right hand page--------> trim size = 10.875 x...
TRANSCRIPT

Volume 46 January 2008 No. 9
See Fee, page 8 See Certification, page 16
Massive Medicare fee cutaverted for 6 months
President’s ColumnScouting continued
competence
3 9
Glance at the StatesOhio expands orals
authority, scope of practice
Just prior to its adjourn-ment for 2007, Congressapproved legislation that
included a stop-gap planbacked by the AOA that hassuccessfully blocked a mas-sive 10.1 percent Medicarephysician payment cut thatwas due to take effect on Jan.1, 2008.
The measure, which wassigned by President Bush onDec. 29, wards off a cut inMedicare Part B reimburse-ments for six months and
delivers ODs, MDs and otherproviders a marginal 0.5 per-cent increase in theirMedicare Part B reimburse-ments.
However, as the AOAWashington office noted in ayear-end report, optometrywill again be urging Congressto address the Medicarephysician reimbursementissue again during the firsthalf of this year.
Otherwise, the plannedfee cut will take effect on
July 1 and could then be fol-lowed by a further reductionin January 2009.
The AOA and otherhealth care provider groupsare already preparing for amassive lobbying effort aimedat securing a long-overduereform of the Medicare fee-setting formula and a long-term stabilization of the feder-al government health plan’sphysician reimbursements.
Seattle's lively and dynamic waterfront offers sightseeing, dining andshopping galore. Registration opens in February for the 111th AnnualAOA Congress & 38th Annual AOSA Conference: Optometry’s Meeting™in Seattle at www.optometrysmeeting.org. See coverage, page 7.Photo: Seattle's Convention and Visitors Bureau.
Profession takingfresh look at board certification
Over the next twoyears, representativesof six optometric
organizations hope to use thelessons learned by optometry,as well as other health careprofessions, to propose amodel for board certificationin optometry. The modelwould then be presented todecision-making bodies with-in the six organizations – inthe AOA’s case, the House ofDelegates, for review, discus-sion and approval.
The Joint BoardCertification Project Teamincludes representatives whowere chosen by the leadershipof their respective organiza-tions; the American Academyof Optometry (AAO), theAOA, American OptometricStudent Association (AOSA),the Association of RegulatoryBoards of Optometry(ARBO), the Association ofSchools and Colleges ofOptometry (ASCO), and theNational Board of Examinersin Optometry (NBEO). Thegroup met in November fortheir third formal meeting.Another is scheduled for
February.“Of all the prescribing,
doctoral-level health care pro-fessions in the United States,optometry is the only profes-sion that does not have aboard certification processavailable as a measure ofongoing advanced clinicalcompetence,” said AOA VicePresident Randy Brooks,O.D., chair of the Joint BoardCertification Project Team.
He noted that some pro-fessions have multiple certifi-cation bodies, each with dif-ferent standards. For exam-ple, podiatry has three certifi-cation organizations, eachwith different criteria for cer-tification.
Meanwhile, demand isbuilding for proof that ahealth care professional haskept current with training andhas demonstrable patient careskills.
The federal governmentthrough its Pay-for-Performance initiatives, man-aged care organizations withincreased recordkeeping and
January.qxp 1/10/2008 3:11 PM Page 1
Fri Jan 11 10:29:49 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_1.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

January.qxp 1/10/2008 3:13 PM Page 2
Fri Jan 11 10:30:14 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_2.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

American Optometric Association News (ISSN: 0094-9620) is published 18 times per year by Elsevier Inc., 360 Park Avenue South, New York, NY 10010. Months of issue are once monthly in January, June, July, August, November, and December
and twice monthly in February, March, April, May, September and October. Business Office: 11830 Westline Industrial Drive, St. Louis, MO 63146.
Editorial Office: 243 N. Lindbergh Blvd., St. Louis, MO 63141. Accounting and Circulation Offices: 6277 Sea Harbor Drive, Orlando, FL 32887-4800.
Domestic subscriptions: $97. International subscriptions: $126. Customer service: 800-654-2452 (US and Canada) or 407-363-9661 (other countries).
Periodicals postage paid at New York, NY and at additional mailing offices.POSTMASTER: Send address changes to American Optometric Association News,
Elsevier Periodicals Department, 6277 Sea Harbor Drive, Orlando, FL 32887-4800.
PRESIDENT’S COLUMN
Change of address: Notify pub-lisher at least six weeks in advance,including both mailing label from themost recent issue and the newaddress with proper ZIP code. Accep-tance for advertising for publicationsdoes not constitute approval orendorsement by the NEWS or theAOA. All advertising is subject toreview for acceptability by the AOACommunications Group. Acceptanceand/or publication of editorial mate-rial in the NEWS does not constituteapproval or endorsement by theNEWS, or the AOA.
Advertising
Display AdvertisingAileen Rivera
Advertising Sales RepresentativeElsevier
360 Park Avenue SouthNew York, NY 10010-1710
(212) 633-3721Fax: (212) 633-3820
E-Mail: [email protected]
Classified AdvertisingKeida Spurlock
Advertising Sales RepresentativeElsevier
360 Park Avenue SouthNew York, NY 10010-1710
(212) 633-3986Fax: (212) 633-3820
E-MAIL: [email protected]
AOA Board
Kevin L. Alexander, O.D., Ph.D.PRESIDENT
Peter H. Kehoe, O.D.PRESIDENT-ELECT
Randolph E. Brooks, O.D.VICE PRESIDENT
Joe E. Ellis, O.D.SECRETARY-TREASURER
C. Thomas Crooks, III, O.D.IMMEDIATE PAST PRESIDENT
TRUSTEES
Dori M. Carlson, O.D.David A. Cockrell, O.D.
Ronald L. Hopping, O.D., M.P.H.Steven A. Loomis, O.D.
Mitchell T. Munson, O.D.Andrea Thau, O.D.
AOA News Staffwww.aoanews.org
Bob Foster EDITOR- IN-CHIEF
Bob Pieper SENIOR EDITOR
Tracy OvertonASSOCIATE EDITOR
Stephen M. WassermanDIRECTOR, COMMUNICATIONS GROUP
243 N. Lindbergh Blvd.St. Louis MO 63141
(800) 365-2219www.aoa.org
In the 1800s, as wagontrains of enterprising pio-neers moved westward,
they employed scouts to showthem the way.
It was the role of thescout to identify challengesand dangers ahead and findthe best route through difficultterrain. Scouts would oftentravel several days ahead ofthe wagon train returningevery few days to report whatthey found and make recom-mendations to the wagon traincaptain. Sometimes the pio-neers happily received thereport—beautiful country andsafe passage ahead.
Sometimes the reportswere not well received, withdanger and hostile conditionsjust around the corner.Through it all, it was thescout that helped prepare thepioneers for what was ahead.
Leaders in optometricorganizations can sometimesfeel like scouts—scanning thefuture—trying to anticipatewhat lays ahead and reportingback to colleagues. Such isthe case with continued com-petence.
Leaders from six organi-zations—the AOA, theAmerican Optometric StudentAssociation (AOSA), theAmerican Academy ofOptometry (AAO), theAssociation of Schools andColleges of Optometry(ASCO), the Association ofRegulatory Boards ofOptometry (ARBO) and theNational Board of Examinersin Optometry (NBEO)—metat the 2006 Academy meetingto discuss the trend towarddemonstrated, continued com-
petence by practitioners. Thediscussion culminated in thedecision to form a JointBoard Certification ProjectTeam (JBCPT) to develop aprototype board certificationmodel as a means to addressdemonstrable, ongoing con-tinued competence within theprofession. The JBCPT wasannounced at SECO last yearand has met twice since then.
In this issue of the AOANews, the JBCPT delivers thefirst of many reports. Theprocess of developing a boardcertification process to meet
the needs of the professionwill take time—perhaps up totwo years. Once completed,the decision to adopt a boardcertification process will bediscussed thoroughly by theprofession, and a collectivedecision to move forward willcome from the profession.
What makes your leader-ship think that optometristswill be held more accountablein the years ahead? There aremany reasons.
First and foremost is thepublic’s expectation of qualitycare.
Today’s public demandscompetence and will go togreat lengths to find it. Rightnow, you can go online andsee how your hospital, and inmany cases your primary carephysician, ranks among peers.We have moved into an age oflisting “the good docs and thebad docs.”
You may now make yourdecisions on whom to see forcare, or where to have a pro-cedure, based on this kind of
public review.Second is the concern
with medical mistakes. Whilethis may not be quite as criti-cal for optometric practice asit is for hospital-based care,the fix for this problem isgoing to carry over into alltypes of practice—includingoptometry. Optometry, ingeneral, is not prepared forthe kind of scrutiny requiredto reduce medical errors.Peer review, credentialing and
privileging, regular recordreview, adherence to bestpractices—these types ofmonitoring are foreign tomost of us.
Third is the adoption ofelectronic medical records(EMRs). The adoption ofEMRs will facilitate theexchange of information byinsurers, regulatory agenciesand the government. Whilesafeguards to protect privacyare being put into place, thereis no question that EMRs willlead to the monitoring of thequality of care—both the caredelivered by individual practi-tioners and by comparingpractitioners to standard mod-els of care.
Lastly, the trend toward“pay for performance” neces-sitates the ability of a profes-sion to have in place a way todemonstrate ongoing compe-tence to third-party payers.We have already started downthis path with the Medicare“Pay-for-Performance” initia-tive. As stated in the AOANews article, optometry is at adisadvantage over other pro-fessions in that we do not
Scouting continued competence
See President, page 18
Dr. Alexander
January 2008 3
I believe the need to developboard certification
as a means to demonstrate continued competence is
very real. I ask for patience by the profession as we
explore this issue thoughtfully,deliberately, slowly
and with the input of many.
January.qxp 1/10/2008 3:13 PM Page 3
Fri Jan 11 10:30:30 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_3.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim
4 AOA NEWS
“Although buying con-tacts online can be more cost-effective and convenient, westrongly urge patients to
understand that there are risksinvolved to wearing contactlenses,” said Dr. Sclafani.“Because of this, it’s neces-sary that patients visit theireye doctor on a regular basisand communicate any recentvisual changes and discomfort
experienced as a result ofcontact lens wear.”
The study was conductedby Dr. Fogel and Zidile ofBrooklyn College. Using aconvenience sample of 151students from the university,participants completed aquestionnaire on topics relat-ed to Internet use and contactlenses, time pressure,
FDA recommendationsfor purchasing contact lensesonline, demographic items,and other items about beliefsand attitudes toward theInternet. There were no specific exclussion criteria other than not wearing contact lenses.
Purchasing contactlenses online maysave consumers time,
but the process could causemore problems in the longrun, according to a newstudy reported in theJanuary issue of Optometry:Journal of the AmericanOptometric Association.
The research, conduct-ed by Joshua Fogel, Ph.D.,and Chaya Zidile ofBrooklyn College, foundthat individuals who did notpurchase their contact lensesfrom an eye doctor, butfrom an online site or store,are potentially placingthemselves at greater risk.
The findings indicatedthat online and store pur-chasers (consumers who gettheir contacts at a wholesaleclub or optical chain outlet)are less likely to adhere tohealthy eye care practices,as recommended by theireye doctors.
Since the study resultswere announced, the studyhas been mentioned onmore than 150 Web sitesincluding Marketwire,ScienceDaily.com andSmartMoney.com and morethan a dozen broadcast out-lets.
To date, more than 54million people are likely tohave seen the study refer-enced in the days since itwas released.
According to theContact Lens Institute(CLI), more than 30 millionindividuals wear contactlenses. Under the Fairnessto Contact Lens ConsumersAct, mandating that the pre-scribing eye doctor providea copy of the contact lensprescription at no charge tothe patient, consumers havethe option to purchase theirlenses (with a valid pre-scription) elsewhere.
Consumers are increas-ingly purchasing their con-tact lenses online.
“We found that a pat-tern exists regarding themethod of contact lens pur-chasing and following rec-ommendations from theFood and DrugAdministration (FDA),” said
Dr. Fogel. “Those whobought contact lenses at theirdoctor’s office followed anumber of FDA recommenda-
tions more so than those whobought contact lenses else-where.”
The study, whichresearched the purchasing andeye care behaviors of contactlens wearers, found that 86percent of individuals whopurchased their lenses froman eye doctor received a year-ly comprehensive eye exam.But, only 76.5 percent ofthose individuals who pur-chased their lenses via theInternet saw an eye doctor ona routine basis.
“Frequent optometricexaminations are a vital partof a contact lens wearer’s pre-ventive health care routine,”said Louise Sclafani, O.D.,chair of the AOA’s ContactLens and Cornea Section.
“Having one’s eye healthand vision examined on a reg-ular, timely basis is importantto maintaining overall healthand can even lead to earlydetection of various diseases.”
According to the study,35 percent of online pur-chasers did not check that theprescription was correct.
One of the largest dis-crepancies found between in-office and out-of-office con-tact lens purchases was seenin the number of individualswho saw an eye doctor for afollow-up appointment toensure the proper fit of theirlenses.
Fifty-seven percent ofindividuals who purchasedtheir lenses from an eye doc-tor went in for a follow-upappointment; as compared toonly 29 percent of online pur-chasers.
The research also indicat-ed that the majority of con-sumers feel more confidentpurchasing their contact lens-es from a familiar and reliableplace such as their eye doctor
or store rather than throughthe Internet.
In fact, 89 percent and 91percent of respondents
respectively said they feltconfident purchasing contactlenses from their familiar,reliable eye doctor or store.
That number decreasedto 77 percent when surveyingindividuals who made a pur-chase via the Internet.
Study shows online CL buyers less compliant
Two marketers of non-corrective, cos-metic contact lenses have agreed to settleFederal Trade Commission (FTC) chargesthat they violated federal law by selling lens-es without prescriptions.
According to FTC complaints, BeWild,Inc. along with its president, Brian Cohen,and Pretty Eyes, LLC along with its owner,Christianne McNulty, have violated theFTC’s Contact Lens Rule and the FTC act byselling non-corrective contact lenses on theirWeb sites, www.bewild.com andwww.prettyeyes.org, without obtaining con-sumers’ prescriptions or verifying the pre-scriptions with the prescribers, and failing tokeep proper records of prescriptions andverifications.
As AOA News went to press, no con-tact lenses were offered for sale at BeWild’ssite, and prettyeyes.org had been vacated.
BeWild and Cohen also are chargedwith violating the Contact Lens Rule by rep-resenting that their contact lenses can beobtained without a prescription.
Under the proposed settlements, thedefendants are prohibited from selling con-tact lenses without obtaining prescriptions orverifying the prescriptions directly from theprescribers, from failing to maintain recordsof prescriptions and verifications, and fromviolating the Contact Lens Rule.
BeWild and Cohen also are prohibitedfrom misrepresenting that contact lenses maybe obtained without a prescription and willpay a civil penalty of $11,000.
The FTC is waiving all but $2,500 of a$25,000 civil penalty ordered for PrettyEyes and McNulty, based on their financialcondition.
The FTC charged the two retailers
under terms of the 2003 Fairness toContact Lens Consumers Act (FCLCA),which imposed new prescription releaseand verification requirements on prescribersand sellers of contact lenses.
The settlements mark the latest in aseries of actions by the FTC in recentmonths to curb illegal contact lens sales byretailers. On Oct. 12, FTC staff sent warn-ing letters to 15 sellers of non-corrective,cosmetic contact lenses who appeared tobe providing contact lenses to consumerswithout valid prescriptions.
The FTC notes that the consent decreesare for settlement purposes only and do notconstitute an admission by the defendants ofa law violation. A consent decree is sub-ject to court approval but has the force oflaw when signed by the judge.
The AOA Advocacy Group urgesoptometrists to report violation of the federalContact Lens Rule to the FTC. Complaintscan be filed through the FTC Web site(www.ftc.gov/ftc/complaint.shtm) or bycalling 877-382-4357. The AOA alsorequests optometrists forward copies of anycomplaints to the AOA Washington office(at FTCcomplaint @aoa.org).
“The FTC Contact Lens Rule: A commonsense approach to compliance,” a detailedlook at the rule compiled by the AOAOffice of Counsel in light of recent enforce-ment actions by the FTC, appears in theFebruary edition of Optometry: Journal ofthe American Optometric Association.
AOA members can find additionalinformation on federal contact lens laws aswell as links to AOA Washington office andthe FTC on the AOA Web site FCLCApage (www.aoa.org/x4843.xml).
FTC halts unlawful contact lens sales by 2 retailers
“Those who bought contact lenses at their doctor’s office followed a number of FDArecommendations more so than those who
bought contact lenses elsewhere.”
January.qxp 1/10/2008 3:13 PM Page 4
Fri Jan 11 10:32:00 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_4.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim
January 2008 5
Evaluation andManagement:Nursing facilityservices andinitial nursingfacility care
New or Established PatientRevised CPT Codes99304: Initial nursing facilitycare, per day, for the evalua-tion and management of apatient, which requires thesethree key components; added“Physicians typically spend25 minutes with the patientand/or family or caregiver.”99305: Initial nursing facilitycare, per day, for the evalua-tion and management of apatient, which requires thesethree key components; added“Physicians typically spend35 minutes with the patientand/or family or caregiver.”99306: Initial nursing facilitycare, per day, for the evalua-tion and management of apatient, which requires thesethree key components; added“Physicians typically spend45 minutes with the patientand/or family or caregiver.”
Administrators for the billing code systems used by public and privatehealth plans often implement changes around the beginning of each year,and 2008 is no exception.
A number of coding changes this year are applicable to optometry. The American Medical Association’s (AMA) 2008 Physician’s CurrentProcedural Terminology (CPT) code set provides new CPT Category 1Evaluation and Management (E&M) and procedure codes for “non-face-to-face” physician services such as telephone consultations and online medicalevaluations.
Also included in the 2008 CPT Category I codes are new E&M codesfor nursing facility services, new and revised eye and ocular adnexa surgi-cal codes, and a new code for ocular photoscreening.
The 2008 CPT code set also includes several new CPT Category IIcodes for eye care. CPT Category II provides supplementary tracking codesthat can be used for performance measures in programs such as Medicare’sPhysician Quality Reporting Initiative.
The 2008 code also provides two CPT Category III codes that may beapplicable to optometry. CPT Category III provides temporary codes for
Subsequentnursing facilitycare99307: Subsequent nursingfacility care, per day, for theevaluation and management ofa patient, which requires atleast two of these three keycomponents; added“Physicians typically spend 10minutes with the patient and /or family or caregiver.”99308: Subsequent nursingfacility care, per day, for theevaluation and management ofa patient, which requires atleast two of these three keycomponents; added“Physicians typically spend 15minutes with the patient and /or family or caregiver.”99309: Subsequent nursingfacility care, per day, for theevaluation and management ofa patient, which requires atleast two of these three keycomponents; added“Physicians typically spend 25minutes with the patient and /or family or caregiver.”99310: Subsequent nursingfacility care, per day, for theevaluation and management ofa patient, which requires atleast two of these three keycomponents; added“Physicians typically spend 35minutes with the patient and /or family or caregiver.”
emerging technology, services and procedures. The codes are used todescribe products or services that are the subject of clinical trials.
The latest regularly scheduled updating of the International Classificationof Diseases, Ninth Revision (ICD-9) and the U.S. Department of Health andHuman Services’ Health Care Procedures Coding System, (HCPCS) codeshave also resulted in several changes in the coding used to report eye orvision care services.
The AOA Coding Subcommittee has outlined major coding changesrelevant to optometric practice in this issue of AOA News.
The 2008 edition of the AOA’s Codes for Optometry, the only compre-hensive coding guide developed specifically for optometric practices, pro-vides a complete listing of all codes relevant to eye and vision care.
Codes for Optometry can be purchased through the AOA OrderDepartment by calling 800-262-2210, faxing orders to 314-991-4101(Attn: Order Department), logging on to the AOA Web site OrderDepartment page (www.aoa.org/x4795.xml) or [email protected].
Other nursingfacility services99318: Evaluation and man-agement of a patient involv-ing an annual nursing facilityassessment, which requiresthese three key components;“Physicians typically spend30 minutes with the patientand / or family or caregiver.”
Non-face-to-face physicianservicesTelephone ServicesTelephone services are non-face-to-face evaluation andmanagement (E/M) servicesprovided by a physician to apatient using the telephone.
These codes are used toreport episodes of care by thephysician initiated by anestablished patient orguardian of an establishedpatient. If the telephone serv-ice ends with a decision tosee the patient within 24hours or next available urgentvisit appointment, the code isnot reported; rather theencounter is considered partof the preservice work of thesubsequent E/M service, pro-cedure, and visit. Likewise, ifthe telephone call refers to anE/M service performed andreported by the physician
within the previous sevendays (either physician request-ed or unsolicited patient fol-low-up) or within the postop-erative period of the previous-ly completed procedure, thenthe service(s) are consideredpart of that previous E/M serv-ice or procedure. (Do notreport 99441-99443 if report-ing 99441-99444 performed inthe previous seven days.)
New CPT Codes99441: Telephone evaluationand management service pro-vided by a physician to anestablished patient, parent, orguardian not originating froma related E/M service provid-ed within the previous sevendays nor leading to an E/Mservice or procedure withinthe next 24 hours or soonestavailable appointment; 5-10minutes of medical discus-sion.99442: 11-20 minutes ofmedical discussion99443: 21-30 minutes ofmedical discussion
Online medical evaluation
An online electronicmedical evaluation is a non-face-to-face evaluation and
EYE ON WASHINGTON
New year again brings coding changes
management E/M service bya physician to a patient usingInternet resources in aresponse to a patient’s onlineinquiry. Reportable servicesinvolve the physician’s per-sonal timely response to thepatient’s inquiry and mustinvolve permanent storage(electronic or hard copy) ofthe encounter.
The service is reportedonly once for the sameepisode of care during a sevenday period, although multiplephysicians could report theirexchange with the samepatient. If the online medicalevaluation refers to an E/Mservice previously performedand reported by the physicianwithin the previous sevendays (either physicianrequested or unsolicitedpatient follow-up) or withinthe postoperative period ofthe previously completed pro-cedure, then the service(s) areconsidered covered by theprevious E/M service or pro-cedure. A reportable serviceencompasses the sum of com-munication (e.g., related tele-phone calls, prescription pro-visions, laboratory orders)pertaining to the onlinepatient encounter.
AOA outlines changed CPT Codes for 2008
See Codes, page 6
January.qxp 1/11/2008 9:51 AM Page 5
Fri Jan 11 11:49:31 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_5.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

6 AOA NEWS
99444: Online evaluationand management service pro-vided by a physician to anestablished patient, guardian,or health care provider notoriginating from a relatedE/M service provided withinthe previous seven days,using the Internet or similarelectronic communicationsnetwork.
Surgery/eye and ocularadnexaNew surgical codes67041: With removal of pre-retinal cellular membrane (eg,macular pucker).67042: With removal ofinternal limiting membrane orretina (e.g., for repair of macular hole, diabetic macu-lar edema), includes, if per-formed, intraoculartamponade (ie, air, gas, or sil-icone oil) and laser photoco-agulation.67043: With removal of sub-retinal membrane (eg, choro-dial neovascularization),includes, if performed,intraocular tamponade (ie, air,gas or silicone oil) and laserphotocoagulation.67113: Repair of complexretinal detachment (eg, prolif-erative vitreoretinopathy,stage C-1 or greater, diabetictraction retinal detachment,retinopathy of prematurity,retinal tear of greater than 90degrees), with vitrectomy andmembrane peeling, mayinclude air, gas or silicone oiltamponade, cryotherapy,endolaser photocoagulation,drainage of subretinal fluid,scleral buckling, and / orremoval of lens.67229: Preterm infant (lessthan 37 weeks gestation atbirth), performed from birthup to 1 year of age (eg,retinopathy of prematurity),photocoagulation or cryother-apy.68816: With transluminalballoon catheter dilation
Revised surgical CPT codes:67227: Destruction of exten-sive or progressive retinopa-thy (eg, diabetic retinopathy),one or more sessions,cryotherapy, diathermy.67228: Treatment of exten-sive or progressive retinopa-thy, one or more sessions,cryotherapy, diathermy.
MedicineSection: Non-face-to-facenonphysicianservices
Revised Descriptor92135: Scanning computer-ized ophthalmic diagnosticimaging, posterior segment,(eg, scanning laser) withinterpretation and report, uni-lateral.
Non-face-to-facenonphysicianservicesTelephone ServiceTelephone services are non-face-to-face assessment andmanagement services provid-ed by a qualified health careprofessional to a patient usingthe telephone.
These codes are used toreport episodes of care by thequalified health care profes-sional initiated by an estab-lished patient or guardian ofan established patient. If thetelephone service ends with adecision to see the patientwithin 24 hours or the nextavailable urgent visit appoint-ment, the code is not report-ed; rather the encounter isconsidered part of the preser-vice work of the subsequentassessment and managementservice, procedure and visit.
Likewise, if the tele-phone call refers to a serviceperformed and reported bythe qualified health care pro-fessional within the previousseven days (either qualifiedhealth care professionalrequested or unsolicitedpatient follow-up) or withinthe postoperative period ofthe previously completed pro-cedure, then the service(s) are
considered part of that previ-ous service or procedure. (Donot report 98966-98969 ifreporting 98966-98969 per-formed in the previous sevendays.)
New:98966: Telephone assess-ment and management serv-ice provided by qualified non-physician health care profes-sional to an establishedpatient, parent, or guardiannot originating from a relatedassessment and managementservice provided within theprevious seven days not lead-ing to an assessment andmanagement service or proce-dure within the next 24 hoursor soonest available appoint-ment; 5-10 minutes of med-ical discussion.98967: 11-20 minutes ofmedical discussion98968: 21-30 minutes ofmedical discussion
Online medicalevaluation:98969: Online assessmentand management service pro-vided by a qualified non-physician health care profes-
sional to an establishedpatient, guardian, or healthcare provider not originatingfrom a related assessment andmanagement service providedwithin the previous sevendays, using the Internet orsimilar electronic communi-cations network.
Other servicesand procedures:New:99174: Ocular photoscreen-ing with interpretation andreport, bilateral.
Category II Codes(The following Category IIcodes were released inOctober 2006 online but didnot appear in the AMA’s-CPTbook until January 2008.)
Newly listed CPT codes 1055F: Visual function sta-tus assessed2019F: Dilated macularexam performed, includingdocumentation of the pres-ence or absence of macularthickening or hemorrhageAND the level of maculardegeneration severity.2020F: Dilated fundus evalu-
ation performed within sixmonths prior to cataract sur-gery.2021F: Dilated macular orfundus exam performed,including documentation ofthe presence or absence ofmacular edema AND level ofseverity of retinopathy.2027F: Optic nerve headevaluation performed.3073F: Pre-surgical(cataract) axial length, cornealpower measurement andmethod of intraocular lenspower calculation document-ed within six months prior tosurgery.5010F: Findings of dilatedmacular or fundus exam com-municated to the physicianmanaging the diabetes care.Category III CPT Codes(The following Category IIIcodes were released July 1,2007, and implemented Jan.1, 2008.)0186T: Suprachoroidal deliv-ery of pharmacologic agent(does not include supply ofmedication).0187T: Scanning computer-ized ophthalmic diagnosticimaging, anterior segment,with interpretation and report,unilateral.
Codesfrom page 5
ICD-9 update brings new codesThis year’s regularly scheduled updating of the International Classification of Diseases,
Ninth Revision (ICD-9) codes has resulted in a several changes in coding used to reporteye or vision care services. The coding changes took effect Oct. 1. They include:v A new code modifier V49.85 (Dual sensory impairment, Blindness with deafness) tobe used to indicate combined visual-hearing impairment with the hearing impairment(389.00-389.9) and visual impairment (369.00-369.9) codes, andv A number of changes in the 364.8 and 364.9 codes requiring greater specificityin the reporting of conditions of the iris. A diagnosis code for intraoperative floppy iris syn-drome (IFIS), 364.81, has been added.
In addition, there are some new V codes—such as V68.01 - Disability examinationand V68.09 - Other issue of medical certificates—which optometrists may need to knowabout in light of their disability determination authority under Social Security.
The ICD-9-CM codes are updated annually as stated in the Medicare ClaimsProcessing Manual, Chapter 23 (Fee Schedule Administration and Coding Requirements),Section 10.2 (Relationship of ICD-9-CM Codes and Date of Service).
The CMS reminds health care providers that ICD-9-CM codes are required for all pro-fessional claims (including those from physicians, non-physician practitioners, independentclinical diagnostic laboratories, occupational and physical therapists, independent diagnos-tic testing facilities, audiologists, ambulatory surgical centers), and for all institutional claims.
MM5643 can be viewed on the CMS Web site atwww.cms.hhs.gov/MLNMattersArticles/downloads/MM5643.pdf or CMS ChangeRequest CR 5643 at http://www.cms.hhs.gov/Transmittals/downloads/R1269CP.pdf.
All new, revised, and discontinued ICD-9-CM diagnosis codes on the CMS Web sitecan be viewed at www.cms.hhs.gov/ICD9ProviderDiagnosticCodes/ 07_summaryta-bles.asp#TopOfPage or at the National Center for Health Statistics (NCHS) Web site atwww.cdc.gov/nchs/icd9.htm.
January.qxp 1/10/2008 3:14 PM Page 6
Fri Jan 11 10:32:00 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_6.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

January 2008 7
Christopher Gardner,the author of “ThePursuit of
Happyness,” will be thekeynote speaker at theOpening General Session forthe 2008 Optometry’sMeeting™. Sponsored byEssilor, the Opening GeneralSession will be Thursday, June26 from 8 a.m. to 9:30 a.m.
In “The Pursuit ofHappyness,” Gardner chroni-cled his long, painful, yet ulti-mately rewarding, journeyfrom inner-city Milwaukee tothe pinnacle of Wall Street.
Gardner is also the inspi-ration for the acclaimed movie“The Pursuit of Happyness,”for which Will Smith, starringas Gardner, received GoldenGlobe, Screen Actors Guild,and Academy Award nomina-tions.
Gardner’s autobiographywas a New York Times andWashington Post No. 1 best-seller.
In the book, Gardnersolidly depicted growing upblack and male in late 20th-century urban America.
Surmounting acute obsta-cles throughout his life,Gardner is an avid motiva-tional speaker, addressing thekeys to self-empowerment,beating odds and breakingnegative cycles.
Gardner is the owner andCEO of Christopher GardnerInternational Holdings withoffices in New York, Chicago,and San Francisco.
Gardner is also a pas-sionate philanthropist com-mitted to many charitableorganizations.
Always hard-workingand tenacious, a series of cir-cumstances in the early 1980sleft Gardner homeless in SanFrancisco and the soleguardian of his toddler son.
Unwilling to give upChris Jr. or his dream offinancial independence,Gardner started at the bottom. Without connections or a col-lege degree, he earned a spotin the Dean Witter Reynoldstraining program.
Often spending his nightsin a church shelter or thebathroom at a Bay Area
The 2008 Optometry’s Meeting™ will be hosted atthe Washington State Convention and Trade Center inSeattle June 25-29.
The Emerald City is home to more than just its reputa-tion for rain—it’s filled with the myriad delights of thePacific Northwest.
One of Seattle’s top sights is the Space Needlewhere visitors can observe Seattle’s multifaceted geogra-phy from 520 feet. The needle was originally built for the1962 World’s Fair.
Another way to enjoy Seattle’s unique geography is byferry ride. Observers can glimpse spectacular views of thecity, Cascade and Olympic Mountains and the shoreline.
The Pike Place Market is another well-known attrac-tion. Filled with fish, flowers and fun, the market has over200 businesses to stroll through and enjoy.
Whale watching is another popular activity. Visitorscan observe the orcas who call the Puget Sound theirhome.
Optometry’s Meeting™ attendees can also take BillSpeidel’s Underground Tour and explore the ruins of thecity of Seattle before it was engulfed in flames in 1889.
The city is also home to the Seattle Public Library. Book lovers and architecture buffs alike will be drawn tothis award-winning building made of steel and glass.Visitors can return to the past at Tillicum Village. They cantake a tour of a Native American island village and learnabout the ways of the Northwest’s original residents.Seattle is filled with outdoor adventures.
The area offers a wealth of outdoor activities fornature enthusiasts including hiking, whitewater rafting,cycling, scuba diving, golfing, camping, mountain bikingand sea kayaking.
Of course, a visit to Seattle would not be completewithout drinking some coffee.
Optometry’s Meeting™ attendees can grab a cup ofjava at one of the capital of coffee’s 628 coffee shopsbefore focusing on the more than 200 hours of worldclass education, exhibit hall displays, House of Delegatebusiness, social events, and networking opportunities.
Registration opens in February. Visit www.optometrys-meeting.org for more information.
Rapid Transit station inOakland, Gardner was thesole trainee offered a job atDean Witter Reynolds in1981.
He spent 1983 to 1987 atBear Stearns & Co., where hebecame a top earner.
In 1987, he founded thebrokerage firm Gardner Rich& Co. in Chicago.
Gardner’s remarkablestory of struggle, faith, entre-preneurialism, and fatherlydevotion has catapulted himbeyond the notoriety he hasfound on Wall Street.
Gardner has been fea-tured on the “Evening Newswith Dan Rather,” “20/20,”the “Oprah Winfrey Show,”the “Today Show,” “TheView,” “EntertainmentTonight,” CNN, CNBC, andFox as well as being the sub-ject of profiles in numerousmedia including People, USAToday, Associated Press, TheNew York Times, Fortune, Jet,Reader’s Digest, TraderMonthly, Chicago Tribune,San Francisco Chronicle, TheNew York Post and theMilwaukee Journal Sentinel.Gardner lives in Chicago andNew York.
Optometry’s Meeting™registration opens inFebruary. For more informa-tion, visit www.optometrys-meeting.org.
‘The Pursuit of Happyness’ author to speak at Optometry’s Meeting™
The beautiful Seattle skyline and Puget Sound seen from BainbridgeIsland at night. Photo: Tim Thompson
Attractions for all beckon in Seattle
Christopher Gardner
January.qxp 1/10/2008 3:14 PM Page 7
Fri Jan 11 10:31:23 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_7.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

8 AOA NEWS
Fees,from page 1
The U.S. Centers forMedicare & MedicaidServices (CMS) updatesMedicare physician reim-bursement with the start ofeach calendar year.
On Nov. 1, the CMSannounced plans to cut reim-bursement levels for 2008,marking the seventh time inas many years the agency hasproposed cuts in theMedicare physician feeschedule.
At the urging of theAOA and other groups moni-toring the issue inWashington, D.C., Congresshas intervened to safeguard
health care practitioners andpatients from these devastat-ing reductions.
This year’s plannedMedicare physician reim-bursement cut was postponedunder terms of the Medicare,Medicaid, and SCHIPExtension Act of 2007 (S.2499), which was passed bythe Senate Dec. 18, and bythe House of Representativesa day later.
The legislation wasintroduced in the House byRep. Charles Rangel (D-N.Y.) and Rep. Jim McCrery(R-La.) and in the Senate bySen. Max Baucus (D-Mont.)and Sen. Charles Grassley(R-Iowa).
In addition to protectingMedicare physician reim-bursement over the first halfof this year, the measureextends funding for the StateChildren’s Health InsuranceProgram (SCHIP), Medicarequality reporting programssuch as the Physician QualityReporting Initiative (PQRI),Medicare Advantage andother Medicare and Medicaidprograms.
AOA Advocacy GroupDirector Jon Hymes credited
the successful inclusion of atemporary Medicare fee-fixin the bill to efforts by Sen.Baucus and Sen. Grassley aswell as Rep. Rangel andother key leaders inCongress. Sen. Grassley andSen. Rangel are recipients ofthe AOA’s Health CareLeadership Award.
The congressional actioncame after several weeks ofeffective grassroots lobbyingby AOA Keypersons andactive AOA members, Hymessaid.
Hymes also pointed tovery effective Capitol Hilltestimony on the impact of
Medicare physician paymentscuts on optometry that wasprovided on Nov. 8 by JohnWhitlow, O.D., president ofthe Georgia OptometricAssociation, before a U.S.House subcommittee hearing.
Dr. Whitlow was theonly non-MD selected to tes-tify before the panel.
Lawmakers also appearto have been prompted toaction by numerous personalcalls, letters and e-mails tolegislators from health careproviders, Hymes said. Manyof those e-mails were sentthrough services such as theAOA’s online Legislative
Both the Centers for Medicare andMedicaid Services (CMS) and providergroups blame the string of proposedMedicare fee cuts over recent years on aneconomic indicator known as theSustainable Growth Rate (SGR). The SGR isamong the factors considered in a complexformula that under federal law is used to setMedicare physician reimbursements. Theindicator ties Medicare fee levels to theoverall performance of the U.S. economy.
Left unchanged, the formula will continueto result in fee reductions each year, accord-ing to speakers at last year’s AOACongressional Conference. The formula willreduce physician reimbursements by aroundone-third over the next few years alone, AOAFederal Relations Committee Chair MicheleHaranin, O.D., told the conference.
The AOA and other provider groupshave made a top priority of changing thefee-setting formula to permanently stabilizeMedicare physician reimbursement. TheMedicare Payment Advisory Commission,the body established by Congress to makerecommendations on Medicare paymentissues, has recommended replacing the
SGR with another cost indicator.However, many in Congress reportedly
want to tie any fee stabilization measures toquality enhancement efforts such as pay-for-performance programs. This year’s short-termfee fix in the just-passed legislation was cou-pled to an extension of the physician qualityreporting system, AOA Advocacy GroupDirector Jon Hymes noted.
With physicians facing the prospect ofa fee cut in just six months, provider groupswill have to “re-double” their efforts this yearto both ensure the short-term stability ofMedicare reimbursement and, they hope,achieve a “permanent fix” for the Medicarefee formula, Hymes said.
“The AOA and other health providergroups pushed hard in 2007 for Congressand the president to fix the flawed Medicarereimbursement formula,” Hymes said.“However, there’s no consensus as yet onany one solution that will work for the long-term. It now becomes critically important forlawmakers, the White House, and providerorganizations to continue to work toward afair and reasonable reimbursement formulathat protects doctors and patients.”
Flawed formula continues to erode physician pay
Action Center, he said. Lawmakers will official-
ly reconvene for the secondsession of the 110th Congresson Jan. 22.
The AOA AdvocacyGroup’s 2008 CongressionalConference, organizedoptometry’s major annualCapitol Hill lobby effort, isscheduled April 6-10, just aslawmakers are likely to beconsidering Medicare physi-cian reimbursement legisla-tion.
Because of the latechange in the Medicare feeschedule, the CMS hasannounced that it will allow
Call for posters openThe AOA is inviting participation in the Clinical and Scientific Poster Session at the
111th Annual AOA Congress & 38th Annual AOSA Conference: Optometry’sMeeting™.
The program creates a national forum for clinicians, students, and faculty to com-municate interesting cases and unique research to their colleagues.
The poster preview session will be held Friday, June 27, 2008, and the interactivesession offering continuing education credit will be Saturday, June 28, 2008, from 11a.m. to 2 p.m. at the Washington State Convention and Trade Center.
Poster abstracts must be submitted electronically and must be received by Feb. 6,2008. For details and an electronic submission form, log on to www.optometrysmeet-ing.org and click on the Call for Posters icon. For more information, contact Stacy Smithat (314) 983-4254 or at [email protected].
New HCPCS IOL codesUpdates to the U.S. Department of Health and
Human Services’ Health Care Procedures Coding System(HCPCS) for 2008 include two changes pertinent to thepractice of eye or vision care. Administrators haveadded two new material codes:V2787 – Astigmatism Correcting Function of Intraocular
Lens.V2788 – Presbyopia Correcting Function of Intraocular
Lens.The HHS maintains the HCPCS to describe services
and supplies not covered under the CPT codes.
At the urging of the AOAand other groups, Congress has intervened to safeguard
health care practitioners and patients from these devastating reductions.
physicians an additional 45days to decide whether toparticipate in the Medicareprogram for 2008.
Health care practitionersnow have until Feb. 15 todetermine whether to partici-pate or not.
January.qxp 1/10/2008 3:14 PM Page 8
Fri Jan 11 10:33:02 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_8.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

January 2008 9
Ohio Gov. TedStrickland (D)signed H.B. 149,
expanding the oral prescrip-tive authority ofoptometrists in the state andadding the use of injectablesto treat anaphylaxis and useof blood sugar testingdevices, on Dec. 21.
The bill also exemptsstudents from optometryschools in other states par-ticipating in a training pro-gram in Ohio from licensureand requires the OhioOptical Dispensers Board toregulate the dispensing ofplano contact lenses.
“The passage of ourscope bill was a thoroughand deliberate process,” saidCheryl Archer, O.D., imme-diate past president of theOhio OptometricAssociation (OOA).“Numerous leaders in theassociation worked to makethis happen.”
The bill, sponsored byState Reps. David Daniels(R) and Fred Strahorn (D),amended the definition ofthe practice of optometry torepeal the limitation to treat-ment of the “anterior seg-ment.”
In addition, the defini-tion was amended to includethe use of a commerciallyavailable glucose-monitoringdevice.
The previous formularyof specific diagnostic drugsavailable for use or applica-tion was repealed.
The previous formularyof specific oral drugs for useor prescription was repealed,and all appropriate oraldrugs in the following class-es are now authorized:v anti-infectives, includingantibiotics, antivirals,antimicrobials, and antifun-gals;v anti-allergy agents; v anti-glaucoma agents;v analgesics, includinganalgesic drugs that areavailable without a prescrip-tion, analgesic drugs or dan-gerous drugs that require aprescription but are not con-
trolled substances, andSchedule III controlled sub-stances that are approved bythe state board of optometryin rules;v anti-inflammatories(excluding all oral steroidsexcept methylpredisolone);and
v any other oral drugapproved by the board ofoptometry (in consultationwith the board of pharmacy)that is approved or exemptfrom approval or certified orexempt from certification bythe Federal Food and DrugAdministration for oph-thalmic purposes.
Oral methylpredisolonemay be prescribed if all ofthe following conditions aremet:v the drug is prescribedfor use in allergy cases;v the drug is prescribedfor use by an individual who
is 18 years of age or older;v the drug is prescribedon the basis of an individ-ual’s particular episode ofillness; and v the drug is prescribed inan amount that does notexceed the amount packagedfor a single course of therapy.
The bill gave specificauthority for optometrists todispense vision correctiondevices, including, but notlimited to, contact lensesthat have vision correctionas their primary purpose butalso combine with that pur-pose the delivery of a drugthrough the device, if thedrug delivered by the devicewould otherwise be a topicalocular pharmaceutical agentor oral therapeutic pharma-ceutical agent.
The bill sets continuingeducation hours required forlicense renewal to 25 hours
(the law previously allowedthe board of optometry toset the required hoursbetween six and 25 hours).The 25-hour requirementincludes at least 10 hours inpharmacology (up from theprevious five hours).
“Ohio is proud of ournew scope of practice billand considers it a significantwin for our patients,” saidKaren Riccio, O.D., OOApresident. “The new aspectsof Ohio scope of practicewill prove to be cost-effec-tive and assure the highestquality of primary eye care.”
The bill also requirescontact lens prescriptions toinclude all information speci-fied by the federal Fairness toContact Lens Consumers Act.
The ophthalmic dis-penser law requiring a pre-scription for the dispensingof contact lenses wasamended to include in thedefinition of a contact lens:“zero-powered plano contactlenses, cosmetic contactlenses, performance-enhanc-ing contact lenses, and anyother contact devices deter-mined by the optical dis-pensers board to be contactlenses.”
GLANCE AT THE STATES
Ohio expands orals authority for ODs
The SouthernCalifornia College ofOptometry (SCCO)
selected AOA PresidentKevin Alexander, O.D.,Ph.D., as its president,effective July 1.
Dr. Alexander willreplace Lesley Walls, O.D.,M.D., who is retiring after11 years in the position.
Dr. Alexander is cur-rently the dean of theMichigan College ofOptometry at Ferris StateUniversity.
“Experience and leader-ship in the areas of academe
and the optometric profes-sion are key assets that fac-tored into the selection ofDr. Kevin Alexander as thenext president of theSouthern California Collegeof Optometry,” said CharlesMunson, chair of the SCCOBoard of Trustees. “Hisexperience as a dean at anoptometric college and hisyears of leadership withinorganized optometry makehim an excellent choice towork with our students, fac-ulty and alumni in advancingthe mission of SCCO. Heand his wife, Carol, also an
optometrist, will be wonder-ful additions to our greatteam.”
Dr. Alexander graduatedfrom The Ohio StateUniversity College ofOptometry, where he laterheld a faculty position.
He has practiced in pri-vate and group settings, pub-lished scientific papers andlectured for continuing edu-cation.
Dr. Alexander hasserved on numerous AOAcommittees and chaired theOptometry 2020 Summits.
His many awards
include The Ohio StateUniversity College ofOptometry H. Ward EwaltMedal for DistinguishedService (2007), theMichigan OptometricAssociation Keyperson ofthe Year (2002),Distinguished Practitioner ofthe National Academies ofPractice (2000), theOutstanding Service Awardfrom the Ohio OptometricAssociation (OOA) (1992and 1998) and the OOAWarren Morris Optometristof the Year (1989).
“I am thrilled to have
“Ohio is proud of our new scope of practicebill and considers it a significant win for ourpatients. The new aspects of Ohio scope of
practice will prove to be cost-effective and assurethe highest quality of primary eye care.”
SCCO selects Alexander as presidentbeen named the president ofthe Southern CaliforniaCollege of Optometry andeager to join the collegefamily as we take our insti-tution to the next level ofexcellence,” said Dr.Alexander.
“I look forward toworking with the students,faculty and alumni in build-ing upon the college’s stronghistory of providing anexcellent educational pro-gram, exceptional patientcare and outstanding leader-ship for the optometric pro-fession,” he added.
January.qxp 1/10/2008 3:15 PM Page 9
Fri Jan 11 10:32:12 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_9.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

10 AOA NEWS
tions due to recent technicalcorrections. The notes are alsoavailable on the CMS Website PQRI page(www.cms.hhs.gov/pqri).
For practitioners seekingeven more detailed guidance,the American MedicalAssociation’s (AMA) PQRIParticipation Tools aredesigned to help physiciansand other eligible profession-als identify measures relevantto their practice and facilitate
the data collection required toreport clinical performancedata.
Information is availablefor each of the 119 PQRIquality measures. The toolsare now available online atwww.ama-assn.org/go/toolsMedicarePQRI.
All of the listed resourcescan be accessed through theAOA Web site PQRI page athttp://www.cms.hhs.gov/pqri.xml.
or revised resources designedto assist practitioners withsuccessful participation in the2008 PQRI.
PQRI Measures 2008, aguide to PQRI participationdeveloped specifically foroptometrists by the AOACoding Subcommittee, out-lines all 11 PQRI eye care,administrative and screeningor counseling measures appli-cable to optometric practicethis year, along with detailedreporting instructions. Theguide appears in this issue ofAOA News.
AOA PQRI Web page
The AOA Web site’sPQRI page has been updatedto reflect changes in the 2008PQRI program pertinent tooptometry. The Web pageincludes:v An introduction to thePQRIv Changes in the measuresthat optometrists can reportunder the 2008 PQRI pro-gramv The latest PQRI newsand alerts from the CMS v A complete “How to
AOA resources offer detailed guidance on PQRICode for Eye Care Measures”section including:v PQRI coding definitions v Tools and resources v A PQRI summary chart v Filing specifications andexamples v The AOA’s and CMS’sPQRI PowerPointPresentationsv An explanation of PQRIbonus incentive paymentv The CMS Coding forQuality Handbook
The CMS’s new 2008PQRI Coding for QualityHandbook, released in lateDecember, outlines codingand reporting principles anddescribes successful reportingfor each measure. The hand-book is available through theCMS Web site PQRI page(www.cms.hhs.gov/pqri).
CMS PQRImeasure specificationsnotes
The CMS 2008 MeasureSpecifications Release Notes,also made available inDecember, describe recentchanges to measure specifica-
Health care providerstaking part inMedicare’s 2008
Physician Quality ReportingInitiative (PQRI) can earn abonus of approximately 1.5percent of their total Medicarereimbursement for the year,according to the U.S. Centersfor Medicare & MedicaidServices (CMS).
However, health carepractitioners should also beaware that the CMS has madea number of changes in thePQRI program this year,according to the AOA CodingSubcommittee.
Program rules issued bythe CMS Nov. 27 in theFederal Register expand thePQRI reporting period to afull year (Jan. 1 – Dec. 31) in2008, eliminate several eyecare measures that werereportable under the 2007program, and add several newmeasures to the program.
Additional guidanceissued by CMS in lateDecember clarified codingand reporting specification fora number of measures.
The AOA, CMS andother health provider organi-zations are now offering new
January is GlaucomaAwareness Month
The U.S. Centers for Medicare & Medicaid Services(CMS) is asking optometrists to help make patients awareof Medicare coverage for glaucoma-related services in con-junction with the January observance of NationalGlaucoma Awareness Month.
As part of its Optometry Awareness and Public Affairscampaign, the AOA Communications Group, through thepublic relations firm of Hill & Knowlton, this month issued anational press release to help raise public awarenessregarding the eye disease.
Approximately 3 million Americans have glaucoma,the CMS notes. However, because the disease often pro-gresses in the initial stages with no symptoms, it is estimatedthat up to half do not know they have it.
Medicare CoverageMedicare provides coverage of an annual glaucoma
screening for beneficiaries in at least one of the followinghigh-risk groups:v Individuals with diabetes mellitus; v Individuals with a family history of glaucoma; v Blacks age 50 and older; and v Hispanics age 65 and older. A covered glaucoma screening includes:v A dilated eye examination with an intraocular pressure(IOP) measurement; and v A direct ophthalmoscopy examination or a slit-lampbiomicroscopic examination.
What practitioners can doUnfortunately, many Medicare patients remain unaware
that the government health program covers glaucoma-relat-ed services.
“CMS needs your help to ensure that all eligible peo-ple with Medicare take full advantage of the annual glau-coma screening benefit,” the agency emphasized in astatement to eye care providers this month.
To help health care professionals and their staffs under-stand coverage, coding, billing, and reimbursement for pre-ventive services and screenings covered by Medicare, theCMS offers the Medicare Learning Network (MLN)Preventive Services Educational Products Web Page thatprovides descriptions and ordering information for allprovider specific educational products related to preventiveservices.
The Web page is www.cms.hhs.gov/MLNProducts/35_PreventiveServices.asp.
January.qxp 1/10/2008 3:15 PM Page 10
Fri Jan 11 10:34:20 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_10.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

January 2008 11
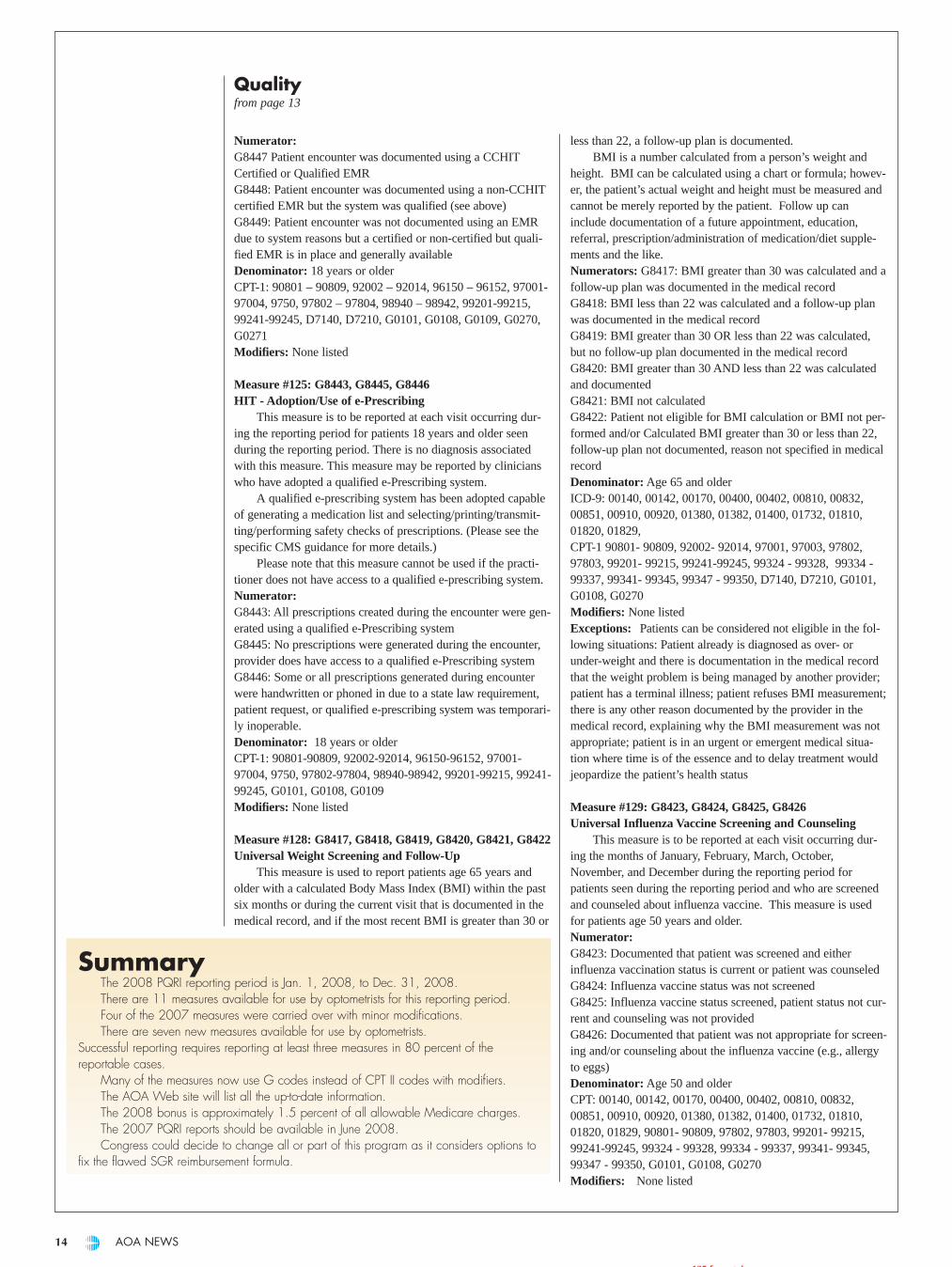
2008 PQRI measures: What ODs need to knownumber of optometrists participating in this program will yieldpositive recognition of optometry within the CMS.
There are 119 measures available for reporting in 2008.
Retired measures
15 measures were retired in 2008, including the followingeye care measures:v Measure #13: 4007F ARMD - AREDSPrescribed/Recommended v Measure #15: 1055F Cataracts - Visual Functional StatusAssessmentv Measure #16: 3073F Cataracts - Pre-surgicalMeasurements v Measure #17: 2020F Cataracts - Pre-surgical DilatedFundus Evaluation
Edited measures
The remaining 2007 measures have had some edits made.Please see the details of the measures later in the article forthose changes. The remaining available measures are:v Measure #12: 2027F Primary Open Angle Glaucoma -Optic Nerve Evaluationv Measure #14: 2019F ARMD - Dilated MacularExaminationv Measure # 18: 2021F Diabetic RetinopathyDocumentation of Presence or Absence of Macular Edema andLevel of Severity of Retinopathyv Measure # 19: 5010F with G8397 OR G8398 DiabeticRetinopathy Communication with Physician Managing OngoingDiabetes Carev In addition, a new measure is available relating to eye care.Measure #117: 2022F, 2024F, 2026F, OR 3072F Dilated EyeExam in Diabetic Patient
Additional measures
Additional measures that may be available for use by eyecare professionals (and others) are:v Measure #114: 1000F AND 1034F/1035F/1036F - InquiryRegarding Tobacco Usev Measure #115: G8456&G8402 OR G8456&G8457 ORG8455&G8403 - Advising Smokers to Quitv Measure #124: G8447, G8448, OR G8449 HIT - Adoption/Use of Health Information Technology (HIT)(Electronic Health Records)v Measure #125: G8443, G 8445. OR G8446 HIT - Adoption/Use of e-Prescribingv Measure #128: G8422, G8421, OR G8419 - UniversalWeight Screening and Follow-Upv Measure #129: G8423, G8426, G8424, OR G8425 -Universal Influenza Vaccine Screening and Counseling*Use of appropriate G-code depends on specification guidance
Thus, 11 measures are potentially available for use by eyecare professionals. The guidelines still state a practitioner mustreport at least three measures on 80 percent of the reportablecases to be eligible for the bonus payment.
By Rebecca H. Wartmann, O.D.AOA Coding Subcommittee
The year of 2008 brings changes to the Physician QualityReporting Initiative (PQRI) measures that optometrists can use.Several of the measures from the 2007 PQRI program havebeen withdrawn and new measures have been added. This arti-cle will review the origins for the PQRI measures, the reportingto expect from the 2007 initiative, and the 2008 measures asthey are currently published. Please refer to the AOA Web sitefor any updates that might occur and all the tools practitionersmay need for the 2008 PQRI reporting period. For the sake ofaccuracy, the terminology in this article, whenever possible,was taken directly from the CMS regulation.
Background
The PQRI was created as a part of the Tax Relief andHealthcare Act of 2006 that provides the statutory authority forthe quality improvement program. PQRI reporting will focusattention on quality of care rather than resources utilized. Thebasis for this initiative is evidence-based measures developed byprofessionals and endorsed by national consensus groups suchas the National Quality Forum (NQF) and the AQA (formerlythe Ambulatory Care Quality Alliance). When the approvedquality measurements are reported frequently enough, theMedicare provider will be rewarded financially. The hope isthat PQRI will result in improved patient care. Eventually, it isexpected that Medicare will move to a true “pay-for-perform-ance” system.
2007 report results
The reports of the 2007 PQRI analysis and bonus paymentswill be available in June 2008. No interim reports were madeavailable. This means that no one will know how they per-formed in 2007 until halfway through the 2008 reporting period.
Several reporting challenges were found during the 2007reporting periods.
These challenges included National Provider Identification(NPI) numbers being stripped off claims, inappropriate denialsfor provider types, and clearinghouses stripping PQRI CPT IIcodes from claims. At this time, no one knows how widespreadthese problems were or the ultimate impact on the success ofreporting measures and earning bonuses.
The reports of the 2007 PQRI results will be sent to theholder of the Tax Identification Number (TIN) but broken downby NPI number. The report results will not be publicly avail-able. Each report will give details of the number of claims eli-gible that were filed compared to the number of eligible claimsthat were properly filed with the appropriate PQRI reportingcodes. Many other statistical details will be listed on eachreport.
2008 PQRI measures
Participation in the 2008 PQRI program remains voluntary,and the bonus amount will still be approximately 1.5 percent ofall allowable Medicare claims, including the –TC componentsof procedures. While a 1.5 percent bonus incentive may not besignificant in terms of monetary reward, the result from a large
BonusesBonus payments will
be made in a one-timelump sum payment in mid-2009, for PQRI reportingin 2008. The bonus pay-ment will be made to theholder of the TaxIdentification Number (TIN)broken down by NPI num-ber.
The maximum bonuswill be 1.5 percent of ALLMedicare allowablecharges filed during thereporting period, includingthe –TC component of anydiagnostic services.
In some instances, acap may be applied to thebonus. This cap would beapplied when an individ-ual provider only has asmall number of claims inwhich measures couldapply compared to thetotal number of claims thatprovider actually filed.
Because there are fiveeye care-specific measuresand six additional meas-ures available for report-ing, most optometrists willnot be impacted by thebonus payment cap.
Details of how thiscap is calculated can befound atwww.cms.hhs.gov/PQRI orwww.aoa.org/PQRI.xml.
EYE ON WASHINGTON
See Quality, page 12
January.qxp 1/10/2008 3:15 PM Page 11
Fri Jan 11 10:33:46 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_11.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim
12 AOA NEWS
Measure #12: 2027FPrimary Open Angle Glaucoma - Optic Nerve EvaluationThis measure is applied to patients 18 years old and older diag-nosed with primary open-angle glaucoma who have had anoptic nerve evaluation at least once within the past 12 months.This measure should be reported at least once within the report-ing period. Numerator: 2027F Denominator: 18 years or olderICD-9: 365.01, 365.10, 365.11, 365.12, 365.15CPT-1: 92002, 92004, 92012, 92014, 99201-99205, 99212-99215, 99241-99245, 99304-99310, 99324-99328, 99334-99337*Modifiers:1P: Optic nerve head evaluation not performed for documentedmedical reasons * 3P: Optic nerve head evaluation not performed for system rea-son (provider is not primarily responsible for glaucoma manage-ment)8P: Optic nerve head evaluation not performed, reason not oth-erwise specified
*Denotes a new edit to the measureIf a patient was seen prior to the reporting period for an
optic nerve evaluation and returns for an IOP check during thereporting period but an optic nerve evaluation is not performedat that visit, the measure is still reported because the guidelinesstate “optic nerve evaluation at least once with 12 months.”
Thus, the measure should be reported or the encounter willcount against the reporting totals as a missed reporting opportu-nity. Please note that the practitioner may be required to reportthis measure more than once within the reporting periodbecause the reporting period covers an entire 12 months.
Measure #14: 2019FARMD - Dilated Macular ExaminationThis measure applies to patients 50 years old and older diag-nosed with age related macular degeneration (ARMD) whohave had a dilated macular examination performed at least oncewithin the past 12 months. Documentation must include thepresence or absence of macular thickening or hemorrhage ANDthe level of severity of the ARMD. Numerator: 2019FDenominator: 50 years or olderICD-9: 362.50 362.51 362.52CPT-1: 92002, 92004, 92012, 92014, 99201-99205, 99212-99215, 99241-99245, 99304-99310, 99324-99328, 99334-99337*Modifiers:1P: Medical reason(s) for not performing a dilated macularexamination2P: Patient reason for not performing a dilated macular exami-nation* 3P: Optic nerve head evaluation not performed for system rea-son (provider is not primarily responsible for ARMD manage-ment)8P: Other reasons for not performing a dilated macular exami-nation
*Denotes a new edit to the measure
Measure #18: 2021F Diabetic Retinopathy Documentation of Presence orAbsence of Macular Edema and Level of Severity ofRetinopathyThis measure applies to patients 18 years or older who have the
diagnosis of diabetic retinopathy who have had a dilated macu-lar or fundus examination at least once within the last 12months. The documentation must indicate the presence orabsence of macular edema AND the level of severity of the dia-betic retinopathy.
The classification guidelines for the levels of diabeticretinopathy are well documented. The summary of this classifi-cation is posted at www.aoa.org/x7990.xml. Please note that thecorrect use for the diabetic ICD-9 codes require that diabeticretinopathy (362 .01-362 .06) must be coded if you are going tocode 362 .07 for macular edema. Also note this measure is notused for diabetes without retinopathy.Numerator: 2021F Denominator: 18 years or olderICD-9: 362.01, 362.02, 362.03, 362.04, 362.05, 362.06 CPT-1: 92002, 92004, 92012, 92014, 99201-99205, 99212-99215, 99241-99245, 99304-99310, 99324-99328, 99334-99337*Modifiers:1P: Documentation of medical reason dilated macular/fundusexam not performed2P: Documentation of patient reasons dilated macular/fundusexam not performed *3P: Documentation of system reason for exclusion when theprovider is not primarily responsible for the management of theretinopathy8P: Documentation of other reasons dilated macular/fundusexam not performed
*Denotes a new edit to the measure
Measure #19: 5010F, G8397, G8398Diabetic Retinopathy Communication with PhysicianManaging Ongoing Diabetes Care*Reported with the following G code and no longer reportedwith 2021FG8397: Dilated macular or fundus exam performed, includingdocumentation of the presence or absence of macular edemaAND level of severity of retinopathy OR reported with the following G code by itself (without 5010F)G8398: Dilated macular or fundus exam not performed
This measure applies to patients 18 years or older who havethe diagnosis of diabetic retinopathy who have had a dilatedmacular or fundus examination at least once within the last 12months with documented communication with the physicianwho is managing the patient’s diabetes.
Communication is defined as follows: Documentation inthe medical record indicating that the results of the dilated mac-ular or fundus exam were communicated (e.g., verbally, by let-ter) to the clinician managing the patient’s diabetic care OR acopy of a letter in the medical record to the clinician managingthe patient’s diabetic care outlining the findings of the dilatedmacular or fundus exam.Numerator: 5010F (without without a modifier) AND G8397or G8398Denominator: All patients with diabetic retinopathyICD-9: 362.01, 362.02, 362.03, 362.04, 362.05, 362.06CPT-1: 92002, 92004, 92012, 92014, 99201-99205, 99212 –99215, 99241-99245, 99304-99310, 99324-99328, 99334-99337*Modifiers:2P: Documentation of patient reasons for not communicatingresults to physician
NotesAll the applicable meas-ures are detailed in thisarticle. Frequent review ofthe CMS guidance isstrongly recommendedand encouraged.
The 2008 reportingperiod is Jan. 1, 2008 -Dec. 31, 2008. Notethat practitioners may berequired to report meas-ures more than once withinthe reporting periodbecause the reporting peri-od covers an entire 12months. As in 2007, theAOA recommendation isthat the measures bereported in every instanceto ensure that anoptometrist meets all theminimum coding guide-lines to earn the bonuspayments.
Also note that severalof these measures areusing G codes for thereporting in addition to themore familiar CPT IIcodes. G codes are usedwhen there is not a CPT IIcode to adequatelydescribe the measure.When a G code is used,the modifiers 1P, 2P, 3Pand 8P are not used.Instead, a different Gcode is used to describeeach coding situation.
The AOA Web sitewill have all the toolsneeded to properly utilizeall the 2008 PQRI meas-ures. Please visit this sitefrequently. Updates willbe posted as they becomeavailable.
Reporting quality measures – filing specifics
See Quality, page 13
January.qxp 1/10/2008 3:15 PM Page 12
Fri Jan 11 10:32:09 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_12.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim
Qualityfrom page 12
January 2008 13
*3P: Documentation of system reason for exclusion when theprovider is not primarily responsible for the management ofthe retinopathy8P: Documentation of other reasons for not communicatingresults to physician
*Modifier 1P has been eliminated from this measureThe correct combination of numerator codes must be
reported on the claim form in order to properly report thismeasure. The “correct combination” of codes may require thesubmission of multiple numerator codes.5010F and G8397: DR communication occurred and dilatedmacular or fundus exam performedG8398: DR communication occurred and no dilated macular orfundus exam performed5010F 2P and G8397: No DR communication occurred due topatient reasons but dilated macular or fundus exam performed 5010F 3P and G8397: No DR communication occurred due to
system reasons but dilated macular or fundus exam performed 5010F 8P and G8397: No DR communication occurred due to
unspecified reasons but dilated macular or fundus exam per-formed
Therefore, reporting on diabetic retinopathy might includeup to three measures for each claim:
For example, when using 92004 with a diagnosis of362.04, the practitioner might also report 2021F, 5010F andG8397 if the dilated retinal exam was performed, diabeticretinopathy was found, and the findings were communicated tothe primary care physician responsible for caring for the dia-betes.
*Denotes a new edit to the measure
Other measures potentially available for use by optometrists
Please note that the measures 114, 115, and 129 do not listthe 92002-92014 series of codes as denominators at the timethis article was written. The measures included here do list the99201-99215 series of evaluation and management codes sothey are available for those optometrists who can and do utilizethe 99 codes series for some of their patient encounters.Measures 117, 124, 125, 128 do specifically list the 92 codeseries.
Measure #114: 1000F and 1034F or 1035F or 1036FInquiry Regarding Tobacco Use
This measure applies to patients 18 years or older whosmoke and are queried about their tobacco use at least oncewithin the past 24 months. This measure requires two CPT IIcodes per submission.Numerator: 1000F: Tobacco use assessedAnd one of the following:1034F: Current tobacco smoker 1035F: Current smokeless tobacco user1036F: Current tobacco non-userDenominator: 18 years or older99201- 99205, 99212-99215Not associated with any specific ICD-9 diagnosis codeModifiers:8P: Tobacco used not assessed, reason not specifiedAttach to 1000F, only this CPT II required to be reported whenuse not assessed.
Measure #115: G8402, G8403, G8455, G8456, G8457Advising Smokers to Quit(No CPT II codes available for use with this measure).
This measure applies to patients age 18 years and olderwho smoke and who received advice to quit smoking. If smok-er, must file with two appropriate G codes.Numerator:G8402: Tobacco (smoker) use cessation intervention, counselingOR G8403 Tobacco (smoker) use cessation intervention notcounseled AND G8455 Current tobacco smoker OR G8456Current smokeless tobacco user OR G8457 Tobacco non-userDenominator: 18 years or olderCPT-1: 99201 – 99205, 99212 – 99215, 99217- 99220, 99242-99245
Measure #117: 2022F, 2024F, 2026F, 3072FDilated Eye Exam in Diabetic Patient
This measure is used to report patients age 18 through 75years with a diagnosis of diabetes mellitus who had a dilatedeye exam and is used a minimum of once within 12 months. Numerator:2022F: Dilated retinal eye exam with interpretation by an oph-thalmologist or optometrist documented and reviewed2024F: Seven standard field stereoscopic photos with interpreta-tion by an ophthalmologist or optometrist documented andreviewed2026F: Eye imaging validated to match diagnosis from sevenstandard field stereoscopic photos results documented andreviewed3072F: Low risk for retinopathy (no evidence of retinopathy inthe prior year)Denominator: 18 to 75 years old
ICD-9: 250.00, 250.01, 250.02, 250.03, 250.10, 250.11,250.12, 250.13, 250.20, 250.21, 250.22, 250.23, 250.30, 250.31,250.32, 250.33, 250.40, 250.41, 250.42, 250.43, 250.50, 250.51,250.52, 250.53, 250.60, 250.61, 250.62, 250.63, 250.70, 250.71,250.72, 250.73, 250.80, 250.81, 250.82, 250.83, 250.90, 250.91,250.92, 250.93, 357.2, 362.01, 362.02, 362.03, 362.04, 362.05,362.06, 362.07, 366.41, 648.00, 648.01, 648.02, 648.03, 648.04
CPT I: 92002, 92004, 92012, 92014, 99201-99205. 99212– 99215, 99217-99220, 99242-99245, 99455-99456Modifiers:8P Dilated eye exam was not performed, reason not otherwisespecified. 8P modifier does not apply to code 3072F.
Measure #124: G8447, G8448, G8449HIT - Adoption/Use of Health Information Technology(Electronic Health Records)
This measure is to be reported at each visit occurring dur-ing the reporting period for patients 18 years and older seenduring the reporting period. There is no diagnosis associatedwith this measure. This measure may be reported by clinicianswho have adopted and are using health information technology.
Patient encounter documentation substantiates use of certi-fied/qualified EMR (CCHIT) or the EMR is non-certified but iscapable of generating a medication list, a problem list and enter-ing laboratory tests as discrete searchable data elements. Todate, there are no commercially available, optometry-specificEMRs that have obtained certification.
Note that this measure cannot be used if the practitionerdoes not have an EMR that meets the qualifications listedabove.
PQRI pollThe AOA WashingtonOffice is conducting a sur-vey to determine howmany optometrists are par-ticipating in Medicare’sPhysician QualityReporting Initiative (PQRI).
AOA members areurged to respond byanswering the followingquestion:Are you participating inthe PQRI program toreport quality indicatorsfor eye care services?
YES, and I plan to doso in ‘08
YES, but I will not do soin ‘08
NO, but I plan to do soin ‘08
NO, and I do not planto do so in ‘08
To participate in the poll,log on to the AOA Website PQRI page(www.aoa.org/pqri.xml).
See Quality, page 14
January.qxp 1/10/2008 3:15 PM Page 13
Fri Jan 11 10:31:54 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_13.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim
14 AOA NEWS
Numerator:G8447 Patient encounter was documented using a CCHITCertified or Qualified EMR G8448: Patient encounter was documented using a non-CCHITcertified EMR but the system was qualified (see above)G8449: Patient encounter was not documented using an EMRdue to system reasons but a certified or non-certified but quali-fied EMR is in place and generally availableDenominator: 18 years or olderCPT-1: 90801 – 90809, 92002 – 92014, 96150 – 96152, 97001-97004, 9750, 97802 – 97804, 98940 – 98942, 99201-99215,99241-99245, D7140, D7210, G0101, G0108, G0109, G0270,G0271Modifiers: None listed
Measure #125: G8443, G8445, G8446HIT - Adoption/Use of e-Prescribing
This measure is to be reported at each visit occurring dur-ing the reporting period for patients 18 years and older seenduring the reporting period. There is no diagnosis associatedwith this measure. This measure may be reported by clinicianswho have adopted a qualified e-Prescribing system.
A qualified e-prescribing system has been adopted capableof generating a medication list and selecting/printing/transmit-ting/performing safety checks of prescriptions. (Please see thespecific CMS guidance for more details.)
Please note that this measure cannot be used if the practi-tioner does not have access to a qualified e-prescribing system.Numerator:G8443: All prescriptions created during the encounter were gen-erated using a qualified e-Prescribing systemG8445: No prescriptions were generated during the encounter,provider does have access to a qualified e-Prescribing systemG8446: Some or all prescriptions generated during encounterwere handwritten or phoned in due to a state law requirement,patient request, or qualified e-prescribing system was temporari-ly inoperable.Denominator: 18 years or olderCPT-1: 90801-90809, 92002-92014, 96150-96152, 97001-97004, 9750, 97802-97804, 98940-98942, 99201-99215, 99241-99245, G0101, G0108, G0109Modifiers: None listed
Measure #128: G8417, G8418, G8419, G8420, G8421, G8422Universal Weight Screening and Follow-Up
This measure is used to report patients age 65 years andolder with a calculated Body Mass Index (BMI) within the pastsix months or during the current visit that is documented in themedical record, and if the most recent BMI is greater than 30 or
less than 22, a follow-up plan is documented. BMI is a number calculated from a person’s weight and
height. BMI can be calculated using a chart or formula; howev-er, the patient’s actual weight and height must be measured andcannot be merely reported by the patient. Follow up caninclude documentation of a future appointment, education,referral, prescription/administration of medication/diet supple-ments and the like.Numerators: G8417: BMI greater than 30 was calculated and afollow-up plan was documented in the medical recordG8418: BMI less than 22 was calculated and a follow-up planwas documented in the medical recordG8419: BMI greater than 30 OR less than 22 was calculated,but no follow-up plan documented in the medical recordG8420: BMI greater than 30 AND less than 22 was calculatedand documentedG8421: BMI not calculatedG8422: Patient not eligible for BMI calculation or BMI not per-formed and/or Calculated BMI greater than 30 or less than 22,follow-up plan not documented, reason not specified in medicalrecordDenominator: Age 65 and olderICD-9: 00140, 00142, 00170, 00400, 00402, 00810, 00832,00851, 00910, 00920, 01380, 01382, 01400, 01732, 01810,01820, 01829,CPT-1 90801- 90809, 92002- 92014, 97001, 97003, 97802,97803, 99201- 99215, 99241-99245, 99324 - 99328, 99334 -99337, 99341- 99345, 99347 - 99350, D7140, D7210, G0101,G0108, G0270Modifiers: None listedExceptions: Patients can be considered not eligible in the fol-lowing situations: Patient already is diagnosed as over- orunder-weight and there is documentation in the medical recordthat the weight problem is being managed by another provider;patient has a terminal illness; patient refuses BMI measurement;there is any other reason documented by the provider in themedical record, explaining why the BMI measurement was notappropriate; patient is in an urgent or emergent medical situa-tion where time is of the essence and to delay treatment wouldjeopardize the patient’s health status
Measure #129: G8423, G8424, G8425, G8426Universal Influenza Vaccine Screening and Counseling
This measure is to be reported at each visit occurring dur-ing the months of January, February, March, October,November, and December during the reporting period forpatients seen during the reporting period and who are screenedand counseled about influenza vaccine. This measure is usedfor patients age 50 years and older.Numerator:G8423: Documented that patient was screened and eitherinfluenza vaccination status is current or patient was counseledG8424: Influenza vaccine status was not screenedG8425: Influenza vaccine status screened, patient status not cur-rent and counseling was not providedG8426: Documented that patient was not appropriate for screen-ing and/or counseling about the influenza vaccine (e.g., allergyto eggs)Denominator: Age 50 and olderCPT: 00140, 00142, 00170, 00400, 00402, 00810, 00832,00851, 00910, 00920, 01380, 01382, 01400, 01732, 01810,01820, 01829, 90801- 90809, 97802, 97803, 99201- 99215,99241-99245, 99324 - 99328, 99334 - 99337, 99341- 99345,99347 - 99350, G0101, G0108, G0270Modifiers: None listed
SummaryThe 2008 PQRI reporting period is Jan. 1, 2008, to Dec. 31, 2008.There are 11 measures available for use by optometrists for this reporting period.Four of the 2007 measures were carried over with minor modifications.There are seven new measures available for use by optometrists.
Successful reporting requires reporting at least three measures in 80 percent of thereportable cases.
Many of the measures now use G codes instead of CPT II codes with modifiers.The AOA Web site will list all the up-to-date information.The 2008 bonus is approximately 1.5 percent of all allowable Medicare charges.The 2007 PQRI reports should be available in June 2008.Congress could decide to change all or part of this program as it considers options to
fix the flawed SGR reimbursement formula.
Qualityfrom page 13
January.qxp 1/10/2008 3:15 PM Page 14
Fri Jan 11 10:34:48 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_14.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

January 2008 15
Former AOA PresidentLester Hussey, O.D.,died on Dec. 21. He
was the only member of theOptometric Physicians ofWashington (then theWashington OptometricAssociation) to serve as presi-dent of the AOA.
Dr. Hussey served asAOA president during the1970-1971 program year.
He served the AOA for32 years, including service onthe AOA’s InsuranceCommittee, in the AOADepartment of Public Health,and in the AOA Departmentof Organization.
He was president of theWashington OptometricAssociation (WOA) from1958 to 1960.
The WOA named himthe Optometrist of the Year in1960.
Dr. Hussey graduated
Former AOA PresidentDon A. Frantz, O.D.,died Dec. 3, 2007, at
the age of 91. He served as AOA presi-
dent during the 1961-1962program year.
Dr. Frantz was the char-ter chair of the AOA commit-tee on practice management.He served eight years as sec-retary of the AOA council onoptometric education andserved as chair of the Long-Term Planning Committee.He served as vice president ofthe Illinois OptometricAssociation (IOA) and was incharge of public information.
The IOA named Dr.Frantz the Optometrist of theYear in 1962.
Dr. Frantz graduatedfrom the Northern IllinoisSchool of Optometry in 1937.
After graduation, Dr.
from the Los Angeles Collegeof Optometry in 1938. Hiswork included the areas ofvision and reading and sub-normal vision.
He interrupted his prac-tice in Spokane, Wash., toserve in the Navy for fouryears beginning in 1943.
After returning to prac-tice, Dr. Hussey served aspresident of the SpokaneRehabilitation Center, as thechair of the Spokane Employthe Handicapped Committee,and as president of theEastern Washington Societyfor Crippled Children andAdults.
He also worked with theSpokane Central Lions Cluband the Easter Seal Society.
Dr. Hussey was a boardmember of the VisionInstitute of America and theVision Conservation Instituteof the Northwest.
Dr. Hussey is survived byhis wife, Margaret, and twosons, Dana (wife Gail)Hussey and Eric (wife Lisa)Shaw Hussey. He had fivegrandchildren.
Contributions may bemade to Liberty Park UnitedMethodist Church, 1526 E.11th, Spokane, WA 99202 orthe Union Gospel Mission,PO Box 4066, Spokane, WA99202.
Frantz practiced in DeKalb,Ill., for 40 years.
He also taught practicemanagement at the IllinoisCollege of Optometry andwas named to a Health,Education and Welfare com-mission under PresidentNixon.
Dr. Frantz wrote numer-ous articles on practice man-agement, vision training, tele-vision vision, home lighting,and other optometric subjects.He was a distinguished mem-ber and lecturer for theOptometric ExtensionProgram and was a fellow ofthe American Academy ofOptometry and a past presi-dent of the Illinois chapter ofthe Academy.
As a pioneer in develop-ing natural stereoscopicrefraction techniques, Dr.Frantz produced the
Kodachrome slide series usedby the AOA.
He was also active inRotary clubs in Illinois andFlorida.
Dr. Frantz is survived byhis wife, Alta; two daughters,Pam (husband Doug)Schnetzler, and Carol (hus-band Dave) Oberg; fivegrandchildren; six great-grandchildren; and a brother,Charles Frantz.
Hussey served AOA 32 years
Frantz: Noted educator, authorPast AOA presidents remembered
COVD honors ODs,elects officers
The 37th AnnualMeeting of theCollege of
Optometrists in VisionDevelopment in St.Petersburg, Fla., was attendedby 610 people, setting a newattendance record.
For the two days prior tothe meeting, intensive courseswere given in the areas ofvisual information acquisi-tion, visual information pro-cessing, strabismus andamblyopia, and acquired braininjury. In addition, a one-day“VT 101” course was present-ed for vision therapists.
COVD’s President’sAward was presented to LindaSanet, from Lemon Grove,Calif., in recognition of hersignificant contributions toteaching and mentoring visiontherapists.
The Optometry & VisionDevelopment Award for bestpublished article during thepast year was given to YiPang, O.D., Ph.D., of theIllinois College of Optometryfor his article “Myopia: CanIts Progression BeControlled?” Additionalauthors on this article wereDominick Maino, O.D., MEd;Guoming Zhang, M.D.,Ph.D.; and Fan Lu, O.D.,M.D.
Harold Solan, O.D., ofCliffside Park, N.J., receivedthe 2007 G.N. Getman Awardin recognition of his clinical
expertise in developmentaloptometry and his dedicationto patient care. The 2007 A.M.Skeffington Award for out-standing contributions to theoptometric literature in theareas of behavioral vision careand vision therapy was givento Kenneth Ciuffreda, O.D.,Ph.D. The 2007 CertifiedOptometric Vision Therapist ofthe Year Award was given toLyna Dyson of Poway, Calif.,for her outstanding dedicationto behavioral optometry andpatient care.
Fourteen optometrists atthe meeting became BoardCertified Fellows (FCOVD)of COVD, while four becameBoard Certified AcademicFellows (FCOVD-A). Thesewere added to four optom-etrists who became BoardCertified Fellows (FCOVD)in Mexico a month earlier.
COVD elected Dan L.Fortenbacher, O.D., as presi-dent. Also serving during thecoming year are: President-elect Bradley E. Habermehl,O.D.,; Vice President CaroleL. Hong, O.D.; Secretary-Treasurer Robert S. Byne,O.D.; Immediate PastPresident Drusilla H. Grant,O.D.; East Regional DirectorIda Chung, O.D.; CentralRegional Director David A.Damari, O.D.; West RegionalDirector Julie B. Ryan, O.D.;Regional Director-at-LargeJason Clopton, O.D.
Call for posters openThe AOA is inviting participation in the Clinical and
Scientific Poster Session at the 111th Annual AOACongress & 38th Annual AOSA Conference:Optometry’s Meeting™. The poster preview session willbe held Friday, June 27, and the interactive session offer-ing continuing education credit will be Saturday, June28, from 11 a.m. to 2 p.m. at the Washington StateConvention and Trade Center. Poster abstracts must besubmitted electronically by Feb. 6, 2008. For detailsand an electronic submission form, log on towww.optometrysmeeting.org and click on the Call forPosters icon. For more information, contact Stacy Smith at314-983-4254 or at [email protected].
January.qxp 1/10/2008 3:49 PM Page 15
Fri Jan 11 10:20:18 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_15.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

the project team is looking atboard certification as well asmaintenance of certificationin optometry and does notanticipate a sub-specialtycomponent at this time.
Consensus so far
At a November meeting,the Joint Board CertificationProject Team agreed to“Develop and propose anattainable, credible, anddefensible model for BoardCertification in Optometryand maintenance of certifica-tion for adoption by the pro-fession. This model willestablish standards for volun-tary board certification andmaintenance of certificationin the practice of optometry.This model will communicateinformation about these stan-dards to support the public’squest for safe high-qualityhealth care.”
Dr. Brooks noted that asthe group continues to gathermore information about boardcertification in other healthcare professions, it will con-tinue to weigh the goals forthe profession as outlined inthe Optometry 2020Summits.
To date, the Joint BoardCertification Project Teamhas studied more than 3,000pages of background material.
He explained that whilethe joint project team ischarged with creating a modelboard certification processrather than a final product, thegroup will neither become acredentialing organization normake a decision on whethersuch a process goes forward.
“I think board certifica-tion represents another step inthe maturation of optometryas a profession,” Dr. Brookssaid.
“It’s gratifying to seerepresentatives of six diverseorganizations working togeth-er toward a goal that will ben-efit the optometrist, the pro-fession as a whole and ulti-mately our patients. Wepromise an open and trans-parent process with regularcommunications to keep theprofession informed as wedevelop a process to advancethe profession,” he said.
16 AOA NEWS
Certification,from page 1
quality assurance standards,and patients themselves whoare growing to expect “scorecards” for providers are alldriving the trend toward per-formance assessment and cre-dentialing.
“Pay-for-Performancemay intensify the need forboard certification foroptometrists,” Dr. Brookssaid. “Optometry is a profes-sion where certification andmaintenance of certificationcould be important, but thereis no mechanism yet forapplying it.”
The trend toward boardcertification and maintenanceof certification is accelerat-ing. Of practicing physiciansin the United States, morethan 85 percent are board cer-tified, up from 50 percent inthe 1960s.
In 2006, the AmericanBoard of Medical Specialties’24 member boards adopted aprogram of continuous pro-fessional development—ABMS Maintenance ofCertification —as a formalmeans of measuring a physi-cian’s continued competencein his or her certified special-ty.
“Board certification isnot only important to hospi-tals. Insurers, health careorganizations and even largeemployers not traditionallyassociated with health careare now interested in boardcertification as a measure ofquality health care delivery,”said AOA President Kevin L.Alexander, O.D., Ph.D.
Continuing discussion
Within optometry, thereis growing recognition thatODs should not only have thecurrent skills to treat patientsusing the highest standards ofcare, but must be able toprove they have those skills.
Dr. Brooks noted that asfar back as the 1960s, theprofession has looked at waysof proving practitioner com-petence.
The issue came to theforefront seven years agowhen the American Board of
Optometric Practice(ABOP) was proposed andultimately rejected. TheAOA House of Delegates, invoting down funding forABOP, called for the AOAto lead a profession-widesummit and study the issueof specialization and boardcertification. This summitwas called the Summit onBoard Certification andContinued Competency.
Following that sum-mit’s report to the AOAHouse of Delegates in June2001, two subsequent proj-
ect teams studied the issueof advanced competence,specialization and board cer-tification.
The final report in 2005of the second project team,the Advanced ClinicalCompetence Project Team,recommended that discus-sion in this area occur aspart of the upcomingOptometry 2020 Summit.
Dr. Brooks noted that itwas significant that otherorganizations at theOptometry 2020 Summit —including AAO, ARBO,ASCO and NBEO — select-
ed specific futures relating toadvanced competence andboard certification in August2006.
AOA representativesagreed to work with theseorganizations to explore thesefutures.
In addition, in May 2006,ARBO — at the NationalOptometric ContinuingEducation Conference —concluded that “renewed dia-logue should be consideredinvolving all stakeholders,organized by ARBO andAOA leadership, to reassess
the continued competenceand board certification topic.”
It was in light of thesedevelopments that the AOAsupported the formation of ajoint project team with repre-sentatives appointed by keystakeholder organizations, Dr.Brooks said.
“It’s important that theentire profession agree on onemodel,” said Dr. Alexander.“The issue of advanced com-petence and credentialingshouldn’t belong to just oneoptometric organization, andwe clearly don’t want anorganization outside of
optometry to take on thatrole.”
“To me, the issue of pur-suing board certification inoptometry is very much likethe profession’s decision topursue therapeutic pharma-ceutical privileges in pastdecades,” Dr. Brooks said.
“There were argumentsthat therapeutic practicewould create different classesof practitioners and createobstacles to ODs. There aresimilar arguments nowagainst board certification,but I would contend that, just
as gaining the ability to man-age and treat patients witheye disease has improved ourprofession, being able todemonstrate, through boardcertification, a level ofadvanced clinical competencewill open new doors tooptometrists – and is the rightthing to do.”
The Joint Project Teamhas agreed that board certifi-cation must be credible, yetattainable for the practicingOD and needs to be a volun-tary process not tied to licen-sure.
Dr. Brooks also said that
Working definitionsThe Joint Board Certification Project Team has unanimously agreed to these “working def-initions.”
Board Certification in OptometryA voluntary process that establishes standards that denotes a doctor of optometry hasexceeded the requirement(s) necessary for licensure. It provides the assurance that adoctor of optometry maintains the appropriate knowledge, skills, and experience neededto deliver quality patient care in optometry.
Advanced Competence in OptometryThe possession of knowledge, skills, and experience beyond the requirement(s) neces-sary for licensure.
Maintenance of Certification in OptometryA formal means of measuring cumulative and ongoing qualifications to deliver qualitypatient care.
I would contend that, just as gaining the ability to manage and treat patients with
eye disease has improved our profession, being able to demonstrate, through board certification, a level of advanced clinical
competence will open new doors to optometrists– and is the right thing to do.”
January.qxp 1/11/2008 8:35 AM Page 16
Fri Jan 11 10:28:53 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_16.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

January.qxp 1/10/2008 3:18 PM Page 17
Fri Jan 11 10:31:54 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_17.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

18 AOA NEWS
Call for ApplicationsVSP Research Grants
The American Optometric Foundation (AOF) andVSP have entered into a partnership to support researchinto the efficacy of optometric care and optometric med-ical interventions.
Topics related to private practice and optometricoutcomes will be given high priority. Examples wouldinclude diabetes, diabetic retinopathy, hypertensiveretinopathy, glaucoma, corneal arcus, metabolic syn-drome, and macular degeneration, but proposals inother areas are encouraged as well.
Other areas of emphasis include research investi-gating the possible links between optometry and othermedical maladies and linkage to lifestyle and behav-ioral issues (like obesity) that have medical or optometricramifications.
There will be a single one-year award of up to$42,000. A wide variety of research-oriented entitiesare eligible for this program, including but not limited toindividual researchers; corporations; schools and col-leges of optometry; schools and colleges of publichealth; schools and colleges of medicine; professionalassociations; and private foundations.
Submissions must be received by March 1, 2008.Grant recipients will be announced in May 2008. Eachproposal must be submitted electronically (pdf recom-mended) on 8.5" x 11" sized paper and mustcontain the following components:� Introduction; background and significance; specificaims; preliminary studies; and study designand methods. These sections should total no more thanfive pages.� References (maximum of one page)� Budget and budget justification (maximum of onepage)� Biographical sketch(es) of principal and one co-investigator only (maximum of two pages for eachinvestigator)o Education/training; research and professional experi-ence; honors and awardso Publications (refereed) for the last three years and rep-resentative earlier
Applications that do not follow this outline may notbe considered. Proposals are reviewed by a peerreview committee established by the AAO’s ResearchCommittee. All proposals must be sent by e-mail to AlisaMoore ([email protected]).
The AOF is not to cover any overhead/indirectcosts associated with VSP Research Grants or any otherof our programs.
This policy applies uniformly to all award recipi-ents. Funds support research conducted for a period ofone year. Recipients must submit a report of theirresearch findings to the AOF at the end of the awardperiod and will be encouraged to submit a manuscriptto Optometry and Vision Science.
For additional information, contact Mark Bullimore, MCOptom, Ph.D., president, AOF: 614-292-4724 or [email protected].
have a way to demonstratecontinued competence suchas board certification.
There are many otherconcerns that optometricleaders have about the needto develop a means todemonstrate continuedcompetence.
As AOA president, Iunderstand the concernabout adopting a programsuch as board certification.In subsequent President’scolumns, I intend to exploremany of these concerns.
I believe the need todevelop board certificationas a means to demonstratecontinued competence isvery real. I ask for patienceby the profession as we
Presidentfrom page 3
explore this issue thoughtful-ly, deliberately, slowly andwith the input of many. I askeveryone to remain open tothe idea that these six organi-zations are exploring boardcertification not to “create anew hoop to jump through”as has been suggested bysome, but rather to proactive-ly prepare the profession forthe kind of scrutiny we aregoing to receive in the nearfuture and to do it on ourterms.
We do not want anorganization outside optome-try developing a way for us todemonstrate continued com-petence.
Like the scouting reportof the old wagon trains, I
know that many of you don’tlike the report your optomet-ric scouts are giving youabout the future. Some ofyou have asked—“Don’t youknow that if you polledoptometrists you would findthat they don’t want boardcertification?” Of course, theanswer to that question isobvious—no one wants tohave additional requirementsfor continued practice.
But what if we askedyour patients—“Do you thinkyour optometrist shoulddemonstrate competence on aregular basis?” I’ll bet we’dget a different answer.
“We do not want an organization outsideoptometry developing a way for us to demonstrate continued competence.”
January.qxp 1/10/2008 3:18 PM Page 18
Fri Jan 11 10:32:15 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_18.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

January 2008 19
AOA’s volunteer structure issupported by 96 staff. Formore information on AOA’sprograms and services, youmay contact the staff at thefollowing numbers.Accounts Payable 800-365-2219 x4248Accounts Receivable800-365-2219 x4239Accreditation Council onOptometric Education800-365-2219 x4246,x4262 or [email protected]@[email protected] Changes800-365-2219 x4112 (Leave message)[email protected] News800-365-2219 [email protected]@[email protected] Political ActionCommittee [email protected] Vision800-365-2219 [email protected] Awards(Member Records)800-365-2219 [email protected] Guidance Materials800-365-2219 [email protected]'s Vision TopicalInterest Group (TIG)800-365-2219 [email protected] [email protected] Care Information800-365-2219 x4245/[email protected] Practice Guidelines800-365-2219 x4237/[email protected]/billing questions 703-837-1344 [email protected] onParaoptometric Certification800-365-2219 x4135, [email protected]@aoa.orgCommunications Group800-365-2219 [email protected] Health Centers800-365-2219 x4244 or [email protected] Lens and CorneaSection800-365-2219 x4137 [email protected] Education:Opt. CE-Other Assns. 800-365-2219 [email protected] Analysis Service800-365-2219 [email protected] CE 800-365-2219 x4256Council on Research800-365-2219 x4244 or [email protected]
Getting in touch with the AOA
Don’t know where to start?Call Member Services at800-365-2219 x4179
Help us serve you better. When calling, if you leave amessage be sure to includeinformation on whether thenumber is for your home oroffice and from what timezone you are calling. Better,include information on thebest time for AOA staff toreturn your call.
Diabetes Initiative - CMS [email protected] Fund800-365-2219 [email protected]/Occupational Vision800-365-2219 x4244 or [email protected] and Values800-365-2219 [email protected] [email protected] Care [email protected] x4234Federal GovernmentRelations Center 703-739-9200, [email protected] CenterAccounts Payable 800-365-2219 x4248Accounts Receivable800-365-2219 x4239Geriatrics/Nursing Facility800-365-2219 [email protected] InformationTechnology703 [email protected] Practice800-365-2219 [email protected] Relations800-365-2219 [email protected]’ & Children’s VisionCoalition800-365-2219, [email protected]®800-365-2219 [email protected] Insurance [email protected] x4234Keyperson Program703- [email protected] Aspects of Practice800-365-2219 [email protected] [email protected] [email protected] (ILAMO)800-365-2219 Information and Loansx4117, 4118, 4102, or 4104;
Calendar of Meetings [email protected] Vision Rehabilitation Section800-365-2219 [email protected] [email protected] x4234Media Relations800-365-2219 [email protected] [email protected] [email protected] Records (AOA)800-365-2219 x4131
[email protected] Services800-365-2219 [email protected] and Tributes(Book of Memory)AOA Endowment Fund800-365-2219 [email protected] [email protected] Technology800-365-2219 [email protected] Standards800-365-2219 x4244/[email protected] LeadershipInstitute 800-365-2219 [email protected] RecognitionAwards (ORA)800-365-2219 x4258 or [email protected]:Journal of the [email protected]’s MeetingTM
General information800-365-2219 [email protected] Education800-365-2219 x4254 [email protected] [email protected] Programs800-365-2219 [email protected]'s CareerCenter® (OCC)800-365-2219 x4107 [email protected] DepartmentTo Place An Order:800-262-2210Business Cards/OfficeForms:[email protected] Inquiries:800-365-2219 x4239Paraoptometric Section800-365-2219 x4222 or [email protected]@aoa.orgPediatrics/Binocular Vision800-365-2219 [email protected] AssistanceProgram800-365-2219 [email protected] ManagementResources800-365-2219 [email protected] Strategies800-365-2219 [email protected] Care800-365-2219 x4245/[email protected] [email protected] Health Issues800-365-2219 x4244 or [email protected]
Public Relations800-365-2219 [email protected] Surgery TopicalInterest Group (TIG)800-365-2219 [email protected] Assessment andImprovement, Pay ForPerformance 800-365-2219 [email protected] Your Vision Month800-365-2219 [email protected] of Acceptance800-365-2219 x4244/[email protected] Vision Section800-365-2219 [email protected] Legislation/State Licensure/State Optometry Laws800-365-2219 [email protected] and FacultyPrograms800-365-2219 [email protected]
Surveys800-365-2219 [email protected] [email protected] Party [email protected] x4234Travel Reimbursement800-365-2219 x4239VISION USA800-365-2219 [email protected] Site Information800-365-2219 [email protected]
Direct lines to the AOA:A new phone system allowsAOA members to reachAOA staff directly. For St.Louis staff, dial (314) 983-XXXX, where the four digitsare the four-digit extensioncode listed.
For Washington, DC, officestaff, dial (703) 837-XXXX,where the four digits are thelast four digits listed.
January.qxp 1/10/2008 3:19 PM Page 19
Fri Jan 11 10:31:51 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_19.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

20 AOA NEWS
Advanced MedicalOptics
Alcon
Allergan
Bausch & Lomb
CIBA Vision Corporation
CooperVision
Essilor of America
HOYA Vision Care
Johnson & JohnsonVision Care
Liberty Sport
Luxottica Group
Marchon Eyewear
Optos
TLC Vision Corporation
Transitions Optical
VSP Vision Care
VisionWeb
Industry Profile is aregular feature in AOA News
allowing participantsof the
Ophthalmic Council to express
themselves on issuesand products
they consider impor-tant to the members
of the AOA.
Industry Profile is a regular feature in AOA News allowing participants of the
Ophthalmic Council to express themselves on issues and products
they consider important to the members of the AOA.
Industry Profile: Advanced Medical Optics
Acuvue® 2 Colours®now offersiMakeover™ for
those who are consideringchanging their looks with anew eye color.
The virtual makeovertool allows contact lenspatients to get a sneak peekat what they would look likewith different colored contactlenses that enhance orchange their natural eyecolor.
Visitors towww.imakeover.acuvue.comcan use this virtual changingroom for contact lenses byuploading their own photosand trying on different col-ored lenses.
With 10 color choices,users can find the shades thatbest match their unique fea-tures.
Colored contacts, likeAcuvue 2 Colours, are suit-able for everyday wear or forspecial occasions.
“Like color cosmetics,colored contact lenses are afabulous tool for enhancingyour beauty,” said makeupartist Mally Roncal. “I usecolored contacts as a beautyaccessory. My celebrityclients wear colored contactlenses to change their lookfor films, red carpet eventsand photo shoots.”
Roncal’s beauty tips for
Advanced Medical Optics (AMO) is focused on pro-viding the full range of advanced refractive technologiesand support to help eye care professionals deliver opti-mal vision and lifestyle experiences to patients of allages.
AMO offers market-leading technologies for myopia,hyperopia, astigmatism, presbyopia, cataract, sphericalaberration, contact lens care and corneal health, as wellas proven educational and support programs that helpeye care professionals master refractive technologiesand grow their practices.
Over the past year, AMO fortified its CompleteRefractive Solution strategy through the acquisitions ofIntraLase Corp., the global leader in ophthalmic femtosecond laser technology, and WaveFront Sciences,Inc., a provider of proprietary wavefront diagnostic sys-tems.
Consequently, AMO now offers refractive surgeonsan unrivaled, state-of-the-art LASIK system, which hasbeen approved by the National Aeronautics and SpaceAgency (NASA) for use on U.S. astronauts.
The company also launched several new products in2007, including the WhiteStar Signature™ phacoemulsi-fication system, Tecnis® 1-Piece and Multifocal AcrylicIntraocular Lenses (IOLs) (Europe), and Complete® Multi-Purpose Solution Easy Rub™ Formula.
Products in AMO’s cataract/implant line includeIOLs, phacoemulsification systems, viscoelastics, and relat-ed products used in ocular surgery.
AMO owns or has the rights to such product brandsas ReZoom®, Tecnis®, Clariflex®, Sensar®, andVerisyse® IOLs, Sovereign®, Sovereign® Compact andWhiteStar Signature™ phacoemulsification systems withWhiteStar® technology, Healon® viscoelastics, and theBaerveldt® glaucoma shunt.
Products in the laser vision correction line includewavefront diagnostic devices, femtosecond lasers andassociated patient interface devices, and excimer laservision correction systems and treatment cards.
AMO brands in the laser vision correction businessinclude Star S4 IR®, WaveScan Wavefront®, AdvancedCustomVue™, IntraLase® and IntraLasik®.
Products in the contact lens care line include disin-fecting solutions, enzymatic cleaners and lens rewettingdrops.
Among the eye care product brands the companypossesses are Complete®, Complete® Blink-N-Clean®,Consept®F, Consept® 1 Step, Oxysept® 1 Step,UltraCare®, Ultrazyme®, Total Care™ and blink™branded products.
AMO is based in Santa Ana, Calif., and employsapproximately 4,200 worldwide.
The company has operations in 24 countries andmarkets products in approximately 60 countries.
For more information, visit the company’s Web site atwww.amo-inc.com.
enhancing eye color and afree trial pair certificate areavailable on the iMakeoverWeb site.
How it WorksTo start the virtual expe-
rience, patients can upload ahigh-quality digital photo(iMakeover recommendsJPEG files and a forward-facing photo taken withoutglasses or a flash).
They can then choosefrom various shades ofAcuvue 2 Colours, whichcan be fit for light eyes ordark eyes even if they do notneed vision correction.
After choosing a color,users can then adjust thesize, position and eyelid fitof the lenses to match theireye shape in the photo.
Next, they can choosefrom one of 11 decorativeframes to complete the pic-ture.
The selected color willappear in a description at thebottom of the photo to save“try on” time at theoptometrist’s office.
Finally, users can save,download, and print theiriMakeover photo and freetrial pair certificate to take totheir doctor who will deter-mine if Acuvue® 2 Colours®
Brand Contact Lenses areright for them.
Acuvue 2 Coloursoffers iMakeover on Web site
January.qxp 1/10/2008 3:19 PM Page 20
Fri Jan 11 10:31:50 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_20.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim

January 2008 21
INDUSTRY NEWS
Allergan, Inc.announced the U.S.Food and Drug
Administration’s approval ofCombigan™ 0.2%/ 0.5%, analpha adrenergic receptoragonist with a beta adrener-gic receptor inhibitor, for thereduction of elevated intraoc-ular pressure (IOP) inpatients with glaucoma orocular hypertension whorequire adjunctive or replace-ment therapy due to inade-quately controlled IOP.
Combigan contains bri-monidine and timolol and isthe newest addition toAllergan’s glaucoma portfo-lio, which also includesLumigan® 0.03% andAlphagan® P 0.1% and0.15%.
“Combigan ophthalmicsolution is a medication thatprovides well-documentedsafety and efficacy forpatients with inadequatelycontrolled IOP,” said ScottWhitcup, M.D., Allergan’s
Allergan gets FDA approval for new IOP-lowering drugexecutive vice president,Research and Development.“The development ofCombigan, which hasincluded five key clinicalstudies, underscoresAllergan’s commitment toprovide new treatmentoptions for patients withglaucoma.”
Combigan is a prescrip-tion eye drop that works toreduce elevated IOP.
“There is no cure forglaucoma; however, lower-
ing elevated IOP can slowthe progression of the diseaseand help prevent furthervision loss,” said E. RandyCraven, M.D., director of theGlaucoma Consultants ofColorado and associate clini-cal professor ofOphthalmology, Universityof Colorado School ofMedicine. “Many patientsrequire more than one med-ication to meet their targetIOP. With Combigan, it isexciting to be able to offer
patients two strong agents inone bottle.”
For more information,visit www.allergan.com.
Transitions Optical,Inc. named BrettCraig president, effec-
tive Jan. 1, 2008. Rick Elias,who previously served aspresident, assumed the roleof chief executive officer(CEO).
In the role of president,Craig, who was previouslyacting as chief operating offi-cer (COO), is responsible forTransitions’ business strate-gies, including strengtheningpartnerships withTransitions’ customers, tomeet ongoing growth objec-tives.
“Obviously the role ofpresident is one of greatresponsibility and greatopportunity,” said Elias.
“Throughout the pastmonths as acting COO, Bretthas built solid relationshipswith employees and partners
alike, making his move tothis role a natural one. AsCEO, I will focus my effortson aligning with key cus-tomers globally toward mutu-al, strategic growth,” saidElias.
Craig was named COOin June 2006. He joinedTransitions in July 1999 asmanaging director, AsiaPacific, and then moved tomanaging director, EMEA(Europe, Middle East,Africa), where he played akey role in positioning theEMEA businesses for contin-ued growth.
“I look forward to thechallenges that will comewith my new role as presi-dent of Transitions, as wellas the opportunities and suc-cesses that lie ahead for ourcompany and our partners,”said Craig.
“I intend to support theproducts and programs thatwe have in place, whileexploring new areas of inno-vation that will expand theapplication of our technologyand the advancement ofhealthy sight,” said Craig.
For more informationabout Transitions, visitwww.transitions.com or con-tact Transitions OpticalCustomer Service at 800-848-1506.
Brett Craig, Transitions president
Transitions Optical appoints Craig president, Elias CEO
Panoptx Eyewearlaunched a new logo,along with new models
and new technology, thismonth.
The “7Eye” by Panoptxlogo features a stylizednumeral 7 tied to a new brand“7Eye” with a renewedemphasis on DysfunctionalTear Syndrome (DTS) treat-ment and servicing the inde-pendent dispensaries that carefor people with DTS symp-toms.
“The eye care practition-er who already is focused onDysfunctional Tear Syndrometreatment knows that our eye-wear is essential once apatient reaches stage four ofDysfunctional TearSyndrome,” said JacksonHogen, vice president of mar-keting and research anddesign.
“Yet, our greatest valuemay be to patients whosesymptoms are less severe. Ifpatients start wearing 7Eyebefore they reach stage four,there’s a good chance theireyes won’t just feel better
with our eyewear, they’llactually be better,” saidHogen.
A complete line of 7Eyeby Panoptx products for allcategories will be releasedthis January.
Most models will bearfamiliar names and fits tohelp retailers through thetransition, including the Bora,Churada and Whirlwind mod-els in the Seal ProtectionFactor (SPF) 100 collection,and the Taku, Zephyr, Vortexand Gale models in theSPF75 series.
SPF100 provides 100percent protection with thepatented Orbital Seal™ eye-cup, and SPF75 delivers 75percent coverage through anethylene vinyl acetate (EVA)foam air dam.
Polarized, photochromicand color-enhancing lensesare available in any framestyle and prices vary depend-ing on lens choice.
“We wanted a name withinstant recognition, a logothat would stand out, adomain name that people
could spell, a name withyouthful energy and atti-tude,” said Bob Hall, Panoptxpresident and CEO.
“We found that combi-nation with the logo and7Eye brand. We want to berecognized as an eye healthbrand that helps consumerssee all seven colors in thespectrum of visible light. By
helping people see the worldin all its colors, we help themdo whatever they want betterand in greater comfort,” saidHall.
“The introduction of7Eye is the beginning of anew platform for productdevelopment,” continuedHall.
“We have new eyecup
technology and new framedesigns due to roll out in2008 that will separate usonce and for all from ourlegion of imitators. We arecreating a solid foundationfor brand expansion and salesgrowth, and with new stylesand new technology in thepipeline, 7Eye will fuel thatgrowth.”
Panoptx launches new logo, models, technology
Shown is Panoptx style Churada.
January.qxp 1/10/2008 3:20 PM Page 21
Fri Jan 11 10:33:02 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_21.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim
22 AOA NEWS
February TBI/ABI (OEP CLINICALCURRICULUM) OPTOMETRICEXTENSION PROGRAMFOUNDATION Feb. 9-11, 2008Baltimore, MD Theresa Krejci800/447 [email protected].
TEXAS OPTOMETRICASSOCIATION 2008 TOAANNUAL CONVENTIONFebruary 14-17, 2008Renaissance Hotel AustinBrigitte Kelly 512/707-2020FAX: 512/[email protected]
HEART OF AMERICA CONTACTLENS AND PRIMARY CARECONGRESS Feb. 15-17, 2008Hyatt Regency Crown Center Hotel,Kansas City, MO www.hoacls.org
OREGON OPTOMETRICPHYSICIANS ASSOCIATION/OPTOMETRIC PHYSICIANS OFWASHINGTON COLUMBIAOPTOMETRY CONFERENCEFeb. 15-17, 2008Vancouver Hilton, Vancouver,Washington Judy Balzer425/455-0874 FAX: 425/646-9646 [email protected]
DELAWARE OPTOMETRICASSOCIATION WINTER THAWCONTINUING EDUCATIONEVENT Feb. 16, 2008Embassy Suites, Newark, DelawareTroy Raber, O.D. 302/[email protected]
SUNY, COLLEGE OF OPTOMETRYSKIVISION Feb. 16-20, 2008Snow Mass, CO, 800/868-4888www.skivision.com
AEA CRUISES OPTOMETRICCRUISE SEMINAR – SouthernCaribbean Explorer February 16-23, Aboard the Crown Princess®888/[email protected]
PRESIDENT’S WEEK 2008Feb. 16-23, or Feb. 17-24, Sunset Jamaica Grande Resort &Spa, Ocho Rios, Jamaica
TROPICAL CE BELIZE 2008Feb. 16-23, 2008Ramon’s Village Resort & SunbreezeBeach Hotel, 281/[email protected]
THE PALM BEACH OPTOMETRICASSOCIATION PALM BEACHWINTER SEMINARFebruary 22-24,2008PGA Resort & Spa, Palm BeachGardens, Florida561/792-9110 www.pbcoa.org
ESSENTIALS OF BEHAVIORALVISION CARE (OEP CLINICALCURRICULUM) Optometric ExtensionProgram Foundation
Feb. 23-24, 2008 Phoenix, AZTheresa Krejci 800/447 [email protected]
THE CODING INSTITUTEOPTOMETRY CODING & BILLINGCONFERENCE February 24-26, Bally’s Las Vegas, NevadaLacy Keith 866/251-3060www.codingconferences.com
AEA CRUISES OPTOMETRICCRUISE SEMINAR PANAMA CANALFebruary 25-March 6, 2008Aboard the Crown Princess®888/[email protected]
SECO INTERNATIONAL 2008February 27-March 2, 2008Georgia World Congress Center,Atlanta, GA www.seco2008.com
BIG SKY 2008 SKI CONFERENCEMONTANA OPTOMETRICASSOCIATION Feb. 28-March 1,2008 Big Sky Ski Resort, Big Sky,Montana, Sue A. Weingartner406/443-1160 FAX: 406/[email protected]
MAINE OPTOMETRICASSOCIATIONMarch “CE & SKI” ConferenceFeb. 29-March 1, 2008, GrandSummit Hotel - Sugarloaf,Carrabassett Valley, MEJoann Gagne, 207/[email protected]
MarchNORTHWEST CONGRESS OFOPTOMETRY OPTOMETRICEXTENSION PROGRAMFOUNDATION March 1-2, 2008Pacific University, Forest Grove, OREric [email protected]
SACRAMENTO VALLEYOPTOMETRIC SOCIETY 20THANNUAL OCULAR SYMPOSIUMMarch 2, 2008Marriott Sacramento RanchoCordova Hotel, Rancho Cordova,California, Jerry Sue Hooper916/[email protected]
22ND ANNUAL EYE SKICONFERENCE March 2-8, 2008Park City, Utah, Tim Kime, O.D.419/475-6181FAX: 419/475-5720www.eyeskiutah.com
NORTH DAKOTA OPTOMETRICASSOCIATION 2008CONTINUING EDUCATION/FIGHTING SIOUX HOCKEYCONFERENCE March 6-8, 2008Holiday Inn, Grand Forks, NorthDakota, Nancy Kopp701/[email protected]
VT/VISUAL DYSFUNCTIONS (OEPCLINICAL CURRICULUM)Optometric Extension ProgramFoundation, March 6-10, 2008Baltimore, MD, Theresa Krejci800/447 [email protected].
ALLEGANY OPTICAL NATIONALOPTOMETRY CONTINUINGEDUCATION LECTURE SERIES VIIIMarch 9, 2008Kepler Theater, HagerstownCommunity College, Hagerstown,Maryland, Debbie Staley, BS301/790-2800, ext. [email protected]
GREAT LAKES CONGRESSOPTOMETRIC EXTENSIONPROGRAM FOUNDATIONMarch 9-10, 2008Renaissance North Shore Hotel,Northbrook, IL, John Loesch, O.D.708/[email protected]
OPTOWEST 2008March 13-16, 2008Long Beach Convention Center, LongBeach, CaliforniaTamalon Littlefield800/877-5738, ext. 228FAX: 916/[email protected]
MARYLAND OPTOMETRICASSOCIATION AND WILMER EYEOPTICAL/JOHNS HOPKINSEVIDENCE BASED CARE INCONTACT LENS, GLAUCOMAAND CORNEA THERAPEUTICSMarch 30, 2008Turner Auditorium on the JohnsHopkins Hospital Campus,Baltimore, MarylandKristen Shoemaker410/727-7800; 410/727-1801FAX: 410/[email protected]
FOUNDATIONS 1(OEP Clinical Curriculum)Optometric Extension ProgramFoundation, March 28-30, 2008San Marcos, CA Theresa Krejci800/447 [email protected].
TROPICAL CE PUNTA CANA, D.R. March 29-April 5, 2008Paradisus Punta Cana –All-inclusive reserve suitesStuart Autry, 281/[email protected]
PENNSYLVANIA OPTOMETRICASSOCIATIONPOA TECHNOLOGYCONFERENCE March 30, 2008Sheraton Harrisburg-Hershey,Harrisburg, PennsylvaniaIlene Sauerteig, 717/[email protected]
AprilNEW JERSEY ACADEMY OFOPTOMETRY GOLF CONFERENCEApril 2-6, 2008 Kingston Plantation,Myrtle Beach, SC, 732/[email protected]
VT/LEARNING RELATED VISUALPROBLEMS (OEP CLINICALCURRICULUM)April 3-7, 2008 (Tentative)Optometric Extension ProgramFoundation, co-sponsored by NOVASoutheastern UniversityFt. Lauderdale, FL. Theresa Krejci800/447 [email protected]
NORAOptometric Extension ProgramFoundationApril 12-13, 2008San Antonio, TXwww.nora.cc
PSS 2008: CONFERENCE ONCOMPREHENSIVE EYECAREApril 12-13, 2008Crowne Plaza Niagara Falls, NY 203/[email protected]
THE OHIO STATE UNIVERSITYBINOCULAR VISION/PEDIATRICSAND CHILDREN’S LEARNINGFORUMSApril 17-18, 2008Columbus, OhioMarjean Taylor Kulp614/[email protected]
ARKANSAS OPTOMETRICASSOCIATIONSPRING CONVENTIONApril 17-19, 2007Embassy Suites, Little Rock, ARJennifer Martinez501/661-7675FAX: 501/372-0233www.arkansasoptometric.org
ORTHOKERATOLOGY ACADEMYOF AMERICA & UNIVERSITY OFHOUSTON, COLLEGE OFOPTOMETRYSECOND ANNUAL RESHAPINGTHE WORLD CONFERENCEApril 17-20, 2008Westin San Diego, CaliforniaCary M. Herzberg, O.D., FOAA866/851-9922www.okglobal.org
MISSOURI OPTOMETRICASSOCIATIONSPRING CEApril 17-22, 2008
St. MaartenJoyce Baker573/[email protected]
UNIVERSITY OF CALIFORNIA,BERKELEY, SCHOOL OFOPTOMETRY 23RD ANNUALMORGAN/SARVER SYMPOSIUMApril 18-20, 2008DoubleTree Hotel, Berkeley Marina, Nyla Marnay510/642-6547 or 800/827-2163FAX: 510/[email protected]
DADE COUNTY OPTOMETRICASSOCIATIONMIAMI NICE EDUCATIONSYMPOSIUMAPRIL 19-20, 2008WESTIN COLONNADE HOTEL,CORAL GABLES, FLORIDA800/808-5018FAX: 772/[email protected]
KANSAS OPTOMETRICASSOCIATIONANNUAL CONVENTIONApril 24-26, 2008Capital Plaza Hotel, Topeka, [email protected]
MOUNTAIN WEST COUNCIL OFOPTOMETRISTSMWCO ANNUAL CONGRESSApril 24-26, 2008Bellagio Hotel, Las Vegas, NevadaTracy Abel888/376-6926 or 503/436-0798FAX: 503/[email protected]
106TH KOA ANNUAL SPRINGCONGRESSKENTUCKY OPTOMETRICASSOCIATIONApril 24-27, 2008Marriott Louisville Downtown Hotel,Louisville, [email protected]
VIRGINIA OPTOMETRICASSOCIATIONVOA VOYAGES IN VISION CECONFERENCEApril 24-27, 2008JW Marriott Cancun Resort, Cancun,MexicoBruce B. Keeney, Sr.804/643-0309www.voaeyedocs.org
THE SEAVISION CONFERENCEApril 24-May 3, 2008Scotland & Ireland
To submit an item for the meetings calendar, send a note to [email protected]
MEETINGS
January.qxp 1/10/2008 3:20 PM Page 22
Fri Jan 11 10:31:28 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_22.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim
January.qxp 1/10/2008 3:22 PM Page 23
Fri Jan 11 10:31:52 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_23.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim
24 AOA NEWS
SHOWCASE
Value Enhancement ServicesAppraisalsPractice Sales & FinancingEmployment & Partnership Agreements
Are you buying or selling a practice?Whether buying or selling, let BlackwellConsulting help facilitate a smooth transaction.We are accredited business appraisers and solution oriented advisors.
Marilee Blackwell, MBA, AIBAmblackwell.com
Call us today at 800.588.9636 to learn what we can do for you.
BLACKWELLC O N S U L T I N G
W E B - B A S E D O P T O M E T R I C S O F T W A R EW E B - B A S E D O P T O M E T R I C S O F T W A R E
800-788-3356 WWW.EYECOM3.COMContact us today for a free demo!
Take your practice to a whole new level with web-based optometric software that is easy to use!
WEB-HOSTING
E-COMMERCE
24/7 REMOTE ACCESS
ELECTRONIC BILLING
PAPERLESS
practicemanagement
software
web-basedVA Boston Healthcare System - Optometrist
“Th VABHCS i ki lifi d“Th VABHCS i ki lifi d“The VABHCS is seeking a qualifiedThe VABHCS is seeking a qualifiedThe VABHCS is seeking a qualifiedThe VABHCS is seeking a qualifiedThe VABHCS is seeking a qualified g qg q O iO iOptometristOptometristOptometristOptometristOptometrist pp hhto serve as theto serve as theto serve as theto serve as theto serve as theCh f f h O SChi f f h O S iChi f f th O t t S tiChief of the Optometry SectionChief of the Optometry SectionChief of the Optometry SectionChief of the Optometry Sectionp yp y Th dThi i di iThi i t t di t itThis is an outstanding opportunityThis is an outstanding opportunity. This is an outstanding opportunity. This is an outstanding opportunityg pp yg pp y
l d bli h d hi hl di d d l if dt l d t bli h d hi hl dit d d ltif t dto lead an established highly accredited and multifaceted programto lead an established highly accredited and multifaceted programto lead an established, highly accredited and multifaceted programto lead an established, highly accredited and multifaceted program., g y p g, g y p gR ibili i i l d h d i i i d i h f iR ibili i i l d h d i i i d i h f iResponsibilities incl de the administration and o ersight of an inteResponsibilities include the administration and oversight of an inte-Responsibilities include the administration and oversight of an inte-Responsibilities include the administration and oversight of an inteResponsibilities include the administration and oversight of an intep gp g
d i i i i d f ft d i it t t ti i d f fgrated six site optometry section comprised of a group of accomgrated six- site optometry section comprised of a group of accom-grated six site optometry section comprised of a group of accomgrated six site optometry section comprised of a group of accomg p y p g pg p y p g pli h d d l d i Thi i i ff i lli h d d t l t d t t i t Thi iti ff ti lplished and talented optometrists This position offers exceptionalplished and talented optometrists This position offers exceptionalplished and talented optometrists This position offers exceptionalplished and talented optometrists. This position offers exceptionalp s ed a d ta e ted opto et sts. s pos t o o e s e cept o ap p p pp p p p
d hi i i i d i ht iti i ti t d ti hopportunities in patient care education researchopportunities in patient care education researchopportunities in patient care, education, researchopportunities in patient care, education, researchpp p , ,pp p , d l h l hd l h l hd t l h lthand telehealthand telehealthand telehealth.and telehealth.P i VA i i ll d d kP i VA ti t i ll d t t d t kPrior VA patient care experience as well as a demonstrated trackPrior VA patient care experience as well as a demonstrated trackPrior VA patient care experience as well as a demonstrated trackPrior VA patient care experience as well as a demonstrated trackp pp p
d i li i l d i d i i id i li i l d i d i i irecord in clinical education administrationrecord in clinical education administrationrecord in clinical education administrationrecord in clinical education, administrationrecord in clinical education, administration, , d h i f dd h i f dand research is preferredand research is preferredand research is preferredand research is preferred.and research is preferred.ppTh Ch f O S d d lTh Chi f O S i d i i di l iTh Chi f O t t S ti d ti i t di tl iThe Chief Optometry Section oversees and participates directly inThe Chief Optometry Section oversees and participates directly inThe Chief, Optometry Section oversees and participates directly inThe Chief, Optometry Section oversees and participates directly in, p y p p yp y p p y
i ll h d i f d idti t ll th d ti f t t t d t id tpatient care as well as the education of optometry students, residentspatient care as well as the education of optometry students, residentspatient care as well as the education of optometry students, residents,p p, p pand fellows. In addition, the Chief supervises the section s professionand fellows. In addition, the Chief supervises the section s professionand fellows In addition the Chief supervises the section s profession-and fellows In addition the Chief supervises the section s profession-and fello s In addition the Chief s per ises the section's professiond f ll I ddi i h Chi f i h i ' f id f ll I ddi i h Chi f i h i ' f i
pp ppp , pal and support staff, monitors implementation of VA clinical andal and support staff, monitors implementation of VA clinical andal and support staff monitors implementation of VA clinical andal and support staff monitors implementation of VA clinical andl d t t ff it i l t ti f VA li i l dl d ff i i l i f VA li i l dAp pp pad st at ve p otoco s as we as V pe o a ce easu es.administrative protocols as well as VA performance measures.administrative protocols as well as VA performance measuresadministrative protocols as well as VA performance measuresadministrative protocols as well as VA performance measuresd i i t ti t l ll VA fd i i i l ll VA f
p p gp p gSuperior leadership and management skills with a commitment toSuperior leadership and management skills with a commitment toSuperior leadership and management skills with a commitment toSuperior leadership and management skills with a commitment toS i l d hi d t kill ith it t tS i l d hi d kill i h iS l d h d k ll hppand passion for excellence are essential attributes. The selected indiand passion for excellence are essential attributes. The selected indiand passion for excellence are essential attributes The selected indi-and passion for excellence are essential attributes The selected indid i f ll ti l tt ib t Th l t d i did i f ll i l ib Th l d i di
q y y ppq y y ppvidual must qualify for faculty appointment at the level of Associatevidual must qualify for faculty appointment at the level of Associatevidual must qualify for faculty appointment at the level of Associatevidual must qualify for faculty appointment at the level of Associatevidual must qualify for faculty appointment at the level of Associateid l lif f f l i h l l f A iid l lif f f l i h l l f A ig g p yg g p yProfessor at the New England College of Optometry.Professor at the New England College of Optometry.Professor at the New England College of OptometryProfessor at the New England College of OptometryP f t th N E l d C ll f O t tP f h N E l d C ll f Of h l d C ll f O
yyInterested candidates should submit electronically a letter of interestInterested candidates should submit electronically a letter of interestInterested candidates should submit electronically a letter of interestInterested candidates should submit electronically a letter of interestInterested candidates should submit electronically a letter of interestI d did h ld b i l i ll l f iI d did h ld b i l i ll l f ippand complete curriculum vitae to and complete curriculum vitae toand complete curriculum vitae toand complete curriculum vitae tod l t i l it td l i l i
Anna Leitao Anna LeitaoAnna LeitaoAnna LeitaoAnna LeitaoA L itA L iHuman Resources Management Service
Equal Opportunity Employer.
For more information contactMontana Optometric Association
406/443.1160 • FAX: 406/443.4614E-MAIL: [email protected] • WEBSITE: www.mteyes.com
36 S. Last Chance Gulch, Suite A • Helena, Montana 59601
MOABIG SKY SKI CONFERENCE
FEBRUARY 28 – MARCH 1, 2008
12 Hours of COPE-approved Credit
FACULTYMurray Fingeret, OD • Jay Haynie, OD
Downhill and Cross-Country Skiing • Dinner Sleigh RidesSnowmobiling/Sno-Coach in Yellowstone Park
Dogsledding • & More
montanamontanaLooking for an opportunity to provide eye care to remote Alaskan villages, while providing full scopecare in a rewarding and challenging position, give the Norton Sound Health Corporation a call.
Provide optometry services as follows:
• Comprehensive examinations• Diagnosis and treatment of eye diseases• Prescription of eyeglasses, contact lenses,
and low vision aids• (same as #2 above)• Education and counseling on contact lens
care and visual hygiene• Removal of foreign bodies from the eye• Emphasis on health promotion and
disease prevention
This position is a unique opportunity to work in a small town setting while having the opportunityto fly to the villages in rural Alaska. You will be given the chance to really make a difference in yourpatient’s life. If you are interested please contact our HR department.
Norton Sound Health CorporationP.O. Box 966
Nome,AK 99762888-559-3311 Toll Free
(907) 443-2085
Qualifications:• Degree in Optometry from an accredited
university• Alaska License• Ability to travel to small villages• Must be able to work with diverse (?)
groups of people
Showcase_January_21_08 1/10/08 1:44 PM Page 24

January 2008 25
SHOWCASE
Vice President for Academic AffairsSouthern College of Optometry is searching for a highly qualified individual to apply for this full-time position. The Vice President for Academic Affairs is responsible for the overall management of the academic programs of the College, the implementation of academic policies and for the development, implementation, and outcomes measurement of the optometric curriculum. The position is responsible for the recruitment, retention and development of faculty. The VPAA works in concert with the Vice President for Clinical Programs regarding the scheduling of didactic and clinical programs, and in the assignment of faculty responsibilities.
The successful candidate must have a record of significant academic achievement, experience in optometric education, proven leadership and demonstrate a successful pattern of mentoring faculty and students. The successful candidate should be a visionary, capable of leading an outstanding academic program to meet the challenges of the future practice of optometry. Individuals must possess the capability to incorporate change in curriculum as needed, while maintaining the standard of excellence in clinical education for which the college is noted. An OD degree is required, with additional advanced degrees preferred. The Vice President for Academic Affairs reports directly to the President of the College.
Southern College of Optometry has a long established reputation for excellence in clinical practice, and attracts outstanding students from throughout the country. This is an outstanding opportunity to help lead a prestigious institution in its effort to prepare men and women for highly successful practices in the art and science of optometry. The Search Committee will review all applications and initiate the interview process in early February 2008. Applications, four letters of reference, curriculum vitae and any supportive materials should be submitted to:
Richard W. Phillips, ODPresident
Southern College of Optometry1245 Madison Avenue, Memphis, TN [email protected]
Southern College of Optometry
is an affirmative action, equal opportunity
employer.
March 2nd - 5th, 2008Harveys Resort & Casino
Featured speakers: Bill Townsend, Featured speakers: Bill Townsend, Jim Colagain, Rhonda RobinsonJim Colagain, Rhonda Robinson
Reserve Your Spot Today! 702-220-7444 • Fax: 702-974-4446 • [email protected]
The Ohio State University College of OptometryAffiliated Residency Programs
2008 - 2009
To build a diverse workforce Ohio State encourages applications from individuals with disabilities, minorities, veterans, and women. EEO/AA employer.
The Ohio State University College of Optometry invitesapplications for its affiliatedone-year residency programs inPrimary Eye Care and OcularDisease. All programs begin
July 1, 2008; and a competitive stipend is offered to attract highly-qualified residency candidates. Applicants should be highly inquisitiveand self-motivated to work with challenging patients and state-of-the-art equipment under the direct supervision of outstanding optometriceducators. For information on any of OSU’s seven accredited programs, please visit our website (www.optometry.osu.edu) or contact theappropriate program’s supervisor:
Chillicothe/Columbus VA.... Dr. Brian Montgomery ([email protected]) orDr. Andrew Weibel ([email protected])
Cleveland VA.........................Dr. Stacia Yaniglos ([email protected])
Dayton VA .............................Dr. Gregory Kiracofe ([email protected])
Hampton VA .........................Dr. Gay Tokumaru([email protected])
Cincinnati Eye Institute .......Dr. Kevin Corcoran ([email protected])
Eye Center of Toledo............Dr. David Bejot ([email protected])
Ohio Eye Alliance .................Dr. Scott Young ([email protected])
Announcement ofVA Optometry Residency
Openings 2008-2009Northport VA Medical Center, LongIsland, NY announces the availability of four optometric residency positions.The Residency Program is under theguidance of the Northport VA staff & is affiliated with SUNY State College ofOptometry. The uniqueness of theResidency Program is that the residentswill receive extensive didactic/clinicaltraining & exp in three major areas: (1) Primary Care, including the diagnosis& treatment of all ocular diseases, (2) Rehabilitative Optometry, inc mgmt of head trauma, stroke, vestibular &binocular problems, & (3) Low VisionRehab. Residents will also rotatethrough various clinics within the Med Ctr.
This program begins in July 2008.Please submit apps through ORMS by 2/1/08. Additionally, the followingmaterials need to be submitted directlyto the Residency Program Supervisor:complete curriculum vitae w/ letter ofinterest, optometry school transcripts,National Board scores, three letters of recommendation, & copies of anystate licenses, if obtained. Approxstipend: $32,800.
SEND MATERIALS TO:
Michael McGovern, O.D., F.A.A.O.,Residency Program Supervisor,
Optometry Service (123), Department of Veterans Affairs,
Medical Center, Northport, NY 11768.Email: [email protected]
EOE
V i s i t t h eA O A
W e b s i t ea t
w w w . a o a . o r g
Showcase_January_21_08 1/10/08 1:44 PM Page 25
26 AOA NEWS
SHOWCASE
State University of New YorkState College of Optometry
WWW.MWCO.ORG
Bellagio Hotel Las Vegas
For Bellagio Hotel reservations & informationcall 888-987-8686
Please mention you are with the MWCO conference to receive special room rate.
Information:please contact Tracy Abel at 888-376-6926
or email [email protected]
MWCO008
Mountain West Council of Optometrists
THE STRENGTH TO HEALTHE STRENGTH TO HEAL
our nation’s defenders.
As an optometrist and Offi cer on the U.S. Army Health Care Team, your responsibilities will include caring for Soldiers when they need it most. You’ll work alongside dedicated professionals in a collaborative environment. You’ll utilize the most advanced technology and enjoy the resources of one of the most comprehensive health care organizations in the world. You’ll make a difference.
To learn more about the U.S. Army Health Care Team, call 888-216-9285 or visit healthcare.goarmy.com/info/optra.
©2007. Paid for by the United States Army. All rights reserved.
A Nonprofit Corporation Dedicated To Research in Photoretinogy
The Therapeutic Application of Light To The Visual System
76th International Conference on Light & VisionPhoenix, Arizona
Dates: May 1-4, 2008Embassy Suites Hotel
Phoenix – NorthContact: Ron Wahlmeier
Phone: (866)486-0190e-mail: [email protected]
website: www.syntonicphototherapy.com
COLLEGE OF SYNTONIC OPTOMETRY
Showcase_January_21_08 1/10/08 1:44 PM Page 26

January 2008 27
SHOWCASE
The Cornea and Laser Eye Institute – Hersh Vision Group in Teaneck,New Jersey is seeking an optometrist with interest in refractive surgerypatient management and specialty contact lens fitting.
The Cornea and Laser Eye Institute is a nationally recognized practicededicated to clinical care, research, and teaching in corneal diseasesand refractive surgery. With the complete range of corneal diagnostictools and surgical instrumentation, the Cornea and Laser Eye Instituteoffers patients access to years of specialized experience, advancedtechnologies, and treatment alternatives, and offers the practitioner anopportunity to participate in and expand a unique subspecialty practice.
In addition to direct clinical care, CLEI participates in a number ofnationwide clinical trials, including refractive surgery, device, drug, andcontact lens studies. Complementing these efforts are active researchprograms in collaboration with UMDNJ-New Jersey Medical School andPrinceton University.
We currently have an opening for a full-time optometrist. Candidatesmust have earned a Doctor of Optometry degree from an accredited col-lege or school of optometry and possess a current New Jersey license.The position entails pre and postoperative care of refractive surgerypatients (LASIK, PRK/LASEK, CK and Intacs), specialty contact lens fit-ting (postops, keratoconus), and clinical research opportunities. This isa unique subspecialty career position. Fellowship opportunities alsoconsidered. Some Saturdays and evenings required. Salary commen-surate to training and experience.
Please send CV and letter of interest to:
Stacey Lazar, General Managerslazar@vision- inst i tute .com
info@vision- inst i tute .comFax – 201-692-9646
CORNEA AND LASER EYE INSTITUTE - OPTOMETRIST
The New England Eye Institute (NEEI), the clinical system of the New England College of Optometry (NECO), invites applications for professional staff members to serve as attending optometrists and clinicianeducators within NEEI’s community health center network locations.
Our mission is to improve the visual health of populations through excellencein collaborative and community-oriented patient care, service, education, andresearch. A NEEI optometrist is a highly qualified doctor of optometry andclinician-educator who works within a dynamic team-oriented, multidiscipli-nary non-profit eye care network serving the visual health needs of populationsin greater Boston. NEEI attending optometrists also receive adjunct teachingappointments with NECO and thus will have opportunity to advance both ourservice and teaching mission.
Network opportunities are now available at our community health center affili-ates. Required qualifications include an OD degree, advanced professionalcredentials such as residency training or equivalent clinical experience, eligibili-ty to be licensed in Massachusetts and an active commitment to excellence inpatient care and teaching.
We offer a very competitive salary and benefit package. Start dates for theseappointments will vary, ranging from March 1, 2008 – July 1, 2008.Applicants should submit a letter of application and curriculum vitae byFebruary 1, 2008 to:
Roger Wilson, O.D. Vice President, Health Center Programs New England Eye Institute
940 Commonwealth Avenue, Suite 2Boston, MA 02215-1203
617.587.5511 ext. [email protected]
www.newenglandeye.org
New England EyeInstitute Invites Applications forProfessional Staff Appointments
WWe want you to enjoy the natural beauty ofe want you to enjoy the natural beauty ofGrand TGrand Teton and Yeton and Yellowstone National Parks.ellowstone National Parks.
So after an excellent day of continuing education,So after an excellent day of continuing education,please “please “ hit the rhit the r oa doa d” to the most beautiful place on earth.” to the most beautiful place on earth.
Speakers:Speakers:
For more information about our18 hour doctor program, exhibits,
and paraoptometric program, inbeautiful Jackson Hole, Wyoming
please contact us at:
Northern RockiesNorthern RockiesOptometric ConferenceOptometric Conference
716 Randall Ave., Cheyenne, W Y 82001Ph: 307/637-7575
Fax: 307/638-8472www.NROCmeeting.com
“ Hit The Road – Pal ”“ Hit The Road – Pal ”
Dr. Mark AndreDr. Mark AndreDr. Ian GaddieDr. Ian Gaddie
Dr. Gary OliverDr. Gary OliverDr. Mark DunbarDr. Mark Dunbar
scheduled for July 17-19, 2008
k
Showcase_January_21_08 1/10/08 1:44 PM Page 27
28 AOA NEWS
SHOWCASE
Earn Cope-approved Continuing Education credits while sailing on luxurious ships to yourchoice of destinations. Let our 10+ years of experience make your seminar and cruise experi-ence educational, as well as enjoyable, for you, your family and friends.
Southern Caribbean Explorer, 2/16/08-2/23/08, Crown Princess®. San Juan, St. Thomas, St.Kitts, Granada, Bonaire (Netherland Antilles), Aruba, San Juan. Cruise fares from $899.**President’s Day** Speaker: Dr. Christine Sindt
Panama Canal, 2/25/08-3/6/08, Coral Princess®. Ft. Lauderdale, Aruba, Cartagena, PanamaCanal, Costa Rica, Ocho Rios, Ft. Lauderdale. Cruise fares from $1499. Speaker: Dr. TimothyMcMahon.
Greek Isles, 6/5/08-6/17/08, Emerald Princess®. Venice, Dubrovnik, Corfu, Katakolon, Athens,Mykonos, Kusadasi, Rhodes, Santorini, Naples/Capri, Rome(Civitavecchia). Cruise fares from$1245. Speaker: Dr. Harue Marsden
Alaska, 6/29/08-7/6/08, Star Princess®. Seattle, Ketchikan, Tracy Arm Fjord, Juneau, Skagway,Victoria, Seattle. Cruise fares from $1049. ***Follows the AOA Congress in Seattle 6/25-6/29/08*** ~July 4th!~ Speakers: Dr Louise Sclafani and Dr. Paul Karpecki.
British Isles, 7/1/08-7/13/08, Grand Princess®. London (Southampton), Guernsey, Cork,Dublin, Liverpool, Belfast, Glasgow, Inverness/Loch Ness, Edinburgh, Paris/Normandy, London(Southampton). Cruise fares from $1207. Speaker: Dr. Robert Wooldridge.
Holy Land, 11/4/08-11/16/08, Pacific Princess®. Rome (Civitavecchia), Sorrento/Capri,Alexandria, Port Said, Jerusalem, Galilee/Nazareth, Kusadasi, Patmos, Santorini, Athens.Cruise fares from $2890 (oceanview).
Eastern Caribbean, 1/25/09-2/1/09, Crown Princess®. Ft. Lauderdale, Princess Cays, St.Maarten, St. Thomas, Grand Turk, Ft. Lauderdale. Cruise fares from $659.
Classic Southern Caribbean, 2/15/09-2/22/09, Caribbean Princess®. San Juan, Barbados, St.Lucia, Antigua, Tortola, St. Thomas, San Juan. Cruise fares from $909.**President’s Day** Speakers: Janet Betchkal & Rick Bendel
Fares are cruise only, per person, USD, based on double occupancy, capacity controlled and subject to availability. Government fees and taxes are additional. © 2006 Princess Cruises. Ships of Bermudan Registry
© 2006 Silversea Cruises. Ship registry: Bahamas
AEA Cruises: Dr. Mark Rosanova, President
More than a travel agent, your colleague & innovative partner in Cruise Seminars since 1995.Sponsored by the Illinois Optometric Association and Advanced Eyecare Associates 10-12 hoursof COPE approved lectures per seminar
Visit us at www.optometriccruiseseminars.com,
email [email protected] call us at 1-888-638-6009
AEA Optometric Cruise Seminars 2008-2009
April 2 – 6, 2008at Hilton Embassy Suites at Kingston Plantation • Myrtle Beach, SC
3 Rounds of Golf at Myrtle Beach Premier Golf Courses
• SHAFTSBURY GLENN • TIDEWATER • LEGENDS HEATHLANDSaturday Night Awards Banquet with Door Prizes
REGISTRATION 16 HOURS COPE CE One and Two Bedroom Lodges$850 Jimmy Bartlett, O.D., F.A.A.O. Accomodations Include:
Golfing Non O.D. $475 Jeff Gerson, O.D., F.A.A.O. Daily Breakfast Buffet,NonGolfing O.D. $450 Evening Cocktail Reception,
Hilton Honors Points and Miles,
**16 C.O.P.E. Approved Hours**
GOLF CONFERENCE
GOLF CONERENCE
NEW JERSEY CHAPTER
American Academy of Optometry
Registration includes all CE, Golfing,Carts and Greens Fees, and Banquet
For Accomodations and additional information please call: Dennis H. Lyons, O.D., F.A.A.O.Phone: 732-920-0110 FAX: 732-920-7881 E-MAIL; [email protected]
Early B
ird
Rates u
ntil
12/31/07THE EYE CENTERAT SOUTHERN COLLEGE OF OPTOMETRY
The Eye Center at SCO has faculty positions available for clinicians in various disciplines. While our greatest need for clinicians is in the primary care area, those with interests in other areas are also encouraged to apply. The successful candi-date will have excellent clinical skills, leadership abilities and a high degree of intellectual curiosity. Additional skills such as classroom education and clinical research are also desirable.
The position requires a Doctor of Optometry degree with full scope licensure in Tennessee (or eligibility for such licensure.) An advanced degree and/or residency training are highly desirable.
Salary is commensurate with level of education, training and experience.
Please submit CV/supporting materials to:Robin Drescher, O.D.Interim Director for Academic AffairsSouthern College of Optometry1245 Madison AvenueMemphis, Tennessee 38104-2222(901) 722-3234Email: [email protected] online: www.sco.edu/faculty/apply
SCO is an equal opportunity, affirmative action employer and encourages women and members of racial or ethnic minorities to enter into candidacy for this position.
Showcase_January_21_08 1/10/08 1:44 PM Page 28
January 2008 29
SHOWCASE
Western University of Health Sciences is a thriving center for health care and veterinary education.
Western University www.westernu.edu is headquarters to five colleges – Allied Health, Graduate Nursing,Osteopathic Medicine, Pharmacy and Veterinary Medicine.
The University’s core values have propelled the University to impeccable levels of excellence.
The University values a diverse institutional community and is committed to unparalled excellence in itsfaculty, staff and students. Western University seeks applicants of distinguished academic and administra-tive accomplishments who possess a passion for excellence and can illustrate a proven track record ofachievements.
The University is embarking on a new journey, adding another four graduate colleges at the same time by2009 – Dentistry, Optometry, Podiatry and the Graduate College of Biomedical Sciences.
Chief of Pediatric Optometry / Chief of Neuro-Optometric Rehabilitation
The Western University of Health Sciences College of Optometry seeks two clinical faculty with specialexpertise in Pediatric Optometry and in Neuro-Optometric Rehabilitation. Successful candidates will have a history of achievement in patient care within their area of specialty and experience in optometriceducation. Essential functions include direct patient care, supervision of students and residents while providing patient care in the area of specialty, administration of the specialty service at the on-campus clinic, practice development and promotion, community service, supervising and mentoring faculty andstaff, and lecturing. A track record of scholarly accomplishments and successful practice building arerequired. Demonstrated entrepreneurship and leadership abilities are highly desired. Faculty rank will be commensurate with experience. Salary and benefits are competitive. Requirements include the abilityto obtain California licensure within one year of appointment.
Applicants should submit the following to Daniel Kurtz, PhD, OD, Associate Dean of Academic Affairs ,Western University College of Optometry, 309 E. Second St., Pomona, CA 91766-1854 <[email protected]>:
1. a current curriculum vitae2. a cover letter explaining how the applicant’s background meets the requirements of this position.
This letter may include a brief statement including examples of teaching experience, philosophy,and goals. Please include your contact information.
3. a completed Employment Application found at http://www.westernu.edu/bin/hr/pdf/application_for_employment.pdf
Positions are open until filled.Western University of Health Sciences is an equal opportunity employer.
WESTERN UNIVERSITY OF HEALTH SCIENCESCOLLEGE OF OPTOMETRY
Showcase_January_21_08 1/10/08 1:44 PM Page 29

30 AOA NEWS
CLASSIFIEDS
Professional Opportunities
ALL STATES-PRACTICES FORSALE plus 100% FINANCINGLargest database of qualifiedBuyers. Confidentiality main-tained. Seller receives free consul-tation. Advertising/Marketing. 888-277-6633. Visit www.promed-financial.com.
ASSOCIATESHIP POSITIONSCurrently available in California,Florida, Michigan, New York,Texas, etc. More to come.Request info from [email protected] or call 888-277-6633.
BUYING or SELLING? A NEWVISION IN PRACTICE SALES.Practice Concepts specializes inpractice sales for eyecare pro-fessionals. Led by Alissa Wald,O.D. and Scott Daniels, ournationwide team combines over75 yrs experience in finance,management and hands onpractice ownership. We’re inpractice to advance your prac-tice™. For more information andcurrent listings visit www.practiceconcepts.com or call877-778-2020.
California – OD’s needed to helpservice nursing home population.Active Medicare and Medi-Calproviders with TPA licensureonly. Please send resume [email protected].
Central Maine. Busy multi OD/MD surgical practice has immed.opening for full and part time OD’sfor clinics. State of the art equip-ment Reliance Haag Streit, digitalfundus and fluroscein, EMR,Stratus OCT, NIDEK Lasik, largeoptical shop and lab. Well staffedwith trained techs. Salary, Bonus,401k Medical. Voted top ten bestplaces to raise a family in the US.EMAIL CV TO: [email protected]
COLORADO. Practice for sale. Apremier well-established practicegrossing $1,700,000+ annuallyproviding full scope of serviceswith a medical emphasis. Highlydesirable community. State of theart equipment. Up to 100%financing available. 800-416-2055
New Hampshire- Practice forsale. Grossing $330,000, netting$150,000+ annually on 32 OD-Hours/week. Primary care andcontact lens practice located in agreat community. Retiring seller isavailable for transition assistance.100% Financing. 800-416-2055
New Hampshire, Nashua. 40Miles North of Boston. Estab-lished full scope practice seeksFull or P/T O.D. Great staff andequipment including OPTOS.Excellent earnings potential/bene-fits. Fax C.V. to 603.888.1621 orEmail [email protected]
Ohio-Hamilton County. Practicefor Sale. Grossing $800,000,Netting $300,000+ annually on 4.5OD days. Long established, fullyequipped. 100% FinancingAvailable. Call 800-416-2055
Optometrist Needed –Syracuse, NYEmpire Vision Center is seeking afull time or part time doctor. Alongwith an excellent compensationand a monthly incentive program,fulltime offers comprehensivebenefits to include major medical,dental, 401K with employer %match, CE, malpractice, paid vaca-tion benefit plus more. Part timeposition offers partial benefits.Contact Tom Ferris, VPProfessional Services toll free at 1-877-446-3145, extension 7599 ore-mail [email protected]
OPTOMETRISTS NEEDEDNATIONALLY
LasikPlus has excellent opportuni-ties for highly motivated and com-mitted professionals seeking toenhance their career! We’re cur-rently looking for Optometristsand Center Directors in the follow-ing locations:
1. Jacksonville, FL2. Oklahoma City & Tulsa, OK3. Raleigh, NC4. San Antonio, TX5. Other locations Nationwide
We offer a competitive salary andbenefits package. To become partof our exciting team please reply to:
www.lasikplus.com Email: [email protected]
PHONE : 1-866-763-3030FAX: 513-792-5626
OPTOMETRY SPACE IN NJSMITTY’S – NEW space in 40KSF supermarket located in full-service shopping center to sub-lease to optometrist. Located inSmithville10 miles N of AtlanticCity. Tenant improvement allow-ance. Contact Bob Jackey: [email protected] or 609-748-0707.
Pharma Sales Established phar-ma/device co. seeks independentreps for territories throughout theU.S. Non-competing lines ok.Excellent commission and leadreferrals. Trade show travel andexpenses paid. Consult www.ocu-soft.com Send resumes in confi-dence to: Mary Harris; email:[email protected].
ST. LOUIS, MO. - FULL TIME OP-TOMETRIST. Full time Optom-etrist needed for private practice inSt. Louis. Highly progressive prac-tice, state-of-the -art equipment,full scope eye care. Great benefitpackage and great salary. Pleaseforward CV and inquire via e-mailto: [email protected]
South Carolina Coast- Beautiful,historic Charleston. Busy 2 day/wk practice grossing $150,000.Selling for $75,000. Option forbuilding purchase. Email [email protected] or 843-345-1259
SOUTHWEST VIRGINIAOur 5 location group practicewants a long term relationshipwith an energetic, hard working,personable OD for our busyChristiansburg, VA office.Purchase Opportunity in severalyears. See AOA PlacementService for more information.Email [email protected]
Virginia- Private practice lookingfor an associate to join us.Gorgeous Charlottesville, nearthe University of Virginia.Modern, clean office environ-ments with new instrumenta-tion. No evenings, Sundays, orholidays. Limited Saturdays.Great pay & benefits. www.Char lot tesv i l leEyecare.comContact: [email protected] or call (434) 977-2020.
Miscellaneous
ALL LOANS for PRACTICESUnsecured Working Capital,Acquisition, Debt consolidation,Equipment, Expansion, Realestate, Start up. Up to 100% avail-able. Call 888-277-6633 or visitwww.promed-financial.com.
ALL STATES - PRACTICEOPPORTUNITIES: ownership ataffordable investment. Work in amore peaceful surround. Call Erickat 240 592 7960
DO YOU WANT TO HELP CHILDREN? 1 out of 4 childrenstruggle with vision problemsthat interfere with reading andlearning. Detection and treatmentof these vision problems could beyour niche. Learn more aboutmaking vision therapy a profitableservice in your practice. Call todayto schedule a free consultationwith Toni Bristol at ExpansionConsultants, Inc., specializing inVision Therapy practice manage-ment and marketing since 1988.Toll free 877/248-3823.
FILL YOUR OLD TRIAL SETSAssorted wire rimmed trial lensesfor sale in + or - spheres and + or- cylinders. $20 for each trial lens -includes shipping. Call (262) 989-0014 for power availability.
I NEED FRAMES, temples,bridges stamped 1/10th 12kG.F.(gold filled). New, old stock, orUsed. Full, Semi, or Rimlessstyles. Contact GF Specialties,Ltd. 800/351-6926.
Interested in the best systematicapproach to Vision Therapy?OEP Clinical Curriculum Coursescan help you no matter where youare in our career. Call 800 447 0370.
V O S H - I N T E R N AT I O N A LNEEDS YOUR OUTDATEDEQUIPMENT!!How would you like to donateyour outdated equipment to aworthy cause and receive a taxdeduction at the same time?VOSH-INTERNATIONAL with thesupport of WCO and UNESCOhas embarked on a program ofequipment-technology transfer tofledgling Optometry programs inSouth America and Africa. This isbeing done with a new partnerIMEC (International MedicalEquipment Collaborative); a non-profit 501c3 that gathers, servic-es, cleans and packages entireeye clinics, hospitals and othermedical facilities and ships themto an organization that gives thema second life.
Please look through yourgarage, closets, basement for allyour unused books, equipment,instruments, stock frames andlenses and any items that mightbe of use to a Optometry school,a student or eye clinic.Instructions on how to proceedare available by going to theVOSH website (www.vosh.org)and click on Technology TransferProgram. Information about IMECis available at www.imecamerica.
The most desirable items thatprograms in developing countriesneed are: Trial lens kits, batterypowered hand scopes, assortedpliers and optical tools, handstones for edging glass lenses,uncut lenses (both SV and BF),manual lensometers, phoropters,lens clocks, color vision tests, ker-atometers and biomicroscopes.
This list is certainly not com-plete but gives an idea of some ofthe basic needs these developingprograms can benefit from. Allitems may be shipped directly to:VOSH INTERNATIONALC/O IMEC1600 Osgood StreetNorth Andover, Mass. 01845
Assistance with shipping costmay be available through yourlocal Rotary or Lions Clubs.Contact www.vosh.org with anyquestions or email [email protected] and [email protected].
Equipment for Sale
Davis, CA: Complete set of dis-pensary furniture in excellentcondition, includes displays for1000 frames, three dispensingtables and mirrors. Fully furnishyour new or second office inex-pensively. Contact Joann @ 530-758-2122.
Classified Advertising InformationEffective the October 9, 2006 issue onwards, Classified advertising rates are are as follows: 1 column inch = $50 (40 words maximum) 2 column inches - $100 (80 words maximum) 3 column inches = $150 (120 words maximum). This includes the placement of your advertisement in the classified section of the AOA Member Web site for two weeks. An AOA box number charge is $30.00 and includes mailing of responses. The envelope will be forwarded, unopened, to the party who placed the advertisement. Classifieds are not commissionable. All advertising copy must be received by e-mail at [email protected] or by fax at 212.633.3820 attention Keida Spurlock, Classified Advertising. You can also mail the ads to Elsevier, 360 Park Avenue South, 9th floor, New York, NY 10010.
Advertisements may not be placed by telephone. Advertisements must be submitted at least 30 days preceding the publication. All ad placements must be confirmed by the AOA – do not assume your ad is running unless it has been confirmed. Cancellations and/or changes MUST be made prior to the closing date and must be made in writing and confirmed by the AOA. No phone cancellations will be accepted. Advertisements of a “personal” nature are not accepted. The AOA NEWS publishes 18 times per year(one issue only in January, June, July, August, November, and December, all other months, two issues.) and posting on the Web site will coincide with the AOA NEWS publication dates. Call Keida Spurlock - Elsevier ad sales contact - at 212.633.3986 for advertising rates for all classifieds and showcase ads.
Showcase_January_21_08 1/10/08 1:44 PM Page 30
January.qxp 1/10/2008 3:23 PM Page 31
Fri Jan 11 10:32:16 EST 2008Trim Size = 10.875 X 14.375
RIGHT HAND PAGE-------->
AOAN 46-9 AOAN_31.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim
January.qxp 1/10/2008 3:25 PM Page 32
Fri Jan 11 10:31:35 EST 2008Trim Size = 10.875 X 14.375
<------LEFT HAND PAGE
AOAN 46-9 AOAN_32.pdf
blac
kyel
low
mag
enta
cyan
TrimBleed
.125 from trim