richter transformation in the oral and maxillofacial area
TRANSCRIPT

Vol. 131 No. 1 January 2021
Richter transformati
on in the oral and maxillofacial area:report of 2 cases and literature review Vasileios Ionas Theofilou, DDS, MSc Student,a Nikolaos Katsoulas, MD, DDS, MSc,bKonstantinos I. Tosios, DDS, PhD,c Alexandra Sklavounou, DDS, MSc, PhD,d and
Nikolaos G. Nikitakis, MD, DDS, PhDe
Richter transformation (RT) is a term used to refer to the development of an aggressive lymphoma, usually of diffuse large B-cell
lymphoma type, in a patient with a history of chronic lymphocytic leukemia. It may present with heterogeneous manifestations,
including the occurrence of tumors at extranodal sites. To date, only 6 cases of RT involving the oral and maxillofacial region
have been reported. Here, we present 2 rare cases of lymphoma initially affecting the maxilla and the lower gingiva, respectively,
of female patients with chronic lymphocytic leukemia and review the English language literature about RT manifesting in the oral
and maxillofacial tissues. (Oral Surg Oral Med Oral Pathol Oral Radiol 2021;131:e14�e20)
The term Richter transformation (RT) or Richter
syndrome describes the development of an aggressive
lymphoma in a patient with chronic lymphocytic leuke-
mia (CLL). This is usually a non-Hodgkin lymphoma
(NHL), more commonly a diffuse large B-cell lym-
phoma (DLBCL)1,2 and rarely Hodgkin lymphoma
(HL-Richter),3 or another aggressive lymphoid malig-
nancy, such as composite lymphoma,4 dendritic cell
sarcoma,5 or plasmablastic lymphoma.6 Multiple mye-
loma may also develop in patients with CLL, although
it is controversial whether this is coincidental or repre-
sents a Richter-like phenomenon.7
The prevalence of RT among patients with CLL
varies from 0.7% to 23%.8 In a prospective cohort
study,1 in approximately 2% of patients with CLL,
DLBCL developed in 5 years, whereas the 10-year
incidence of RT has ranged from 4.9%1 to 16.2%.9
RT is more common in males and median age is
greater than 60 years.1,2 Predisposing factors include
advanced-stage CLL1,9; lymph nodes 3 cm or greater9;
expression by neoplastic cells of proteins ZAP70,1,9
CD38,1,9 or CD49d1; nonmutated immunoglobulin
heavy-chain variable region gene (IGHV)1; IGHV4-39
usage9; absence of del (13q14)9 and presence of del
aDepartment of Oral Medicine and Pathology, Faculty of Dentistry,
National and Kapodistrian University of Athens, Athens, Greece.bDepartment of Oral Medicine and Pathology, Faculty of Dentistry,
National and Kapodistrian University of Athens, Athens, Greece.cAssociate Professor, Department of Oral Medicine and Pathology,
Faculty of Dentistry, National and Kapodistrian University of
Athens, Athens, Greece.dProfessor, Department of Oral Medicine and Pathology, Faculty of
Dentistry, National and Kapodistrian University of Athens, Athens,
Greece.eProfessor and Chair, Department of Oral Medicine and Pathology,
Faculty of Dentistry, National and Kapodistrian University of
Athens, Athens, Greece.
Received for publication Nov 24, 2019; returned for revision Jan 16,
2020; accepted for publication Feb 17, 2020.
� 2020 Elsevier Inc. All rights reserved.
2212-4403/$-see front matter
https://doi.org/10.1016/j.oooo.2020.02.016
e14
(11q22.3) or del (17p13)1; and prior treatment for
CLL.1
We report here 2 cases of CLL in which DLBCL
developed in the oral cavity and review the literature
on oral and maxillofacial involvement by RT.
CASE REPORTSCase 1An 82-year-old female was referred by her dentist for
evaluation of “poor soft tissue healing following periodon-
tal scaling.” Five years earlier, the patient had been diag-
nosed with CLL stage I that did not necessitate any kind
of treatment, and she was under regular follow-up by her
hematologist. Complete blood count a month before pre-
sentation to us showed lymphocytosis (76%; normal range
18%�44%) and increased lactate dehydrogenase (LDH;
326 units/L; normal range 122�214 units/L), as well as
normocytic anemia (red blood cell [RBC] count
3,620,000/mL; normal range 4,200,000�5,400,000/mL;hematocrit [Hct] 35%; normal range 36%�46%; hemo-
globin [Hgb] 11.4 g/100 mL; normal range 12�16 g/100
mL; mean corpuscular volume [MCV] 97 fL; normal
range 77�98 fL); and neutropenia (13%; normal range
35%�80%). These findings were considered consistent
with the underlying disease by her attending hematologist.
She was treated for rheumatoid arthritis with hydroxy-
chloroquine and for chronic atrophic gastritis with
monthly injections of B12. Her medical history also
included hyperthyroidism, hypertension, and osteoporosis
that were not being treated.
Clinical examination showed that the patient was
edentulous, except for 4 teeth in the anterior mandible
(Figure 1). The gingiva surrounding those teeth were
enlarged, erythematous, and ulcerated. The rest of the
oral mucosa was within normal limits. A panoramic
radiograph showed limited alveolar bone loss around
teeth, consistent with chronic periodontitis.
Because of the history of CLL, infiltration of the gingiva
by the hematologic malignancy was suspected, and inci-
sional biopsy was performed. Microscopic examination

Fig. 1. Patient 1. Diffuse gingival enlargement affecting the
anterior mandibular gingiva.
OOOO CASE REPORT
Volume 131, Number 1 Theofilou et al. e15
showed diffuse infiltration by small cells with morphologic
characteristics of lymphocytes, mostly in the superficial
lamina propria (Figure 2A), and large atypical mononucle-
ated or binucleated cells with anaplastic characteristics in
the deeper locations (Figure 2B). Abundant mitoses were
also present. After a provisional hematoxylin and
eosin�based diagnosis of lymphoproliferative lesion, fur-
ther examination of the biopsy tissue was performed by an
expert hematopathologist. Immunohistochemically, the
small cells were CD20+, CD79a+, CD5+, OCT+,
CD23�, CD30�, CD15�, CD3�, and multiple myeloma
oncogene (MUM)�, whereas in situ hybridization for
Epstein-Barr virus (EBV)�encoded RNA was negative.
The large cells were CD20+ and CD79a+ (in equal num-
bers), CD23+, CD30+>>CD15+, OCT+, MUM+, CD5-,
Fig. 2. Patient 1. Microscopic examination shows (A) small cells with
location and (B, C) large pleomorphic cells with anaplastic features
magnification£ 400). A high-resolution version of this slide for use wit
CD3-, whereas EBV�encoded RNA was positive. Poly-
merase chain reaction was performed for
the identification of immunoglobulin heavy-chain
(IGVH) gene mutational status and proved a clonal
relationship between the underlying and the present
hematologic malignancy. The final diagnosis was
gingival infiltration by a CD5+, CD23� B-cell lym-
phoproliferative lesion with small lymphocytic fea-
tures, consistent with CLL, with transformation to a
diffuse high grade EBV(+) B-cell lymphoma com-
posed of large anaplastic CD30+>>CD15+ cells, in
the context of Richter syndrome.
The patient was treated with 6 cycles of chemother-
apy with rituximab (500 mg), cyclophosphamide (1000
mg), vincristine (1.8 mg), and prednisolone (75 mg), as
well as 30 cycles of radiotherapy (total dose 30 Gy).
However, she was lost to follow-up.
Case 2A 70-year-old female presented for the evaluation and
management of a painless mass in the upper lip.
According to her account, it had been first noticed
approximately 3 years earlier, but in the past 3 weeks,
it had enlarged and excreted pus-like material. Her den-
tist had ruled out a dental or periodontal origin. Her
medical history was significant for CLL stage I, diag-
nosed approximately 8 years earlier. She had not
received any treatment for CLL and was under regular
follow-up by her attending hematologist. Blood tests
phenotypic characteristics of lymphocytes in a more superficial
in the deep lamina propria (hematoxylin and eosin stain; initial
h the Virtual Microscope is available as eSlide: VM05760.

Fig. 3. Patient 2. Large mass in the anterior maxilla projec-
ting to the (A) sulcus and (B) palate.
Fig. 4. Patient 2. Three-dimensional (3-D) reconstruction of
the cone beam computed tomography scan shows a hypo-
dense lesion causing perforation of the buccal and palatal cor-
tical plates and extending to the floor of the nasal cavity.
ORAL ANDMAXILLOFACIAL PATHOLOGY OOOO
e16 Theofilou et al. January 2021
during this period showed CLL-associated leukocytosis
and anemia managed with folic acid per os. LDH was
within normal limits (377 units/L; normal range
230�460). The patient was also being treated for
hypertension with amlodipine besylate, hypothyroid-
ism with levothyroxine sodium, and osteopenia with
risedronate sodium.
Clinical examination revealed a tumor in the middle
of the maxilla and extending to the sulcus and the pal-
ate (Figures 3A and 3B). The tumor was covered by
normal-appearing mucosa and was soft to fluctuant and
painless on palpation. The involved teeth showed class
II mobility. The rest of the oral mucosa was within nor-
mal limits. Cone beam computed tomography showed
an ill-defined soft tissue density lesion in the anterior
region of the maxilla, measuring approximately
3.5 £ 3.0 £ 2.5 cm, causing perforation of both the
frontal and palatal cortical plates and extending to the
floor of the nasal cavity (Figure 4).
Incisional biopsy was performed with the patient under
local anesthesia, and histopathologic examination showed
diffuse infiltration by large atypical neoplastic cells
(Figure 5) with pleomorphic grooved nuclei and indistinct
nucleoli. Mitoses, some of them atypical, were also
detected. Additionally, small cells with phenotypic charac-
teristics consistent with lymphocytes were distinguished
focally, mostly in perivascular and perineural localization.
Crush artifacts were observed. These features were consis-
tent with NHL, and after further investigation by an expert
hematopathologist, the immunoprofile of the tumor was
shown to be positive for CD20, CD79a, bcl2, bcl6, CD23,
and CD30 and negative for c-myc, CD10, MUM-1, CD5,
and CD138; the Ki67 index was 80% to 90%. Based on
the histologic and immunohistochemical examination, the
diagnosis was diffuse large B-cell lymphoma with features
not otherwise specified, probably originating from the ger-
minal center.
A full workup of the patient was undertaken, but no
significant findings were revealed on chest and abdomi-
nal CT scans, the imaging features being similar to the
latest evaluation performed 3 years ago.
The patient underwent 8 cycles of treatment with carfil-
zomib. Five months after commencement of therapy, her
clinical condition and laboratory findings were satisfac-
tory, and the maxillary lesion had regressed completely
(Figure 6). Twenty-one months later no sign of recurrence
was present.
DISCUSSIONWe reported here 2 cases of DLBCL developing in the
oral cavity of patients with CLL, which conformed to the
diagnosis of RT.2 An English language literature review
disclosed 6 previously reported cases of oral and maxillo-
facial RT,10-15 whose main features, along with those of
the present cases, are summarized in Table I. Mean age
was 65.1 years, and females were more commonly
affected compared with males (female/male ratio 6:2).
The latter finding is in contrast to the more common find-
ing of more involvement in males by both RT1,2 and oral
and maxillofacial lymphomas.16
DLBCL, the most frequently encountered type of
NHL in the oral and maxillofacial area16 and the most
common lymphoma in RT,1,2 was diagnosed in the

Fig. 5. A, B, Patient 2. Diffuse proliferation by large atypical
basophilic cells with occasional mitoses, intermixed with
smaller cells with morphologic features of lymphocytes
(hematoxylin and eosin stain; initial magnification £ 400). A
high-resolution version of this slide for use with the Virtual
Microscope is available as eSlide: VM05761.
OOOO CASE REPORT
Volume 131, Number 1 Theofilou et al. e17
majority of cases (6 patients), whereas in 2 patients, the
diagnosis was plasmablastic lymphoma. Mean time
between diagnosis of CLL and development of RT was
approximately 5 years. The jaws were the most com-
mon site of involvement, with 6 of 8 cases (2 cases in
the maxilla, 2 in the mandible, 1 with simultaneous
involvement of both jaws, and 1 in an unspecified jaw),
followed by the gingiva and the cheek, with 1 case
each. This distribution is in agreement with the com-
mon and equal involvement of both jaws by NHL.16,17
Lymphomas in RT are, in most cases, clonally related to
the pre-existing CLL directly—that is, lymphoma cells
Fig. 6. Patient 2. Complete response of the maxillary lesion 5
months after initiation of chemotherapy.
derive from the original CLL clone (linear evolution); or
indirectly, both CLL and lymphoma cells derive from a
common precursor cell (branching evolution).18 Clonal
relationship should be established by IGHV-D-J rearrange-
ment analysis.8,19 This is considered essential because of
differences in the therapeutic management of clonally
related and clonally unrelated RT, with the latter being
treated in a similar fashion to de novo DLBCL.8,19 A clonal
relationship between CLL and lymphoma was proved in
one of our cases (case 1) and in that of Evans et al.14
In approximately 20% of NHL developing in
patients with CLL, a clonal relationship cannot be
established.20 In those cases, the biologic features and
prognoses are more comparable with those of conven-
tional NHL; therefore, they are considered to be de
novo malignanicies.8
Even though the exact molecular mechanisms of RT
have not been fully elucidated, there are reports of genetic
alterations in CLL cells that cause transformation to the
clonally related lymphoma. Approximately 90% of RT
cases exhibit genetic lesions in pathways that cause disrup-
tion of general cell regulators, such as tumor suppression,
cell cycle, and cell proliferation (e.g., TP53, NOTCH1,
MYC, and CDKN2A).18 Those genetic lesions are associ-
ated with the aggressive clinical behavior resulting from
acquired features—resistance to chemotherapy and rapid
disease progression.18
Previous therapy has also been suggested as a risk
factor for the development of RT, although a mecha-
nism has not been described.1 From another point of
view, CLL requiring chemotherapy is usually an
aggressive disease with poor biologic behavior, where
the risk for the development of a lymphoma is, never-
theless, high.1 We reported for the first time 2 cases
where RT developed in the oral cavity of patients with
no previous treatment for CLL because in the previ-
ously reported 6 cases, different types of chemothera-
peutic regimens had been applied.
RT in CLL-untreated patients is rarely EBV related,
whereas in patients in immunosuppressive therapy, it is
suggested that EBV reactivation may drive the devel-
opment of the aggressive lymphoma.21 One of the
cases presented here (case 1) is the first EBV-positive,
clonally related oral RT in a previously untreated
patient with CLL. Although the EBV status of the
patient before RT was not known, it may be hypothe-
sized that in this case, a secondary EBV infection drove
the lymphomatogenesis.
Diagnosis of RT is based on clinical and pathologic
examinations, as well as imaging. Severe deterioration
in a patient with CLL manifesting fever, rapid lymph-
adenopathy, extranodal involvement presenting with
tumors mostly of the gastrointestinal tract or bones,
severe weight loss, hypercalcemia, and markedly ele-
vated LDH are features that could raise the suspicion
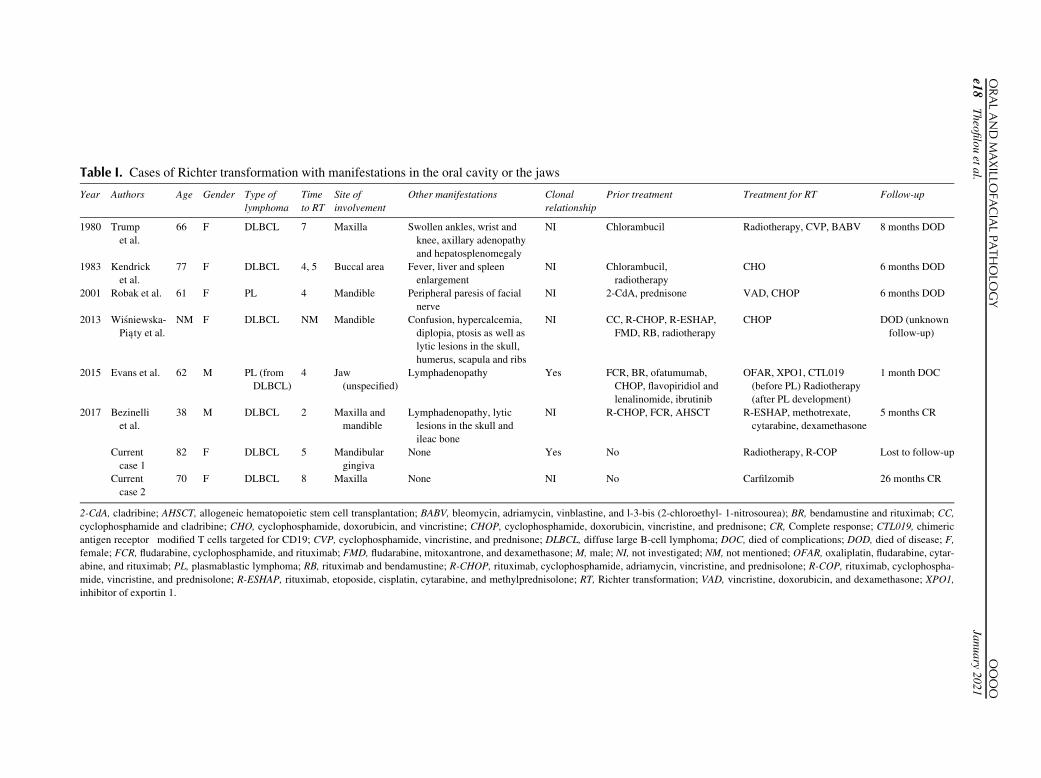
Table I. Cases of Richter transformation with manifestations in the oral cavity or the jaws
Year Authors Age Gender Type of
lymphoma
Time
to RT
Site of
involvement
Other manifestations Clonal
relationship
Prior treatment Treatment for RT Follow-up
1980 Trump
et al.
66 F DLBCL 7 Maxilla Swollen ankles, wrist and
knee, axillary adenopathy
and hepatosplenomegaly
NI Chlorambucil Radiotherapy, CVP, BABV 8 months DOD
1983 Kendrick
et al.
77 F DLBCL 4, 5 Buccal area Fever, liver and spleen
enlargement
NI Chlorambucil,
radiotherapy
CHO 6 months DOD
2001 Robak et al. 61 F PL 4 Mandible Peripheral paresis of facial
nerve
NI 2-CdA, prednisone VAD, CHOP 6 months DOD
2013 Wi�sniewska-Piaty et al.
NM F DLBCL NM Mandible Confusion, hypercalcemia,
diplopia, ptosis as well as
lytic lesions in the skull,
humerus, scapula and ribs
NI CC, R-CHOP, R-ESHAP,
FMD, RB, radiotherapy
CHOP DOD (unknown
follow-up)
2015 Evans et al. 62 M PL (from
DLBCL)
4 Jaw
(unspecified)
Lymphadenopathy Yes FCR, BR, ofatumumab,
CHOP, flavopiridiol and
lenalinomide, ibrutinib
OFAR, XPO1, CTL019
(before PL) Radiotherapy
(after PL development)
1 month DOC
2017 Bezinelli
et al.
38 M DLBCL 2 Maxilla and
mandible
Lymphadenopathy, lytic
lesions in the skull and
ileac bone
NI R-CHOP, FCR, AHSCT R-ESHAP, methotrexate,
cytarabine, dexamethasone
5 months CR
Current
case 1
82 F DLBCL 5 Mandibular
gingiva
None Yes No Radiotherapy, R-COP Lost to follow-up
Current
case 2
70 F DLBCL 8 Maxilla None NI No Carfilzomib 26 months CR
2-CdA, cladribine; AHSCT, allogeneic hematopoietic stem cell transplantation; BABV, bleomycin, adriamycin, vinblastine, and l-3-bis (2-chloroethyl- 1-nitrosourea); BR, bendamustine and rituximab; CC,
cyclophosphamide and cladribine; CHO, cyclophosphamide, doxorubicin, and vincristine; CHOP, cyclophosphamide, doxorubicin, vincristine, and prednisone; CR, Complete response; CTL019, chimeric
antigen receptor�modified T cells targeted for CD19; CVP, cyclophosphamide, vincristine, and prednisone; DLBCL, diffuse large B-cell lymphoma; DOC, died of complications; DOD, died of disease; F,
female; FCR, fludarabine, cyclophosphamide, and rituximab; FMD, fludarabine, mitoxantrone, and dexamethasone; M, male; NI, not investigated; NM, not mentioned; OFAR, oxaliplatin, fludarabine, cytar-
abine, and rituximab; PL, plasmablastic lymphoma; RB, rituximab and bendamustine; R-CHOP, rituximab, cyclophosphamide, adriamycin, vincristine, and prednisolone; R-COP, rituximab, cyclophospha-
mide, vincristine, and prednisolone; R-ESHAP, rituximab, etoposide, cisplatin, cytarabine, and methylprednisolone; RT, Richter transformation; VAD, vincristine, doxorubicin, and dexamethasone; XPO1,
inhibitor of exportin 1.
ORALAND
MAXILLO
FACIALPATHOLO
GY
OOOO
e18
Theofilouetal.
January
2021

OOOO CASE REPORT
Volume 131, Number 1 Theofilou et al. e19
of RT development.8,19 In both cases presented here,
the patients did not have any signs or symptoms other
than swelling in the oral cavity. The most common
signs in previously reported cases of oral and maxillo-
facial RT (see Table I) were lymphadenopathy in 3
cases, followed by hepatosplenomegaly and lytic
lesions in bones other than the jaws in 2 cases each.
Histopathologic examination most commonly
reveals diffuse infiltration by large atypical cells exhib-
iting pleomorphism and a centroblastic morphology.20
They are CD20 positive, with the markers CD5 and
CD23 suggestive of CLL being expressed in 32% and
14%, respectively.20 RT cases most commonly show a
nongerminal phenotype, whereas germinal center B-
cell type DLBCL cases are rarer.20,22
When RT is suspected in the absence of clinically
evident nodal or extranodal masses, imaging with F-18
fluorodeoxyglucose positron emission tomography is
the diagnostic procedure of choice.8,19 The characteris-
tics of the lesions detected, along with the standardized
uptake value, exhibit a significant sensitivity and indi-
cate whether biopsy should be performed, facilitating
the diagnosis of RT.8
RT treatment is challenging. Immunochemotherapy,
stem cell transplantation, and novel targeted therapeutic
agents have been tested with varying results with regard to
patients’ response and overall survival.8. DLBCL in
patients with RT acquires significant resistance to chemo-
therapy.8 Some of the chemotherapeutic regimens exhibit
a low complete response rate (7%), with higher overall
survival (21 months) and low treatment-induced mortality
(5%),23 whereas others show a better response (complete
response 38%) with a lower overall survival (10 months)
because of the high toxicity of the chemotherapeutic
agents.24 Allogenic and autologous stem cell transplanta-
tions have been used. Overall 3-year survival of patients
receiving allogenic stem cell transplantation and autolo-
gous stem cell transplantation is 36% and 59%, respec-
tively, as indicated by a retrospective analysis.25 However,
in most cases, stem cell transplantation is not an option
because patients are unfit, either because of their age or
because of insufficient response to initial chemotherapeutic
treatment.25 Novel agents that target the molecular path-
ways deregulated in patients with RT include the Bruton
tyrosine kinase inhibitor ibrutinib, the B-cell lymphoma 2
antagonist venetoclax, the programmed cell death protein
1 antagonist pembrolizumab, and the exportin 1 inhibitor
selexinor. The overall response rate varies from 33% for
selexinor26 to 75% for ibrutinib,27 but the number of cases
studied is too limited for any conclusions to be reached.
Of the 8 cases presented in Table I, different immuno- or
chemotherapeutic regimens were applied in 5 cases, com-
bination of chemotherapy with radiation therapy in 2 cases,
solely radiation in 1 case.
The median survival of patients with CLL with RT is
approximately 2 years,1 with clonally unrelated cases
exhibiting a behavior similar to that of de novo DLBCL,
whereas clonally related cases have a significantly lower
survival rate. Additional factors diminishing overall sur-
vival are LDH levels greater than 1.5 times the normal,28
tumor size greater than 5 cm,28 platelet count less than
100 £ 109/L,28 number of prior therapies greater than
1,28 Zubrod score greater than 1,21,28 TP53 deletions or
mutations,19 and poor response to RT treatment.19 Five of
the patients with oral and maxillofacial RT died either as
a result of the spread of the lymphoma or because of che-
motherapeutic toxicity, at a mean period of approxi-
mately 5 months, and 2 patients showed signs of
remission at the 5-month follow-up.
CONCLUSIONSAlthough first presentation of RT in the oral and maxil-
lofacial area is extremely rare, clinicians should have a
high level of suspicion when dealing with patients with
CLL showing atypical lesions in the area because these
lesions could be manifestations of an underlying RT.
ACKNOWLEDGMENTSWe are grateful for the expert assistance of Ms. Maria
Manou, technician.
REFERENCES1. Parikh SA, Rabe KG, Call TG, et al. Diffuse large B-cell lym-
phoma (Richter syndrome) in patients with chronic lymphocytic
leukaemia (CLL): a cohort study of newly diagnosed patients.
Br J Haematol. 2013;162:774-782.
2. Tadmor T, Shvidel L, Bairey O, et al. Richter’s transformation to
diffuse large B-cell lymphoma: a retrospective study reporting
clinical data, outcome, and the benefit of adding rituximab to
chemotherapy, from the Israeli CLL Study Group. Am J Hema-
tol. 2014;89:E218-E222.
3. Parikh SA, Habermann TM, Chaffee KG, et al. Hodgkin trans-
formation of chronic lymphocytic leukemia: incidence, out-
comes, and comparison to de novo Hodgkin lymphoma. Am J
Hematol. 2015;90:334-338.
4. Michelis FV, Kourti G, Skertsou M, Karmiris T, Rontogianni DP,
Harhalakis N. Richter transformation of chronic lymphocytic leu-
kemia into composite diffuse large B-cell and Hodgkin lym-
phoma. Leuk Lymphoma. 2012;53:2302-2303.
5. Fraser CR, Wang W, Gomez M, et al. Transformation of chronic
lymphocytic leukemia/small lymphocytic lymphoma to interdig-
itating dendritic cell sarcoma evidence for transdifferentiation of
the lymphoma clone. Am J Clin Pathol. 2009;132:928-939.
6. Martinez D, Valera A, Perez NS, et al. Plasmablastic transforma-
tion of low-grade b-cell lymphomas: report on 6 cases. Am J
Surg Pathol. 2013;37:272-281.
7. Alley CL, Wang E, Dunphy CH, et al. Diagnostic and clinical
considerations in concomitant bone marrow involvement by
plasma cell myeloma and chronic lymphocytic leukemia/mono-
clonal B-Cell lymphocytosis: a series of 15 cases and review of
literature. Arch Pathol Lab Med. 2013;137:503-517.
8. Rossi D, Gaidano G. Richter syndrome: pathogenesis and man-
agement. Semin Oncol. 2016;43:311-319.

ORAL ANDMAXILLOFACIAL PATHOLOGY OOOO
e20 Theofilou et al. January 2021
9. Rossi D, Cerri M, Capello D, et al. Biological and clinical risk
factors of chronic lymphocytic leukaemia transformation to
Richter syndrome. Br J Haematol. 2008;142:202-215.
10. Trump DL, Mann RB, Phelps R, Roberts H, Conley CL.
Richter’s syndrome: diffuse histiocytic lymphoma in patients
with chronic lymphocytic leukemia. A report of five cases and
review of the literature. Am J Med. 1980;68:539-548.
11. Kendrick RW, Schwartz HC. Richter’s syndrome presenting as a
facial swelling. Oral Surg Oral Med Oral Pathol. 1983;56:301-304.
12. Robak T, Urba�nska-Ry�s H, Strzelecka B, et al. Plasmablastic
lymphoma in a patient with chronic lymphocytic leukemia
heavily pretreated with cladribine (2-CDA): an unusual variant
of Richter’s syndrome. Eur J Haematol. 2001;67:322-327.
13. Wi�sniewska-Piaty K, Helbig G, Wo�zniczka K, Frankiewicz A,
Dziaczkowska-Suszek J, Kyrcz-Krzemie�n S. Richter’s syndrome
manifested as diffuse large B-cell lymphoma of the mandible
with lytic lesions and hypercalcemic crisis. Acta Haematol Pol.
2013;44:409-412.
14. Evans AG, Rothberg PG, Burack WR, et al. Evolution to plas-
mablastic lymphoma evades CD19-directed chimeric antigen
receptor T cells. Br J Haematol. 2015;171:205-209.
15. Bezinelli LM, de Paula Eduardo F, Marques da Graca Lopes R,
Pasqualin D da C, Hamerschlak N, Correa L. Tumor mass in the
palate after bone marrow transplantation. Oral Surg Oral Med
Oral Pathol Oral Radiol. 2017;124:107-113.
16. Guevara Canales JO, Morales Vadillo R, de Faria PEA, Sacsa-
quispe Contreras SJ, Leite FPP, Chavez MGMA. Systematic
review of lymphoma in oral cavity and maxillofacial region.
Acta Odontol Latinoam. 2011;24:245-251.
17. Matsuzaki H, Katase N, Hara M, et al. Primary extranodal lym-
phoma of the maxilla: a case report with imaging features and
dynamic data analysis of magnetic resonance imaging. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod. 2011;112:e59-e69.
18. Fabbri G, Khiabanian H, Holmes AB, et al. Genetic lesions asso-
ciated with chronic lymphocytic leukemia transformation to
Richter syndrome. J Exp Med. 2013;210:2273-2288.
19. Khan M, Siddiqi R, Thompson PA. Approach to Richter trans-
formation of chronic lymphocytic leukemia in the era of novel
therapies. Ann Hematol. 2018;97:1-15.
20. Mao Z, Quintanilla-Martinez L, Raffeld M, et al. IgVH muta-
tional status and clonality analysis of Richterʼs transformation.
Am J Surg Pathol. 2007;31:1605-1614.
21. Garc�ıa-Barchino MJ, Sarasquete ME, Panizo C, et al. Richter
transformation driven by Epstein-Barr virus reactivation during
therapy-related immunosuppression in chronic lymphocytic leu-
kaemia. J Pathol. 2018;245:61-73.
22. Rossi D, Spina V, Deambrogi C, et al. The genetics of Richter
syndrome reveals disease heterogeneity and predicts survival
after transformation. Blood. 2011;117:3391-3401.
23. Langerbeins P, Busch R, Anheier N, et al. Poor efficacy and tolera-
bility of R-CHOP in relapsed/refractory chronic lymphocytic leuke-
mia and Richter transformation. Am J Hematol. 2014;89:E239-E243.
24. Dabaja BS, O’Brien SM, Kantarjian HM, et al. Fractionated
cyclophosphamide, vincristine, liposomal daunorubicin (dau-
noxome), and dexamethasone (hyperCVXD) regimen in
Richter’s syndrome. Leuk Lymphoma. 2001;42:329-337.
25. Cwynarski K, van Biezen A, de Wreede L, et al. Autologous and
allogeneic stem-cell transplantation for transformed chronic
lymphocytic leukemia (Richter’s syndrome): a retrospective
analysis from the chronic lymphocytic leukemia subcommittee
of the chronic leukemia working party and lymphoma working
party of the European Group for Blood and Marrow Transplanta-
tion. J Clin Oncol. 2012;30:2211-2217.
26. Kuruvilla J, Savona M, Baz R, et al. Selective inhibition of
nuclear export with selinexor in patients with non-Hodgkin’s
lymphoma. Blood. 2017;129:3175-3183.
27. Tsang M, Shanafelt TD, Call TG, et al. The efficacy of ibrutinib in
the treatment of Richter syndrome. Blood. 2015;125:1676-1678.
28. Tsimberidou AM, O’Brien S, Khouri I, et al. Clinical outcomes and
prognostic factors in patients with Richter’s syndrome treated with
chemotherapy or chemoimmunotherapy with or without stem-cell
transplantation. J Clin Oncol. 2006;24:2343-2351.
Reprint requests:
Vasileios I. Theofilou
Department of Oral Medicine and Pathology
Faculty of Dentistry
2 Thivon Street
11526 Athens
Greece.