rheumatoid arthritis of the shoulder - uoftorthopaedics.ca · rheumatoid arthritis of the shoulder...
TRANSCRIPT

Journal of the American Academy of Orthopaedic Surgeons12
Rheumatoid arthritis (RA) is a chronic,systemic inflammatory disorder ofunclear etiology characterized by anerosive, symmetrical polyarthritisthat may lead to progressive disabil-ity. The estimated prevalence is 1%worldwide, with a female-to-maleratio of 3:1 that diminishes with age.The prevalence increases starting inthe third decade of life; RA affectsmore than 5% of the populationolder than 70 years. Approximately91% of patients with long-standingRA (>5 years’ duration) developshoulder symptoms.1,2
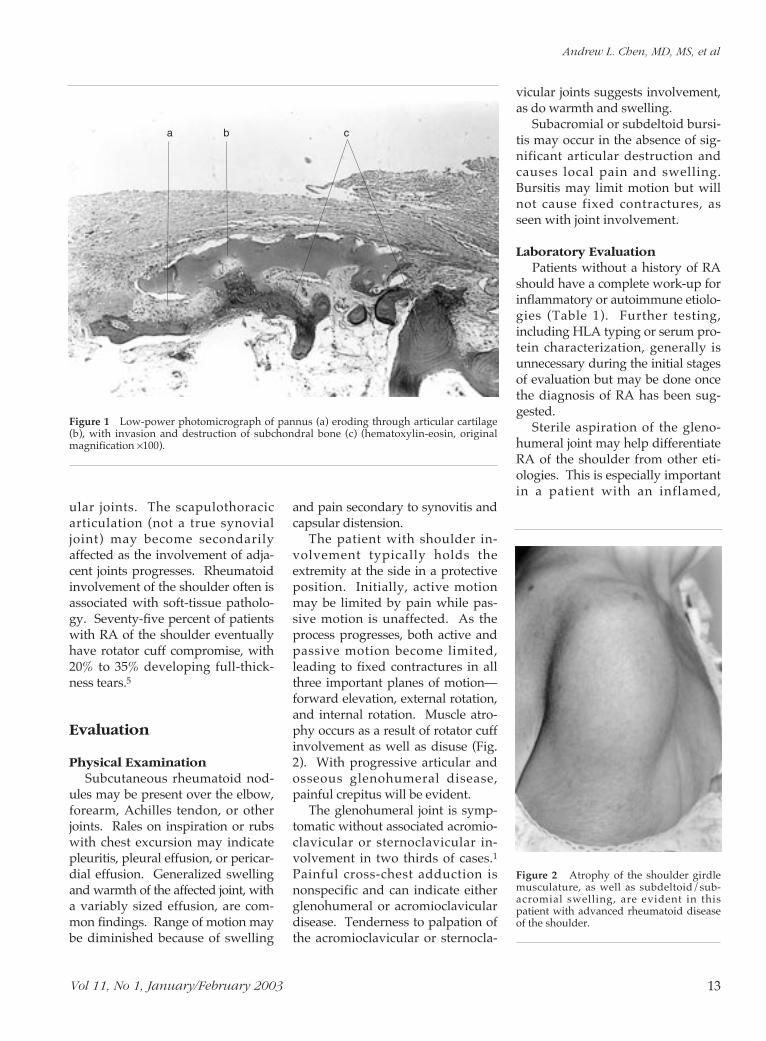
Rheumatoid disease causes amicrovascular injury and mild syn-ovial cell proliferation, with perivas-cular lymphocytosis. The continuedinflammation results in the forma-tion of an erosive, hyperplastic syn-ovium (pannus) as well as jointswelling (Fig. 1). Immune complexdeposition and complement activa-tion on the articular surfaces pro-duce degradation of proteoglycans
and collagen. The release of inflam-matory cytokines results in contin-ued cartilage damage, bone erosion,and soft-tissue degradation, ofteninvolving the insertion of the rotatorcuff. In addition, through poorlyunderstood mechanisms, chondro-cytes themselves may play a role inarticular destruction through possi-ble participation in proteolyticdigestion of cartilage matrix.3,4
Clinical Course
The initial presentation of RA ishighly variable; however, more than90% of patients report generalizedsymptoms of fatigue, musculoskele-tal pain, variable fever, and weightloss.1,2 Some may present with jointpain alone, which may be monoar-ticular or polyarticular without sys-temic findings. Early involvementtypically affects the small joints ofthe hand and foot. The knee, ankle,
wrist, and elbow usually are in-volved later. Particularly in theearly phases of the disease, the clini-cal course may be characterized byquiescence during periods of remis-sion.
Rheumatoid involvement of theshoulder may present with an in-sidious onset of pain, swelling, andprogressive loss of motion, reflect-ing both articular and periarticularinvolvement. Patients often areunaware of the early loss of motion,perhaps because of their ability tocompensate with motion at adjacentjoints or with the contralateral ex-tremity. As motion loss progresses,the patient may find it difficult toreach previously accessible objectson high shelves or to perform activi-ties behind the back, such as fasten-ing a brassiere or obtaining objectsfrom a back pocket. RA may affectall of the synovial joints of theshoulder region—the glenohumeral,acromioclavicular, and sternoclavic-
Dr. Chen is Chief Resident, Department ofOrthopaedic Surgery, New York University–Hospital for Joint Diseases, New York, NY.Dr. Joseph is Chief Resident, Department ofOrthopaedic Surgery, New York University–Hospital for Joint Diseases. Dr. Zuckerman isProfessor and Chairman, Department of Ortho-paedic Surgery, New York University–Hospitalfor Joint Diseases.
Reprint requests: Dr. Zuckerman, 301 East17th Street, New York, NY 10003.
Copyright 2003 by the American Academy ofOrthopaedic Surgeons.
Abstract
Rheumatoid arthritis affecting the shoulder region is a progressive disorderthat results in pain, loss of range of motion, and functional disability. Theinflammatory response, which is of unknown etiology, results in synovitis,pannus formation, and articular destruction. Even when patient history andphysical examination suggest rheumatoid involvement of the shoulder, labora-tory assessment and radiographic evaluation often are necessary to establishthe diagnosis. Nonsurgical management is the primary treatment, includingpharmacologic and physical therapy regimens for patients with mild symp-toms and functional disability. Surgical intervention is indicated in patientswith significant pain and functional limitation when nonsurgical treatmentfails to provide relief. The procedure selected depends on careful assessment ofthe degree of articular cartilage injury and compromise of the periarticularsoft tissues.
J Am Acad Orthop Surg 2003;11:12-24
Rheumatoid Arthritis of the Shoulder
Andrew L. Chen, MD, MS, Thomas N. Joseph, MD, and Joseph D. Zuckerman, MD
Andrew L. Chen, MD, MS, et al
Vol 11, No 1, January/February 2003 13
ular joints. The scapulothoracicarticulation (not a true synovialjoint) may become secondarilyaffected as the involvement of adja-cent joints progresses. Rheumatoidinvolvement of the shoulder often isassociated with soft-tissue patholo-gy. Seventy-five percent of patientswith RA of the shoulder eventuallyhave rotator cuff compromise, with20% to 35% developing full-thick-ness tears.5
Evaluation
Physical ExaminationSubcutaneous rheumatoid nod-
ules may be present over the elbow,forearm, Achilles tendon, or otherjoints. Rales on inspiration or rubswith chest excursion may indicatepleuritis, pleural effusion, or pericar-dial effusion. Generalized swellingand warmth of the affected joint, witha variably sized effusion, are com-mon findings. Range of motion maybe diminished because of swelling
and pain secondary to synovitis andcapsular distension.
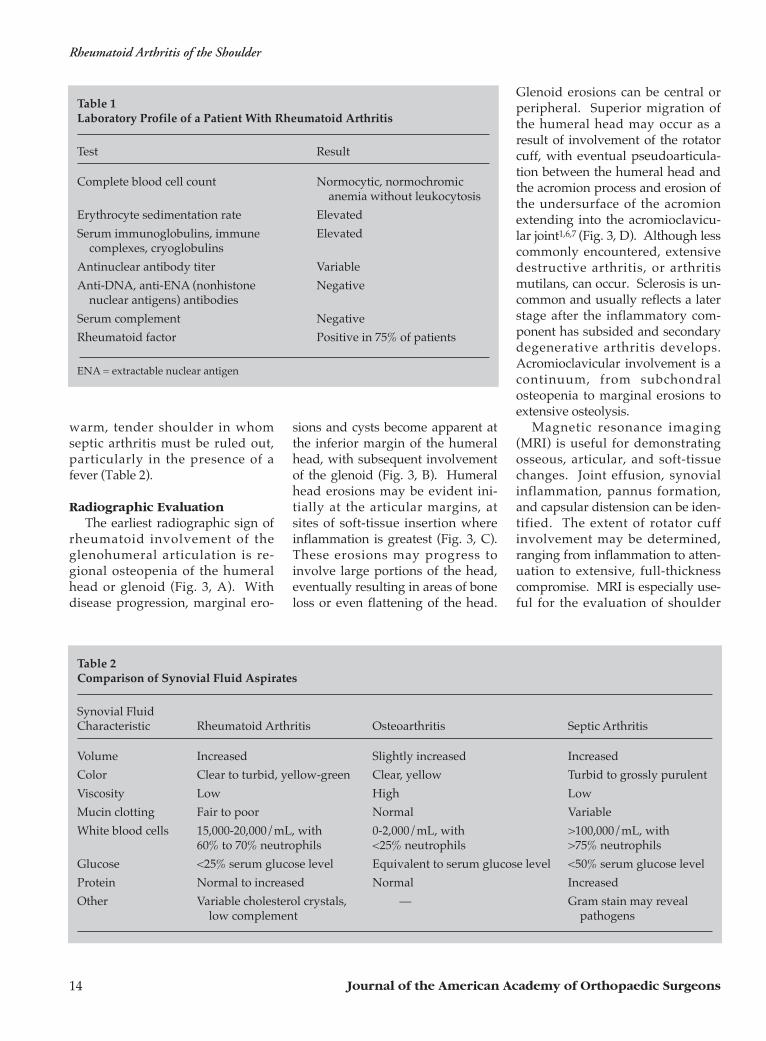
The patient with shoulder in-volvement typically holds theextremity at the side in a protectiveposition. Initially, active motionmay be limited by pain while pas-sive motion is unaffected. As theprocess progresses, both active andpassive motion become limited,leading to fixed contractures in allthree important planes of motion—forward elevation, external rotation,and internal rotation. Muscle atro-phy occurs as a result of rotator cuffinvolvement as well as disuse (Fig.2). With progressive articular andosseous glenohumeral disease,painful crepitus will be evident.
The glenohumeral joint is symp-tomatic without associated acromio-clavicular or sternoclavicular in-volvement in two thirds of cases.1Painful cross-chest adduction isnonspecific and can indicate eitherglenohumeral or acromioclaviculardisease. Tenderness to palpation ofthe acromioclavicular or sternocla-
vicular joints suggests involvement,as do warmth and swelling.
Subacromial or subdeltoid bursi-tis may occur in the absence of sig-nificant articular destruction andcauses local pain and swelling.Bursitis may limit motion but willnot cause fixed contractures, asseen with joint involvement.
Laboratory EvaluationPatients without a history of RA
should have a complete work-up forinflammatory or autoimmune etiolo-gies (Table 1). Further testing,including HLA typing or serum pro-tein characterization, generally isunnecessary during the initial stagesof evaluation but may be done oncethe diagnosis of RA has been sug-gested.
Sterile aspiration of the gleno-humeral joint may help differentiateRA of the shoulder from other eti-ologies. This is especially importantin a patient with an inflamed,
Figure 1 Low-power photomicrograph of pannus (a) eroding through articular cartilage(b), with invasion and destruction of subchondral bone (c) (hematoxylin-eosin, originalmagnification ×100).
a b c
Figure 2 Atrophy of the shoulder girdlemusculature, as well as subdeltoid/sub-acromial swelling, are evident in thispatient with advanced rheumatoid diseaseof the shoulder.
Rheumatoid Arthritis of the Shoulder
Journal of the American Academy of Orthopaedic Surgeons14
warm, tender shoulder in whomseptic arthritis must be ruled out,particularly in the presence of afever (Table 2).
Radiographic EvaluationThe earliest radiographic sign of
rheumatoid involvement of theglenohumeral articulation is re-gional osteopenia of the humeralhead or glenoid (Fig. 3, A). Withdisease progression, marginal ero-
sions and cysts become apparent atthe inferior margin of the humeralhead, with subsequent involvementof the glenoid (Fig. 3, B). Humeralhead erosions may be evident ini-tially at the articular margins, atsites of soft-tissue insertion whereinflammation is greatest (Fig. 3, C).These erosions may progress toinvolve large portions of the head,eventually resulting in areas of boneloss or even flattening of the head.
Glenoid erosions can be central orperipheral. Superior migration ofthe humeral head may occur as aresult of involvement of the rotatorcuff, with eventual pseudoarticula-tion between the humeral head andthe acromion process and erosion ofthe undersurface of the acromionextending into the acromioclavicu-lar joint1,6,7 (Fig. 3, D). Although lesscommonly encountered, extensivedestructive arthritis, or arthritismutilans, can occur. Sclerosis is un-common and usually reflects a laterstage after the inflammatory com-ponent has subsided and secondarydegenerative arthritis develops.Acromioclavicular involvement is acontinuum, from subchondralosteopenia to marginal erosions toextensive osteolysis.
Magnetic resonance imaging(MRI) is useful for demonstratingosseous, articular, and soft-tissuechanges. Joint effusion, synovialinflammation, pannus formation,and capsular distension can be iden-tified. The extent of rotator cuffinvolvement may be determined,ranging from inflammation to atten-uation to extensive, full-thicknesscompromise. MRI is especially use-ful for the evaluation of shoulder
Table 1Laboratory Profile of a Patient With Rheumatoid Arthritis
Test Result
Complete blood cell count Normocytic, normochromic anemia without leukocytosis
Erythrocyte sedimentation rate Elevated
Serum immunoglobulins, immune Elevatedcomplexes, cryoglobulins
Antinuclear antibody titer Variable
Anti-DNA, anti-ENA (nonhistone Negativenuclear antigens) antibodies
Serum complement Negative
Rheumatoid factor Positive in 75% of patients
ENA = extractable nuclear antigen
Table 2Comparison of Synovial Fluid Aspirates
Synovial Fluid Characteristic Rheumatoid Arthritis Osteoarthritis Septic Arthritis
Volume Increased Slightly increased Increased
Color Clear to turbid, yellow-green Clear, yellow Turbid to grossly purulent
Viscosity Low High Low
Mucin clotting Fair to poor Normal Variable
White blood cells 15,000-20,000/mL, with 0-2,000/mL, with >100,000/mL, with60% to 70% neutrophils <25% neutrophils >75% neutrophils
Glucose <25% serum glucose level Equivalent to serum glucose level <50% serum glucose level
Protein Normal to increased Normal Increased
Other Variable cholesterol crystals, — Gram stain may reveal low complement pathogens

Andrew L. Chen, MD, MS, et al
Vol 11, No 1, January/February 2003 15
weakness and pain not fully ex-plained by bony changes seen onplain radiography.8
Computed tomography (CT)may be indicated when preopera-tive analysis of humeral headdefects and glenoid articular ero-sions is necessary. Albertsen et al9
reported agreement between preop-erative CT results and intraopera-tive findings, concluding that CTcould characterize osseous defectsand bone loss more accurately thancan standard radiography (Fig. 4).This is particularly important inevaluating glenoid erosion to deter-mine whether implantation of a gle-noid component is possible.
Differential DiagnosisAlthough RA is the most com-
mon inflammatory arthritis toaffect the shoulder, its variable,nonspecific presentation may re-quire that other conditions beexcluded before the diagnosis canbe established. Glenohumeral aspi-ration is often helpful (Table 2).Patients with septic arthritis oftenhave high fever and local findingsof erythema and swelling. Rotatorcuff arthroplasty may be associatedwith anterosuperior instability andsuperior humeral migration, oftenwith secondary erosive changes onthe inferior aspect of the acromionand the acromioclavicular joint.
Crystalline arthropathies of theshoulder can have presentationssimilar to that of RA. An insidiousonset of mild shoulder discomfortwith low-grade inflammationaccompanied by blood-tinged syn-ovial fluid replete with debris,hydroxyapatite crystals, and fewinflammatory cells (mostly mono-cytes) is indicative of Milwaukeeshoulder (calcium hydroxyapatitecrystalline arthropathy). Positivestaining of crystals with alizarin redS confirms the diagnosis. Both gout(sodium urate crystal deposition)and pseudogout (calcium pyrophos-phate dihydrate crystal deposition)may have articular cartilage calcifi-cations but may be differentiated onsynovial fluid examination; calciumpyrophosphate dihydrate depositionhas positively birefringent rhom-boid-shaped crystals, while gout hasnegatively birefringent needle-shaped crystals.5,10,11
Osteoarthritis is the most com-mon form of glenohumeral arthritis,affecting up to 80% to 85% of womenolder than 70 years.12 Osteoarthritismay be secondary to trauma or frac-ture, developmental dysplasia, orold sepsis, or may be a manifestationof “burned out” inflammatory arthri-tis. Its characteristic radiographicpresentation shows asymmetric jointspace narrowing, subchondral scle-rosis, and osteophytes about the glen-oid and humeral head (Fig. 5).
Classification
The Laine classification of RA of theglenohumeral articulation has threestages based on clinical and radio-graphic findings.13 In stage I, slightlimitation of shoulder motion is pres-ent, with mild to moderate pain andtenderness to palpation. Crepi-tation may be appreciated on rangeof motion. Radiographs show onlygeneralized osteopenia. Stage II ischaracterized by moderate limita-tion of shoulder motion, moderate
A B
C D
Figure 3 A, Anteroposterior radiograph showing early changes of rheumatoid disease.Osteopenia, with minimal articular degenerative changes, and superior migration of thehumeral head consistent with rotator cuff compromise are present. B, Intermediatechanges of symmetric glenohumeral joint space loss and early cyst formation. C, As thedisease progresses, more extensive erosions are evident about the humeral head and gle-noid; progressive glenoid bone loss results in medialization of the humeral head. Thesuperior migration of the humeral head indicates progressive rotator cuff deterioration.D, Extensive articular destruction, or arthritis mutilans, reflects end-stage changes withextensive erosions and bone loss.

Rheumatoid Arthritis of the Shoulder
Journal of the American Academy of Orthopaedic Surgeons16
to severe pain, and crepitus. Radio-graphic findings include osteopenia,erosive bony changes, and jointspace narrowing. In stage III, severefunctional deficits are present; rangeof motion is painful and limits activ-ities of daily living. Radiographsshow advanced erosive changes ofthe humeral head and glenoid.13
Neer14 classified RA of the shoulderinto three categories based on clini-cal and radiographic findings; hisdry, wet, and resorptive stages areapproximately equivalent to thoseof Laine et al.13
Nonsurgical Management
Nonsurgical management of therheumatoid shoulder is indicatedfor mild to moderate (stage I) dis-ease, when synovial inflammation isthe primary manifestation beforesignificant bony changes occur. Theemphasis is on optimal use of med-ications (Fig. 6).
Intra-articular CorticosteroidInjection
Intra-articular injection of corti-costeroids for RA of the shoulderhas been described for the treat-ment of acute and subacute inflam-matory synovitis. Although theintra-articular administration of
corticosteroids often may result indramatic symptomatic relief, itshould be considered as only atemporizing measure for patientswho have not responded to oralmedications. Multiple injectionscan have a deleterious effect onconnective tissue structures, in-cluding the articular cartilage andthe rotator cuff tendons, and there-fore should be avoided.1,15 Mostphysicians suggest limiting injec-tions to three and to consider re-peat injections only when signifi-cant improvement has resultedfrom the previous injection.
Physical TherapyMaintenance and/or improve-
ment of shoulder motion may beenhanced by physical therapy con-sisting of passive and active-assistedrange-of-motion exercises. Duringperiods of active synovitis, motionshould be maintained with assistedand passive motion exercises focus-ing on forward elevation, externalrotation, and internal rotation be-hind the back. As the synovitis andinflammation improve, stretchingcan be initiated to improve the over-all range of motion. Isometric exer-cises for the deltoid muscle androtator cuff can effectively maintainmuscle tone and strength duringperiods of exacerbation. With reso-
lution of the acute episode, therapycan progress to include more rigor-ous strengthening and stretching toregain full range of motion. Ideally,exercises should be performed fivetimes a day in 10-minute sessionsrather than in one or two long ses-sions.
A B C
Figure 4 Axial CT views of the shoulder. A, Early involvement, with joint space narrowing (arrows) but maintenance of glenoid mor-phology. B, Later-stage changes showing significant glenoid bone loss and erosion (arrows) into the glenoid neck. C, Advanced changes,with extensive erosion (arrows) of the glenoid and humeral head.
Figure 5 Anteroposterior radiograph of anosteoarthritic glenohumeral joint showssubchondral sclerosis, cyst formation,humeral head flattening, and osteophyteformation. This classic appearance is readilydistinguishable from the radiographicchanges typical of RA (Figure 3).

Andrew L. Chen, MD, MS, et al
Vol 11, No 1, January/February 2003 17
Surgical Management
Surgical management of the rheu-matoid shoulder is indicated whenmedications and physical therapyare no longer effective in relievingpain and maintaining function.Selection of procedure is based ona careful assessment of the degreeof involvement of the articular car-tilage, subchondral bone, and peri-articular soft tissues. Cartilage-pre-serving procedures are indicatedwhen some articular cartilage re-mains intact and the goal is to pre-vent or slow disease progression by
methods such as synovectomy.Cartilage-sacrificing procedures (eg,hemiarthroplasty, total shoulderarthroplasty, and arthrodesis) areindicated when articular cartilageloss is extensive and beyond preser-vation.
Basic Principles
Staging of Procedures The polyarticular nature of RA
often necessitates multiple surgicalprocedures. Most authors agreethat the most disabling articulationshould be addressed first;16-19 how-
ever, staging also depends on thenature of the procedures (eg, arthro-scopic or open). Given equal symp-tomatology, opinions vary regard-ing prioritization of upper versuslower extremity. When shouldersurgery is done first, lower extremi-ty procedures should be delayed atleast 3 months to avoid weight bear-ing on the recovering shoulder.This period may be extended tomore than 6 months to allow heal-ing of additional soft-tissue proce-dures such as rotator cuff repair.When the lower extremity is ad-dressed first, shoulder surgeryshould be delayed until assistiveambulatory devices are no longernecessary.
When multiple upper extremityprocedures are necessary, the mostsymptomatic joint should be ad-dressed first. In general, prioritiza-tion should be given to the proce-dure that results in the greatest func-tional improvement. Neer et al17
maintained that hand or wristinvolvement should be addressedbefore ipsilateral elbow or shoulderdisease because functional limita-tions of the hand or wrist may pre-clude rehabilitation of the elbow orshoulder due to a lack of incentive touse the involved upper extremity.Friedman and Ewald18 stated thatthe elbow should be addressedfirst; giving priority to surgicalmanagement of the elbow yieldsgreater subjective and objectivefunctional improvement of the up-per limb and allows for a longerinterval between arthroplasties.Gill et al19 reported that arthroplas-ty of both the shoulder and elbowfor end-stage RA may be donesuccessfully independent of thesequence of joint replacements.With multiple upper extremity in-volvement, technical considerationssuch as humeral component stemlength in shoulder or elbow arthro-plasty also must be taken into ac-count in anticipation of future pro-cedures.
MildModerate-Severe
RehabilitationObservation
Cartilage-preservingSynovectomyDébridement
Cartilage-sacrificingProsthetic replacement
Signs and symptomsPainErythemaSwellingLoss of range of motion
Nonsurgical treatmentActivity modificationMedications
NSAIDsDisease-modifying drugsAntimetabolicsOral corticosteroids
Physical therapyIntra-articular corticosteroid injection
HemiarthroplastyPrimary humeral head involvementIrreparable rotator cuff tearInadequate glenoid bone stock for
total shoulder arthroplasty
Total shoulder arthroplastyHumeral and glenoid involvementRotator cuff intact or reparableAdequate glenoid bone stock
Minimal or no radiographic changes
Mild to severe radiographic changes
Failure/progression Surgical
treatment
Severe radiographic
changes
Symptomaticimprovement
Mild to moderateradiographic changes
Figure 6 Algorithm for treatment of RA of the shoulder.

Rheumatoid Arthritis of the Shoulder
Journal of the American Academy of Orthopaedic Surgeons18
TimingThe timing of surgical manage-
ment should be dictated by thedegree of symptoms and the clini-cal presentation. Early surgical in-tervention with synovectomy orbursectomy may be indicated forpatients with only a diminishedrange of motion or a decreasedsubacromial space. Surgical inter-vention also may be based on thedegree of bone loss rather than justpain and disability because furtherdisease progression could precludelater reconstructive surgery.
Systemic ConsiderationsThe systemic nature of RA re-
quires careful multidisciplinaryassessment before surgery. The cer-vical spine must be evaluated forstability before endotracheal intuba-tion. Subtle myelopathy secondaryto cord compression from C1-C2instability may be mistaken for dif-fuse joint involvement resulting inweakness. Of particular concern arethe possible need for perioperativecorticosteroids, the increased risk ofinfection because of immunosup-pression, and perioperative anemia.
Cartilage-Preserving ProceduresBursectomy and/or synovectomy
is indicated for patients with primar-ily active synovitis without evidenceof extensive articular destruction.Although joint débridement mayprovide symptomatic relief in pa-tients with soft-tissue swelling andevidence of inflammation, it seldomresults in a significant increase inrange of motion.20 Synovectomyalso may be done in patients withrapidly progressing synovitis in aneffort to slow disease progression.However, the results of synovecto-my generally depend on the degreeof articular cartilage involvement;the best results are obtained inpatients with early (stage I) disease.1Synovectomy may be either open orarthroscopic, with successful returnto pain-free motion in up to 80% of
patients.21 Arthroscopic gleno-humeral synovectomy and subacro-mial bursectomy appear to allowearly return to function. Acromio-plasty or coracoacromial ligamentrelease is generally not done inpatients with RA because doing socould compromise the coracoacro-mial arch and may lead to antero-superior instability, particularly inpatients with rotator cuff dys-function.
Cartilage-Sacrificing ProceduresWhen either nonsurgical man-
agement or cartilage-preservingprocedures fail to provide adequaterelief, prosthetic replacement isindicated for patients with unremit-ting or progressive pain and func-tional limitation. Approximately20% to 35% of patients who requireprosthetic replacement have con-comitant rotator cuff tears; thesemay be addressed at the time ofarthroplasty, necessitating a modifi-cation of the postoperative course.Rozing and Brand22 examined theresults of rotator cuff repair at thetime of shoulder arthroplasty forRA and concluded that concomitantcuff repair significantly (P = 0.002)improved postoperative clinicalshoulder scores compared withpatients in whom tears were notrepaired.
The modular humeral compo-nents are available in a range ofstem sizes and humeral heads. Thevarying stem sizes enable secure fix-ation both with and without cement.Cement fixation is more often usedin rheumatoid patients because ofthe poor bone quality and proximalbone loss. Humeral heads are avail-able in varying neck lengths anddiameters, allowing improved soft-tissue balancing that enhances thestability of the implant. Asymmetrichumeral heads are used to modifyoffset as well as to change the orien-tation of the component. Thesemodifications are designed to im-prove soft-tissue balancing and the
stability of the articulation. Famili-arity with the components of thesystem allows the surgeon to opti-mize fixation, making a stable, func-tional articulation more likely.
A range of shoulder implant sys-tems is available. Most use an all-polyethylene glenoid component;metal-backed components are nolonger common. The glenoid com-ponent is designed for cement fixa-tion, with a keel or multiple pegs forinsertion into the glenoid.
HemiarthroplastyIndications for proximal humeral
replacement (shoulder hemiarthro-plasty) include extensive humeralhead involvement with minimal orno involvement of the glenoid artic-ular surface (uncommon in therheumatoid shoulder); extensivehumeral head and glenoid involve-ment with associated osteopeniaand/or bone loss, such that securefixation of the glenoid component isunattainable; and extensive articularcartilage deterioration in the pres-ence of a massive, irreparable rotatorcuff tear. In younger patients (<65years) who wish to maintain anactive lifestyle, concerns about gle-noid component loosening have ledsome to avoid the use of glenoidcomponents. However, long-termpain relief is less reliable than withglenoid resurfacing, and continueddegeneration of the glenoid canresult in progressive symptoms.23,24
The procedure is done with thepatient in a beach-chair position,using an anterior deltopectoralapproach. During the exposure,soft tissues are handled carefully asthey may often be attenuated. Thesubscapularis tendon and under-lying capsule are divided 1 cmmedial to the insertion on the lessertuberosity. There may be significantcontracture of the anterior softtissues requiring mobilization ofthe subscapularis tendon and theunderlying capsule. This is general-ly done by releasing the adhesions

Andrew L. Chen, MD, MS, et al
Vol 11, No 1, January/February 2003 19
of the subscapularis at the base ofthe coracoid and along the anteriorglenoid neck. This should allowsignificant lateral excursion of thesubscapularis tendon and muscle,which will enhance postoperativeexternal rotation. In general, a cir-cumferential capsular releasearound the glenoid margin, freeingthe inferior and posterior capsules,will mobilize the rotator cuff,enhancing both intraoperative expo-sure and postoperative mobility.
After resection of the humeralhead, the glenoid is carefully in-spected to evaluate the integrity ofthe articular cartilage and the pres-ence and degree of bone loss. Rarelyis the articular cartilage of the gle-noid sufficiently intact to obviate theneed for resurfacing, particularlywhen significant humeral headchanges are present. Therefore, iso-lateral humeral destruction is not thecommon indication for hemiarthro-plasty in rheumatoid patients. Moreoften, there is extensive glenoidbone loss, or the remaining bone isof insufficient quality to allowsecure fixation of the glenoid com-ponent. When there is significantasymmetric glenoid wear, reamingof the glenoid should be consideredto restore the concavity and therebyenhance the stability of the prosthet-ic glenoid articulation. The rotatorcuff also should be carefully in-spected: irreparable defects of thesupraspinatus, infraspinatus, orteres minor tendons also precludeinsertion of a glenoid component.
The proximal humeral osteotomyis performed to place the componentin 25° to 40° of retroversion. Se-quential reaming of the humeralshaft determines the appropriatecomponent size. The decision toplace a cemented or cementlesshumeral component generally ismade intraoperatively. Cementlessimplantation is acceptable in mostcases. However, in patients with ex-tensive rheumatoid involvement ofthe proximal humerus with large
cyst formation, cementing often isnecessary to achieve rotational andaxial stability. A modular implant ispreferable because it provides anopportunity to adjust the soft-tissuebalancing and enhance stability.Repair of the subscapularis tendonis critical. When the closure is com-plete, the amount of external rota-tion possible without undue tensionon the subscapularis repair shouldbe documented to guide the postop-erative rehabilitation program.
Hemiarthroplasty results in reli-able pain relief and improvement offunction and range of motion, al-though the outcome is not as pre-dictable in patients with RA as inpatients with osteoarthritis.25 This isthought to be the result of poor bonestock and compromised soft tissues.Koorevaar et al26 examined the out-comes of 19 cases of shoulder hemi-arthroplasty for RA at a mean of 8years; 64% of patients reported littleor no pain, and no patient com-plained of severe pain. Recurrenceof symptoms and functional debili-tation because of progressive gle-noid degeneration may necessitateglenoid resurfacing, primarily inpatients in whom the indication forhemiarthroplasty was a reasonablyintact glenoid surface.
Total Shoulder ArthroplastyTotal shoulder arthroplasty is in-
dicated for patients with debilitatingpain and end-stage RA of the shoul-der with extensive humeral headand glenoid articular cartilage loss,yet with sufficient bone stock andsoft-tissue integrity to achieve a sta-ble articulation. The initial exposureand preparation are the same as forthe patient undergoing hemiarthro-plasty. Exposure of the glenoid isobtained by subscapularis mobiliza-tion and capsular releases. With theglenoid exposed, the anterior gle-noid neck is palpated to identify thedirection for preparation of the gle-noid component fixation. The glenoid is prepared using a combi-
nation of drills, reamers, and burrs.The reaming should provide anexacting congruency with the backsurface of the glenoid component.Proper alignment of the reamer willcorrect asymmetric glenoid wearand allow restoration of moreanatomic component orientation.Proper glenoid preparation is con-firmed by insertion of a trial compo-nent. A dry field is obtained foroptimal bone-cement interface, andthe glenoid component is thencemented in place. The humeralhead component is then inserted, asdescribed. Appropriate soft-tissuebalancing, which is essential for astable articulation, is achieved by acombination of selective soft-tissuereleases and insertion of appropri-ately sized prosthetic components(Fig. 7).
Rotator cuff tears should be re-paired at the time of total shoulderarthroplasty. The repair sequencevaries, but generally the extent ofthe rotator cuff tear is identified withthe initial exposure. The edges ofthe tear are tagged with sutures, andthe rotator cuff is mobilized so that itcan be advanced laterally to itsinsertion. After insertion of the gle-noid component but before insertionof the humeral component, suturesare passed through drill holes in thegreater tuberosity that will later beused for the tendon-to-bone repair.These sutures are left in place whilethe humeral component is inserted.When the components are in placeand the humeral head is reduced,the rotator cuff repair is completedusing the previously placed tendon-to-bone sutures. Any additionaltendon-to-tendon sutures can beplaced, as well. Performing the finalportion of the rotator cuff repairafter implantation of the compo-nents eliminates the stress on therepair that would occur if significantmanipulation of the shoulder werenecessary. Occasionally, additionalsurgical releases and rotator cuffmobilization are necessary to allow

Rheumatoid Arthritis of the Shoulder
Journal of the American Academy of Orthopaedic Surgeons20
for secure repair to the greatertuberosity. The coracoacromial liga-ment usually is not released duringhemiarthroplasty or total shoulderarthroplasty. When rotator cuffrepair is necessary, the undersurfaceof the acromion should be inspect-ed carefully, but acromioplasty israrely necessary. The goal is tomaintain the integrity of the coraco-acromial arch because of its contri-bution to glenohumeral stability inthese significantly compromisedshoulders.
Several investigators have report-ed that total shoulder arthroplastyfor end-stage RA results in short-and long-term pain relief, satisfac-tory increases in range of motion,and markedly improved functionalstatus.27-29 Because of soft-tissuecompromise and the inflammatorynature of the disease, the results oftotal shoulder arthroplasty in pa-tients with RA have not been shownto be as satisfactory or reliable asthose in patients with osteoarthri-tis.25 Despite concerns about proxi-mal humeral migration and glenoidradiolucent lines, long-term resultshave shown that the degree of painrelief, range of motion, abductionforce, and functional status do notdiminish significantly over time.30
Postoperative RehabilitationThe postoperative rehabilitation
regimen must be tailored to the spe-cific needs of each patient. Designof the regimen is based on the sur-geon’s intraoperative assessment ofthe quality of the soft tissues, com-ponent stability, and any associatedrepairs. Patients should be coun-seled that maximum benefit afterprosthetic shoulder replacementmay not be realized until 6 monthsto 1 year after surgery.
Rehabilitation begins on the firstpostoperative day, with active rangeof motion for the ipsilateral hand,wrist, and elbow, and passive andactive-assisted range of motion forthe shoulder. Initially, this includes
supine passive forward elevationand external rotation exercises withthe arm at the side. The degree ofexternal rotation allowed during the
initial 6 postoperative weeks isdetermined by the intraoperativerepair of the subscapularis tendon;in general, 30° to 40° of external rota-
A B
C D
E F
Figure 7 Anteroposterior (A) and axillary (B) radiographs of the left shoulder in a 69-year-old woman with seropositive RA and debilitating pain for 1 year. T1-weighted coro-nal (C) and axial (D) magnetic resonance images of the same patient showing attenuationof the rotator cuff tendon (black arrow) but without a full-thickness tear. The humeralhead erosions (asterisk) are extensive and well delineated. Glenoid bony architecture(white arrow) indicates that there is probably sufficient bone stock for placement of a gle-noid component. Anteroposterior (E) and axillary (F) radiographs immediately after totalshoulder arthroplasty.
* *
Andrew L. Chen, MD, MS, et al
Vol 11, No 1, January/February 2003 21
tion may be tolerated without plac-ing undue tension on the repair. Atapproximately 4 to 6 weeks, a moreactive shoulder range of motion isinitiated along with internal rotationbehind the back. Isometric strength-ening exercises are started 4 weeksafter surgery, and resistive strength-ening exercises usually are initiated10 to 12 weeks postoperatively whenactive range of motion has pro-gressed.
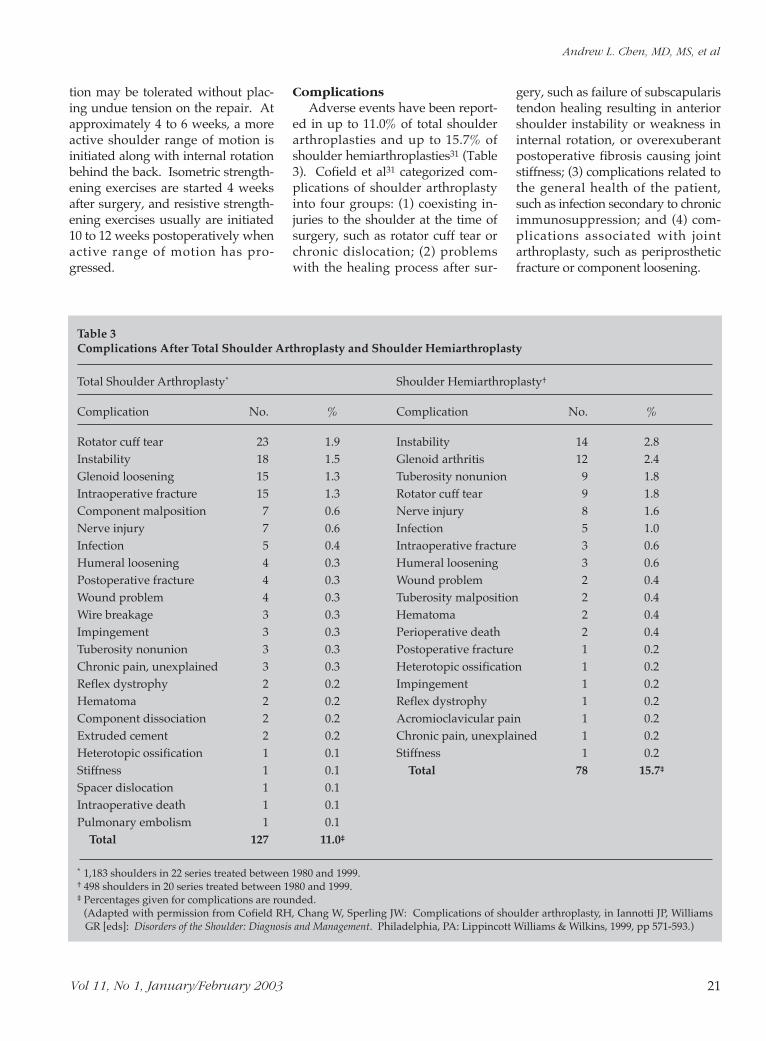
ComplicationsAdverse events have been report-
ed in up to 11.0% of total shoulderarthroplasties and up to 15.7% ofshoulder hemiarthroplasties31 (Table3). Cofield et al31 categorized com-plications of shoulder arthroplastyinto four groups: (1) coexisting in-juries to the shoulder at the time ofsurgery, such as rotator cuff tear orchronic dislocation; (2) problemswith the healing process after sur-
gery, such as failure of subscapularistendon healing resulting in anteriorshoulder instability or weakness ininternal rotation, or overexuberantpostoperative fibrosis causing jointstiffness; (3) complications related tothe general health of the patient,such as infection secondary to chronicimmunosuppression; and (4) com-plications associated with jointarthroplasty, such as periprostheticfracture or component loosening.
Table 3Complications After Total Shoulder Arthroplasty and Shoulder Hemiarthroplasty
Total Shoulder Arthroplasty* Shoulder Hemiarthroplasty†
Complication No. % Complication No. %
Rotator cuff tear 23 1.9 Instability 14 2.8Instability 18 1.5 Glenoid arthritis 12 2.4Glenoid loosening 15 1.3 Tuberosity nonunion 9 1.8Intraoperative fracture 15 1.3 Rotator cuff tear 9 1.8Component malposition 7 0.6 Nerve injury 8 1.6Nerve injury 7 0.6 Infection 5 1.0Infection 5 0.4 Intraoperative fracture 3 0.6Humeral loosening 4 0.3 Humeral loosening 3 0.6Postoperative fracture 4 0.3 Wound problem 2 0.4Wound problem 4 0.3 Tuberosity malposition 2 0.4Wire breakage 3 0.3 Hematoma 2 0.4Impingement 3 0.3 Perioperative death 2 0.4Tuberosity nonunion 3 0.3 Postoperative fracture 1 0.2Chronic pain, unexplained 3 0.3 Heterotopic ossification 1 0.2Reflex dystrophy 2 0.2 Impingement 1 0.2Hematoma 2 0.2 Reflex dystrophy 1 0.2Component dissociation 2 0.2 Acromioclavicular pain 1 0.2Extruded cement 2 0.2 Chronic pain, unexplained 1 0.2Heterotopic ossification 1 0.1 Stiffness 1 0.2Stiffness 1 0.1 Total 78 15.7‡
Spacer dislocation 1 0.1Intraoperative death 1 0.1Pulmonary embolism 1 0.1
Total 127 11.0‡
* 1,183 shoulders in 22 series treated between 1980 and 1999.† 498 shoulders in 20 series treated between 1980 and 1999.‡ Percentages given for complications are rounded.
(Adapted with permission from Cofield RH, Chang W, Sperling JW: Complications of shoulder arthroplasty, in Iannotti JP, WilliamsGR [eds]: Disorders of the Shoulder: Diagnosis and Management. Philadelphia, PA: Lippincott Williams & Wilkins, 1999, pp 571-593.)

Rheumatoid Arthritis of the Shoulder
Journal of the American Academy of Orthopaedic Surgeons22
Significant instability after shoul-der arthroplasty usually is recogniz-able by physical examination andradiography and can be related toimproper soft-tissue balancing, rota-tor cuff disruption, component mal-position, improper component sizing,or component loosening. Other fac-tors associated with instability afterprosthetic replacement of the shoul-der include older age, chronic preop-erative shoulder dislocation, andaberrant glenoid anatomy resultingfrom glenoid bone deficiency orasymmetric wear. Soft-tissue balanc-ing intraoperatively should allow forup to 50% translation both anteriorlyand posteriorly. Superior subluxationof the glenohumeral component isnot necessarily indicative of rotatorcuff disruption; inferior subluxation inthe immediate postoperative periodusually represents deltoid atony butcan indicate inadequate soft-tissuetensioning, which may require sec-ondary surgical corrections.
Axillary nerve neurapraxia is themost common injury. The musculo-cutaneous nerve may also be injuredduring exposure or overzealousretraction of the conjoined tendon.Radial nerve palsy also has beendescribed secondary to cementextrusion from the canal distally,especially with revision arthroplastyor inadvertent humeral cortical pen-etration. If this finding is noted onpostoperative radiographs, explo-ration is indicated. Continuity of thenerve should be confirmed and allcement removed. In most othercases of nerve injury, an initial peri-od of observation is indicatedbecause most nerve injuries repre-sent neurapraxia. If neurologicimprovement does not occur within4 weeks, electromyography shouldbe done to document the degree ofneurologic injury and assess thepotential for recovery. Explorationmay be indicated for nerve palsiesthat do not improve by 12 weeks.
Periprosthetic fractures may occurintraoperatively or postoperatively.
Intraoperative fractures can occurduring humeral shaft preparation orinsertion of the humeral component;postoperative fractures usually are aresult of trauma. Fractures entirelydistal to the humeral componentmay be treated nonsurgically with afracture brace. Fractures proximal tothe tip of the stem can be treated bycerclage wiring, plate fixation com-bined with cerclage wires, or, forintraoperative fractures, insertion ofa long-stem component combinedwith cerclage wiring.
The risk of infection after pros-thetic replacement is increased in thepresence of diabetes mellitus, RA,lupus erythematosus, remote sites ofinfection, prior shoulder surgery, oruse of immunosuppressive medica-tions. Little has been published thatspecifically addresses the treatmentof infected shoulder arthroplasty.For acute or subacute infection (<3months after prosthetic replace-ment), open irrigation and débride-ment, followed by 6 to 8 weeks ofintravenous antibiotics, is usuallyadequate. For delayed infection,component removal and insertion ofantibiotic-impregnated cement isnecessary. Staged reimplantationmay be undertaken after the suc-cessful eradication of infection, asdocumented by normalization of thewhite blood cell count, sedimenta-tion rate, C-reactive protein level,and intraoperative frozen section.
Prosthetic loosening almost always involves the glenoid compo-nent and is best minimized by careful glenoid preparation withpreservation of bone stock, meticu-lous cement technique, and closeattention to soft-tissue balancing.Massive, unreconstructable rotatorcuff tears are a relative contraindica-tion to glenoid replacement. Thesetears underscore the importance ofthe rotator cuff in maintaining jointposition and preventing excessive,eccentric glenoid loading that canincrease the risk of early loosening.Clinically significant glenoid loosen-
ing is uncommon compared withradiographic findings suggestive ofloosening. Accordingly, it is im-portant to exclude other causes ofshoulder pain, such as occult infec-tion or rotator cuff tear. If glenoidrevision is done, removal of the loosecomponent may reveal a large cen-tral glenoid defect that may not bestructurally amenable to componentreinsertion, even after bone grafting.In such cases, impaction graftingmay be done with contouring of theremaining glenoid bone to a slightconcavity for pseudocongruencewith the humeral head component.
ArthrodesisAlthough arthrodesis of the gleno-
humeral joint has been described forend-stage RA,32 advances in pros-thetic replacement and surgical tech-nique have largely supplantedarthrodesis as the predominant pri-mary treatment of the end-stagerheumatoid shoulder. Arthrodesisof the rheumatoid shoulder shouldbe undertaken only for selected indi-cations. These indications includefailed total shoulder arthroplasty orend-stage involvement with a recenthistory of joint sepsis. In these situa-tions, patients may benefit fromglenohumeral fusion in 30° of abduc-tion, 30° of forward flexion, and 30°of internal rotation to allow for hand-to-mouth and hygiene activities.Arthrodesis can be done using a vari-ety of techniques, including screwfixation or plate-and-screw fixation.Although plate-and-screw fixationoffers the potential avoidance of post-operative spica immobilization, thebone quality in rheumatoid patientsmay limit the security of the fixation,and additional external (spica) immo-bilization still will be needed postop-eratively. The utility of shoulderarthrodesis must be evaluated in thecontext of ipsilateral and contralateralupper extremity involvement.
Acromioclavicular InvolvementRheumatoid involvement of the

Andrew L. Chen, MD, MS, et al
Vol 11, No 1, January/February 2003 23
References
1. Cuomo F, Greller MJ, Zuckerman JD:The rheumatoid shoulder. Rheum DisClin North Am 1998;24:67-82.
2. Petersson CJ: Painful shoulders inpatients with rheumatoid arthritis:Prevalence, clinical and radiological fea-tures. Scand J Rheumatol 1986;15:275-279.
3. Lipsky PE: Rheumatoid arthritis, inWilson JD, Braunwald E, IsselbacherKJ, et al (eds): Harrison’s Principles ofInternal Medicine, ed 12. New York,NY: McGraw-Hill, 1991, pp 1437-1442.
4. Shiozawa S, Shiozawa K: A review ofthe histopathological evidence on thepathogenesis of cartilage destructionin rheumatoid arthritis. Scand J Rheu-matol Suppl 1988;74:65-72.
5. Curran JF, Ellman MH, Brown NL:Rheumatologic aspects of painful con-ditions affecting the shoulder. ClinOrthop 1983;173:27-37.
6. Cofield RH: Degenerative and arthrit-ic problems of the glenohumeral joint,in Rockwood CA Jr, Matsen FA III(eds): The Shoulder. Philadelphia, PA:WB Saunders, 1990, pp 678-749.
7. Cruess RL: Rheumatoid arthritis ofthe shoulder. Orthop Clin North Am1980;11:333-342.
8. Kieft GJ, Dijkmans BA, Bloem JL,Kroon HM: Magnetic resonance imag-
ing of the shoulder in patients withrheumatoid arthritis. Ann Rheum Dis1990;49:7-11.
9. Albertsen M, Egund N, Jonsson E,Lidgren L: Assessment at CT of therheumatoid shoulder with surgical cor-relation. Acta Radiol 1994;35:164-168.
10. Ellman MH, Brown NL, Curran JJ:Shoulder arthritis: Distinguishingamong the many causes of inflamma-tion. Postgrad Med 1983;73:158-167.
11. Weiss TE, Gum OB, Biundo JJ Jr:Rheumatic diseases: 1. Differential diag-nosis. Postgrad Med 1976;60:141-150.
12. Brandt KD, Kovalov-St. John K:Osteoarthritis, in Wilson JD, BraunwaldE, Isselbacher KJ, et al (eds): Harrison’sPrinciples of Internal Medicine, ed 12.New York, NY: McGraw-Hill, 1991, pp1475-1479.
13. Laine VAI, Vainio KJ, Pekanmäki K:Shoulder affections in rheumatoid arthri-tis. Ann Rheum Dis 1954;13:157-160.
14. Neer CS: The rheumatoid shoulder, inCrubbs RL, Mitchell NS (eds): The Sur-gical Management of Rheumatoid Arthritis.Philadelphia, PA: JB Lippincott, 1971,pp 117-127.
15. Rozental TD, Sculco TP: Intra-articularcorticosteroids: An updated overview.Am J Orthop 2000;29:18-23.
16. Neer CS II: Reconstructive surgery andrehabilitation of the shoulder, in KelleyWN, Harris ED Jr, Ruddy S, Sledge CB(eds): Textbook of Rheumatology, ed 2.Philadelphia, PA: WB Saunders, 1985,vol 2, pp 1855-1870.
17. Neer CS II, Watson KC, Stanton FJ:Recent experience in total shoulderreplacement. J Bone Joint Surg Am1982;64:319-337.
18. Friedman RJ, Ewald FC: Arthroplasty ofthe ipsilateral shoulder and elbow inpatients who have rheumatoid arthritis.J Bone Joint Surg Am 1987;69:661-666.
19. Gill DR, Cofield RH, Morrey BF:Ipsilateral total shoulder and elbowarthroplasties in patients who haverheumatoid arthritis. J Bone Joint SurgAm 1999;81:1128-1137.
20. Hess EV: Rheumatoid arthritis: Treat-ment, in Schumacher HR Jr, KlippelJH, Robinson DR (eds): Primer on theRheumatic Diseases, ed 9. Atlanta, GA:Arthritis Foundation, 1988, pp 93-96.
21. Petersson CJ: Shoulder surgery inrheumatoid arthritis. Acta OrthopScand 1986;57:222-226.
22. Rozing PM, Brand R: Rotator cuff re-pair during shoulder arthroplasty inrheumatoid arthritis. J Arthroplasty1998;13:311-319.
acromioclavicular joint is common,affecting up to 63% of rheumatoidpatients with painful shoulders.33
It is often adequately addressednonsurgically with medicationsand corticosteroid injection. How-ever, persistent or progressivelydebilitating pain secondary toextensive, symptomatic erosionsmay necessitate distal clavicularresection with synovectomy, typi-cally with successful results.7
Petersson33 reported acromioclavic-ular joint resection and subacromi-al bursectomy to be an effectiveprocedure at follow-up of 18 to 62months. Either open or arthroscop-ic resection of the distal claviclemay be done. In the setting of RA,however, resection rarely is per-formed as an isolated procedure;more often, it is done at the time ofprosthetic replacement.
Sternoclavicular InvolvementThe reported incidence of rheu-
matoid involvement of the sterno-clavicular joint ranges from 1% to41%.34 Symptomatology typically isovershadowed by glenohumeralinvolvement and usually respondsto nonsurgical intervention andintra-articular injections. Recalci-trant symptoms lasting more than 6to 12 months may be addressedwith sternoclavicular joint débride-ment and medial clavicle resec-tion.34 Care must be taken to pre-serve the stabilizing ligaments toavoid complications associated withsternoclavicular instability.
Summary
Care of the patient with RA of theshoulder requires a multidisciplin-
ary approach involving the primarycare provider, rheumatologist,orthopaedic surgeon, and physi-cal/occupational therapists. Earlyrheumatoid involvement of theshoulder with minimal articular de-struction and functional limitationsmay be managed nonsurgicallywith medications and physical ther-apy. Advanced rheumatoid diseaseof the shoulder with significant painand articular destruction may neces-sitate surgical intervention, rangingfrom synovectomy to total shoulderarthroplasty. Although the resultsof prosthetic shoulder replacementfor end-stage RA are not compara-ble to those achieved for osteo-arthritis, symptomatic improvementoften is dramatic, with satisfactoryrelief of pain, improved range ofmotion, and increased functionalability.

Rheumatoid Arthritis of the Shoulder
Journal of the American Academy of Orthopaedic Surgeons24
23. Cofield RH, Frankle MA, ZuckermanJD: Humeral head replacement forglenohumeral arthritis. Semin Arthro-plasty 1995;6:214-221.
24. Boyd AD Jr, Thomas WH, Scott RD,Sledge CB, Thornhill TS: Total shoul-der arthroplasty versus hemiarthro-plasty: Indications for glenoid resur-facing. J Arthroplasty 1990;5:329-336.
25. McCoy SR, Warren RF, Bade HA III,Ranawat CS, Inglis AE: Total shoulderarthroplasty in rheumatoid arthritis. JArthroplasty 1989;4:105-113.
26. Koorevaar RC, Merkies ND, de WaalMalefijt MC, Teeuwen M, van denHoogen FH: Shoulder hemiarthro-plasty in rheumatoid arthritis: 19 casesreexamined after 1-17 years. ActaOrthop Scand 1997;68:243-245.
27. Sojbjerg JO, Frich LH, Johannsen HV,
Sneppen O: Late results of total shoul-der replacement in patients withrheumatoid arthritis. Clin Orthop1999;366:39-45.
28. Stewart MP, Kelly IG: Total shoulderreplacement in rheumatoid disease: 7-to 13-year follow-up of 37 joints. JBone Joint Surg Br 1997;79:68-72.
29. Friedman RJ, Thornhill TS, ThomasWH, Sledge CB: Non-constrainedtotal shoulder replacement in patientswho have rheumatoid arthritis andclass-IV function. J Bone Joint Surg Am1989;71:494-498.
30. Sneppen O, Fruensgaard S, JohannsenHV, Olsen BS, Sojbjerg JO, AndersenNH: Total shoulder replacement inrheumatoid arthritis: Proximal migra-tion and loosening. J Shoulder ElbowSurg 1996;5:47-52.
31. Cofield RH, Chang W, Sperling JW:Complications of shoulder arthroplasty,in Iannotti JP, Williams GR (eds):Disorders of the Shoulder: Diagnosis andManagement. Philadelphia, PA: Lip-pincott Williams & Wilkins, 1999, pp571-593.
32. Rybka V, Raunio P, Vainio K: Arthrodesisof the shoulder in rheumatoid arthri-tis: A review of forty-one cases. J BoneJoint Surg Br 1979;61:155-158.
33. Petersson CJ: The acromioclavicularjoint in rheumatoid arthritis. ClinOrthop 1987;223:86-93.
34. Wirth MA, Rockwood CA Jr: Chronicconditions of the acromioclavicular andsternoclavicular joints, in ChapmanMW, Madison M (eds): OperativeOrthopaedics, ed 2. Philadelphia, PA: JBLippincott, 1993, vol 2, pp 1673-1693.