respite task force report to… · this report provides an overview of respite programs in the...
TRANSCRIPT
Respite Task ForceReport


3
Respite Task Force ReportTable of Contents1 Acknowlegements
3 Preface
5 Executive Summary
8 Introduction
10 ConcernsIdentifiedThroughtheRespiteTaskForce
13 RecommendationstoImproveAccesstoRespiteandSupportFamilyCaregivers
13 Programmatic Suggestions
15 Administrative Suggestions
15 Summary
Appendix NebraskaLifespanRespiteNetworkBrochurewithStateMapofRegions
ThisprojectissupportedinpartbytheNebraskaPlanningCouncilonDevelopmentalDisabilitiesandthefederalAdministrationonIntellectualandDevelopmentalDisabilitiesfundsawardedtotheUniversityofNebraskaMedicalCenter’sMunroe-MeyerInstitutebytheNebraskaDepartmentofHealthandHumanServices.

4
ThisprojectwasledbyJanetL.Miller,MS,respite/adultservicesassociatewiththeUNMCMunroe-MeyerInstitute(MMI).Ms.Millerpreviouslyservedastheprogramcoordinatorfor“Respite Across the Lifespan,” projectatMMIandoneofthesixregionalrespitenetworksofthestatewideNebraskaLifespanRespiteNetwork.Shehasworkedinthedisabilityfieldformorethan35years.
Forquestions,[email protected].

1
TheRespiteTaskForceisaworkgroupmadeupoffamilycaregivers,stateandcommunitynonprofitagencies,andcoordinatorsfromtheNebraskaLifespanRespiteNetwork.ThisgroupwasformedinOctober2017inresponsetoagrantawardedtotheUniversityofNebraskaMedicalCenter’sMunroe-MeyerInstitute(MMI)bytheNebraskaPlanningCouncilonDevelopmentalDisabilities.AlsoprovidingfeedbackweremembersoftheNebraskaSystemofCaregroup,facultyandstaffattheMMIUniversityCenterforExcellenceinDevelopmentalDisabilities(UCEDD),andtheUniversityofNebraska-LincolnCenteronChildren,FamiliesandtheLaw.Referencealsoismadetothe“NebraskaLifespanRespiteNetwork:ProducingPositiveOutcomesforFamilies2015-2017EvaluationFinalReport”.ThisrespiteevaluationwasconductedbyJoleneJohnson,Ed.D.ofMMI,madepossiblewithfederalfundingawardedbytheNebraskaDepartmentofHealthandHumanServicesLifespanRespiteProgram.
Partners on the Respite Task ForceNebraskaDepartmentofHealthandHumanServices(DHHS)Representatives:• DivisionofChildrenandFamilyServices• DivisionofDevelopmentalDisabilities• DivisionofMedicaidandLongTermCare• SixlocalLifespanRespiteNetworks
NebraskaCaregiverCoalition
AgingPartners,Lincoln
NebraskaTotalCare
Parentsandotherfamilycaregivers
NebraskaFamilyCollaborative(nowPromiseShip)
BrainInjuryAllianceofNebraska
SpecialEducationPara-Educator,BigSprings,Nebraska
UNMCMunroe-MeyerInstitute,UniversityCenterforExcellenceinDevelopmentalDisabilities
WewishtoacknowledgethemanyfamilycaregiversacrossthestatewhorespondedtoaneedssurveylookingatgapsandbarrierstoaccessingrespitecareservicesinNebraska.
ThisreportprovidesanoverviewofrespiteprogramsinthestateandaddressestheidentifiedgapsandbarrierstotheutilizationofrespitecareservicesinNebraska.MembersoftheRespiteTaskForce(hereafterreferredtoasRTF)generatedrecommendationstoaddresstheseissues.
Acknowledgements

2

3
ThefollowingnarrativewaswrittenbyMandySullivanandMaryAnnCarson,amotheranddaughterwhoservedontheRespiteTaskForce.Thesetwofamilycaregiverspaintapictureofthesupportaffordedtofamilycaregiversinourstateandthenegativeoutcomesthatoccurwhensupportisnotprovided.
Carry Another Person’s Burden for a Few Steps, and You Can See for Miles
Carryinganotherperson’sburdenistheverydefinitionofrespite.Yet,howdoyougoaboutit?Howdoyousustainit?Thesearethequestionsposedbythosewhocontrolthefateofthisquintessentialprogram.Theansweris,youinvestinyourpeople,yourNebraskans.IfyouarefromNebraska,chancesareyouhaveheardindividualsfromotherstatessay,“Nebraskansarejustsodowntoearth.Whyisthat?”BecauseweNebraskansworkwiththeearth.WeworkwithMotherNature,andwehavelearnedthatwhenweworkagainsther,weloseeverytime.ThesameholdstrueforourNebraskafamilycaregivers.Ifthepoliciesandlawsworkagainstourcaregivers,wewillallloseeverytime.
Wewanttogrowourstate.WewanttheyoungtoreturntoNebraskaandcarrythelegacyoftheirparents.Theproblemis,thefamilyfarmhasbeensold.GrandpaandGrandmaoutlivedtheirmoney.MomandDadhadtoselltheirretirementinvestment,thefamilyfarm,topayforthe
$7,000-per-monthnursinghomebill.Therewasnotenoughhelporassistancetokeepthemhome.Nowthekidsandgrandkidshavenothingtoreturnto.
ThesameholdstrueforourNebraskafamilieswithachildwhohasadisability.Quiteoften,oneparentwillneedtostepawayfromtheircareerpathtocarefortheirchild’sspecialneeds,usuallycripplinganalreadystrainedhouseholdbudget.Forfamiliesintheagriculturalsector,thisequatestoequipment,livestockorlandsales.
Nebraskansareproudpeople.Theywanttocarefortheirown.Neithersnownorrainnorheatnorgloomofnightdetersthesecaregiversofthelandandlivestockfromcompletionoftheirduties.Neitherlackoffundingnorunfavorablegovernmentalpoliciesnorself-needdeterthesecaregiversfromthecompletionoftheirdutiesfortheirlovedones.
Preface

4
Thetruthis,without“respite”thefamilycaregiverworkshimorherselfintotheground.Theyignoretheirownhealthneeds.Theyignoretheirownfinanciallimits.Theyignoretheirownsocialandemotionalneeds.TheyfindthemselvesabandoningtheirroutinereligiouspracticesbecauseGrandpagetstoodisruptiveduringtheservice.Theirmarriagesarestrainedbecausealltheirenergyisdevotedtotheirspecialneedschild,leavingthememotionlessfortheirspouse.Weeklyinvitationsforcoffeestopcomingbecausetheycanceledonetoomanytimes.Themostdevastatingoutcomeis,theyforgettoputontheirownlifevest,cancelingamammogrambecausetheirhusbandfellagainthismorning.
We’renotaskingformillionsofdollars.We’renotaskingfortractsofrealestatewithbrickandmortarfacilitiestofundandmaintain.We’reaskingyoutoinvestinyourpeople.Thepeopleyousofaithfullyserve–theNebraskacaregivers.Theverypeoplewhobelievedenoughinyoutogetthejobdoneright.Pleasebelieveinthemsotheycancontinuetodotheirjobright.
“Carryanotherperson’sburdenforafewsteps,andyoucanseeformiles.Lightenanotherperson’sloadandtogetheryoucancompletethejourney.”

5
AccordingtoJillKagan,DirectoroftheAccesstoRespiteCareandHelp(ARCH)NationalRespiteNetworkandResourceCenter,1Nebraskahistoricallyhasbeenheldasanationalmodelforrespiteprogramming(2017).SuccessoftheNebraskaLifespanSubsidyProgram2becamethemodelforCongresstopasstheNationalLifespanRespiteCareProgramof2006,whichhasbeenreauthorizedannually.
Researchshowsthatfamilycaregiverscontinuallyfaceincreasedlevelsofdepression,stress,riskforheartdisease,andotherhealthconditions.3 Researchalsodemonstratesthatprovidingfamilycaregiversaccesstorespitedecreasescaregiverandcarerecipientstress(JoleneJohnson,2017),lowerssiblingstrain,4improvesmaritalquality,5 anddecreaseslong-termcareexpendituresby
1 https://archrespite.org2 http://dhhs.ne.gov/Pages/hcs_services_respite.aspx3 https://www.caregiver.org/caregiver-health4 https://www.canchild.ca/en/resources/206-respite-services-a-critical-review-of-the-literature5 https://link.springer.com/article/10.1007/s10803-013-1812-06 ImpactofRespiteCareServicesforFamiliesWithChildrenExperiencingEmotionalandBehavioralProblems.Children’s
Services: Social Policy, Research, and Practice, 3(1), 39-61).7 https://www.aarp.org/home-family/caregiving/info-08-2013/the-aging-of-the-baby-boom-and-the-growing-care-gap-AARP-
ppi-ltc.html
keepingindividualsintheirhomesratherthaninlong-termcarefacilities.6Asourpopulationages,theneedtoidentifystrategiestobettersupportfamilycaregiverswillbeparamountasthecaregiversupportratiodeclinesfrom1:7in2010to1:3by2050.7Thismeansthatforeverypersoninneedoflong-termcareservicesandsupports(LTSS)in2050,thereonlywillbethreefamilycaregiverswhowillbeavailabletoprovidethissupport.
TheEasternRegionoftheNebraskaLifespanRespiteNetwork,housedatMMI,wasawardedagrantfromtheNebraskaPlanningCouncilonDevelopmentalDisabilitiesinOctober2017totacklethepressingissuesaroundrespiteinNebraska.TheRespiteTaskForce(RTF)wasgatheredinNovember2017,comprisedofanarrayofstakeholdersfromacrossthestate,toactively
Executive Summary
Respite:Plannedoremergencycareprovidedtoachildoradultwithspecialneedsinordertoprovidetemporaryrelieftofamilycaregiverswhoarecaringforthatchildoradult.
Lifespan Respite Care Act definition (PL 109-442)

6
collaborateinaddressingtheneedsoffamilycaregiversinNebraska.TheRTFmetmonthly,offeringface-to-facemeetingsaswellasreachingonlinestakeholdersfromacrossthestatethroughonlinetechnology.
ItwastheaimoftheRTFtodevelopaframeworktostrengthen,support,andexpandtheNebraskaLifespanRespiteNetworkandtoadvancethecapacitytodeliverrespitecareservicestofamilycaregiversinourstate.
BasedonsurveyresultsandRTFdiscussions,thisreportidentifiesgapsandbarriersinaccessingrespiteservicesaswellasrecommendationsonhowtoaddress
thesepressingissues.MembersoftheRTFworkedtoaddressrecommendations/strategiesatthesystemslevel,programmaticlevelandconsumerleveltostrengthenandimprovetheutilizationofrespiteservicesinallprograms.SpecialconsiderationwasgiventotheNebraskaLifespanRespiteSubsidyProgramwithintheDHHSDivisionofChildrenandFamilyServices,asitprovideswiderprogrameligibilityandflexibilityduetonotbeinggovernedbyMedicaidrules.
State and National Respite Programs
The Nebraska Lifespan Respite NetworkbeganwithagroupofindividualscomingtogetheratastatewideconferenceinAugust1997.Inthespringof1998,arequestforproposalswasissuedbyNebraskaDHHStoconveneastatewideinitiativetopromoterespite,developpermanentfunding,promotethedevelopmentoftrainingofprovidersandfamilies,andestablishacentralizedinformationandreferralsourceforservices.In1999,LB148wasintroducedbystateSenatorDennisByars.Thebillwaspassed,establishingtheNebraskaLifespanRespiteServicesPrograminstatestatute(Neb.Rev.Stat.§68-1520through1528).Itconsistsofthefollowing:
1. TheLifespanRespiteNetworkwasdesignatedtocoordinatecommunityrespiteservices;and
2. TheLifespanRespiteSubsidyProgramwasdesignatedtoprovidefundingforcaregiverstopurchaserespiteservices.
TheNebraskaLifespanRespiteSubsidyProgramiscentralizedandadministeredthroughNebraskaDHHSandsupportedwithstatefundingfromtheNebraskaCashSettlementTobaccoFund.TheLifespanRespiteNetworkbecameoperationalin2000.Thestatewasdividedintosixareas,contractswereawarded,andcoordinatorswerehiredforeacharea.Amapandlocalcontactinformationisincludedintheappendixofthisreport.
In1999,LifespanRespiteSubsidyProgramfundingwasmadeavailablewiththeratesetat$125permonthtooffsetthecostsofsecuringrespiteservicesforfamilies(Title464NAC1-4).Thelegislatureannuallyallocates$404,464foradministrativesupportand$810,000forservicestosupporttheNebraskaLifespanRespiteSubsidyProgram.Themonthlysubsidyamounthasnotbeenincreasedsincetheprogramstartin1999.
CAREGIVER SUPPORT RATIO
2010
YEAR In Need of LTSS Number of Family Caregivers
2050

7
Thereareadditionalsourcesofrespitefundingavailableforfamilycaregivers.However,theamountsoffundingforrespiteservicesisoftenlimitedinscopeandrequiresstringenteligibilitycriteriawithnotwoprogramshavingthesamerequirements.Someofthesegovernment-fundedsourcesincludethefollowing:
• TheAged&DisabledMedicaidWaiver(Aged,AdultsandChildren)
• TheDevelopmentDisabilitiesWaiver
• AdultandChildProtectiveServices,FosterCare,SubsidizedAdoptions
• TitleIIIOlderAmericansAct
• U.S.AirForceExceptionalFamilyMemberProgramandVeteransCaregiverSupport.
Theneedtoenhancethesupportsprovidedtofamilycaregiversisgainingnationalattention.AbipartisanbillcalledtheRecognize,Assist,Include,SupportandEngage(RAISE)FamilyCaregiversAct8waspassedbyCongressandsignedintolawbyPresidentDonaldTrumpin2018.TheActcreatesanadvisorycouncilchargedwithmakingrecommendationstosupportfamilycaregivers.9
8 https://www.aarp.org/politics-society/advocacy/info-2017/senate-passes-family-caregivers-act-fd.html9 https://www.aarp.org/politics-society/advocacy/info-2018/senate-family-caregivers-act.html10 https://arch.wildapricot.org/resources/Documents/2016_Natl_Respite_Conf/PPTs/C-4%20J.%20Johnson%20Nebraska%20Eval.pdf
TheRTFdeterminedthatashortstatewiderespiteneedssurveytobuildupontheresultsofthepreviousrespiteevaluationauthoredbyUNMC/MMIin2015-201710wouldbebeneficial.Asurveywasdevelopedanddisseminatedacrossthestatethroughthesixlocalnetworks,onFacebook,anddistributedtoconstituentsofRTFmembers,throughagencynewsletters,andmore.Approximately250surveyresponseswerereceivedwithmanypeoplesharingstoriesabouttheirrespiteexperiencesandneeds.AdditionalinsightsweresharedbyRTFmembersdrawingfromtheirownpersonalexperienceswithrespiteandissuessharedbytheirfriendsandcolleagues.SimilarneedswereidentifiedbetweentheRTFsurveyandthe2015-2017evaluationconductedbyUNMC/MMI.
Theneedtosupportfamilycaregiverswillbecomeamorepressingissueasouragingpopulationrequiresmorelong-termservicesandsupports.Manystatesarestartingtoprovidemoreservicestobettersupporttheneedsoffamilycaregiverstoreduceordelaytheneedfor24/7servicesineffortstoreduceMedicaidexpenditures.
Nebraska Lifespan Respite Services Program Mission (Neb.Rev.Stat.68-1520through1528)
A service designed to give family caregivers a break from the demands of providing ongoing care for an individual with special needs.
Atermunfamiliartomany,respiteishelpforthehelpers.TheNebraskaLifespanRespiteNetworkprovidesinformationandreferral,providerandcaregivertraining,andresourcedevelopmentforrespiteservices.Theavailabilityandusageofrespiteenablesfamilycaregiverstimeforthemselvestorefreshandrejuvenate,thusimprovingtheirphysicalandemotionalhealth.
8
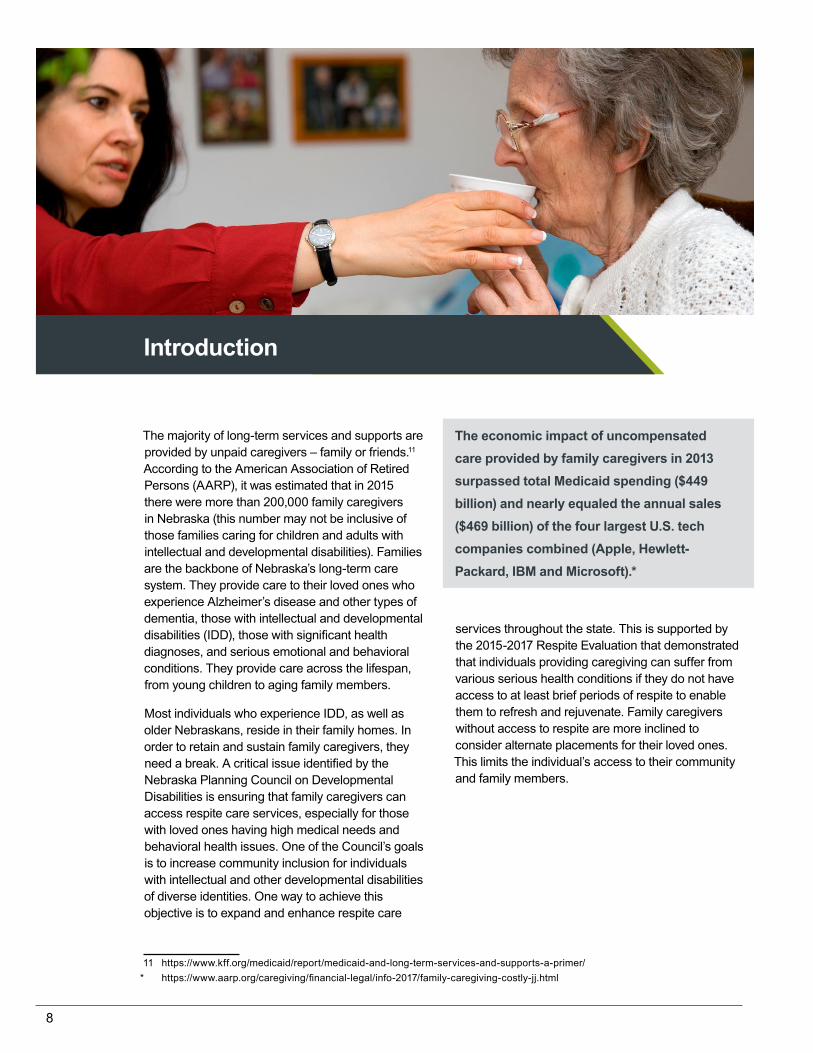
Themajorityoflong-termservicesandsupportsareprovidedbyunpaidcaregivers–familyorfriends.11 AccordingtotheAmericanAssociationofRetiredPersons(AARP),itwasestimatedthatin2015thereweremorethan200,000familycaregiversinNebraska(thisnumbermaynotbeinclusiveofthosefamiliescaringforchildrenandadultswithintellectualanddevelopmentaldisabilities).FamiliesarethebackboneofNebraska’slong-termcaresystem.TheyprovidecaretotheirlovedoneswhoexperienceAlzheimer’sdiseaseandothertypesofdementia,thosewithintellectualanddevelopmentaldisabilities(IDD),thosewithsignificanthealthdiagnoses,andseriousemotionalandbehavioralconditions.Theyprovidecareacrossthelifespan,fromyoungchildrentoagingfamilymembers.
MostindividualswhoexperienceIDD,aswellasolderNebraskans,resideintheirfamilyhomes.Inordertoretainandsustainfamilycaregivers,theyneedabreak.AcriticalissueidentifiedbytheNebraskaPlanningCouncilonDevelopmentalDisabilitiesisensuringthatfamilycaregiverscanaccessrespitecareservices,especiallyforthosewithlovedoneshavinghighmedicalneedsandbehavioralhealthissues.OneoftheCouncil’sgoalsis to increase community inclusion for individuals withintellectualandotherdevelopmentaldisabilitiesofdiverseidentities.Onewaytoachievethisobjectiveistoexpandandenhancerespitecare
11 https://www.kff.org/medicaid/report/medicaid-and-long-term-services-and-supports-a-primer/* https://www.aarp.org/caregiving/financial-legal/info-2017/family-caregiving-costly-jj.html
servicesthroughoutthestate.Thisissupportedbythe2015-2017RespiteEvaluationthatdemonstratedthatindividualsprovidingcaregivingcansufferfromvariousserioushealthconditionsiftheydonothaveaccesstoatleastbriefperiodsofrespitetoenablethemtorefreshandrejuvenate.Familycaregiverswithoutaccesstorespitearemoreinclinedtoconsideralternateplacementsfortheirlovedones.Thislimitstheindividual’saccesstotheircommunityandfamilymembers.
Introduction
The economic impact of uncompensated care provided by family caregivers in 2013 surpassed total Medicaid spending ($449 billion) and nearly equaled the annual sales ($469 billion) of the four largest U.S. tech companies combined (Apple, Hewlett-Packard, IBM and Microsoft).*

9

10
The process to access respite funding and usage is perceived as “too confusing and bureaucratic.”
Quote from surveyed family member
1.THEPROCESSTOACCESSRESPITEFUNDINGISCONFUSING.
Eachprogramthatprovidesrespitehasspecificrulesandrequirementspertainingtorespiteeligibility,usage,anddeterminationofaccesstorespitefunding.
• TheNebraskaLifespanRespiteSubsidyProgramissupportedwithstategeneralfundsandhasrequirementsforeligibilityandestablishedrequirementsforproviders.
• StateMedicaidWaiverPrograms(Aged&DisabledWaiverandDevelopmentalDisabilityWaivers)havetheirowneligibilityrespiterequirementsanddifferentrequirementsforproviders.
• TheNebraskaLifespanRespiteProgramstatuterequiresthattheLifespanNetwork(consistingofthe6regionalcoordinatorsacrossthestate)coordinateallcommunityrespiteprograms;however,inpractice,theLifespanRespiteSubsidyistheprimaryprogramsupportedbytheNebraskaRespiteNetwork.
EffortsareneededtosimplifytheNebraskaLifespanRespiteSubsidyeligibilityprocessforfamiliesandaligntherequirementsofrespiteprovidersacrossallprograms.
2.NEBRASKALIFESPANRESPITESUBSIDYAPPLICATIONANDELIGIBILITYPROCESS.
TheprocesstodetermineeligibilityfortheNebraskaLifespanRespiteSubsidyhasstringentfinancialguidelinesasreferencedinTitle464NAC1-4.12EffortstosimplifytheLifespanRespiteSubsidyapplicationprocesshavebeenattempted,butfamiliesstillindicatethattheapplicationprocessislongandcumbersome.Manyfamilieshavesharedthattheapplicationprocessisnotworththetimethatittakestoprovideallofthenecessarydocumentsandtocompletethepaperwork.Othersindicatethattheallocationof$125permonthdoesnotcovertheexpensesnecessarytoproviderespitecare.Oursurveyshowed,andtheNebraskaRespiteNetworkServicescoordinatorscorroborate,thatmany
12 http://dhhs.ne.gov/Documents/Title-464-Complete.pdf
familieswhoaredetermined“overincome”foreligibilityarestillstrugglingfinancially.Thisisparticularlytrueforfarmersandrancherswhoare“landrichbutmoneypoor.”Often,whenfamiliesareaskedtosubmitbankstatementsinordertodetermineeligibilityforthesubsidy,manyalreadyfeeltheywillbedeniedanddonotcontinuetheprocessbecausetheirfinancialsituationisverydifferentonpaperthaninactuality.
Recently,theNebraskaLifespanRespiteSubsidyProgramhasimplementedtwoinitiativesthatareworkingtohelpmeetfamilyneeds:theabilityforfamilieseligibleforthesubsidytobanktheirmonthlyallocationtouseforspecialrespiteactivities,andthecreationofanenhancementtofundingforfamilieswhohaveexceptionalneedsorcircumstance.Whilefamiliesmaybeeligibleforanadditional$1,000forExceptional Need/Circumstances,theycannotreceivethisfundinguntiltheyhavebeenapprovedfortheinitialLifespanRespiteSubsidyfunding,aprocesswhichcantakeanaverageofamonthormore.
Unfortunately,thiskeepsthosewhoareincrisisfromaccessingrespite.Manyfamilycaregiversareinfight-or-flightmodeandoftenhitapointwhereacrisisconditionisimmediatebut,becauseofthewayNebraska’sprogramsaresetup,theycannotaccessanyrespitesupportswithoutalreadybeingeligibleforaprogram.
Anotherconcernthatfamilieswhoaresubsidy-eligiblehaveisthepotentialtolosetheirprogrameligibilityiftheyarenotconsistentlyusingtheprogrammonthly.Familieswhodon’tbillfor60ormoredaysarecontactedbyaRespiteCoordinatorandofferedassistancewithlocatingproviders,instructedonbilling,givensuggestionsonhowtouseauthorizedrespitefunds,etc.Familiesareadvisedthatiftheydon’tbill,itindicatesalackofrespiteneed,andtheyriskhavingtherespitecaseclosed.Programstaffregularlyoffertobankunusedmonthstopreventfamiliesfromlosingrespitefunds.Unfortunately,this policy does not allow the family flexibility to self-direct respite services and denies families the ability to use respite supports when they need it.Forexample,afamilyfightingtheflubugreportedthattheydidnotwantanyrespiteproviderstocometotheirhomeforfearoftransmittingthevirus.Thefollowingmonth,therespiteproviderfellill.WithouttheRespiteCoordinatorsteppinginandsuggestingthatthefamilybankthesetwo
Concerns Identified Through the Respite Report

11
months,basedonthecurrentprogram,thefamilywouldlikelyhavelosttheireligibilityforthisprogram.
3.PAYMENTPROCESSESANDBARRIERSLEADTOSLOWPAYMENTS.
SeveralrespiteprovidershaveindicatedthatNebraskaDHHSdoesnotpayinatimelymanner,creatingadditionalbarriersforproviders.However,muchoftheissueseemstobethatprovidersaresubmittingbillingdocumentswitherrors,includingnotkeepingaddressesupdated,havingincorrectdates,orchangingbankinginformationwhileapaymentisprocessing.Whenanerroroccurs,it’slikelythatDHHSwillrequestthatthefamily/providersubmitsanewbillingdocument.
Paymentprocessesvarybyprogrambutdosharetheissueofclaimsprocessinggoingthroughseveralstepsanddepartmentsbeforeapaymentcanbegenerated.NebraskaMedicaidiscurrentlyexploringelectronicoptionstomeetthe21stCenturyCuresAct.13HavingtheRespiteSubsidyProgramconsiderthismayreducepaymentprocessingtimesinthefuture.
Funding provided to family caregivers for respite services is perceived as “woefully inadequate.”
Quote from surveyed family member
4.INCREASETHENEBRASKARESPITELIFESPANWhiletheLifespanRespiteSubsidyprovideseligiblefamilieswithupto$125permonthforrespiteservices,familiescansupplementtheproviderpaymentandareabletodictateornegotiatetheratewiththerespiteprovider.However,thisfundingamountfallsveryshortforfamilieswhoprovidecareforindividualswithhighmedicalorbehavioralhealthneeds.Inadequatesubsidyfundingforcostlyspecializedin-homeorin-facilityrespitecareimpactsfamiliesandrespiteproviders.
13 The 21st Century Cures Act, signed December 13, 2016 by President Barack Obama, promotes and funds the acceleration of research into preventing and curing serious illnesses; accelerates drug and medical device development; attempts to address the opioid abuse crisis; and tries to improve mental health service delivery. The Act includes a number of provisions that push for greater interoperability, adoption of Electronic Health Records Systems (EHRS), and support for human services programs.
Whenfamiliesmustpay$25-$40perhourinordertoobtaintheservicesofaskilledprovider,thisallowsonlythreetofivehourspermonthofrespite,makingitdifficultforfamilycaregiverstoobtainasufficientamountoftimetotrulytakeabreakfromtheongoingresponsibilitiesofprovidingcare.Duetothelimitedamountoffundingprovidedbythesubsidy,manyfamiliesfinditdifficulttorecruitprovidersneededtomeetthehighercareneedsoftheirlovedoneorretainproviderswithwhomtheyhavedevelopedrelationships.
5.THEREAREGAPSINSUPPORTINGINDIVIDUALSWITHHIGHMEDICALNEEDSORWHOEXPERIENCEHIGHBEHAVIORALHEALTHNEEDSINBOTHHOMEANDAGENCYSETTINGS.
Familieswhoaresupportinganindividualwhomeetsanursinghome-level-ofcare,maybeeligibleforoneofthestate’sMedicaidWaiverPrograms.Sometimestheseprogramsmayprovidemorefundingforrespite.However,evenwiththisincreasedfunding,manyfamiliesindicatetheycannotfindproperlytrainedproviders.
“Respite money is not enough to pay for a caregiver with the skills necessary to meet my daughter’s needs: suctioning, tracheotomy care, low body temps, oxygen needs, feeding pumps, g-tube feeds and medications, lifting, transferring, positioning and so much more. My husband and I have not been
“My child was highly volatile, and we were unable to find someone qualified to provide respite for him for the money allotted by the respite program. Our child would have needed much more time to develop a relationship with the care provider and feel safe with them... When you have the fulltime care required of a child with serious mental illness, locating a cheap but qualified provider in the community is really burdensome and acts as a serious deterrent to families using the Nebraska system.”
Quote from surveyed family member
The Nebraska Respite Subsidy was established in 1999 and established the allocation of $125/month to family caregivers. This rate has not been increased since the program started – almost 20 years ago.
Quote from an RTF Stakeholder

12
out, alone, for over 5 years. Not having respite not only affects the caregiver, it affects marriages and families.”
Quote from surveyed respondent
Thissentimentwasreflectedacrossthestateasfamilycaregiverswhoneedrespiteservicesthemostarefrequentlythosewhocannotfindoraffordthecostsassociatedwithpayingforhigherskilledworkers,suchasbehaviorspecialistsornursingstaff.Onefamilywrotethatthehusbandhadtoquithisjobinordertostayhomeandcarefortheirsonbecausetheywereunabletofindadequatecare.Anothermentionedtheyhadtomakethedecisiontomovetheirchildintoaninstitutionalfacilitybecausethestressofcaringfortheirchildwithnoback-upsupportwastoogreatfortheirfamily.
ThereisalsoaneedtoidentifywaystobettersupportIndependentproviders.Independentprovidersfacetheirownchallengesastheyassumetheriskofprovidingservices.UnderNebraska’scurrentsystem,incaseofinjurybythecarerecipientorintheeventanaccidentwouldoccur,thefamilyandcareproviderwouldhavetonegotiatethecostanddecidewhowillbeliable.Thisriskisfrequentlycitedasonereasonrespiteproviderswillnotprovidecareforthosewhohavehighercareneeds.Theseindividualprovidersareconsideredself-employedandmostlikelylackbenefitssuchasworkers’compensation,payfortheirownhealthcareinsurance,andfrequentlycannotaffordtonothavefundstoaddresstheseadditionalcosts.Theyarealsoresponsibleforpayingforalltheirincometaxeswhichalsocutsdeeplyintothelimitedhourlypaytheyreceive.
In order to keep families together and defer institutional placements, the state likely needs to invest in additional training for respite provider and other direct care staff.
6.MORESPECIALIZEDTRAININGFORRESPITEPROVIDERSISNEEDED
Thelackoftrainingforindividualrespitecareprovidersand,conversely,thecorrespondingpayincreasetypicallyidentifiedwithproviderswhohavereceivedcontinuingeducationarefrequentlycitedasbarrierstoaccessingqualifiedrespiteproviders.
14 http://dhhs.ne.gov/behavioral_health/SOC/Pages/Home.aspx
WhiletheNebraskaLifespanRespiteNetworkrequiresageneralonlineorientationfornetwork-screenedrespiteproviders,thisorientationonlycoversbasicinformationaboutprovidingrespitecare.Itdoes notaddressthespecializedskillsnecessarytoworkwithindividualswhohaveintellectualanddevelopmentaldisabilities,significantbehavioralhealthorhighmedicalneeds,includingAlzheimer’sdisease,stroke,ortraumaticbraininjuries.Additionally,thistrainingisnotrequiredacrossotherrespiteprogramsnoristhereanyconsistenttrainingrequirementacrossallstaterespiteprograms.There is a need to offer uniform training that leads to higher wages or a career-path which improves the quality of care and helps to sustain the current workforce.
TheNebraskaBehavioralHealthSystemofCare14partnersdiscussedthatevenwhentheyhaveindividualsskilledincaringforpersonswithmoresignificantbehavioralneeds,theyareoftenunabletogetthemtobecomerespiteproviders.Withoutasystematicapproachtotrainandretainbothindependentandagency-basedproviders,thestate’s3%unemploymentratemeansthatmanypeoplewhocouldberespiteprovidersrealizethattheycanmakemorebyworkingatfastfoodrestaurantsorlocalbusinessesandbeeligibleforpayraises,collegereimbursement,andbenefitspackages.
7.CAPACITYBUILDINGNEEDSFindingchildcarewasanotherconcernexpressedbysurveyrespondents.Familycaregiversstatethatthebarrierstoidentifyingchildcareproviderswilling/abletotaketheirchildwithspecialneedsdeterstheirabilitytoremainemployedandsupporttheirfamilies.Forexample,twodaycareprogramsinOmahaoriginallyestablishedtocareforthosewithmedicaland/orbehavioralneedshavestoppedservingchildrenwhohavemoreextensivebehavioralneeds.Oneofthetwoisfocusingonlyonchildrenwithmoresignificantmedicalneeds.
Respite coordinators frequently field calls by frantic parents/guardians looking for childcare for children with high needs. While childcare is not considered respite, obtaining more specialized childcare is a barrier for family caregivers and one that the state Respite Coordinators are frequently asked to meet.
LTC Stakeholder
“It takes a certain level of knowledge and experience to care for a special needs child with autism."
Family member quote

13
“Honestly,thereneedstobefacilitiesacrossthestateforindividualswithseverebehavioralneedssowell-trainedstaffcanprovidetheshort-termbreaksthatfamiliesneed.WehavenothinglikethisinwesternNebraska.”
LTC sStakeholder
Barriersalsoexistforyoungadultswithdisabilitieswho,becauseoftheirage,areconsideredtoooldtobeindaycaresettingsbutstillneedsupport.Forexample,youngadultsontheautismspectrumtypicallyneedadditionalsupportsduringthesummermonthsandoverschoolbreaks.
Somefamiliesofchildrenoradultswithsignificantbehaviorsexpressinterestinhavingplacesoutsideofthehomewheretheirlovedonecanreceivecareonashort-termbasis.Manyfamilieswhohavechildren/adultswithco-occurringconditions(e.g.,mentalhealthanddevelopmentaldisabilities)havealsoexpressedtheneedforhavingmoreofabreakthanjustafewhoursofrespite.Theyareneedingadayorevenaweekendtobeabletotakecareoftheirwholefamilywithoutconstantlydevotingtheirundividedattentiontotheindividualwiththe
co-occurringcondition.ThisisacriticalissueacrossthestateofNebraskaasthereareverylimitednumbersofagenciesorindividualswhoaretrainedandwillingtoprovidecareforthoseindividualswithhighmedicalorbehavioralhealthneeds.
There is a need in Nebraska for places providing emergency or crisis respite care for those situations where the family is in a crisisortheindividualhappenstobeinabehavioralconditionthatmakesitunsafeforthemselvesortheirfamily.Frequently,respitecoordinatorsreceive incoming calls from stressed family caregivers looking foremergencyfacilitieswheretheycantaketheirlovedone.Currently,therearenotsufficientprogramsthatsupportfamiliesincrisis.Iftheyexist,thereareadditionalbarriersforthosewithbothdevelopmentaldisabilitiesandmentalhealthissues.These calls exceed the current services available within Nebraska’s Respite programs.Inthesesituations,theRespiteCoordinatorofferssupportandassistswithreferralstotheNebraskaFamilyHelpline,mentalhealthprovidersorlawenforcement,ifnecessary.
Recommendations to Improve Access to Respite and Suport Family Caregivers
ManyofthefollowingrecommendationsarespecificallytargetedtotheNebraskaLifespanRespiteNetworkandSubsidyprograms.However,thereareseveralrecommendationsthatapplytoallprogramsthatproviderespiteservicestosupportfamilycaregivers.TheRTFbelievesthathavingthestateprogramsworktogethertobettersupportfamilycaregiverswillleadtobetteroutcomesforboththecarerecipientandcareprovider.ThiswilllikelyalsoreduceMedicaidexpendituresbysupportingthefamiliesandkeepingthemintheircaregivingroleandtheindividualswhoneedlong-termcareoutsideofcostlyinstitutionalcare.
Programmatic Suggestions
1. Increase the Lifespan Respite Network Subsidy rate. TheNebraskaLifespanRespiteSubsidyprogramshouldbeincreasedfromthe$125monthlysubsidythatwasestablishedwhentheprogramwascreated.Theincreaseshouldaccountforthecostoflivingincreasesthathaveoccurredinthepasttwentyyearsandshouldalsoestablisharequiredcostoflivingincreaseforfutureyearssotheprogramwillremaincompetitiveandviable.Additionally,therespitesubsidyshouldprovideahigheramountoffundingtothosefamilieswhoareproviding
careforindividualswhohavehighercareneeds.AssessmentsadministeredbytheNebraskaDivisionofDevelopmentalDisabilitiescouldbereferencedasonewaytodeterminethelevelofcareanindividualneedsandcorrespondingfundingallocatedtomeettheindividual’sneeds.
2. Pilot the use of Medicaid Support Waivers. In an efforttokeepindividualsinlesscostlyhome-andcommunity-basedsettings,andtodecreasethewaiting

14
listsforhome–andcommunity-basedservices,statesarestartingtoimplementMedicaidSupportWaivers.Thesewaiversprovidealimitedbudgettofamiliesandbudgetpredictabilityforstates.Familiesareallocatedasetbudgetwhichcanbeself-directedandutilizedtopayforrespite,transportation,andspecializedchildcareasexamples.StatessuchasTennessee,Pennsylvania,andMassachusettsareimplementingthesewaiverswithanannualbudgetrangestartingat$12,000.15 16 17Thiswouldalsoremovetheissueofnotutilizingservicesinauniformbasisfrommonthtomonthorhavetheprograminterruptedwithoutinterventionbythecaseworker.
ItisrecommendedthattheDivisionofChildren&FamilyServicesandNebraskaLifespanRespiteNetwork,togetherwiththeDivisionofMedicaidandLongTermCare,plantosubmitforaMedicaidSupportWaiver.Initially,theNebraskaLifespanRespiteSubsidystatefunds(TobaccoCashSettlementFunds)couldbeusedtopilotalimitednumberoffamilysupportwaiverslotstodemonstrateimpact.ThiswouldallowdatatobecollectedinordertobuildthebusinesscasetoexpandtheprogramthroughaMedicaidmatch.
Family Support Waivers could:• Provideahigherannualbudgettoenable
familiestopayprovidersahigherrate,thusbettercompensatingproviderswhohaveobtainedspecializedtrainingtosupportindividualswithhighmedicalandbehavioralhealthneeds.
• Helpretaineffectiveproviderswhohavedevelopedrelationshipswiththefamilyandcarerecipient.
• HelpremediatemanyconcernsarticulatedbyNebraskastakeholdersbyallowingfamiliestodirecttheirbudgettoprovidefortheservicestheyneed.
• ExpandstatefundingwithMedicaidmatchtobothenhanceandmaximizethesupportavailableforfamilycaregivers.
TheNebraskaLifespanRespiteNetworkcouldcoordinatethisnewprogram.ThisprogramshiftalignswiththeoriginallegislativeintentoftheNebraskaLifespanRespiteNetworkandSubsidyProgram,andalsoalignswiththenetwork’scurrentsustainabilityplan.Medicaidmatchcouldbeutilizedforrespiteservicecostsandcouldbeusedtosupporttheadministrativecostsassociatedwiththerespitecoordinatorsalaries,
15 TennesseeCommunityFirstChoice:https://www.tn.gov/content/dam/tn/tenncare/documents/introductionToEcfChoices.pdf16 MarylandFamilySupportsWaiverFrequentlyAskedQuestions:https://dda.health.maryland.gov/Documents/Family%20Supports%20Waiver%20
FAQs%207-10-17%20Final.pdf17 PennsylvanioaPerson/FamilyDirectedSupportWaiver:http://www.dhs.pa.gov/learnaboutdhs/waiverinformation/personfamilydirectedsupportwaiver/
index.htm
whichcreatesbothenhancedfundingandprogramsustainability.
3. Provide a higher reimbursement for providers who must drive long distances to provide care. In manylocations,respiteprovidersmustdrivesignificantdistancesinordertoofferin-homerespitecareservices.Thisistrueinrural,urban,andwesterngeographicareas.Drivingtoaperson’shomeencompassesboththeprovider’stimeandmoney.Thecostofgasandupkeepontheirvehiclesareexpensesthatcurrentlyarenotreimbursed.WhiletheNebraskaLifespanRespiteSubsidyProgramwillallowfamiliestopayahigherratetooffsettheseexpenses,thiscutsintothefamilies’fundingtoaccessrespite.Thelackofreimbursementcandeterindividualprovidersfromwantingtotravellongdistancestoprovidein-homerespitecare.DHHSshouldconsiderallocatingahigherreimbursementforfamilieslivinginruralcommunitiesorforproviderswhomustdriveoverasetnumberofmiles(20milesormore).
4. Identify strategies to eliminate the risk to families and providers. Familiesconsistentlyindicatethattheycannotfindproviderswhoarewillingtoprovidesupportforthosewithhighmedicalandbehavioralhealthneeds.Arootcauseforthisistheself-directedconsultantmodelthatNebraskausesfortheNebraskaLifespanRespiteProgram.Underthismodel,theriskofprovidingcareforanindividualwithhighneedsissharedbyboththefamilyandtheprovider.Unfortunately,inatimewheneventhebestofintentionscanresultinalawsuit,manyindependentprovidersfeeltheycannotaffordtotakeontheriskofprovidingcareforsomeonewithhighneeds.Mostindependentprovidersdonothavethefundstopurchaseliabilityorworkers’compensationinsurance,orevenhaveadequatehealthinsurancetopayforanunintendedinjurytothemselvesortheircarerecipient.However,thereareoptionsthatwouldlikelyremovethesebarriers.
A. Set up agreements with agencies in each local network to provide respite.DHHScouldcontractwithdevelopmentaldisabilityagencies,childcareprovidersorassistedlivingfacilities,payingthemadailyrateforfamiliesdeemedeligiblefortheLifespanRespiteSubsidyProgram.Asuggestionwouldbetoallocatetwodayspermonthofrespitecareinanagencysetting.Agencieshaveliabilityinsuranceand

15
typicallyoffermedicalandworkers’compensationinsurancetotheirstaff,sothemajorityoftheriskisshoulderedbytheprovidingagency.Thiswouldgivefamilieswhoareprovidingcareforanindividualwithhigherneedstheopportunitytohaveabreakwhiletheirlovedoneissupportedinasettingthatcouldaccommodatetheirneeds.
B. Adopt a fiscal intermediary agency model. As partofthestate’slong-termcareredesign,apriorityrecommendationistoutilizeafiscalintermediaryagencytomanageindependentproviders.18ThereportbytheNationalAssociationofStatesUnitedforAgingandDisabilities(NASUAD)explainsthatthiswillhelpindividualshireandtraintheirownprovidersbutnothavetheresponsibilityfor
18 http://dhhs.ne.gov/medicaid/Documents/Nebraska-Long-Term-Care-Redesign-Plan.pdf19 http://dhhs.ne.gov/medicaid/Documents/Long%20Term%20Care%20Redesign%20Plan%20-%20Draft%20by%20Mercer%20Health%20Benefits,%20
Inc%20v2.pdf(seepages28-29)
payrollortaxwithholding,norpurchaseworkers’compensationandliabilityinsurance.TheuseofafiscalintermediaryminimizestherisksthatNebraska’scurrentmodelplacesonboththerespiteproviderandthefamily.DHHScouldsubcontractthisroleouttoacommunity-basedorganizationorissueacompetitiveRequestforProposalsforanorganizationtoassumetheroletomanageallindependentrespiteprovidersacrossallNebraskaprograms.TheRespiteNetworkcoordinatorscouldserveasthebrokerageservice,detailedintheNASUADreport,whichwouldbeneededtoprovidethesupportsforindividualsandfamiliestolocateandtrainrespiteprovidersforthosewhochoosetoparticipate.19
Administrative Suggestions
1. Investigate a change in policy when considering a family’s assets in determining financial eligibility for the Lifespan Respite Subsidy. Farmers,ranchers,andothersmayappeartohavesignificantassetsonpaperbutactuallyhaveverylimited“liquid”assetsavailabletopayforthecostofrespitecare.WhiletheRTFbelievesthattheincomeguidelinesforeligibilityareprettylenient,itwasfeltthatadjustmentsshouldbeconsideredforthosewhoseassetsareattachedtolandandequipmentandretirementaccountsthatarenotreadilyconvertedintocash.
Note: Program currently disregards irrevocable burial funds, educational savings accounts while child is school-age, retirement savings for working-age adult, and IDEA savings.
2. Improve the current billing system requirements for providers to receive payment for providing respite services. FamiliesandtheirrespiteprovidersmustsubmitDHHSbillingdocumentsmonthly.BothfamiliesandprovidershaveexpressedconcernandfrustrationinhavingtocompletemonthlybillingdocumentsintheirentiretywhentheDepartmentalreadyhasmostoftheinformationonfile.WhileDHHShasamulti-stepreviewandapprovalbillingprocess,thereisaneedtoimproveefficienciesandstreamlinethisprocess.Paymentdelaysoccurwhenstafffindbillingdocumentswhichhavenotbeencompleted,resultingintheprovidernotgettingpaidfortherespiteservicestheyprovidedthepreviousmonth.Improvementsneedtobemadetoboth
billingrequirementsandreimbursementprocesses.TheNebraskaLifespanRespiteNetworkhaslostrespiteprovidersduetotheslowpaymentprocess.
3. Streamline the application process for those individuals seeking to become respite providers. Currently,theNebraskaLifespanRespiteNetworkisworkingtodevelopanonlineapplicationprocessforthoseapplyingtobecomeindependentrespiteprovidersthroughtherespitewebsite(www.nrrs.ne.gov).ThiswillexpeditethescreeningprocessforthoseinterestedinbecomingarespiteproviderfortheNebraskaLifespanRespiteNetwork.However,becausetherearedifferentrequirementsforrespiteprovidersacrossprograms,familiesarenotabletodrawfromonesinglepoolofrespiteproviders.Instead,anyonewhoisanindependentprovidermustgothroughaseparateprocessforeachprogramtobereimbursed.Thisprocessisconfusingformanyprovidersandlimitstheproviderpool.Tohelpstreamlineandsimplifythisprocess,encouragingthesamerequirementsacrossallprogramsmaybebeneficial.AnotheroptionmightincludehavingtheRespiteNetwork-screenedprovidersgothroughthesameprocessrequiredbyMedicaid-fundedprograms.
4. Address the lack of understanding of how respite is defined and where to go to access services. Whilemanyindividualswhorespondedtooursurveyappearedtoknowaboutrespite,wealsolearnedthatsomefamiliesarenotawareofwhatrespiteactuallymeans.TheRTF

16
reviewedtheexistingNetworkbrochureanddeterminedmoreclarificationwasneeded.Anewrespitebrochurewasdrafted,reviewedbytheRTF,andfinalizedbyDHHSgraphicdesignersandapproved.AcopyofthenewlydesignedbrochureisincludedinthisreportintheAppendix.Additionaloutreachwillbeneededtohelpfamilycaregiversunderstandtheimportanceofrespiteandhowtheycanaccessthisvaluableprogram.
TherearemanyactionableactivitiesthatcanbeimmediatelyadoptedbytheNebraskaLifespanRespiteNetworkandotherDHHSprogramstobettersupportfamilycaregivers.Asprogramshaveshiftedfrominstitutionalplacementstosupporthome-andcommunity-basedsystems,theincreasedcaregivingdemandsplacedonfamilycaregivershavenotbeenadequatelyaddressed.Theadverseimpactsofprovidingcontinualcarebyfamilieswhoarealsoworkingisbecomingasignificantpublichealthissue.Asourpopulationagesandthecorrespondingdemandsoffamilycaregiversincrease,itisimperativeforstatestoidentifywaystoenhancethesupportsprovidedtofamilycaregiversnow.Researchconsistentlydemonstratesthataccesstorespitecareisonewaytoimprovebothcarerecipientandcaregiverhealth.Whentheburdenoffamilycaregiversislightened,thesecaregiversaremoreabletocontinueintheircaregivingrole.
Summary

17
Pro
vid
ers
Wan
ted
Are
yo
u in
tere
sted
in
bec
om
ing
an
in
dep
end
ent
re
spit
e p
rovi
der
?•
Do y
ou e
njoy
set
ting
your
ow
n ho
urs?
• Do
you
enj
oy w
orki
ng w
ith
fam
ilies
?
• Do
you
wan
t to
mak
e a
fam
ily
care
give
r’s li
fe a
littl
e ea
sier
?
Cont
act y
our l
ocal
Res
pite
Coo
r- di
nato
r at
the
num
ber l
iste
d on
th
e in
side
of t
his
broc
hure
or g
o
to n
rrs.
ne.g
ov/r
espi
te to
app
ly.
Cal
l Sta
tew
ide
1-8
66-R
ES
PIT
E
1-8
66-7
37-7
483
Taki
ng
car
e of
yo
urs
elf —
is o
ne
of
the
bes
t w
ays
to h
elp
yo
ur
love
d o
ne!
We
Car
e fo
r
Tho
se W
ho
Car
e
for
Oth
ers
1-8
66-R
ES
PIT
E
1-8
66-7
37-7
483
htt
p://
nrr
s.n
e.go
v/re
spit
e
Did
Yo
u K
now
. .
.Th
ere
are
ove
r 21
9,0
00
id
enti
fied
fam
ily
care
giv
ers
in N
ebra
ska.
Res
pit
e Fu
nd
ing
S
ou
rces
For
mo
re in
form
atio
n o
n
resp
ite
fun
din
g g
o t
o:
nrr
s.n
e.go
v/re
spit
e/fu
nd
ing
• Ag
ed &
Dis
able
d M
edic
aid
W
aive
r (Ag
ed, A
dults
& C
hild
ren)
• Ad
ult P
rote
ctiv
e Se
rvic
es
• Al
tern
ativ
e Re
spon
se
• Ch
ild P
rote
ctiv
e Se
rvic
es/
Fost
er C
are
• De
velo
pmen
tal D
isab
ilitie
s
Med
icai
d W
aive
rs
• Di
sabl
ed C
hild
ren’s
Pro
gram
• N
ebra
ska
Life
span
Res
pite
Su
bsid
y Pr
ogra
m
• Pr
ivat
e Pa
y
• Su
bsid
ized
Ado
ptio
n
• Ti
tle II
I Old
er A
mer
ican
’s Ac
t
• U.
S. A
ir Fo
rce
Exce
ptio
nal F
amily
M
embe
r Pro
gram
• Ve
tera
ns C
areg
iver
Sup
port
For
assi
stan
ce w
ith
res
pit
e
fun
din
g o
r fi
nd
ing
a r
esp
ite
p
rovi
der
, co
nta
ct y
ou
r
loca
l Res
pit
e C
oo
rdin
ato
r.
CFS-
PAM
-26
5/2
018
Appendix

18
Wh
at is Resp
iteH
elp for the helpers. Respite is a break for unpaid fam
ily caregivers caring for a loved one w
ith special needs.
Respite allows the fam
ily caregiver tim
e away to care for their personal
needs.
Research shows that w
hen family
caregivers take time for them
selves, they im
prove their physical and em
otional health.
You can use respite to:
• G
o to the grocery store
• Visit the doctor
• H
ave lunch with a friend
• Take a nap
• O
r anything else you need or w
ant to reduce stress
Am
I a Family C
aregiver?
A family caregiver is a person w
ho provides ongoing care for an individual unable to care for them
self due to age, physical or m
ental disability, or illness. If your loved one cannot be left alone due to a special need, w
e can help.
Co
ntact Yo
ur Lo
cal Co
ord
inato
r to Learn
Mo
re:
Western A
rea308-432-8190respite@
wchr.net
Southw
est Area
308-345-4990respite@
swhealth.ne.gov
Central A
rea308-745-0780 ext. 139respite@
centralnebraskacap.com
Northern A
rea308-745-0780 ext. 145respite@
centralnebraskacap.com
Southeast402-300-8448southeastrespite@
unmc.edu
Eastern
402-559-5732eastrespite@
unmc.edu
SIO
UX
DA
WE
SS
HE
RID
AN
BO
X B
UTTE
SC
OTTS
BLU
FFM
OR
RILL
GA
RD
EN
BA
NN
ER
KIM
BA
LLC
HE
YE
NN
E
DE
UE
L
CH
ER
RY
GR
AN
T
AR
THU
R
KE
ITH
PE
RK
INS
CH
AS
E
DU
ND
YH
ITCH
CO
CK
HA
YE
S
LINC
OLN
MC
PH
ER
SO
N
HO
OK
ER
TH
OM
AS
LOG
AN
KE
YA PA
HA
BO
YD
BR
OW
NR
OC
K
HO
LT
BLA
INE
LOU
PG
AR
FIELD
WH
EE
LER
CU
STE
RV
ALLE
YG
RE
ELE
Y
SH
ER
MA
NH
OW
AR
D
DA
WS
ON
BU
FFALO
HA
LL
FRO
NTIE
R
RE
DW
ILLOW
GO
SP
ER
FUR
NA
S
PH
ELP
S
HA
RLA
N
KE
AR
NE
YA
DA
MS
FRA
NK
LINW
EB
STE
R
CLA
YFILLM
OR
E
NU
CK
OLLS
THA
YE
R
HA
MILTO
N
YO
RK
ME
RR
ICK
PO
LK
NA
NC
E
BO
ON
E
PLA
TTEC
OLFA
XD
OD
GE
WA
SH
- IN
GTO
N
AN
TELO
PE
MA
DIS
ON
STA
NTO
NC
UM
ING
BU
RT
KN
OX
CE
DA
R
DIX
ON
DA
KO
TA
THU
RS
TON
BU
TLER
SE
WA
RD
SA
LINE
JEFFE
RS
ON
SA
UN
DE
RS
LAN
CA
STE
R
GA
GE
OTO
E
JOH
NS
ON
NE
MA
HA
PAW
NE
E
PIE
RC
EW
AY
NE
RIC
HA
RD
SO
N
DO
UG
LAS
SA
RP
Y
CA
SS
Western
No
rthernC
entral
So
uth
west
So
uth
east Eastern
Wh
at is the
Neb
raska Lifespan
R
espite N
etwo
rkCaregiving is rew
arding, but also dem
anding and stressful. We offer
information, education & support.
We are th
e place
to co
ntact
to d
iscuss yo
ur
respite n
eeds.
Wh
o P
rovides R
espite
There is some flexibility in finding
providers. Your local Respite Coordin- ator can assist you w
ith finding a provider in your area. You m
ay be able to use fam
ily mem
bers, friends or neighbors as paid providers. Depending upon funding source, other possibilities include: organiza-tions, cam
ps, a trusted agency, a local volunteer-led organization or group, volunteer-led school-based program
, equine program
, faith-based or other approved activities. W
hile your loved one is attending an activity, you are getting a break —
and that’s what
respite is all about!Yo
u can
locate screen
ed resp
ite pro
viders
at: nrrs.n
e.gov/resp
ite
Click o
n: “Fin
d a P
rovider”

