riparazione per rigenerazione e...
TRANSCRIPT
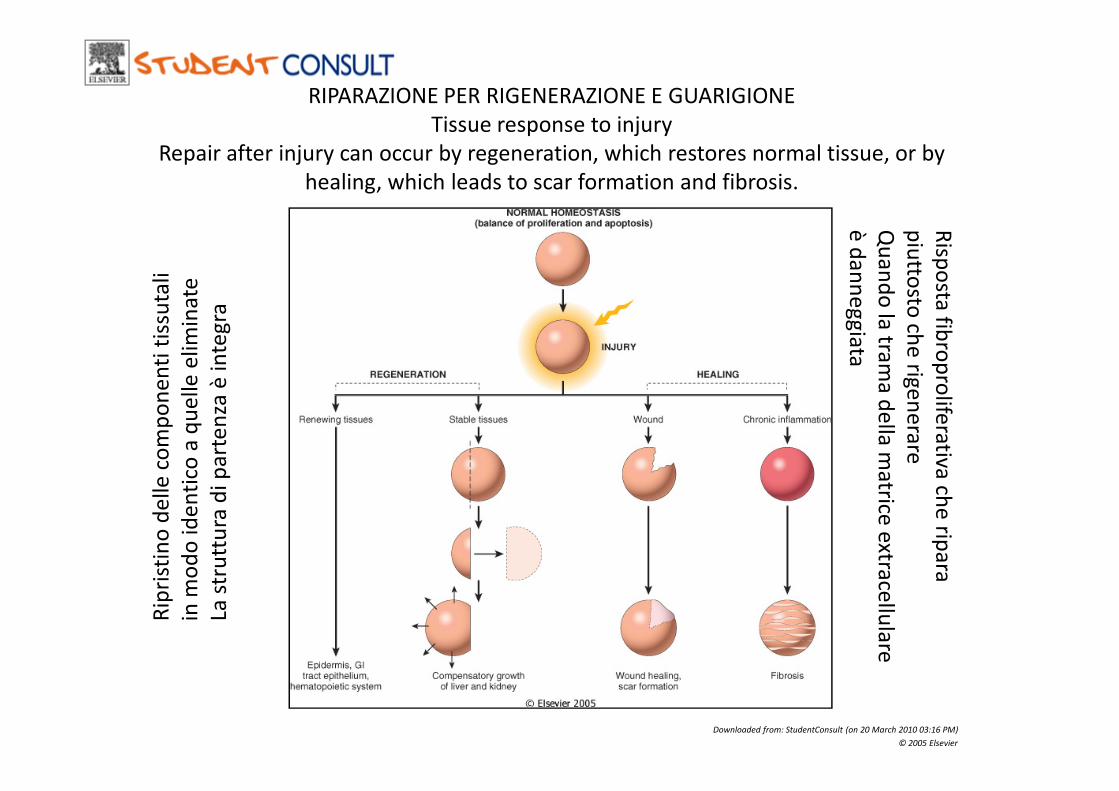
RIPARAZIONE PER RIGENERAZIONE E GUARIGIONE
Tissue response to injury
Repair after injury can occur by regeneration, which restores normal tissue, or by
healing, which leads to scar formation and fibrosis.R
ipri
stin
o d
ell
e c
om
po
ne
nti
tis
suta
li
in m
od
o i
de
nti
co a
qu
ell
e e
lim
ina
te
La s
tru
ttu
ra d
i p
art
en
za è
in
teg
ra
Risp
osta
fibro
pro
lifera
tiva
piu
ttosto
che
rige
ne
rare
Qu
an
do
la tra
ma
de
lla m
atrice
extra
cellu
lare
è d
an
ne
gg
iata
Downloaded from: StudentConsult (on 20 March 2010 03:16 PM)
© 2005 Elsevier
Rip
rist
ino
de
lle
co
mp
on
en
ti t
issu
tali
in m
od
o i
de
nti
co a
qu
ell
e e
lim
ina
te
La s
tru
ttu
ra d
i p
art
en
za è
in
teg
ra
fibro
pro
lifera
tivach
e rip
ara
piu
ttosto
che
rige
ne
rare
Qu
an
do
la tra
ma
de
lla m
atrice
extra
cellu
lare
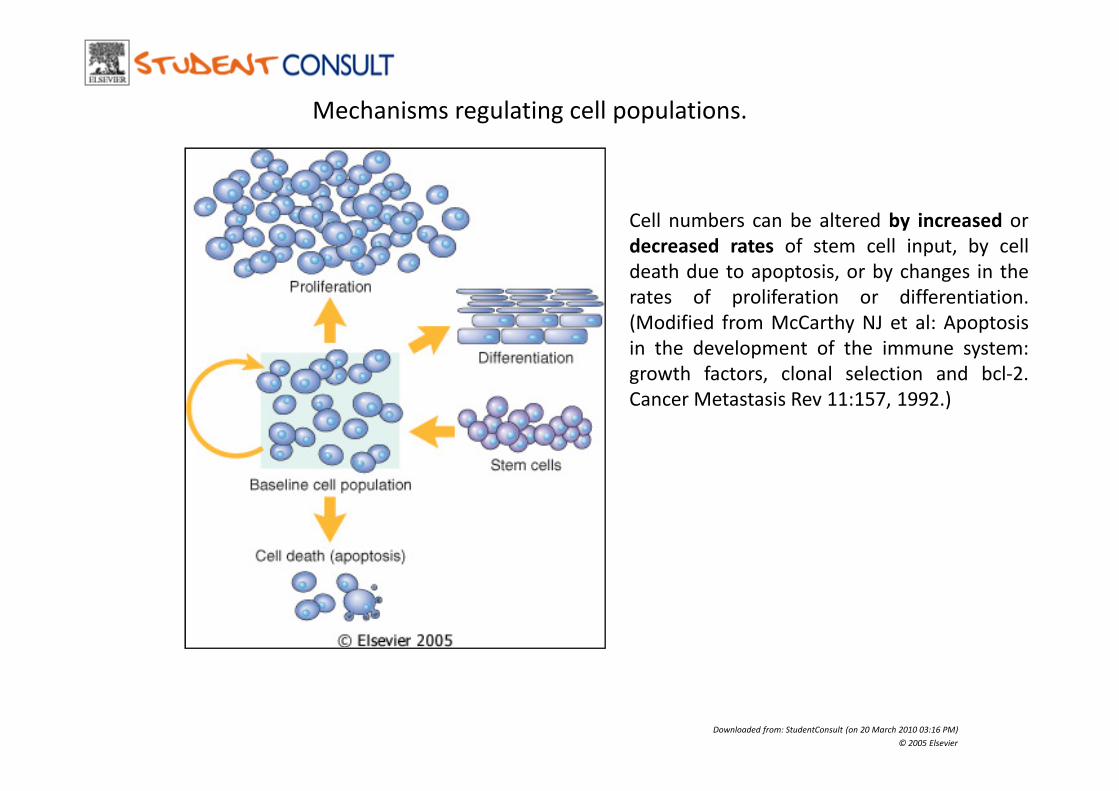
Cell numbers can be altered by increased or
decreased rates of stem cell input, by cell
death due to apoptosis, or by changes in the
rates of proliferation or differentiation.
(Modified from McCarthy NJ et al: Apoptosis
in the development of the immune system:
growth factors, clonal selection and bcl-2.
Cancer Metastasis Rev 11:157, 1992.)
Mechanisms regulating cell populations.
Cancer Metastasis Rev 11:157, 1992.)
Downloaded from: StudentConsult (on 20 March 2010 03:16 PM)
© 2005 Elsevier

Cell-cycle landmarks
Downloaded from: StudentConsult (on 20 March 2010 03:16 PM)
© 2005 Elsevier
The figure shows the cell-cycle phases (G0, G1,G2, S, and M), the location of the G1
restriction point, and the G1/S and G2/M cell-cycle checkpoints. Cells from labile
tissues such as the epidermis and the gastrointestinal tract may cycle continuously;
stable cells such as hepatocytes are quiescent but can enter the cell cycle;
permanent cells such as neurons and cardiac myocytes have lost the capacity to
proliferate. (Modified from Pollard TD and Earnshaw WC: Cell Biology. Philadelphia,
Saunders, 2002.)
LESIONELESIONE
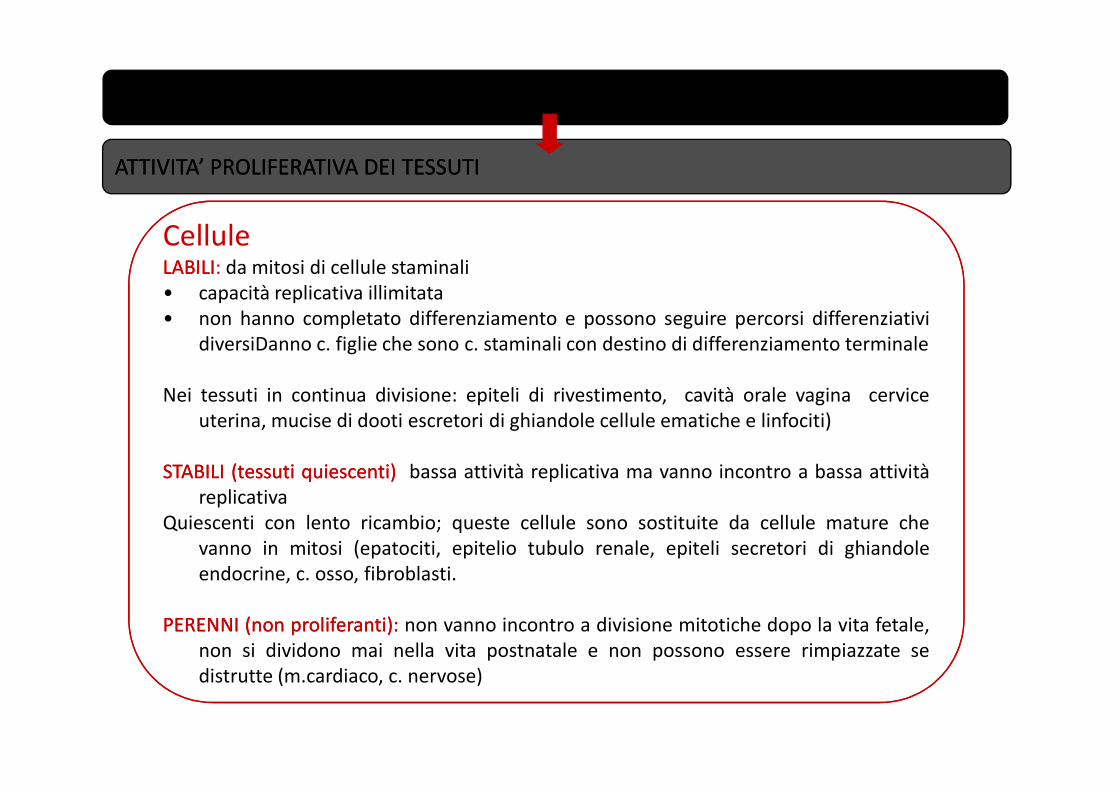
ATTIVITA’ PROLIFERATIVA DEI TESSUTIATTIVITA’ PROLIFERATIVA DEI TESSUTI
CelluleLABILILABILI: da mitosi di cellule staminali
• capacità replicativa illimitata
• non hanno completato differenziamento e possono seguire percorsi differenziativi
diversiDanno c. figlie che sono c. staminali con destino di differenziamento terminale
Nei tessuti in continua divisione: epiteli di rivestimento, cavità orale vagina cerviceNei tessuti in continua divisione: epiteli di rivestimento, cavità orale vagina cervice
uterina, mucise di dooti escretori di ghiandole cellule ematiche e linfociti)
STABILISTABILI (tessuti(tessuti quiescenti)quiescenti) bassa attività replicativa ma vanno incontro a bassa attività
replicativa
Quiescenti con lento ricambio; queste cellule sono sostituite da cellule mature che
vanno in mitosi (epatociti, epitelio tubulo renale, epiteli secretori di ghiandole
endocrine, c. osso, fibroblasti.
PERENNIPERENNI (non(non proliferanti)proliferanti):: non vanno incontro a divisione mitotiche dopo la vita fetale,
non si dividono mai nella vita postnatale e non possono essere rimpiazzate se
distrutte (m.cardiaco, c. nervose)
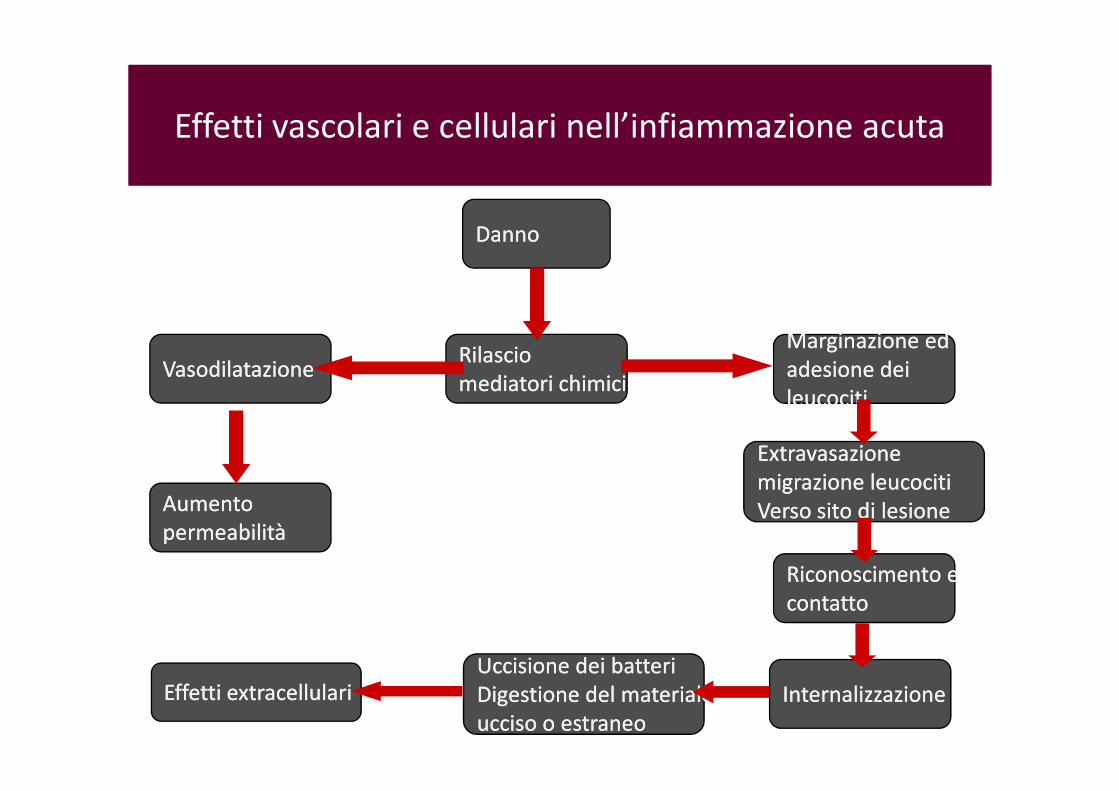
DannoDanno
RilascioRilascio
mediatori chimicimediatori chimiciVasodilatazioneVasodilatazione
Marginazione ed Marginazione ed
adesione deiadesione dei
leucocitileucociti
Effetti vascolari e cellulari nell’infiammazione acuta
mediatori chimicimediatori chimici
Effetti extracellulariEffetti extracellulari
AumentoAumento
permeabilitàpermeabilità
leucocitileucociti
ExtravasazioneExtravasazione
migrazione leucocitimigrazione leucociti
Verso sito di lesioneVerso sito di lesione
Riconoscimento e Riconoscimento e
contattocontatto
InternalizzazioneInternalizzazione
Uccisione dei batteriUccisione dei batteri
Digestione del materiale Digestione del materiale
ucciso o estraneoucciso o estraneo
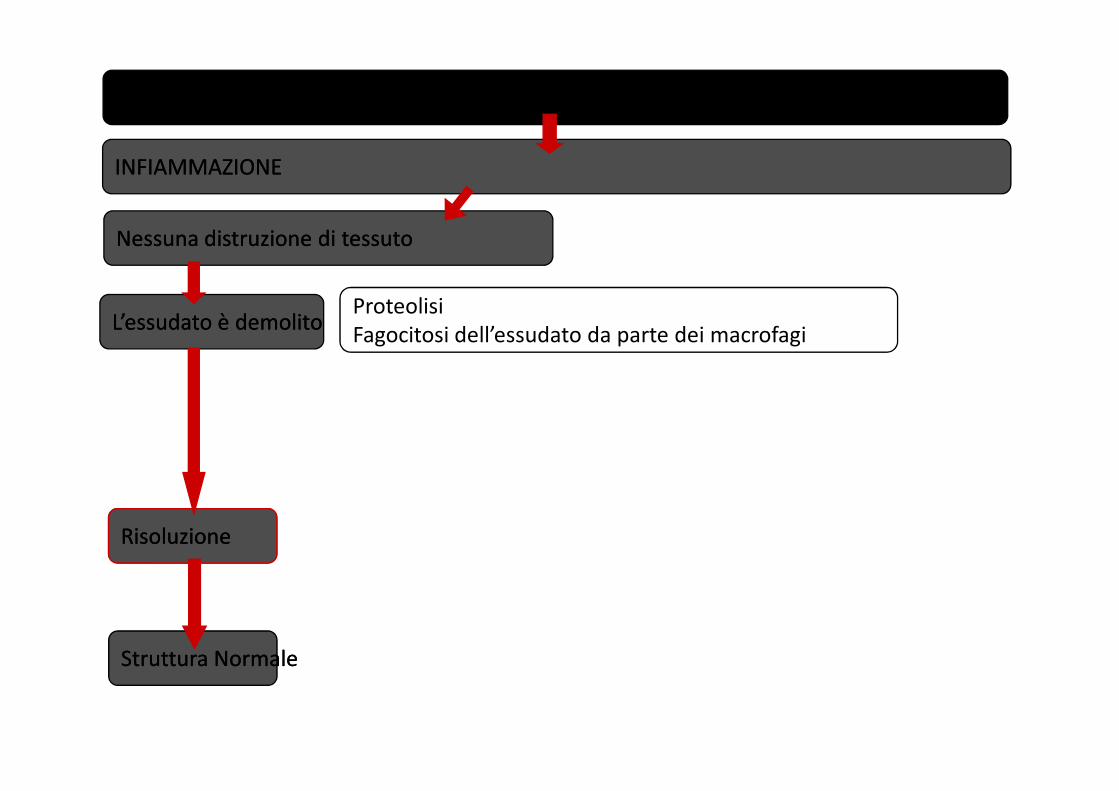
LESIONELESIONE
INFIAMMAZIONEINFIAMMAZIONE
Nessuna distruzione di tessutoNessuna distruzione di tessuto
L’essudato è demolitoL’essudato è demolitoProteolisi
Fagocitosi dell’essudato da parte dei macrofagi
RisoluzioneRisoluzione
Struttura NormaleStruttura Normale
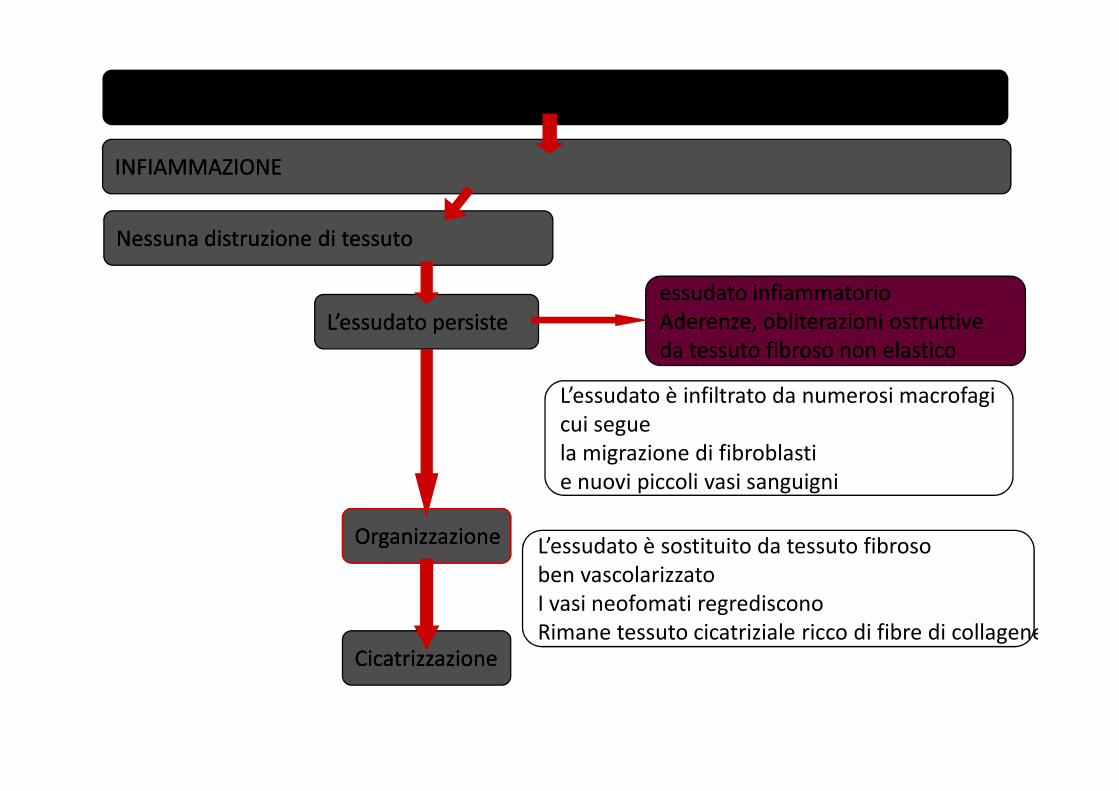
LESIONELESIONE
INFIAMMAZIONEINFIAMMAZIONE
Nessuna distruzione di tessutoNessuna distruzione di tessuto
L’essudato persisteL’essudato persiste
L’essudato è infiltrato da numerosi macrofagi
essudato infiammatorioessudato infiammatorio
Aderenze, obliterazioni ostruttive Aderenze, obliterazioni ostruttive
da tessuto fibroso non elasticoda tessuto fibroso non elastico
OrganizzazioneOrganizzazione
CicatrizzazioneCicatrizzazione
L’essudato è infiltrato da numerosi macrofagi
cui segue
la migrazione di fibroblasti
e nuovi piccoli vasi sanguigni
L’essudato è sostituito da tessuto fibroso
ben vascolarizzato
I vasi neofomati regrediscono
Rimane tessuto cicatriziale ricco di fibre di collagene

LESIONELESIONE
INFIAMMAZIONEINFIAMMAZIONE
Distruzione di tessutoDistruzione di tessuto
Cellule labili o stabiliCellule labili o stabili
ImpalcaturaImpalcatura
CelluleLABILILABILI: da mitosi di cellule staminali
• non hanno completato differenziamento
• Non hanno limite fisso di capacità replicativa
• Danno c. figlie che sono c. staminali con
destino di differenziamento terminale
Sostituiscono cellule che non possono dividersi
(epiteli di rivestimento, cellule ematiche e ImpalcaturaImpalcatura
connettivaleconnettivale
intattaintatta
RigenerazioneRigenerazione
e guarigionee guarigione
Struttura NormaleStruttura Normale
Buona riuscita della rigenerazione
dipende da:
1. Le cellule perdute devono essere
rimpiazzate da cellule identiche
2. L’architettura connettivale e vascolare
deve essere intatta o ricostruita
come era prima del danno
(epiteli di rivestimento, cellule ematiche e
linfocidi)
STABILISTABILI:: quiescenti con lento ricambio; queste
cellule sono sostituite da cellule mature che
vanno in mitosi (epatociti, epitelio tubulo
renale, epiteli secretori di ghiandole
endocrine, c. osso, fibroblasrti.
PERENNIPERENNI:: in generate nella vita fetale, non si
dividono mai nella vita postnatale e non
possono essere rimpiazzate se distrutte
(m.cardiaco, c. nervose)
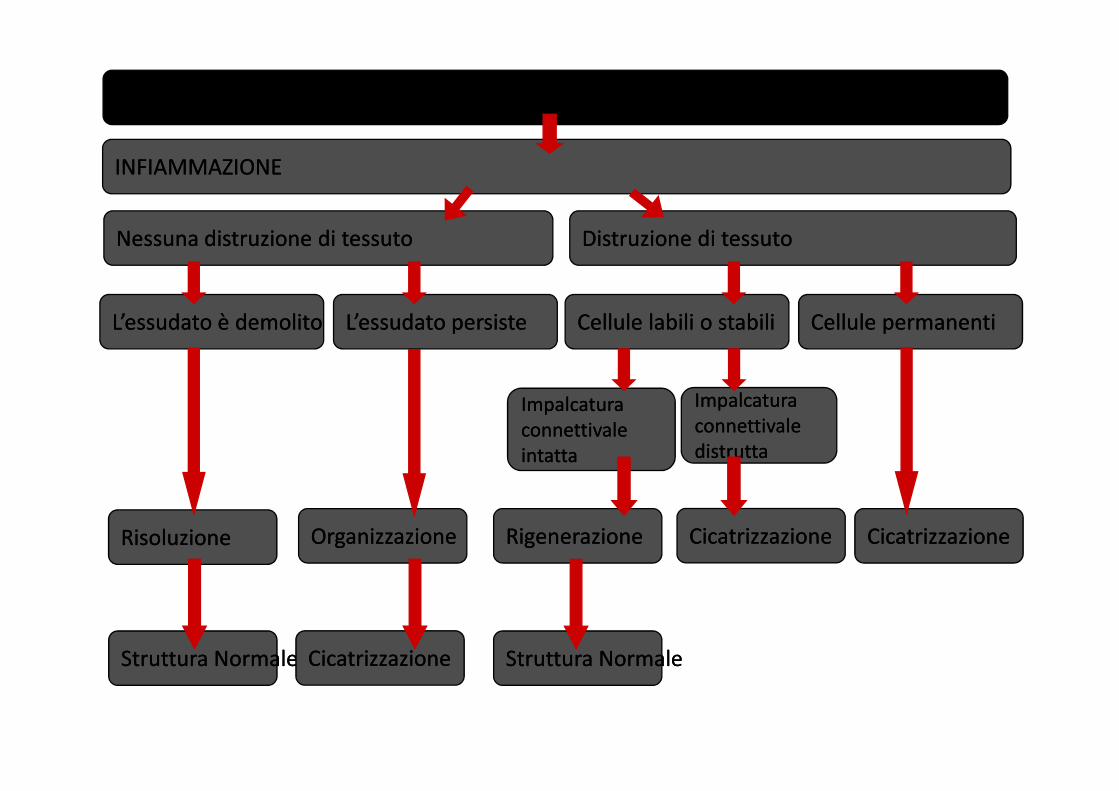
LESIONELESIONE
INFIAMMAZIONEINFIAMMAZIONE
Nessuna distruzione di tessutoNessuna distruzione di tessuto Distruzione di tessutoDistruzione di tessuto
L’essudato è demolitoL’essudato è demolito L’essudato persisteL’essudato persiste Cellule labili o stabiliCellule labili o stabili Cellule permanentiCellule permanenti
ImpalcaturaImpalcatura ImpalcaturaImpalcaturaImpalcaturaImpalcatura
connettivaleconnettivale
intattaintatta
ImpalcaturaImpalcatura
connettivaleconnettivale
distruttadistrutta
RisoluzioneRisoluzione OrganizzazioneOrganizzazione
Struttura NormaleStruttura Normale CicatrizzazioneCicatrizzazione
RigenerazioneRigenerazione
Struttura NormaleStruttura Normale
CicatrizzazioneCicatrizzazione CicatrizzazioneCicatrizzazione
Riparazione mediante guarigione,
cicatrizzazione e fibrosi
• Obiettivo della riparazione è di ripristinare il
tessuto riportandolo nella sua condizione
originaria.
• La guarigione è una risposta fibroproliferativa
tesa a riparare piuttosto che rigenerare un
certo tessuto
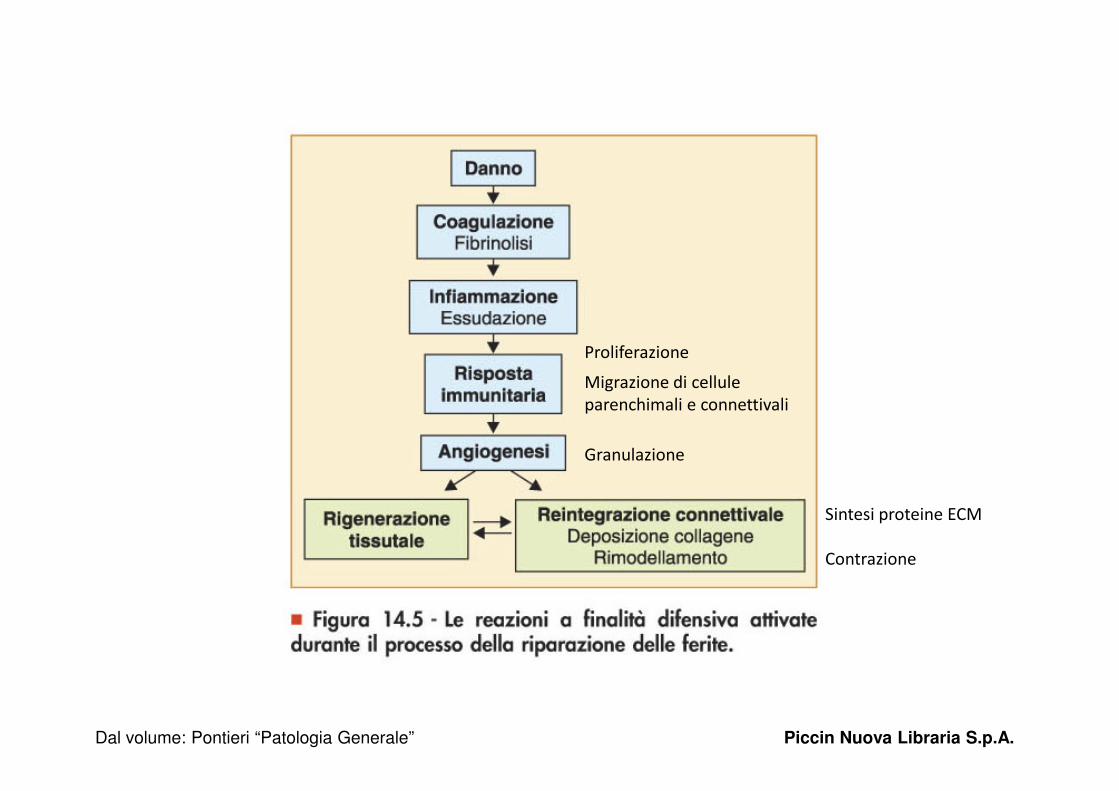
Figura 14.5 - Le reazioni a finalità difensiva attivate durante il processo della riparazione delle ferite.
Proliferazione
Migrazione di cellule
parenchimali e connettivali
Dal volume: Pontieri “Patologia Generale” Piccin Nuova Libraria S.p.A.
parenchimali e connettivali
Granulazione
Sintesi proteine ECM
Contrazione

Fattori che influenzano la riparazione
• Tessuto ed estensione del danno
• Intensità e durata dello stimolo dannoso
• Condizioni inibenti (mancata rimozione di
corpi estranei, alterato apporto ematico)corpi estranei, alterato apporto ematico)
• Presenza di malattie
• Trattamenti farmacologici (steroidi)
Dal volume: Pontieri “Patologia Generale” Piccin Nuova Libraria S.p.A.
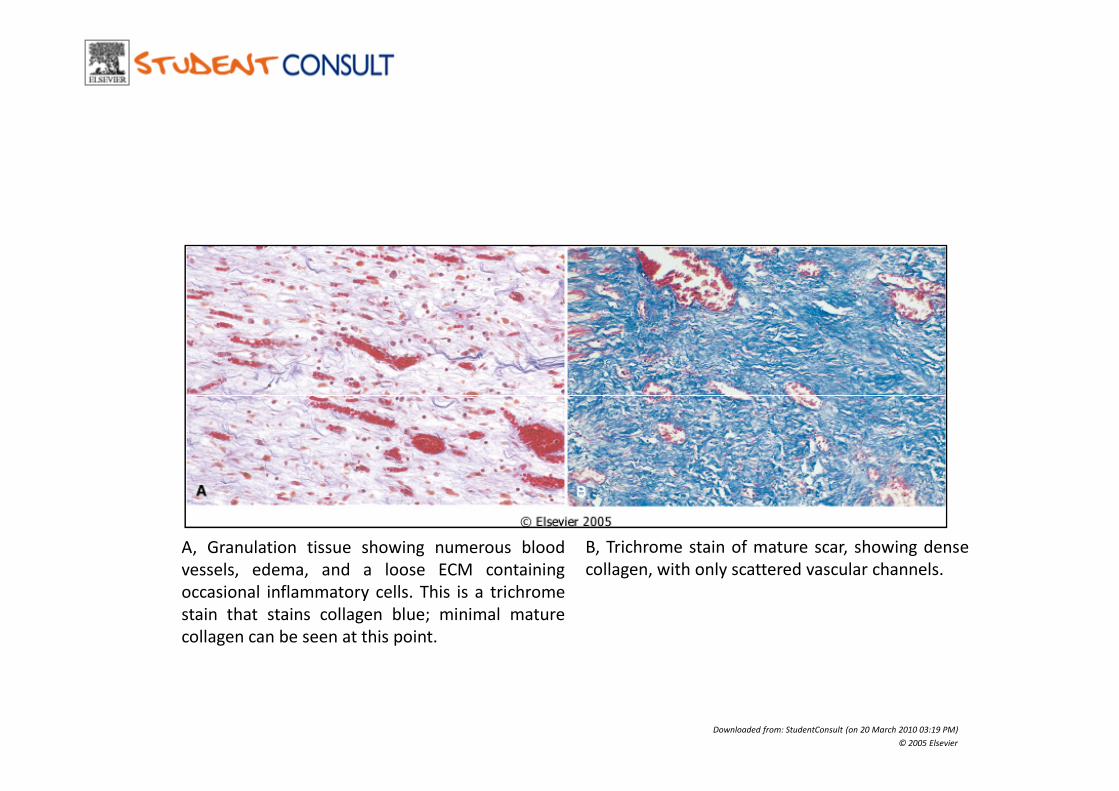
B, Trichrome stain of mature scar, showing dense
collagen, with only scattered vascular channels.
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier
A, Granulation tissue showing numerous blood
vessels, edema, and a loose ECM containing
occasional inflammatory cells. This is a trichrome
stain that stains collagen blue; minimal mature
collagen can be seen at this point.
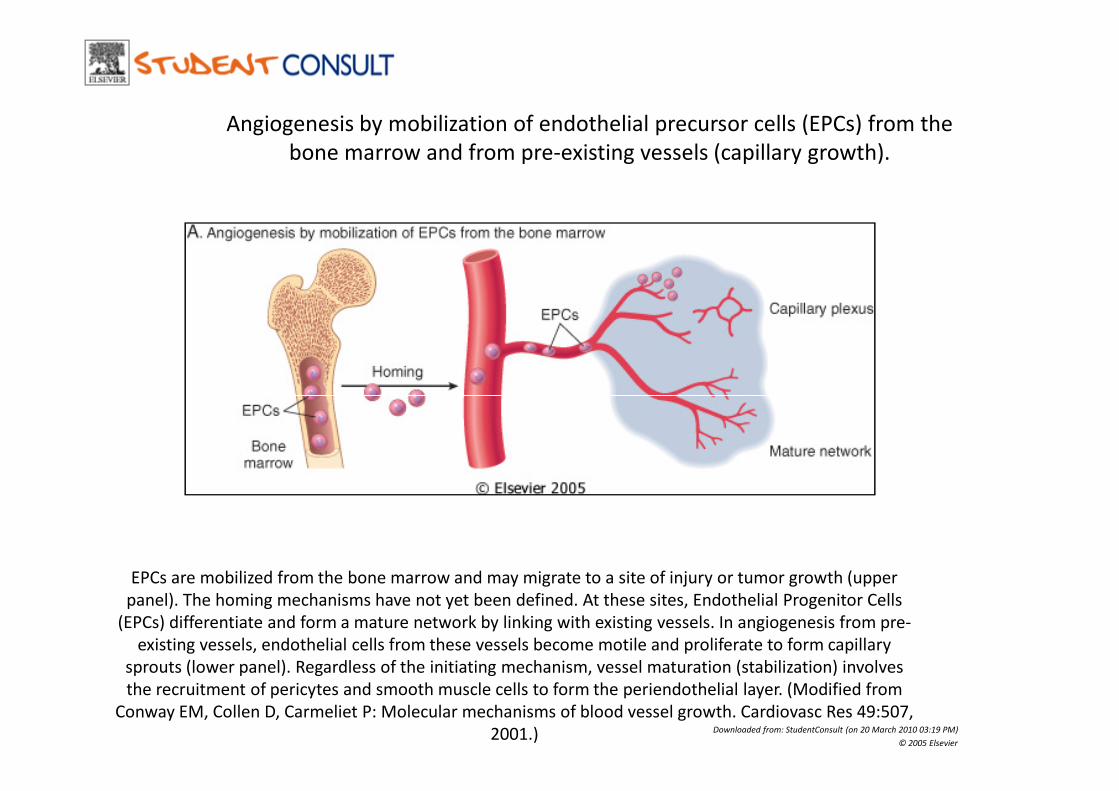
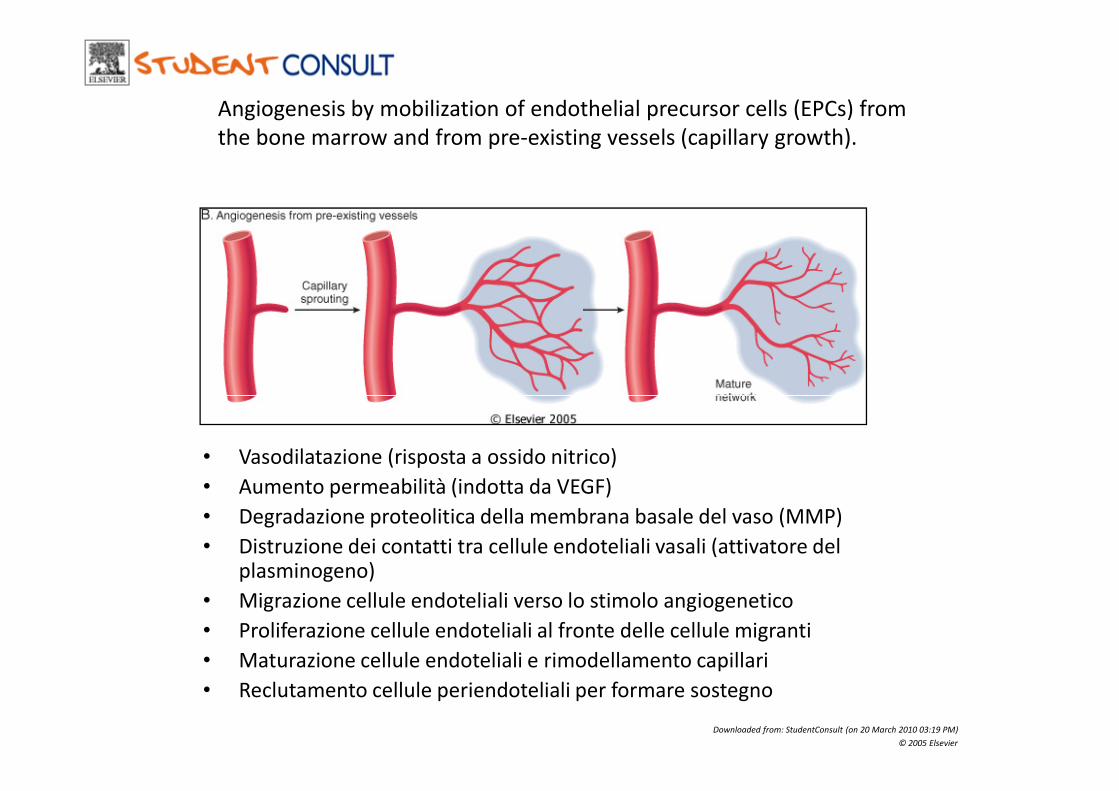
Angiogenesis by mobilization of endothelial precursor cells (EPCs) from the
bone marrow and from pre-existing vessels (capillary growth).
EPCs are mobilized from the bone marrow and may migrate to a site of injury or tumor growth (upper
panel). The homing mechanisms have not yet been defined. At these sites, Endothelial Progenitor Cells
(EPCs) differentiate and form a mature network by linking with existing vessels. In angiogenesis from pre-
existing vessels, endothelial cells from these vessels become motile and proliferate to form capillary
sprouts (lower panel). Regardless of the initiating mechanism, vessel maturation (stabilization) involves
the recruitment of pericytes and smooth muscle cells to form the periendothelial layer. (Modified from
Conway EM, Collen D, Carmeliet P: Molecular mechanisms of blood vessel growth. Cardiovasc Res 49:507,
2001.) Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier
Angiogenesis by mobilization of endothelial precursor cells (EPCs) from
the bone marrow and from pre-existing vessels (capillary growth).
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier
• Vasodilatazione (risposta a ossido nitrico)
• Aumento permeabilità (indotta da VEGF)
• Degradazione proteolitica della membrana basale del vaso (MMP)
• Distruzione dei contatti tra cellule endoteliali vasali (attivatore del plasminogeno)
• Migrazione cellule endoteliali verso lo stimolo angiogenetico
• Proliferazione cellule endoteliali al fronte delle cellule migranti
• Maturazione cellule endoteliali e rimodellamento capillari
• Reclutamento cellule periendoteliali per formare sostegno
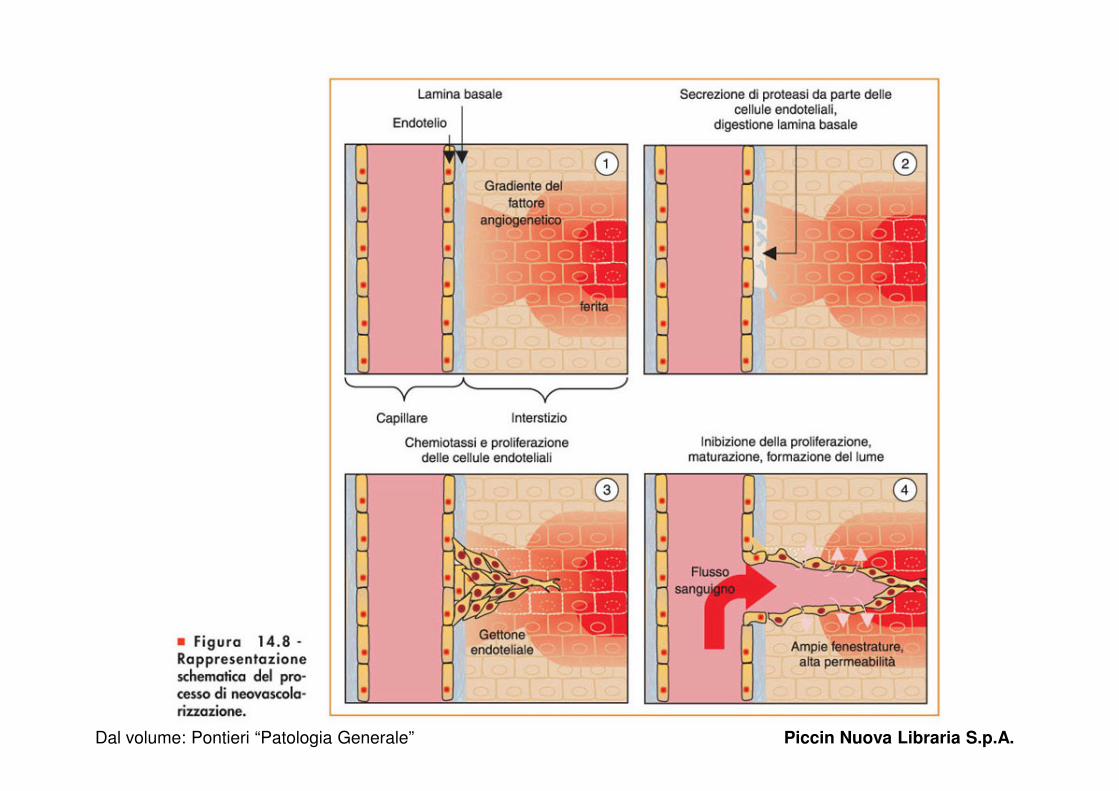
Figura 14.8 - Rappresentazione schematica del processo di neovascolarizzazione.
Dal volume: Pontieri “Patologia Generale” Piccin Nuova Libraria S.p.A.

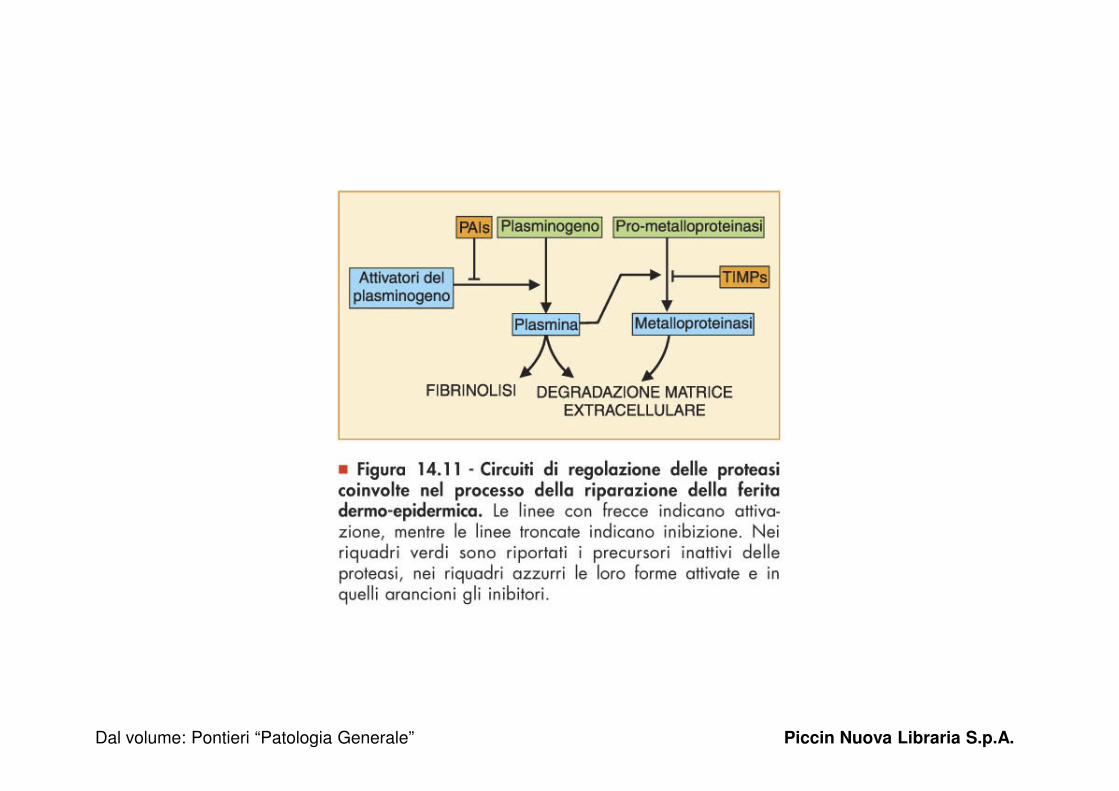
Four mechanisms are shown:
(1) regulation of synthesis by growth factors or
cytokines,
(2) inhibition of synthesis by corticosteroids or
TGF-β
(3) regulation of the activation of the secreted
but inactive precursors,
(4) blockage of the enzymes by specific tissue
inhibitors of metalloproteinase (TIMPs).
Matrix metalloproteinase regulation
inhibitors of metalloproteinase (TIMPs).
(Modified from Matrisian LM:
Metalloproteinases and their inhibitors in
matrix remodeling. Trends Genet 6:122,
1990, with permission from Elsevier Science.)
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier
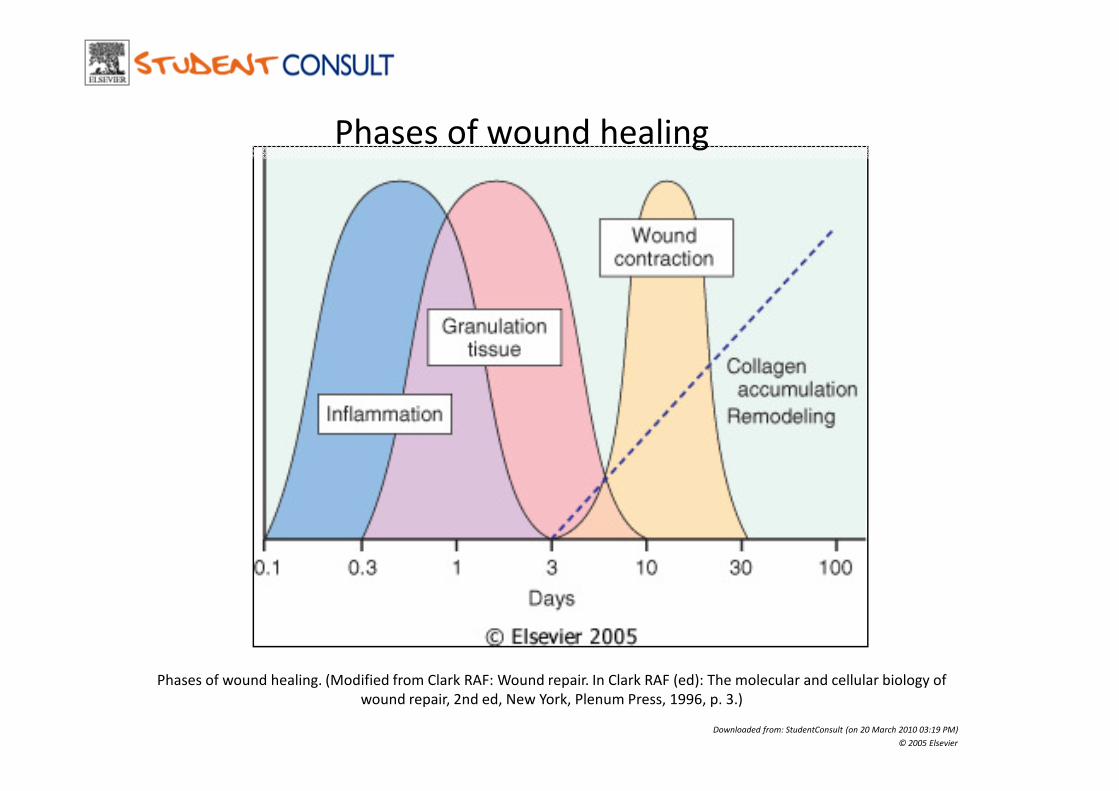
Phases of wound healing
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier
Phases of wound healing. (Modified from Clark RAF: Wound repair. In Clark RAF (ed): The molecular and cellular biology of
wound repair, 2nd ed, New York, Plenum Press, 1996, p. 3.)
Guarigione delle feriteGuarigione delle ferite
Meccanismi del processo di guarigione delle ferite:
• Prima intenzione:
– Guarigione di una ferita prodotta da incisione – Guarigione di una ferita prodotta da incisione netta con margini ravvicinati
• Seconda intenzione:
– Guarigione di una ferita con ampia distruzione di epitelio e sottoepitelio da rimpiazzare con tessuto cicatriziale
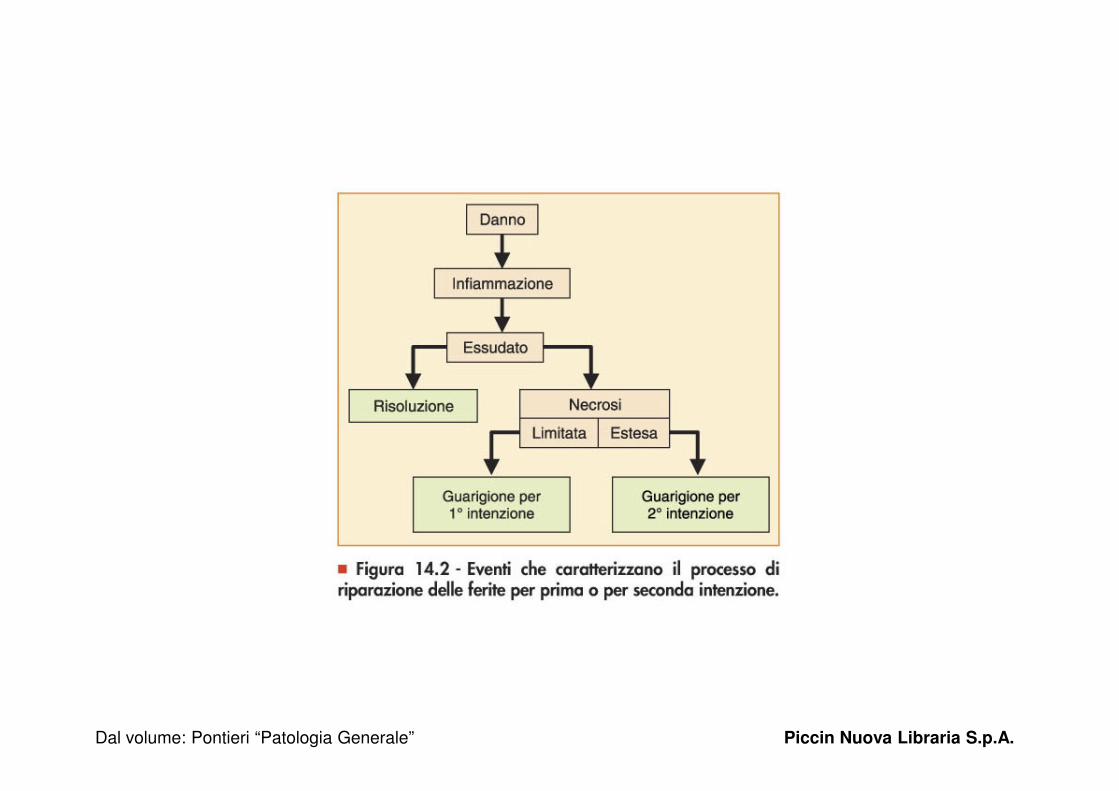
Figura 14.2 - Eventi che caratterizzano il processo di riparazione delle ferite per prima o per seconda intenzione.
Dal volume: Pontieri “Patologia Generale” Piccin Nuova Libraria S.p.A.
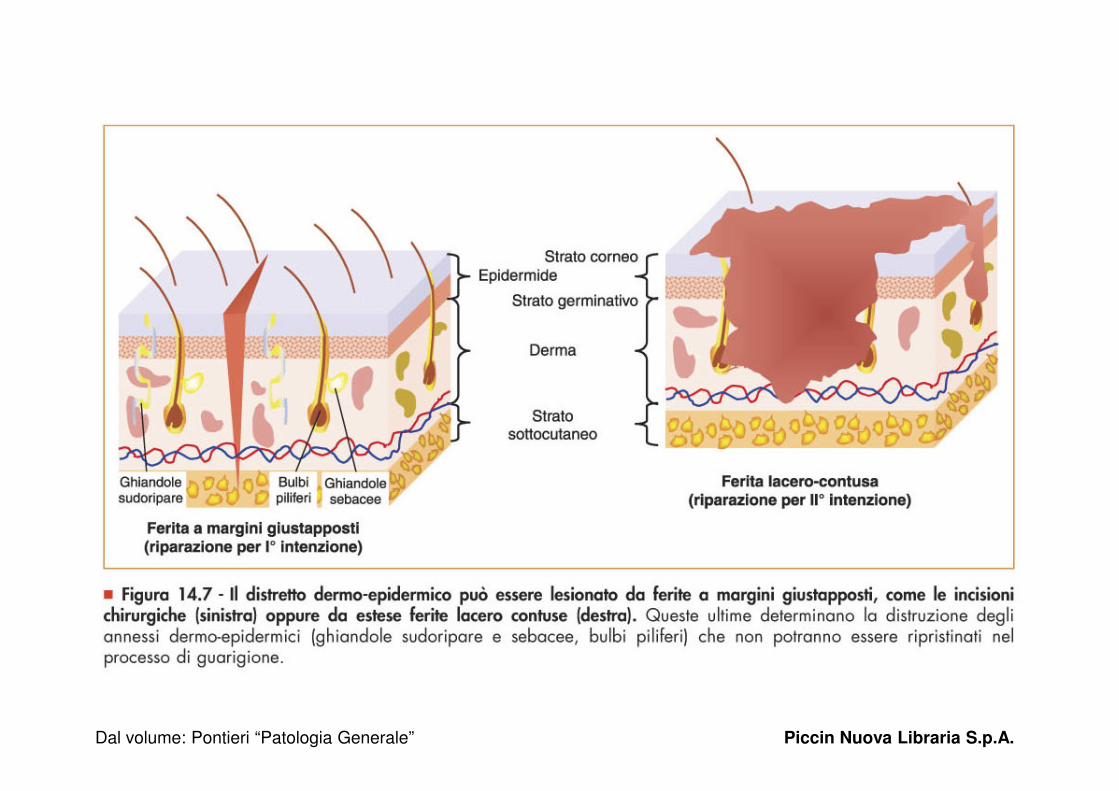
Figura 14.7 - Il distretto dermo-epidermico.
Dal volume: Pontieri “Patologia Generale” Piccin Nuova Libraria S.p.A.
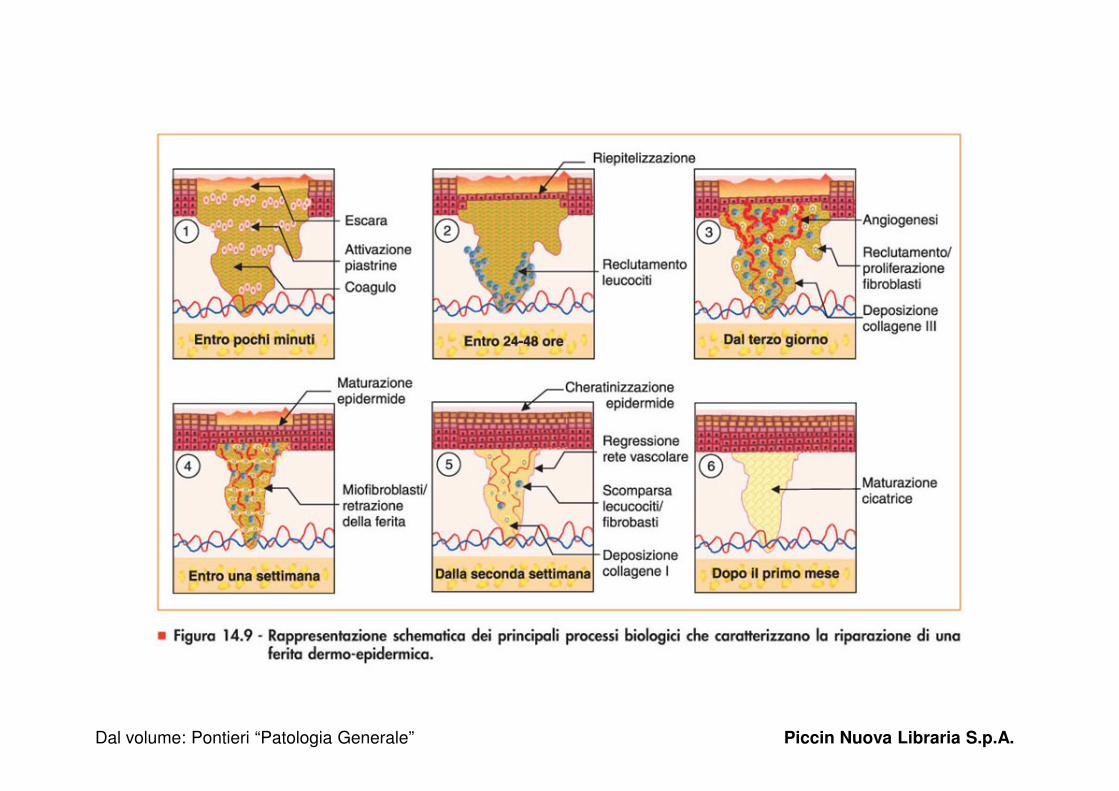
Figura 14.9 - Rappresentazione schematica dei principali processi biologici che caratterizzano la riparazione di una
ferita dermo-epidermica.
Dal volume: Pontieri “Patologia Generale” Piccin Nuova Libraria S.p.A.

Steps in wound healing by first intention (left) and second intention
(right). Note large amounts of granulation tissue and wound contraction
in healing by second intention.
large amounts of
granulation tissue and
wound contraction in
healing by second
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier
healing by second
intention.
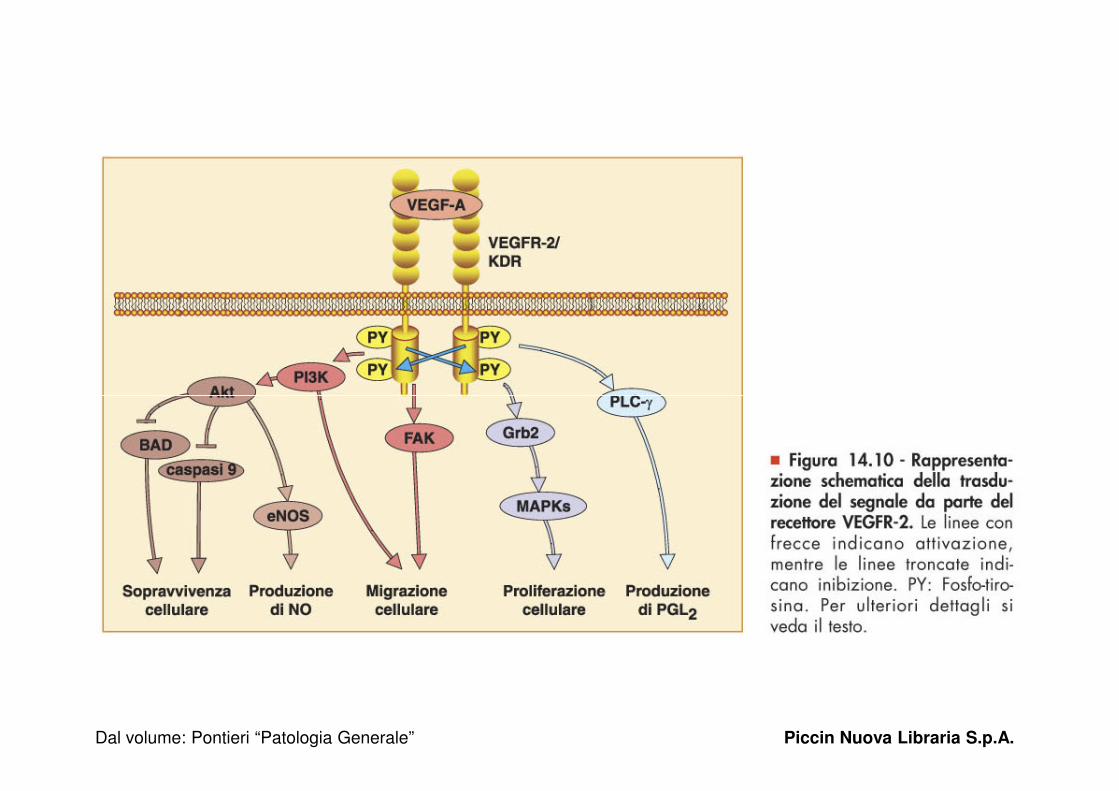
Figura 14.10 - Rappresentazione schematica della trasduzione del segnale da parte del recettore VEGFR-2.
Dal volume: Pontieri “Patologia Generale” Piccin Nuova Libraria S.p.A.
Dal volume: Pontieri “Patologia Generale” Piccin Nuova Libraria S.p.A.
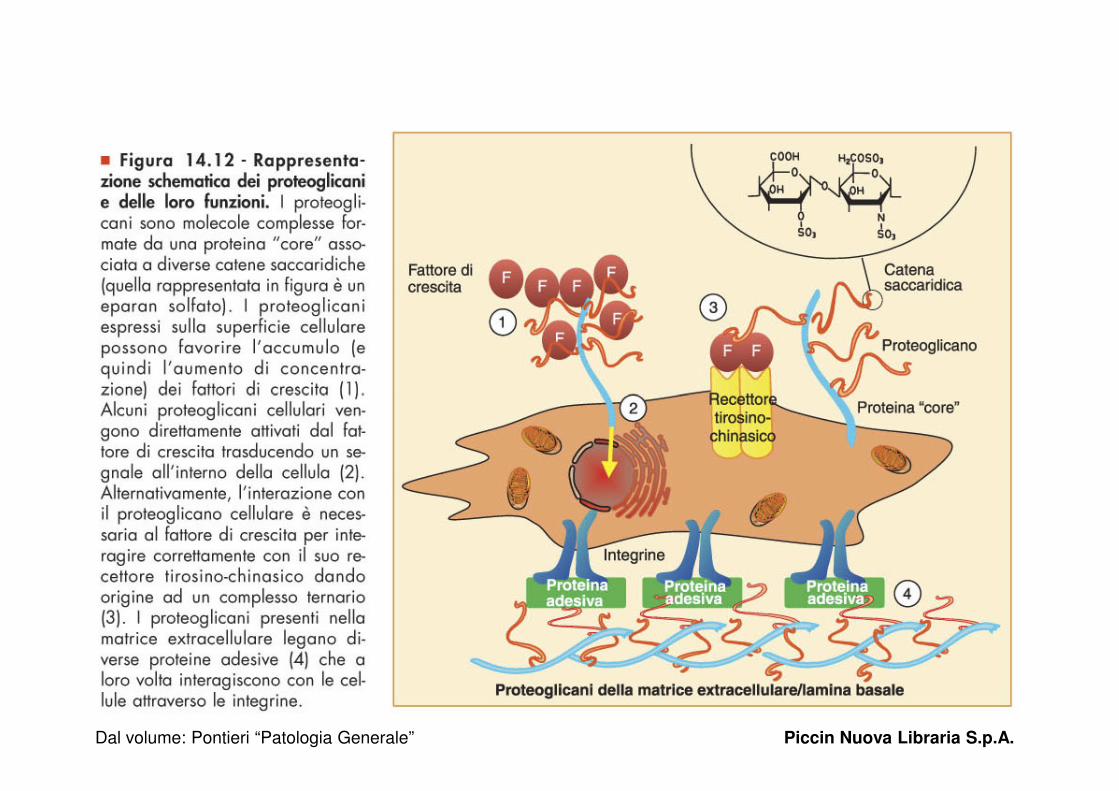
Figura 14.12 - Rappresentazione schematica dei proteoglicani e delle loro funzioni.
Dal volume: Pontieri “Patologia Generale” Piccin Nuova Libraria S.p.A.
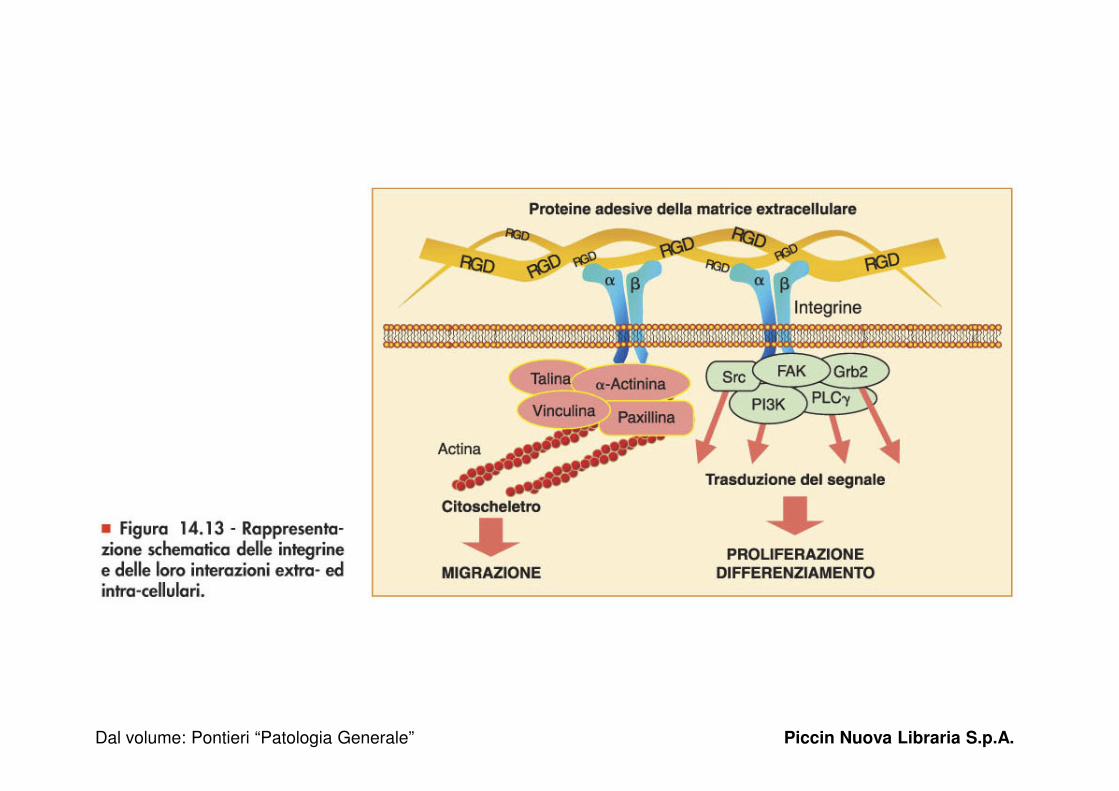
Figura 14.13 - Rappresentazione schematica delle integrine e delle loro interazioni extra- ed intra-cellulari.
Dal volume: Pontieri “Patologia Generale” Piccin Nuova Libraria S.p.A.
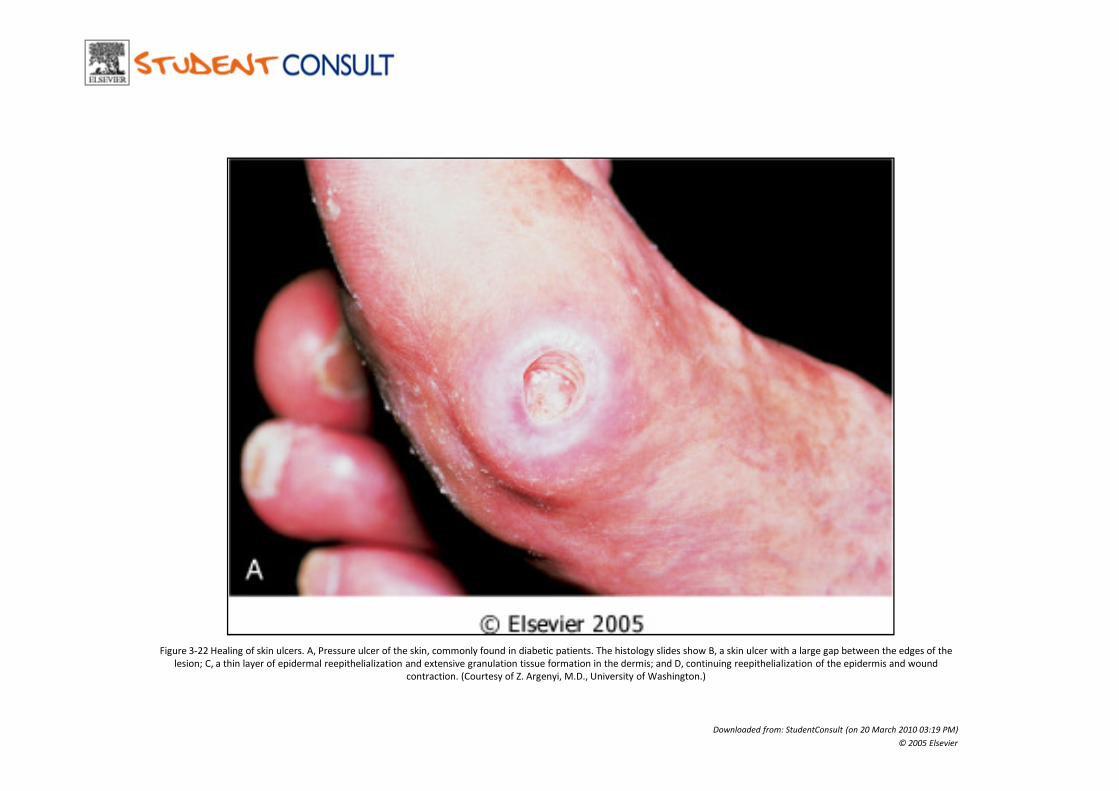
Figure 3-22 Healing of skin ulcers. A, Pressure ulcer of the skin, commonly found in diabetic patients. The histology slides show B, a skin ulcer with a large gap between the edges of the
lesion; C, a thin layer of epidermal reepithelialization and extensive granulation tissue formation in the dermis; and D, continuing reepithelialization of the epidermis and wound
contraction. (Courtesy of Z. Argenyi, M.D., University of Washington.)
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier

Figure 3-22 Healing of skin ulcers. A, Pressure ulcer of the skin, commonly found in diabetic patients. The histology slides show B, a skin ulcer with a large gap between the edges of the
lesion; C, a thin layer of epidermal reepithelialization and extensive granulation tissue formation in the dermis; and D, continuing reepithelialization of the epidermis and wound
contraction. (Courtesy of Z. Argenyi, M.D., University of Washington.)
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier

Figure 3-22 Healing of skin ulcers. A, Pressure ulcer of the skin, commonly found in diabetic patients. The histology slides show B, a skin ulcer with a large gap between the edges of the
lesion; C, a thin layer of epidermal reepithelialization and extensive granulation tissue formation in the dermis; and D, continuing reepithelialization of the epidermis and wound
contraction. (Courtesy of Z. Argenyi, M.D., University of Washington.)
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier

Figure 3-22 Healing of skin ulcers. A, Pressure ulcer of the skin, commonly found in diabetic patients. The histology slides show B, a skin ulcer with a large gap between the edges of the
lesion; C, a thin layer of epidermal reepithelialization and extensive granulation tissue formation in the dermis; and D, continuing reepithelialization of the epidermis and wound
contraction. (Courtesy of Z. Argenyi, M.D., University of Washington.)
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier
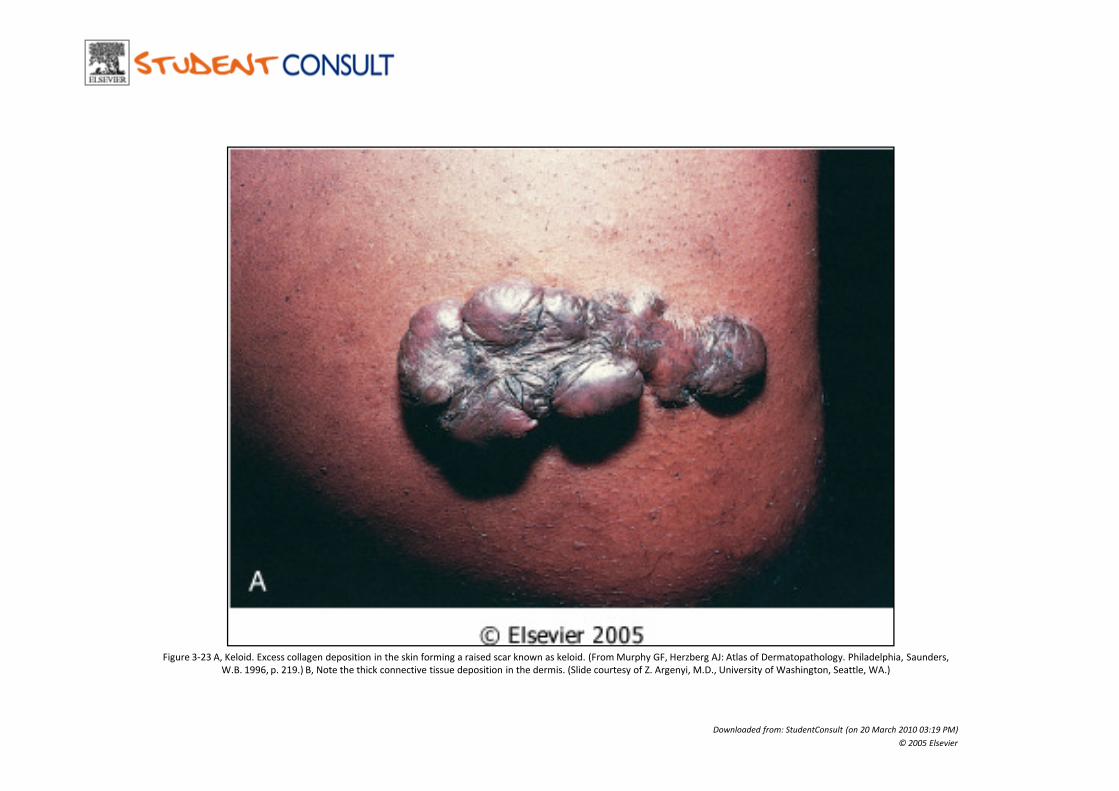
Figure 3-23 A, Keloid. Excess collagen deposition in the skin forming a raised scar known as keloid. (From Murphy GF, Herzberg AJ: Atlas of Dermatopathology. Philadelphia, Saunders,
W.B. 1996, p. 219.) B, Note the thick connective tissue deposition in the dermis. (Slide courtesy of Z. Argenyi, M.D., University of Washington, Seattle, WA.)
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier
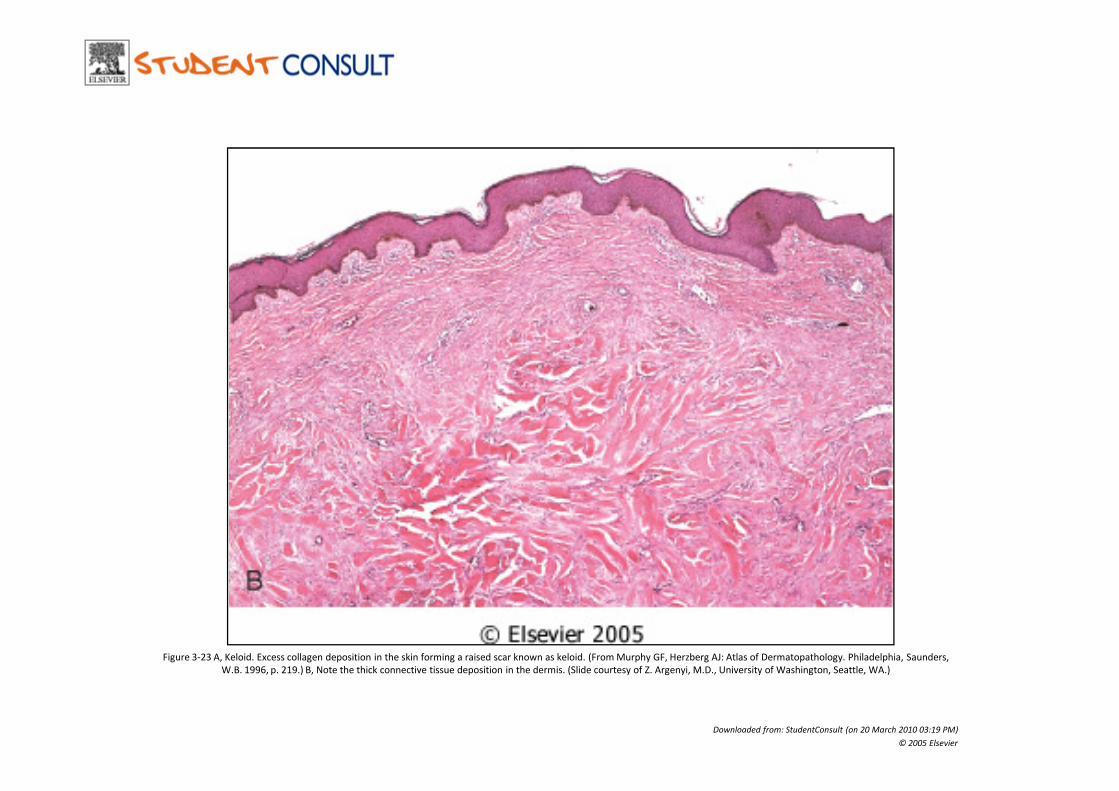
Figure 3-23 A, Keloid. Excess collagen deposition in the skin forming a raised scar known as keloid. (From Murphy GF, Herzberg AJ: Atlas of Dermatopathology. Philadelphia, Saunders,
W.B. 1996, p. 219.) B, Note the thick connective tissue deposition in the dermis. (Slide courtesy of Z. Argenyi, M.D., University of Washington, Seattle, WA.)
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier
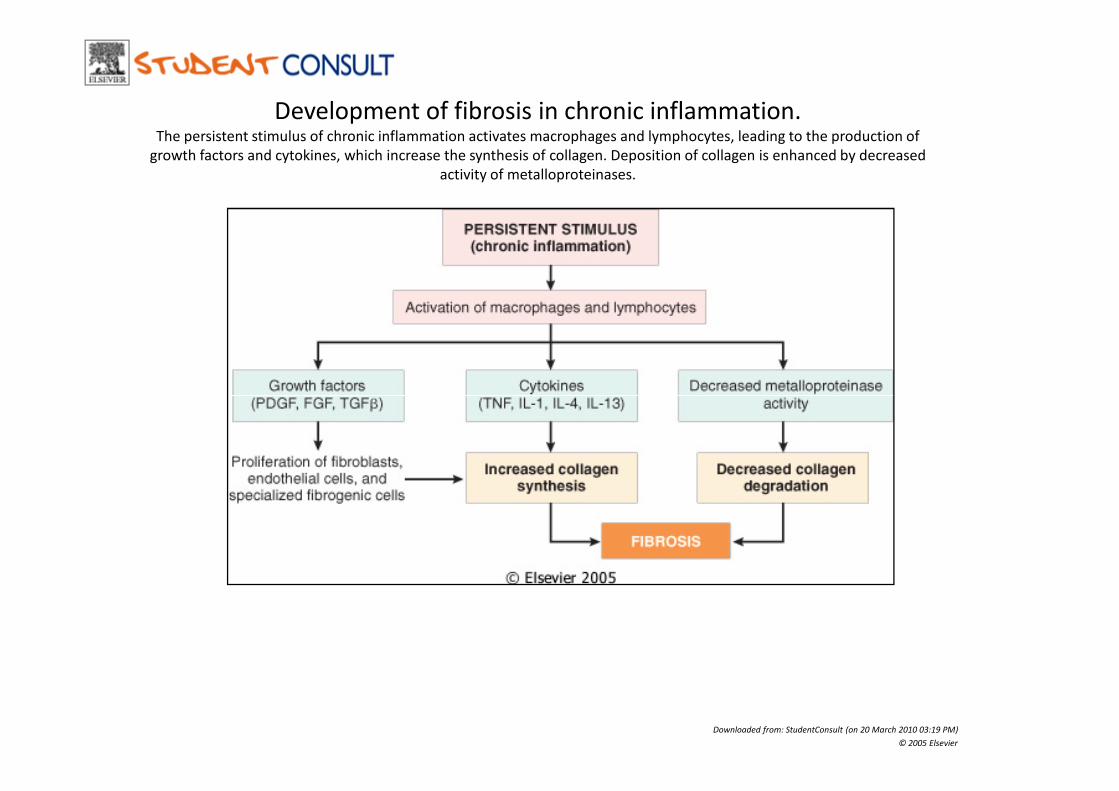
Development of fibrosis in chronic inflammation.The persistent stimulus of chronic inflammation activates macrophages and lymphocytes, leading to the production of
growth factors and cytokines, which increase the synthesis of collagen. Deposition of collagen is enhanced by decreased
activity of metalloproteinases.
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier
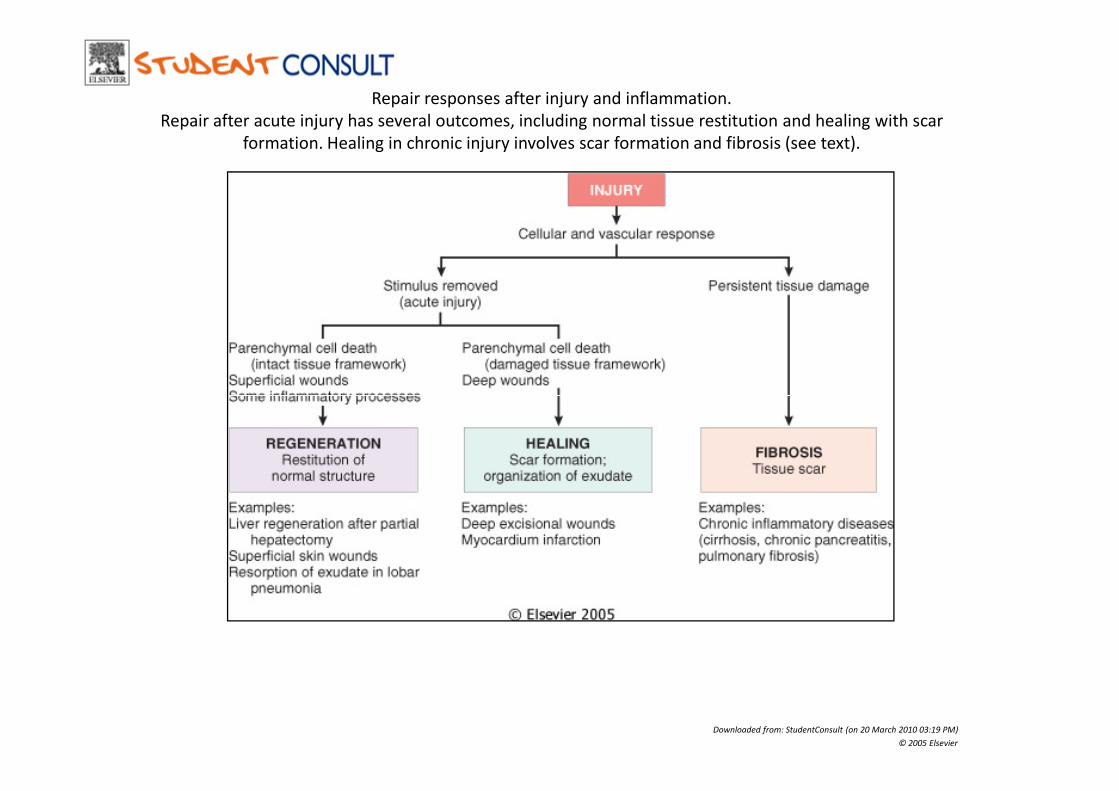
Repair responses after injury and inflammation.
Repair after acute injury has several outcomes, including normal tissue restitution and healing with scar
formation. Healing in chronic injury involves scar formation and fibrosis (see text).
Downloaded from: StudentConsult (on 20 March 2010 03:19 PM)
© 2005 Elsevier
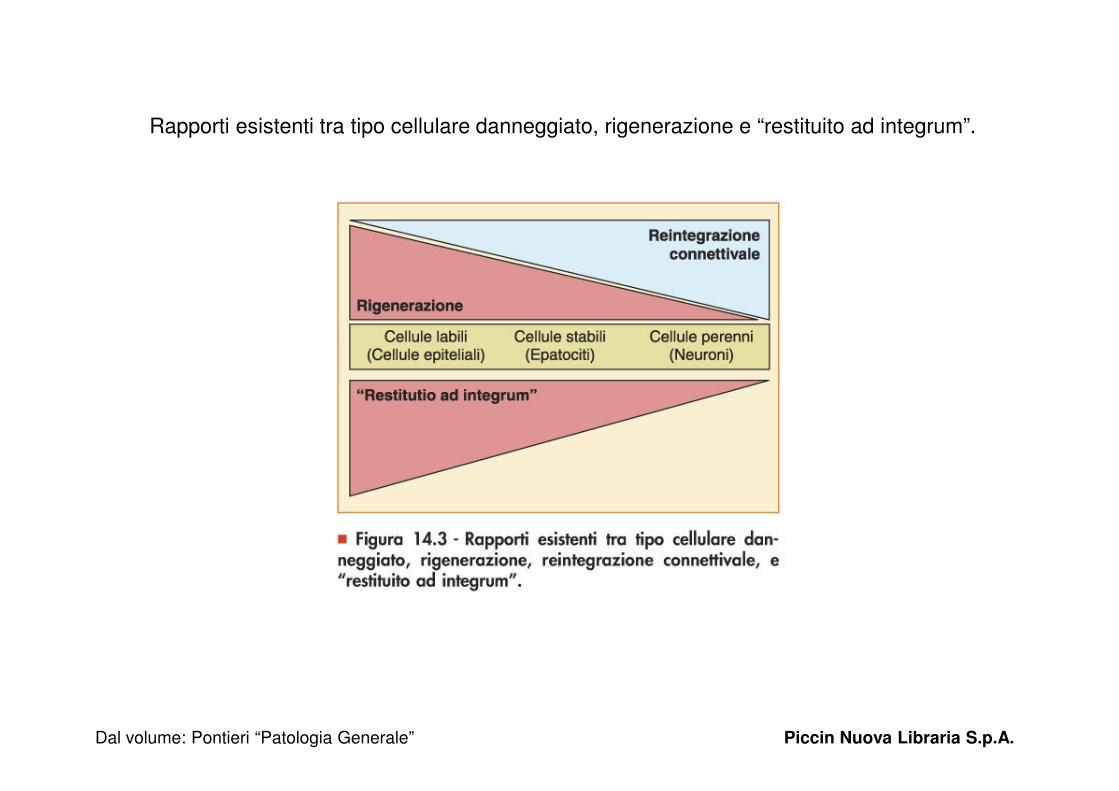
Rapporti esistenti tra tipo cellulare danneggiato, rigenerazione e “restituito ad integrum”.
Dal volume: Pontieri “Patologia Generale” Piccin Nuova Libraria S.p.A.