resident update talk jtw online
TRANSCRIPT

Managing Curing Type 1 Diabetes
Jeremy Warshauer PGY-2
Internal Medicine
UT Southwestern
Objectives
bull Overview of type 1 diabetes
bull Bionic Pancreas
bull Islet Transplantation
bull Stem Cell Therapy
Prevalence
bull In 2012 291 million Americans or 93 of the population had diabetes
ndash 125 million American children and adults have type 1 diabetes
bull $245 billion in 2012 impact on economy
Normal Islet Cells
httpwwwbritannicacomEBcheckedtopic329670islets-of-Langerhans
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
bull Beta cell regeneration and transplantation
bull Immune research
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
Artificial or bionic pancreas
ldquoInsulin is not a cure for diabetes it is a treatment It enables the diabetic to burn sufficient carbohydrates so that proteins and fats may be added to the diet in sufficient quantities to provide energy for the economic burdens of liferdquo
ndash Sir Frederick Grant Bantingduring his Nobel lecture on September 15 1925
From JDRF
Bionic Pancreas
bull Addresses dysfunctional alpha cells and insulin deficiency
bull Embraces technology CGMS insulin and glucagon pumps
α-cell dysfunction
Diabetes Care Volume 37 May 2014
4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Objectives
bull Overview of type 1 diabetes
bull Bionic Pancreas
bull Islet Transplantation
bull Stem Cell Therapy
Prevalence
bull In 2012 291 million Americans or 93 of the population had diabetes
ndash 125 million American children and adults have type 1 diabetes
bull $245 billion in 2012 impact on economy
Normal Islet Cells
httpwwwbritannicacomEBcheckedtopic329670islets-of-Langerhans
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
bull Beta cell regeneration and transplantation
bull Immune research
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
Artificial or bionic pancreas
ldquoInsulin is not a cure for diabetes it is a treatment It enables the diabetic to burn sufficient carbohydrates so that proteins and fats may be added to the diet in sufficient quantities to provide energy for the economic burdens of liferdquo
ndash Sir Frederick Grant Bantingduring his Nobel lecture on September 15 1925
From JDRF
Bionic Pancreas
bull Addresses dysfunctional alpha cells and insulin deficiency
bull Embraces technology CGMS insulin and glucagon pumps
α-cell dysfunction
Diabetes Care Volume 37 May 2014
4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Prevalence
bull In 2012 291 million Americans or 93 of the population had diabetes
ndash 125 million American children and adults have type 1 diabetes
bull $245 billion in 2012 impact on economy
Normal Islet Cells
httpwwwbritannicacomEBcheckedtopic329670islets-of-Langerhans
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
bull Beta cell regeneration and transplantation
bull Immune research
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
Artificial or bionic pancreas
ldquoInsulin is not a cure for diabetes it is a treatment It enables the diabetic to burn sufficient carbohydrates so that proteins and fats may be added to the diet in sufficient quantities to provide energy for the economic burdens of liferdquo
ndash Sir Frederick Grant Bantingduring his Nobel lecture on September 15 1925
From JDRF
Bionic Pancreas
bull Addresses dysfunctional alpha cells and insulin deficiency
bull Embraces technology CGMS insulin and glucagon pumps
α-cell dysfunction
Diabetes Care Volume 37 May 2014
4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Normal Islet Cells
httpwwwbritannicacomEBcheckedtopic329670islets-of-Langerhans
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
bull Beta cell regeneration and transplantation
bull Immune research
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
Artificial or bionic pancreas
ldquoInsulin is not a cure for diabetes it is a treatment It enables the diabetic to burn sufficient carbohydrates so that proteins and fats may be added to the diet in sufficient quantities to provide energy for the economic burdens of liferdquo
ndash Sir Frederick Grant Bantingduring his Nobel lecture on September 15 1925
From JDRF
Bionic Pancreas
bull Addresses dysfunctional alpha cells and insulin deficiency
bull Embraces technology CGMS insulin and glucagon pumps
α-cell dysfunction
Diabetes Care Volume 37 May 2014
4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
bull Beta cell regeneration and transplantation
bull Immune research
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
Artificial or bionic pancreas
ldquoInsulin is not a cure for diabetes it is a treatment It enables the diabetic to burn sufficient carbohydrates so that proteins and fats may be added to the diet in sufficient quantities to provide energy for the economic burdens of liferdquo
ndash Sir Frederick Grant Bantingduring his Nobel lecture on September 15 1925
From JDRF
Bionic Pancreas
bull Addresses dysfunctional alpha cells and insulin deficiency
bull Embraces technology CGMS insulin and glucagon pumps
α-cell dysfunction
Diabetes Care Volume 37 May 2014
4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
bull Beta cell regeneration and transplantation
bull Immune research
T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
Artificial or bionic pancreas
ldquoInsulin is not a cure for diabetes it is a treatment It enables the diabetic to burn sufficient carbohydrates so that proteins and fats may be added to the diet in sufficient quantities to provide energy for the economic burdens of liferdquo
ndash Sir Frederick Grant Bantingduring his Nobel lecture on September 15 1925
From JDRF
Bionic Pancreas
bull Addresses dysfunctional alpha cells and insulin deficiency
bull Embraces technology CGMS insulin and glucagon pumps
α-cell dysfunction
Diabetes Care Volume 37 May 2014
4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

T1DM
α-cell dysfunction
autoimmune β-cell destruction insulin deficiency
Artificial or bionic pancreas
ldquoInsulin is not a cure for diabetes it is a treatment It enables the diabetic to burn sufficient carbohydrates so that proteins and fats may be added to the diet in sufficient quantities to provide energy for the economic burdens of liferdquo
ndash Sir Frederick Grant Bantingduring his Nobel lecture on September 15 1925
From JDRF
Bionic Pancreas
bull Addresses dysfunctional alpha cells and insulin deficiency
bull Embraces technology CGMS insulin and glucagon pumps
α-cell dysfunction
Diabetes Care Volume 37 May 2014
4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

ldquoInsulin is not a cure for diabetes it is a treatment It enables the diabetic to burn sufficient carbohydrates so that proteins and fats may be added to the diet in sufficient quantities to provide energy for the economic burdens of liferdquo
ndash Sir Frederick Grant Bantingduring his Nobel lecture on September 15 1925
From JDRF
Bionic Pancreas
bull Addresses dysfunctional alpha cells and insulin deficiency
bull Embraces technology CGMS insulin and glucagon pumps
α-cell dysfunction
Diabetes Care Volume 37 May 2014
4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

From JDRF
Bionic Pancreas
bull Addresses dysfunctional alpha cells and insulin deficiency
bull Embraces technology CGMS insulin and glucagon pumps
α-cell dysfunction
Diabetes Care Volume 37 May 2014
4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12
Bionic Pancreas
bull Addresses dysfunctional alpha cells and insulin deficiency
bull Embraces technology CGMS insulin and glucagon pumps
α-cell dysfunction
Diabetes Care Volume 37 May 2014
4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

α-cell dysfunction
Diabetes Care Volume 37 May 2014
4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

4-10x
Old way
Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Bionic Pancreas
288x
Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Bionic Pancreas Setup
Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Bionic Pancreas improved glucose control
How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

How much did the bionic pancreas help
bull Average blood glucose reduced
ndash 159 mgdL to 133 mgdL (A1C = 62)
bull Hypoglycemia reduced
ndash 37 to 15 of the time with a blood glucose lt60mgdL
How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

How much did they improve
Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Is this really a cure
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12
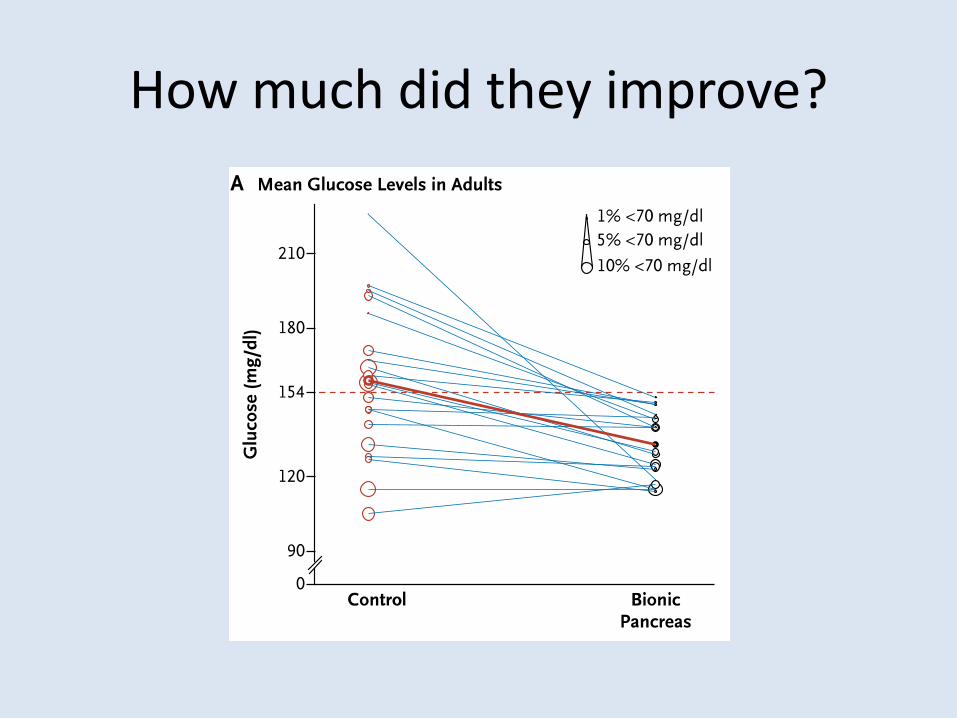
Problems with Bionic Pancreas
bull Invasive
bull Possibility of technology malfunction
bull No stable preparation of glucagon
bull Insulin time of onset
bull Not physiologic
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12
α-cell dysfunction
Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Underlying problem with insulin injections
Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Islet transplantation
Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Edmonton Protocol -immunosuppresion
bull Glucocorticoid-free immunosuppressive therapy
bull Daclizumab
bull Tacrolimus
bull Sirolimus
11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

11131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121111312111131211113121
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12
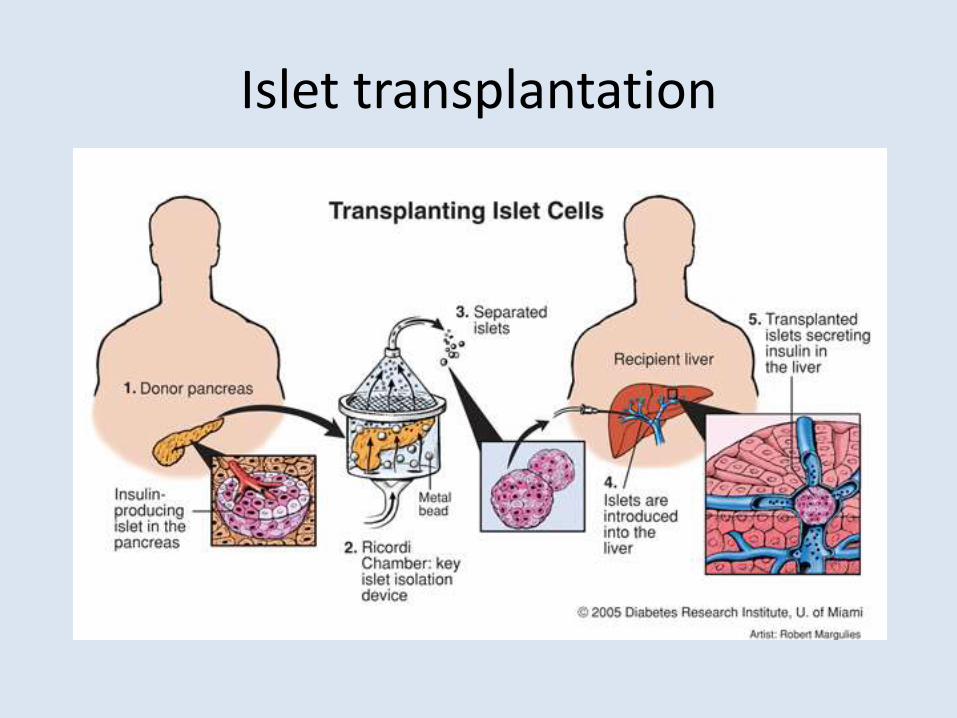
Edmonton Protocol ndash a long term solution
Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Why doesnrsquot everybody get this
bull Patient needs unstable glycemic control that cannot be corrected by standard conventional and intensive insulin therapies
bull Remaining challengesndash expansion of the islet donor supply
ndash improving islet isolation techniques
ndash strategies to improve engraftment
ndash mediating the anti-inflammatory response post-transplant
ndash improving recipient immunosuppression regimens
Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Prevelance
Diabetes Metabolic Syndrome and Obesity Targets and Therapy 20147 submit your manuscript | wwwdovepresscom
Dovepress
Dovepress
213
Islet transplantation for type 1 diabetes
from 2007ndash2010 as evidenced by retained C-peptide levels
reduction of HbA1c
and reduced islet reinfusion rates19 This
success in part can be attributed to shifts in immunosuppres-
sion strategies However improvements to islet engraftment
and subsequent survival are critical in achievement of durable
insulin-independence
Within North America few islet transplant centers are
currently active despite the substantial transplant activity
of international islet transplant centers This is reflected in
the classification of islet transplantation as an experimental
therapy in the United States resulting in a lack of available
funds to conduct and support large scale clinical trials
Currently two pivotal Phase III clinical trials are being con-
ducted in specialized islet transplantation centers through
the Clinical Islet Transplant (CIT) Consor tium (CIT-06 and
CIT-07 NCT00468117 and NCT00434811 respectively) in
an effort to support the US Food and Drug Administration
biological license application mandate Successful licensure
will inevitably recognize islet transplantation as a clinical
therapy expanding its therapeutic benefit for patients with
T1DM in the United States
The University of Albertarsquos Clinical Islet Transplant
Program continues to be the most active center participating
within the CITR In 2013 alone 66 islet transplants were
conducted at the Edmonton site The Edmonton group also
reports that of over 200 patients transplanted with more than
400 intraportal islet preparations 79 of recipients continue
to show full or partial islet graft function20 The median
duration of insulin independence is 346 and 11 months
for subjects with full or partial graft function respectively
whereas the duration of C-peptide is 533 and 704 months
respectively for those same patients20ndash22
Prior to the Edmonton Protocol insulin independence
was an uncommon achievement Though clinical success
has improved markedly over the past 14 years further
obstacles must be overcome if islet transplantation is to be
more broadly applied in the T1DM population Such remain-
ing challenges include expansion of the islet donor supply
improving islet isolation techniques strategies to improve
engraftment mediating the anti-inflammatory response
post-transplant and improving recipient immunosuppres-
sion regimens Several clinical trials are currently under
active investigation to address these obstacles in an attempt
to improve this important therapy (Table 1)
Clinical islet transplantation obstacles and refine me nt sDonor selection and availabilityThe number of pancreas donors required to treat one recipient
limits the number of transplants that can occur A component
of islet transplantation that may improve clinical outcomes is
donor selection Retrospective studies at single centers have
identified several donor-related variables that may contribute
to islet isolation outcomes These variables include donor
80
60
Edmonton
North America
International
40
20
Year
Islet transplant recipients per
year registered with CITR
Nu
mb
er
of
isle
t tr
an
sp
lan
t re
cip
ien
ts
0
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Figure 1 Number of islet transplant recipients from 1999ndash2013 in Edmonton North America and International Islet Transplant Centers
Notes This data is kindly reproduced with express permission from the CITR Coordinating Center and Investigators The Collaborative Islet Transplant Registry 2011
Seventh Annual Report Reported data is unavailable from 2010ndash2013 for North America and International Islet Transplant Centers15
Abbreviation CITR Collaborative Islet Transplant Registry
From the Clinical Islet Transplantation (CIT) Consortium
Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Stem cell Therapy
bull 2 Key features
ndash Ability to renew themselves through cell divisionwhile remaining undifferentiated
ndash When given the appropriate signals stem cells can differentiate into many specialized cell types
Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Encapsulation
bull Protect against immune rejection ndash Encaptradevice by Viacyte
httpviacytecomproductsvc-01-diabetes-therapy
Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

Conclusions
bull A cure is in site but there are several obstacles that still must be overcome
ndash Immune modulation
ndash Not enough supply
References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12

References
bull Bruni A et al (2014) Islet cell transplantation for the treatment of type 1 diabetes recent advances and future challenges Diabetes Metab Syndr Obes 7 211-223
bull Derr R et al (2003) Is HbA(1c) affected by glycemic instability Diabetes Care 26(10) 2728-2733
bull Kudva Y C et al (2014) Closed-loop artificial pancreas systems physiological input to enhance next-generation devices Diabetes Care 37(5) 1184-1190
bull Peyser T et al (2014) The artificial pancreas current status and future prospects in the management of diabetes Ann N Y Acad Sci 1311 102-123
bull Pagliuca F W et al (2014) Generation of functional human pancreatic beta cells in vitro Cell 159(2) 428-439
bull Russell S J et al (2014) Outpatient glycemic control with a bionic pancreas in type 1 diabetes N Engl J Med 371(4) 313-325
bull Shapiro A M et al (2006) International trial of the Edmonton protocol for islet transplantation N Engl J Med 355(13) 1318-1330
bull Unger R H and L Orci (2010) Paracrinology of islets and the paracrinopathy of diabetes ProcNatl Acad Sci U S A 107(37) 16009-16012
bull Unger R H and A D Cherrington (2012) Glucagonocentric restructuring of diabetes a pathophysiologic and therapeutic makeover J Clin Invest 122(1) 4-12