resources engage faculty/staff, students and parents as gatekeepers€¦ · ·...
TRANSCRIPT

PENN STATE ALTOONA
Suicide Prevention Gatekeeper Training: Integrating Educational Resources to Engage Faculty/Staff,
Students and Parents as Gatekeepers



Topics
Data Review
Gatekeepers
Health Services Providers
Faculty/staff and Student Web‐based products and
results
Parents study and results
Challenges

Penn State Altoona• Integrated care model
• Health services• Counseling Services• Disability Services• Health Promotion
• 4,000 undergraduates• 2/3 live on or around
the campus• SAMHSA grant- 2009-
2011

18% of undergraduates reported having seriously considered a suicide attempt at some point;
6% reported serious suicidal ideation in the past 12 months (Drum et al., 2009). Another study: Suicidal ideation among college students ranged from 32% to 70% (Gutierrez, Osman, Kopper, Barrios, & Sacks, 2000).
The majority of students who contemplate suicide do not seek professional help (Drum et al., 2009)
80% of students who die by suicide never received services at their campus counseling centers (Kisch, Leino, and Silverman, 2005).
.
Student Mental HealthAmong College Students…

Solitary binge drinkers are more than four times as likely to have made previous suicide attempts and experience depression (Gonzalez, 2012).
Healthy Minds Study (Altoona, n=860), 2010 64% of our students would first talk to their
parents if they were experiencing emotional distress
Of those who seek help, only 36% do so with parental encouragement
51% experienced academic difficulty due to MH symptoms in past 4 wks.

PARENT DATA

Literature Review
Parents are less comfortable talking about mental health than about other health concerns. (Locke & Eichorn, 2008)
There is still a high level of stigma around mental health. (Locke & Eichorn, 2008)
Most parents believe professional help is useful for mental health issues, but most would refer to a general practitioner first. (Jorm et al., 2007)

Literature Review Parents’ attitudes toward therapy influence help seeking,
engagement, retention, and outcome. They are based on perceptions related to benefits/risks. (Morrissey‐Kane & Prinz, 1999 &Vogel et al., 2009)
Parents are more willing to refer a friend’s child to professional help than their own. (Raviv et al. 2009)
50% of parents believe that a student can “pull themselves together” if they have an MH problem. (Locke & Eichorn, 2008)

Literature Review
Parents’ attitudes toward help seeking play a role in their students’ intentions to seek psychological help; also the quality of the relationship is significant as to if the student adopts the parental attitudes (Vogel,et al., 2009)
Jed Foundation, American Psychiatric Foundation, Academy for Educational
Development (2008)
N=1,007‐parents/guardians of 16‐20 yr. olds (38% parents of college students, 90% Caucasian)
One third thought that others would avoid their student if MI was discovered.
20% believed MH problems should be handled privately; parents are less comfortable discussing suicidal thoughts than other health topics.

JED continued
64.5% related that they had not received any information on MH services from their school, 9% didn’t know.
Most parents (53.9%) would refer to a family doctor, 26.1% counselor, 21.3% clergy
JED continued
80% are confident that they could identify a MH problem; although only 3.4% identified suicidal thoughts as a sign of depression, and only 15% were able to name more than one or two signs.
Almost 2/3 do not think their children are likely to experience a MH problem in college‐although they believe any person can develop a problem.
Limitations of Research
Limited replicated studies on mental health and the parent population in higher education.
Little is known about how parents want health information from their student’s university
Little data on the correlation between parental knowledge/ attitudes with intention to intervene and refer. Especially with cultural, geographic differences.

The Need
#1 action taken by universities to overcome the increasing number of at‐risk students is gate‐keeper training
Conducting face‐to‐face training for faculty/staff, parents and students is both expensive and difficult to administer.

Challenges1. Significantly depressed students are often unidentified on campuses, refuse
formal counseling, or drop out of treatment‐Less than 10% seek help at their counseling center; Almost 80% of students that commit suicide aren’t seen by a counselor
2. Accuracy of recognition of depression in primary care is low; and most present only with physical symptoms. (69% presented with physical symptoms; only 22% accurately diagnosed depression when symptoms were physical
3. Short term models, separation periods from care
4. Collaboration between Medical and Counseling systems
5. Tracking and monitoring of very high risk students is difficult; defining quality treatment and it’s impact on retention is a challenge.
Kisch, Leino & Silverman, 2005; American College Counseling Association’s 2007 National Survey of Counseling Center Directors; J. Gen Intern Med. 2008 Jan, 23(1):25‐36; Simon,GE, et al. N. Engl. J Med. 1999, 34(18): 1320‐1335; ,Stafford, R.S, J. Clin. Psych, 2000; Kirmayer LJ, et.al. Am J Psychiatry:1993,150(5):734‐741;

Best Practices‐ Public Health Approach
JeJedJIdentify Students at Risk‐Screen
Increase Help Seeking behavior
Provide MH and Crisis Services
Restrict Access to Potentially Lethal Means
Promote Development of Life Skills
Promote Social Engagement
Jed Foundation/SPRC

HEALTH SERVICES PROVIDERS AS GATEKEEPERS
US Preventive Services Task Force Recommendation: Patients should be screened in Primary Care for depression when “care supports” are in place. American College of Preventive Medicine states that primary care should have systems in place to ensure the accurate diagnosis and treatment of this condition.

Improving Depression Identification Early Detection: Maximize existing health and mental health
resources to identify and treat depression
WHY? –Under detection must be addressed aggressively. During a 1 yr. study (Young, 2001)‐ 83% with Dep/Anx. saw a PCP‐ < 30% received appropriate care.
Primary care physicians assess for suicide in patients with depression in only about 1/3 of visits
Young, A., et al. Arch Gen Psychiatry ;2001:58:55‐61
Institute for Clinical Systems Improvement (ICSI). Major depression in adults in primary care. Bloomington (MN): Institute for Clinical Systems Improvement (ICSI); May 2008. 84 p. [244 references]
Feldman MD, et. Al MedCare 2006:44 (12): 1107‐1113

Adoption of a Collaborative Care Model
Previous Model
Screening only through annual medical history form
If not in CAPS‐ no MH meds in Primary Care
Lack of guidelines for follow‐up
CAPS‐ limited use of objective monitoring tools
Evidence based approach
Screening at each visit in primary care
Treatment protocols based on objective measures
Collaborative care related to follow‐up and treatment‐MDT
Objective measures for monitoring outcomes
Self‐management and Case management

‐ improve individual outcomes by assisting in treatment planning; highlights the urgency for improved function in semester based schedules.
‐ group level outcomes can serve as benchmarksand goals that can be used as critical information to confirm or address effectiveness of service model changes.
‐ Creates a common language across disciplines and providers to promote effective integration
‐ Just like taking vitals
Why Measurement?

PHQ‐2
During the past two weeks, have you been bothered by:
Little interest or pleasure in doing things? □No □Yes
Feeling down, depressed or hopeless? □No □Yes
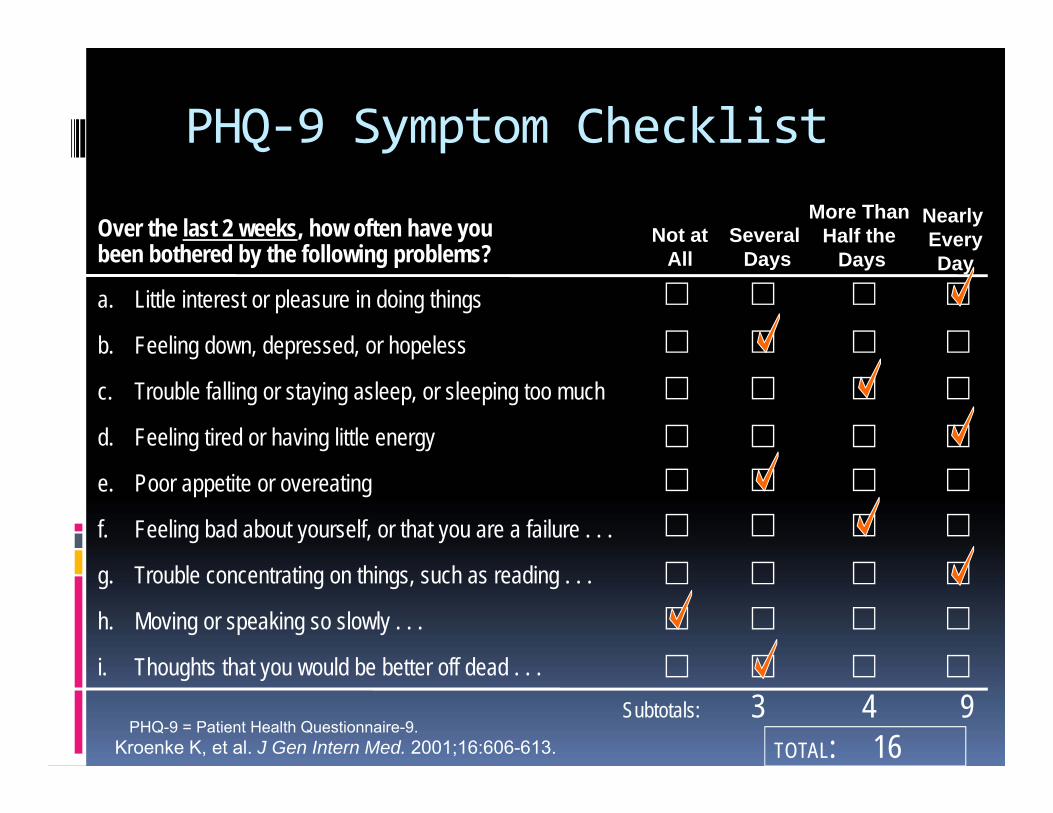
TOTAL: 16
PHQ‐9 Symptom Checklist
Kroenke K, et al. J Gen Intern Med. 2001;16:606-613.
a. Little interest or pleasure in doing things
b. Feeling down, depressed, or hopeless
c. Trouble falling or staying asleep, or sleeping too much
d. Feeling tired or having little energy
e. Poor appetite or overeating
f. Feeling bad about yourself, or that you are a failure . . .
g. Trouble concentrating on things, such as reading . . .
h. Moving or speaking so slowly . . .
i. Thoughts that you would be better off dead . . .
Over the last 2 weeks, how often have you been bothered by the following problems?
Subtotals: 3 4 9
Not at All
Several Days
More ThanHalf the
Days
Nearly EveryDay
PHQ-9 = Patient Health Questionnaire-9.

Delivery System Redesign
Link depression screening to vision, mission, and goals of primary care
Integrate depression screening into QI program Make the depression screening a standing
agenda item at treatment team meetings Ensure senior leaders actively support
improvement effort by removing barriers and support with incremental incentives/resources (TIME)

Delivery System Re‐design‐ Implement ACTIVE Follow‐up of Patients
Primary Care: PHQ‐9, baseline and at 4,8,12 wks; Use Lucas Functional
assessment at baseline and once between 8‐12 weeks Self‐management plan
Counseling: Celeste Health for screening Use PHQ‐9 for assessment and follow‐up of patients Use Lucas Functional assessment at baseline and at
follow‐up (8 ‐ 12 weeks) Self–management plan/tx. plan

Outcomes 2011‐2012
333 students screened positive for depression in primary care (9%)
Referrals to CAPS increased 10%, visits increased 38%
Development of Triage, Bio‐feedback program and Case management services

STUDENT TRAINING

At-Risk Gatekeeper Training
• 30-minute, online
• Includes simulated conversation with at-risk student avatars
• Utilized to train all freshmen, RA-s, high risk groups

1. Recognize common signs of psychological distress
2. Manage a conversation with an at-risk student and how to effectively motivate them to seek help & refer them to the counseling center
3. Avoid common pitfalls such as attempting to diagnose the problem or giving unwarranted advice during the conversation
4. Know what to do if the friend refuses to seek help or you feel uncomfortable to engage in the conversation
5. Learn about own college specific counseling center and referral process
Learning Objectives
.

Users assume the role of a student named Jesse, who has four friends. He’s worried that one of his friends is struggling, and it’s the
learner’s job to figure out who.
Step 1: Introduction

Learner first observes student’s behavior over a semester in several social events such as a Thanksgiving dinner at the Dining Hall
© 2010 Kognito Interactive. All Rights Reserved.
Step 2: Examine Student Behaviors

1. Alcohol/Substance Abuse 2. Bipolar Disorder 3. Depression 4. Eating Disorders
5. Panic Disorder 6. Post Traumatic Stress Disorder 7. Social Phobia
Symptoms exhibited by the student avatars correlate to the most common and most severe psychological illnesses among young adults:
© 2010 Kognito Interactive. All Rights Reserved.
Step 2: Examine Student Behaviors

Step 3: Talk to StudentsUsers engage in conversations with the student avatars.
Practice and learn to use open-ended questions, reflective listening and other motivational interviewingtechniques to effectively:
1. Broach the topic of psychological distress
2. Motivate the student to seek help
3. Avoid common pitfallssuch as attempting to diagnose the problem or giving unwarranted advice

The learner controls the conversation by choosing what topic to bring up and what specific things to say. Learners receive instant feedback through the student’s verbal responses and body language …
Step 3: Talk to Students

… as well as encouragement and constructive criticism on their decisions from a virtual coach. Critical errors lead to immediate
corrective feedback as well as the opportunity to undo and correct their decision
Step 3: Talk to Students

Once the learner successfully refers the student avatar to counseling, the training is complete and the learner is given a few helpful links to more
information such as what to do if the friend refuses to go to the counseling center.
Step 4: Conclusion

PENN STATE ALTOONA STUDENTSRESULTS AT‐RISK
2011‐2012

Results at Penn State Altoona ‐ Students
© 2012 Kognito Interactive. All Rights Reserved.
Demographic data is collected following the course in a post‐survey.(n=260)

© 2012 Kognito Interactive. All Rights Reserved.
Following the At‐Risk training, students rated significantly higher their preparedness to:
P<0.01
Results at Penn State Altoona ‐ Students

© 2012 Kognito Interactive. All Rights Reserved.
1. Skills and Behavioral Intention (cont.):
Results at Penn State Altoona ‐ Students
Users reported significantly higher levels of confidence in their ability to help a suicidal student

© 2012 Kognito Interactive. All Rights Reserved.
2. Learning Experience:
Results at Penn State Altoona ‐ Students
67.3% of users rated the course as Very Good or Excellent. An additional 28.1% rated the course as Good (n=260).
81.5% of users would recommend the training to a friend (n=260)

© 2012 Kognito Interactive. All Rights Reserved.
2. Learning Experience (cont.):
Results at Penn State Altoona ‐ Students
88.8% of users reported that engaging in simulated conversation with at‐risk students was helpful in preparing them for similar conversations in real life (n=260)

© 2012 Kognito Interactive. All Rights Reserved.
3. Adoption of Training School‐Wide:
87.3% of students agree that all students at their school should take this course (n=260).
Results at Penn State Altoona ‐ Students

FACULTY/STAFF TRAINING

AT RISK‐ Faculty/staff
Faculty/Staff Product: In Prof. Hampton’s class, there are six students he’s concerned about.

Three are “at risk.” Users must approach them & refer them to the
Counseling Center. The others are not “at risk.”
They can be approached. (optional for completing the simulation) During conversation, users should realize their problems are not psychological. Users can refer them or implement other solutions (e.g., setting boundaries and
expectations for future behavior).

PENN STATE ALTOONA FACULTY/STAFF RESULTS

© 2012 Kognito Interactive. All Rights Reserved.
1. Skills and Behavioral Intention‐ Following the training, users rated significantly higher their preparedness to::
P<0.01
Results at Penn State Altoona ‐ Faculty

© 2012 Kognito Interactive. All Rights Reserved.
Users reported significantly higher levels of confidence in their ability to help a suicidal student
Confidence to help a Suicidal Student
Results at Penn State Altoona ‐ Faculty

© 2012 Kognito Interactive. All Rights Reserved.
95.5% of users reported that engaging in simulated conversation with at‐risk students was helpful in preparing them for similar conversations in real life (n=22)
2. Learning Experience (cont.):
Results at Penn State Altoona ‐ Faculty

© 2012 Kognito Interactive. All Rights Reserved.
2. Learning Experience:
63.6% of users rated the course as Very Good or Excellent. An additional 34.4% rated the course as Good (n=22).
100% of users would recommend the training to a colleague (n=22)
Results at Penn State Altoona ‐ Faculty

© 2012 Kognito Interactive. All Rights Reserved.
3. Adoption of Training School‐Wide:‐ 95.5% agree that all faculty/staff at their school should take this course.
Results at Penn State Altoona ‐ Faculty
PARENTS AS GATEKEEPERS

Barriers To Help‐Seeking Healthy Minds Study (n=860, 2010)
50% believe that most people think less of those with MH problems
54% believe that most people see tx. as a sign of weakness
51% believe that stress is normal
45% do not perceive the need
37% believe that problems will resolve themselves
Hypothesis: Some of the same barriers to help‐seeking identified with students will relate to parents as well.
Parents hold great influence

Research Questions
What factors correlate with increased referral to
counseling?
What is most
related to tendency to
refer?
What most impacts willingness/comfort in talking with students
about issues?
Is parent’s willingness
to talk about mental health
concerns a mediator?

Belief of helpfulness of
therapy
Beliefs about mental health and Services
Beliefs about suicide and signs of depression
Knowledge of mental health
issues
Confidence in abilities to know how to seek help

Study Design
Conduct a random sampling of parents from two distinctly different schools
Look at geographic, ethnic and cultural differences‐ A rural small liberal arts school‐ 4,000 An urban multi‐culturally diverse school‐ 15,000

Study Design
Sample size 300 $10 incentive‐ gift card, metro card Phone surveyors Structured training Statistical analysis – Descriptive statistics using linear regression, correlation and multivariate analysis

Potential Outcomes
An understanding of the educational needs of parents Perceived risks and benefits to intervening Knowledge base regarding symptoms and referral options
Development of products which seek to decrease barriers to help‐seeking

Demographics
75% of respondents were mothers
64.7% of respondents were ages 45‐54
59% of respondents were White;20% Black/African American;21% Hispanic
27% of respondents live in rural areas;43% urban, 28% suburban

Communication Preferences (Somewhat to very interested)
Parent Web‐site (75%) Parent Newsletter‐mailed (79%) Parent Newsletter‐ emailed (69%) Parent Training during orientation (79%) Video or CD accessed on‐line or mailed (50%)

Demographics
Income: 25% 100,000 or more, 29% 50,000 to less than 100,000, 15.5% less than 20,000
Education: 27.7% some college, 10% technical school, 33.7% college
25% were not born in US

Communicating With Students

Frequency of Communication

Understanding Mental Health
Parents report ‐Top three signs of depression Withdrawn‐18.5% Change in weight‐17.9% Sleeping‐ too much‐14% Thoughts of suicide‐ 3.8%‐second to the last (drop in grades‐2.9%)

Potential Barriers (Somewhat agree/agree)
Services may not be confidential‐ 40% Records might impact future plans‐ 40.3% Providers may not be sensitive to cultural issues‐ 36.4%; Religious beliefs‐ 28%
Lack of knowledge about services‐ 28.4% Prefer to handle things within the family‐29.7%

Beliefs Barriers‐ Beliefs (somewhat agree/agree)
I would think less of a person who has received MH TX‐ 93.6%
Receiving TX. Is a sign of personal failure‐98.3%
People with MH problems just need to “pull themselves together”‐ 89.3%
MH disorders are not real illnesses‐ 93.6% Seen in a less favorable way‐ 61.3%

Referral
Family Doctor or Health Center‐ (3.7) Counseling (3.3) Talk to family/friends (3.2) Clergy (3.02) Web‐site (2.9)

What Impacts Likelihood of Referral
Significant impact: Awareness of crisis hotline Perceived helpfulness of therapy Not thinking less of a person who has received treatment; and recognizing stigma
Disagreeing that people with MH problems just need to pull themselves together.
Higher income, higher educated, having a male student

More Frequent Communication
Is Positively Related to:
Referral to the Campus Counseling Center Asking the student to call the Crisis Center Talking to their student about drugs, alcohol, eating disorders and suicidal ideation

Higher Frequencies of Communicating In Person are significantly POSITIVELY
Related to:
Comfort in talking about suicide. Belief that their student will disclose if having a mental health problem
Likelihood of referring to a family doctor or Health Service
The belief that they can talk them out of it

Understanding of mental health Only 47.3% of parents are sure they would
know how to help their student for depression.
Only 44% of parents are sure they would know how to help their student for other mental health issues.
Over 50% of parents believe they know the signs of depression, substance abuse, anxiety, suicide. (cutting)
Less than 50% believe they know the signs related to eating disorders, bipolar disorder, cutting behaviors, schizophrenia

Willingness to intervene 38.3% reported their student would likely tell them about a mental health issue; and 22% believe the college would inform them.
19% of respondents were not aware of at least one resource on campus.
27.7% were not aware of at least one crisis hotline.
Less than half (44%) are sure that they would know when to seek help
75% would refer to primary care provider‐(mean‐3.7)

Parent DVD Contracted with a professional educational media company. info@academic‐channel.com
Created the content‐themes Distributed the DVD to all parents fall 2011 Completed a web‐based evaluation spring 2012

Parent DVD Objectives
Identify warning signs Learn how to approach/talk to your student Refer, seek services of a professional Themes: Asking about suicide doesn’t plant the seed Treatment is effective It is your responsibility to be aware as a parent Psychological issues can happen to anyone

Parent DVD Follow‐up Survey
78 Parents responded to the survey via an email invitation sent on the parent listserv.
The survey was open for three weeks and two reminder emails were sent.

Results 86% of parents reported watching the DVD. 99% of the parents had freshman students. 83% of the parents that responded were female.
97% of parents rated the DVD as good, very good, or excellent.
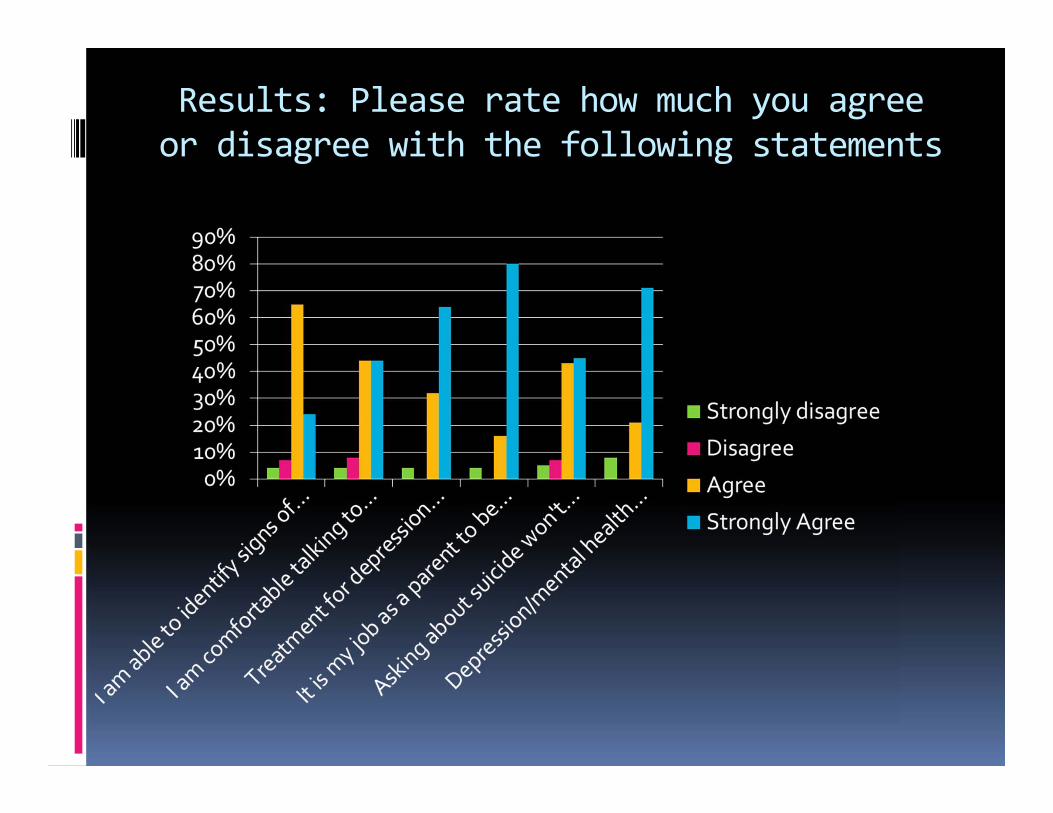
Results: Please rate how much you agree or disagree with the following statements

Results
89% able to identify signs of suicide/distress 88% comfortable talking to my student 88% believe tx. for depression is valuable 92% believe MH issues can affect anyone 88% believe that asking about suicide will not give their student the idea
96% believe that it’s their job to know what’s going on with their student

Additional Parent Strategies
Parent Web‐site www.altoona.psu.edu/stress
Parent newsletters each semester‐mailed to the home and on‐line
New Student Orientation, parent session
Parent List‐serve messages

Parent Webpage

Parent Newsletter

Parent Newsletter

Challenges
Comprehensive System for Early InterventionHit all the Gatekeepers
Access to care‐ seamless Resources for increased volume
Parents Access‐ tap in to web‐sites, processes that are in place (orientation)
“Just in time” information Funding, man‐power

Challenges
Faculty/staff (n=158; 67% staff, 33% faculty) Administrative‐ top down approach (funding) Frequent messages and invitations Combining the invitation with current issues or events
Incentives
Student buy‐in First year student mandate Clubs, Athletes and Greek Cost

Questions