review of cardiothoracic transplant service in scotland of... · review of cardiothoracic...
TRANSCRIPT

National Services Division
Review of Cardiothoracic
Transplant Service in Scotland
April 2004

Cardiothoracic transplantation review
page 1
Executive SummarExecutive SummarExecutive SummarExecutive SummarExecutive Summaryyyyy
1. National Services Division (NSD) of the Common Services Agency commissions designatednational specialist services and some national screening programmes at an ‘all Scotland’level including cardiothoracic (heart and lung) transplantation services for residents of Scotland.
2. Currently these services are provided from five hospitals in the UK – predominantly fromGlasgow Royal Infirmary and the Freeman Hospital, Newcastle.
3. Following the suspension of the adult heart transplantation service at Glasgow Royal InfirmaryIn February 2000 and its re-establishment in September 2001, NSD was asked by theScottish Executive Health Department to review the provision of the service for residents ofScotland two years after the Glasgow service was re-established. The aim of the review wasto make recommendations on the future pattern of cardiothoracic transplant services requiredto best meet the needs of the people of Scotland, taking into account developing therapies forpeople with severe heart failure.
4. The annual need for cardiothoracic transplantation for residents of Scotland over the next 5-10 years is projected to be around:
• 13-15 adult heart transplants• 8-12 adult heart/lung and lung transplants• 1-2 paediatric heart, heart/lung and lung transplants.
5. The actual number of transplants undertaken will depend on the availability of suitabledonor organs.
6. In addition there are now some complex surgical procedures and mechanical heart assist devicesthat can provide a bridge to or an alternative to, heart transplantation for some people withsevereheart failure. The projected need for these procedures is around:
• 10-15 complex surgery• 5-10 cardiac resynchronisation therapy• 2-5 ventricular assist devices (currently only available within a UK evaluation).
7. Current outcomes achieved for heart transplantation performed in Glasgow for residents ofScotland are comparable with the results achieved throughout the UK. Results for paediatriccardiothoracic transplantation performed in Newcastle and Great Ormond Street and for adultlung transplantation performed in Newcastle are among the best in the UK.
8. The approach adopted to assess the optimum service to meet Scottish needs over the next10 years was to conduct an options appraisal of a range of possible options. The processinvolves a structured assessment of the relative costs and benefits of each option.
9. Seven options were assessed and the option that scored highest in the options appraisalprocess involved:
• retention of adult heart transplantation service in Glasgow but as an integral component ofan extended modern comprehensive advanced heart failure service

Cardiothoracic transplantation review
page 2
• no expansion of the Glasgow service into lung transplantation
• retention of paediatric cardiothoracic transplantation from Newcastle and Great OrmondStreet
• retention of adult lung and heart/lung transplantation from Newcastle, Papworth, andHarefield
• retention of the option of referral to other UK centres such as Manchester for any aspects ofadult cardiothoracic transplantation.
10. The cost of this option is around £3.9 million a year, an increase of £336,000 on currentfunding. This reflects the proposed extension into advanced heart failure.
11. Given the rapid developments in mechanical heart assist devices and the dynamic nature ofhighly specialised servcies such as cardiothoracic transplantation, the review concludes thatstrategic stocktakes of this service should take place every three years.

Cardiothoracic transplantation review
page 3
ContentsContentsContentsContentsContents
EXECUTIVE SUMMARYEXECUTIVE SUMMARYEXECUTIVE SUMMARYEXECUTIVE SUMMARYEXECUTIVE SUMMARY 11111
CONTENTSCONTENTSCONTENTSCONTENTSCONTENTS 33333
1.1.1.1.1. INTRODUCTIONINTRODUCTIONINTRODUCTIONINTRODUCTIONINTRODUCTION 555551.1 Background 51.2 Aim 51.3 Remit 51.4 Methodology 51.5 Plan 6
2.2.2.2.2. LITERALITERALITERALITERALITERATURE REVIEWTURE REVIEWTURE REVIEWTURE REVIEWTURE REVIEW 777772.1. Cardiothoracic transplantation 7
2.1.1 Introduction 72.1.2 Heart transplantation 72.1.3 Example of care pathway 8
2.2 Conditions leading to adult heart transplantation 92.2.1 Cardiomyopathy 92.2.2 Left ventricular dysfunction 92.2.3 Ischaemic heart disease 92.2.4 Congenital heart disease 102.2.5 Heart transplantation volume 11
2.3 Outcomes 122.4 Heart failure 122.5 Heart failure treatment options 13
2.5.1 Pharmacological options 132.5.2 Electrical device therapy 142.5.3 Surgical options 142.5.4 Interventional cardiology 152.5.5 Mechanical circulatory support 16
2.6 Adult lung transplantation 172.6.1 Indications for lung transplantation 172.6.2 Volume of transplantation (lung) 182.6.3 Outcomes (lung) 18
2.7 Adult heart/lung transplantation 192.8 Paediatric cardiothoracic transplantation 20
2.8.1 Paediatric heart transplantation 202.8.2 Paediatric lung transplantation 202.8.3 Paediatric heart/lung transplantation 20
2.9 Volume versus outcome 212.10 Conclusions 22
3.3.3.3.3. EXPECTED NEEDEXPECTED NEEDEXPECTED NEEDEXPECTED NEEDEXPECTED NEED 23232323233.1 Introduction 233.2 Nature of candidate conditions 233.3 Heart failure 243.4 Congenital heart disease 243.5 Cystic fibrosis 243.6 Current provision 25

Cardiothoracic transplantation review
page 4
3.7 Waiting lists 263.8 International comparison 273.9 Alternatives to transplantation 293.10 Projected service need 29
3.10.1 Adult cardiothoracic transplantation 293.10.2 Adult advanced heart failure 303.10.3 Paediatric cardiothoracic transplantation 31
4.4.4.4.4. CURRENT SERVICE FOR RESIDENTS OF SCOTLANDCURRENT SERVICE FOR RESIDENTS OF SCOTLANDCURRENT SERVICE FOR RESIDENTS OF SCOTLANDCURRENT SERVICE FOR RESIDENTS OF SCOTLANDCURRENT SERVICE FOR RESIDENTS OF SCOTLAND 32323232324.1. Interaction with UK Transplant 324.2. Geography & distance in Scotland 334.3. Organ retrieval 334.4. Accommodation & facilities in Glasgow 354.5. Accommodation and facilities in Newcastle 354.6. Proposed advanced heart failure service 364.7 Capacity in English services 36
5.5.5.5.5. PROFESSIONAL & STPROFESSIONAL & STPROFESSIONAL & STPROFESSIONAL & STPROFESSIONAL & STAFF OPINIONAFF OPINIONAFF OPINIONAFF OPINIONAFF OPINION 37373737375.1. Professional & staff opinion 375.2 Professional stakeholders’ response 38
6.6.6.6.6. PAPAPAPAPATIENT/PUBLIC OPINIONTIENT/PUBLIC OPINIONTIENT/PUBLIC OPINIONTIENT/PUBLIC OPINIONTIENT/PUBLIC OPINION 40404040406.1. Introduction 406.2. Focus groups 406.3. Other patient views 416.4. Summary of patient/public views 42
7.7.7.7.7. OUTCOMES/QUALITYOUTCOMES/QUALITYOUTCOMES/QUALITYOUTCOMES/QUALITYOUTCOMES/QUALITY 44444444447.1. Adult heart transplantation 447.2. Adult lung transplantation 457.3. Paediatric heart transplantation 467.4. Paediatric lung transplantation 467.5. Interpretation of data 46
8.8.8.8.8. OPTIONS APPRAISALOPTIONS APPRAISALOPTIONS APPRAISALOPTIONS APPRAISALOPTIONS APPRAISAL 48484848488.1. Options 488.2. Non-financial benefits 498.3. Weighting and scoring the non-financial aspects 518.4. Results 528.5. Conclusion 55
9.9.9.9.9. COSTSCOSTSCOSTSCOSTSCOSTS 56565656569.1. Current expenditure 569.2 benchmarking and costing of options 579.3 Expected future numbers 579.4 Costing of options 589.5 Cost/benefit appraisal 61
10.10.10.10.10. CONCLUSIONSCONCLUSIONSCONCLUSIONSCONCLUSIONSCONCLUSIONS 6363636363
11.11.11.11.11. RECOMMENDARECOMMENDARECOMMENDARECOMMENDARECOMMENDATIONSTIONSTIONSTIONSTIONS 6565656565
Appendix I Membership of review group 66Appendix II Indications for cardiac transplantation candidacy 67Appendix III References 68Appendix IV Focus group feedbackAppendix V Cost profile - Freeman Hospital, NewcastleAppendix VI Cost profile - Glasgow Heart Transplant Unit

Cardiothoracic transplantation review
page 5
1.1.1.1.1. IntroductionIntroductionIntroductionIntroductionIntroduction
1.11.11.11.11.1 BackgroundBackgroundBackgroundBackgroundBackgroundNational Services Division (NSD) of the Common Services Agency commissions cardiothoracic
transplantation services for the residents of Scotland. Currently these services are provided as follows; adultheart transplantation at Glasgow Royal Infirmary and Freeman Hospital, Newcastle, adult lung transplantationat Freeman Hospital and paediatric transplantation for both hearts and lungs at Freeman Hospital and GreatOrmond Street Hospital in London. There is the facility to commission services from the other cardiothoracictransplantation units in England if required.
In 2000 the Glasgow heart transplant unit closed when the surgeon providing the service left suddenly.The patients on the Glasgow waiting list were transferred to the waiting list for Freeman Hospital. Considerableresources and effort were put into re-establishing the unit, including recruiting a new Director for thetransplant programme. In September 2001 the unit was reopened and the then Minister for Health andSocial Inclusion stated that the unit and the service it provides would be reviewed by NSD after a period oftwo years.
1.21.21.21.21.2 AimAimAimAimAimTo make recommendations on the best future pattern of cardiothoracic transplantation services to
meet the needs of the people of Scotland.
1.31.31.31.31.3 RemitRemitRemitRemitRemitTo review current provision of cardiothoracic transplantation services for residents of Scotland in light
of developing treatments for acute heart failure. With this information, to make recommendations to ScottishMinisters on the future pattern of services required to meet the needs of residents of Scotland for highquality, sustainable, accessible, clinically and cost effective cardiothoracic transplantation services.
1.41.41.41.41.4 MethodologyMethodologyMethodologyMethodologyMethodologyThe Nursing and Quality Adviser of NSD was designated to lead the review with the support of the
multidisciplinary team of the Division. A project manager and project support officer from within the Divisionundertook the bulk of the work and were responsible for the operational management of the review.
The review is structured around an option appraisal process of the non-financial benefits. This entailedthe development of a list of possible options for the future delivery of the service and an assessment of theoptions against criteria. A health economist was employed on a consultancy basis to manage the optionsappraisal and a firm specialising in qualitative research was engaged to undertake a series of focus groups aspart of the process of involving patients and the public in the review.
A steering group chaired by Professor John Wallwork, Director of Transplantation at Papworth Hospitalin Cambridgeshire, was established to weight and score the options and to provide expert advice. Thisgroup included patient, surgical, cardiology and managerial representatives (the full list of members isavailable at Appendix I).
The Nursing and Quality Adviser, the project manager and the project support officer from NSD metwith staff from the Glasgow unit to advise them on the review process and the options to be considered. Asmall group of patients also met with NSD staff and comments from both meetings were fed into the reviewprocess to be considered in scoring the options. Views were also sought from past and potential hearttransplant patients via the Glasgow unit, and from cardiologists and respiratory physicians around Scotland.

Cardiothoracic transplantation review
page 6
1.51.51.51.51.5 PlanPlanPlanPlanPlanThe proposed plan for the review group meetings was as follows:
Thursday 9 October 2003 – at this meeting the group was provided with the background to thereview and an explanation of the current service. The group identified and agreed the available options andagreed the criteria on which the options were to be appraised. The group also identified the evidencerequired for each criterion to facilitate scoring.
Tuesday 9 December 2003 – the group weighted the criteria and scored the available options basedon the evidence presented.
Thursday 22 January 2004 – the group revised and agreed the final draft report.
The final report will be submitted to NSAG in May 2004.

Cardiothoracic transplantation review
page 7
2.2.2.2.2. Literature ReviewLiterature ReviewLiterature ReviewLiterature ReviewLiterature Review
2.1.2.1.2.1.2.1.2.1. Cardiothoracic transplantationCardiothoracic transplantationCardiothoracic transplantationCardiothoracic transplantationCardiothoracic transplantation
2.1.1 IntroductionBy 2002 over 61,000 procedures had been performed in over 330 centres worldwide. In the UK over
4,500 patients were registered with the UK Cardiothoracic Audit between April 1995 and March 2003. Ofthese patients, 1,439 went on to have a heart transplant, 946 a lung transplant and 197 a heart/lungtransplant (Rogers et al 2003). The Registry of the International Society for Heart and Lung Transplantation(ISHLT) shows that the number of reported heart transplants in Europe continues to decline (2002). Althoughit is not known for certain, it is thought that this is an actual decline in transplant numbers rather thansimply under reporting.
2.1.2 Adult heart transplantationOver the past two decades heart transplantation has evolved from a rarely performed experimental
procedure to an accepted therapy for patients with end stage congestive cardiac failure (CCF) (Costanzo etal 1995). Despite major developments in the pharmacological management of heart failure, cardiactransplantation remains the most effective treatment for selected patients with end-stage heart failure (Renlundand Taylor 1994).
Most patients being considered for transplantation usually have New York Heart Association class III toIV symptoms with best medical treatment (Renlund and Taylor 2002). Transplantation is appropriate forpatients who require hospitalisation for parenteral medical therapy or mechanical circulatory support orwho have refractory ventricular arrhythmias (Costanzo et al 1995).

Cardiothoracic transplantation review
page 8
Died on Waiting ListTransplant
Good ResponseStable
DeathCardiac or Other
Referred for assessment
Intractable CCF
Currently accepted maximal drug therapy( in a multidisciplinary care setting)
Deteriorating
VAD Not Suitable
Transplant Waiting List
OperativeDeath
Retransplant
DilatedCardiomyopathy
Ischaemic Heart Disease Congenital and OtherDisorders
1Year Survival
3 YearSurvival
Continuedmedicaltherapy
Died
2.1.3 Example of care pathway

Cardiothoracic transplantation review
page 9
2.22.22.22.22.2 Conditions leading to adult heart transplantationConditions leading to adult heart transplantationConditions leading to adult heart transplantationConditions leading to adult heart transplantationConditions leading to adult heart transplantation
2.2.1 CardiomyopathyThe cardiomyopathies can be defined simply as diseases of the myocardium associated with cardiac
dysfunction (Lutton, Ratliff and Young 2002). Some experts feel that the term cardiomyopathy should onlyrefer to a dynamic cardiac muscle process that evolves after myocyte injury of any sort. Over time thedistinction between cardiomyopathy and specific heart disease has become blurred. The World HealthOrganisation has recently revised their classification of the myopathies. The classification now reflects thepathogenesis of the heart muscle disorder. The classification is as follows:
a) Dilated cardiomyopathyDilated cardiomyopathy (DCM) is characterised by myocyte hypertrophy and ventricular chamber
dilation with diminution of systolic function. This is the most common of the cardiomyopathies and accountsfor 44.7% of patients being listed for a heart transplant in the UK between April 1995 and March 1999(Anyanwu, Rogers and Murday 2002).
b) Restrictive cardiomyopathyThis is primarily a diastolic disorder with impairment of ventricular relaxation and filling, usually resulting
from an infiltrative or fibrotic process. The myocyte and its surrounding interstitium can also be affected.
c) Hypertrophic cardiomyopathyHypertrophic cardiomopathy is a syndrome that results in heart failure due to left ventricular outflow
tract obstruction, diastolic cardiac dysfunction, global cardiac ischaemia, dysrhythmias and sudden cardiacdeath. Myocardial hypertrophy and mitral valve abnormalities are gross characteristics of the difficulty withmyocardial histology, revealing cellular hypertrophy and disarray with substantive interstitial fibrosis.Inheritance is seemingly in an autosomal dominant fashion, due to mutations in multiple and differentcontractile protein genes.
d) Right ventricular abnormalitiesArrhythmogenic right ventricular cardiomyopathy is a disorder that primarily affects the right ventricle
and may be the result of uncontrolled apoptosis which is the deletion of cells by fragmentation andphagocytosis.
e) Unclassified cardiomyopathiesThis category includes disorders such as fibroelastosis, noncompacted myocardium and systolic
dysfunction with minimal dilation. These diseases either have features that overlap the other classificationsor do not regularly fit any category.
2.2.2 Left ventricular dysfunctionLeft ventricular dysfunction begins with an injury to the myocardium and is usually a progressive
process, even in the absence of any further injury. The principal manifestation of such progression is aprocess known as remodelling, which occurs in association with homeostatic attempts to decrease wallstress through increases in wall thickness. This ultimately results in changes of the left ventricle such that thechamber dilates, hypertrophies and becomes more spherical. The process of cardiac remodelling generallyprecedes the development of symptoms but continues after their development and may continue despitetreatment (Hunt et al 2002).
2.2.3 Ischaemic heart diseaseIschaemic heart disease defines a disease spectrum of diverse aetiology, with the common factor being
an imbalance between myocardial oxygen supply and demand. This imbalance is usually related to eitheran absolute reduction in coronary blood flow or an inability to increase the blood flow relative to the needsof the heart. It is almost always due to narrowing of the lumen of one or more major coronary arteries byatheroma, often with complete occlusion (Anderson 1985). Ischaemic heart disease accounted for 38.1%

Cardiothoracic transplantation review
page 10
of patients listed for heart transplant in the UK between April 1995 and March 1999 (Anyanwu, Rogers andMurday 2002). It can present as:
a) Angina pectorisSevere chest pain brought on by factors that increase the work of the heart. Angina usually first occurs
during physical exertion or emotional distress which make the heart work harder and increase its need foroxygen (Warnica 2003). If the artery is narrowed enough (usually by more than 70%), angina can occureven at rest when the heart’s demands are at a minimum. Unstable angina refers to angina in which thepattern of symptoms change. The attacks may become more severe, occur more frequently or with lessexertion. Such changes usually signal a rapid progression of coronary artery disease, with an increasingnarrowing of the coronary artery (White 2002). The risk of myocardial infarction is high with this condition.
b) Myocardial infarction (MI)Occurs when some of the heart blood supply is suddenly and severely reduced or cut off, causing the
heart muscle to die. Coronary atheroscelotic disease is the underlying cause in nearly all patients with acuteMI (Warnica 2003). An atheroma may rupture or tear, narrowing the artery further or blocking it with a clot.The ruptured atheroma not only reduces the flow of blood but also exposes subendothelial matrix elements(such as collagen, which stimulates platelet activation and thrombus formation)(Topol and Van de Werf2002). Uncommonly, an MI results when a blood clot forms in the heart itself, breaks away and lodges in acoronary artery or a spasm of a coronary artery stops the blood flow. The heart’s ability to keep pumpingafter an MI is directly related to the extent and location of dead or damaged tissue. Dead tissue is eventuallyreplaced with scar tissue that does not contract. If more than half of the heart muscle is damaged severedisability or death is likely. Even if the damage is less severe the heart may not be able to function adequatelyso that heart failure develops.
c) Sudden deathUsually from ventricular fibrillation, which is an uncoordinated series of very rapid, ineffective contractions
of the ventricles caused by many chaotic electrical impulses. The ventricles quiver instead of contracting ina coordinated manner so that no blood is pumped from the heart. It is fatal unless treated immediately. Themost common cause of ventricular fibrillation is inadequate blood flow to the heart muscle.
d) Heart failureThis is a disorder in which the heart pumps inadequately, leading to a reduction in blood flow, congestion
of blood in the veins and lungs and other changes that may further weaken the heart. This is discussed indetail below.
e) Cardiac arrhythmias(Or abnormal heart rhythms) are sequences of heartbeats that are irregular - either too fast, too slow
or conducted via an abnormal pathway through the heart. The most common causes of arrhythmias arecoronary heart disease, heart valve disorders and heart failure (Mitchell 2003). They can also be caused bysome drugs or by anatomic heart defects present at birth. Arrhythmias have consequences that range fromharmless to life threatening.
Other coronary artery lesions causing ischaemic heart disease are uncommon. They include the lesionsof polyarteritis nodosa, embolism and narrowing of the mouths of the coronary arteries by syphilitic aortitis.
See appendix II for indications for cardiac transplantation candidacy.
2.2.4 Congenital heart diseaseOf the patients listed for heart transplant in the UK between April 1995 and March 1999 only 6.2%
were due to congenital heart disease (Anyanwu, Rogers and Murday 2002). Congenital heart malformationsremain one of the most common birth defects with a live born prevalence of approximately 8 per 1000 livebirths in Western countries (Freedom and Nykanen 2002). Surgery can often palliate even the most aberrantcardiac anatomy, and frequently gives the child several years before a transplant is needed. With paediatric
Cardiothoracic transplantation review
page 11
transplantation, more children are listed for structural congenital heart defects than for the paediatriccardiomyopathies. It has been estimated that up to 10-20% of all children with congenital heart disease willrequire a heart transplant at some point in their lives (Mendeloff 2002). There are no absolute anatomiccontra-indications for cardiac transplantation (Kickuk-Chrisant 2002). The most written about condition ishypoplastic left heart syndrome (HLHS). HLHS comprises 7.5% of all symptomatic cardiac defects and is thefourth most frequent congenital defect producing symptoms in the newborn (Mendeloff 2002).
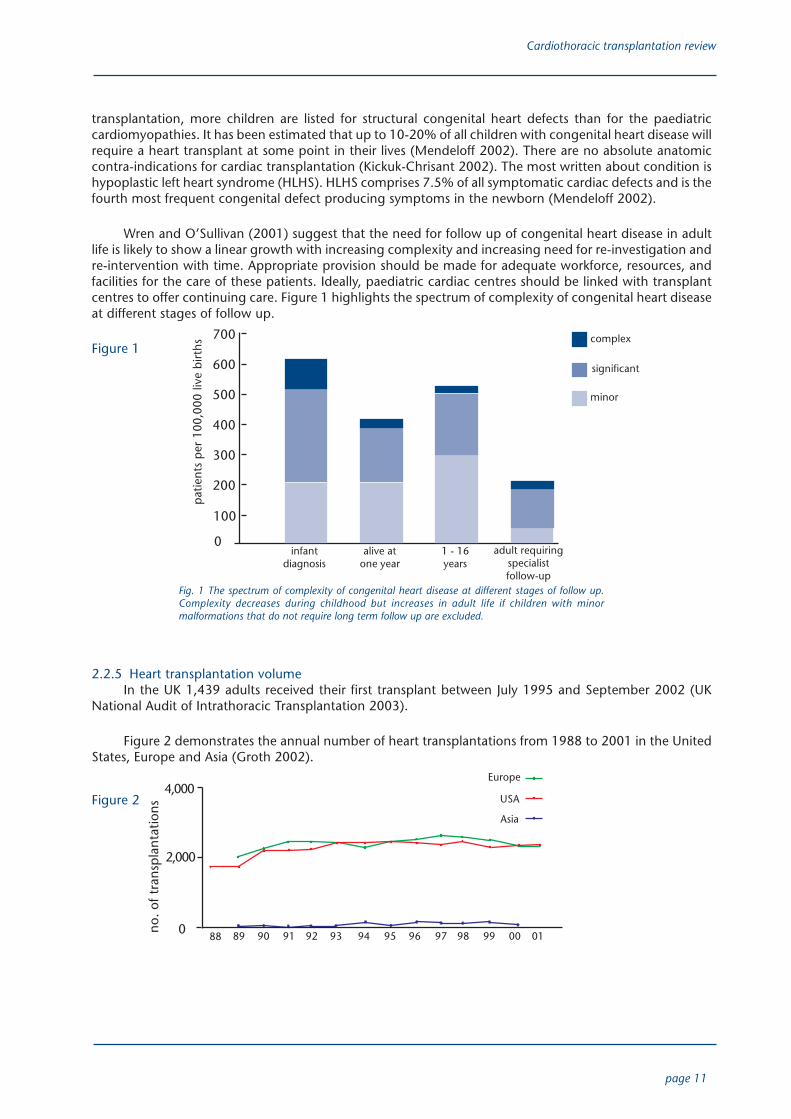
Wren and O’Sullivan (2001) suggest that the need for follow up of congenital heart disease in adultlife is likely to show a linear growth with increasing complexity and increasing need for re-investigation andre-intervention with time. Appropriate provision should be made for adequate workforce, resources, andfacilities for the care of these patients. Ideally, paediatric cardiac centres should be linked with transplantcentres to offer continuing care. Figure 1 highlights the spectrum of complexity of congenital heart diseaseat different stages of follow up.
Figure 1
2.2.5 Heart transplantation volumeIn the UK 1,439 adults received their first transplant between July 1995 and September 2002 (UK
National Audit of Intrathoracic Transplantation 2003).
Figure 2 demonstrates the annual number of heart transplantations from 1988 to 2001 in the UnitedStates, Europe and Asia (Groth 2002).
Figure 2
minor
patie
nts
per
100,
000
live
birt
hs
700
600
500
400
300
200
infantdiagnosis
alive atone year
1 - 16years
adult requiringspecialistfollow-up
complex
significant
Fig. 1 The spectrum of complexity of congenital heart disease at different stages of follow up.Complexity decreases during childhood but increases in adult life if children with minormalformations that do not require long term follow up are excluded.
4,000
2,000
no. o
f tra
nsp
lant
atio
ns
88 89 90 91 92 93 94 95 96 97 98 99 00 01
100
0
0
USA
Europe
Asia

Cardiothoracic transplantation review
page 12
2000 2005 2010 2020
Individuals
Survive incidenthospitalisation*
140
120
100
80
60
40
20
0
2.32.32.32.32.3 OutcomesOutcomesOutcomesOutcomesOutcomesData from the Registry of the International Society for Heart and Lung Transplantation provides
information on over 55,000 heart transplants worldwide. Actuarial survival over the past two decades showsa patient half-life of nine years and a conditional half-life of 12 years (Grover et al 2003). Risk factors for oneyear mortality in adult heart transplantation include pre-operative ventilator dependence, prior hearttransplantation, congenital heart disease as the indication, pre-operative ventricular assist or intra-aorticballoon pump dependence, use of a female donor in a male recipient and increasing donor ischaemic time.At one-year follow up, the majority of deaths are because of infection and acute rejection. By five years themajority of deaths are secondary to chronic rejection, malignancy and non-specific forms of graft failure.
2.42.42.42.42.4 Heart failureHeart failureHeart failureHeart failureHeart failureIt has been estimated that in the year 2000 there were 45,000 women aged 45 years or over and
40,000 men aged 45 years or over within the Scottish population who required treatment for heart failure(Stewart et al 2003). It has been suggested that the number of people with chronic symptomatic heartdisease is increasing. This can be linked to the fact that that the proportion of elderly people in the populationis rising rapidly and that this group has the highest incidence of heart disease and also that survival inpatients with heart disease is improving. Stewart et al (2003) anticipate that by 2020 the total number ofindividuals requiring treatment will have risen to 105,000. This figure allows for demographic changes inthe Scottish population but assumes little or no change in the prevalence of heart failure. See Figure 3 forprojected burden of heart failure in Scotland.
Summary of the projected burden of heart failure in Scotland, 2000 to 2020Figure 3
Estimated individuals with heart failure and general practitioner visits specific to year.*Figures reflect accumulated number in the previous fiveyears (for example, total number of patients who survived an incident hospital admission 2006 to 2010). ‘All hospitalisation’ refers to incident(‘first ever’) and other hospital discharges with heart failure as the principal coding (Stewart 2003).
Heart failure is a complex syndrome that can result from any structural or functional cardiac disorderthat impairs the ability of the left ventricle to fill with or eject blood. The main symptoms of heart failure areshortness of breath and fatigue which may limit exercise tolerance, and fluid retention which may lead topulmonary and peripheral oedema (Hunt et al 2002). Coronary artery disease is the underlying cause ofheart failure in approximately two thirds of patients with left ventricular systolic dysfunction.
The majority of patients with symptomatic left ventricular dysfunction are treated with a combinationof four types of drugs; a diuretic to increase urine formation and decrease fluid volume throughout thebody; an angiotensin converting enzyme (ACE) inhibitor which reduces blood pressure by lowering theblood levels of the hormones angiotensin ii and aldosterone, causing blood vessels to dilate and the kidneys
140
120
100
80
60
40
20
0
Men Women
GP visits perannum
Allhospitalisation*
2000 2005 2010 2020
000s
000s

Cardiothoracic transplantation review
page 13
to excrete more urine, a beta-adrenergic blocker which slows the heart rate and reduces the force of heartcontractions, and usually digitalis which slows the heart and increases the force of each heart contraction.(Hunt et al 2002). Beta-blockers used to be avoided in treating heart failure and they may initially worsensymptoms, however, by blocking the hormone norepinephrine they produce long-term improvement inheart function and survival (Arnold 2003).
The majority of patients with heart failure respond favourably to pharmacological and non-pharmacological treatment and enjoy a good quality of life and enhanced survival. However there are somepatients who, despite maximal treatment, do not improve or continue to decline. These patients often havesymptoms such as fatigue and shortness of breath with minimal exertion or at rest. They are unable toperform most activities of daily living and require intensive management.
These patients should be considered to have refractory heart failure and should be considered forspecialised treatment options such as mechanical circulatory support, continuous intravenous inotropictherapy, referral for heart transplantation or hospice care.
2.52.52.52.52.5 Heart failure treatment options Heart failure treatment options Heart failure treatment options Heart failure treatment options Heart failure treatment optionsThe options for the patient with heart failure who may have progressed to transplantation have changed.
Trials of angiotensin converting enzyme inhibitors in advanced heart failure indicate that up to 90% ofpatients are alive a year after starting treatment (Anyanwu and Treasure 2003). Furthermore, surgicalalternatives to transplantation such as implantable ventricular assist devices are continuing to be developed.
2.5.1 Pharmacological options
a) To achieve improvement in symptoms
· Diuretics - these increase the excretion of sodium and water by the kidneys, thereby providingsymptomatic relief from the symptoms of heart failure, particularly oedema. They remain the first line oftreatment for heart failure but there is no evidence that they improve prognosis.
· Digoxin - this drug increases the force of the contraction of the heart muscle and reduces theconductivity and hence the rate of the heart.
· ACE inhibitors - angiotensin converting enzyme inhibitors work on the natural chemicals in the bodythat are involved in regulating blood pressure. The most important of these is angiotensin ii, which isresponsible for narrowing blood vessels and raising blood pressure. Angiotensin ii is produced in the bodyby the conversion of another chemical, angiotensin i. ACE inhibitors work by blocking the action of theenzyme that makes this conversion and so lowers blood pressure and reduces the strain on the heart.
b) To achieve improvement in survival
· ACE inhibitors - in lowering blood pressure and reducing the work of the heart, not only are thesymptoms of fatigue and breathlessness improved but hopefully survival is increased as well.
· Beta-blockers - these block the beta-adrenoreceptors in the heart, peripheral vasculature, bronchi,pancreas and liver. They work by blocking the action of noradrenaline at receptors in arteries and heartmuscle. Noradrenaline is a chemical that transmits messages between nerves and muscles or between oneset of nerves and another. By blocking its action, beta-blockers can cause arteries to widen, slow the actionof the heart and decrease its force of contraction. This results in a fall in blood pressure and reduced work bythe heart.
· Oral nitrates plus hydralazine - these drugs are vasodilators that act in heart failure by either dilatingthe arterioles, which decreases peripheral vascular resistance and left ventricular pressure, or by venousdilation which decreases the venous return to the heart.

Cardiothoracic transplantation review
page 14
Move to use of beta-blockers in treatment of heart failureIn heart failure, there is a drop in cardiac output that leads to decreased organ perfusion, a compensatory
increase in activity in the sympathetic nervous system and the subsequent release of neurohormones suchas noradrenaline. This in turn stimulates ventricular contraction and increases vascular resistance, therebyincreasing cardiac output and blood pressure (Foody et al 2002). Although this increase in sympatheticactivity is a compensatory response to the failing heart, the continuous pressure on the heart leads topotentially deleterious effects.
Although the short-term effects of beta blockers may result in a temporary exacerbation of symptoms,their long-term effects are uniformly beneficial (Jessup and Brozena 2003). The long-term mechanical stressin conjunction with cardiac fibrosis and necrosis promoted by noradrenaline contributes to cardiac remodelling(a process by which mechanical, neurohormonal and possibly genetic factors alter ventricular size, shapeand function (Jessup and Brozena 2003)) and a dilated, less contractile ventricle. This can lead to a poorprognosis. Long-term treatment with beta-blockers has been shown to reverse the deleterious changesassociated with remodelling and to lead to improved haemodynamics (Foody et al 2002).
2.5.2 Electrical device therapy
a) Cardiac resynchronisation therapy (CRT)Cardiac resynchronisation therapy is a pacemaker-based approach to the treatment of patients with
heart failure who have myocardial conduction system delay. A percutaneous, three-lead biventricularpacemaker system is used. One lead is placed in the right atrium, one in the right ventricle, and a third ispassed through the right atrium, through the coronary sinus, and into a cardiac vein on the lateral wall ofthe left ventricle.
Beneficial effects include reverse remodelling resulting in decreased heart size and ventricular volumes,improved ejection fraction and decreased mitral regurgitation. Clinical improvements in exercise tolerance,quality of life, and the rate of hospitalization have been recorded. To date, however, resynchronisationtherapy has not been shown to enhance survival (Jessup and Brozena 2003).
b) Implantable cardioverter defibrillator (ICD)An implantable cardioverter defibrillator is a device that monitors and if necessary corrects episodes of
rapid heartbeat. Implantation can be performed under local anaesthetic supplemented with intravenoussedation. ICDs are implanted via the subclavian, axillary or cephalic veins. ICDs should be considered forpatients who have episodes of cardiac arrest or haemodynamically significant sustained ventricular tachycardiathat is not due to a reversible cause and for patients who have coronary artery disease, left ventriculardysfunction, and in whom non-sustained ventricular tachyarrhythmias can be induced during electrophysiologic testing.
Randomised controlled trials have demonstrated the superiority of the cardioverter defibrillator overantiarrhythmic drug treatment in patients with serious ventricular arrhythmias. Trials on the impact of ICDson overall survival still need to be completed (Pinski and Peng-Sheng 2003).
2.5.3 Surgical options
a) DorSurgical restoration of left ventricular size and shape in patients with an akinetic scar or dyskinetic
aneurysm resulting from a myocardial infarction and leading to CHF is widely accepted. Results are goodand largely predictable because the remote, non-infarcted segments often retain normal function.Endoventricular patch plasty repair, as proposed by Dor, combined with septal exclusion when necessary,seems to offer some advantages over traditional linear repair. Investigators have documented good midtermresults, with both clinical and functional improvements (Alfieri, Maisano and Schreuder 2003).

Cardiothoracic transplantation review
page 15
b) Coronary artery bypass graft surgery (CABG)The number of patients with coronary artery disease and CHF in whom coronary revascularisation
alone is effective in reversing remodelling is quite limited. CABG is indicated only when the extension of thehibernating areas is such that a significant impact on global left ventricular function is expected. In theabsence of significant areas of viability, surgery is not usually indicated unless the patient has severe leftventricular dysfunction with dyspnoea and angina, when CABG is recommended (Alfieri, Maisano andSchreuder 2003).
c) Correction of mitral valve regurgitationCorrection of mitral valve regurgitation is expected to reverse remodelling over time by abolishing
chronic left ventricular overload. Although the benefits of mitral valve surgery in patients with CHF and alow left ventricular ejection fraction are probably limited in the long term because of the underlyingcardiomyopathy, the hospital mortality, considering the high-risk status of these patients, is low and short-term results are good. In a recent report from the University of Michigan, the overall operative mortality was5% in a series of 92 patients. The actuarial survival rate was 80% at 1 year and 70% at 2 years.
d) Passive containmentPreviously a conditioned skeletal muscle was wrapped around the ventricle to prevent further stress
but this was a complex operation with a high mortality and was abandoned. However, patients who survivedexperienced some clinical improvement so that the concept of diastolic supports remains valid. A newsurgical option has been proposed for selected patients with CHF. This would involve passive containmentof the heart using a special fabric net. The operative mortality is around 10% but consistent improvement inventricular function, stable over time, with some evidence of reverse remodelling at six months has beenreported (Alfieri, Maisano and Schreuder 2003).
e) Surgical restoration of the left ventricle (Batista et al)This operation consists of reducing the volume of the left ventricle, usually obtained by wide resection
of the lateral free wall of the ventricle. The rationale for the operation is to restore a normal ratio betweenthe wall thickness and the radius of the left ventricle to normalise the systolic wall stress. Clinical short-termresults appeared promising, but the operative mortality was high at 10% - 25% and selection criteria werenever fully established so that outcome was difficult to predict. Because of the inability to predict outcome,investigators concluded that this operation was not a reliable option to heart transplantation in Westerncountries but deserved further investigation in other cultural and social settings (Alfieri, Maisano and Schreuder2003).
2.5.4 Interventional cardiologyPercutaneous transluminal coronary angioplasty (PTCA) is an invasive procedure performed to reduce
or eliminate blockages in the coronary arteries. The goal of PTCA is to restore blood flow to blood-deprivedheart tissue, reduce the need for medication, and eliminate or reduce the number of attacks of angina. Thearteries are accessed through a needle puncture that is usually made into the femoral artery in the groin.
Opening a blockage or a plaque in a coronary artery typically involves the use of an angioplastyballoon. When the blockage has calcified or is so dense that a balloon cannot be placed, other devices areused. Plaque can be cut out, vaporized with a laser, or bored out with a surgical drill bit. Often a stent isimplanted after angioplasty to keep the artery open and prevent restenosis (cardiologychannel.com 2003).
The stent is implanted on an angioplasty balloon. When the balloon is deflated and withdrawn, thestent is left in place. Within a few weeks the natural lining of the artery grows over the metallic surface of thestent. A new type of stent, the drug eluting stent (DES) has recently been approved for use in Europe. Thisis basically a bare metal stent that is coated with a slow to moderate-release drug, sometimes inbedded ina polymer. It is hoped that the drugs will prevent or at least reduce restenosis. Two types of drugs arecurrently being used - an immunosuppressive agent, sirolimus, and a chemotherapeutic drug, paclitaxel.Both have proven effective in clinical trials (angioplasty.org 2003).

Cardiothoracic transplantation review
page 16
2.5.5 Mechanical circulatory supportMechanical circulatory support (MCS) devices are mechanical pumps that take over the function of
the damaged ventricle and restore normal haemodynamics. These devices are useful in two groups ofpatients. The first group consists of patients who require ventricular assistance to allow the heart to rest andrecover its function, and the second group are patients with myocardial infarction, acute myocarditis, orend-stage heart disease who are not expected to recover adequate cardiac function and who requiremechanical support as a bridge to transplantation (Goldstein, O.Z. and Rose 1998). The available ventriculardevices include intra-aortic balloon pump (IABP), extracorporeal membrane oxygenation (ECMO),univentricular and biventricular extracorporeal nonpulsatile devices and the total artificial heart.
a) Intra-aortic balloon pumpThe IABP is the most widely used MCS system in the world today. The 40 to 60ml balloon is attached
to the tip of a catheter, which is inserted into the common femoral artery and then advanced to the descendingthoracic aorta. Optimal device function depends on satisfactory timing of the balloon cycle and is sub-optimal in the presence of arrhythmias. The IABP cannot be used in patients with atherosclerotic or aneurismaldisease of the thoracic aorta or significant aortic regurgitation (Delgado 2003).
b) Extra corporeal membrane oxygenationThe concept of prolonged support with extra corporeal gas exchange developed from the success of
cardiac bypass in cardiac surgery. A pump ensures continuous flow of blood through the oxygenator andback to the patient. Roller pumps are most commonly used. As the effects of negative pressure in the rightatrium could be potentially dangerous and risk air entrapment, the venous drainage needs to be passive.The silicone membrane oxygenator was the cornerstone of this therapy for many years. Recently a hollow-fibre alternative has become available in Europe that has some advantages so that ECMO is now known asextra corporeal life support (ECLS) (Walker, Liddell and Davis 2003).
c) Ventricular assist devices (VADs)Technological advances in miniaturisation have resulted in the development of electrically powered,
wearable devices that in some cases allow the patient to leave hospital and resume an independent existence.A UK evaluation of VADs as a bridge to transplantation is underway to ascertain whether they improvesurvival. Mechanical circulatory support tends to reverse the complex systemic abnormalities that characterisethe body’s response to heart failure. Renal and hepatic dysfunction is often reversed, and neurohormonalactivation returns to normal levels. As a result, patients are generally restored to NYHA functional class Iwhile awaiting transplantation and this may enhance their long-term post-transplant survival. Bridging totransplantation is indicated for transplant candidates whose haemodynamic status deteriorates despitemaximal pharmacological therapy or IABP assistance (Delgado 2003).
Figure 4
A wearable left ventricular assist device and its components. The inflow cannula is inserted into the apex of the left ventricle, and the outflowcannula is anastomosed to the ascending aorta. Blood returns from the lungs to the left side of the heart and exits through the left ventricularapex and across an inflow valve into the pumping chamber. Blood is then actively pumped through an outflow valve into the ascending aorta.The pumping chamber is placed within the abdominal wall. One transcutaneous line carries the electrical cable and air vent to the batterypack and electronic controls, which are worn on a shoulder holster or belt (Goldstein 1998).

Cardiothoracic transplantation review
page 17
A number of patients have now undergone removal of their VAD after a prolonged period and havehad a sustained improvement in their cardiac function and symptoms. So far the number of patients inwhich VADs have been used as a bridge to recovery is small. In a group of 16 patients in Texas who requiredtheir VAD to be removed for either infection or device failure, 10 responded favourably, and seven havesurvived long-term (Delgado 2003). At Harefield the use of VADs as a bridge to recovery has been used incombination with a selective β2 receptor antagonist clenbuterol (the Harefield protocol) to sustain the reverseremodelling experienced with the VAD (Jimmy and Yacoub 2003).
In the recent randomised Evaluation of Mechanical Assistance for the Treatment of Congestive HeartFailure (REMATCH) trial, 129 patients with symptoms whose severity resembled those for transplantationrecieved a VAD. The assist devices decreased mortality by 48% over two years. The improvement in survivalwas greater for patients receiving intravenous inotropic therapy.
VADs have been used in over 3,500 patients as a bridge to transplantation with over 50% of recentimplantable device recipients being discharged home. Although some patients have demonstrated majorrecovery, fewer than 10% of patients have demonstrated sufficient recovery of left ventricular functionwithin 3-6 months to undergo device explantation (Stevenson and Rose, 2003).
2.62.62.62.62.6 Adult lung transplantationAdult lung transplantationAdult lung transplantationAdult lung transplantationAdult lung transplantationProgress in lung transplantation has lagged behind other solid organ transplantation. One reason for
this is that unlike other newly transplanted organs, the lung has an extensive surface area through which itinterfaces and is directly exposed to viral and bacterial pathogens in the external environment (Mendeloff2002).
The first attempt at human lung transplantation was made in 1963 but long-term clinical success wasnot achieved until 1981 with a combined heart/lung transplant. The first successful isolated single lungtransplant was performed in 1983. After a period of rapid growth during the early 1990s, the annualnumber of lung transplants increased only slightly in the second half of the decade. Since 1995 lung transplantshave been relatively equally divided between unilateral and bilateral procedures and about 67% of lungrecipients have been reported from US centres (Hertz et al 2002). Transplantation is now the treatment ofchoice for selected patients with lung disease. Currently the two most important barriers to successfulapplication of transplantation are a shortage of suitable donor organs and chronic allograft deterioration asa result of bronchiolitis obliterans syndrome (Stewart and Patterson 2001).
Obliterative bronchiolitis (OB) usually occurs six months to one year post transplant but may be presentin up to 40% of patients at two years, up to 60% at three years and up to 70% of patients at five years(DeMeo and Ginns 2001, Choi et al 2003). OB is thought to be a manifestation of chronic allograft rejection,defined histologically by the presence of obliterative lesions in the epithelium of the terminal and respiratorybronchioles (DeMeo and Ginns 2001, Choi et al 2003). Because the disease process is multifocal, diagnosiscan be difficult with biopsy. In most patients, however, a presumptive clinical diagnosis (termed bronchiolitisobliterans syndrome) is made when the patient’s forced expiratory volume in one second (FEV1) declinesirreversibly by more than 20% in the absence of other causes for allograft dysfunction.
2.6.1 Indications for lung transplantation
a) Chronic obstructive pulmonary disease and alpha antitrypsin deficiency emphysemaEmphysema due to chronic pulmonary disease or, more rarely, alpha-antitrypsin deficiency is the most
common indication for lung transplantation. Provided patients receive supplementary oxygen and participatein pulmonary rehabilitation they are usually able to survive the time it takes to receive an appropriate donororgan. Of the patients listed for lung transplant in the UK between April 1995 and March 1999, 185 or26.3% were due to emphysema (Anyanwu, Rogers and Murday 2002).

Cardiothoracic transplantation review
page 18
b) Cystic fibrosisCystic fibrosis is a lung disorder that results in copious thick secretions that lead to chronic infection
and airway obstruction. Respiratory failure is the cause of death in the vast majority of patients. Cysticfibrosis accounted for 122 (17.3%) lung transplants in the UK between April 1995 and March 1999 (Anyanwu,Rogers and Murday 2002).
c) Primary pulmonary hypertension (PPH)Primary and secondary pulmonary hypertension can be treated by lung transplant. The isolated lung
graft provides long-term reduction in pulmonary after load and permits right heart recovery. Medical treatmentfor pulmonary hypertension has improved considerably with the development of prostacyclin therapy andtransplantation should be reserved for those patients who are non-responders to vasodilators or who arelate failures with therapy. Heart/lung transplantation has been the preferred treatment for PPH in the UK.
d) Pulmonary fibrosisPatients with interstitial pulmonary fibrosis usually experience a rapid decline in lung function and
physiological status. Referral for transplant should be made early in the course of the disease. Between April1995 and March 1999 pulmonary fibrosis accounted for 201 or 28.6 % of lung transplants performed in theUK (Anyanwu, Rogers and Murday 2002).
Figure 5
Indications for single and bilateral/double lung transplantationFigure 5 shows the indications for 10,822 procedures. CF, cystic fibrosis; A1A, [alpha]1-antitrypsin deficiency; PPH, primary pulmonaryhypertension; Retx, retransplantation; IPF, interstitial pulmonary fibrosis; Misc, miscellaneous. Reprinted from Hosenpud et al with permissionfrom Elsevier Science (Stewart and Patterson 2001).
2.6.2 Volume of transplantation (lung)A total of 946 adults received a first lung transplant between July 1995 and September 2002 inclusive
(UK National Audit of Intrathoracic Transplantation 2003).
2.6.3 Outcomes (lung)International statistics convey one, three and five year survivals of 74%, 58% and 47% respectively
(DeMeo 2001). One study has evaluated survival benefits of lung transplantation for patients with cysticfibrosis, interstitial fibrosis and emphysema. The findings indicate there is a survival benefit when comparedto waiting time for cystic fibrosis and interstitial fibrosis but not for emphysema (Hosenpud et al 1998).Bilateral lung transplant for emphysema has been associated with improved lung function and a trend forimproved survival.
Most patients who undergo lung transplantation experience a marked improvement in functionalcapacity and quality of life. By the end of the first year, most patients report no restriction in activity and sixminute walk results are at least twice the pre-operative value. Ten Vergert et al (1998) found that lungtransplantation improves quality of life secondary to improved mobility and energy, improved sleep,diminished dyspnoea and the ability to accomplish activities of daily living.
42.6%
2.4%
3.9%18.7%
19.5%
2.3%
10.6%
Emphysema CF PPH Misc. IPF Re tx A1A
17.5%
31.5%
9.2%
22.9%
7.1%
2.2%
9.6%
Emphysema CF PPH Misc. IPF Re tx A1A
single lung bilateral/double lung

Cardiothoracic transplantation review
page 19
Indications for adult lung transplantation between 1995 and 2001Table 1
DiagnosisDiagnosisDiagnosisDiagnosisDiagnosis Single lung txSingle lung txSingle lung txSingle lung txSingle lung tx Bilateral lung txBilateral lung txBilateral lung txBilateral lung txBilateral lung tx TTTTTotalotalotalotalotal(n=4,663)(n=4,663)(n=4,663)(n=4,663)(n=4,663) (n=4,118)(n=4,118)(n=4,118)(n=4,118)(n=4,118) (n=8,781)(n=8,781)(n=8,781)(n=8,781)(n=8,781)
COPD/emphysema 2536 54.4% 962 22.5% 3462 39.4%
Idiopathic pulmonary fibrosis 1110 23.8% 376 9.1% 1486 16.9%
Cystic fibrosis 52 1.1% 1360 33.0% 1412 16.1%
α-antitrypsin deficiency emphysema 408 8.7% 407 9.9% 815 9.3%
Primary pulmonary hypertension 611 1.3% 340 8.3% 401 4.6%
Sarcoidosis 126 2.7% 106 2.6% 232 2.6%
Bronchiectasis 14 0.3% 176 4.3% 190 2.2%
Congenital heart disease 8 0.2% 95 2.3% 103 1.2%
Lymphangiomyomatosis 42 0.9% 53 1.3% 95 1.1%
Re-tx obliterative bronchiolitis 44 0.9% 43 1.0% 87 1.0%
Obliterative bronchiolitis (non re-tx) 32 0.7% 50 1.2% 82 0.9%
Re-tx: non-OB 33 0.7% 36 0.9% 69 0.8%
Connective tissue disorder 20 0.4% 18 0.4% 38 0.4%
Cancer 7 0.2% 28 0.7% 35 0.4%
Histiocytosis X 11 0.2% 8 0.2% 19 0.2%
Other 159 3.4% 96 2.3% 255 2.9%
Registry of the International Society for Heart and Lung Transplantation 2002
2.72.72.72.72.7 Adult heart/lung transplantationAdult heart/lung transplantationAdult heart/lung transplantationAdult heart/lung transplantationAdult heart/lung transplantationA total of 254 adult heart/lung transplants were undertaken in the UK between July 1995 and December
2001 inclusive (UK National Audit of Intrathoracic Transplantation 2002).
Data from the Registry of the International Society for Heart and Lung Transplantation (Trulock et al2003) reports that the number of centres performing heart/lung transplants dropped from a high of 63 in1994 to 35 in 2001. Annual activity in heart/lung transplantation has decreased by 50% since 1995. Someof this decrease has been attributed to under reporting but the decline in numbers of heart/lung transplantsis also due to lung transplantation at least partially supplanting heart/lung for some conditions includingcystic fibrosis, chronic obstructive pulmonary disease and primary pulmonary hypertension.
Heart/lung transplantation has a high three month mortality rate. The Registry shows a three monthsurvival of approximately 70%. Thereafter there was a steady attrition and the survival rates at one, five andten years were 61%, 40% and 25% respectively. The survival half-life was 2.7 years, however the conditionalhalf-life was 8.1 years because mortality was concentrated in the first year (Trulock et al 2003).
PPH and pulmonary hypertension associated with Eisenmenger’s syndrome/congenital heart diseasehave been the main indications for heart/lung transplantation in adults. Despite the widespread use ofbilateral lung transplantation, CF remains the third most common diagnosis among heart-lung recipients.

Cardiothoracic transplantation review
page 20
2.82.82.82.82.8 Paediatric cardiothoracic transplantationPaediatric cardiothoracic transplantationPaediatric cardiothoracic transplantationPaediatric cardiothoracic transplantationPaediatric cardiothoracic transplantation2.8.1 Paediatric heart transplantation
Heart transplant is now a treatment option for infants and children with end-stage heart failure orcomplex congenital cardiac defects. Although there are rare reported cases of technically successful paediatricheart transplants from as early as 1967, it has been since the introduction of cyclosporine as a selectiveinhibitor of T-cell function in 1981 that transplantation has begun to develop as a routine therapy for end-stage heart disease (Kichuk-Chrisant 2002). According to the ISHLT Registry, over the last 20 years nearly4,000 infants and children have received a heart transplant (Mendeloff 2002). In the UK 159 paediatricheart transplants were carried out between 1 July 1995 and 31 December 2001 (UK National Audit ofIntrathoracic Transplantation 2002). It must be noted that in the UK paediatrics cases are considered as lessthan 16 years of age where as the cut off used by ISHLT is 18 years of age.
One of the differences between cardiac transplantation in adults and children is in the indications forthe operation. In children under 12 months of age congenital defects account for about 75% of thoselisted, with hypoplastic left heart syndrome being the most common defect. In the one to ten age group,slightly over 50% have cardiomyopathy and approximately 37% have congenital heart disease. In adolescentsthe main indication is cardiomyopathy (64%) with congenital disease accounting for 26%. In 2001 forpaediatric patients overall, cardiomyopathy accounted for 54% of registrations and congenital disease for40% (Colombani et al 2003 and Kichuk-Chrisant 2002).
Graft survival rates are slightly lower for patients under one year of age. There is an 86% survival atthree months compared to 88% in all other age groups. Overall paediatric patient survival at three monthsranges from 85% to 92% and at five years, survival ranges from 63% to 74%. These survival rates areslightly better than for older patient groups and most likely are a result of the benefits of younger donorgrafts with less risk of coronary disease (Colombani et al 2003). Boucek et al (2001) explain the higher threemonth mortality in patients less than 12 months of age as most likely being a result of abnormally complexanatomy and physiology and the fact that these infants may have to wait for a lengthy period of time in avery poor condition.
2.8.2 Paediatric lung transplantationPaediatric lung transplantation continues to be a rare procedure. Statistics from ISHLT indicate that
waiting list registrations peaked in 1998 at 152 and decreased to 105 and 115 in 2000 and 2001 respectively(Colombani et al 2003).
For infant recipients, congenital lung abnormality, followed by primary pulmonary hypertension werethe most common indication for transplantation. For children aged between one and ten years, cysticfibrosis was the most common indication followed by primary pulmonary hypertension. In the adolescentage group the reasons for transplantation were cystic fibrosis, primary pulmonary hypertension and idiopathicpulmonary fibrosis (Boucek et al 2001).
Patient survival for paediatric lung transplant patients appears to be similar or slightly higher than thatseen in adult patients. The five year survival for patients aged less than 12 months was 33%, for those agedsix to ten years, 64% and for patients aged 11-17 years, 45% were alive at five years post-transplant(Colombani et al 2003).
2.8.3 Paediatric heart/lung transplantationThe number of paediatric patients registering for heart/lung transplantation has remained fairly constant
over the last decade. In 2001, 25 patients were added to the waiting list but only six transplants wereperformed (Colombani et al 2003).
Congenital abnormalities of the heart and/or lung are now the leading indication for heart/lungtransplantation in young children and cystic fibrosis has become the leading cause in 11-17 year olds(Boucek et al 2001).

Cardiothoracic transplantation review
page 21
Meaningful data on graft and patient survival is available only for 11-17 year olds. The 54% five yearsurvival is similar or slightly better than that for heart/lung transplants in all age groups (Colombani et al2003).
2.92.92.92.92.9 VVVVVolume versus outcomeolume versus outcomeolume versus outcomeolume versus outcomeolume versus outcomeHosenpud et al (1994) studied outcome data from 7,893 heart transplants performed in 150 centres
in the USA between October 1987 and December 1991 to explore the effect of centre volume on outcome.The results showed that the risk of mortality decreased to a basal level in those centres performing betweeneight and ten transplants per year. In centres performing fewer than nine transplants per year, mortalityincreased sharply and exponentially. Once the threshold of nine transplants was reached there did notappear to be improved survival with increased numbers of operations.
To determine whether differences in low-volume centres were a function of the low volume directly ora function of overall experience, outcomes were collected annually for two years in 13 low-volume centres.This showed that mortality rates actually increased statistically in the second year (Hosenpud 1994), whichsuggested that a second year of experience was not a solution to the poor outcomes seen in low-volumecentres.
Figure 6
2003ISHLTJ Heart Lung Transplant 2003; 22: 610-72.
AVERAGE CENTER VOLUMEHeart Transplants: January 1, 1998 - June 30, 2002
6049
79
2913 6 5 30
10
20
30
40
50
60
70
80
1-4 5-9 10-19 20-29 30-39 40-49 50-74 75+Average number of heart transplants per year
Num
ber o
f cen
ters
Hosenpud et al (1994) stress in their commentary that the requirement of nine transplant proceduresper year was based on an approximation of the ‘break point’ in the relationship between centre volume andoutcome. They also comment that these data merely demonstrate that some level of experience and repetitionis required to guarantee survival rates. However, it is interesting to note that once a centre performs anaverage of one heart transplantation every 30 to 45 days, the mortality rates are comparable with thosecentres performing the procedure on a more regular basis.
A similar study was conducted by Edwards et al (1999) looking at liver transplantation. Again arelationship between centre volume and outcome was demonstrated. Using the same methods as Hosenpud,Edwards found that centres that perform 20 or less liver transplantation per year had a one year mortality of25.9% whereas those performing more than 20 transplantations had a one year mortality of 20%.
Recently the Thoracic Advisory Committee of Eurotransplant (an organ exchange organisation in whichdonor hospitals, transplant centres, and tissue typing centres in Austria, Belgium, Germany, Slovenia andthe Netherlands collaborate) started a quality initiative that divides standards of care into three categories:size, skills and surveillance. The overall goal is that transplant centres should be large enough to offercontinuous, skilled and comprehensive heart transplant care, including all treatment options for advancedheart failure treatment (Smits et al 2003).

Cardiothoracic transplantation review
page 22
Figure 7
2003ISHLTJ Heart Lung Transplant 2003; 22: 610-72.
ADULT HEART TRANSPLANTS (1/1995-6/2001)Risk Factors for 1 Year Mortality
Center volume
0
0.5
1
1.5
2
0 10 20 30 40 50 60 70
Center Volume (cases per year)
Odd
s of
1 Y
ear M
orta
lity
1995-19981999-6/2001
p = 0.003p < 0.0001
Dudley et al (2000) studied the literature and the California Discharge Database to identify proceduresand diagnoses for which there is good evidence that a volume-outcome relationship exists. For 11 conditions,the best study showed a statistically significant volume-outcome relationship in which high volume hospitalshave lower mortality rates than low volume hospitals. Among the 11 conditions for which mortality wassignificantly lower in high volume centres were coronary artery bypass surgery, coronary angioplasty, paediatriccardiac surgery and heart transplantation.
2.102.102.102.102.10 ConclusionsConclusionsConclusionsConclusionsConclusionsIn recent years there have been major developments in the pharmacological, interventional cardiology
and surgical treatment of patients with heart failure but for a small number of patients with end stagedisease cardiac transplantation remains the most effective treatment.
It has been estimated that by 2020 the total number of patients in Scotland requiring treatment forheart failure will have risen to over 105,000. This figure allows for demographic changes in the Scottishpopulation but assumes little or no change in the prevalence of heart failure.
Progress in lung transplantation has lagged behind other solid organ transplantation primarily becauseunlike other organs, the lung has an extensive surface area that is directly exposed to viral and bacterialpathogens. However there was a rapid period of progress in the first half of the last decade and a steady risein numbers since then. In contrast, activity in heart/lung transplantation has decreased by half since 1995.
Data from the ISHLT and independent studies have demonstrated a relationship between centre volumeand the odds of mortality but also show that there are very few centres performing the number of transplantoperations shown to be statistically important in improving the odds of mortality.
Actuarial survival for heart transplantation shows a patient half-life of nine years and a conditional half-life of 12 years. For lung transplantation international statistics convey one, three and five year survivals of74%, 58% and 47% respectively. Heart/lung transplantation has a high three month mortality rate andsteady attrition thereafter. However one, five and ten year survival rates of greater than 70%, 50% and 25%have been achieved. As transplantation offers good quality survival of almost 50% at 10 years for heartfailure patients, those suitable for VADs will continue to proceed to transplantation for the near future(Stevenson and Rose 2003).
Although other treatment options are becoming increasingly effective and there is better care withearlier diagnosis of heart failure, there remains at this time and for the foreseeable future a small group ofpatients for whom cardiothoracic organ transplantation remains the only treatment option which offers anyhope for survival. It is not known for certain whether the improved medical options available to heart failurepatients are preventing the need for transplantation or merely postponing that need for several years.

Cardiothoracic transplantation review
page 23
3. Expected needExpected needExpected needExpected needExpected need
3.13.13.13.13.1 IntroductionIntroductionIntroductionIntroductionIntroductionThe assessment of need for a defined service entails the identification and quantification of patients
who stand to benefit from the service; i.e, the number of individuals for whom the intervention adds yearsto life and/or adds life to years and can be supported in resource terms by the community. Needs assessmentalso requires to take into account alternative interventions and to identify the extent to which the interventionunder consideration confers greater benefit than other available affordable options.
Cardiothoracic organ transplantation comprises:· heart transplantation· lung transplantation· heart and lung transplantation
in adults and children. Transplantation is carried out in patients suffering from one of a number ofcirculatory and pulmonary conditions refractory to less invasive, medical and/or surgical interventions.
Conventionally, need for a service is considered under the following sub-divisions:
‘met need’ reflects the extent to which patients likely to benefit from the intervention as the preferredapproach to the management of their condition have, under the present arrangements, access to theintervention
‘unmet need’ comprises known cases where it is recognised that the intervention would representoptimal care but is for some reason unavailable, together with cases which, if appropriately identified andassessed, would be found to be likely to benefit from transplantation.
Information on met need is available from data on current service provision. Detailed, accurateinformation on Scottish residents who have undergone transplant and on waiting lists for transplantationare held by NSD and by UK Transplant.
Epidemiological data, international comparative service provision data and information on those waitingfor transplantation, including those dying while waiting, provide insights on unmet need although care isrequired interpreting such data. In particular, resource constraints, such as the supply of organs fortransplantation, and secular trends in the availability and efficacy of alternative forms of intervention mustbe considered.
3.23.23.23.23.2 Nature of candidate conditionsNature of candidate conditionsNature of candidate conditionsNature of candidate conditionsNature of candidate conditionsDetails on conditions requiring cardiothoracic transplantation are included in section 2 above. In
summary, the primary causes of all UK cardiothoracic transplantation between 1990 and 2000, withapproximate percentage, include:
Cardiomyopathy 28% Ischaemic heart disease 25%Congenital heart disease 5% Primary pulmonary hypertension 2%Valvular heart disease 1% Cystic fibrosis 8%Fibrosing lung disease 5% Emphysema 4%Congenital heart/lung disease 3% Other disease 15%Not reported 3%

Cardiothoracic transplantation review
page 24
3.33.33.33.33.3 Adult heart failureAdult heart failureAdult heart failureAdult heart failureAdult heart failureBy far the greatest group of potential adult cardiopulmonary organ recipients are patients suffering
from New York Heart Association Class III and IV heart failure despite optimum medical treatment. Heartfailure is a functional state in which the heart is unable to sustain an output of circulating blood volumeand/or pressure sufficient to maintain essential bodily functions ranging from exertion to renal perfusion.As such, it occurs as a consequence of a range of cardio-respiratory disorders. A further group of conditionsgenerate indications for cardiothoracic transplantation not necessarily through the development of heartfailure as the primary functional abnormality.
Chronic heart failure (CHF) affects 1.5% of the Scottish population (approx 32,500 people) and, assuch, constitutes a major public health problem. The predominant underlying pathology is ischaemic heartdisease. The mean age of patients suffering from CHF in Scotland is 75 years of whom 25% are under 66years of age. The age profile of patients is likely to change in future as people may present later fortransplantation following other interventions, or as a result of trends towards better health in later life in thepopulation. The annual mortality of CHF patients aged <45, (i.e, those most likely to be considered fortransplantation) admitted to Scottish hospitals between 1986 and 1995 was 24%
Acute heart failure (AHF) is predominantly due to acute myocardial infarction (AMI) with a muchsmaller number of cases arising out of acute, usually viral, myocarditis. Some 15-20% of AMI admissions toa coronary care unit die, often due to AHF non responsive to treatment. It is exceptional for such patients tobe considered candidates for heart transplant. Fulminant acute myocarditis is rare but often mimics AMIand is associated with AHF which is refractory to medical management. In cases sufficiently severe towarrant consideration for transplantation, the patient often dies before an donor organ can be identified.
3.43.43.43.43.4 Congenital heart diseaseCongenital heart diseaseCongenital heart diseaseCongenital heart diseaseCongenital heart diseaseCongenital heart disease (CHD), usually presenting and treated in infancy or early childhood, contributes
to presentations for heart and heart/lung transplantation in adult life in circumstances where the beneficialeffects of paediatric cardiac surgery are compromised by the maturity of the patient into adult stature or theintervention of late anatomical and/or physiological complications of the underlying condition or of theearlier intervention. In particular, the Mustard procedure for transposition of the great vessels, includingFallot’s tetralogy and the Fontan procedure for complex cardiac lesions are well established to be timelimited in their beneficial effect in a proportion of cases.
The existing adult CHD caseload in the Glasgow Western Infirmary, which carries approximately twothirds of the Scottish CHD caseload, extends to 700 patients estimated to include some 60 potential heartand heart/lung transplant candidates (Professor Stewart Hillis, personal communication). There are, inaddition, approximately 300 15-17 year old patients registered at the Glasgow Royal Hospital for SickChildren, due to transfer to the adult CHD service based at the Western Infirmary. This caseload is estimatedto include 28 potential transplant candidates.
This caseload is estimated by Professor Hillis to be likely to yield 3-5 candidates for heart and heart/lung transplantation per annum in the ratio 80:20 in favour of heart transplantation. Pro-rata Scotland as awhole is likely to generate a need for 5-8 transplants per annum for the foreseeable future, predominantlyheart transplants but including 1-2 heart/lung transplants per annum.
3.53.53.53.53.5 Cystic fibrosisCystic fibrosisCystic fibrosisCystic fibrosisCystic fibrosisDevelopments in the early management of cystic fibrosis has resulted in the majority of patients born
with the condition surviving into adolescence and adult life. However, the inexorable lung damageconsequent on repeated and/or chronic respiratory infection results in a predictable annual need for lungtransplantation. The age of candidates and the organised nature of Scottish services for adults with cysticfibrosis are such that those who are considered to merit transplantation on clinical grounds and agree to theintervention are likely to be admitted to the transplant waiting list.

Cardiothoracic transplantation review
page 25
3.63.63.63.63.6 Current provisionCurrent provisionCurrent provisionCurrent provisionCurrent provision
Adult heart transplants – Scottish residents, 1995-2003Table 2
Year Transplants Transplants Total Rate perin Scotland outwith Scotland million population
1995 12 4 16 3.11996 26 3 29 5.71997 22 0 22 4.31998 30 2 32 6.31999 33 0 33 6.52000 3 7 10 2.02001 5 6 11 2.22002 14 0 14 2.8
Adult heart/lung transplants - Scottish residents, 1995-2003Table 3
Year Transplants Rate permillion population
1995 1 0.21996 1 0.21997 0 01998 1 0.21999 4 0.82000 1 0.22001 0 02002 0 0
Adult lung transplants – Scottish residents, 1995-2003Table 4
Year Transplants Rate permillion population
1995 4 0.81996 5 1.01997 3 0.61998 8 1.61999 11 2.22000 3 0.62001 5 1.02002 10 2.0
Paediatric cardiothoracic transplants – Scottish residents, 1995-2002Table 5
Year Heart Lung
1995 1 01996 0 01997 0 01998 1 01999 0 02000 5 22001 2 02002 0 0

Cardiothoracic transplantation review
page 26
1995 1997 1999 2001
3.73.73.73.73.7 WWWWWaiting listsaiting listsaiting listsaiting listsaiting listsWaiting list statistics are often of assistance in providing information on levels of need, although they
require to be interpreted carefully in the context of other known influences on the presentation of cases ascandidates for care. In particular, where waiting lists are increasing over time there is some support for theargument that this represents a measure of unmet need for the intervention in question. Static or decliningwaiting lists are more difficult to interpret. Figures 8 and 9 show the UK year end waiting list trends forheart and heart/lung transplantation respectively over the period 1993-2002. While there has been asteady decline in the numbers of heart and heart/lung transplants performed over this period, the waitinglists for both procedures have declined as well. How much of this is attributable to improvements inalternative forms of care, described elsewhere in this report, and how much to more stringent case selectionby referring cardiologists, for the purposes of waiting list management, is difficult to quantify. It is likely thatthe former makes at least some contribution to the decline in waiting lists and that it is not entirely attributableto the latter. There is some support for this contention in the contrasting trend in the national lungtransplantation waiting statistics (Figure 10). Here, despite the fairly static number of transplants annually,the numbers waiting have consistently risen, year on year. One should, however, recognise that in generalthe referral and assessment processes for lung transplantation are materially different from those for hearttransplantation.Figure 8
Source: UK Transplant Activity Report 2002
Figure 9
Source: UK Transplant Activity Report 2002
Heart only transplants and active transplant list at year end in the UK, 1993-2002
1993
no. o
f tra
nsp
lant
s/on
tra
nsp
lant
list
350
300
250
200
150
100
50
1994 1996 1998 2000 2002
no. o
f tra
nsp
lant
s/on
tra
nsp
lant
list
1994 1996 1998 2000 2002
Heart/lung only transplants and active transplant list at year end in the UK, 1993-2002
200
180
160
140
120
100
80
60
40
20
transplant list
transplants
transplant list
transplants
1993 1995 1997 1999 2001

Cardiothoracic transplantation review
page 27
no. o
f tra
nsp
lant
s/on
tra
nsp
lant
list
1994 1996 1998 2000 2002
transplant list
transplants
300
250
200
150
100
50
Lung only transplants and active transplant list at year end in the UK, 1993-2002
1993 1995 1997 1999 2001
Figure 10
Source: UK Transplant Activity Report 2002
Information specific to the Glasgow heart transplant programme waiting list is shown in Table 6. Thetable demonstrates the trends over time in numbers of assessments, waiting lists, patients dying on thewaiting list for transplantation and heart transplant numbers.
GRI heart transplant activity and waiting list 1997/8 to 2002/3Table 6
Year Assessed Waiting list Deaths on Transplantsw.l.
1997-98 102 32 0 321998-99 58 33 4 321999-00 36 25 4 252000-01 46 12 1 6*2001-02 55 8 1 82002-03 78 8 1 12
* Performed at Freeman Hospital, Newcastle
Despite the dramatic impact on transplant numbers when the Glasgow service was suspended in2000, the assessment numbers have continued at broadly comparable levels and the waiting list has reducedmore or less in line with the number of transplants carried out reflecting the national trend.
3.83.83.83.83.8 International comparisonsInternational comparisonsInternational comparisonsInternational comparisonsInternational comparisonsTables 7 to 9 show heart, heart/lung and lung transplant rates for European countries since 1999. The
data is incomplete for some countries.

Cardiothoracic transplantation review
page 28
Heart transplant rates per million population (1999-2002)Table 7
Country (pop’n * 106) 1999 2000 2001 2002
Austria (8.2) 11.5 10.5 7.6 8.8
Belgium & Luxembourg (10.7) 8.5 7.8 7.5 7.9
Denmark (5.4) 4.9 5.2 5.7 5.2
Eire*^ (3.9) 2.8 3.8 3.6 3.9
France* (60.2) - - - 5.6
Finland (5.2) 2.5 2.7 2.5 3.5
Germany (82.4) 5.8 4.9 4.8 4.8
Italy* (58.0) - - - 5.5
Netherlands (16.2) 2.6 2.3 2.2 2.6
Norway (4.6) 7.2 5.6 6.0 5.7
SCOTLAND (5.1) 6.5 2.0 2.2 2.8
Slovenia (1.9) - 3.6 2.1 1.5
Spain* (40.2) - - - 7.4
Sweden (8.9) 3.8 2.3 2.8 2.1
UK (including Scotland) (60.1) 3.8 3.4 2.8 2.6
* includes heart/lung transplants^̂̂̂̂ financial year data
Heart/lung transplant rates per million population (1999-2002)Table 8
Country (pop’n * 106) 1999 2000 2001 2002
Austria (8.2) 0.1 0.2 0.2 0.2
Belgium & Luxembourg (10.7) 0.5 0.6 0.4 0.5
Denmark (5.4) 0.0 0.0 0.0 0.2
Finland (5.2) 0.4 0.6 0.6 0.0
Germany (82.4) 0.2 0.1 0.2 0.2
Netherlands (16.2) 0.1 0.1 0.1 0.1
Norway (4.6) 0.0 0.4 0.4 0.0
SCOTLAND (5.1) 0.8 0.2 0.0 0.0
Slovenia (1.9) 0.0 0.0 0.0 0.0
Sweden (8.9) 0.3 0.2 0.1 0.2
UK (including Scotland) (60.1) 0.8 0.5 0.5 0.3

Cardiothoracic transplantation review
page 29
Lung transplant rates per million population (1999-2002)Table 9
Country (pop’n * 106) 1999 2000 2001 2002
Austria (8.2) 8.1 7.0 7.0 10.9
Belgium & Luxembourg (10.7) 2.6 3.4 4.9 4.6
Denmark (5.4) 8.6 5.7 5.3 8.4
Eire (3.9) - - - 0.0
France (60.2) - - - 1.4
Finland (5.2) 0.0 1.5 0.8 0.7
Germany (82.4) 1.5 1.8 1.5 2.4
Italy (58.0) - - - 1.1
Netherlands (16.2) 1.0 1.0 1.5 2.6
Norway (4.6) 2.5 3.3 2.9 2.6
SCOTLAND (5.1) 2.2 0.6 1.0 2.0
Slovenia (1.9) 0.0 0.0 0.0 0.0
Spain (40.2) - - - 3.8
Sweden (8.9) 2.9 3.0 2.4 5.7
UK - including Scotland (60.1) 1.8 1.6 1.5 1.9
3.93.93.93.93.9 Alternatives to transplantationAlternatives to transplantationAlternatives to transplantationAlternatives to transplantationAlternatives to transplantationa. Drug treatment
In recent years the substantial improvements in the non-surgical management of patients with heartfailure described in section 2 of this report have shifted the balance of advantage for many patients whomight have been candidates for heart transplantation five years ago in favour of continuing pharmacologicalintervention. Fewer patients with heart failure, secondary to ischaemic heart disease in particular, are nowbeing assessed as requiring heart transplantation and other clinical indications are now accountable for anincreasing proportion of candidates for transplantation.
b. Non-transplant surgical interventionsA range of innovative surgical interventions short of transplantation are now available for the
management of candidate conditions for transplantation. Notable among these is the use of ventricularassist devices (VADs). However, their introduction into UK practice is at an evaluative stage and it remains tobe established how many such procedures will be clinically indicated for the Scottish population. In themeantime, it is not anticipated that the annual number of VAD insertions into Scottish patients will exceedfive. The impact of this, or an expanded VAD programme in due course, on transplant demand remains tobe clarified. Certainly, ventricular support will be capable of sustaining life for a period of time in a numberof candidates for transplantation who, without such support, would never reach a point where a donororgan became available.
3.10 Projected ser3.10 Projected ser3.10 Projected ser3.10 Projected ser3.10 Projected service needvice needvice needvice needvice need3.10.1 Adult cardiothoracic transplantation.
In strict economic appraisal terms, need does not equate to demand. In particular, need must take intoaccount resource constraints. In transplant services, a key resource constraint is organ availability. Whetherdevelopments in drug treatment have led to a shift in the balance of advantage in favour of medical treatment, thefact is that all suitable thoracic organs donated for transplantation purposes are offered and the majority transplanted.

Cardiothoracic transplantation review
page 30
Organ supply must be assumed to be the definitive limiting factor in determining the number andrate of adult cardiothoracic transplantation in the UK and in Scotland.
International statistics show a greater resistance to organ donation in the UK than in most Europeancomparators. It is common to find national rates of heart transplantation of around 5 per million with asmall number of transplant programmes achieving 7-8 per million. Presumably these rates are clinicallywarranted, notwithstanding developments in non-transplant treatments for candidate conditions, notablyCHF. Whether we will ever see again such levels in the UK is extremely doubtful and cannot be a reasonablebasis of service planning.
The donor organ availability to a Scottish population in the foreseeable future is likely to remainaround the current UK annual rates of:
2.6 to 3.0 per million for heart transplant0.3 to 0.5 per million for heart/lung transplant1.5 to 2.0 per million for lung transplant.
Corresponding to:
13 to 15 adult heart transplants1 to 2 adult heart/lung transplants7 to 10 adult lung transplants per annum.
A more optimistic projection of the return of donor organ availability levels to those of several yearsago would permit rates of:
4.0 per million for heart transplant1.0 per million for heart-lung transplant2.0 per million for lung transplant.
Corresponding to:up to 20 adult heart transplantsup to 5 adult heart-lung transplantsup to 15 adult lung transplants.
For the purposes of planning, the more conservative of these approaches represents a more prudentprojection of the level of service that can be aspired to over the next few years for adult cardiothoracictransplantation. In any event, it will be necessary to monitor changes in organ availability and their impacton transplantation rates on an ongoing basis.
3.10.2 Adult advanced heart failureHeart failure represents a spectrum of heart disease from moderate to severe conditions. In this report
only patients with severe heart failure (NYHA class III and IV heart failure despite optimum medical treatment)are considered. This is because only patients at this very severe end of the spectrum need the highly specialistinterventions of an advanced heart failure service that includes transplantation. Less severe heart failure canbe treated effectively in the specialised tertiary regional cardiac services in Glasgow, Aberdeen and Edinburgh.
The numbers of patients involved depends entirely on the definition of severity applied. Many thousandsof patients suffer heart failure but only very few cannot be treated effectively within local cardiac servicenetworks and regional tertiary cardiac centres.
The estimated numner of adult patients each year that may benefit from treatment and expertise onlyavailable withing Scotland in Glasgow at the national heart centre is as follows:

Cardiothoracic transplantation review
page 31
100 patients referred for specialist assessment and advice on management13-15 requiring heart transplantation (as outlined above)10-15 requiring advanced complex heart surgery5-10 requiring cardiac resynchronisation therapy.
In addition it is expected that some 2-5 patients may present each year requiring VADs. Such patientswould be referred to one of the three English centres taking part in the current UK evaluation at present.Once the evaluation is complete, a decision will be taken on whether the Glasgow advanced heart failureservice should provide this therapy in addition to those listed above.
Predicting need in this area of rapidly evolving techniques and technology is an inexact science. Asmechanical heart assist devices develop, the number of patients who may benefit may change significantly.Glasgow specialists predict that in a few years’ time the need for VADs may be 7-10 patients rather than thecurrent 2-5; and that cardiac resynchronisation numbers may be as high as 40 per annum.
3.10.3 Paediatric cardiothoracic transplantationUnlike adult cardiothoracic transplantation, the numbers of paediatric cardiothoracic transplants for
residents of Scotland have not been constrained by the availability of donor organs.
Comparisons with rates of paediatric transplantation in the rest of the UK would suggest a need inScotland for some five paediatric transplants per year. Actual numbers have, on average, been between oneand two a year. Work with cardiologists in Scotland has identified no unmet need. As a result the continuingprojected need for paediatric cardiothoracic transplantation for residents of Scotland is assessed to be:
1-2 paediatric transplants per year.

Cardiothoracic transplantation review
page 32
4.4.4.4.4. Current serCurrent serCurrent serCurrent serCurrent service for residents of Scotlandvice for residents of Scotlandvice for residents of Scotlandvice for residents of Scotlandvice for residents of Scotland
Cardiothoracic transplantation and advanced heart surgical services for the residents of Scotland arecurrently commissioned by NSD and delivered by a number of different hospitals in the UK. To date thehospitals to which Scottish residents have been referred are:
•Glasgow – adult heart transplantation, advanced paediatric cardiac surgery supported by paediatricECLS.
•Newcastle – adult and child heart, heart/lung and lung transplantation, ventricular assist devices foradults and children, advanced paediatric cardiac surgery supported by paediatric ECLS.
•Cambridge – adult heart, heart/lung and lung transplantation, ventricular assist devices for adults.
•London (Harefield and Great Ormond Street) - adult and child heart, heart/lung and lungtransplantation, ventricular assist devices for adults and children, advanced paediatric cardiac surgerysupported by paediatric ECLS.
•Birmingham - - - - - advanced paediatric cardiac surgery.
Heart transplantation for adults is primarily carried out at Glasgow Royal Infirmary (GRI) with a smallnumber of patients having their transplant at the Freeman Hospital in Newcastle. Adult lung and heart/lungtransplants are predominantly performed at the Freeman Hospital and paediatric transplantations for bothhearts and lungs are carried out at Freeman and Great Ormond Street.
For the exceptional cases when patients are referred to other centres, NSD has in place service agreementsfor Scottish access to other cardiothoracic transplantation and advanced heart surgical services in Englandthrough NSD’s sister organisation – the National Specialist Commissioning Advisory Group (NSCAG). Thisarrangement covers any Scottish referrals for VADs within the UK evaluation.
The present service level agreement between NSD and the Glasgow Trust is for 15 heart transplantsper annum. The agreement with Freeman Hospital is for four heart transplants, including paediatric cases,and 15 lung and heart/lung transplants.
4.1. Interaction with UK T4.1. Interaction with UK T4.1. Interaction with UK T4.1. Interaction with UK T4.1. Interaction with UK TransplantransplantransplantransplantransplantUK Transplant (UKT) was developed out of the 1998-99 review of United Kingdom Transplant Services
Special Authority (UKTSSA). That review concluded that UKT should continue to perform the core functionsof a national transplantation support body and in addition should have responsibility for improvingarrangements for transplant co-ordination services and improving organ donation and procurement ratesacross the UK.
UKT, which is a special health authority, is responsible for supporting services across the whole of theUK and for organising organ transfer arrangements between different units depending on the specificorgan that is to be transplanted. It maintains the national waiting list, maintains a 24-hour office to organisethe retrieval, allocation and transport of organs and it maintains the national transplant database. The UKTadvisory committees decide on the organ allocation arrangements so that organs go to the most suitablerecipient.
Since May 2002 UKT has maintained an organ donor register. The Scottish Executive Health Department(SEHD) makes a contribution to the running costs of UKT to cover Scotland’s share of the service and itsdevelopments.
In Scotland, the Scottish Transplant Group (STG) has evolved from the Renal Sub-Group of the Acute

Cardiothoracic transplantation review
page 33
Services Review. A working group was established to examine the process of organ donation, retrieval andtransplantation. It was recognised by SEHD that it would be useful to have a source of advice on transplantationin general and not just for renal issues. The Chief Executive and Medical Director of UKT sit on the STG toensure the UK perspective is integrated into the work of the group.
The Scottish Transplant Co-ordinators Network (STCN) was established at around the same timefollowing the Acute Services Review. NSD commissions the service and this has allowed for appointments tobe made in Edinburgh, Glasgow, Dundee, Inverness and Aberdeen. Members of the STCN sit on the UKTTransplant Co-ordinator Advisory Group and its sub-groups.
The consultant hepatologist from the Edinburgh Liver Transplantation Service sits on the Board of UKTand the Director of the Glasgow unit sits on the Cardiothoracic Advisory Group.
4.2. Geography & distance in Scotland4.2. Geography & distance in Scotland4.2. Geography & distance in Scotland4.2. Geography & distance in Scotland4.2. Geography & distance in ScotlandScotland has a distinct geography from the rest of the United Kingdom in that it is large and relatively
sparsely populated.
Approximately 50% of the population of Scotland live in the central belt and can commute to Glasgowwithin an hour by car.
Figure 11 provides a map of all Scottish residents that have received a heart transplant in GlasgowRoyal Infirmary in relation to distance from centre. As noted from the map the majority of patients arewithin 1 hour drive of Glasgow Royal Infirmary.
Figure 11
4.3. Organ retrieval4.3. Organ retrieval4.3. Organ retrieval4.3. Organ retrieval4.3. Organ retrievalMulti-organ retrieval is a complex process that usually takes place outwith normal working hours and
puts pressure on the elective work of the hospital where the retrieval team is based and on the donorhospital where theatres, theatre staff and anaesthetists may be needed for several hours. Currently patients
!(!(!(!(
!(!(
!(
!(!(
!( !( !(!(
!(
!( !(!(!(!(
!( !(!(!(!(
!(!(!( !(!(
!(!(!(!(!(!(!(!(!(
!(!( !(!(!(
!(!(!(!(!(
!(
!(
!(!(
!(!(!(!(!(
!(!(
!(
!(!(!(
!( !( !(
!( !(
!(
!(!(
!(!(!(!(
!(!(!(!(
!(
!(
!(
!(
!(
!(
!(G
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!!
!
!
!
!
!
!
!
!
!
!
Ayr
Oban
Wick
Perth
Elgin
Thurso
Dundee
Mallaig
Glasgow
Braemar
Selkirk
Ullapool
Dingwall
Greenock
Stirling
Dumfries
Aberdeen
Inverness
Inveraray
Pitlochry
Edinburgh
Helmsdale
Newtonmore
Crianlarich
Campbeltown
Fraserburgh
Fort William
Kyle of Lochalsh
Berwick-upon-Tweed
Legend! Place
!( Patients
Glasgow Royal Infirmary 60 min extent
Health Board boundary
G Glasgow Royal Infirmary ¸
Map of Cardio-Thoracic Patients in Scotland, Attending GRI for Transplant
with 1 Hour Travel Time

Cardiothoracic transplantation review
page 34
declared dead by brain stem testing are considered for multi-organ donation. This requires the local co-ordinator to ensure the arrival of the various retrieval teams at the appropriate time. At present the liverteam travel from Edinburgh and the intrathoracic team travel from Glasgow. Kidneys are retrieved by theliver team in all regions other than Glasgow. The kidney team is often drawn from the liver team but onoccasion and particularly in Glasgow the local transplant team will participate in the retrieval.
Organ retrieval is not popular amongst consultants and rotas rely heavily on trainees although inScotland, unlike in the rest of the UK, consultants regularly attend more than one third of retrievals. Theimpact of the new consultant contract and European Working Time Directive is stretching the sustainabilityof even large transplant programmes. There has been a move in England to provide the service from fewercentres.
Zonal organ retrieval was introduced in the UK in November 1993. Under this arrangement Scotlandis deemed a zone for all solid organ retrievals. Since the introduction of the zonal arrangements it has beenrare for a retrieval team from outwith Scotland to be called to a Scottish donor. The zonal arrangementsmean that lungs from Scottish patients go to Newcastle in the first instance.
In Scotland, a proposal to develop a Single Organ Retrieval Team (SORT) has been approved by NHSBoard Chief Executives and the Scottish Executive Health Department on a trial basis for a year. The keyproposal is that the new team will include an anaesthetist so that the donor hospital is not committed toproviding that resource. As at present, the liver and kidney surgeons will come from Edinburgh and thecardiothoracic surgeons from Glasgow. For the purposes of the trial the anaesthetist will come from Edinburghbut long term it is hoped that there will be funding for an anaesthetic rota based most likely in Glasgow.
Donors in Scotland (solid organs only)Table 10
Number of per milliondonors population
1998/99 71 14.21999/00 70 13.92000/01 58 11.62001/02 62 12.42002/03 59 11.8
Source: Scottish Transplant Co-ordinator Network
Donors in Scotland (thoracic organs only) (Scottish service suspended Feb 2000 – Aug 2001)Table 11
Time Period Total Hearts Lungs Heart/lungs
Feb 1998 – Aug1999 66 44 4 18Feb 2000 – Aug 2001 19 7 10 2Feb 2002 – Aug 2003 43 22 16 5
Source: Scottish Cardiopulmonary Transplant Unit
As can be seen from tables 10 and 11 the total number of donors for all solid organs during thesuspension of the Scottish heart transplant service reflected the generally downward trend that has beenseen in UK donor numbers. However, for cardiothoracic organs there was a marked reduction in organsretrieved during the time the service was suspended. This trend is widely assumed to be partly due tochanges in management of neurosurgical patients and to improved road safety.
These tables cover only one relatively short time period when there were several other issues in play,

Cardiothoracic transplantation review
page 35
but they do serve as an illustration of the difficulties involved in organ retrieval and the effect that theremoval of one service can have on available organs.
4.4. Accommodation and facilities in Glasgow4.4. Accommodation and facilities in Glasgow4.4. Accommodation and facilities in Glasgow4.4. Accommodation and facilities in Glasgow4.4. Accommodation and facilities in GlasgowThe current cardiac transplantation programme is situated in the cardiothoracic unit at the GRI. The
accommodation consists of a dedicated ward with five separate single patient rooms. Within the ward thereis a room with facilities for endomyocardial biopsy and right heart catheterisation. The ward has bedsideand ambulatory monitoring. The ward adjoins the cardiothoracic intensive care unit, which has ten beds,including two rooms appropriate for isolation with ventilatory support. There is a dedicated transplant clinicarea, which includes two consulting rooms on a lower floor of the same building for outpatient clinics. Theunit has four flats available for use by relatives of transplant patients or by patients as a step down facility.This accommodation is located on the Glasgow Royal Infirmary site.
There is a proposed merger of the cardiothoracic units currently situated at Glasgow Royal Infirmaryand the Western Infirmary in Glasgow, together with the thoracic surgical unit at Hairmyres Hospital in EastKilbride in Lanarkshire and the existing cardiac surgical service at the Golden Jubilee Hospital in Clydebank.One option under consideration is for the site of this merged service to be at the Golden Jubilee Hospital,Clydebank. At present the timescale for a decision has not been determined.
If this option were developed it would create the largest unit of its type in the UK with 15 consultantcardiac, cardiothoracic and thoracic surgeons. The physical plant available is of a very high standard. Atpresent the transplant unit has all the specialty adjacencies that can be expected in a large teaching hospital.Patients with severe heart failure are often very ill and have other health problems at the same time as heartdisease. They need a range of specialists to provide holistic care to meet their needs. If the service is relocatedto the Clydebank site these services will be within the same city but will not be available onsite. The Clydebanksite is a considerable distance from any other teaching hospital facility. A successful transplantation programmeis heavily dependant on the intergral working of the transplant team with other clinical and hospital disciplinesincluding pharmacy, dietetics, psychiatry and psychology, laboratory services such as virology, bacteriologyand histology, renal and vascular physicians and surgeons. None of these could be provided easily at theClydebank site, and therefore there is potential for patients not to have immediate access to the full rangeof services needed - e.g, renal specialists. Whilst rotas for all staff disciplines could be managed within thecardiothoracic service it would make management of interaction with staff at all levels of training andexperience much more difficult and would inevitably result in some duplication of services across Glasgow.This model would be in opposition to the current trend in the UK which is to avoid single speciality hospitals.As a result the expert review group recommends against the provision of adult heart transplantation on asite remote from other required specialities.
If the cardiac transplantation service were to remain in its present location the available accommodationand plant is adequate and has in the recent past coped with a caseload of 35 transplants per annum.
4.5. Accommodation and facilities in Newcastle4.5. Accommodation and facilities in Newcastle4.5. Accommodation and facilities in Newcastle4.5. Accommodation and facilities in Newcastle4.5. Accommodation and facilities in NewcastleThe current cardiothoracic transplantation programme is situated within Freeman Hospital, Newcastle,
in the specialist cardiothoracic centre adjacent to other specialities in the main hospital.
As in Glasgow, the accommodation is of a high standard and has been designed specifically to meetthe needs of cardiothoracic transplantation patients. It consists of dedicated wards with several separatesingle patient rooms and includes dedicated theatre and intensive care and the full range of specialistfacilities required for both heart and lung transplantation. There are facilities in the Freeman Hospital forECLS and Newcastle is one of the three sites approved to implant VADs within the UK evaluation.
There are seperate facilities for adults and children and the paediatric service is on the same site as thepaediatric cardiac surgery service. This is, however, on a different site from the main paediatric intensivecare service.

Cardiothoracic transplantation review
page 36
4.6. Proposed advanced heart failure ser4.6. Proposed advanced heart failure ser4.6. Proposed advanced heart failure ser4.6. Proposed advanced heart failure ser4.6. Proposed advanced heart failure serviceviceviceviceviceThe proposed development of a comprehensive advanced heart failure service for Scotland would
ensure that the management of advanced heart failure would be modernised and cutting edge treatmentscould be provided to patients suffering with heart failure. A multidisciplinary approach is essential to providehigh quality care and the integration of the heart transplant centre into this service would have an overallbenefit to patients in the long term.
It is envisioned that an advanced heart failure service for adults in Scotland would be established inGlasgow with transplantation and advanced surgery as integral components.
This service would provide assessment and advice on the management of patients who cannot bemanaged at a tertiary centre. This may include some investigations. In addition where there are innovativetreatments that are new to Scotland, these would first be offered at the centre until such time as it wasconsidered appropriate to roll them out to tertiary centres across Scotland. An example of this at present iscardiac resynchronisation therapy. They would also be responsible for the dissemination of new and goodpractice, through established national managed clinical networks.
At present the use of VADs is restricted in the UK as a bridge to transplantation in a multi centre trial atPapworth, Harefield and Freeman hospitals. If the trial results are favourable and VADs are implanted atother UK centres this would in future be offered as part of the Glasgow heart failure service.
It is expected that the advanced heart centre would be involved in research and have close academiclinks.
4.7. Capacity in English ser4.7. Capacity in English ser4.7. Capacity in English ser4.7. Capacity in English ser4.7. Capacity in English servicesvicesvicesvicesvicesEnglish centres were asked to provide information on potential capacity in their services to cope with
residents of Scotland requiring heart transplant. The transplant unit in Manchester responded suggestingthat they were confident that they would be able to cope with the increased capacity if the recommendationwere to withdraw adult heart transplantation from Glasgow, based on the current number of heart transplants.
The Newcastle Trust responded to the same request noting that NSCAG had requested informationabout resources required to comply with EC Working Time Directives and the estimated resources requiredto address the impact of the new consultants contract. The Newcastle Trust had submitted additional bidsfor developments to NSCAG, mainly for staffing and equipment. If these developments were approved thiswould enable the unit to support the provision of existing transplant services and take on the additionalScottish adult heart transplant surgical activity. However, they did highlight that it would be essential tolook at the links to the Scottish organ retrieval team to assess the impact of retrieval on the Newcastle teamand the follow up arrangements for existing patients, as out patient services were currently at full capacity.
No quantifiable indications were provided and requirements such as additional ITU beds were nothighlighted by either the Manchester or Newcastle Trusts.

Cardiothoracic transplantation review
page 37
5.5.5.5.5. Professional and staff opinionProfessional and staff opinionProfessional and staff opinionProfessional and staff opinionProfessional and staff opinion
5.1. Professional and staff opinion5.1. Professional and staff opinion5.1. Professional and staff opinion5.1. Professional and staff opinion5.1. Professional and staff opinionA number of approaches were implemented to obtain the views of as many stakeholders as possible
including writing to NHS Board Chief Executives, Regional Planning Groups, consultant cardiologists andrespiratory physicians, paediatric cardiologists and cardiac surgeons.
Staff responseAn open meeting was held on 28 October 2003 for staff either working directly in the transplant
service or connected with it as part of the service they provide. 25 members of staff attended this meetingand staff of all grades and disciplines were then given the opportunity to meet with NSD on an individualbasis or in small groups. Staff from the following groups took the opportunity to speak to us.
· Anaesthetists· Consultant cardiothoracic surgeons· Nurse managers· Outpatient nursing staff· Perfusionists· Pharmacists· Social workers· Theatre nursing staff· Transplant co-ordinators· Transplant fellows· Virologists· Ward nursing staff
Questions and comments covered all of the options and criteria, the process and timing of the reviewand the concerns and aspirations of the staff. They are summarised below.
Review processIn general the staff felt that review was disenfranchising staff who were interested in transplantation
and consequently, staff were finding it difficult to remain positive and manage morale in the unit. Theextreme case was staff feeling powerless and isolated and not feeling that they had the opportunity to putacross their case fairly, as there was no representative from the unit involved in the actual formal reviewprocess.
Staff felt the review process had been handled badly the last time (when the service was suspended)and unfortunately some staff had found out about the review from the press. Practical issues such asrecruitment and retention were difficult to manage and there was a request that if the recommendationwere to close the unit, that this be done without delay.
In general the review process was thought to be distressing for staff and patients alike.
Improved serviceWithout exception all staff commented on the improvement in management of the unit since re-
opening. It was suggested that the review must acknowledge the work that has gone into re-establishingthe service which has vastly improved on what was previously offered.
One member of staff noted that ‘this is a good unit to work in, it is well run and the spirit of teamworking is tremendous’.

Cardiothoracic transplantation review
page 38
Future serviceIn respect to the proposed advanced heart failure service there was split opinion on whether a service
could deliver an VAD service with/without transplantation. The staff in the unit were keen to see the serviceevolve and would welcome the opportunity to expand the service to include lung transplantation andsuggested that the unit had the capacity to cope with this expansion. However, some of the anaesthetistswere unsure about how they would cope with lung transplants and suggested that if this was the decisionfurther discussion and planning would be required.
OptionsThere was a general consensus of opinion that if Glasgow closed there would be difficulties with
retrievals and the retrieval service would consequently deteriorate. Similar to the patients’ concerns, thequestion regarding donor rates in Scotland being adversely affected if the Scottish transplant centre closedwas raised.
Options 6 and 7 (where transplant surgery would be performed in England but patients would befollowed up in Scotland) were not perceived as viable options. The reasons against these options were thatit would complicate the follow-up of these patients, it would be confusing for patients, and recruiting andretaining staff would be difficult if the workload only consisted of follow-up patients. Managing the carepathway for patients from the Islands and other remote areas was also highlighted as a disadvantage ofthese two options.
5.25.25.25.25.2 Professional stakeholders’ responseProfessional stakeholders’ responseProfessional stakeholders’ responseProfessional stakeholders’ responseProfessional stakeholders’ responseAs noted, views were requested from a range of stakeholders in Scotland. The following provides the
main issues highlighted.
TrainingFew centres currently undertake cardiothoracic transplants in the UK, therefore the unit in Glasgow is
a major asset for trainees both in Glasgow and throughout the rest of Scotland. Trainees are not onlyexposed to transplant surgery but also to techniques of retrieving intrathoracic organs and the assessmentand management of severe heart failure. It was suggested that the closure of the unit would be a great lossto cardiothoracic surgical training. In addition, the research and audit opportunities available for traineeswas perceived to be valuable training.
Advanced heart failure serviceThere was general support for an advanced heart failure service for Scotland, although there was some
disagreement on what this would entail. One view was that this would provide valuable advice to cliniciansthroughout Scotland, co-ordinate trials and develop treatments. It was not regarded in all cases that hearttransplantation must be a prerequisite of this service.
Lung transplantationIt was suggested by a respiratory physician that the ideal scenario would be if patients could have lung
and heart/lung transplants nearer to home. However, if the expansion into lung transplantation did nothave an overall effect on the numbers of available organs then it was perceived that this benefit would beslight. Another essential requirement was equity of quality of care throughout the UK.
General opinionThere was divergence of opinion regarding the viability of the unit. Concerns raised were in relation to
the low numbers, whether there were enough cases to maintain skills and expertise and maintenance ofsuch a costly service. One NHS Board had discussed the options with adult and paediatric consultants acrossthe Board and concluded that the unit should be decommissioned and patients should be referred toNewcastle, suggesting option 4 to be the most viable option for residents of Scotland. The main reasonsidentified are as noted above, reiterating that the more procedures performed in a centre the greater thelevel of expertise.
The counter view to this argument from some stakeholders was that the unit has the skills and expertiseto expand into lung transplantation and/or an advanced heart failure service.

Cardiothoracic transplantation review
page 39
To conclude, the range of views across the stakeholders is as diverse as the individuals involved. However,there was a general consensus that Scotland should have an advanced heart failure service, regardless of theoutcome of the review.

Cardiothoracic transplantation review
page 40
6.6.6.6.6. Patient/public opinionPatient/public opinionPatient/public opinionPatient/public opinionPatient/public opinion
6.1. Introduction6.1. Introduction6.1. Introduction6.1. Introduction6.1. IntroductionDifferent approaches were employed to ensure that a broad range of views was received from the
public and patients who have either had a heart transplant or who suffer from heart failure. This involvedthe use of focus groups as described below, a meeting for patients with NSD and an invitation to patients togive their opinions to the review. In order to maintain patient confidentiality, the transplant units in Glasgowand Newcastle were asked to forward a letter from NSD informing people about the review and givingthem the opportunity to make known their views and opinions on the future delivery of cardiothoracictransplant services for residents of Scotland. Letters were sent from Glasgow Royal Infirmary (GRI) to allpatients who had received a transplant in the past informing them of the review and allowing them theopportunity to contact NSD, to volunteer to participate in externally run focus groups and also to attend ashort presentation given by the Nursing & Quality Adviser for NSD at GRI in September 2003.
A patient representative has been a member of the steering group and has worked tirelessly to keeppatients informed about the review and to ensure that the views of as many patients as possible have beengiven full consideration throughout the review. The Convenor of the Scottish Association of Health Councilshas also been a member of the steering group to represent the wider public.
6.2. Focus groups6.2. Focus groups6.2. Focus groups6.2. Focus groups6.2. Focus groupsFollowing advice from the Involving Patients team within the Scottish Executive Health Department it
was agreed that focus groups should be organised to obtain public/patient views. Following a tenderingexercise Stimulating World were awarded the contract. It was agreed that information from the focus groupsshould be gathered on the following issues:
ChoiceThis would include choice of treatment, care, clinician, location, timing.
AccessibilityCovering accessibility of the right health care professionals, support networks, and also accessibility of
the hospital. Included in this may be that some individuals choose to visit their GP for support.
Quality of life including social/family lifeIn relation to diagnosis, treatment and follow-up.
Financial impactFinancial impact that treatment has had on patients’ lives.
Non-clinical supportHow important is a support network, whether it be a support group with other patients/carers, support
from GP or support from the hospital. Availability of accommodation for patients/carers.
Continuity of careIs the care that patients receive linked together? The term ‘seamless care’ across all specialities may
help explain this.
Clinical effectivenessThis means that the care and treatment that the patient receives is effective and achieves the desired
outcome. Related to this are issues such as survival and procedures, for instance short term outcomes suchas complications following surgery. Long term outcome would be survival.
It was suggested that asking patients/public to respond to the agreed options would not elicit valuableinformation. The aim of the research was to elicit the views on what are regarded as important factors in

Cardiothoracic transplantation review
page 41
relation to the future of the service. The main findings of the research are detailed below.
Research objectivesThe objective of the research was to establish what individuals with heart failure or individuals who
have had a heart transplant consider to be the most important factors in relation to the service, in order toinform decisions about future service provision.
Summary of focus group findingsThe research was conducted with both heart transplant and heart failure patients. The findings
highlighted commonality of views in both groups on what matters most when facing and undergoing heartsurgery, especially transplant surgery. Their experience of being treated for a heart condition was always asignificant life event having a considerable impact on their lives as well as those of their families, affectingthem physically, emotionally, socially and financially. Consequently how and by whom their treatment washandled was of utmost importance and great trust was invested in specialist hospital care. Almost withoutexception, they perceive NHS provision in terms of clinical care for heart patients to be first-class. Survivalwas the priority, but it was hard for the focus group participants to make judgements about the means bywhich this is delivered. Many assumed that the clinical aspects of their treatment are delivered with thehighest level of skill and expertise.
In this context, participants highlighted other factors with which they are more familiar as indicatorsor the overall quality of the service. The top four of these in order are:
• being treated as a whole person• availability of support staff, especially nurses, with an open attitude to helping and advising
patients• good and appropriate explanations of what to expect• good follow up support form the unit/hospital after treatment
In terms of the other factors explored within the research:
• geographical accessibility of the unit/hospital is only an issue when there is a choice oflocationand all other things are equal
• patient support groups are generally not valued during treatment (patients prefer to seeksupport more informally), but may be more useful during longer-term rehabilitation
• all other factors were considered relatively or not at all important
Appendix IV provides a complete record of the focus group feedback.
In addition to the focus group the following summary provides feedback from letters, telephone callsand the patients’ meeting held in GRI.
6.3. Other patient views6.3. Other patient views6.3. Other patient views6.3. Other patient views6.3. Other patient viewsTo date there have been 10 letters received from transplant patients or their relatives. The meeting
held on 28 October 2003 was attended by 22 patients and relatives. The issues raised are summarisedunder recurrent themes.
AccessibilityThe impact of travelling long distances to hospital was highlighted by patients and carers. In general
the Scottish weather was highlighted as a problem when travelling in the winter. The cost of travel to thepatient and their family was also highlighted and the need for overnight stays adding to the cost and timerequired.
Distance travelled could increase patients’ anxiety levels, especially while on the waiting list. Travellingto hospital for treatment and follow-up was noted as ‘exhausting’ and one patient recounted the ‘terrible,

Cardiothoracic transplantation review
page 42
frightening ordeal driving from Aberdeen to Newcastle’ when they were ill. It is often necessary for relatives/carers to provide transport for hospital appointments and also to accompany patients. This required thecarers to take time off work and make arrangements for other dependents e.g, children, elderly parents.
Patients with disabilities had additional problems with accessibility, e.g, the need for a wheelchair. Insome cases a few patients were unfit to travel by air for the transplant operation, therefore requiring transportby road. One patient raised the question ‘does the need for extra travel affect survival after transplant?’
Excellence of care provided in GlasgowPraise for the care at Glasgow and the quality of the information provided by the unit were highlighted
in all the letters received. The security of being familiar with the unit and the staff was an important factor,especially the relationships that have developed between staff and patients/relatives.
Scottish unit for Scotland/politics behind closureSeveral patients noted that there were political reasons for maintaining the unit in Glasgow citing
devolved health, the fact that MSPs had originally agreed to the unit reopening and suggesting that MSPsshould have learnt lessons from the previous closure of the unit. The cultural differences between Scottishand English populations were highlighted as a reason for having a Scottish unit. Ensuring equal access forScottish patients was important. One patient suggested that Scotland as a nation should have its own unit,and that Scottish taxpayers had a right to a Scottish unit. One patient asked ‘billions of pounds are spent onthe NHS, why does none of it reach patients?’
It was generally suggested that there must be political and financial reasons for considering closure ofthe unit as patients found it difficult to believe that SEHD would want to close such an ‘excellent unit’ andfelt that SEHD should just accept the cost of running the unit in Scotland. In relation to funding, concernover the charitable money that had been raised specifically for the Scottish unit was raised.
The known high incidence of heart disease in Scotland was another justification for retaining a Scottishunit. Another question was whether, if the Unit were closed, the number of Scottish patients transplantedwould be in proportion to the number of Scottish donors if all transplants were provided in England.
Review processThere was general discontent regarding the review process, with some patients stating that they were
unaware that a review would take place following assurances given to them about the future of the unitwhen it was reopened. The agreed options shared with the patients were felt to be biased towards closingthe unit.
There were suggestions that the review process should take into consideration the possibility of takingreferrals for heart transplants from Ireland and the North of England. There was also a concern that if theunit closed and patients had to be transplanted in England that it would take too long to retrieve organsfrom Scottish donors.
Regrettably, the review process had caused added stress for patients and families and the constantworry of possible closure was decreasing the quality of patients’ lives.
To summarise, the patients’ and relatives’ views from the meeting at GRI and letters received indicatedoverwhelming support to for keeping the Scottish unit open. Some patients went as far as to say that if itwasn’t for the unit they would not be here today, and felt that closure would take away their ‘safety net’.
6.4 Summar6.4 Summar6.4 Summar6.4 Summar6.4 Summary of patient/public viewsy of patient/public viewsy of patient/public viewsy of patient/public viewsy of patient/public views
The focus groups were extremely useful in highlighting the topics patients with heart disease considerto be important in general terms in the provision of a cardiothoracic transplantation service and provided auseful platform from which to determine the issues that need to be considered when evaluating a service ofthis type. Indeed, the commonality of views between both patient groups lends strong support to theirvalidity.

Cardiothoracic transplantation review
page 43
The desire for specialist hospital care and the implicit wish to be treated by professionals who understandthe specific needs of patients cannot be underestimated and was common to all the groups who participatedin the exercise. This was seen to apply not only to the surgeons and medical consultants but to the wholeteam caring for the patient, including the follow-up period once discharged from the acute hospital setting.
The feedback received through letters and the meeting with patients and relatives at Glasgow RoyalInfirmary brought to light more specific issues related to concerns for the future for the Glasgow unit.Although the comments received at the meeting and in correspondence reflected personal concerns overfuture care provision, they have real value and are important to the review process.
It is worth mentioning in particular the difficulties that travelling long distances cause not only thepatients, but also their familes and carers, and that this may impose a financial as well as physical burden onthem. It must be noted that the Glasgow cardiothoracic transplant unit was praised extensively for the careand treatment it provides by all the patients and people who contributed to this review.

Cardiothoracic transplantation review
page 44
7.7.7.7.7. Outcomes/qualityOutcomes/qualityOutcomes/qualityOutcomes/qualityOutcomes/quality
The following information is from The Royal College of Surgeons of England Clinical EffectivenessUnit, UK National Audit of Intrathoracic Transplantation, end of year report from the Audit Steering Groupto the National Specialist Commissioning Advisory Group (NSCAG) September 2003.
7.1. Adult heart transplantation7.1. Adult heart transplantation7.1. Adult heart transplantation7.1. Adult heart transplantation7.1. Adult heart transplantationDuring the study period 1,439 transplants were reported. The outcome at 30 days was known for all
but 3 transplants. Overall, the unadjusted 30 day mortality remains unchanged from the last report at12.1% (95% confidence interval 10.4% to 14.0%). This is slightly higher than the 7.6% adult (18+ years)mortality rate reported by the United Network for Organ Sharing (UNOS), although four of the eightcentres encompass this value within their 95% confidence intervals (UNOS data are not adjusted for riskfactors).
Papworth continues to be the centre showing the best overall performance with a significantly lower30 day mortality rate compared to other centres, both with and without risk adjustment (smallest centreeffect). For the period since April 2000 the effect was less apparent, partly due to the smaller sample sizebut also because the mortality rate increased slightly. There was no evidence of significant variation betweencentres for this latter period.
The plateau in mortality rate observed at Newcastle appears to have continued, although furthertransplants still need to be accrued before this can be confirmed or otherwise. Unfortunately 11 of the 13transplants undertaken at Newcastle since January 2002 were not included in the risk adjusted analyses dueto missing data returns.
Results at Sheffield, Birmingham and Manchester continue to show a trend towards lower than expectedmortality rates, both with and without risk adjustment, and results at Harefield remain consistent with thenational trend.
Both the adjusted and unadjusted mortality at St George’s remain unchanged from the previousreport, as the St George’s transplant programme ceased in September 2000. Results at Glasgow since theprogramme was re-established in September 2001 are in line with the national overall 30 day mortality rate.
Continuous monitoring of risk adjusted mortality with boundaries aimed at detecting a 50% increasein risk identified only one centre (St George’s) with results worse than expected (the chart reached theupper ‘increased risk’ boundary when the transplant programme closed). Papworth was the only centre tocross the lower boundary, confirming that performance at Papworth was as good or better than expected.Charts for the other centres remain between the boundary lines, indicating that monitoring should continue.
30 day mortality after adult heart transplantation by centre unadjusted for patient riskTable 12
Centre No. of cases No. of deaths Mortality rate 95% CI Odds ratio
Newcastle 206 34 16.5 11.7 – 22.3 1.43Sheffield 102 8 7.8 3.4 – 14.9 0.62Papworth 300 23 7.7 4.9 – 11.3 0.60Harefield 272 36 13.2 9.4 – 17.9 1.11St George’s 124 23 18.6 12.1 – 26.6 1.65Birmingham 147 14 9.5 5.3 – 15.5 0.76Manchester 137 15 10.9 6.2 – 17.5 0.89Glasgow 148 21 14.2 9.0 – 20.9 1.20All centres 1436 174 12.1 10.4 – 14.0 1.00

Cardiothoracic transplantation review
page 45
Risk adjusted 30 day mortality after adult heart transplantation by centreTable 13
Centre Fixed centre effect
Newcastle 0.17Sheffield -0.41Papworth -0.43Harefield 0.04St George’s 0.80Birmingham -0.16Manchester -0.12Glasgow 0.12
7.2. Adult lung transplantation7.2. Adult lung transplantation7.2. Adult lung transplantation7.2. Adult lung transplantation7.2. Adult lung transplantation946 adult lung transplants were identified. One transplant was excluded because the 30 day outcome
was unknown. The overall 30 day mortality for the adult lung transplant programme as a whole (bilateral-sequential, single and heart/lung transplants combined) was 13.4% (95% confidence interval 11.3% to15.8%), which is higher than that reported by UNOS for their lung programme (7.1%), but less than theirreported 30 day mortality after heart/lung transplantation (19.4%). There was also some evidence to suggestmortality rates have improved over the time. Overall unadjusted mortality rates were similar across centresbut after risk adjustment the fixed effect analysis suggested St George’s results were weakly divergent.However, this was not confirmed by the empirical Bayes analysis, which suggested that there was no significantvariance between centres.
Newcastle has had consistently good results throughout the audit period with fewer deaths overallthan predicted by the risk model. Harefield, after an initial run of better than expected results, has performedbroadly in line with expectation. Papworth also performed better than expected to mid to late 1996;although in contrast to their adult heart transplant programme, there was then a gradual decline to mid1999. This was followed by another period of lower than expected mortality, and since Autumn 2000 theirresults, both with and without case-mix adjustment, have been broadly in line with expectation. Reasonsfor this fluctuation are unclear and were not explained by differences in case-mix.
Manchester, Birmingham and Sheffield performed similarly. All had an initial run of poor results,which was followed by a period with far fewer deaths than expected. At Manchester, much of thisimprovement was due to case-mix, as they transplanted fewer high-risk patients than other centres.
Continuous monitoring of risk adjusted mortality for Newcastle and Harefield would have confirmedthat results at these centres were as expected. Sequential monitoring results for other centres remaininconclusive, insofar as the neither the upper nor lower boundary lines have been crossed and monitoringshould continue.
30 day mortality after adult lung transplantation by centre unadjusted for patient riskWhole audit periodTable 14
Centre No. of cases No. of deaths Mortality rate 95% CI Odds ratio
Newcastle 201 18 9.0 5.3 to 13.8 0.63Sheffield 28 4 14.3 4.0 to 32.7 1.07Papworth 266 39 14.7 10.6 to 19.5 1.11Harefield 229 32 14.0 9.7 to 19.2 1.05St George’s 47 10 21.3 10.7 to 35.7 1.74Birmingham 58 10 17.2 8.5 to 29.5 1.34Manchester 102 13 12.7 6.9 to 20.8 0.94Gt Ormond St 14 1 7.1 1.8 to 33.9 0.50All centres 945 127 13.4 11.3 to 15.8 1.00

Cardiothoracic transplantation review
page 46
Risk adjusted 30 day mortality after adult lung transplantation by centreWhole audit periodTable 15
Centre Fixed centre effect
Newcastle -0.28Sheffield 0.02Papworth 0.07Harefield -0.09St George’s 1.00Birmingham 0.16Manchester -0.13Gt Ormond St -1.00
7.3. Paediatric heart transplantation7.3. Paediatric heart transplantation7.3. Paediatric heart transplantation7.3. Paediatric heart transplantation7.3. Paediatric heart transplantation176 paediatric patients received a first transplant during the study period and the outcome at 30 days
was known for all transplants. Results at individual centres and overall are similar to those reportedinternationally. The 30 day unadjusted mortality varied from 3.8% (95% confidence interval 0.4% to 13.0%)at Newcastle to 15.2% (95% confidence interval 5.1% to 31.9%) at Harefield. Great Ormond Street reporteda 5.8% (95% confidence interval 1.9% to 13.1%) 30 day mortality. Overall, the mortality rate was 7.0%(95% confidence interval 3.6% to 11.9%), but there has been a steady decline over time from a high of35% in the first year to an average 3.9% thereafter.
30-day mortality after paediatric heart transplantation by centre unadjusted for patient riskWhole audit periodTable 16
Centre No. of cases No. of deaths Mortality rate 95% CI
Newcastle 5 1 20.0 0.5 to 71.7Papworth 4 0 0.0 0.0 to 60.3Harefield 9 2 22.2 2.8 to 60.0Gt Ormond Street 24 4 16.7 4.7 to 37.4All centres 42 7 16.7 6.9 to 31.4
7.4. Paediatric lung transplantation7.4. Paediatric lung transplantation7.4. Paediatric lung transplantation7.4. Paediatric lung transplantation7.4. Paediatric lung transplantationThe paediatric lung transplant programme is very small with just 42 grafts reported since the audit
began. The programme appears to be in decline - the last paediatric lung transplant was reported in August2001. 27 of 42 grafts (64%) were heart/lung procedures and the 30 day mortality for the group as a wholewas 16.7% (95% confidence interval 6.9% to 31.4%).
30 day mortality after paediatric lung transplantation by centre unadjusted for patient riskWhole audit periodTable 17
Centre No. of cases No. of deaths Mortality rate 95% CI
Newcastle 53 2 3.8 0.4 – 13.0Harefield 33 5 15.2 5.1 – 31.9Gt Ormond Street 86 5 5.8 1.9 – 13.1All centres 172 12 7.0 3.6 – 11.99
7.5. Interpretation of data7.5. Interpretation of data7.5. Interpretation of data7.5. Interpretation of data7.5. Interpretation of dataThe interpretation of results presented in this report is not easy. There are several caveats:

Cardiothoracic transplantation review
page 47
• some of the analyses are unadjusted for risk factors• risk adjustment (when present) is always incomplete and inadequate• there were multiple comparisons, which incorporates dangers related to performing multiple
statistical tests, and risks obtaining ‘chance’ findings• we cannot take account of differences in the management of patients on the waiting list for
intrathoracic transplantation or differences in mortality later in the post-transplant period.
Where results are unadjusted for risk factors, interpretation should proceed with extreme caution aswith comparisons with data from other registries, which may not have rigorous data validation procedures.Furthermore, in many analyses the number of transplants considered are relatively small and estimates willnecessarily be imprecise.
An analysis of the potential causes of the differences between the centres requires further work thatcan only be done with a collation of audits from individual cardiopulmonary transplant centres. Until this isundertaken, it would be inappropriate to go beyond the conclusions that are presented in this report.

Cardiothoracic transplantation review
page 48
8.8.8.8.8. Options appraisalOptions appraisalOptions appraisalOptions appraisalOptions appraisal
This section sets out the options and criteria agreed by the review group at the meeting held on 9October 2003 and an explanation of the options appraisal process and results.
8.1. Options8.1. Options8.1. Options8.1. Options8.1. Options1 Maintain the status quo
Retain full adult heart transplantation service in Glasgow, obtain all paediatric cardiothoracictransplantation from Newcastle and Great Ormond Street and adult lung and heart/lung transplantationfrom Newcastle, Papworth and Harefield. Provide only existing range of cardiac surgery and cardiologyprocedures in Glasgow and obtain other elements of a comprehensive advanced heart failure service - suchas VADs - from English designated sites - Papworth, Newcastle, Harefield and Great Ormond Street.
2 Extend Glasgow service to include advanced heart failureRetain full adult heart transplantation service in Glasgow as an integral component of a modern
comprehensive advanced heart failure service1. Obtain paediatric cardiothoracic transplantation fromNewcastle and Great Ormond Street2.
3 Extend Glasgow service to include advanced heart failure and lung transplantationRetain full adult heart transplantation service in Glasgow as an integral component of a modern
comprehensive advanced heart failure service and expand to include thoracic transplants. Obtain paediatriccardiothoracic transplantation from Newcastle and Great Ormond Street.
4 Decommission heart transplant in Glasgow and transfer to NewcastleCease to provide any aspects of adult heart transplantation in Glasgow and obtain full adult and
paediatric cardiothoracic transplantation service (including organ retrieval, specialist assessment, transplantsurgery and follow up care) from Newcastle. Develop cardiac services in Glasgow to provide an extendedadvanced heart failure service (including provision of specialist interventional cardiology, artificial heartassist devices in appropriate circumstances and specialist cardiac surgery).
5 Decommission heart transplant in Glasgow and transfer to other English centresCease to provide any aspects of adult heart transplantation in Glasgow and obtain full adult and
paediatric cardiothoracic transplantation service (including organ retrieval, specialist assessment, transplantsurgery and follow up care) from one or more of the English cardiothoracic transplantation centres. Developcardiac services in Glasgow to provide an extended advanced heart failure service (including provision ofspecialist interventional cardiology, artificial heart assist devices in appropriate circumstances and specialistcardiac surgery).
6 Transfer adult heart transplant surgery service to Newcastle but retain satellite adult heart transplantationcentre in Glasgow
Cease heart transplantation in Glasgow and obtain adult cardiothoracic transplantation surgery andfull paediatric cardiothoracic transplantation service from Newcastle. Retain specialist transplantation expertisein Glasgow to provide adult heart transplantation assessment and follow up in Glasgow. Develop cardiacservices in Glasgow to provide an extended advanced heart failure service (including provision of specialistinterventional cardiology, artificial heart assist devices in appropriate circumstances and specialist cardiacsurgery).
7 Transfer adult heart transplant surgery service to English centres but retain satellite adult hearttransplantation centre in Glasgow
Cease heart transplantation in Glasgow and obtain adult cardiothoracic transplantation surgery andfull paediatric cardiothoracic transplantation service from one or more of the English cardiothoracictransplantation centres. Retain specialist transplantation expertise in Glasgow to provide adult hearttransplantation assessment and follow up. Develop cardiac services in Glasgow to provide an extendedadvanced heart failure service (including provision of specialist interventional cardiology, artificial heart

Cardiothoracic transplantation review
page 49
assist devices in appropriate circumstances and specialist cardiac surgery).
8.28.28.28.28.2. . . . . Non financial benefitsNon financial benefitsNon financial benefitsNon financial benefitsNon financial benefitsCriteria
The 16 criteria were divided into structure, process and outcome of care and also impact on non-transplant services.
No. Criteria DefinitionStructure of care
1 Attract and retain skilled staff The availability of the full range of skilled staffand the arrangements for sustainability includingsuccession planning. This will include medical,nursing, administrative staff and alliedhealth professionals.
2 Physical infrastructure The actual set-up for the service, from thebuildings to the organisational structure.
3 Support from other specialties Support from wider specialities. An option thatinvolves the advanced heart failure serviceincluding transplantation in a multi-speciality siteis more robust than an option that hasheart transplantation remote from othersimilar services.
4 Support from non-NHS services Non-clinical support. Options should be assessed(e.g. social work) on the extent to which the full needs of patients
and carers are addressed for example:·5 Accommodation for patient/relatives accommodation for both patients and their
carersfacilities provided to care for the full range of
needs of patients, such as social work support.
Process of care6 Continuity of care ‘Continuity of care is a multi faceted concept used in
a series of different ways including continuity acrossorganisational boundaries; continuity of personnel;continuity of information and continuity over periodsof time.’ (Freeman et al, 2000,http://www.sdo.lshtm.ac.uk/continuityofcare.htm)
7 Flexible capacity to meet changes The service needs to be adaptable inin number of patients order to accommodate changes in the provision
of the service as and when required. Optionsshould be scored in relation to the relative easewith which they could accommodate changes in:
Case-mix and activity 8 Capacity to adapt to new Technology & techniques
technology/techniques Comprehensiveness in comparison toGlasgow unit (for example further developmentin cardiac surgery (artificial cardiac
Cardiothoracic transplantation review
page 50
No. Criteria DefinitionProcess of care (continued)
support implantation devices) and improvementsin medication (e.g. beta blockers) which willreduce the need for cardiothoracictransplantation).
9 Ease of access to service for Clinical and social elements of the distance thatpatient/family patients and their family require to travel and
the ease of access to the hospitals is animportant consideration in the future provisionof cardiothoracic transplant services.
10 Time between retrieval of organs The distance that the retrieval team withand transplant donor organ has to travel.
11 Choice Patients and their family have a choice indecisions about the care that they receive,including assessment, surgery and follow-up,and where this care is delivered.
Outcome of care12 Short-term outcomes to It is regarded that cardiothoracic transplant
discharge (e.g. complications) surgery including effectiveness of retrievalshould be effective in terms of patientoutcomes including mortality and morbidity.Clinical effectiveness should also be looked at
13 Long-term outcomes (e.g. survival) in relation to the patient’s follow-upcare/treatment. In assessing options the fullspectrum of care should be taken into accountfrom initial assessment through surgery tolong term follow-up. A component ofclinical effectiveness is the availability of the fullrange of multidisciplinary specialist skillsrequired, another is continuity of care.Training arrangements for all staff andinvolvement in research would also beincluded under clinical effectiveness.
‘The extent to which specific clinical interventions, when deployed in the field for a particular patient orpopulation, do what they are intended to do - that is, maintain and improve health and secure the greatestpossible health gain from available resources.’ NHS Executive (1996).
Impact on non-transplant services14 Impact on other heart services Options should be assessed in relation to the
in Scotland wider impact these would have on other servicesif the option were to be implemented, such ascardiac services, surgical theatres, intensivecare, high dependency units and out-patientclinics. It would also include impact oncardiology services and primary care.

Cardiothoracic transplantation review
page 51
Impact on non-transplant services (continued)No. Criteria Definition
The possible impact on retrieval teamsand ambulance services should also be taken into consideration.
15 Impact on organ retrieval There are constraints to organising andin Scotland conducting retrieval over large distances,
especially when the geography of Scotland istaken into account. Options should be assessedin relation to the impact there would be onorgan availability (for example any optionsthat provide retrieval arrangements from abase south of the border may lead to fewerorgans being retrieved successfully).
16 Academic dimension The impact on opportunities for trainingand research should be assessed.
8.38.38.38.38.3. . . . . WWWWWeighting and scoring the non-financial aspectseighting and scoring the non-financial aspectseighting and scoring the non-financial aspectseighting and scoring the non-financial aspectseighting and scoring the non-financial aspects
OutlineHaving agreed the criteria, a meeting of the advisory group was convened with the specific purpose of
(i) weighting the criteria, and (ii) scoring each of the options against the criteria following a discussion of theevidence. Scoring was undertaken individually without further discussion and option 2 emerged as thepreferred option. This conclusion appears to be robust under any reasonable assumptions about weights.
MethodThe advisory group agreed the criteria and options to be used in the exercise and the next stages were
(i) to consider how important the criteria are relative to each other and to weight them and (ii) to considerthe evidence for each option against each criterion and then to score their likely performance in eachrespect. The majority of members were able to attend and those who could not had the opportunity tosubmit written comments to the chairman.
NSD staff prepared briefing papers that were circulated in advance of the meeting. The key elementswere as follows:
(i) Explanation of the process of options appraisal to ensure that all members were aware of how theiranswers would feed into the exercise.
(ii) Proposed weights for the criteria. This was not an attempt to dictate to the group but to suggesta set of weights that were open for discussion. It was hoped that the majority of these would not becontentious and hence that this would ensure the group’s time was used to best effect.
(iii) Evidence gathered from the different plausible cardiac transplant centres that could be used relatingto the different criteria. Four pieces of evidence were available to members in addition to their personalexperience. These were as follows:
• evidence from a previous UK-wide exercise conducted by NSCAG in 2002 which wassupplemented with additional questions to each of the centres (while this was generally veryhelpful it was unfortunate that replies were not available from all of the English centres. Datawere available for Glasgow, Newcastle, Harefield and Manchester. Fortunately, members ofthe advisory group were able to use their experience of the different centres to fill in the main

Cardiothoracic transplantation review
page 52
gaps and this was not thought to have adversely affected the exercise).• a written submission from the clinical team at the Glasgow centre
• a report on the views of patients/carers and staff at the Glasgow centre derived from focusgroup meetings
• a presentation at the meeting by Professor Dargie, cardiologist at the North Glasgow AcuteTrust and University of Glasgow, regarding the role and potential of the advanced heart failurecentre envisaged under options 2 to 7.
In addition, members were invited to visit the Glasgow unit on the day before the advisory groupmeeting.
(iv) Plan for scoring the options and analysing the responses. Members were asked to score eachoption against each criterion on a scale from 0 to 100 where 100 represented the best imaginable serviceand 0 the worst imaginable service from the point of view of the population of Scotland. Members weretherefore being asked to put aside any loyalties they had to particular institutions and as the subsequentreport will show, they did this very successfully. The stated intention was simply to aggregate scores acrossthe group and report total and average weighted scores for each option. Where there was a significantdisagreement the majority view would be used in the ‘baseline analysis’ and the minority view in a sensitivityanalysis to see what difference this made to the conclusion. This analysis was not undertaken at the meetingand a final meeting of the advisory group was convened for 22 January 2004 to consider the analysis anddraft report.
At the meeting itself, the weights were discussed first. While most people agreed with most of theweights proposed, alternative views were put forward. These were noted and have been considered inmore detail in the sensitivity analysis. The group then considered how to score the options. The approachused was to take each criterion in turn and discuss all of the evidence available.
8.4. Results8.4. Results8.4. Results8.4. Results8.4. Results
Weighting the criteriaThe papers circulated by NSD staff in advance of the meeting proposed a classification system for the
criteria with three categories of importance; high, medium and low. The suggested allocation of criteria tocategories was as follows:
HighAbility to attract and retain staffSupport from other specialtiesContinuity of careTime between organ retrieval and transplantShort-term outcomes (to discharge)Long-term outcomesImpact on organ retrieval in Scotland
MediumPhysical infrastructureFlexible capacity to cope with changes in patient numbersCapacity to adapt to new technology/techniquesEase of access for patient & familyImpact on other heart services in Scotland
LowAccommodation for patients and relativesSupport from non-NHS servicesChoiceAcademic dimension

Cardiothoracic transplantation review
page 53
It was proposed that each criterion in each group be given a weight as follows:
high importance 20medium importance 10low importance 5
In other words, the high importance category would be twice as important as the medium category,which in turn would be twice as important as the low category.
The main comments expressed that differed from this view were as follows:
• The criterion ‘academic dimension’ should carry more weight and should be at least in themedium category
• The criterion ‘choice’ should be at least in the medium category.
• The difference between the weights attached to each of the categories should be reducedfrom 20/10/5 to 15/10/8.
The following analysis has proceeded with the initial NSD proposals for the weights but the alternativesuggestions are fully considered in the section on sensitivity analysis.
Scoring the optionsAll members scored all of the options without any apparent difficulty. The process of discussing the
evidence before scoring appeared to be helpful, although time was limited.
Weighted scores for each optionThe following table shows the total and average weighted scores for each option.
Table 18
Options Definition Review Averagegroup score
1 Maintain the status quo 15,345 1,5352 Extend Glasgow service to include
advanced heart failure service (QHF) 16,415 1,6423 Extend Glasgow service to include
QHF & lung transplantation 14,058 1,4064 Decommission heart transplant & transfer
service to Newcastle 12,583 1,2585 Decommission heart transplant & transfer
service to other English centres 12,320 1,2326 Transfer heart transplant surgery to Newcastle
but retain satellite centre in Glasgow 8,760 8767 Transfer heart transplant surgery to English
centres but retain satellite centre in Glasgow 8,753 875
Option 2 received the highest weighted total points score. The Glasgow options (options 1, 2 and 3)scored higher than any others, followed by the options where all care would take place at an English site(options 4 and 5) with the options where care was shared between England and Glasgow receiving the

Cardiothoracic transplantation review
page 54
lowest scores (options 6 and 7).
The following table shows the total weighted score awarded by each person scoring for each option.
Table 19Options
Scorer 1 2 3 4 5 6 7
A 1,150 1,270 780 1,160 1,250 465 465B 1,340 1,665 1,490 1,425 1,240 825 815C 1,625 1,730 1,620 1,360 1,285 950 940D 1,435 1,455 1,390 1,048 885 745 740E 1,260 1,380 1,070 830 815 760 785F 1,700 1,765 1,715 1,390 1,645 913 930G 1,555 1,590 1,230 1,145 1,050 645 605H 1,570 1,640 1,353 1,270 1,280 1,210 1,195I 1,875 2,045 1,830 1,620 1,540 1,425 1,425J 1,835 1,875 1,580 1,335 1,330 823 853
This shows that all 10 members of the group scoring gave the most points to option 2.
Option 2 appears to be the preferred option in terms of non-financial benefits (costs have not beentaken into account here) so the final table in this section looks at how this option performed on eachcriterion to assess particular strengths and weaknesses. If this were the option that were eventuallyimplemented this information might help to ‘fine tune’ the option to maximise benefits. This table showswhere each group of scorers ranked option 2 compared to the other options.
Table 20 Review group
Criterion Option 2 rank Top rank option
1 12 13 14 15 1= 16 17 2 18 19 2 310 2 311 2 312 2 513 114 115 2 316 2 3
The advisory group saw option 2 as being the best option on 9 of the 16 criteria and did not rank itbelow second place on any criteria. When another option was preferred this was generally option 3 (5 casesout of 7, with options 1 and 5 getting one preference each).
The group agreed that option 2 was the second ranked option on the following criteria:
• option 7 - flexible capacity to meet changes in patient numbers within the current service.

Cardiothoracic transplantation review
page 55
• option 9 - ease of access for patient and family - option 3 came top because Scottish lungtransplant patients would also be treated in Glasgow.
• option 10 - time between retrieval of organs and transplant - option 3 came top, presumablyfor similar reasons.
• option 11 - choice - option 3 came top, presumably for similar reasons.
• option 12 - short-term outcomes - option 5 came top, presumably because historically someEnglish centres have achieved slightly higher results than Glasgow. However, as the advisorygroup now appears to have faith in the structure and process of care in Glasgow (judging fromthe scores) it seems reasonable to infer that expert opinion would support the view that Glasgowis now performing to the standard clinical peers would expect.
• option 15 - impact on organ retrieval in Scotland - option 3 was ranked first, presumablybecause of beneficial effect on lung retrieval in Scotland.
• option 16 - academic dimension - option 3 came top, presumably because this was seen asgiving one more aspect to academic work that could be carried out.
While option 2 is not the top ranked option on every criterion, this can be relatively easily understoodby the inclusion of lung transplant patients in option 3. The only other criterion is short-term outcomes. Itis recommended that NSD keep these data under regular review to ensure that the anticipated outcomesare being achieved and that Glasgow can offer the anticipated standards of care.
Sensitivity analysisThe analysis above has all been carried out on the basis of the original weighting system proposed by
NSD staff prior to the 9 December meeting. The various amendments proposed at that meeting weretested in a sensitivity analysis.
Change weights on categories of criteria from 20/10/5 to 10/8/5This makes very little difference to the rank order of results with option 2 coming first, followed by
options 1 and 3.
Change category of ‘choice’ and ‘academic dimension’ criteria from low to medium to highInitially these were given the lowest weights. Changing them to the medium weight category and
then to the high weight category made no difference to the rank order of results. The group felt that option3 scored a little higher than option 2 on both of these criteria. It was evident that the difference betweenoptions 3 and 2 was slightly smaller but this was not enough to change the ordering.
8.5. Conclusion8.5. Conclusion8.5. Conclusion8.5. Conclusion8.5. ConclusionThe options appraisal total weighted scores for non-financial benefits revealed a degree of consensus
amongst all of those involved that was not apparent at the start of the exercise. When considering non-financial benefits the following findings appear to command at least a consensus and near unanimoussupport:
• There was strong and consistent support for a full cardiac transplant service to remain inGlasgow
• There was a decisive rejection of carrying out pre- and post- surgery care in Glasgow with theprocedure itself being carried out in England
• Option 2 has highest weighted score but further analysis shows option 3 does well and shouldnot be completely ruled out as the way forward at some stage.

Cardiothoracic transplantation review
page 56
99999..... CostsCostsCostsCostsCosts
9.1 Current expenditure9.1 Current expenditure9.1 Current expenditure9.1 Current expenditure9.1 Current expenditureSection 4 ‘Current service for residents of Scotland’ outlined the current commissioning arrangements.
In summary, NSD has three service agreements for cardiothoracic transplantation with a total value ofapproximately £3.4 million. The split can be seen in Figure 12 which shows that 69% (£2.4 million) of thetotal funds are currently made available to NHS Greater Glasgow, North Glasgow University Hospitals Divisionto cover the costs of adult heart transplantation.
Cardiothoracic Transplant Funding 2003/04
69%
4%
27%
North Glasgow UniversityHospitals Papworth Hospital
Freeman Hospital
The planned activity in service agreements is outlined below. If expenditure in Glasgow is comparedwith planned activity, the unit costs of adult heart transplantation are high. The main reason for this variationdates back to when the Glasgow service was suspended in 2000. At that time the service agreement andfunding were based upon a service that was undertaking on average, 30 transplants a year. When theservice was re-established in September 2001, NSD was asked by the SEHD to ensure that a fully staffedcardiothoracic transplantation service was put in place to provide a sustainable service for residents ofScotland and to review the provision of the service two years after the service was re-established. Significantcapital and set-up costs were invested in 2001 to ensure that the service was able to meet the needs of thepopulation of Scotland. Annual revenue costs were increased from £1.7 million to £2.2 million based upona service that had a core team and infrastructure to undertake approximately 100 assessments and 30-35transplants a year along with appropriate follow-up for patients after transplant. Activity has, however, beenmuch lower than expected since the service was re-established. The unit has been performing on averageone transplant per month, i.e, less than half its capacity. The current service agreement is for 15 transplantsa year.
Figure 12
Activity%total%total%total%total%total %total%total%total%total%total
£000s£000s£000s£000s£000s fundingfundingfundingfundingfunding heartsheartsheartsheartshearts lungs & h/lungslungs & h/lungslungs & h/lungslungs & h/lungslungs & h/lungs totaltotaltotaltotaltotal activityactivityactivityactivityactivity
North Glasgow University HospitalsNorth Glasgow University HospitalsNorth Glasgow University HospitalsNorth Glasgow University HospitalsNorth Glasgow University Hospitals 2,365 69% 15 0 15 44%Papworth HospitalPapworth HospitalPapworth HospitalPapworth HospitalPapworth Hospital 139 4% 0 0 0 0%Freeman HospitalFreeman HospitalFreeman HospitalFreeman HospitalFreeman Hospital 907 27% 4 15 19 56%
3,411 100% 19 15 34 100%
Table 2

Cardiothoracic transplantation review
page 57
9.2. Benchmarking and costing of options9.2. Benchmarking and costing of options9.2. Benchmarking and costing of options9.2. Benchmarking and costing of options9.2. Benchmarking and costing of optionsAs highlighted in section 4, in addition to Glasgow, only Freeman Hospital Newcastle provided a
comprehensive cost profile (Annex V) for the provision of all or part of the required service for Scotland.NSD already had access to expenditure figures from the English National Specialist Commissioning AdvisoryGroup (NSCAG) which detailed the costs at cardiothoracic centres in England for 2003/04.
For the purpose of benchmarking, Figure 13 below compares the full unit costs of heart and lungtransplants in UK cardiothoracic transplant services for 2003/04. One word of caution is that these figuresare taken from service agreements which reflect the funding made available to the service for a plannedlevel of activity. This may not be the actual activity as explained in relation to the Glasgow service above.There may be a differencebetween the planned and the actual activity undertaken by a centre. The figureshave been adjusted to remove post transplant follow up costs and names of NHS Trusts have also beenremoved except for Glasgow.
Figure 13
0
50,000
100,000
150,000
200,000
Full Unit Cost £
Hospitals
Comparision of Full Costs 2003/04At Cardiothoracic Transplant Centres
Heart Transplant 99,455 64,527 54,404 115,846 71,732 49,481 125,015
Lung Transplant 145,868 94,639 79,792 169,907 105,208 72,572
A B C D E F G
Glasgow
Figure 13 shows that compared with other UK centres, Glasgow, with its planned activity level of 15transplants, has the highest unit costs. As discussed previously, this reflects the fact that the Glasgow serviceis geared towards an activity level of 30 heart transplants per year. If activity was at its previous level of 30per year, average unit costs per transplant would drop from £125K to approx £70K, comparable with othercentres in the UK. The financial viability of a transplant centre is directly related to activity levels becausethere is a minimum size of multi-disciplinary skilled team needed to provide a service whether it is for 10 or30 transplants. All smaller centres in the UK are currently closely monitoring their future sustainability in theface of diminishing organ availability and the impact of the working time directive.
9.3 Expected future numbers9.3 Expected future numbers9.3 Expected future numbers9.3 Expected future numbers9.3 Expected future numbers9.3.1 Cardiothoracic transplantation
As outlined above in section 3, given current trends, the future need for adult heart transplantation inScotland is assessed to be:
13-15 adult heart transplants per year8-12 adult heart/lung and lund transplants1-2 paediatric transplants

Cardiothoracic transplantation review
page 58
These have therefore been used as the planning figures on which future costs are based.
9.3.2 Advanced heart failureIn addition to transplantation, section 3 outlines assessed needs for severe heart failure services. The
key change in developing the existing cardiothoracic transplant services into advanced heart failure servicesis in providing different management options for patients in end stage heart failure rather than purelytransplantation. Possible treatments included cardiac resynchronisation therapy, advanced surgery andventricular assist devices.
New treatments are continually becoming available and need evaluation. The actual range of optionsavailable for the management of patients is therefore a dynamic situation and it might be appropriate for anadvanced heart failure centre in Glasgow to play a part within NHS Scotland in pioneering new techniquesand in taking part in clinical trials to evaluate services. Such a role would allow a planned approach to betaken in rolling out the availability of such services within Scotland to regional cardiac centres.
Due to the changing and evolving nature of mechanical assist devices available, it was difficult todetermine which particular ones might be part of an advanced heart failure service in Scotland at any onetime. If the service had been set up some years ago, it might have been appropriate for ICDs to be firstimplanted under the auspices of an advanced heart failure service but now these are very much part of theservice available at regional tertiary cardiac centres. It was decided that ICDs should therefore not beconsidered as a national component of the advanced heart failure service proposal.
A technology currently being developed is cardiac resynchronisation therapy (CRT) and the reviewconsidered that there were many advantages in CRT being undertaken in Glasgow in the immediate futurewith a likely roll-out to Edinburgh and Aberdeen once the technology was established and training hadtaken place. CRT was likely to be something that would be part of regional tertiary provision in future. As aresult, NSD guided those calculating costs for the cardiothoracic review to identify seperately costs for CRTso that this component of cost might be considered as a distinct element.
Lastly, another group of mechanical assist devices was considered: ventricular assist devices (VADs).These new devices are being evaluated in the UK at present as a bridge to transplantation. The clinical andcost effectiveness of VADs, both as a bridge to transplant and as a bridge to recovery, has not yet beenestablished, and the Department of Health currently recommends that VADs should only be provided underthe auspices of the current UK evaluation until the evaluation is complete. The review group endorsed thisrecommendation and costs of VADs have therefore been excluded from costing the options below, becausein all cases VADs are provided from the same three centres in England and the cost impact on every optionis the same.
9.4 Costing of options9.4 Costing of options9.4 Costing of options9.4 Costing of options9.4 Costing of options
9.4.1. Maintain the status quo - £3.6 millionThe current cost of this option is £3.4 million. The Freeman Hospital, Newcastle is however in negotiation
with all its commissioners to rebase the funded value of service agreements and is likely to require anadditional £200K from Scotland to reflect Scottish activity. This incresed amount has therefore been includedin costing all the options that involve transplantation being performed in Newcastle for consistency.
Est. costEst. costEst. costEst. costEst. costSerSerSerSerServicevicevicevicevice ProviderProviderProviderProviderProvider (£000)(£000)(£000)(£000)(£000)
Adult heart transplant Glasgow & other (option to refer) 2,365Advanced heart failure service English centresPaediatric cardiac transplant Freeman & GOS 162Heart/lung Freeman, Papworth & Harefield 1,087
3,6143,6143,6143,6143,614

Cardiothoracic transplantation review
page 59
9.4.2. Extend Glasgow service to include advanced heart failure - £3.9 million
This option involves retaining adult heart transplantation services in Glasgow as an integral componentof an extended modern advanced heart failure service. Glasgow submitted a comprehensive cost profilethat lays out the current staffing and infrastructure that is associated with the adult heart transplant serviceand also the extra resources required to undertake the elements of delivering an advanced heart failureservice. In effect there is only a marginal additional cost to adding advanced heart failure services to thecurrent service because the required staffing infrastructure is already supported through transplantation. Inaddition to transplantation this option provides in Glagow: specialist assessment of some 100 patients,assessment, transplantation and follow up for 15 heart transplant patients, complex heart surgery for 10patients and CRT for 5 patients. The cost profile for the Glasgow service is detailed in Appendix VI.
Est. costEst. costEst. costEst. costEst. costSerSerSerSerServicevicevicevicevice ProviderProviderProviderProviderProvider (£000)(£000)(£000)(£000)(£000)
Adult heart transplant Glasgow & other (option to refer) 2,365Advanced heart failure service Glasgow 336Paediatric cardiac transplant Freeman & GOS 162Heart/lung Freeman, Papworth & Harefield 1,087
3,9503,9503,9503,9503,950
Based upon the costs currently submitted and the caveats mentioned above, the estimated costs ofthis option are £3.9 million. This does not include any capital/set up costs which have been mentioned, butnot yet costed.
9.4.3. Extend Glasgow service to include advanced heart failure and lung transplantation – £4.4 million
This option was not considered appropriate at this point in time.
Est. costEst. costEst. costEst. costEst. costSerSerSerSerServicevicevicevicevice ProviderProviderProviderProviderProvider (£000)(£000)(£000)(£000)(£000)
Adult heart transplant Glasgow 2,365Advanced heart failure service Glasgow 336Paediatric cardiac transplant Freeman & GOS 162Heart/lung & lung Glasgow 1,573
4,4364,4364,4364,4364,436
The estimated costs of this option are £4.4 million. This does not include any capital/set up costswhich have been mentioned, but not costed, by Glasgow.
9.4.4 Decommission heart transplant in Glasgow and transfer to Newcastle - £4.6 million
If this option had involved the withdrawal of all advanced heart failure services from Glasgow, then thecost of this option would be approx. £2.4 million, because fixed costs would be removed. The optioninvolves, however, the Glasgow service being developed to provide elements of an advanced heart failureservice without transplantation. There are fixed costs involved in sustaining a team of specialists to providean advanced heart failure service with or without transplantation and conversely, there are economies ofscale in providing both together. The costs of providing advanced heart failure in this option therefore differfrom the previous options beacuse in this case the full, rather than the marginal additional costs, are required.This brings the cost of this option to an estimated £4.6 million.

Cardiothoracic transplantation review
page 60
Est. costEst. costEst. costEst. costEst. costSerSerSerSerServicevicevicevicevice ProviderProviderProviderProviderProvider (£000)(£000)(£000)(£000)(£000)
Adult heart transplant Freeman 1,138Advanced heart failure service Glasgow 2,200Paediatric cardiac transplant Freeman & GOS 162Heart/lung & lung Freeman 1,087
4,5874,5874,5874,5874,587
9.4.5 Decommission heart transplant in Glasgow and transfer to other English centres - £5.0 millionAgain as mentioned in 9.4.4 above, the cost of this option would be approx £2.8 million if the Glasgow
service was not required to provide elements of an advanced heart failure service.
Est. costEst. costEst. costEst. costEst. costSerSerSerSerServicevicevicevicevice ProviderProviderProviderProviderProvider (£000)(£000)(£000)(£000)(£000)
Adult heart transplant One or more English centres 1,600Advanced heart failure service Glasgow 2,200Paediatric cardiac transplant Freeman & GOS 162Heart/lung & lung Freeman 1,087
5,0495,0495,0495,0495,049
9.4.6 Transfer adult heart transplant surgery services to Newcastle but retain satellite adult hearttransplantation centre in Glasgow - £4.8 million
Both options 6 & 7 include an estimated cost of the marginal additional costs of retaining a satelliteheart transplant service in addition to elements of an advanced heart failure service in Glasgow. There was,however, a decisive rejection by the review group under the assessment of non financial benefits of carryingout pre- and post-surgery care in Glasgow with the procedure itself being carried out in an English centre.
Est. costEst. costEst. costEst. costEst. costSerSerSerSerServicevicevicevicevice ProviderProviderProviderProviderProvider (£000)(£000)(£000)(£000)(£000)
Adult heart transplant Freeman 1,138Advanced heart failure service Glasgow 2,400Paediatric cardiac transplant Freeman & GOS 162Heart/lung & lung Freeman 1,087
4,7874,7874,7874,7874,787
9.4.7 Transfer adult heart transplant surgery service to English centres but retain satellite adult hearttransplantation centre in Glasgow - £5.2 million
Est. costEst. costEst. costEst. costEst. costSerSerSerSerServicevicevicevicevice ProviderProviderProviderProviderProvider (£000)(£000)(£000)(£000)(£000)
Adult heart transplant One or more English centres 1,600Advanced heart failure service Glasgow 2,200Paediatric cardiac transplant Freeman & GOS 162Heart/lung & lung Freeman 1,087
5,0495,0495,0495,0495,049

Cardiothoracic transplantation review
page 61
9.5 Cost/benefit appraisal9.5 Cost/benefit appraisal9.5 Cost/benefit appraisal9.5 Cost/benefit appraisal9.5 Cost/benefit appraisal
The appraisal of the non–financial benefits ranked option 2 (extending the Glasgow service to includeadvanced heart failure) highest. In terms of costs, this option came second to option 1 (status quo) by£336K. i.e, NHS Scotland would have to invest an additional £336K revenue funding over current expenditureon cardiothoracic transplantation to implement this option.
Options Definition non financial fiancialcosts rank benefits rank
1 Maintain the status quo 2 12 Extend Glasgow service to include
advanced heart failure service (AHF) 1 23 Extend Glasgow service to include
AHF & lung transplantation 3 34 Decommission heart transplant &
transfer service to Newcastle 4 45 Decommission heart transplant &
transfer service to other English centres 5 66 Transfer heart transplant surgery to Newcastle
but retain satellite centre in Glasgow 6 57 Transfer heart transplant surgery to English
Centres but retain satellite centre in Glasgow 7 7
The appraisal of the costs and benefits of other options demonstrates that all the other options involveincreased costs and less benefit. As defined, therefore, these other options should not be considered furtherbecause they confer no additional benefit for extra costs. Therefore the two options that need to be comparedin relation to costs and benefits are only options 1 and 2. The additional benefits of option 2 in relation tothe marginal additional costs were considered by the review group to represent value for money. Hence thereview group’s recommendation is for option 2.
All the options except option 1, however, involved the development of cardiac services in Glasgowinto an advanced heart failure service. This was because the Scottish Executive Health Department plan forCHD recommended the development of such a centre in Glasgow. As described above there are costsassociated with maintaining the specialist team required for such a service because the staffing andinfrastructure costs are similar to those required for transplantation.
If, on the other hand, there was a total transfer of advanced heart failure services, including hearttransplantation, from Glasgow to English centres such that the current fixed costs of transplantation couldbe removed, there are potential material cost savings to be gained from referring activity to English Trustsdue to larger economies of scale. Such a withdrawal of service could potentially save £1.2 million perannum on current costs. This potential saving must, however, be weighed up against a number of otherfactors that affect the overall viability of services for residents of Scotland - including the wider provision ofcardiac surgical and cardiology services. An advanced heart failure centre in Glasgow provides a resourceand centre of expertise for Scotland, and is important in relation to training, research and development,and therefore the future sustainability of specialist cardiac services.
Moreover, the position in relation to UK cardiothoracic transplantation services remain dynamic, andthe following issues are likely to have an impact on the pattern of UK services over the next few years:
•the diminishing number of available organs potentially eroding the overall clinical and financial viabilityof smaller centres
•the impact on medical staffing rotas of compliance with the European Working Time Directive

Cardiothoracic transplantation review
page 62
•the new Consultant Contract•recruitment and retention difficulties•the evaluation of ventricular assist devices.
There are clearly a number of issues that require to be addressed within a UK context in order tomaintain the high quality, sustainable, accessible and clinically cost effective transplantation services neededthroughout the UK.
For residents of Scotland, option 2 proposes a modest investment in an extended service and keepsoptions open about future delivery of services in Scotland at a time when the model of service delivery forthe UK may change in the future. It also assists in the support of the wider Scottish cardiac programme; and,with an activity level of 100 assessments a year and around 30 advanced heart failure interventions, unitcosts are comparable with other UK centres.
Cardiothoracic transplantation review
page 63
10.10.10.10.10. ConclusionsConclusionsConclusionsConclusionsConclusions
10.1. Heart, heart/lung and lung transplantation are accepted clinically effective therapies in specificconditions.
10.2. Despite major developments in the pharmacological management of adult heart failure, cardiactransplantation remains the most effective treatment for selected patients with end-stage heart failure.
10.3. Lung transplantation is an effective procedure in chronic obstructive pulmonary disease, cysticfibrosis, primary pulmonary hypertension and pulmonary fibrosis.
10.4. Paediatric cardiothoracic transplantation continues to be a rare procedure. Paediatric hearttransplantation is an effective treatment option for infants and children with end-stage heart failureor complex congenital cardiac defects. Lung transplantation is occasionally used for infants and childrenwith congenital lung abnormality, primary pulmonary hypertension and cystic fibrosis. Patient survivalfor paediatric lung transplant patients appears to be similar or slightly higher than that seen in adultpatients.
10.5. There has been a steady decline in the number of adult heart transplants undertaken due toalternative therapies being increasingly available for ischaemic heart disease. This trend is likely toplateau or reverse in future as older people present later in life needing transplantation. The numbersof adult lung transplants and paediatric cardiothoracic transplants have remained fairly static. Thereis a growing caseload of congenital heart disease patients likely to require heart transplantation infuture.
10.6. There is a link between the volume of cases undertaken by a transplant centre and the clinicaloutcomes achieved for patients. In centres performing fewer than nine transplants per year, the riskof mortality is significantly higher than in centres performing nine or more transplants a year. Oncethe threshold of nine transplants was reached there did not appear to be improved survival withincreased numbers of operations.
10.7. The annual need for cardiothoracic transplantation for residents of Scotland over the next 5-10years is projected to be around:
13 -15 adult heart transplants8 -12 adult heart/lung and lung transplants1-2 paediatric heart, heart/lung and lung transplants
10.8. The actual number of transplants undertaken will depend on the availability of suitable donororgans.
10.9. In addition there are now some complex surgical procedures and mechanical heart assist devicesthat can provide a bridge to or an alternative to, heart transplantation for some people withsevereheart failure. The projected need for these procedures is around:
10-15 complex surgery5-10 cardiac resynchronisation therapy2-5 ventricular assist devices (currently only available within a UK evaluation).
10.10. Current outcomes achieved for residents of Scotland are comparable with the results achievedthroughout the UK. Results for paediatric cardiothoracic transplantation in Newcastle and GreatOrmond Street and for adult lung transplantation in Newcastle are among the best in the UK.

Cardiothoracic transplantation review
page 64
10.11. Possible future cardiothoracic transplantation and advanced heart failure services for residentsof Scotland could be provided from a range of centres in England and Scotland. Seven optionswere considered by the review group – listed in detail above – through a process of optionsappraisal.
10.12. The options appraisal total weighted scores for non-financial benefits revealed a degree ofconsensus amongst all of those involved. When considering non-financial benefits the followingfindings commanded at least a consensus and near-unanimous support:
• there was strong and consistent support for a full adult cardiac transplant service to remain inGlasgow
• there was a decisive rejection of carrying out pre- and post- surgery care in Glasgow with theprocedure itself being carried out in England.
Option 2 has highest weighted score but further analysis showed option 3 scored well and should notbe completely ruled out as the way forward at some stage.
10.13. Option 2 is the preferred option in terms of non-financial benefitsin terms of non-financial benefitsin terms of non-financial benefitsin terms of non-financial benefitsin terms of non-financial benefits.
10.14. The cost of this option is around £3.9 million a year. This compares to £3.6 million for thestatus quo and £4.4 million for option 3 – extending the Glasgow service to include both advancedheart failure and lung transplantation.

Cardiothoracic transplantation review
page 65
11.11.11.11.11. RecommendationsRecommendationsRecommendationsRecommendationsRecommendations
In keeping with the findings of the options appraisal, it is recommended that the option that scoredhighest in the options appraisal process should be implemented.
This involves:
• retention of adult heart transplantation service in Glasgow but as an integral component of anextended modern comprehensive advanced heart failure service
• no expansion of the Glasgow service into lung transplantation
• retention of paediatric cardiothoracic transplantation from Newcastle and Great Ormond Street
• retention of adult lung and heart/lung transplantation from Newcastle, Papworth, and Harefield
• retention of the option of referral to other UK centres such as Manchester for any aspects ofadult cardiothoracic transplantation.
The cost of this option is around £3.9 million a year, an increase of some £336,000 over current costs.
The option of further extension of the Glasgow service to include also lung transplantation should notbe completely ruled out as the way forward at some stage.
The main reason why an extension of the Glasgow service into lung transplantation was not consideredappropriate at this stage was because the outcomes achieved for residents of Scotland were excellent atpresent and there was clear clinical evidence of a link between volume of transplants undertaken by a centreand the outcomes achieved in lung transplantation.
Given the rapid developments in mechanical heart assist devices and the dynamic nature ofhighly specialised servcies such as cardiothoracic transplantation, the review concludes thatstrategic stocktakes of this service should take place every three years.

Cardiothoracic transplantation review
page 66
Appendix IAppendix IAppendix IAppendix IAppendix I Membership of Review GroupMembership of Review GroupMembership of Review GroupMembership of Review GroupMembership of Review Group
CARDIOTHORACIC TRANSPLANTCARDIOTHORACIC TRANSPLANTCARDIOTHORACIC TRANSPLANTCARDIOTHORACIC TRANSPLANTCARDIOTHORACIC TRANSPLANTAAAAATION REVIEW 2003TION REVIEW 2003TION REVIEW 2003TION REVIEW 2003TION REVIEW 2003
Remit:
To review current provision of cardiothoracic transplantation services for residents of Scotland (adultsand children) in the light of developing treatments for acute heart failure and to make recommendations tothe National Services Advisory Group on the future pattern of services required to meet the needs of residentsof Scotland for high quality, sustainable, accessible, clinically and cost effective cardiothoracic transplantservices.
Proposed membership of review group:
Professor John Wallwork (Chair) Chairman, UK Transplant Cardiothoracic Transplant Group,transplant surgeon
Mr Stephan Schueler President, International Society for Heart and Lung Transplantation,Freeman Hospital, Newcastle
Dr Nick Banner Consultant in cardiology and transplant medicine, HarefieldHospital
Mr Robert Craig Deputy Director of Operations, Harefield Hospital
Dr Geoffrey Carrol Medical Director, Specialist Health Services Commission for Wales
Dr Bill Gutteridge NSCAG
Mr Victor Tsang Consultant cardiothoracic surgeon, Adult Congenital HeartSurgery Service, University College London
Professor Henry Dargie Consultant cardiologist, North Glasgow University Hospitals Trust
Ms Jen Lumsdaine Transplant co-ordinator, Lothian University Hospitals NHS Trust
Mr Chris Rudge Medical Director, UK Transplant
Mr Brian Gorman Transplant Unit’s Patient Support Group
Ms Kate Adamson Scottish Association of Health Councils
Miss Katherine Collins National Services Division, Nursing Adviser, Review Lead
Dr Adam Bryson National Services Division, Medical Director
Mrs Deirdre Evans National Services Division, Director, Secretary of review group
Ms Carole Morton National Services Division, Project manager
Ms Carol Brown National Services Division, Project support

Cardiothoracic transplantation review
page 67
Appendix IIAppendix IIAppendix IIAppendix IIAppendix II Indications for cardiac transplantation candidacyIndications for cardiac transplantation candidacyIndications for cardiac transplantation candidacyIndications for cardiac transplantation candidacyIndications for cardiac transplantation candidacy33333
• Cardiogenic shock or low-output state requiring mechanical assistance (e.g. respirator, intraaorticballoon pump, ventricular assist device, total artificial heart) with, at worst, reversible end-organ damage.
• Refractory heart failure or low-output state requiring continuous inotropic support and invasivemonitoring.
• NYHA4 class III or IV symptoms with objective documentation of marked functional limitationand poor 12-mo prognosis despite optimal medical therapy (peak oxygen consumption <14mL/kg/min,documented progression of heart failure symptoms, clinical instability, or marked serial decline in peakoxygen consumption).
• Recurrent or rapidly progressive heart failure symptoms unresponsive to optimal dosage ofvasodilators and diuretics.
• Severe hypertrophic or restrictive cardiomyopathy with NYHA class IV symptoms.
• Refractory angina pectoris despite maximally tolerated dosage of beta-blockers, calcium channelblockers, and nitrates, not amenable to revascularization or transmyocardial laser revascularization due todistal vessel disease or severity of left ventricular dysfunction with severe ischaemic symptoms consistentlylimiting day-to-day activities, accompanied by objective evidence of myocardial ischaemia within the firsttwo stages of a standard Bruce exercise protocol.
• Recurrent symptomatic, life-threatening ventricular arrhythmias despite maximal antiarrhythmictherapy by all appropriate conventional medical and surgical modalities (multiple firings from an ICD5 fordocumented VT6 and VF7 or prolonged periods of documented electromechanical dissociation after ICDconversion of VT or VF).
• Cardiac tumours confined to the myocardium with a low likelihood of metastasis at time oftransplantation.
• Hypoplastic left heart syndrome.
• Complex congenital heart disease with progressive ventricular failure that is not amenable toconventional surgical repair or palliation.
• In infants, children, and adolescents, progressive deterioration in left ventricular ejection fractionor functional status despite optimal medical therapy, failure to grow secondary to advanced heart failuresymptoms, or a progressive rise in pulmonary vascular resistance that would be expected to precludetransplantation at a later date.
3 Source: Books@Ovid, Copyright © 2002 by Lippincott Williams & Wilkins, Eric J. Topol,Textbook of Cardiovascular Medicine
4 New York Heart Association5 ICD - Implantable cardioverter defibrillator6 VT – Ventricular tachycardia7 VF – Ventricular fibrillaion

Cardiothoracic transplantation review
page 68
Appendix IIIAppendix IIIAppendix IIIAppendix IIIAppendix III References References References References References
Alfieri, O., Maisanao, F. and Schreuder, J.J. ‘Surgical methods to reverse left ventricular remodelling incongestive heart failure’ American Journal of Cardiology 91 (9) (2003) pp. s81 - s87
Anderson, J.R. in Anderson, J.R. (ed.) Muir’s Textbook of Pathology (Edward Arnold, London, 1985), pp.15.6-16
Anyanwu, A.C. , Rogers, C.A. and Murday, A.J. ‘Intrathoracic organ transplantation in the UnitedKingdom 1995-99: results from the UK cardiothoracic transplant audit’ Heart, 87 (5) (2002) pp. 449 – 454
Anyanwu, A. and Treasure, T. ‘Prognosis after heart transplantation: transplants alone cannot be thesolution for end stage heart failure’ British Medical Journal 326 (7388) (2003) pp 509 - 510
Arnold, M. ‘Heart Failure’ in The Merk Manual 2nd Ed (2003) http://www.merk.com/pubs/mmanual_home2
Boucek, M.M. ‘The Registry of the International Society for Heart and Lung Transplantation: fourthofficial pediatric report 2000’ Journal of Heart and Lung Transplantation 20 (1) (2001) pp.39 - 52
Choi, Y.W. et al ‘Bronchiolitis Obliterans Syndrome in Lung Transplant Recipients’ Journal of ThoracicImaging 18(2) (2003) pp. 72 – 79
Colombani, P.M. et al ‘Pediatric Transplantation’ American Journal of Transplantation supplement, vol3 supp 4 (2003) pp. 53 - 63
Costanzo, M.R. et al ‘Selection and treatment of candidates for heart transplantation’ Circulation92(12) ) ) ) ) (1995) pp. 3593 – 3612
Degado, R.M. ‘The future of mechanical circulatory support ‘ Current Opinion in Cardiology 18 (3)(2003) pp.199 - 209
DeMeo, D. and Ginns, L.C. ‘Clinical Status of Lung Transplantation’ Transplantation 72 (11) (2001)pp. 1713 – 1724
Dudley, R. A. ‘Selective Referral to High-Volume Hospitals: Estimating Potentially Avoidable Deaths’JAMA 283 (9) (2000) pp. 1159 – 1166
Edwards, E.B. et al ‘The Effect of the Volume of Procedures at Transplant Centers on Mortality afterLiver Transplantation’ New England Journal of Medicine 341 (27) (1999) pp. 2049 – 2053
Foody, J.M. et al ‘Beta- blocker therapy in heart failure: scientific review’ JAMA 287 (7) (2002) pp.883 - 889
Freedom, R.M. and Nykanen, D.G. in Topol, E.J. (ed.) Textbook of Cardiovascular Medicine (LippincottWilliams and Wilkins, 2002) http://pco.uk.ovid.com/lrpbooks/topol/textbook
Goldstein, D.J., Oz , M.C. and Rose, E.A. ‘Medical Progress: Implantable left ventricular assist devices’New England Journal of Medicine 339(21) (1998) pp. 1522 - 1533
Groth, C.G. ‘Presidential Address 2002: organ transplantation as a patient service worldwide’Transplantation 75 (8) (2002) pp. 1098 -1100
Grover, F.L. ‘ Thoracic Transplantation’ American Journal of Transplantation vol 3 supp 4 pp. 91 - 102

Cardiothoracic transplantation review
page 69
Hertz, M.I. et al ‘The Registry of the International Society for Heart and Lung Transplantation: NineteenthOfficial report ‘ Journal of Heart and Lung Transplantation 21 (2002) pp. 950 – 970
Hosenpud, J.D. et al ‘Effect of diagnosis on survival benefit of lung transplantation for end-stage lungdisease’ Lancet 351(9095) (1998) pp. 24
Hosenpud, J.D. et al ‘The effect of transplant center volume on cardiac transplant outcome: A reportof the United Network for Organ Sharing Scientific Registry’ JAMA 271 (23) (1994) pp. 1844 - 1849
Hunt, S.A. et al ‘ACC/AHA guidelines for the evaluation and management of chronic heart failure inthe adult.’ Journal of Heart and Lung Transplantation 21(2) (2002) pp. 189 – 203
Jimmy, K.F. and Yacoub, M.H. ‘Bridge to recovery with the use of left ventricular assist device andclenbuterol’ Annals of Thoracic Surgery 75 (6) (2003) pp. s36 – s41
Jessop, M. and Brozena, S . ‘Medical Progress: Heart Failure’ New England Journal of Medicine 348 (20)(2003) pp. 2007 - 2018
Kichuk-Chrisant, M.R. ‘Children are not small adults: some differences between pediatric and adultcardiac transplantation’ Current Opinion in Cardiology 17(2) (2002) pp. 152 - 159
Lutton, S.R., Ratliff, N.R. and Young, J.B. in Topol, E.J. (ed.) Textbook of Cardiovascular Medicine (LippincottWilliams and Wilkins, 2002) http://pco.uk.ovid.com/lrpbooks/topol/textbook
Mitchell, .BL. ‘ Abnormal Heart Rhythms’ The Merk Manual 2nd ed. (2003) http://www.merk.com/pubs/mmanual_home2
Pinski, S.L. and Peng-Shen ‘Implantable Cardioverter-Defibrillators’ in Topol, E.J. (ed.) Textbook ofCardiovascular Medicine (Lippincott Williams and Wilkins 2002) http://pco.uk.ovid.com/lrpbooks/topol/textbook
Renlund, D.G. and Taylor, D.O. in Topol, E.J. (ed.) Textbook of Cardiovascular Medicine (((((LippincottWilliams and Wilkins 2002) http://pco.uk.ovid.com/lrpbooks/topol/textbook
Rogers, C, Ganesh, J.S., Banner, N.R., Bonser, R.S. and van der Meulen, J. The Royal College of Surgeonsof England Clinical Effectiveness Unit. UK National Audit of Intrathoracic Transplantation. End of Year Report fromthe Audit Steering Group to the NSCAG, September 2003
Smits, J.M. et al ‘Mortality rates after heart transplantation: How to compare center-specific outcomedata?’ Transplantation 75 (1) (2003) pp. 90 - 96
Stevenson, L.W, and Rose, E.A, ‘Left Ventricular Assist Devices: Bridges to Transplantation, Recoveryamd Destination for Whom’ Circulation 108 (25) pp. 3059-3063
Stewart, K.C. and Patterson, G.A. ‘Current trends in Lung Transplantation’ American Journal ofTransplantation 1(3) (2001) pp. 204 - 210
Stewart, S. et al ‘Heart failure and the aging population: an increasing burden in the 21st century?’Heart 89(1) (2003) pp. 49 – 53
Ten Vergert, E.M. et al ‘ The effect of lung transplantation on health-related quality of life: a longitudinalstudy’ Chest 113 (2) (1998) pp. 358
Topol, E.J. and Van De Werf ,F.J. in Topol, E.J. (ed.) Textbook of Cardiovascular Medicine (LippincottWilliams and Wilkins 2002) http://pco.uk.ovid.com/lrpbooks/topol/textbook

Cardiothoracic transplantation review
page 70
Trulock, E.P. et al ‘ The registry of the international society for heart and lung transplantation: twentiethofficial adult lung and heart-lung transplant report 2003 ‘ The Journal of Heart and Lung Transplantation 22(6) (2003) pp. 625 – 635
Walker, Liddell, M. and Davis, C. ‘Extracorporeal Life Support – state of the art’ Paediatric RespiratoryReview 4 (2003) pp. 147 - 152
Warnica, J.W. ‘Heart Attack’ The Merk Manual 2nd Ed http://www.merk.com/pubs/mmanual_home2
White, H.D. in Topol ,E.J. (ed.) Textbook of Cardiovascular Medicine (((((Lippincott Williams and Wilkins,2002) http://pco.uk.ovid.com/lrpbooks/topol/textbook
Wren, C. and O’Sullivan, J.J. ‘Survival with congenital heart disease and need for follow up in adult life’Heart 85 (2001) pp. 438 - 443

Freeman Newcastle
ADDITIONAL RESOURCES REQUIRED (@2003/4 p&p)
WTE15 Transplant Programme
8 Transplant Programme
STAFF
MEDICAL:-Sp Registrar 1.00 76,241 76,241Consultant Microbiologist (2 Sessions) 0.18 15,124 15,124
SUB-TOTAL MEDICAL STAFF 1.18 91,365 91,365
ADMINISTRATIVE:-Transplant Co-Ordinator ( Grade H) 1.00 50,049 50,049A&C 3 1.50 24,669 24,669
SUB-TOTAL ADMINISTRATIVE 2.50 74,718 74,718
NURSING:-ITU - Grade G 1.00 38,460 38,460ITU - HCA 1.00 17,592 17,592
Wards (2.5 bed) / HDU (1.0 bed):-Grade E 6.50 167,980 83,990
Outpatients - Grade E 1.00 8,599 8,599
SUB-TOTAL NURSING 9.50 232,631 148,641
PARAMEDICAL:-Technicians (Echo, Heart /Lung) 2.33 76,923 76,923Physiotherapist - Snr II 0.50 14,670 14,670
SUB-TOTAL PARAMEDICAL 2.83 91,592 91,592
OTHER:-Psychology (3 sessions) 25,067 25,067Social Worker 0.50 17,500 17,500
SUB-TOTAL OTHER 0.50 42,567 42,567
ANCILLARY:-Portering 1.00 10,835 10,835Other 0.50 5,418 5,418
SUB-TOTAL ANCILLARY 1.50 16,253 16,253
TOTAL STAFF 18.01 549,125 465,135
NON-STAFF
Donor Organ Retrieval - Transport Cost (30 retrievals) 87,000 26,100Outreach clinics - additional costs 8,800 8,800Accommodation 43,200 16,056
Variable Costs of Activity :-15 Transplants @ £6431 96,465 51,44878 Assessments @ £415 32,370 16,185160 In Patient Follow-Ups @ £515 82,400 41,200632 O/Patient Attendances @ £32 20,224 10,112
SUB-TOTAL NON-STAFF 370,459 169,901
Overhead 210,757 157,702Cap charges on new equipment 7,617 7,617
SUB-TOTAL OVERHEAD 218,374 165,319
TOTAL 18.01 1,137,958 800,355
CAPITAL COSTSVentilator 20,000 20,000Gym Equipment 5,000 5,000Theatre Tray & Equipment 15,000 15,000Other 7,500 7,500TOTAL CAPITAL COSTS 47,500 47,500
PROVISION of HEART TRANSPLANTATION SERVICE to SCOTLAND
Appendix V Cost profile - Freeman Hospital, NewcastleAppendix V Cost profile - Freeman Hospital, NewcastleAppendix V Cost profile - Freeman Hospital, NewcastleAppendix V Cost profile - Freeman Hospital, NewcastleAppendix V Cost profile - Freeman Hospital, Newcastle

Glasgow Heart Transplant Unit including Advanced Heart Failure
Base Cost : 15 Transplants10 Complex Heart Surgery5 CRTDs REDUCTION CRTD/ICD
Contract Added Back Total Additional2003/04 Cost 2003/04 requirements
WTE £ £ £ £Staff Costs
SurgeryConsultant 2.00 220,285 220,285 100,000 Funded by SCINResearch posts 2.00 83,787 83,787 Registrars 2.00 159,593 159,593 SHO 0.80 138,228 138,228
Asso Specialist 1.00 0 0 0
Sub Total 7.80 601,893 601,893 100,000
Anaesthetists Consultant 0.75 69,998 69,998 0
Medical Physician 1.00 88,332 88,332 0
Medical Sub Total 9.55 760,224 760,224 100,000
NursingWards Coordinator (Memo) 2.00 105,665 105,665
Grade G 1.00 35,714 35,714 Grade F 1.00 31,294 31,294 Grade E 9.00 248,227 248,227 0Grade D 3.00 82,548 82,548 Grade A 2.80 38,367 38,367 0
Sub Total 18.80 541,815 541,815 0
Theatre/Cath lab Grade IGrade HGrade G 0.18 9,188 9,188 Grade F 0Grade E 0.45 13,963 13,963 0Grade D 0.35 7,690 7,690 0Grade A 0.35 4,218 4,218 0Grade E 2.00 47,134 47,134
Sub Total 3.33 82,193 82,193 0
Clinic Grade E 1.00 22,919 22,919 0Grade D 1.00 21,937 21,937 0
Nursing sub total 24.13 668,864 668,864 0
TechniciansPhysiotherapy 0.50 15,245 15,245 0Dietician 0.30 9,147 9,147 0Perfusionists 51,943 51,943 Med Cardiology 0.25 7,068 7,068 0
+ Pharmacy support 0.25 0 9,249Sub Total 1.30 83,403 83,403 9,249
Admin / Clerical 3.50 55,318 55,318 1.00 0Sec supp Co Ordinators 7,924 7,924 Travel & Training 9,132 9,132 0
TOTAL STAFF COSTS 38.48 1,576,942 1,576,942 109,249
Pharmacy SuppliesWard / Theatre 209,921 71,691 281,611 15 trans 80,535 Devices 0 0 88,125 5 CRTDs
Other Directorates Labs/ECG 0Biochemistry 38,046 4,726 42,772 0Bacteriology 23,961 2,977 26,938 Haematology 26,551 3,298 29,850 Pathology 47,873 5,947 53,820 Tissue Typing 23,313 2,896 26,209 Radiology 61,844 7,682 69,526
Sub Total 431,509 22,756 530,726 168,660
General ServicesCatering 6,176 1,607 7,782 0Portering 4,787 4,787 0Linen 4,372 1,138 5,510 0Cleaning 20,893 20,893 0Other Costs 12,516 12,516 0
Sub Total 48,744 51,489 0
OverheadsMaintenance 11,609 11,609 Heat & Light 7,540 7,540 Rates 7,660 7,660 Transportation 89,045 89,045 Equipment 0 0 0
Sub Total 115,855 115,855 0
Capital Charges 247,927 247,927
TOTAL COSTS 2,420,976 101,962 2,522,938 277,909 Total Excluding SCIN 2,700,847
Appendix VI Cost profile,Glasgow Heart TAppendix VI Cost profile,Glasgow Heart TAppendix VI Cost profile,Glasgow Heart TAppendix VI Cost profile,Glasgow Heart TAppendix VI Cost profile,Glasgow Heart Transplant Unitransplant Unitransplant Unitransplant Unitransplant Unit