revenue integrity: preparing for contractor combat east tennessee fraud working group tennessee...
TRANSCRIPT
Revenue Integrity: Preparing for Contractor Combat
East Tennessee Fraud Working GroupTennessee Hospital Association
Fall Compliance Conference 2009
October 21, 2009
Sara Kay WheelerKing & Spalding LLP
Revenue Integrity: Preparing for Contractor Combat
East Tennessee Fraud Working GroupTennessee Hospital Association
Fall Compliance Conference 2009
October 21, 2009
Sara Kay WheelerKing & Spalding LLP

2
Overview• Topics to Address:
• Contractor Overview
• Procurement Timeline
• Important Developments
• Practical Strategies
• Approach to Materials

Reality
• Issue: – Increased number of government contractors actively
trying to identify Medicare and Medicaid overpayments and potential fraud
• Solution:– Organizations need effective processes to facilitate
proactive and reactive steps to prepare for and manage contractor inquiries and disputes

Pressure on Claims• Growing number of entities (federal agencies,
state agencies and government contractors) reviewing federal healthcare provider reimbursement – Not limited to inpatient and outpatient hospital claims– Scrutiny will come from all directions
• Weapons becoming more powerful:– Enhanced federal false claims act– Newly introduced state false claims acts
• e.g., Tennessee Medicaid False Claims Act– Employee education requirements designed to
encourage whistle blowing

Low Hanging Fruit• Government agencies and contractors firmly believe
there is massive fraud and abuse in the system– CMS estimates:
• $10.4 Billion “improper payments” in general Medicare program• $18.6 Billion in “improper payments” in Medicaid program
– OIG reports:• $2.04 Billion in investigative receivables (FY 2006-2008)• $1.22 Billion in audit disallowances (same time period)• $16.7 Billion in savings (2008)
– FBI projects:• 3-10% of total health spending ($75-$250 billion in FY 2009)
• Reality: More pressure on gov’t to recover

Core Areas
• Core areas critical to ability to successfully manage this complex process– Government contractor landscape (players, current
developments, etc.)– Effective strategies for analyzing internal and external
audit findings– Administrative appeal processes– Federal and state litigation strategies– Compliance oriented processes to help organize effort– Fraud and abuse analyses

Contractor Landscape
• Older Contractors– FIs – Fiscal Intermediaries (Medicare Part A)– Carriers (Medicare Part B)– DMERCs – Durable Medical Equipment Regional
Carriers– PROs – Peer Review Organizations– QIOs – Quality Improvement Organizations– Many others

Contractor Landscape
• Newer Contractors– MACs – Medicare
Administrative Contractors
– PSCs – Program Safeguard Contractors
– ZPICs – Zone Program Integrity Contractors
– RACS – Recovery Audit Contractors
– MEDICs – Medicare Drug Integrity Contractors
– RVCs – Recovery Audit Validation Contractors
– QICs – Qualified Independent Contractors
– MICs – Medicaid Integrity Contractors
– MIG – Federal Medicaid Integrity Group (engages MICs)

Pharmacy Retail Contractors• Currently:
– MEDICs - Medicare Drug Integrity Contractors– MICs - Medicaid Integrity Contractors
• Eventually:– ZPICs - Zone Program Integrity Contractors
(will replace the MEDICs)
10
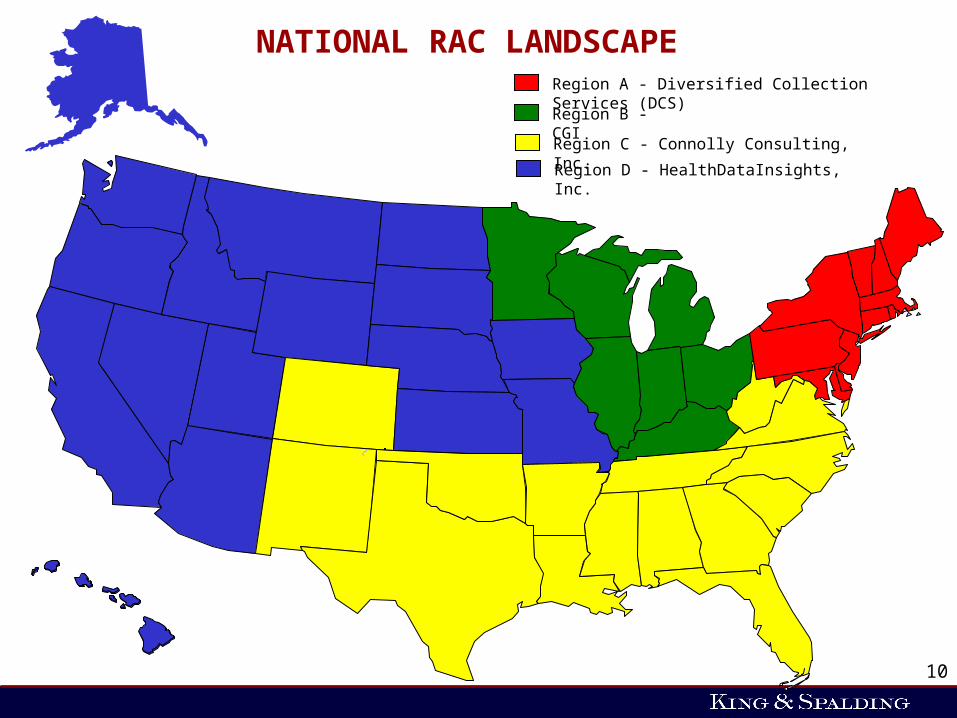
NATIONAL RAC LANDSCAPERegion A - Diversified Collection Services (DCS)
Region B - CGI
Region C - Connolly Consulting, Inc.
Region D - HealthDataInsights, Inc.

MICs – Regional Organization
• Region 1 and 2: New York / Boston
• Region 3 and 4: Atlanta / Philadelphia
• Region 5 and 7: Chicago / Kansas City
• Region 6 and 8: Dallas / Denver
• Region 9 and 10: San Francisco / Seattle

Review of Provider MIC Zones Awarded
AdvanceMed Corporation
Thomson Reuters
Umbrella Contracts Also Awarded to:
ACS Healthcare Analytics
IMS Government Solutions
SafeGuard Services
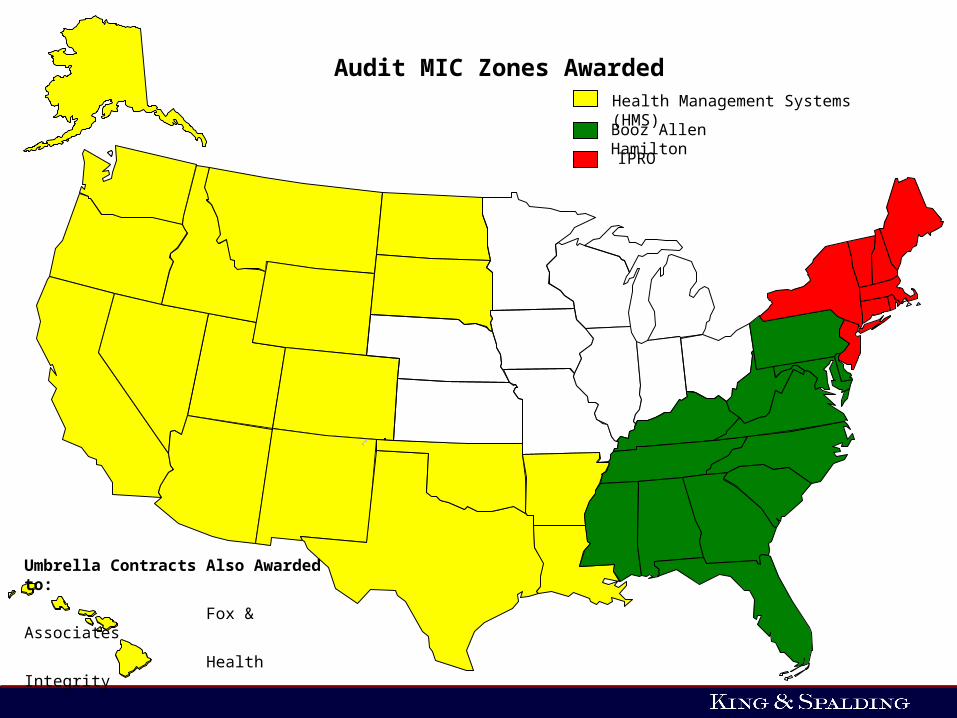
Audit MIC Zones AwardedHealth Management Systems (HMS)
Booz Allen Hamilton
Umbrella Contracts Also Awarded to:
Fox & Associates
Health Integrity
IPRO

Education MICs
• Umbrella contracts have been awarded to:
–Information Experts
–Strategic Health Solutions
• Contracts expected to be awarded by September 2009

ZPIC Implementation
• CMS organized ZPIC procurement in cycles to establish 7 zones that align with MAC jurisdictions– Cycle 1 (Zones 4, 5 and 7)– Cycle 2 (Zones 1 and 2)– Cycle 3 (Zones 3 and 6)
• The ZPIC in each zone will perform benefit integrity functions for Medicare Parts A, B, C, D, DME, Home Health and Hospice, and Medi-Medi

ZPICs Health Integrity LLC (Zone 4)
AdvanceMed Corporation (Zone 5)*
SafeGuard Services LLC (Zone 7)

RAC Developments
• February 4, 2009 - RAC bid protest resolved; CMS proceeded with RAC implementation
• Provider outreach efforts underway

RAC Developments (cont’d)
• Issues to monitor– RAC discussion period – Efforts to limit recoupment
• CMS Code 432 versus Code 469– RAC licensing of Milliman Care Guidelines
• e.g., HealthDataInsights and Connolly– Ability to rebill claims denied by the RAC– CMS rules and guidelines regarding exclusion and
suppression of claims from RAC Data Warehouse
MIC Developments
• Efforts to improve provider outreach (announced during July 15, 2009 Open Door Forum)– Hosting of Open Door Forum Conference Calls– Publishing of documents to assist providers
• FAQs on Medicaid Integrity Program• Procurement timelines• Audit A-Z
– Look for documents: www.cms.hhs.gov/MedicaidIntegrityProgram
– Addressing provider questions submitted through Medicaid Integrity Program mailbox:[email protected]

MIC Developments (cont’d)• Division of Fraud Research & Detection
– Director: Jim Gorman– Received data subsets from all states– Loaded into database in California– Running queries and algorithms – Analyzed data for 50% of states– Expects to finish analysis for remaining states by end of 2009– Medicaid managed care data is a “work in progress” because there is state variation
with respect to data reporting requirements
• Source: July 15, 2009 CMS Open Door Forum

MIC Developments (cont’d)
• Division of Field Operations– Director: Robb Miller– Actively screening data for the entire country by end
of year– Actively conducting audits in 17 states – 500 audits currently underway (70 of which are in
Texas)• 44% of audits are of hospitals• 29% of audits are of long term care facilities• 21% of audits are of pharmacies
• Source: July 15, 2009 CMS Open Door Forum

RACs and MICs Compared
• RACs– Provider outreach
mandatory
– Review period – set
– Time to produce records – 45 days (possible extensions)
– Number of records – limited
– Appeal process – consistent across regions
• MICs– Provider outreach not
mandatory
– Review period – not set
– Time to produce records – shorter (possible extensions)
– Number of records – no limit
– Appeal process – mirrors state Medicaid appeal process

MIC Appeal Process• Audit MIC contacts provider
• Provider produces records
• Audit MIC analyzes info
• Audit MIC generates draft audit
report and submits to CMS MIG
• CMS MIG reviews and sends to
state Medicaid agency
• State may make comment
• Audit MIC sends draft report to
provider
• Provider has 30 days to review
and provide comments
• Additional review by CMS MIG
• CMS MIG issues final audit
report to state Medicaid agency
for "execution”
– CMS MIG can also refer to law
enforcement at this time
• State issues demand to provider
regarding alleged overpayment
which triggers appeal procedures

Preparedness
• Infrastructure– Contractor committee(s)
– Information management• Records collection• Control • Production• HIPAA
– Document and records hosting
– Chain of responsibility
– Management of overlapping deadlines
• Other Activities– Governance considerations
– Pre-audit testing
– Data mining
– Contractor intelligence• E.g., HMS website for
MIC audits

Comprehensive Analysis and Related Strategies
• Critical to proactively assess interactions with government contractors
• OIG expects $2.4 billion in recoveries for health programs in FY 2009

Comprehensive Analysis and Related Strategies (cont’d)
• Example: RACs– Potential RAC outcomes not limited to overpayments– RAC Statute… “A recovery of an overpayment…
under [the RAC Statute] shall not be construed to prohibit the Secretary [i.e., OIG] or the Attorney General [i.e., DOJ] from investigating and prosecuting, if appropriate, allegations of fraud or abuse arising from such overpayment.”
– RAC Statement of Work requires RAC to report instances of potential fraud immediately to the CMS Project Officer
– Enforcement agencies expect RACs to make referrals

Comprehensive Analysis and Related Strategies (cont’d)
• Exposure– With certain limitations, RACs can audit a small
sample of a provider’s records and extrapolate any overpayment finding to the provider’s patient population. RACs will receive their full contingency fee for extrapolated claims. See CMS FAQs No. 9405.
• FCA Liability
Ancillary Documents Relevant to Revenue Integrity Discussion
• Yellow Book Audit Standards– See http://www.gao/govaud/ybko1.htm
• Comprehensive Medicaid Integrity Plan (FYs 2009-2013)
• Medicaid Integrity Program A-Z
• Comprehensive Integrity Review Schedule
• Example: MIC Audit-Entrance Conference Agenda
• Example: MIC Audit-Institutional Provider In-Take Questionnaire

29
Thank you
Questions and Answers
296460459/v1
Sara Kay WheelerPartnerKing & Spalding LLP1180 Peachtree St., NEAtlanta, GA 30309-3521Phone: (404) 572-4685E-mail: [email protected]