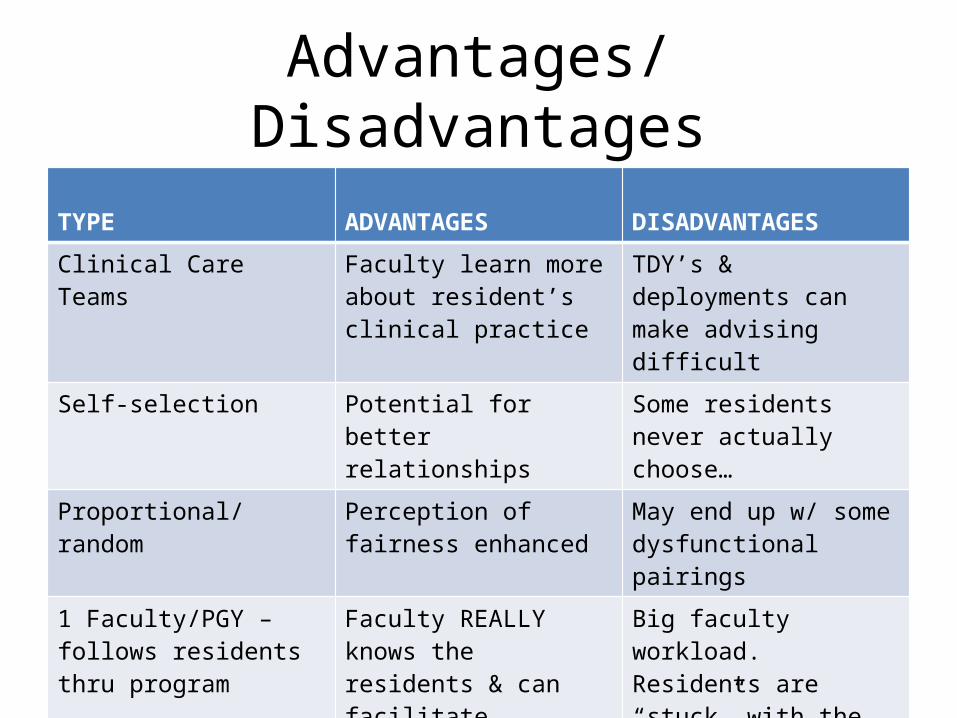
Advantages/Disadvantages TYPE ADVANTAGES DISADVANTAGES
Clinical Care Teams Faculty learn more about resident’s clinical practice
TDY’s & deployments can make advising difficult
Self-selection Potential for better relationships
Some residents never actually choose…
Proportional/random Perception of fairness enhanced
May end up w/ some dysfunctional pairings
1 Faculty/PGY – follows residents thru program
Faculty REALLY knows the residents & can facilitate improvements
Big faculty workload. Residents are “stuck” with the same faculty for length of training
1 Faculty/PGY - yr. specific The faculty REALLY knows the issues each specific year group faces and knows better how to problem-solve
Big faculty workload.

Key Issues w/each system
• Who does OER’s/OPR’s/FitReps?– Evaluation sabotages advising & mentoring!! It must exist –
but, separate from the advisor system.Many cites: Davis OC, Nakamura J. A proposed model for an optimal mentoring
environment for medical residents: a literature review. Acad Med. 2010;85:1060-1066
Sambunjak D et al. What makes a good mentor-mentee relationship? JCOM. 2010;17:152-154
• Distributing Faculty workload
• Who manages change requests?– Chief resident? Prog Dir?

Key Issues• Who gives out discipline?
– Should not be the advisor– Advisor should always wear a “white hat”– The Prog Director or Dept Chair should wear the
“black hat”

Key Developmental Tasks of Residents in Training
• Martin & O’Donnell. Resident Developmental Issues. Fam Med 1999;31:614-615.
• 10 Common Developmental Issues for Faculty advisors to facilitate

10 Developmental Issues ISSUE
1 Do not assume all residents progress at the same pace
2 Be available to residents to listen to and explore their concerns
3 Model a balanced life
4 Be willing to be vulnerable and share how you learned from your mistakes
5 Model flexibility in the face of chaos and model how you deal w/ uncertainty
6 Promote paced change and continuous growth
7 Give positive feedback
8 Help residents move towards independence & life after residency training ends
9 Be patient with growth and changes
10 Set boundaries

Advisor/Mentor Qualities
• We have all experienced good & bad faculty advisors and mentors?– You can get better at this!– Many of the skills are those that serve you well in
your clinical work with patients.
– Reference: Sambunjak D et al. A Systematic Review of Qualitative Research on the Meaning and Characteristics of Mentoring in Academic Medicine. J Gen Intern Med. 2009;25:72-78.

Positive Qualities in a Faculty Advisor? ?

Positive Qualities in a Faculty Advisor
Most Important (literature support) Other positive qualities
ADVOCATE Competent
MENTOR Sounding Board
PLANS IMPROVEMENT “Bitch & Moan Sponge”
DELIVERS HONEST FEEDBACK Nurturing
EXPERIENCED Reality Check
AVAILABLE Aware
APPROACHABLE Doer
INSIGHTFUL Fair
GOOD LISTENER Dedicated
PROMOTES RESPECT Resourceful
ROLE MODEL Social Director

Negative QualitiesQualities to Avoid
Social Director
Disciplinarian
Plays Favorites
Unavailable
Overextended
Inconsistent
Intimidating
Cynical & Jaded
Evaluator & Rater

Optimum System
• Six core interactional foundations
1) Emotional safety2) Responsiveness3) Support4) Protégé-centeredness5) Respect6) Informality

How would an optimum system appear?
• Evaluation is NOT confused with advising & mentoring
• Advisors who embrace the positive qualities• Equal distribution of faculty workload• Resident buy-in• Structure
– Fits w/ your institution & training environment– Thoughtfully selected

Optimum System
• Meeting Frequency & Guidelines– Informal “chats”: at least monthly– Formal faculty:advisee meetings every 3-4 mths– Need pre-planning ( initial vs. follow-up mtgs.)– Advisors need to get FULL faculty input– Avoid gossip sessions– Faculty need to keep records

Records
• Without records a faculty forgets or confuses• Confusion sabotages the faculty-advisee
relationship• Focus of the records is fourfold:
– Includes review of rotations & areas of concern– Includes faculty expectations & resident goals– Includes a Resident summative self-assessment– Ends with an Educational Rx

CONCERNS YES/NO
NOT REVIEWED
CONCERNS YES/NO
NOT REVIEWED
1 . Conference Attendance
9. In-Training Exam
2. Time Management 10. Licensing3. Relationships with Colleagues
1 1. Research Project
4. Family/Personal Adjustment
12. PME/Officership
5. Life Balance 13. TDY Interests6. Procedures 14. AHLTA/Coding7. Chart Reviews 15. Reading/Study
8. Core Competencies 16. Teaching/Supervision
RESIDENT ADVISEMENTROTATIONS:
(1)
(2)
(3)
(4)
AREAS OF CONSIDERATIONComments regarding above topics:
ADVISEMENT RECORD EXAMPLE
Name:Date:

Unsatisfactory Marqinal Below Effective and Verv Fine Exceptionally OutstandingAverage Competent Fine
Performance Lacks May continue Satisfactorily A continuing Performs Extremelyfails to meet motivation, in program, meets the level of high outstandingly rare,standards of interest, and but stated performance in most Excels inacceptance. performance performance objectives. in most aspects of everything.Rehabilitation is limited. is below aspects of job. Initiative, Performs faris doubtful. Cannot standards. stated leadership beyond level
continue objectives. and of training.without personalitysubstantial are worthy ofimprovement. special
notice.
FACULTY EXPECTATIONS RESIDENT GOALS ____________
RESIDENT SELF-EVALUATION:
Educational Rx:
Advisor & Resident Signatures

Potential Quicksand
• Social• Friendship• Being a Clinician for advisee • Acting as a disciplinarian• Not involving the PD• Not proactively making time for meetings

Take Home Points
• 5 primary structures of faculty-resident advisor systems exist and you should thoughtfully select one.
• Evaluation sabotages advising & mentoring!! It must exist – but, separate from the advisor system.
• All residents work through 10 major developmental tasks at their own individual pace.
• There are advisor qualities to emulate and those to avoid. You can improve your skills as an advisor.
• An optimum system can be designed and put in place

Thanks & Questions