review article new models of emergency prehospital care that...
TRANSCRIPT

Hindawi Publishing CorporationThe Scientific World JournalVolume 2013, Article ID 182102, 6 pageshttp://dx.doi.org/10.1155/2013/182102
Review ArticleNew Models of Emergency Prehospital Care ThatAvoid Unnecessary Conveyance to Emergency Department:Translation of Research Evidence into Practice?
Helen Anne Snooks, Mark Rhys Kingston,Rebecca Elizabeth Anthony, and Ian Trevor Russell
Centre for Health Information Research and Evaluation (CHIRAL), Institute of Life Science, College of Medicine, Swansea University,Singleton Park, Swansea SA2 8PP, UK
Correspondence should be addressed to Helen Anne Snooks; [email protected]
Received 21 December 2012; Accepted 15 April 2013
Academic Editors: S. Huckson, E. Lang, and B. Rowe
Copyright © 2013 Helen Anne Snooks et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Background. Achieving knowledge translation in healthcare is growing in importance butmethods to capture impact of research arenot well developed. We present an attempt to capture impact of a programme of research in prehospital emergency care, aiming toinform the development of EMSmodels of care that avoid, when appropriate, conveyance of patients to hospital for immediate care.Methods.Wedescribe the programme and its dissemination, present examples of its influence onpolicy andpractice, internationally,and analyse routine UK statistics to determine whether conveyance practice has changed. Results. The programme comprises eightresearch studies, to a value of >£4m. Findings have been disseminated through 18 published papers, cited 274 times in academicjournals. We describe examples of how evidence has been put into practice, including newmodels of care in Canada and Australia.Routine statistics in England show that, alongside rising demand, conveyance rates have fallen from 90% to 58% over a 12-yearperiod, 2,721 million fewer journeys, with publication of key studies 2003–2008. Comment. We have set out the rationale, keyfeatures, and impact on practice of a programme of publicly funded research. We describe evidence of knowledge translation,whilst recognising limitations in methods for capturing impact.
1. Background
The gap between the production of research evidence andimplementation into routine clinical practice has been wellacknowledged and has been referred to as the second transla-tional gap; the first gap is that between laboratory scienceand clinical research [1]. With increasing recognition of theimportance of not only carrying out research but also ofensuring that research findings are taken up and used bythose making health care policy and providing health care,researchers and research funders are now paying more atten-tion to dissemination, particularly active forms which havethe ability to influence care delivery, and also to capturing theimpact of research [2–4].
In the field of emergency care, research evidence tounderpin care has been criticised both for its scarcity and
quality [5]. In the prehospital setting these concerns areeven more acute [6–8]. Emergency prehospital care is a fieldwithout a strong academic tradition, but patient volume ishigh and outcomes are linked to responses provided by emer-gency medical systems (EMS). In this growing field, demon-strating impact in practice is fundamental to the continuedattraction of research funding, building of research skills andculture, and thus a high-quality evidence based to informfuture policy and practice.
With sustained increases in demand for emergency pre-hospital care across the developed world, current systems areunable to maintain services that traditionally respond to allemergency calls to the ambulance service with a paramedicstaffed patient carrying vehicle travelling on lights and sirens,andwith a default of conveyance to an emergency department(ED) for medical care unless the patient refused to travel.

2 The Scientific World Journal
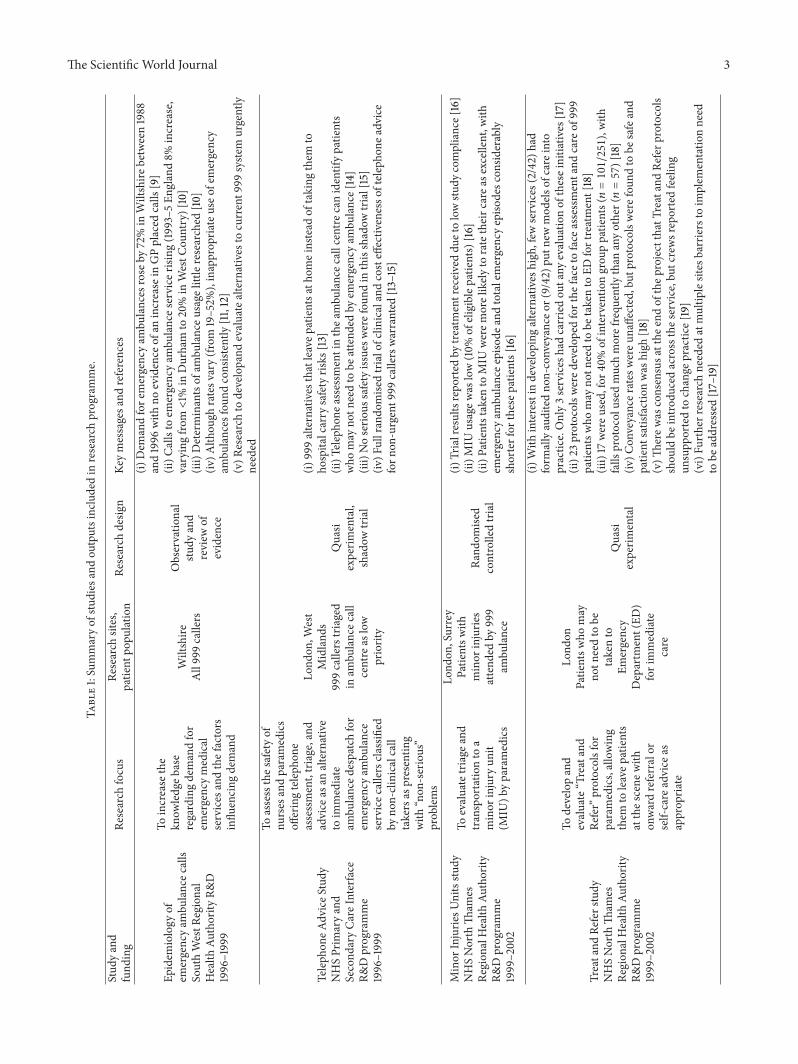
Researches focussing on the needs and outcomes of patientsfor whom emergency (999) calls to the ambulance serviceare made have shown that a substantial proportion of thesepatients (up to 52%) [11, 12, 15, 28] do not need immediatemedical care, but that triage systems at the despatch centreand on scene that identify patients for self- or community-based care carry significant safety risks [15–17, 22]. Unneces-sary transportation can also be an issue for patients who havelittle or no chance of survival [29].
In this paper we describe a programme of research relatedto the development and implementation of new models ofcare that allow ambulance services to offer alternatives tothe traditional response and to safely reduce conveyance ofpatients to ED and present data that demonstrate the impactof this research.
2. Summary of Research Programme
Supported by over £4m in research grants, the programmeof work includes studies that have followed the UK’s MedicalResearch Council’s Framework for the Development andEvaluation of Complex Interventions [30, 31] and comprisesreviews of existing research and practice and experimentalresearch, including randomised controlled trials (Table 1).Research findings indicate and describe the problem [9–13]and then the costs and effectiveness of alternatives to currentpractice [14–19, 22]. Study findings have been widely dissem-inated to generic and specialist audiences through publica-tion in peer reviewed and practitioner journals, as well as atconferences at local, national, and international levels. Theresearch team works closely with prehospital care providersand policy makers in the UK but does not follow a formalknowledge transfer strategic approach.
3. Impact on Policy and Practice:Knowledge Transfer
3.1. Methods. We tracked citations using Google Scholar,undertook extensive electronic searching of policy docu-ments, and gathered ad hoc information related to servicedevelopments in which studies from this programme of workwere cited. We analysed routine national data provided by allindividual services as part of their required performancestatistics for the period before and since publication of find-ings from studies within the programme.
3.2. Results. Papers reported in Table 1 have been cited inacademic journals 274 times to date. An influential systematicreview of 999 alternatives for the UK Department of Health(2005) draws heavily upon the work of the research team andhas gone on to influence guidance emanating from statutoryUK bodies [32–34]. Nontransport (to ED) guidelines fromthe Ambulance Service Association and Department ofHealth, which cite elements of this work, have been widelyadopted, as have “Treat and Refer” protocols.
Enhanced telephone triage has been adopted across theUK ambulance service providers, in line with the recommen-dations of the Department of Health and the Ambulance
Service Association—both of which respond to work pub-lished within this programme. Through correspondence anddesktop reviewswe are aware of similar servicemodels havingbeen adopted internationally, in Canada, for example, and inSouth Australia, where the Ambulance Service was able toreport financial savings following implementation across thestate of Victoria, having cited findings from the TelephoneAdvice Study [13–15], in their business case.
“Prior to 2003 we sent an ambulance to all callsreceived via the “000” ambulance emergency callcentre. Professor Snooks work, including the evi-dence of very high caller satisfaction and very fewadverse events from referrals instead of con-veyance, was used to show the need for a referralservice at point of call. In the year following imple-mentation we were able to show cost savings andhave now fully implemented the service, and themodel is being rolled out across Australia.” SeniorResearch Fellow, Ambulance Victoria, Australia.
“We have used Professor Snooks published work[on pre hospital clinical decision making tools] toinform policies in Nova Scotia and Alberta. Thereare similar challenges being faced in the UK andCanada.” Senior Performance Strategist, AlbertaHealth Services Emergency Medical Services.
Evidence of the impact of the work in prehospital carecan be seen in conveyance rates—90% of emergency calls inEngland resulted in hospital conveyance in 2000 compared to58% in 2012 (see Figures 1 and 2)—equivalent to 2,721 millionfewer journeys.
4. Discussion
4.1. Key Points. Findings from this programme of work haveconsistently highlighted the need for alternatives to routineconveyance of 999 patients to ED and the team have devel-oped, implemented, and tested a range of approaches toimproving and providing evidence about the quality, safety,and cost effectiveness of care.
Working collaborativelywith theNHS and policymakers,lessons from the programme of work have been disseminatedwidely in peer-reviewed articles, policy literature, interna-tional conferences, and through personal invitations to visitservice providers.
Nationally and internationally, evidence from this pro-gramme of work has been cited in policy documents and inservice developments, including the provision of telephoneadvice and Treat and Refer protocols.
In the face of consistent increases in demand for the 999emergency ambulance service in the UK and internationally,we have demonstrated evidence of falling conveyance ratesand an increasing proportion of patients treated at scene inEngland since the publication of our findings.
4.2. Strengths and Limitations. Methods for capturing impactof research are not well developed and include a variety of
The Scientific World Journal 3
Table1:Summaryof
studies
andou
tputsincludedin
research
programme.
Stud
yand
fund
ing
Research
focus
Research
sites,
patie
ntpo
pulatio
nRe
search
desig
nKe
ymessagesa
ndreferences
Epidem
iology
ofem
ergencyam
bulancec
alls
SouthWestR
egional
Health
Authority
R&D
1996–1999
Toincrease
the
know
ledgeb
ase
regardingdemandfor
emergencymedical
services
andthefactors
influ
encing
demand
Wiltshire
All999callers
Observatio
nal
study
and
review
ofevidence
(i)Dem
andfore
mergencyam
bulances
rose
by72%in
Wiltshire
between1988
and1996
with
noevidence
ofan
increase
inGPplaced
calls
[9]
(ii)C
allsto
emergencyam
bulances
ervice
rising(19
93–5
England8%
increase,
varyingfro
m<1%
inDurham
to20%in
WestC
ountry)[10]
(iii)Determinantsof
ambu
lanceu
sage
little
researched
[10]
(iv)A
lthou
ghratesv
ary(fr
om19–52%
),inapprop
riateuseo
femergency
ambu
lances
foun
dconsistently
[11,12]
(v)R
esearchto
developand
evaluatealternatives
tocurrent9
99syste
murgently
needed
Teleph
oneA
dviceS
tudy
NHSPrim
aryand
Second
aryCa
reInterfa
ceR&
Dprogramme
1996–1999
Toassessthes
afetyof
nurses
andparamedics
offeringtelep
hone
assessment,triage,and
advice
asan
alternative
toim
mediate
ambu
lanced
espatchfor
emergencyam
bulance
servicec
allerscla
ssified
byno
n-clinicalcall
takersas
presentin
gwith
“non
-serious”
prob
lems
Lond
on,W
est
Midland
s999callerstriaged
inam
bulancec
all
centre
aslow
priority
Quasi
experim
ental,
shadow
trial
(i)999alternatives
thatleavep
atientsa
thom
einstead
oftaking
them
toho
spita
lcarry
safetyris
ks[13]
(ii)T
eleph
onea
ssessm
entinthea
mbu
lancec
allcentre
canidentifypatie
nts
who
may
notn
eedto
beattend
edby
emergencyam
bulance[14]
(iii)Noserio
ussafetyissuesw
erefou
ndin
thisshadow
trial[15]
(iv)F
ullrando
mise
dtrialofclin
icalandcosteffectiv
enesso
ftelepho
neadvice
forn
on-urgent9
99callerswarranted
[13–15]
Minor
Injurie
sUnitsstu
dyNHSNorth
Tham
esRe
gion
alHealth
Authority
R&Dprogramme
1999–2002
Toevaluatetriage
and
transportatio
nto
aminor
injury
unit
(MIU
)byparamedics
Lond
on,Surrey
Patie
ntsw
ithminor
injurie
sattend
edby
999
ambu
lance
Rand
omise
dcontrolledtrial
(i)Trialresultsrepo
rted
bytre
atmentreceiveddu
etolowstu
dycompliance[16]
(ii)M
IUusagew
aslow(10%
ofeligiblep
atients)[16]
(ii)P
atientstaken
toMIU
werem
orelikely
toratetheirc
area
sexcellent,w
ithem
ergencyam
bulancee
pisode
andtotalemergencyepiso
desc
onsid
erably
shorterfor
thesep
atients[16]
Treatand
Referstudy
NHSNorth
Tham
esRe
gion
alHealth
Authority
R&Dprogramme
1999–2002
Todevelopand
evaluate“Treatand
Refer”protocolsfor
paramedics,allowing
them
toleavep
atients
atthes
cene
with
onwardreferralor
self-care
advice
asapprop
riate
Lond
onPatie
ntsw
homay
notn
eedto
betakento
Emergency
Departm
ent(ED
)forimmediate
care
Quasi
experim
ental
(i)With
interestin
developing
alternatives
high
,few
services
(2/42)
had
form
allyauditedno
n-conveyance
or(9/42)
putn
ewmod
elsof
care
into
practic
e.Only3services
hadcarriedou
tany
evaluatio
nof
theseinitia
tives
[17]
(ii)2
3protocolsw
ered
evelop
edforthe
face
toface
assessmentand
care
of999
patie
ntsw
homay
notn
eedto
betakento
EDfortreatment[18]
(iii)17
wereu
sed,for4
0%of
interventio
ngrou
ppatie
nts(𝑛=101/251),with
falls
protocolused
muchmorefrequ
ently
than
anyother(𝑛=57)[18]
(iv)C
onveyancer
ates
wereu
naffected,but
protocolsw
erefou
ndto
besafeand
patie
ntsatisfactionwas
high
[18]
(v)Th
erew
asconsensusa
tthe
endof
thep
rojectthatTreatand
Referp
rotocols
shou
ldbe
intro
ducedacrossthes
ervice,but
crew
sreportedfeeling
unsupp
ortedto
change
practice[
19]
(vi)Fu
rtherresearchneeded
atmultip
lesites
barriersto
implem
entatio
nneed
tobe
addressed[17–19]

4 The Scientific World Journal
Table1:Con
tinued.
Stud
yand
fund
ing
Research
focus
Research
sites,
patie
ntpo
pulatio
nRe
search
desig
nKe
ymessagesa
ndreferences
Fittobe
Left
NSF
forO
lder
peop
leR&
Dprogramme
2003–2006
Todesig
n,develop,
implem
entand
evaluateatoo
ldesigned
tosupp
ortambu
lance
staff
tomakec
onsistent
andform
alise
ddecisio
nsconcerning
thec
onveyanceo
folder
peop
lewho
have
fallen
Lond
onPatie
ntsa
ged65+
attend
edby
a999
ambu
lance
follo
wingafall
Observatio
nal,
quasi
experim
ental
(i)Patie
ntsleft
atho
meb
ytheira
ttend
ingcrew
follo
wingafallw
erea
thighris
kof
afurther
fall,999attend
ance,E
Dcontactand
deathwith
in2weeks
[20]
(ii)D
ecision
stoleaveo
lder
peop
leatho
mefollowingafallw
erec
omplex
and
multifactorial[21]
Non
serio
us999calls
managed
bynu
rsea
dvise
rsby
teleph
one
NHSServiceD
eliveryand
Organisa
tionR&
Dprogramme,2002–2005
Anevaluatio
nof
the
costs
andbenefitso
ftransfe
rringsomelow
priority999calls
toNHSDire
ctnu
rse
advisersforfurther
assessmentand
advice
SouthWales,
Tham
esVa
lley
Greater
Manchester
999callerswith
prob
lemsa
ssessed
inam
bulancec
all
centre
asno
n-urgent
Rand
omise
dcontrolledtrial
(i)Transfe
rringno
n-urgent
999calls
forfurther
advice
andassessment
provides
asafea
ndcost-
effectiv
eservice
forsom
ecalls[22]
(ii)A
lmosth
alfo
fcallstransfe
rred
werer
eturnedto
thea
mbu
lances
ervice
for
anam
bulancer
espo
nseind
icatingthat,alth
ough
non-urgent,m
anyof
these
calls
arefor
patie
ntsw
honeed
transporto
rsom
eform
offace
toface
assessment[22]
(iii)Fu
rtherresearchrequ
iredtodevelopandevaluatemod
elso
fcarethatsuit
ther
ange
of999callers[22]
Non
conveyance
Wales
Office
ofR&
D,
2004–2006
Explorationof
ambu
lancec
rew
mem
bers’attitudes
towards
clinical
documentatio
nand
non-conveyed
patie
nts
SouthWales
Patie
ntsleft
atho
mefollowingan
attend
ance
byem
ergency
ambu
lance
Qualitative
study,focus
grou
ps
(i)Decision
makingcomplex
fortworeason
s:capacityof
patie
ntstomake
decisio
nsandinpu
tofp
atients,friend
s,family
andam
bulancec
rew[23]
(ii)M
ismatch
betweenpo
licyandpractic
eneeds
tobe
addressedthroug
hresearch
[23]
(iii)Lo
wrateso
fclin
icaldo
cumentatio
nfor9
99patie
ntsn
ottakento
EDpo
sealitigatio
nris
kbu
tthe
processisn
otvalued
byclinicalstaffor
adequately
auditedby
managers[24]
ParamedicPractitioner
Older
Peop
leStud
yTh
eHealth
Foun
datio
n2003–2006
Toevaluatethes
afety,
effectiv
enessa
ndcost
effectiv
enesso
fclin
ical
decisio
nsmadeb
yParamedic
Practitionersop
erating
with
inthen
ewservice
comparedwith
standard
practic
eof
EMStransfe
rand
EDtre
atment
Sheffi
eld999patie
ntsa
ged
65+
Rand
omise
dcontrolledtrial
(i)Patie
ntsintheinterventiongrou
pwerelesslikely
toattend
ED,require
hospita
ladm
issionwith
in28
days,exp
erienced
asho
rter
episo
deof
care
time,
andwerem
orelikely
torepo
rtbeinghigh
lysatisfiedwith
theirc
are,with
nodifferencein28
daymortality[25]
(ii)2
19/2025patie
ntsa
ttend
edED
with
in7days
oftheirind
excall,in
which
16(0.8%)w
erejud
gedto
have
received
subo
ptim
alcare.N
odifferencew
asfoun
din
ratebetweeninterventio
nandcontrolarm
s[26]P
aram
edicsw
ithextend
edskillsc
anprovidea
safe,clin
icallyandcosteffectiv
ealternativetostandard
ambu
lancetransfera
ndtre
atmentinan
EDfore
lderlypatientsw
ithacute
minor
cond
ition
s[25–27]

The Scientific World Journal 5
0
1
2
3
4
5
6
7
8
920
00-0
1
2001
-02
2002
-03
2003
-04
2004
-05
2005
-06
2006
-07
2007
-08
2008
-09
2009
-10
2010
-11
2011
-12
Mil
lio
ns
Total emergency callsEmergency attendances Treated at scene only
Period of publication of
evaluative reports from
work programme
Patient journeys (conveyed)
Figure 1: Ambulance Service Summary Statistics (a), England,2000–2012.
0
10
20
30
40
50
60
70
80
90
100
2000
-01
2001
-02
2002
-03
2003
-04
2004
-05
2005
-06
2006
-07
2007
-08
2008
-09
2009
-10
2010
-11
2011
-12
Total emergency callsconveyed (%)
Period of publication of
evaluative reports from
work programme
Total emergency calls resulting in emergency attendances (%)
Figure 2: Ambulance Service Summary Statistics (b), England,2000–2012.
approaches [35, 36]. In this under researched area, policy doc-uments are often consensual rather than based on evidenceand citation of underpinning research is rare.
In this paper we have described the scope, characteristics,and impact of a research programme in emergency prehospi-tal care. For inferences about impact on practice we have hadto rely on citations and ad hoc reports of service innovationalongside routine statistics related to emergency demand andtreatment. Citations are recognised as a weak indicator of realimpact [36]. Routine data are reliable but observational.
We are conscious that there are other potential causesfor these changes. In an ideal or planned world with multi-ple indicators and well-defined interventions, the statisticaltechnique of interrupted time series can draw stronger con-clusions about cause and impact, as in the Respect trial [37,38]. In the real world inferences about causation are moredifficult.
4.3. Implications. Demonstration of impact of research isincreasingly important in times when resources are scarceand competition is heavy. Research funders and researchersare under pressure to report impact but methods are under-developed. Policy and treatment guidelines often lack trans-parent underpinning research evidence. Measuring impact isour only way of capturing knowledge transfer from researchevidence to patient care.
Against this setting we have attempted to set out therationale, key features, and resulting impact on practice ofa programme of research funded through the public pursein the UK. We argue that findings have been influential atnational and international levels although we recognise thatthe rigour of methods for identifying and attributing impactis not as high as in the traditional “gold standard” RCT.
References
[1] D. Cooksey, A Review of UK Health Research Funding, HMTreasury, London, UK, 2006.
[2] L. A. Bero, R. Grilli, J. M. Grimshaw, E. Harvey, A. D. Oxman,and M. A. Thomson, “Getting research findings into practice.Closing the gap between research and practice: an overview ofsystematic reviews of interventions to promote the implemen-tation of research findings,” British Medical Journal, vol. 317, no.7156, pp. 465–468, 1998.
[3] WorldHealthOrganization,World Report onKnowledge for Bet-ter Health: Strengthening Health Systems, World Health Organi-zation, Geneva, Switzerland, 2004.
[4] S. R. Hanney, M. A. Gonzalez-Block, M. J. Buxton, and M.Kogan, “The utilisation of health research in policy-making:concepts, examples andmethod of assessment,”Health ResearchPolicy and Systems, vol. 1, no. 1, article 2, 2003.
[5] V. Bounes, E. Dehours, V. Houze-Cerfon, B. Valle, R. Lipton,and J. L. Ducasse, “Quality of publications in emergency medi-cine,”American Journal of EmergencyMedicine, vol. 31, no. 2, pp.297–301, 2013.
[6] D.W. Spaite, E. A. Criss, T. D. Valenzuela, and J. Guisto, “Emer-gency medical service systems research: problems of the past,challenges of the future,”Annals of EmergencyMedicine, vol. 26,no. 2, pp. 146–152, 1995.
[7] Sheffield University, “Building the evidence base in pre hospitalurgent and emergency care: a review of research evidence andpriorities for future research,” 2010.
[8] S. Brace and M. Cooke, “What are the priorities for prehospitalresearch?” Journal of Paramedic Practice, vol. 2, no. 11, pp. 502–504, 2010.
[9] H. Wrigley, S. George, H. Smith, H. Snooks, A. Glasper, and E.Thomas, “Trends in demand for emergency ambulance servicesinwiltshire over nine years: observational study,”BritishMedicalJournal, vol. 324, no. 7338, pp. 646–647, 2002.
6 The Scientific World Journal
[10] H. Wrigley, H. Snooks, E. Thomas, H. Smith, A. Glasper, andS. George, “Epidemiology and demography of 999 ambulancecalls: a review,” Pre-Hospital Immediate Care, vol. 3, pp. 94–98,1999.
[11] H. Snooks, H. Wrigley, S. George, E. Thomas, H. Smith, andA. Glasper, “Appropriateness of use of emergency ambulances,”Journal of Accident and Emergency Medicine, vol. 15, no. 4, pp.212–215, 1998.
[12] H. Snooks, S.Williams, R. Crouch, T. Foster, C. Hartley-Sharpe,and J. Dale, “NHS emergency response to 999 calls: alternativesfor cases that are neither life threatening nor serious,” BritishMedical Journal, vol. 325, no. 7359, pp. 330–333, 2002.
[13] H. A. Snooks, J. Dale, C. Hartley-Sharpe, and M. Halter, “On-scene alternatives for emergency ambulance crews attendingpatients who do not need to travel to the accident and emer-gency department: a review of the literature,” Emergency Medi-cine Journal, vol. 21, no. 2, pp. 212–215, 2004.
[14] J. Dale, J. Higgins, S. Williams et al., “Computer assisted assess-ment and advice for “non-serious” 999 ambulance servicecallers: the potential impact on ambulance despatch,” Emer-gency Medicine Journal, vol. 20, no. 2, pp. 178–183, 2003.
[15] J. Dale, S. Williams, T. Foster et al., “Safety of telephone con-sultation for “non-serious” emergency ambulance servicepatients,” Quality and Safety in Health Care, vol. 13, no. 5, pp.363–373, 2004.
[16] H. Snooks, T. Foster, and J. Nicholl, “Results of an evaluationof the effectiveness of triage and direct transportation tominor injuries units by ambulance crews,” Emergency MedicineJournal, vol. 21, no. 1, pp. 105–111, 2004.
[17] H. Snooks, N. Kearsley, J. Dale, and M. Halter, “New modelsof care for 999 callers with conditions that are neither life-threatening nor serious: results of a national survey,” Pre-Hos-pital Immediate Care, vol. 4, pp. 180–182, 2000.
[18] H. Snooks, N. Kearsley, J. Dale, M. Halter, J. Redhead, and W.Y. Cheung, “Towards primary care for non-serious 999 callers:results of a controlled study of “Treat and Refer” for ambulancecrews,”Quality and Safety in Health Care, vol. 13, no. 6, pp. 435–443, 2004.
[19] H. A. Snooks, N. Kearsley, J. Dale, M. Halter, J. Redhead, and J.Foster, “Gaps between policy, protocols and practice: a qualita-tive study of the views and practice of emergency ambulancestaff concerning the care of patients with non-urgent needs,”Quality and Safety in Health Care, vol. 14, no. 4, pp. 251–257,2005.
[20] H. A. Snooks, M. Halter, J. C. T. Close, W. Cheung, F. Moore,and S. E. Roberts, “Emergency care of older people who fall: amissed opportunity,” Quality and Safety in Health Care, vol. 15,no. 6, pp. 390–392, 2006.
[21] M. Halter, S. Vernon, H. Snooks et al., “Complexity of thedecision-making process of ambulance staff for assessment andreferral of older people who have fallen: a qualitative study,”Emergency Medicine Journal, vol. 28, no. 1, pp. 44–50, 2011.
[22] J. Turner, H. Snooks, A. Youren et al., “The costs and benefitsof managing some low-priority 999 ambulance calls by NHSDirect nurse advisers,” Report for National Co-OrdinatingCentre for NHS Service Delivery and Organisation R&D,NCCSDO, 2006.
[23] A. Porter, H. Snooks, A. Youren et al., “‘Should I stay or should Igo?’ Deciding whether to go to hospital after a 999 call,” Journalof Health Services Research and Policy, vol. 12, supplement 1, pp.S1–S1, 2007.
[24] A. Porter, H. Shooks, A. Youren et al., ““Covering our backs”:ambulance crews’ attitudes towards clinical documentationwhen emergency (999) patients are not conveyed to hospital,”Emergency Medicine Journal, vol. 25, no. 5, pp. 292–295, 2008.
[25] S. Mason, E. Knowles, B. Colwell et al., “Effectiveness of para-medic practitioners in attending 999 calls from elderly peoplein the community: cluster randomised controlled trial,” BritishMedical Journal, vol. 335, no. 7626, pp. 919–922, 2007.
[26] S. Mason, E. Knowles, J. Freeman, and H. Snooks, “Safety ofparamedics with extended skills,” Academic Emergency Medi-cine, vol. 15, no. 7, pp. 607–612, 2008.
[27] S. Dixon, S. Mason, E. Knowles et al., “Is it cost effective tointroduce paramedic practitioners for older people to the ambu-lance service? Results of a cluster randomised controlled trial,”Emergency Medicine Journal, vol. 26, no. 6, pp. 446–451, 2009.
[28] S. Thakore, E. A. McGugan, and W. Morrison, “Emergencyambulance dispatch: is there a case for triage?” Journal of theRoyal Society of Medicine, vol. 95, no. 3, pp. 126–129, 2002.
[29] L. J. Morrison, L. M. Visentin, A. Kiss et al., “Validation of arule for termination of resuscitation in out-of-hospital cardiacarrest,”NewEngland Journal ofMedicine, vol. 355, no. 5, pp. 478–487, 2006.
[30] Medical Research Council, “A Framework for developmentand evaluation of RCTs for Complex Interventions to ImproveHealth,” 2000.
[31] P. Craig, P. Dieppe, S. Macintyre, S. Michie, I. Nazareth, and M.Petticrew, “Developing and evaluating complex interventions:the new Medical Research Council guidance,” British MedicalJournal, vol. 337, article a1655, 2008.
[32] Department of Health, Taking Healthcare To the Patient, Trans-forming NHS Ambulance Services, 2005.
[33] Welsh Assembly Government, A Guide to Good Practice: Emer-gency Care: Tools and Techniques to Enable the NHS and SocialServices to Improve the Delivery of Health and Social Care, 2004.
[34] HealthWorkforce Australia,National HealthWorkforce Innova-tion and Reform Strategic Framework for Action 2011–2015, 2011.
[35] P. Davis and P. Howden-Chapman, “Translating research find-ings into health policy,” Social Science and Medicine, vol. 43, no.5, pp. 865–872, 1996.
[36] J. Lavis, S. Ross, C. McLeod, and A. Gildiner, “Measuring theimpact of health research,” Journal of Health Services Researchand Policy, vol. 8, no. 3, pp. 165–170, 2003.
[37] RESPECT trial team, “Effectiveness of shared pharmaceuticalcare for older patients: RESPECT trial findings,” British Journalof General Practice, vol. 60, no. 570, pp. e10–e19, 2010.
[38] RESPECT trial team, “Cost-effectiveness of shared pharmaceu-tical care for older patients: RESPECT trial findings,” BritishJournal of General Practice, vol. 60, no. 570, pp. e20–e27, 2010.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com