review - circulation researchcircres.ahajournals.org/content/circresaha/110/5/749.full.pdf ·...
TRANSCRIPT

Review
Interplay Between Heart and Skeletal Muscle Diseasein Heart Failure
The 2011 George E. Brown Memorial Lecture
Elizabeth M. McNally, Jeffery A. Goldstein
Abstract: The study of single gene disorders often provides insight for more complex human disease. Mutations inthe genes encoding the dystrophin protein complex cause muscular dystrophy and cardiomyopathy bydestabilizing the plasma membrane of skeletal myofibers and cardiomyocytes. In these diseases, progressiveskeletal muscle degeneration and weakness contribute to cardiac dysfunction. Moreover, the pace and pattern ofmuscle weakness, along with onset of cardiomyopathy, is highly variable even when associated with the sameidentical mutation. Using a mouse model of muscular dystrophy and cardiomyopathy, we identified genetic locithat modify muscle pathology and cardiac fibrosis. Distinct genetic modifiers were identified for diaphragm andabdominal musculature, and these genetic intervals differ from those that regulate pathology in the skeletalmuscle of the limbs and the heart. One modifier gene was identified and highlights the importance of thetransforming growth factor-� pathway in the pathogenesis of muscular dystrophy and cardiomyopathy. Wedetermined that canonical transforming growth factor-� signaling contributes to heart and muscle dysfunctionusing a Drosophila model. Together, these studies demonstrate the value of using a genetically sensitized modelto uncover pathways that regulate heart failure and muscle weakness. (Circ Res. 2012;110:749-754.)
Key Words: cardiomyopathy � heart failure � muscular dystrophy � modifiers
The George E. Brown Lecture at the annual ScientificSessions, hosted by the Basic Cardiovascular Sciences
Council, honors Dr Brown’s work as a pioneering physicianscientist. His early investigation into human cardiovascularphysiology focused on the peripheral circulation.1,2 Dr Brownwas the first chair of the Section on Circulation and empha-sized the importance of basic investigation for the AmericanHeart Association’s mission. In the current era, the toolboxfor investigation is considerably more complex and the abilityto carefully delineate molecular pathways responsible forpathophysiology grows each day. The work discussed hereinfocuses on rare genetic disorders that affect both heart andskeletal muscle as cardiomyopathy and muscular dystrophy.Although these diseases are not common in the population,the pathways of myocyte injury and degeneration are broadlyshared in many types of disease. By using animal models thatmirror the human pathophysiology, we are positioned todelineate mechanisms that can be extrapolated more broadlyto heart failure and its management.
The Architecture of Striated MuscleCardiomyocytes and skeletal myofibers share a similar basiccellular architecture. Striated muscle cells are composed of
sarcomeres arranged longitudinally in series, as well as inparallel, to optimize force generation and transmission.Electron-dense Z bands, or Z disks, span the diameter ofstriated muscle cells and attach to the plasma membrane byway of specialized units known as costameres.3,4 Costameresare rib-like structures distributed along the surface of thesarcolemma that link the cytoskeleton to the extracellularmatrix. The dystrophin glycoprotein complex is enriched atcostameres and is positioned to transmit force laterally withrespect to the myocyte’s long axis. Dystrophin, the proteinproduct of the Duchenne Muscular Dystrophy gene, is acytoskeletal protein that binds actin at its amino terminus andalong its rod region. The carboxyl terminus of dystrophinlinks directly to transmembrane proteins that then bindcomponents in the extracellular matrix (Figure 1). Theprimary link between the dystrophin complex and the matrixis through the heavily glycosylated protein, dystroglycan. Thesarcoglycan complex, composed of �, �, �, and � subunits,stabilizes the interaction between � and � dystroglycan,thereby reinforcing the connection from the cytoskeletonthrough the membrane into the extracellular matrix. Auto-somal recessive mutations in the sarcoglycan genes cause thephenotype of muscular dystrophy and cardiomyopathy simi-
Original received December 1, 2011; revision received January 1, 2012; accepted January 3, 2012. In December 2011, the average time fromsubmission to first decision for all original research papers submitted to Circulation Research was 14.29 days.
From the Department of Medicine (E.M.M.), the Department of Human Genetics (E.M.M.), the Committee on Molecular Medicine (E.M.M., J.A.G.),and the Department of Pathology (J.A.G.), The University of Chicago.
Adapted from a presentation delivered at the American Heart Association Scientific Sessions, Orlando, Florida, November 12–16, 2011.Correspondence to Elizabeth M. McNally, University of Chicago, 5841 S Maryland, MC6088, Chicago, IL 60637. E-mail [email protected]© 2012 American Heart Association, Inc.
Circulation Research is available at http://circres.ahajournals.org DOI: 10.1161/CIRCRESAHA.111.256776
749
by guest on June 18, 2018http://circres.ahajournals.org/
Dow
nloaded from

lar to what arises from dystrophin mutations. Disruption ofthe dystrophin complex renders heart and muscle cells sus-ceptible to contraction-induced damage and leads to progres-sive weakness and cardiomyopathy.5,6 Nearly all musclegroups are adversely affected by dystrophin and sarcoglycanmutations including the muscles of the limbs and trunk.Respiratory muscle dysfunction leads to hypoventilation andchronic hypoxia. The combination of respiratory and cardiacmuscle is often lethal for patients with dystrophin andsarcoglycan gene mutations. Overall, the phenotypic constel-lation associated with mutations in dystrophin or �-, �-, or �-sarcoglycan is similar, although there is variation in age ofonset and progression.
Although the internal cellular architecture of cardiomyo-cytes and skeletal myofibers shares similarity, the positioningof cells within the heart or muscle group differs. Skeletalmyofibers are elongated syncytial cells; a single cell mayspan the length of a muscle. Myofibers within normal musclehave a consistent cross sectional area. With muscular dystro-phy, there is degeneration of myofibers accompanied byongoing regeneration. This combination of necrotic myofi-bers alongside newly regenerated myofibers results in fibersize variation within the muscle. Myofibers with the largestdiameter are thought to be more susceptible to contraction-
induced damage. In muscular dystrophy, the robust regener-ation that typifies skeletal muscle is exhausted over time, andthe muscle is replaced by fibrosis leading to scar that can bereadily visualized on MRI. Fatty infiltration of muscle alsooccurs, and this replacement of normal muscle by fibrosis andfat defines muscular dystrophy. In contrast to skeletal myo-fibers, normal cardiomyocytes are small and binucleate. Theintercalated disks that link the short axis of cardiomyocytesare enriched with desmosomal proteins. Lateral attachmentsbetween neighboring cardiomyocytes are less uniform, owingto the circumferential arrangement of cells within the ventricles.Dystrophin and sarcoglycan gene mutations are associated withprogressive loss of cardiomyocytes and replacement of the heartby fibrosis. Therefore, although cardiomyocytes and skeletalmyofibers differ in morphology and alignment, both are suscep-tible to contraction-induced disruption in the absence ofdystrophin.5,6
Evidence for Genetic Modifiers in HumanGenetic DiseaseGenetic modifiers are thought to be important for many singlegene mendelian disorders, and also for more complex geneticdiseases.7,8 Modifiers enhance or suppress the disease processthrough pathways unrelated to the primary defect. There is asingle common SGCG mutation responsible for Limb GirdleMuscular Dystrophy (LGMD) 2C.9 This mutation, 521�T,has been described in LGMD patients from nearly everycontinent, and it is notable is that both mild and severe formsof muscular dystrophy are associated with this same singlemutation.10,11 Individuals with the frame-shifting 521�Tmutation may lose ambulation by the early second decade andhave accompanying cardiomyopathy. Alternatively, individ-uals with the 521�T mutation may remain ambulatory be-yond age 30 and the heart may be spared. Skeletal and cardiacmuscle involvement is not always tightly correlated sincecardiomyopathy may develop independent from skeletal mus-cle weakness. The identification of the single common�-sarcoglycan gene mutation underscores the presence ofmodifier features since the primary mutation, on its own, doesnot entirely predict clinical outcome.
Clinical outcome from genetic disease is modified byenvironmental factors, including exercise and diet, and theseinfluences have been documented for other inherited forms ofcardiomyopathy.12–14 Genetic modifiers are those variantswhich when coinherited either enhance or suppress disease.We developed an animal model of LGMD 2C by deleting the�-sarcoglycan gene, Sgcg, to use mice to search for geneticmodifiers.15 Animal models, particularly mice, are useful formapping modifiers given the consistency from inbred strainsand uniform housing conditions that minimize environmentalinfluences. It is hoped that genetic modifiers identified inmice will translate to human disease. It is possible thatgenetic modifiers for one form of disease will also modifyother genetic forms of cardiomyopathy and muscular dystro-phy, or even nongenetic forms of heart failure and muscleweakness.
Mapping Genetic Modifiers Using Mouse Modelsof Human DiseaseQuantitative trait locus (QTL) mapping is a method to mapgenetic modifiers.8 QTL mapping requires quantitative mea-
Non-standard Abbreviations and Acronyms
BMP bone morphogenetic protein
LGMD limb girdle muscular dystrophy
LTBP latent TGF�-binding protein
QTL quantitative trait locus
TGF transforming growth factor
Figure 1. Architecture of striated muscle. Sarcomeres arearranged in series and in parallel, flanked by Z lines.Costameres are the sarcolemma-associated structures wherethe Z lines efface the plasma membrane. The dystrophin com-plex is enriched at costameres and provides an attachment tothe extracellular matrix.
750 Circulation Research March 2, 2012
by guest on June 18, 2018http://circres.ahajournals.org/
Dow
nloaded from

sures of phenotype, and the genetic analysis need not specifythe mode of inheritance. To map QTLs associated withmuscular dystrophy and cardiomyopathy, we used 2 indepen-dent measures. The first assay quantifies membrane fragilityby measuring Evans blue dye uptake within dystrophicmuscle.16 With disruption of the dystrophin complex, asoccurs in genetic forms of muscular dystrophy and cardio-myopathy, the sarcolemma becomes fragile. The patchynature of dye uptake in dystrophic muscle reflects a nonuni-form injury process. Measuring dye content in the entiremuscle eliminates sample bias that can arise from studyingonly sections of muscles. Additionally, this method is suffi-ciently high throughput and reliable to allow for QTLmapping. The second quantitative assay used for QTL map-ping determined the amount of hydroxyproline per givengram of tissue as a reflection of collagen deposition andfibrosis.16 This determination of fibrosis, like the measure-ment of dye uptake, samples the entire muscle group. Map-ping genetic modifiers in mice often relies on inbred strainsof mice to supply genetic homogeneity.17 If interstrain dif-ferences are sufficient to alter the primary phenotype, thegenetic differences between strains can be used for QTLmapping. Through breeding, the Sgcg null mutation wasintroduced into multiple genetic backgrounds to identifygenetic backgrounds that enhanced or suppressed the pheno-type. The DBA/2J background (D2) was found to increaseboth dye uptake and fibrosis of the Sgcg allele, and otherstrains such as C57Bl6/J and 129/SVemst/J(129) suppressedfibrosis and dye uptake.16
Sgcg mice from the D2 and 129 backgrounds were inter-bred to create an F1 generation. This allowed for mixing ofthe genomes from these 2 background strains. F1 mice wereinterbred with an F2 generation to generate recombinationevents between the 2 background strains. To map modifiers,we examined 80 mice from an F2 intercross between the D2and 129 strains.18 A custom array panel of 330 singlenucleotide variants that differed between the D2 and 129strains was used to identify a region on chromosome 7 thatlinked to membrane leakage. Interestingly, we found that thesame interval on chromosome 7 was also associated withhydroxyproline content supporting that this QTL acts on bothmembrane stability and reactive fibrosis. Within this intervalwe identified the modifier gene as Ltbp4, latent transforminggrowth factor (TGF)� binding protein 4.18
Ltbp4 Is a Modifier of Muscular DystrophyLatent TGF�-binding protein (LTBP)4 is a member of thefibrillin superfamily. The fibrillin superfamily includes 4LTBPs and 3 fibrillins, including FBN1, the gene responsiblefor Marfan syndrome. LTBP4 is highly expressed in heart andskeletal muscle as well as the lung.19,20 Mice deleted forLtbp4 develop pulmonary fibrosis and cardiomyopathy.21 Allmembers of this superfamily are characterized by the pres-ence of multiple epidermal growth factor (EGF) repeatsdistributed along the length of the protein. Interspersed are asmaller number of 8-cystine domains, some of which directlybind TGF�. The amino terminus of LTBP4 directly binds tothe extracellular matrix.22 LTBP proteins, together with thelatent TGF�, form the large latent complex in the extracel-
lular matrix. With injury, locally acting proteases cleaveLTBP4 resulting in the release of TGF� to bind neighboringreceptors. TGF� engagement of its receptor activates bothcanonical and noncanonical TGF� signaling. The Ltbp4 genecontains 39 exons distributed over 34 KB. The proline-richregion of the protein is encoded by exons 11, 12, and 13. Aninsertion/deletion polymorphism within exon 12 of Ltbp4gene was identified that encoded an LTBP4 protein withaltered proteolytic susceptibility.18 This insertion/deletionpolymorphism showed the tightest correlation with mem-brane leakage and fibrosis in quadriceps muscle. We repli-cated this finding in an independent cohort of animals findingthat the Ltpb4 insertion/deletion polymorphism is a modifierof muscle disease and muscular dystrophy.18
TGF� Signaling as a ModifierCanonical TGF� signaling relies on SMAD phosphorylationand SMAD-driven gene transcription. To assess whether theinsertion/deletion Ltbp4 polymorphism resulted in differen-tial SMAD signaling, fibroblasts from the 129 and D2backgrounds were treated with the small latent complex. D2fibroblasts were found to produce more pSMAD2/3 in re-sponse to TGF� exposure than those from the 129 back-ground.18 This difference was detected in both the presenceand absence of the Sgcg allele, indicating that this is aninherent feature of the DBA background and not a strictconsequence of the dystrophic process. Together, these datademonstrate the mechanism of action of the insertion/deletionpolymorphism in Ltbp4 and its capacity to modify musculardystrophy.
LTBP proteins and TGF� are coreleased from secretingcells and then deposited in the matrix.23 In the matrix, theLTBP-TGF� complex lies dormant as the large latent com-plex affixed to the matrix though microfibrils.22,24 The dele-tion allele of Ltbp4 was associated with increased nuclearpSMAD2/3 compared with Sgcg mice with the insertionLtbp4 allele.18 Specifically, pSMAD2/3 was seen in myonu-clear clusters in skeletal and cardiac muscle. Interestingly,these clusters were often seen within the right ventricle. Thismodel suggests that levels of TGF� signaling are critical fordetermining severity of disease. We hypothesize that “hyper-TGF�” signaling may be deleterious, particularly in disorderswhere there is chronic injury and hence chronic and contin-uous activation of TGF� signaling.
TGF� receptors activate both canonical and noncanonicalTGF� signaling, and both signaling pathways are positionedto contribute to pathogenesis. Cohn et al25 used a neutralizinganti-TGF� antibody or the angiotensin receptor blockerlosartan to treat the mdx mouse model of Duchenne MuscularDystrophy and found reduced pSMAD, improved fibrosis,and muscle regeneration. This work parallels what had beenshown using losartan to prevent aortic dilation in a mousemodel of Marfan syndrome.26 More recent studies havesuggested that noncanonical TGF� pathways may be partic-ularly important for the vascular disease in Marfan syndrome,specifically ERK1/2 signaling.27,28 Interestingly, the sameanti-TGF� antibody did not protect against the dilation andfibrosis in the murine heart after transaortic constriction in thepressure-overload model of hypertrophy. In contrast, cardio-
McNally and Goldstein Modifiers for Myopathy 751
by guest on June 18, 2018http://circres.ahajournals.org/
Dow
nloaded from
myocyte-specific deletion of Tgfbr2 was associated withreduced fibrosis and preservation of normal cardiac size aftertransaortic constriction.29 The authors attributed this differ-ence in rescue to noncanonical TGF� signaling, specificallyto TGF�-associated kinase (TAK)-1 and observed that bonemorphogenetic protein (BMP)7 signaling may be important.However, the authors also note that the anti-TGF� antibodymay have insufficient access to myocytes and found thatgenetic ablation of Tgfbr2 more effectively reduced elevatedpSMAD2/3 levels than the anti-TGF� antibody. Therefore,pathogenesis is likely mediated by multiple signaling path-ways as well as critical thresholds of activation.
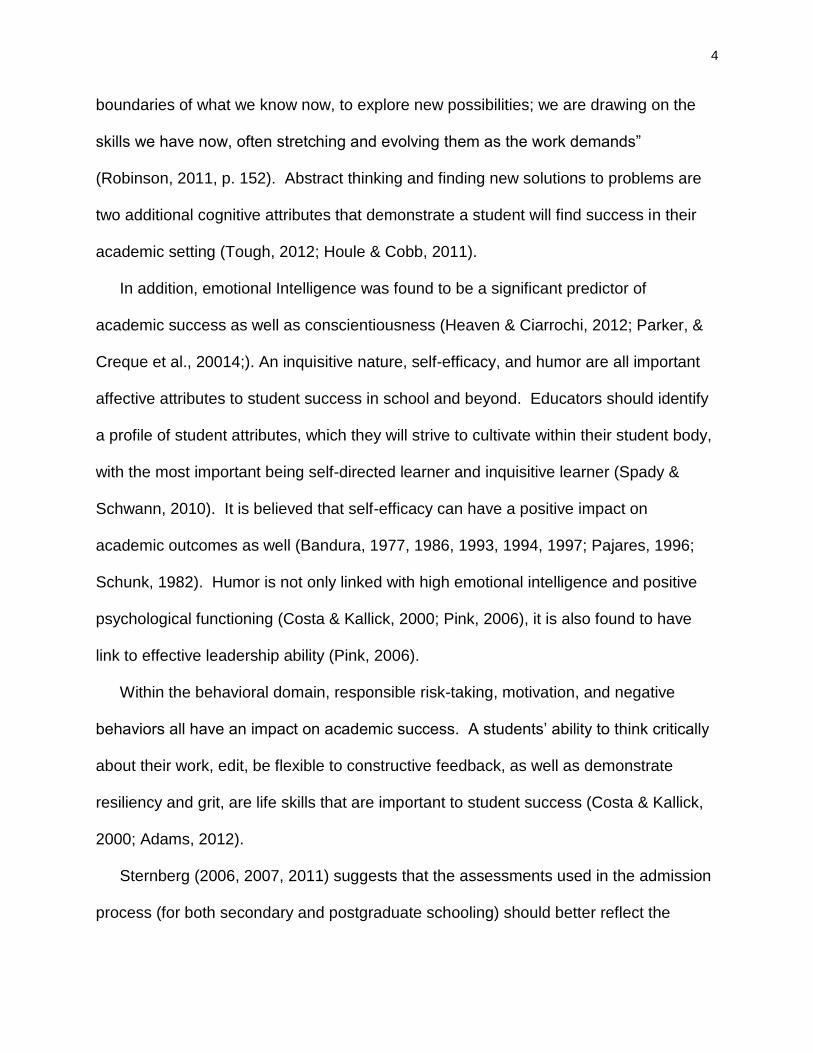
Reducing Canonical TGF� Signaling ImprovesBoth Heart and Muscle FunctionTo investigate whether TGF� signaling is pathogenic, werelied on a Drosophila model of heart and muscle disease.This model was previously generated by deleting the Dro-sophila Sgcd gene using imprecise P element excision.30
Degenerating fly muscle does not become infiltrated byfibroblasts or inflammatory cells, and therefore the features ofthis model may reflect muscle-intrinsic properties. The indi-rect flight muscle in adult Drosophila is composed of 6longitudinally arranged muscles; this muscle displays tearswithin Sgcd null muscle, and such tears are rarely seen inwild-type muscle.30 Sgcd mutant flies allowed ad libitumexercise had larger and more obvious tears within the muscle.Therefore, contraction-induced damage is a feature of theSgcd null muscle similar to what has been noted for mam-malian dystrophic muscle.31 Sgcd mutant flies displayed littleupward walking ability in a 10-second walk test. Sgcdmutants were crossed with an allele in which �-galactosidaseis expressed under the control of a SMAD responsiveenhancer,32 revealing both quantitative and qualitative evi-dence for increased TGF� signaling.31 Myonuclei immedi-ately adjacent to muscle tears had visible �-galactosidaseactivity. When mechanically injured, normal fly muscleshowed increased �-galactosidase activity in those nucleiimmediately adjacent to muscle disruption (Figure 2), indi-cating that hyper-TGF� signaling normally occurs withinmyofibers as a response to injury.
To test whether canonical TGF� signaling was pathogenic,we introduced allele designed to reduce but not eliminatecomponents of the SMAD pathway. We crossed heterozy-gous alleles for Medea (homologous to SMAD4), MAD(SMAD 1/5/8), or Smox (SMAD2/3) each to Sgcd flies.Introducing heterozygous alleles allowed partial reduction ofTGF� signaling.31 We found that reducing the dose of TGF�signaling using a Medea allele improved walking in Sgcd nullflies to normal baseline levels. To ask whether reducingTGF� signaling also improved cardiac function, we analyzedcardiac function in flies. The Drosophila heart tube is a dorsalstructure in the adult fly that beats rhythmically to supply theopen circulatory system. This rhythmic beating and heart tubedimensions can be visualized using optical coherence tomog-raphy. Sgcd flies had a dilated and poorly contractile hearttube characterized by increased end-diastolic and end-systolicdiameters. Reducing SMAD signaling normalized both end-diastolic and end-systolic diameters in mutant flies. Heart
tube function was restored by haploinsufficiency of Medea orSmox but not MAD.31 Interestingly the MAD allele, which ismore important for BMP signaling, did not restore normalcardiac diameters but did restore walking function. Sincegenetic reduction using these alleles is constitutive in all cells,improved walking occurred independent of correcting heartfunction. In this model, improving skeletal muscle function issufficient to improve performance in the walking assay in theabsence of correcting heart tube dysfunction.
Additional Genetic Modifiers for Cardiomyopathyand Muscular DystrophyThe initial search for genetic modifiers in Sgcg mice relied ona subset of 80 animals that showed the most extremephenotypes.18 A genomewide scan was extended to a largernumber of Sgcg null animals (n�280) to search for additionalmodifiers. This analysis confirmed the chromosome 7 mod-ifier containing Ltbp4 as a strong determinant of membranefragility and fibrosis. Nearly 40% of the phenotypic varianceof Evans blue dye uptake was explained by this locus.33
Notably, all limb-based skeletal muscles demonstrated ahighly significant contribution of this locus including thequadriceps, gastrocnemius/soleus, triceps, and gluteus/ham-string muscles. With this same analysis, we identified aregion on chromosome 9 that correlated with cardiac fibro-
Figure 2. Drosophila melanogaster provides a model forstudying heart and muscle function. A, Single Drosophila isshown in cross section highlighting the body components. Theindirect flight muscle (IFM) is the major muscle in the fly and isfound in the thorax. B, Wild-type flies with the dad-lacZ allele,which expresses �-galactosidase under the control of a TGF�-responsive enhancer, were mechanically injured. Those myonu-clei immediately adjacent to the site of injury (arrow) displayincreased �-galactosidase activity (seen as dark staining), indi-cating that TGF� signaling is triggered by normal injury. In Sgcdnull flies, which are a model for cardiomyopathy and musculardystrophy, there is hyper-TGF� signaling. Reducing this signal-ing improves heart and muscle function.31
752 Circulation Research March 2, 2012
by guest on June 18, 2018http://circres.ahajournals.org/
Dow
nloaded from

sis.33 Ongoing efforts are aimed at identifying this gene. Aregion on chromosome 18 correlated with abdominal musclemembrane damage.33 We also identified a region on chromo-some 3 that correlated with both diaphragm muscle fibrosisand abdominal muscle fibrosis providing genetic evidencethat the abdominal muscles contribute to respiratoryfunction.33
Genetic Modifiers Integrate PhysiologyDuring the normal cycle of inspiration and expiration, thediaphragm and abdomen move in concert with each another,34
and respiratory muscle activity can both directly and indi-rectly affect cardiac function. Epaxial muscles (the intercostaland paraspinal muscles) have a distinct developmental origincompared with the hypaxial (limb and abdominal) muscles.35
The diaphragm muscle has a mixed developmental originbecause of its crural and costal aspects. The abdominalmuscles can be viewed as accessory respiratory muscles. Inmuscular dystrophy, abdominal muscle dysfunction occursearly and accompanies decreased respiratory function.36,37
Respiratory dysfunction in muscular dystrophy derives fromprimary pathology in the diaphragm, intercostal and abdom-inal muscles. Hypoventilation and hypoxia trigger increasedpulmonary artery pressure, thereby increasing the workloadof the right ventricle. Thus, chronic hypoxia adversely affectsright ventricular function by elevating pulmonary arterypressures and increasing contraction-induced damaged in theright ventricle. In the Sgcg null mouse model, right ventric-ular cardiomyocyte nuclei were observed with increasedpSMAD2/3 staining,18 consistent with a model where thereare both primary cardiomyocyte defects that are furtherexacerbated by reduced respiratory function.
Heart failure itself, especially in late stages, is associatedwith cachexia. Ablation of the cardiomyocyte myostatin genewas found to prevent skeletal muscle wasting in a pressureoverload model of heart failure.38 These data suggest that theendocrine function of the heart, mediated by myostatin, has asignificant effect on skeletal muscle growth. Other musclegrowth factors such as insulin-like growth factor may also beimportant for cardiac-mediated effects on skeletal musclegrowth. Respiratory function is impeded in a number of statessuch as obesity and chronic lung disease, and therefore inthese settings hypoventilation may contribute significantly tocardiac dysfunction. The similar modifiers affecting dia-phragm and abdominal muscle fibrosis integrate the underly-ing pathophysiology. The role of respiratory muscle functionshould be more carefully considered in other forms ofcardiomyopathy, especially in patients in whom there areoften comorbidities. Together, these findings provide geneticevidence that reinforces what is known from physiologicalstudies. The identification of the genes within the identifiedQTLs will shed further light on the interplay between muscleand heart function and will lead to new pathways to exploitfor diagnostics and therapeutics.
Sources of FundingThis work was supported by the NIH through NHLBI, NIAMS, andNINDS, the Muscular Dystrophy Association and the AmericanHeart Association.
DisclosuresNone.
References1. Brown GE, Sheard C. Measurements on the skin capillaries in cases of
polycythemia vera and the role of these capillaries in the production oferythrosis. J Clin Invest. 1926;2:423–434.
2. Brown GE. Calorimetric studies of the extremities, III: clinical data onnormal and pathologic subjects with localized vascular disease. J ClinInvest. 1926;3:369–390.
3. Pyle WG, Solaro RJ. At the crossroads of myocardial signaling: the roleof Z-discs in intracellular signaling and cardiac function. Circ Res. 2004;94:296–305.
4. Lapidos KA, Kakkar R, McNally EM. The dystrophin glycoprotein com-plex: signaling strength and integrity for the sarcolemma. Circ Res.2004;94:1023–1031.
5. Petrof BJ, Shrager JB, Stedman HH, Kelly AM, Sweeney HL. Dystrophinprotects the sarcolemma from stresses developed during muscle con-traction. Proc Natl Acad Sci U S A. 1993;90:3710–3714.
6. Danialou G, Comtois AS, Dudley R, Karpati G, Vincent G, Des RosiersC, Petrof BJ. Dystrophin-deficient cardiomyocytes are abnormally vul-nerable to mechanical stress-induced contractile failure and injury.FASEB J. 2001;15:1655–1657.
7. Cutting GR. Modifier genes in Mendelian disorders: the example of cysticfibrosis. Ann N Y Acad Sci. 2010;1214:57–69.
8. Zlotogora J. Penetrance and expressivity in the molecular age. GenetMed. 2003;5:347–352.
9. Noguchi S, McNally EM, Ben Othmane K, Hagiwara Y, Mizuno Y,Yoshida M, Yamamoto H, Bonnemann CG, Gussoni E, Denton PH,Kyriakides T, Middleton L, Hentati F, Ben Hamida M, Nonaka I, VanceJM, Kunkel LM, Ozawa E. Mutations in the dystrophin-associated proteingamma-sarcoglycan in chromosome 13 muscular dystrophy. Science.1995;270:819–822.
10. McNally EM, Passos-Bueno MR, Bonnemann CG, Vainzof M, de SaMoreira E, Lidov HG, Othmane KB, Denton PH, Vance JM, Zatz M,Kunkel LM. Mild and severe muscular dystrophy caused by a singlegamma-sarcoglycan mutation. Am J Hum Genet. 1996;59:1040–1047.
11. Kefi M, Amouri R, Driss A, Ben Hamida C, Ben Hamida M, Kunkel LM,Hentati F. Phenotype and sarcoglycan expression in Tunisian LGMD 2Cpatients sharing the same del521-T mutation. Neuromuscul Disord. 2003;13:779–787.
12. Stauffer BL, Konhilas JP, Luczak ED, Leinwand LA. Soy diet worsensheart disease in mice. J Clin Invest. 2006;116:209–216.
13. Konhilas JP, Watson PA, Maass A, Boucek DM, Horn T, Stauffer BL,Luckey SW, Rosenberg P, Leinwand LA. Exercise can prevent andreverse the severity of hypertrophic cardiomyopathy. Circ Res. 2006;98:540–548.
14. McNally EM. Hypertrophic cardiomyopathy: exercise and eat right. CircRes. 2006;98:443–445.
15. Hack AA, Ly CT, Jiang F, Clendenin CJ, Sigrist KS, Wollmann RL,McNally EM. Gamma-sarcoglycan deficiency leads to muscle membranedefects and apoptosis independent of dystrophin. J Cell Biol. 1998;142:1279–1287.
16. Heydemann A, Huber JM, Demonbreun A, Hadhazy M, McNally EM.Genetic background influences muscular dystrophy. NeuromusculDisord. 2005;15:601–609.
17. Keane TM, Goodstadt L, Danecek P, White MA, Wong K, Yalcin B,Heger A, Agam A, Slater G, Goodson M, Furlotte NA, Eskin E, NellakerC, Whitley H, Cleak J, Janowitz D, Hernandez-Pliego P, Edwards A,Belgard TG, Oliver PL, McIntyre RE, Bhomra A, Nicod J, Gan X, YuanW, van der Weyden L, Steward CA, Bala S, Stalker J, Mott R, Durbin R,Jackson IJ, Czechanski A, Guerra-Assuncao JA, Donahue LR, ReinholdtLG, Payseur BA, Ponting CP, Birney E, Flint J, Adams DJ. Mousegenomic variation and its effect on phenotypes and gene regulation.Nature. 2011;477:289–294.
18. Heydemann A, Ceco E, Lim JE, Hadhazy M, Ryder P, Moran JL, BeierDR, Palmer AA, McNally EM. Latent TGF-beta-binding protein 4modifies muscular dystrophy in mice. J Clin Invest. 2009;119:3703–3712.
19. Giltay R, Kostka G, Timpl R. Sequence and expression of a novelmember (LTBP-4) of the family of latent transforming growth factor-betabinding proteins. FEBS Lett. 1997;411:164–168.
McNally and Goldstein Modifiers for Myopathy 753
by guest on June 18, 2018http://circres.ahajournals.org/
Dow
nloaded from

20. Saharinen J, Taipale J, Monni O, Keski-Oja J. Identification and charac-terization of a new latent transforming growth factor-beta-bindingprotein, LTBP-4. J Biol Chem. 1998;273:18459–18469.
21. Sterner-Kock A, Thorey IS, Koli K, Wempe F, Otte J, Bangsow T,Kuhlmeier K, Kirchner T, Jin S, Keski-Oja J, von Melchner H. Disruptionof the gene encoding the latent transforming growth factor-beta bindingprotein 4 (LTBP-4) causes abnormal lung development, cardiomyopathy,and colorectal cancer. Genes Dev. 2002;16:2264–2273.
22. Taipale J, Miyazono K, Heldin CH, Keski-Oja J. Latent transforminggrowth factor-beta 1 associates to fibroblast extracellular matrix via latentTGF-beta binding protein. J Cell Biol. 1994;124:171–181.
23. Saharinen J, Hyytiainen M, Taipale J, Keski-Oja J. Latent transforminggrowth factor-beta binding proteins (LTBPs): structural extracellularmatrix proteins for targeting TGF-beta action. Cytokine Growth FactorRev. 1999;10:99–117.
24. Massam-Wu T, Chiu M, Choudhury R, Chaudhry SS, Baldwin AK,McGovern A, Baldock C, Shuttleworth CA, Kielty CM. Assembly offibrillin microfibrils governs extracellular deposition of latent TGF beta.J Cell Sci. 2010;123:3006–3018.
25. Cohn RD, van Erp C, Habashi JP, Soleimani AA, Klein EC, Lisi MT,Gamradt M, ap Rhys CM, Holm TM, Loeys BL, Ramirez F, Judge DP,Ward CW, Dietz HC. Angiotensin II type 1 receptor blockade attenuatesTGF-beta-induced failure of muscle regeneration in multiple myopathicstates. Nat Med. 2007;13:204–210.
26. Habashi JP, Judge DP, Holm TM, Cohn RD, Loeys BL, Cooper TK,Myers L, Klein EC, Liu G, Calvi C, Podowski M, Neptune ER, HalushkaMK, Bedja D, Gabrielson K, Rifkin DB, Carta L, Ramirez F, Huso DL,Dietz HC. Losartan, an AT1 antagonist, prevents aortic aneurysm in amouse model of Marfan syndrome. Science. 2006;312:117–121.
27. Holm TM, Habashi JP, Doyle JJ, Bedja D, Chen Y, van Erp C, LindsayME, Kim D, Schoenhoff F, Cohn RD, Loeys BL, Thomas CJ, Patnaik S,Marugan JJ, Judge DP, Dietz HC. Noncanonical TGFbeta signalingcontributes to aortic aneurysm progression in Marfan syndrome mice.Science. 2011;332:358–361.
28. Habashi JP, Doyle JJ, Holm TM, Aziz H, Schoenhoff F, Bedja D, ChenY, Modiri AN, Judge DP, Dietz HC. Angiotensin II type 2 receptor
signaling attenuates aortic aneurysm in mice through ERK antagonism.Science. 2011;332:361–365.
29. Koitabashi N, Danner T, Zaiman AL, Pinto YM, Rowell J, Mankowski J,Zhang D, Nakamura T, Takimoto E, Kass DA. Pivotal role of cardio-myocyte TGF-beta signaling in the murine pathological response tosustained pressure overload. J Clin Invest. 2011;121:2301–2312.
30. Allikian MJ, Bhabha G, Dospoy P, Heydemann A, Ryder P, Earley JU,Wolf MJ, Rockman HA, McNally EM. Reduced life span with heart andmuscle dysfunction in Drosophila sarcoglycan mutants. Hum Mol Genet.2007;16:2933–2943.
31. Goldstein JA, Kelly SM, LoPresti PP, Heydemann A, Earley JU,Ferguson EL, Wolf MJ, McNally EM. SMAD signaling drives heart andmuscle dysfunction in a Drosophila model of muscular dystrophy. HumMol Genet. 2011;20:894–904.
32. Tsuneizumi K, Nakayama T, Kamoshida Y, Kornberg TB, Christian JL,Tabata T. Daughters against dpp modulates dpp organizing activity inDrosophila wing development. Nature. 1997;389:627–631.
33. Swaggart KA, Heydemann A, Palmer AA, McNally EM. Distinct geneticregions modify specific muscle groups in muscular dystrophy. PhysiolGenom. 2011;43:24–31.
34. Knight H, Petroll WM, Rochester DF. Relationships between abdominaland diaphragmatic volume displacements. J Appl Physiol. 1991;71:565–572.
35. Ordahl CP, Le Douarin NM. Two myogenic lineages within thedeveloping somite. Development. 1992;114:339–353.
36. D’Angelo MG, Romei M, Lo Mauro A, Marchi E, Gandossini S, BonatoS, Comi GP, Magri F, Turconi AC, Pedotti A, Bresolin N, Aliverti A.Respiratory pattern in an adult population of dystrophic patients. J NeurolSci. 2011;306:54–61.
37. Ugalde V, Walsh S, Abresch RT, Bonekat HW, Breslin E. Respiratoryabdominal muscle recruitment and chest wall motion in myotonicmuscular dystrophy. J Appl Physiol. 2001;91:395–407.
38. Heineke J, Auger-Messier M, Xu J, Sargent M, York A, Welle S,Molkentin JD. Genetic deletion of myostatin from the heart preventsskeletal muscle atrophy in heart failure. Circulation. 2010;121:419–425.
754 Circulation Research March 2, 2012
by guest on June 18, 2018http://circres.ahajournals.org/
Dow
nloaded from

Elizabeth M. McNally and Jeffery A. GoldsteinE. Brown Memorial Lecture
Interplay Between Heart and Skeletal Muscle Disease in Heart Failure: The 2011 George
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 2012 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/CIRCRESAHA.111.2567762012;110:749-754Circ Res.
http://circres.ahajournals.org/content/110/5/749World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Researchin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 18, 2018http://circres.ahajournals.org/
Dow
nloaded from