results of the online survey (december 2010) - … · results of the online survey (december 2010)...
TRANSCRIPT
clinical auditS U P P O R T C E N T R E
The state of clinical audit -Results of the online survey (December 2010)
Developed and produced by
Clinical Audit Support CentreRaising standards in clinical audit
The online survey was devised by Clinical Audit Support Centre (CASC) and
supported by SNAP surveys. CASC sent an e-postcard on 15th December 2010
to a random selection of 700 individuals with an interest in clinical audit inviting
them to participate. The survey remained open for 10 days and closed at
midnight on Christmas Eve.
The survey incorporated a total of 13 main questions relating to a range of
current issues relevant to the clinical audit community.
Over the course of 10 days a total of 182 returns were received. Given that
individuals may have forwarded the initial e-postcard to take part in the survey
to other colleagues it is impossible to determine the exact response rate.
However, it is possible to determine with certainty that the response rate was
not greater than 182/700 (26%). Although this represents a modest response
rate, we would like to thank all those who gave up their time and submitted
responses.
Although our preference would have been for a response rate inexcess of 50%
we are confident that the results of this survey are reflective of the views of the
wider clinical audit community. We would also point out that the response rate
compares favourably to the Healthcare Quality Improvement Partnership’s 2010
stakeholder survey (16% return rate).
It should be noted that it is CASC policy to conduct all healthcare surveys in a
confidential manner and we did not ask respondents to provide any personally
identifiable data.
It should also be noted that comments received via the survey are included in
the appendicies. All comments made by respondents have been left as they
were submitted. We have not made any alterations to these. Where the exact
comment has been received we have grouped these together. All unique
comments are displayed individually.
As stated above, minimal ‘personal’ data was collected as part of the survey.
Respondents were asked a number of ‘demographic’ questions.
These included:
1) How would you classify yourself? (possible answers were ‘clinical audit
professional’, ‘clinical governance professional with responsibility for clinical
audit’, ‘clinician with interest/responsibility for audit, or ‘other’).
Clinical Audit Survey 20102
Background
The respondents
Response rate
2) How long have you worked in clinical audit? (free text response)
3) What sector do you work in? (possible answers were ‘Acute Care’, ‘Primary
Care’, ‘Mental Health’, ‘Ambulance Trust’ or ‘other’). Those who replied ‘other’
could then clarify further via free text.
Of the 182 respondents, the vast majority (67.0%) classified themselves as
‘clinical audit professionals’. Collectively the 182 respondents had amassed
1501 years worth of clinical audit experience. All sectors of healthcare were
represented in the survey with 42.3% of respondents from the acute sector,
21.4% from primary care and 16.5% from mental health. Given that the survey
was carried out online and took approximately ten minutes to complete, the
quality of responses was high – with few missed answers reported.
Clinical audit professional (122) 67.0%
Clinical governance professional with responsibility for audit (46) 25.3%
Clinician with interest/responsibility for audit (9) 4.9%
Other (5) 2.7%
Answers ranged from 1 year (8 responses) to 31 years (1 response). 6
respondents did not reply to this question. Further analysis showed two mode
results 3 and 10 years (both with 19 respondents).
1-5 years (65) 36.9%
6-10 years (56) 31.8%
11-15 years (28) 15.9%
16 years or more (27) 15.3%
The average time worked in clinical audit from the 176 respondents = (1501
years/176 respondents) = 8.53 years.
Acute Care (77) 42.3%
Ambulance Trust (8) 4.4%
Mental Health (30) 16.5%
Primary Care (39) 21.4%
Other (28) 15.4%
See Appendix 1 for further information in terms of how those that replied ‘other’
defined their sector of work.
3Clinical Audit Survey 2010
Q1. How would you classify yourself? (n=182)
Q2. How long have you worked in clinical audit?
Results by age banding were as follows (n=176):
Q3. What sector do you work in? (n=182)
The initial set of results relates to all 182 respondents.
*A total of 30 respondents (16.5%) did not reply as they noted that ‘I did not
work in clinical audit in 2006’. Of the remaining 152:
More positive (90) 59.2%
More negative (18) 11.8%
Neither positive/negative (44) 28.9%
*1 person did not reply. Of the remaining 181:
Yes (136) 75.1%
No (45) 24.9%
*24 (13.2%) respondents stated ‘I have not taken part in National Clinical
Audits’. Of the remaining 158:
Excellent (10) 6.3%
Good (56) 35.4%
Average (74) 46.9%
Poor (17) 10.8%
Very poor (1) 0.6%
A total of 109 (59.9%) qualitative responses were received. Of these, 16 did not
focus on a specific national audit project. For example, comments included:
‘don’t know’, ‘I have not been involved’, ‘I don’t deal with national audits’, ‘any
NBS audit’, etc.
93 responses named a single national audit or a group of national audits, e.g.
‘IBD or care of the dying’. In the small number of instances where multiple
replies were given by one respondent, each named audit has been allocated a
single vote.
Clinical Audit Survey 20104
Results
Q4. In 2006, the Chief Medical Officer stated a need to ‘reinvigorate clinical audit’.With this in mind, do you now feel more positive or negative about audit than in2006?
Q5. Do you still intend to work in clinical audit/or have responsibilities for clinicalaudit in five years’ time?
Q6. Overall, how would you rate the quality of National Clinical Audit projects thatyou have taken part in?
Q7a. What do you consider to be the most effective national audit?
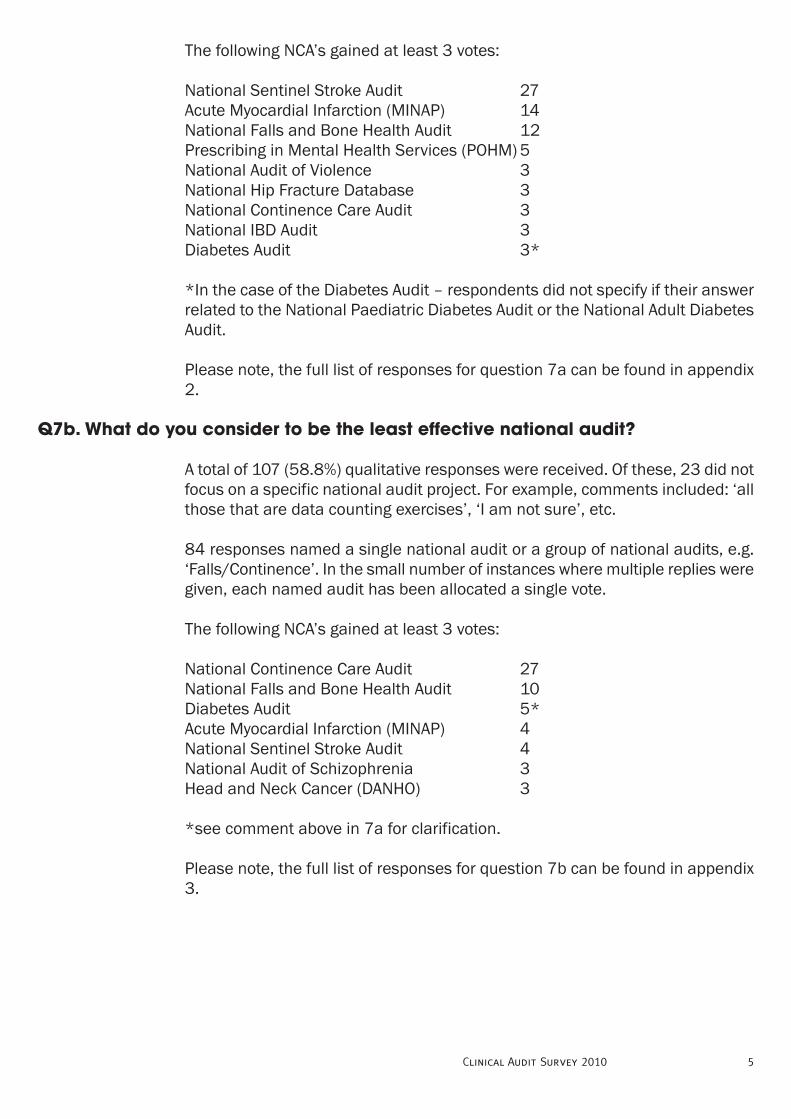
The following NCA’s gained at least 3 votes:
National Sentinel Stroke Audit 27
Acute Myocardial Infarction (MINAP) 14
National Falls and Bone Health Audit 12
Prescribing in Mental Health Services (POHM) 5
National Audit of Violence 3
National Hip Fracture Database 3
National Continence Care Audit 3
National IBD Audit 3
Diabetes Audit 3*
*In the case of the Diabetes Audit – respondents did not specify if their answer
related to the National Paediatric Diabetes Audit or the National Adult Diabetes
Audit.
Please note, the full list of responses for question 7a can be found in appendix
2.
A total of 107 (58.8%) qualitative responses were received. Of these, 23 did not
focus on a specific national audit project. For example, comments included: ‘all
those that are data counting exercises’, ‘I am not sure’, etc.
84 responses named a single national audit or a group of national audits, e.g.
‘Falls/Continence’. In the small number of instances where multiple replies were
given, each named audit has been allocated a single vote.
The following NCA’s gained at least 3 votes:
National Continence Care Audit 27
National Falls and Bone Health Audit 10
Diabetes Audit 5*
Acute Myocardial Infarction (MINAP) 4
National Sentinel Stroke Audit 4
National Audit of Schizophrenia 3
Head and Neck Cancer (DANHO) 3
*see comment above in 7a for clarification.
Please note, the full list of responses for question 7b can be found in appendix
3.
5Clinical Audit Survey 2010
Q7b. What do you consider to be the least effective national audit?
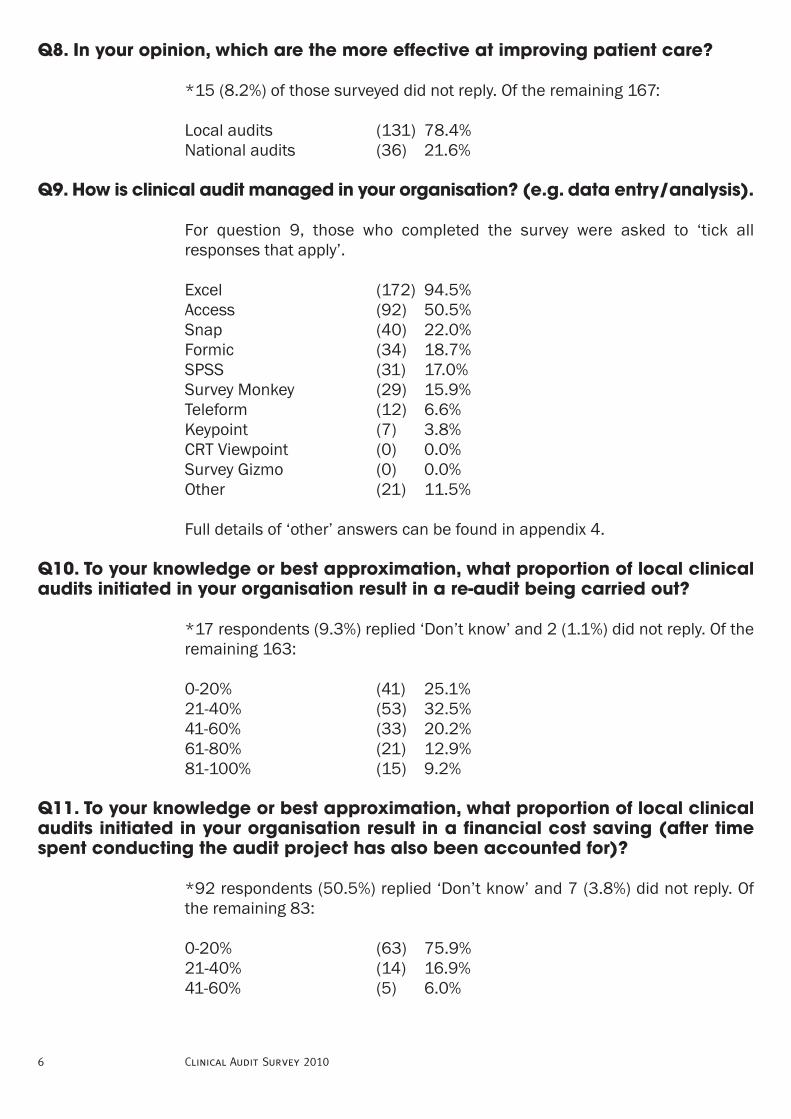
*15 (8.2%) of those surveyed did not reply. Of the remaining 167:
Local audits (131) 78.4%
National audits (36) 21.6%
For question 9, those who completed the survey were asked to ‘tick all
responses that apply’.
Excel (172) 94.5%
Access (92) 50.5%
Snap (40) 22.0%
Formic (34) 18.7%
SPSS (31) 17.0%
Survey Monkey (29) 15.9%
Teleform (12) 6.6%
Keypoint (7) 3.8%
CRT Viewpoint (0) 0.0%
Survey Gizmo (0) 0.0%
Other (21) 11.5%
Full details of ‘other’ answers can be found in appendix 4.
*17 respondents (9.3%) replied ‘Don’t know’ and 2 (1.1%) did not reply. Of the
remaining 163:
0-20% (41) 25.1%
21-40% (53) 32.5%
41-60% (33) 20.2%
61-80% (21) 12.9%
81-100% (15) 9.2%
*92 respondents (50.5%) replied ‘Don’t know’ and 7 (3.8%) did not reply. Of
the remaining 83:
0-20% (63) 75.9%
21-40% (14) 16.9%
41-60% (5) 6.0%
Clinical Audit Survey 20106
Q8. In your opinion, which are the more effective at improving patient care?
Q9. How is clinical audit managed in your organisation? (e.g. data entry/analysis).
Q10. To your knowledge or best approximation, what proportion of local clinicalaudits initiated in your organisation result in a re-audit being carried out?
Q11. To your knowledge or best approximation, what proportion of local clinicalaudits initiated in your organisation result in a financial cost saving (after timespent conducting the audit project has also been accounted for)?
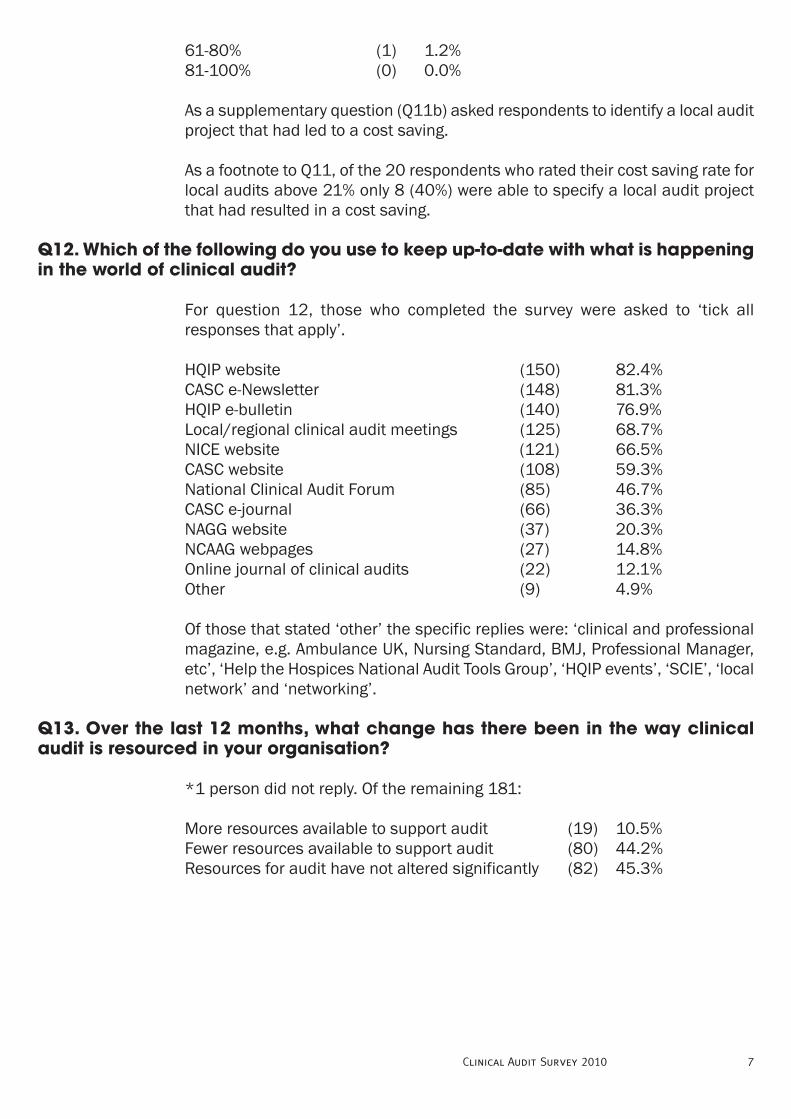
61-80% (1) 1.2%
81-100% (0) 0.0%
As a supplementary question (Q11b) asked respondents to identify a local audit
project that had led to a cost saving.
As a footnote to Q11, of the 20 respondents who rated their cost saving rate for
local audits above 21% only 8 (40%) were able to specify a local audit project
that had resulted in a cost saving.
For question 12, those who completed the survey were asked to ‘tick all
responses that apply’.
HQIP website (150) 82.4%
CASC e-Newsletter (148) 81.3%
HQIP e-bulletin (140) 76.9%
Local/regional clinical audit meetings (125) 68.7%
NICE website (121) 66.5%
CASC website (108) 59.3%
National Clinical Audit Forum (85) 46.7%
CASC e-journal (66) 36.3%
NAGG website (37) 20.3%
NCAAG webpages (27) 14.8%
Online journal of clinical audits (22) 12.1%
Other (9) 4.9%
Of those that stated ‘other’ the specific replies were: ‘clinical and professional
magazine, e.g. Ambulance UK, Nursing Standard, BMJ, Professional Manager,
etc’, ‘Help the Hospices National Audit Tools Group’, ‘HQIP events’, ‘SCIE’, ‘local
network’ and ‘networking’.
*1 person did not reply. Of the remaining 181:
More resources available to support audit (19) 10.5%
Fewer resources available to support audit (80) 44.2%
Resources for audit have not altered significantly (82) 45.3%
7Clinical Audit Survey 2010
Q12. Which of the following do you use to keep up-to-date with what is happeningin the world of clinical audit?
Q13. Over the last 12 months, what change has there been in the way clinicalaudit is resourced in your organisation?

A total of 122 clinical audit professionals completed the online survey and this
section of the report looks at the results specific to them.
Answers ranged from 1 year (6 responses) to 20 years (4 responses). 4
respondents did not reply to this question. Further analysis showed the mode
result was 10 years (with 16 respondents).
Results by age banding were as follows (n=118):
1-5 years (41) 34.7% -2.2%
6-10 years (42) 35.6% +3.8%
11-15 years (16) 13.6% -2.3%
16 years or more (19) 16.1% +0.8%
Acute Care (56) 45.9% -3.6%
Ambulance Trust (7) 5.7% +1.3%
Mental Health (17) 13.9% -2.6%
Primary Care (23) 18.9% -2.5%
Other (19) 15.6% +0.2%
*A total of 19 respondents (15.6%) did not reply as they noted that ‘I did not
work in clinical audit in 2006. Of the remaining 103:
More Positive (60) 58.3% -0.9%
More Negative (14) 13.6% +1.8%
Neither positive/negative (29) 28.2% -0.7%
*1 person did not reply. Of the remaining 121:
Yes (90) 74.4% -0.7%
No (31) 25.6% +0.7%
Clinical Audit Survey 20108
Results by Clinical Audit Professional Only
Q2. How long have you worked in clinical audit?
Q3. What sector do you work in? (n=122):
Q4. In 2006, the Chief Medical Officer stated a need to ‘reinvigorate clinical audit’.With this in mind, do you now feel more positive or negative about audit in 2006?
Q5. Do you still intend to work in clinical audit/or have responsibilities for clinicalaudit in five years’ time?

*14 (11.5%) respondents stated ‘I have not taken part in National Clinical
Audits’. Of the remaining 108:
Excellent (5) 4.6% -1.7%
Good (35) 32.4% -3.0%
Moderate (54) 50.0% +3.1%
Poor (13) 12.0% +1.2%
Very Poor (1) 0.9% +0.3%
The following NCA’s gained at least 3 votes specifically from clinical audit
professionals:
National Sentinel Stroke Audit 17
Acute Myocardial Infarction (MINAP) 11
National Falls and Bone Health Audit 11
Prescribing in Mental Health Services (POHM) 4
National Hip Fracture Database 3
National IBD Audit 3
The following NCA’s gained at least 3 votes specifically from clinical audit
professionals:
National Continence Care Audit 28
National Falls and Bone Health Audit 9
Diabetes Audit 3
Acute Myocardial Infarction (MINAP) 3
National Sentinel Stroke Audit 3
Head and Neck Cancer (DANHO) 3
*10 (8.2%) of those surveyed did not reply. Of the remaining 112:
Local audits (89) 79.5% +1.1%
National audits (23) 20.5% -1.1%
9Clinical Audit Survey 2010
Q6. Overall, how would you rate the quality of National Clinical Audit projects thatyou have taken part in?
Q7a. What do you consider to be the most effective national audit?
Q7b. What do you consider to be the least effective national audit?
Q8. In your opinion, which are the more effective at improving patient care?
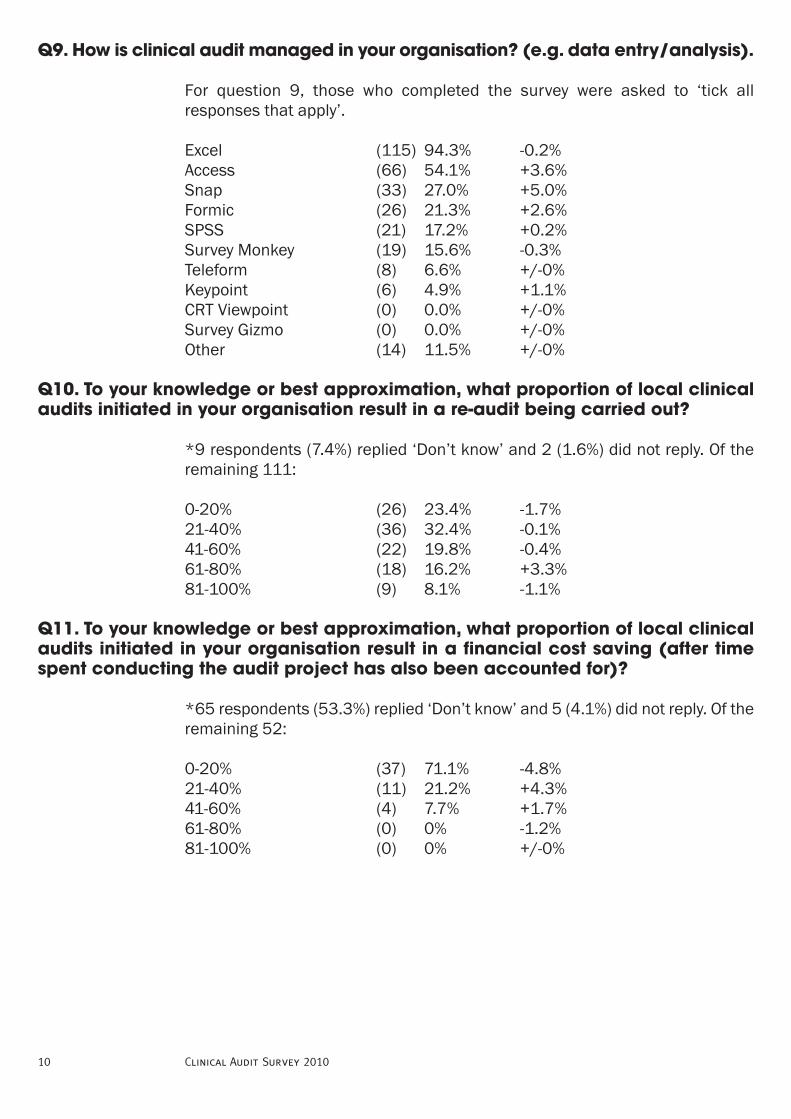
For question 9, those who completed the survey were asked to ‘tick all
responses that apply’.
Excel (115) 94.3% -0.2%
Access (66) 54.1% +3.6%
Snap (33) 27.0% +5.0%
Formic (26) 21.3% +2.6%
SPSS (21) 17.2% +0.2%
Survey Monkey (19) 15.6% -0.3%
Teleform (8) 6.6% +/-0%
Keypoint (6) 4.9% +1.1%
CRT Viewpoint (0) 0.0% +/-0%
Survey Gizmo (0) 0.0% +/-0%
Other (14) 11.5% +/-0%
*9 respondents (7.4%) replied ‘Don’t know’ and 2 (1.6%) did not reply. Of the
remaining 111:
0-20% (26) 23.4% -1.7%
21-40% (36) 32.4% -0.1%
41-60% (22) 19.8% -0.4%
61-80% (18) 16.2% +3.3%
81-100% (9) 8.1% -1.1%
*65 respondents (53.3%) replied ‘Don’t know’ and 5 (4.1%) did not reply. Of the
remaining 52:
0-20% (37) 71.1% -4.8%
21-40% (11) 21.2% +4.3%
41-60% (4) 7.7% +1.7%
61-80% (0) 0% -1.2%
81-100% (0) 0% +/-0%
Clinical Audit Survey 201010
Q9. How is clinical audit managed in your organisation? (e.g. data entry/analysis).
Q10. To your knowledge or best approximation, what proportion of local clinicalaudits initiated in your organisation result in a re-audit being carried out?
Q11. To your knowledge or best approximation, what proportion of local clinicalaudits initiated in your organisation result in a financial cost saving (after timespent conducting the audit project has also been accounted for)?
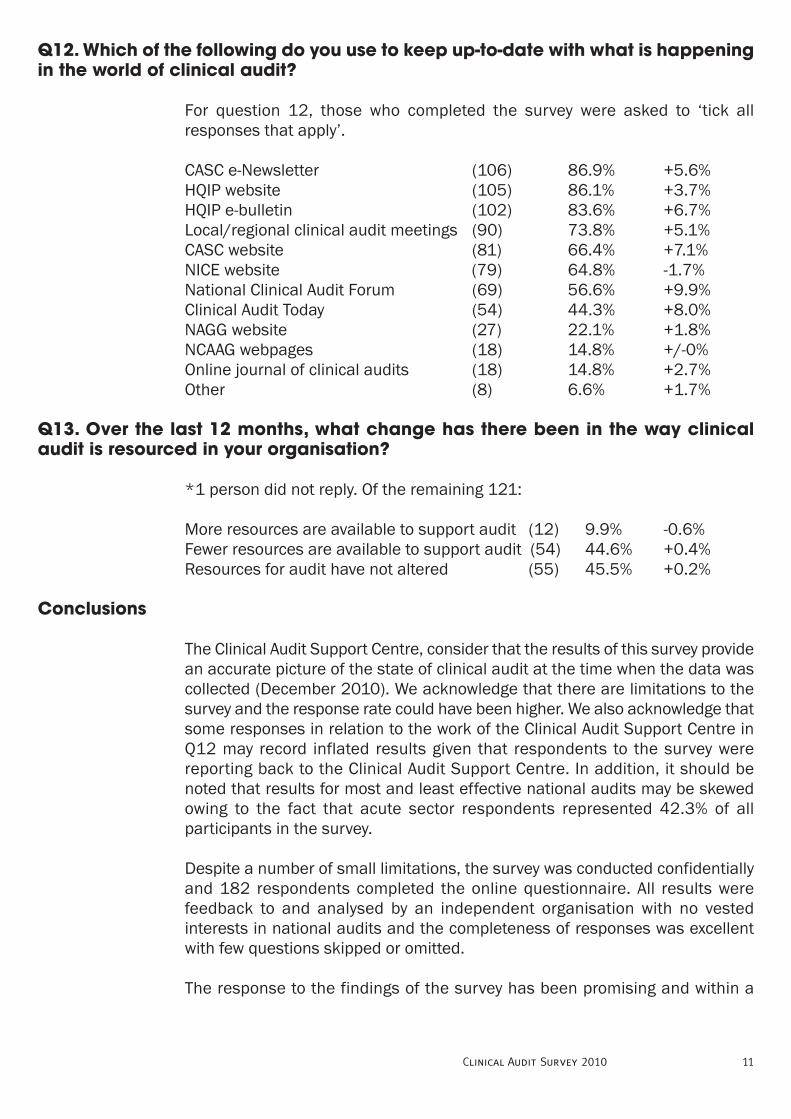
For question 12, those who completed the survey were asked to ‘tick all
responses that apply’.
CASC e-Newsletter (106) 86.9% +5.6%
HQIP website (105) 86.1% +3.7%
HQIP e-bulletin (102) 83.6% +6.7%
Local/regional clinical audit meetings (90) 73.8% +5.1%
CASC website (81) 66.4% +7.1%
NICE website (79) 64.8% -1.7%
National Clinical Audit Forum (69) 56.6% +9.9%
Clinical Audit Today (54) 44.3% +8.0%
NAGG website (27) 22.1% +1.8%
NCAAG webpages (18) 14.8% +/-0%
Online journal of clinical audits (18) 14.8% +2.7%
Other (8) 6.6% +1.7%
*1 person did not reply. Of the remaining 121:
More resources are available to support audit (12) 9.9% -0.6%
Fewer resources are available to support audit (54) 44.6% +0.4%
Resources for audit have not altered (55) 45.5% +0.2%
The Clinical Audit Support Centre, consider that the results of this survey provide
an accurate picture of the state of clinical audit at the time when the data was
collected (December 2010). We acknowledge that there are limitations to the
survey and the response rate could have been higher. We also acknowledge that
some responses in relation to the work of the Clinical Audit Support Centre in
Q12 may record inflated results given that respondents to the survey were
reporting back to the Clinical Audit Support Centre. In addition, it should be
noted that results for most and least effective national audits may be skewed
owing to the fact that acute sector respondents represented 42.3% of all
participants in the survey.
Despite a number of small limitations, the survey was conducted confidentially
and 182 respondents completed the online questionnaire. All results were
feedback to and analysed by an independent organisation with no vested
interests in national audits and the completeness of responses was excellent
with few questions skipped or omitted.
The response to the findings of the survey has been promising and within a
11Clinical Audit Survey 2010
Q12. Which of the following do you use to keep up-to-date with what is happeningin the world of clinical audit?
Q13. Over the last 12 months, what change has there been in the way clinicalaudit is resourced in your organisation?
Conclusions
month of publishing interim results, Professor Nick Black (Chair of the National
Clinical Audit Advisory Group) was presenting data from the study at the national
clinical audit conference in London. Indeed, results of the survey have gained
widespread interest and CASC have presented data at national meetings (e.g.
the National Audit Governance Group in September 2011) and regional
meetings (e.g. South and East London Clinical Audit Network in September
2011). The draft report was tabled and discussed at the National Clinical Audit
Advisory Group meeting in September 2011 (which includes representation from
the Department of Health) and numerous clinical audit/governance
professionals have requested copies of the document.
In Autumn 2011, the Clinical Audit Support Centre circulated the draft report to
the key bodies with a responsibility for clinical audit and requested feedback. It
is disappointing to note that none was received. However, it is clear that the
survey has had an impact at many levels and it is not surprising that on 12th
December 2011 the Healthcare Quality Improvement Partnership announced
that the National Continence Audit (voted the least effective national audit by
27 survey respondents) is undergoing significant revision.
In terms of picking out key findings from the survey, this is not easy given the
significant amount of data obtained. However, the Clinical Audit Support Centre
would draw attention to the following:
• Despite the continued expansion of the national audit programme, those
working in clinical audit are clear that local audit (not national) is a more
effective tool for improving patient care
• National clinical audits continue to divide opinion. Given the huge
financial resources national audits devour each year and considering the
time they take local teams to conduct, the fact that 46.9% of respondents
rated them as ‘moderate’ is hugely concerning
• Results of the survey clearly show that resourcing for clinical audit is
decreasing. This is not surprising given the current financial climate but
it is concerning when one reflects that clinical audit is apparently
undergoing a phase of ‘re-invigoration’
• The study shows that more attention needs to be paid to re-auditing.
Figures indicate the majority of respondents reported a re-audit rate of
40% or less. Given that re-audit is essential if the benefits of any given
clinical audit project are to be realised, efforts must be made to improve
re-audit rates for both local and national clinical audits
• The vast majority of current clinical audits do not result in cost savings.
Furthermore, most respondents do not evaluate whether their audits save
money and therefore more debate is required here.
On a final note, the Clinical Audit Support Centre would like to draw your
Clinical Audit Survey 201012
attention to the fact that the online survey will be repeated in December 2011.
Results and findings of the follow-up survey will be published in Spring 2012
and we consider that the second survey may prove more beneficial than the first
given that we will be in a position to compare results from 2010 with results
from 2011.
Acknowledgements
The Clinical Audit Support Centre would like to pay thanks to:
1) Snap Surveys for providing the online software support
2) All those who took time to complete the online survey as well as those
who encouraged others to take part
Information on the appendix:
All comments listed in the report from this point onwards are printed as they
were received. We have not altered comments from those who took part in the
survey, hence some typos and spelling mistakes will appear from time to time.
For ease, the comments have been placed in alphabetical order.
13Clinical Audit Survey 2010

Appendix 1:
Further responses for those who replied ‘other’ when asked to define their sector
of work:
• ALB (i.e. arms length business)
• All the above (i.e. primary, acute, mental health and ambulance)
• Community Health Service (x2)
• Community provider
• Cross-sector audit
• Hospice (x2)
• I am responsible for clinical audit in the commissioner, community
services and acute sector
• Local Health Board – both primary, acute and mental health care
• Blood and Transfusion (x2)
• Our organisation is unique in that it encompasses all these sections in
one PCT – both provider and commissioner
• Offender health
• PCT (x2)
• Primary care, community services, commissioning, public health
• Provider Services
• Rheumatology/secondary care
• Royal College
• Secondary care
• SHA
• Tertiary specialist care
• Tertiary specialist hospital
Clinical Audit Survey 201014

Appendix 2: Answers to ‘Most Effective’ NCA:
All Royal College of Psychiatrists projects
Ambulance Services still have little direct involvement in many of the Natioanl
Audit Projects. The one which has the most impact is MINAP, and even though
we do not directly contribute data I feel this is an effective national project which
has demonstrated real improvements in care over the years
Any NBS audit has usually proved beneficial, clear audit criteria are set to
measure performance against. In fact any audit that has clear, evidence based
audit criteria will be effective as they show up all strengths and weaknesses
Audits carried out by the Royal College of Physicians tend to be good e.g National
IBD audit
Because of the nature of its services, this Trust only participates in the National
Falls and Bone Health Audit. It is difficult to say how much the audit has affected
services given the extent of general service redesign as a result of NHS
organisational churn in the last 3 years. It is almost certainly helpful in
ascertaining the national overview
Bowel
Cannot comment do not have to complete national audit
Comparative Audit of Blood Transfusion
Continence
Dementia (x2)
Diabetes (x2)
Don't know
Falls (x4)
Falls and Bone Health (x2)
Falls and Bone
Falls in bone health
Falls in elderly
Have not been involved
15Clinical Audit Survey 2010
I am not currently involved in nationla clinical audits
I dont deal with the National Audits
I was involved with the pilot of the controlled drugs audit as a result of the Harold
Shipman events. It was an excellent audit with some very good
recommendations as a result
IBD
IBD or care of the dying
MINAP (x11)
MINAP in its early days
MINAP – Myocardial Infarction National Audit Project
Most effective so far is the NAPT although this hasnt quite finsihed
N/A I haven't personally been involved with any national audits
National audit of falls and bone health in older people PROMS
National Audit of Violence (x3)
National Continence Audit
National Diabetes Audit
National Falls & Bone Health
National Hip Fracture Database (x3)
National intermediate care audit pilot
National Sentinal Stroke Audit
National Sentinel Audit for Stroke
National Sentinel Stroke Audit (x2)
National Sentinel Stroke Audit - do actually see improvements
National stroke - only because it has got attention for a 'Cinderella' service over
many years not because I think the information analysis is robust or the data
submitted is reliable
Clinical Audit Survey 201016
National Stroke & Continence National Audit
National Stroke Audit
NBOCAP - National Bowel Cancer Audit Project
NCEPOD (x2)
NICE audit standards monitoring
No taken part
None (x2)
Not sure - haven't often been privy to any changes implemented after results
are published
Not undertaken sufficient number of national audits to have an opinion
POMH UK (x2)
POMH-UK audits
POMHS
Prescribing in mental health services
Prescribing Observatory for Mental Health national benchmarking projects
RCP National Falls Audit
Relatively few applicable to tertiary cancer care - value often comes from
knowing we compare well with other providers
Reperfusion - adminstration of thrombolysis for MI patients (Call to Needle) as
it encourages cross disciplinary working, individual case investigation and
providing information that steered future care and improvements in treatment
Sentinel
Sentinel Stroke (x3)
Sentinel Stroke Audit (x3)
Sentinel stroke audit. It is multidisciplinary with clear standards and has moved
stroke care forward in defining areas of both good practice and that need more
attention
17Clinical Audit Survey 2010

Sentinel Stroke Audit - it's not easy or intuitive to collect the data and complete
the forms, but they do get excellent participation rates and it does seem to have
resulted in real change and improvement in the management of stroke in this
country - at least in the early yesrs - possibly this has wained a little in recent
times
Staff survey
Stroke (x8)
Stroke audit
Stroke care
Stroke, National Neonatal Audit Programme
Suicide Prevention - NPSA
The best National Audits are the ones that report back with usable information
to Trusts to enable positive change
The Kidney programme
The most effective is probably the national audit of continence care led by the
Royal College of Physicians. It has been promoted well and the support received
from the RCP was great. It is high on the agenda in my organisation and actions
to address issues are in place
The national audits I refer to are based on tools developed by the National Audit
Tools Group of Help the Hospices. All tools are extremely effective
With reference to Wales it would be Sentinel Stroke - it took several rounds but
the national status it has now achieved, is as a result of the persistent reporting
of the national audit
1000 Lives Campaign (Wales)
Clinical Audit Survey 201018
Appendix 3: Answers to ‘Least Effective’ NCA:
All national databases, eg MINAP, ICNARC and the like. Data collection exercises
that may highlight good practice elsewhere but clinicians hide behind the report
(and sometimes don't even share the results) and the fact that 'we' are taking
part so therefore change is not required
All Royal College of Physicians projects
All those that are data counting exercises
Any of the national audits that aren't really audit - just data collection!
Any of the National Patient Experience Surveys - no one accepts ownership for
the results and taking and action plan forward
BTS Audits badly designed
Can't say although previous national falls audit reporting has led to 'accurate'
but very misleading reporting because of the way it was set up (also true of
stroke reporting) which I find counter productive and undermines my confidence
in their use
Cancer audits
Cancer databases, e.g. LUCADA, DAHNO
Clinical Performance Indicators for Ambulance Trusts as these are only snapshot
audits and although encourage local improvement through benchmarking
becomes more of a measure of documentation compliance rather than focusing
on improving why clinical care not given
Continence (x12)
Continence audit (x2)
Continence Care (x5)
Continence in primary care
DAHNO - Data for Head & Neck Oncology
Dementia (x2)
Diabetes
Diabetes Inpatient Audit
19Clinical Audit Survey 2010

Don't know
Emergency medicine audits
Ethnic census
Falls (x2)
Falls and bone health in older people (x2)
Falls and bone health
Falls/Continence
GP
Healthcare Commission Schizophrenia audit 2008 took too long to be reported
on
I am not currently involved in nationla clinical audits
I am not sure
I dont deal with the National Audits
IBD (x2)
Incontinence
Inpatient Diabetes - proper permissions we not achieved prior to undertaking
the audit and organisations did not recieve the feedback promised at the outset.
National audits take a substantial local resource and effort to undertake,
effective outcome reporting is paramount
Inpatient survey
Least effective was the National Audit of Continence Care
MINAP
Minap, Falls
Minap. Massive, problematic, data collection exercise that produces much stress
and no constructive feedback
N/A I haven't personally been involved with any national audits
National audit of Continence
Clinical Audit Survey 201020
National audit of depression
National Continence
National Continence Audit
National Diabetes Audit (x2)
National Falls & Bones
National Heart Failure Audit
National Sentinel Stroke audit
NCEPOD (All, never complete audit cycle, very low participation rates)
No opinion
No view
None (x2)
Not known
Not sure - haven't often been privy to any changes implemented after results
are published
Not undertaken sufficient number of national audits to have an opinion
Parkinsons Disease
Patient Survey
POMH
RCP - Proctologists project which was never reported, allegedly because the
results were so bad
RCP Continence
RCP-National Falls & Bone Health
Relatively few applicable to tertiary cancer care - DAHNO is particularly complex,
ill-thought out and inflexible
Schizophrenia (x2)
21Clinical Audit Survey 2010
SCTS Thoracic - a huge data collecting exercise, that seems to give very little
information back - and only a few trusts participate in it. The same could be
said for several of the CCAD run audits
Sentinel Audit of Stroke
Some of the BTS audits as the turnaround for the audits are too quick not
allowing changes to be implemented
Stroke
Suicide
Surgical site surveillance (HPA)
The initial national diabetes audit project
Thoracic surgery register
Tissue Viability Audit seemed to fall flat on its face!
Unknown
Unsure
We have participated in a number of Oncology audits from the Royal College of
Radiologists over the last 2 years and to date have not recieved any reports!
Clinical Audit Survey 201022

Appendix 4:Qualitative responses to ‘other’ IT used:
• Epi
• Epi Info
• For Enhancing Quality we use the Quality Measures Reporter software
• Infoflex
• Lime survey
• Manual
• Minitab
• Miscrosoft SharePoint
• Most of our data is collected in either Intellect or Infoflex. We also use
chartrunner to run spc charts for many projects
• Optimum - we are unfortunately about to lose Formic due to economic
constraints
• Remote extraction of data from GP systems
• Quasar
• SAS
• SharePoint to Excel or Access
• Sphinx (2)
• Starting to develop info path - does seem to be as easy as survey monkey
• Through trust
• We don't collect data
• Word
23Clinical Audit Survey 2010

© Copyright 2011 Clinical Audit Support Centre Ltd
Clinical Audit Support Centre
PO BOX 8429,
LEICESTER, LE8 0WS,
UNITED KINGDOM
T: +44 (0)116 264 3411
F: +44 (0)116 278 7679
W: clinicalauditsupport.com
Twitter: @cascleicester