rna l. - acd
TRANSCRIPT

SUMMER • 1989
The
RNA L.th°:AMERICAN COLLEGE of DENTISTS

BJECTIVES
of the AMERICAN
COLLEGE of DENTISTS
The American College of Dentists inorder to promote the highest ideals inhealth care, advance the standardsand efficiency of dentistry, developgood human relations and understand-ing, and extend the benefits of dentalhealth to the greatest number, de-clares and adopts the following prin-ciples and ideals as ways and means forthe attainment of these goals.
(a) To urge the extension and im-provement of measures for the con-trol and prevention of oral disorders;
(b) To encourage qualified personsto consider a career in dentistry sothat dental health services will beavailable to all and to urge broadpreparation for such a career at alleducational levels;
(c) To encourage graduate studiesand continuing educational efforts bydentists and auxiliaries;
(d) To encourage, stimulate andpromote research;
(e) To improve the public under-standing and appreciation of oralhealth service and its importance tothe optimum health of the patient;(f) To encourage the free exchange
of ideas and experiences in the in-terest of better service to the patient;(g) To cooperate with other groups
for the advancement of interpro-fessional relationships in the interestof the public;(h) To make visible to professional
persons the extent of their responsi-bilities to the community as well as tothe field of health service and to urgethe acceptance of them;(i) To encourage individuals to
further these objectives, and to recog-nize meritorious achievements andthe potentials for contributions todental science, art, education, liter-ature, human relations or other areaswhich contribute to human welfare—by conferring Fellowship in theCollege on those persons properlyselected for such honor.

VOLUME568NUMBER2•SUMMER1989
Keith P. Blair, DDS, Editor
Associate EditorsWilliam W. Howard, DMDWilliam D. McHugh, LDS, DDScAlvin L. Morris, DDS, PhDPrem S. Sharma, LDS, DDS, MS
Business ManagerGordon H. Rovelstad, DDS, PhD
Editorial Board of ReviewDon L. Allen, DDS, MSMuriel J. Bebeau, MA, PhDWilmer B. Eames, DDSPaul Goldhaber, DDS, MAHarald Loe, DDS, Dr. Odont.James H. McLeran, DDS, MSLawrence H. Meskin, DDS, PhDRichard C. Oliver, DDS, MSRalph W. Phillips, MS, DScJeanne C. Sinkford, DDS, PhDGeorge W. Teuscher, DDS, PhDRaymond P. White, DDS, PhD
Publications AdvisoryCommittee
Thomas W. Slack, DDS ChairmanChris C. Scures, DDSJuliann S. Bluitt, DDSPrem S. Sharma, DDS
Correspondence relating to the Journalshould be addressed to the Editor,Keith P. Blair, DDS, Suite 352N,American College of Dentists,7315 Wisconsin Avenue,Bethesda, MD 20814-3202
The business office for the Journal ofthe American College of Dentists can be
........reached by telephone at (301) 986-0555.
—1
A Quarterly Publication presenting Ideas,
Advancements and Opinions in Dentistry
The Journal of the American College of Dentists (ISSN 0002-7979) is published quarterly by the American College ofDentists, Inc., Suite 352N, 7315 Wisconsin Ave., Bethesda,Maryland 20814, with Second Class Postage paid at Bethesda,Maryland and at additional mailing office. Copyright 1988 bythe American College of Dentists, Inc.Postmaster Send address changes to the Journal of theAmerican College of Dentists, Gordon H. Rovelstad, DDS,Business Manager, 7315 Wisconsin Avenue, Suite 352N,Bethesda, MD 20814-3202.Subscription rate per year for members of the ACD is $20included in the annual membership dues. Subscription rate peryear for non-members is $30. Air mail to Canada and Mexicois an additional $5, all other foreign addresses is an additional$20. Single copies: $6.While every effort is made by the publishers and EditorialBoard to see that no inaccurate or misleading opinions orstatements appear in the Journal, they wish to make it clearthat the opinions expressed in the articles, correspondence, etc.herein are the responsibility of the contributor. Accordingly,the publishers and the Editorial Board and their respectiveemployees and officers accept no liability whatsoever for theconsequences of any such inaccurate or misleading opinion orstatement.
For bibliographic references, the Journal is abbreviated J AmCol Dent and should be followed by the volume number, page,month and year. The reference for this issue is J Am Col Dent56:1-32, Summer 1989
The Journal is a Publication Member of theAmerican Association of Dental Editors

CONTENTSFrom the Editor's Desk 3
Dental Insurance: Its Variations and RelationshipTo The Use of Dental Services 4
H. Barry Waldman
Adhesive Bonding of Composites 10R. L. BowenF. C. EichmillerW. A. MarjenhoffN. W. Rupp
The Placebo Effect in the Management of ChronicMyofascial Pain 14
John W. Stockstill
Motivations for Treatment and Outcomes of Care 19Susan ReisineJudith Weber
Why Not You In The FDI? 25Robert W. Elliott, Jr.
News of Fellows 26
Section Activities 29
Instructions for Authors 32
Directory of Officers 33
SUMMER 1989

JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS 3
William John Gies
The name of William John Gies isseen frequently in matters relatedto the profession of dentistry andparticularly to the American Col-lege of Dentists. Why has this manreceived such unusual recognitionand high honors from dentistry,especially since he was not a den-tist.Dr. Gies was one of dentistry's
greatest benefactors and, becauseof that, he became an adoptedmember of the profession. Largelydue to his early efforts, dentistryattained parity in education withmedicine. As a scientist, educator,author, editor, lecturer and leaderof professional societies, he advo-cated the highest professional ide-als. He contributed tremendouslyto the advancement of dentistryand to the elevation of the profes-sion in the public esteem.He worked his way through col-
lege by tutoring others and choseteaching as his vocation, graduat-ing from Yale in 1897 with a Ph.D.degree in Physiology. He was ap-pointed to the medical teachingstaff at Columbia University wherehe continued to serve for nearlyforty years. As a researcher andauthor, he published volumes onbiological chemistry and dental re-search subjects.In 1916, Dr. Gies recommended
the establishing of a dental schoolat Columbia University and wasinstrumental in its organization. In1919, he founded the Journal ofDental Research and, the next year,founded the International Associa-tion of Dental Research (IADR). In1923, he initiated and led the nego-tiations which combined four sepa-rate groups of dental educators intoa new organization that has contin-ued to function as the American
Keith P. Blair
Association of Dental Schools(AADS).He became the Director for the
Study of Dental Education spon-sored by the Carnegie Foundationand, in 1930, produced the famousCarnegie Report on the survey ofdental education that had been re-quested by the AADS. This workeventually led to much better stan-dards in dental education andhelped to place the control of den-tal literature in the hands of theprofession.He was the first editor for the
Journal of Dental Research andcontinued in that position fornearly twenty years, frequentlymaking up deficits from his ownpocket until that Journal eventuallybecame self supporting. At thesame time, he also served for manyyears as the Secretary for the IADR,guiding it through its early years.Mainly through his efforts, the
American College of Dentists estab-lished the American Association of
FROM THE
EDITOR'SDESK
Dental Editors in 1931. In 1934,when the JOURNAL of the Ameri-can College of Dentists introducedits first issue, Dr. Gies was thefounding editor and continued toserve in that position for a five-yearterm.To honor him, the Gies Founda-
tion for the Advancement of Den-tistry was organized in 1950. Itcontinues • to support ongoingprojects in dental education, dentalresearch and dental journalism.The American College of Dentistshas established the Gies Award torecognize Fellows of the Collegewhose truly outstanding contribu-tions have warranted exceptionalrecognition.From his earliest days, Dr. Gies
preached that dentistry could reachits goals only on the broad front ofeducation, research and journalismand that these three were interde-pendent on each other. Then heproceeded to work with dentistryfor most of his life to accomplishthese goals. It was his tremendouspersonal effort that helped den-tistry develop into the status of areal profession during the 1920'sand 1930's. His initiative, drive andunwavering commitment to princi-ples has benefited the dental pro-fession immensely and simply can-not be fully appreciated. What ismentioned here are only the briefhighlights of his illustrious career.He was a man who had a CALL-
ING. Because he did, the world ofdentists and their patients has beenmade far better. William John Giesrichly deserves to be rememberedand honored by dentistry. A
Keith P. BlairSUMMER 1989

4 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
DENTAL INSURANCE:
Its Variations And Relationship To The Use OfDental Services
H. Barry Waldman*
"In recent decades, dental in-surance plans have been one ofthe fastest-growing items onthe employee benefits scene."(1)
Between 1967 and 1985, thenumber of persons in the UnitedStates with dental coverage grewfrom 4.6 million to almost 100 mil-lion, largely because of the adop-tion of worksite-based groupplans.' In 1986, 71 percent of allfull-time employees in medium andlarge firms participated in dentalplans financed wholly or partiallyby their employers—an increase of25 percent from the proportioncovered in 1980.1 These plans pro-vided a variety of services (withemphasis on preventive care), pro-vider payment procedures and em-ployee contribution mechanisms,all of which contributed signifi-cantly to patient dental visit pat-terns and the extent and type ofprovided services.The following presentation will
review the changing picture of den-tal insurance with emphasis on the1980s and the anticipated develop-ments during the next decade.
Received January 30, 1989.Accepted April 22, 1989.*H. Barry Waldman, BA, DDS, MPH,
PhD, Professor and Chairman, Departmentof Dental Health, School of Dental Medi-cine, State University of New York at StonyBrook.
Some background
Third party coverage of personaldental expenditures was initiatedas a fringe benefit for employees ofthe Denver and Rio Grand Rail-ways Company before the twenti-eth century. A summary of develop-ments during this century havebeen divided into three periods:
1. between 1910 and 1945 as aperiod of isolated prepaymentideas;
2. 1946-1965 as a period of ex-perimentation with variousbenefit plans; and
3. 1965 to 1976 as the majorgrowth period of plans.
The slow growth of dental in-surance plans until the second halfof this century was due in part, "tothe need to afford the average citi-zen some protection from hospitalmedical costs before focusing ondental care cost."'
Expenditures for dental services
Between 1980 and 1987, currentdollar expenditures for dental ser-vices in the United States morethan doubled from $15.4 billion to$32.8 billion. In terms of constantdollars (i.e. removing the effects ofinflation) there was an increase of31 percent (from $11.9 billion to$15.5 billion). It is projected thatconstant dollar national dental ex-
*Douglass and Day provide an extensiveretrospective review and current status ofcosts and payments for dental servicesthrough the mid 1970s.3
penditures will increase by approx-imately one third by the year 2000(Table I).
Dental expenditures per personincreased from $68.42 in 1980 to$134.75 in 1987 (from $52.71 to$64.29 in constant dollars).5•6Based upon population projectionsthrough the end of the century,dental expenditures per person areprojected to increase to $334.38($77.15 constant dollars) (TableI).**In 1987, direct out-of-pocket ex-
penses for hospital and physicianservices represented respectively,10.6 percent and 27.8 percent of thetotal annual expenditures.4 By con-trast, 60.9 percent of dental ex-penses were paid directly by pa-tients. However, the share ofpayments for dental services paiddirectly by patients had decreasedfrom 91.5 percent in 1970 and 72.7percent in 1980 (Table II).While the private insurance's
share of dental expenditures in-creased from 23.4 percent to 37.1percent during the 1980s, govern-ment program share of dental ex-penditures decreased from lessthan four percent to less than twopercent. Based on projectionsthrough the year 2000, there will beminimal changes in governmentand private insurance share of den-tal expenditures (Table II).
**For an extended discussion of dentaleconomic predictions through the year2000, see an earlier presentation by thiswriter in the Journal of the American Col-lege of Dentists.9
VOLUME 36 NUMBER 2

DENTAL INSURANCE 5
Table I. Current and constant dollar national expenditures for dental services by source of paymentand expenditures per person: selected years 1970-2000(4-8)
Total National Expenditures
ExpendituresPer PersonPrivate Public
CurrentDollar
DentalComponent
CPIConstantDollarPrivate Direct Federal State & Current Constant
Year Insurance Payment Gov't Local Total (1977=100) Total Dollars Dollars
(All total national dollar figures are in billions)1970 $.2 $4.3 $.1 $.1 $4.7 64.5 $7.31980 3.6 11.2 .3 .3 15.4 129.8 11.9 $68.42 $52.711986 9.9 19.1 .3 .3 29.6 198.5 14.91987 12.2 20.0 .3 .3 32.8 209.6 15.6 134.75 64.29
Projected1990 14.2 26.8 .4 .4 41.8 248.5 16.8 167.42 67.371995 21.5 39.8 .5 .4 62.2 na2000 31.4 57.1 .6 .5 89.6 433.4 20.7 334.38 77.15
Who has dental insurancecoverage?
Between the late 1960s and 1984,there was a continuing annual in-crease in the number of peoplecovered by dental insurance.*Since 1984, there has been a slowdown and decrease in dental insur-ance coverage (Table III). This de-cline resulted from a number offactors, including:
1. Employment declines in someindustries, such as basic steel,which provided dental bene-fits.
2. Efforts to control health carecosts caused some companiesto reconsider expanding theirbenefit programs to includedental care.
3. Flexible benefit programswhich enabled employees toswitch insurance plans in fa-vor of other benefits.'
By 1986, almost 40 percent ofthe civilian noninstitutionalized
*Any insurance plan specifically designedto pay all or part of the dental expenses ofthe insured individual, except oral surgery.This insurance can be either a group or anindividual policy, with the premiums paidby the individual, the employer, a thirdparty or a combination of these. Benefitscan be received under the plan in the form ofpayment to the individual or to the dentist.'
population of the United States hadsome form of dental insurance.Forty-three percent of children be-tween five and seventeen years ofage had dental insurance. Almostone third of young adults (between18 and 24 years) had insurance;and between 41 percent and 49percent of the population between25 and 54 years had insurance.There was a progressive decrease indental insurance coverage throughthe various age cohorts after 54years of age (Table IV).
There were differences by thevarious demographic characteris-tics in the extent of coverage. Maleswere more likely to have coveragethan were females, particularlythose age 45 and over. A largerproportion of whites than blackshad coverage, and non-Hispanicswere more likely to be insured thanHispanics. A greater proportion ofthose living in the suburbs thanthose residing in the central city, oroutside of Metropolitan StatisticalAreas (MSA), had dental insurance
Table II. Percent distribution of national expenditures for dentalservices by source of payment: selected years 1970-2000(4-7)
Year
Private Public
TotalPrivate
InsuranceDirect
PaymentFederalGov't
State &Local
1970 4.3% 91.5% 2.1% 2.1% 100.0%1980 23.4 72.7 1.9 1.9 99.91986 33.4 64.5 1.0 1.0 99.91987 37.1 60.9 0.9 0.9 99.8
Projected1990 33.9 64.1 1.0 1.0 100.21995 34.6 63.9 0.8 0.6 99.92000 35.0 63.7 0.7 0.6 100.0
Projections for 1990 and beyond were developed prior to the availabilityof 1987 data. The original projects for 1987 were that 33.6 percent ofexpenditures would be paid by priviate insurance and 64.2 by directpayments. (4)
SUMMER 1989

6 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
Table III. Number of personswith private dental insurance:selected years, 1967-1986(11)
Year Number
(In millions)1967 4.61970 11.91975 30.31980 79.4
1981 83.21982 93.11983 100.81984 102.1
1985 99.81986 94.9
coverage. The population living inthe West had the highest rate ofcoverage and those living in theSouth had the lowest. Finally, therewere greater rates of coverage withincreased levels of education andincreased family income (Table V).
Use of dental services
As compared to the populationwithout dental insurance, individu-als with insurance coverage had 1)more visits per person, 2) a greaterpercent with a single dental visitand multiple dental visits in thepast year, and 3) a greater percentwith last visit for a check-up(Table VI). In addition, the dentatepopulation had more than doublethe rate of insurance coverage asdid the edentulous population(Table VII).
Dental insurance for employeesof medium and large firms
Data from the Bureau of LaborStatistics' 1980-86 surveys of full-time employees in medium andlarge firms provide specific infor-mation on developments in dentalinsurance coverage for a signifi-cant segment of the workforce andgeneral population.' The 1986 sur-vey studied a sample of 1,500 estab-lishments which represented ap-proximately 46,000 establishmentsemploying 24 million workers. In
Table IV. Percent distribution of persons 2 years of age and overby private dental insurance status: 1986 (10)
Age
Have privatedental
Insurance
Do nothave private
dentalInsurance Unknown
2-4 yrs. 37.8% 56.7% 5.5%
5-11 yrs. 42.9 53.0 4.1
12-17 yrs. 43.1 52.7 4.2
18-24 yrs. 32.3 59.0 8.7
25-34 yrs. 41.2 53.9 4.9
35-44 yrs. 49.0 46.5 4.5
45-54 yrs. 44.8 50.0 5.2
55-64 yrs. 35.3 59.0 5.7
65-74 yrs. 14.6 78.4 7.0
75+ yrs. 7.3 84.4 8.3
Total 37.8% 56.7% 5.5%
addition, 98 percent of the partici-pants were in dental plans withprovisions that covered all familymembers. The survey studied ap-proximately 1,900 plans providingdental benefits. Five-eighths of theparticipants had dental coveragethat was separate from their mainhealth insurance plan. A majorityof the participants in dental insur-ance plans in 1986 received cover-age paid entirely by their employ-ers.
Reflecting the changes in na-tional dental insurance coverage,between 1980 and 1984, there wereincreases in the proportion of allworkers with dental insurance cov-erage in medium and large firms.Similarly, there were decreases be-tween 1984 and 1986. Throughoutthe 1980s, a greater proportion ofprofessional administrative staff,had insurance coverage than didtechnical and clerical staff. In 1986,production employees had thesmallest proportion of coverage(Table VIII).
Throughout the 1980s, nearly alldental plans covered a wide rangeof services, including examina-tions, restorative procedures andperiodontal care. There was littlechange in the incidence of coverageof services except for an increase oforthodontic services (Table IX).The dental plans paid for covered
services in a variety of arrange-ments:
1. Full or partial payment ofusual, customary and reason-able charges (UCR)-This is arate that is not more than thedentist's usual charge; withinthe customary range of fees inthe locality; and is reasonable,considering the circum-stances.
2. Payment according to aschedule (list) of allowances.Unlike the UCR method,scheduled allowances do notchange automatically as a re-
VOLUME 56 NUMBER 2

DENTAL INSURANCE 7
Table V. Percent distribution of persons 2 years of age and overby various demographic characteristics and private dental
insurance status: 1 986(10)
Have privatedental
Insurance
Do nothave private
dentalInsurance Unknown
SexMale 39.2% 55.2% 5.8%Female 36.5 58.2 5.3
RaceWhite 39.0 55.8 5.2Black 29.1 64.0 6.9
Hispanic OriginNon-Hispanic 38.3 56.2 5.5Hispanic 31.3 63.0 5.7Mexican American 31.3 64.1 4.6Other Hispanic 31.3 61.7 7.0
Place of residenceMSA* 40.6 54.0 5.4Central City 35.3 58.5 6.2Not Central City 44.0 51.0 5.0
Non-MSA 28.7 65.8 5.5Geographic Region
Northeast 38.6 56.4 5.0Midwest 41.7 52.7 5.6South 30.8 62.7 6.5West 44.3 51.8 3.9
Education LevelLess than 9 yrs. 12.7 81.1 6.29-11 yrs. 24.7 69,4 5.912 yrs. 38.3 56.4 5.313 yrs. + 47.0 48.3 4.7
Family IncomeLess than $10,000 9.4 85.6 5.0$10,000-$19,999 24.9 70.0 5.1$20,000-$34,999 46.3 49.6 4.1$35,000 + 59.3 37.2 3.5
'Metropolitan Statistical Area
Table VI. Dental insurance status by dental visit pattern: 198600
NoInsurance Insurance
Number of visits per person per year 2.6 1.7Percent with 1 or more visits past year 70.1% 49.9%Percent with 2 or more visits in past year 44.5% 27.8%Last dental visit was for a check-up 48.0% 29.7%
flection developments in com-munity dental prices. On aver-age, plan sponsors did reviseschedules of allowances to re-flect increases in the price ofdental care.
3. Incentive payment-To en-courage participants to seekpreventive care, under thismethod of reimbursement,the percent of dental expensespaid by the plan increaseseach year if the participant isexamined regularly by thedentist. Preventive procedureswere more likely to be subjectto incentive schedules thancomplex restorative and orth-odontic procedures.
4. Copayment methods-Theparticipant is responsible,generally for a set percent ofcosts. Incentive programs area variation of copaymentmethods.
5. Deductibles-Participants arerequired to pay a specifiedamount of dental expenses be-fore the plan pays any bene-fits.
UCR and schedule of allow-ance programs constitute the vastmajority of all the dental insuranceplans. A major share of examina-tion and orthodontic services arecovered under UCR programs (80percent and 77 percent, respec-tively). Somewhat less of a share offillings and crowns are covered un-der UCR programs (69 percent and70 percent, respectively) (Table X).There have been some major
changes since 1980 in the financialarrangement for dental insurancecoverage. There has been a markedshift from providing benefitsthrough commercial insurance car-riers to self-funded arrangements(by the employers). Commercialcarriers provided benefits to halfthe participants in 1986; downfrom three quarters in 1980. Selffunded plans more than doubled
SUMMER 1989

8 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
Table VII. Percent distribution of persons 34 years of age and overby dentition status and the availability of private
dental insurance: 1986(10)
DentitionStatus
Have privatedental
Insurance
Do nothave private
dentalInsurance Unknown
Dentate 39.4% 55.9% 4.7%
Edentulous 18.5 74.3 7.2
Table VIII. Percent of full-time health insurance participantswith dental benefits in MEDIUM AND LARGE FIRMS:
selected years 1980-1986(1)
All
Year Participant
Professionaland
Administrative
Technicaland
Clerical Production
1980 56% 60% 55% 56%
1982 68 76 68 64
1984 77 79 75 76
1986 71 75 72 68
Table IX. Percent of plan participants in MEDIUM ANDLARGE FIRMS by dental procedure: 1980, 1983, 1986 (1)
Percent of plan participants
Procedure 1980 1983 1986
Examinations 100% 99% 100%
Fillings 100 100 100
Crowns 97 99 98
Orthodontics 62 73 75
their share of participants duringthe same period (from one fifth totwo fifth). Other arrangements,(Health Maintenance Organiza-
tion, Preferred Provider Organiza-tion and dental societies) increasedtheir minor share of participants(Table XI).
Finally, there was a wide range ofpayments (for examinations, fill-ings and crowns) under schedule ofallowance plans. As a result, inmany instances, copayment expen-ditures are required by plan partic-ipants (Table XII).
Overview
Despite the rapid expansion ofdental insurance coverage duringthe last two decades, the reality isthat by the late 1980s, dental carerecipients continue to be responsi-ble directly for 60 percent or moreof dental costs—and minimalchanges are anticipated in the de-cade of the 1990s. For many groupsin the nation, dental care costs are"felt" far more than physician ser-vices. Nevertheless, per capita ex-penditures for dental services havecontinued to rise. And it is antici-pated that this trend will continuethrough the next decade.But in addition, there are the
overall realities that:
1. unions and employees are at-tempting to increase healthbenefits,
2. employers are seeking meth-ods to control the ever in-creasing costs of health care,and
3. the federal government is con-sidering the balance betweenpolitical expediencies and theneed for added revenues fromtaxing fringe benefits.
As dentists attempt to dealwith a seemingly never ending ar-ray of evolving dental insuranceclaim forms and third party over-sight, (at times, uncertain whetherdental insurance is a blessing or acurse) they must remain currentwith the evolving patterns of insur-ance. Only then can they take the
VOLUME 56 NUMBER 2

DENTAL INSURANCE 9
Table X. Method of dental insurance reimbursement IN MEDIUMAND LARGE FIRMS by dental procedure: 1986 (1)
Procedure
Percent of plan participants covered for procedure
Total
Scheduleof cash
UCR AllowancesIncentive CopaymentSchedule Method
Table XII. Percent of full-timeparticipants in MEDIUMAND LARGE FIRM dentalplans with schedule of
allowances by maximumpayable amounts for
selected dental procedures:
Examinations 100% 80% 17% 3% <0.5%19861
Fillings 100 69 27 3 1 PercentCrowns 100 70 27 1 2Orthodontics 100 77 20 3 Examinations
$10 and under 2%$11-$20 19$21-$30 30$31-$40 24$41-$50 22
Table Xl. Percent distribution of funding arrangements IN MEDIUM $50+ 1AND LARGE FIRMS for dental insurance: 1980, 1983, 1986 (1) Fillings
Percent of plan participants $10 and under 14%$11-$15 36
Funding arrangement 1980 1983 1986 $16-20 42$21+ 8
Blue Cross-Blue Shield 5 5 6 CrownsCommercial Carrier 77 66 48 $100 and under 6%Self-funder 18 23 39 $101-$150 22HMO and other 2 5 8 $151-$200 31Total 100% 100% 100% $201+ 40
necessary steps to ensure the con-tinuance of "dentist oriented" den-tal insurance. The profession mustnever lose sight of the reality thatany reduction in employer contri-butions and/or taxation of fringebenefits could affect adversely theextent and range of dental in-surance. A
References
1. Jain, R.S. Employer-sponsored dentalinsurance eases the pain. Monthly La-bor Review, 111:18-23, October, 1988.
2. U.S. Department of Commerce, Bureauof Labor Statistics. Employee Benefitsin Medium and Large Firms, 1986. Bul-letin 2281. Washington, D.C., Govern-ment Printing Office, 1987.
3. Douglass, C.W. and Day, J.M. Cost and
payment of dental services in the UnitedStates. Journal of Dental Education,43:330-348, June, 1979.
4. Division of National Cost Estimates.National health expenditures,1986-2000. Health Care Financing Re-view, 8:1-36, Summer, 1987.
5. Personal Communication. Office of theActuary, Division of National Cost Esti-mates, Health Care Financing Adminis-tration. January, 1989.
6. Gibson, R.M. and Waldo, D.R. Nationalhealth expenditures, 1980. Health CareFinancing Review, 3:1-54, September,1981.
7. Gibson, R.M. and Waldo, D.R. Nationalhealth expenditures, 1981. Health CareFinancing Review, 4:1-35, September,1982.
8. U.S. Department of Commerce. Projec-tions of the Population of the UnitedStates, By Age, Sex, and Race: 1983 to2080. Current Population Reports, Se-
ries P-25, No. 952. Washington, D.C.,Government Printing Office, May, 1984.
9. Waldman, H.B. Favorable economicpredictions. Journal of the AmericanCollege of Dentists, 55:4-7, Fall, 1988.
10. U.S. Department of Health and HumanServices. Use of Dental Services andDental Health, United States: 1986.Data from the National Health Survey,Series 10, No. 165. DHHS Pub. No.88-1593. Washington, D.C., Govern-ment Printing Office, October, 1988.
11. Health Insurance Association of Amer-ica, 1988 Update: Source Book ofHealth Insurance Data. Washington,D.C., 1988.
Reprint requests to:Dr. H. Barry WaldmanSchool of Dental MedicineState University of New YorkStony Brook, NY 11794-8715
SUMMER 1989

10 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
ADHESIVE BONDING OFCOMPOSITES
R. L. Bowen*F. C. Eichmiller**W. A. Marjenhoff***N. W. Rupp****
Since the introduction of com-posite restorative materials ap-proximately 25 years ago, the con-servation of tooth structurehistorically removed for retentionform, resistance form, and exten-tion for prevention, has been anincentive for much research to de-velop durable adhesive bonding.The strength and durability of
bonds to enamel have been ade-quate for numerous clinical proce-dures for many years. Even beforethe invention of dental composites,Dr. Michael Buonocore pioneeredtechniques for filling and sealingdevelopmental pits and fissureswith synthetic resins available atthat time.' Regenos and other den-tal clinicians instituted the etchingof enamel in and around cavitypreparations and discovered thatfractured incisors could be re-paired and restored promptly andesthetically without preparing den-tin for retention form." Methodswere also developed to use acidetching and resins to bond orth-odontic brackets directly to teeth, aprocedure with several advantages
Received February 21, 1989Accepted March 25, 1989*Rafael L. Bowen, DDS, Director**Frederick C. Eicluniller, DDS, Chief Re-
search Scientist***William A. Marjenhoff, Special Pro-
jects Coordinator****Nelson W. Rupp, Associate Director
EmeritusAmerican Dental Association Health
Foundation, Paffenbarger Research Center,National Institute of Standards and Tech-nology, (formerly National Bureau of Stan-dards)
Although the strength anddurability of adhesive bondsto enamel have been adequatefor numerous clinical pro-cedures for many years,commercial products whichdemonstrate a range of effec-tiveness for adhesion to den-tin are relatively new.This paper discusses sev-
eral of the more popular com-mercial dentin and enamelbonding systems, noting dif-ferences in their chemicalcomponents and instructionsfor use. Since simple tech-nique errors can lead to fail-ure, it is important that prac-titioners understand not justthe sequence of protocolsteps, but the function of eachsystem component.
Dentists are encouraged totry dentin and enamel adhe-sives supported by researchliterature in refereed journalsto determine which worksbest for them, and to providefeedback to dental manufac-turers and researchers so thatthese materials and clinicaltechniques can be further im-proved.
over the cementing of bands.' Andthe list goes on. It would be a veryprotracted review to cite all of thecontributions of dedicated re-search scientists to adhesive bond-ing technology. Vast support forthese endeavors has been provided
by the National Institute of DentalResearch, the National Institute ofStandards and Technology, theuniversities, the American DentalAssociation, and other organiza-tions.A result of these contributions is,
in a word, information. It is on thisfoundation of information thatnew and successful products andtechniques are built. For example,the bonding of dental resins toetched enamel has changed from asimple micromechanical interpen-etration of the resin with the rough-ened enamel surface, analogous tomicroscopic riveting, to adhesivebonding that combines mechani-cal interpenetration with specificchemical interactions, perhapsanalogous to riveting plus welding.With the latter, bond strengths arenearly doubled.'The more challenging and there-
fore more exciting problem of ad-hesive bonding of composite resinsto dentin is being met. Products arenow commercially available whichdemonstrate a range of effective-ness for adhesion to dentin. Someare effective with both dentin andenamel simultaneously; this makesthe procedure much more conve-nient for the dentists as comparedto the more difficult method oftreating dentin and enamel as iso-lated surfaces when, in fact, theyare intimately associated in mostlesions.
Eventually there may be one"best" formulation, but currentlythere is no concensus on what thatmight be. The technology is evolv-ing so rapidly that we can expectfurther improvements in the short
VOLUME 56 NUMBER 2
ADHESIVE BONDING OF COMPOSITES 11
term. One consequence of thisrapid development is that longitu-dinal clinical studies of the variousadhesion systems have not beencompleted. In most cases, theyhave barely begun. Most dentistsdo not wish to be the first by whichthe new is tried nor the last to laythe old aside. However, the practi-tioner must continually use profes-sional judgment to draw the linebetween "experimenting" with newproducts, with concern that somemay have had less than ideal re-search done before marketing, andfailing to keep up with valuableadvances in dental therapeutics.Some products have directions
for use that are inadequate in detailor contain terms that are some-times subject to misinterpretation.For example, the word "rinse" tosome dentists means for the patientto use a cup of water, and to otherdentists indicates the use of a watersyringe and a high volume aspira-tor. Using the latter technique in anadhesive bonding procedure, pro-vided there is absolutely no con-tamination, can lead to successfulresults. The rinse with a cup ofwater would allow the organic sol-utes in saliva (that normally de-velop the salivary pellicle) or otherimpurities to adsorb onto the sur-face barring the effective attach-ment of adhesion-promoting ingre-dients.Adhesive bonding materials are
extremely sensitive to variations intechnique. Success of restorationsplaced with these adhesives wouldseem to be as dependent on opera-tor technique as on the composi-tions of the products. Therefore,both the clinical and market suc-cess of these products will dependupon the completeness of instruc-tions and on how accurately theseare followed by dental practitio-ners.Probably no other area in den-
tistry requires continuing educa-tion more than that of adhesivebonding techniques for use with
composite resins. The larger dentalmeetings usually have at least oneclinician or researcher lecturing onmaterials and methods for adhe-sive bonding of composites. An-other source of information is theAmerican Dental Association'sCouncil on Dental Materials, In-struments, and Equipment; thissource is available on the ADA toll-free WATS line, (800) 621-8099.Because of the continually growinginterest in the subject, there is alsoan abundance of valuable informa-tion in refereed dental journals.The following description of a
few dentin and/or enamel bondingproducts is not intended to conveyimplications of relative merit, butrather to provide some understand-ing of the materials and methods.What might be most noteworthy isthe fact that each of the systemsdescribed uses distinctly differentformulations of chemical compo-nents to achieve the same purposeof bonding dental resins with phys-icochemical interactions to thehard tooth tissues.One recent product is Scotch-
bond 2TM (3M Co., St. Paul, MN),a two-component dentin/enamelbonding system consisting of adentin primer and a light-curingadhesive resin.* The Dentin Primeris an aqueous solution of maleicacid and a hydrophilic methacry-late monomer (hydroxyethyl meth-acrylate, HEMA).The clinical technique involves
cavity preparation followed byetching of enamel (if present in thepreparation), followed by waterrinsing and air drying.The entire preparation surface is
*Although certain commercial materialsare identified in this paper, in no instancedoes such identification imply recommen-dation or endorsement by the National Insti-tute of Standards and Technology or theAmerican Dental Association Health Foun-dation or that the materials identified arenecessarily the best available for the pur-pose discussed.
then bathed with the Dentin Primerfor 60 seconds followed by air dry-ing without rinsing. The acid com-ponent of the Dentin Primer func-tions to remove the dentin smearlayer in a controlled manner. Themanufacturer claims that the sur-face smear layer is removed whilethe smear plugs are left in the tu-bule openings, thus limiting pene-tration of acid or resins. The HEMAcomponent of the Dentin Primerfunctions as a surface conditioner,one end of the molecule interactingwith the hydrophilic tooth surfacewhile the other end reacts withhydrophobic monomers.The Light Cure Dentin Adhesive
consists of HEMA, hydrophobicmonomer BIS-GMA, a photoinitia-tor, and a viscosity modifier. A uni-form coat of 75 to 100 micronsthickness of Light Cure Dental Ad-hesive is placed with a brush andlight cured for 20 seconds. Com-posite resin is then placed directlyon the adhesive surface and cured.The Light Cure Dental Adhesivecontains HEMA and BIS-GMAwhich copolymerize with theHEMA laid down by the DentinPrimer. This resin is light cured in arelatively thick (75-100 micron)layer prior to placement of the re-storative material. Oxygen inhib-ited monomer on the adhesive sur-face copolymerizes with monomerin the restorative resin to completethe coupling of tooth surface to therestorative composite.The original ScotchbondTM pro-
vided for strong adhesion of resinto etched enamel with relativelyweak bonds to dentin. However,Light Cured Scotchbond 'I was ef-fective in retaining 97% of the in-crementally-placed SiluxTM restora-tions in Class V "dish-shaped"cavities for one year.' Scotchbond2" is claimed by the manufacturerto be a further improvement in theevolution of this product.The GLUMAT" bonding system,
developed by Drs. C. E. Munks-gaard and Eric Asmussen, has been
SUMMER 1989

12 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
on the European market for severalyears and was recently introducedinto the U.S. market by ColumbusDental (St. Louis, MO). TheGLUMAT" 1 Etchant consists of agel of phosphoric acid which isused to etch enamel for 20-30 sec-onds; the enamel is then washedand dried prior to treatment ofdentin.The GLUMA" 2 Cleanser con-
sists of a dilute solution of EDTA (asodium salt of ethylenediamine-tetra-acetic acid) which, accordingto the manufacturer's claims, re-moves the smear layer leavingsmear plugs in the tubule openingsto prevent penetration. It is appliedfor 30 seconds and then the surfaceis washed and dried.GLUMAT" 3 Primer solution,
containing 5% glutaraldehyde and35% HEMA in water, is applied for30 seconds and then blown dry to athin layer without rinsing. Themanufacturer claims glutaralde-hyde interacts directly with theamine groups of dentin collagenforming groups that then bondchemically with the HEMA and ad-hesive resin.GLUMA" 4 Sealer is a bonding
agent composed of a methacrylatemonomer system which copolyer-mizes with the surface HEMA. Themonomers in the restorative com-posite overlay this resin and all arepolymerized simultaneously bylight activation.Tenure' (Den-Mat Corp., Santa
Maria, CA) utilizes an oxalate sys-tem similar to one developed in theADA's Paffenbarger Research Cen-ter at the National Institute of Stan-dards and Technology.f A second
tA nonexclusive domestic license of theapplicable patents is currently in force be-tween Den-Mat Corporation and the Ameri-can Dental Association Health Foundation.
generation product was introducedto simplify the original treatmentprotocol. The Tenure" DentinConditioner uses a dentin-enameletchant consisting of a dilute nitricacid solution with a small amountof aluminum oxalate. It is claimedthat the acid removes the smearlayer on dentin while leaving a pre-cipitate of reaction products in thedentinal tubules. Enamel is etchedsimultaneously by the nitric acid ina pattern similar to etching withphosphoric acid.The second generation Tenure"
bonding agent consists of two pow-ders, A and B, which are mixedwith a solvent, Tenure" Liquid,prior to application. It is claimedthat Powder A contains the acidicform of NTG-GMA plus a sodiumsalt of this surface active comono-mer, which is capable of initiatingthe polymerization of the subse-quently applied monomer. PowderB is PMDM, a monomer capable ofinteracting with the altered toothsurface while copolymerizing withother PMDM molecules and restor-ative resin monomers. TheTenure" Liquid is an acetone-water solvent used to solubilize thepowdered components for applica-tion.According to the "two-minute"
clinical protocol, after cavity prep-aration, Tenure' Dentin Condi-tioner is applied to the enamel anddentin for 30 seconds, the surfacewashed with clean water for 30seconds and completely dried withan air syringe. Powders A and B aredispensed into a small dish andmixed with three drops of Tenure'Liquid. The dissolved mixture isthen applied to the surface with abrush, the application repeated,and the surface allowed to dry byevaporation of the solvent. Com-posite or other resins can then be
applied directly to the surface andwill copolymerize with the surface-bound PMDM.A third generation product, Ten-
ure Solution' , has now becomeavailable which appears to be simi-lar, except that components A andB are now premixed solutionswhich are combined and applied asbefore.Another new product based on
Paffenbarger Research Center re-search is Mirage Bond' dentin-enamel adhesive (Myron Interna-tional, Inc., Kansas City, KS).f Thismaterial is being initially marketedas an adhesive applied to both den-tin and enamel to bond ceramicrestorations.Part 1 of the adhesive is a solu-
tion of 2.5% nitric acid with 4%NPG (N-phenylglycine). The nitricacid serves to remove smear layerand simultaneously etch enamelwhile the NPG is a surface activedentin conditioner capable of initi-ating the polymerization of thesubsequently applied monomer.This solution is applied to dentinand enamel for 60 seconds, theexcess blown away, and the surfacedried without rinsing.Part 2 of the adhesive is a pre-
mixed 5% solution of PMDM, ahydrophilic monomer, dissolved inan acetone solvent. This solution isapplied to the previously condi-tioned surface and the solvent al-lowed to evaporate prior to applica-tion of resin, composite, or resinbased luting agent.Although these various adhesive
systems contain few common in-gredients, some of the principles
tA nonexclusive domestic license of theapplicable patents is currently in force be-tween Myron International, Inc. and theAmerican Dental Association Health Foun-dation.
VOLUME 56 NUMBER 2

ADHESIVE BONDING OF COMPOSITES 13
utilized are the same. All contain anagent capable of removing a verythin surface layer from dentin and/or enamel. Adhesion to the "smearlayer" can never give bondstrengths that exceed the low cohe-sive strength or weak attachment ofthe smeared layer to the underlyingdentin or enamel. Removal of weaksurface layers is necessary toachieve the presently experiencedhigher values. All these adhesivesystems contain functional com-pounds which can, at least theoret-ically, form chemical bonds tocomponents of the tooth. And also,all of these systems contain mono-mers that are capable of copoly-merizing with restorative resins.Product component and proce-
dural variations make it impera-tive, however, that the operator un-derstand not just the treatmentsequence but the function of eachof the agents to achieve effectiveresults. Rinsing after the applica-tion of Scotchbond 2" DentinPrimer would remove the HEMAand eliminate adhesive interactionwith subsequent resins. The sameis true if water were applied afterthe application of GLUMA' 3Primer. Air thinning of the Scotch-bond 2TM Light Cure Dental Adhe-sive to a thickness of less than 75microns would cause excessive ox-ygen inhibition and prevent surfacepolyermization and subsequent ad-hesion. These are only a few exam-ples of simple common techniqueerrors which can lead to failure.Again, it should be clear in theoperator's mind not just what to doin each step of the procedure butwhy each is performed.In addition to the adhesion sys-
tems described above, there areseveral other dentin adhesion prod-ucts which remain popular, includ-ing Prisma Universal Bond"
(Caulk, Milford, DE), BondliteTM(Kerr, Romulus, MI), and DentinAdhesitTM (Vivadent, Tonawanda,NY). These are unfilled resins withchemical additives that promotebonding to dentin and/or etchedenamel. These adhesives are nowprimarily advocated for the protec-tion of dentin during enameletching.7The protocols described for these
materials demonstrate only the dif-ferences in application of the adhe-sive materials. Isolation, prepara-tion, and pulpal protection muststill follow the basics of good oper-ative technique. Near perfect isola-tion is a necessity with these mate-rials since any fluid contaminationduring application will severelycompromise the results. If contam-ination should occur, each protocolshould be repeated from the begin-ning without skipping over any ofthe steps. Until clinical effective-ness of these adhesives can beproven, preparation design shouldstill contain basic resistance andretention form with adequate pul-pal protection of very deep areaswith the appropriate calcium hy-droxide liners. The necessity of lin-ing all dentin surfaces with calciumhydroxide or glass ionomer, how-ever, should no longer pertain.
Ultimately, both the clinical andmarket success of adhesive prod-ucts will depend on clinical resultsexperienced by dental practitio-ners. To determine which performsbest for them, dentists must bewilling to use dentin and enameladhesives for which there is sup-portive research literature in re-fereed journals. Then, feedbackfrom dentists to dental manufac-turers and researchers is critical forfurther improvement of the materi-als and clinical techniques.The advancement of adhesive
bonding technology holds greatpromise for both preventive andrestorative dentistry. Restorationsplaced without retention formcould result in less drilling per fill-ing, thus preserving more vitaltooth tissue and lessening the needfor anesthetics. Reduced treatmenttime is less fatiguing for dentistsand more comfortable for patients.Broader applications of this tech-nology are already being developedfor tooth desensitization, bondedceramic restorations and protec-tive root coatings. A
References
1. Buonocore, M.G., A Simple Method ofIncreasing the Adhesion of Acrylic FillingMaterials to Enamel Surfaces. J Dent Res34:849-853, 1955.
2. Lasswell, H.R.; Wald, D.A.; and Regenos,G.W., Attachment of Resin Restorationsto Acid Pretreated Enamel. JADA 82:558-563, 1971.
3. Doyle, W.A., in Current Therapy in Den-tistry, Chapter 38, Volume 3, St. Louis: C.V. Mosby Co., 1968; and Doyle, W. A., inDental Clinics of North America, p. 93,Philadelphia: W. B. Saunders Co., 1973.
4. Newman, G.V.; Snyder, W.H.; and Wil-son, C. E. Jr., Acrylic Adhesives for Bond-ing Attachments to Tooth Surfaces. AngleOrthodont 38:12, 1968.
5. Bowen, R.L.; Cobb, E.N.; and Setz, L.E.,Recently Developed Concepts in Adhe-sive Bonding of Composites to Dentinand Enamel. Buffalo Dental Review1:10-12, 1984.
6. Sheth, J.J.; Jensen, M.E.; Wefel, J.S.; andLevy, S.M., Restorations of root carieswith dentinal bonding agent and micro-filled composite resin: 1-year clinicalevaluation. Gerodontics 4:71-77, 1988.
7. Clinical Research Associates Newsletter12(2):2, February 1988.
Reprint requests to:Dr. Rafael L. Bowen, DirectorADA Health FoundationPaffenbarger Research CenterNational Institute of Standards andTechnologyGaithersburg, MD 20899
SUMMER 1989
14 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
THE PLACEBO EFFECT
The Placebo Effect in the Management of ChronicMyofascial Pain: A Review
John W. Stockstill*
The term "placebo" has been de-fined and used since 18111 to meana medicine given more to please thepatient than to benefit him. It hasbeen frequently referred to as apharmacologically inert substancethat was administered to the pa-tient to relieve his or her stresswhen the physician did not wish touse "actual" medication.' However,an "exact" placebo is one that mim-ics all the physical characteristicsof the experimental substance ortreatment, and may be consideredto be active (noninert) or inactive(inert).3 In terms of experimentalanalysis and observation, a placebois "a tool to distinguish pharmaco-logical effects of suggestion and toobtain an unbiased assessment ofthe results of the experiment."' Byformal definition, the placebo canbe classified as "an inactive sub-stance or preparation, formallygiven to please or gratify the pa-tient, now also used in controlledstudies to determine the efficacy ofa medical substance."'
Distinction should be made be-tween the "placebo effect" and the"placebo response." The placebo ef-fect refers to "that portion of thebehavioral change which can beattributed to the symbolic transac-tion of being given medication, ascontrasted with the behavioral
Received November 4, 1988Accepted February 6, 1989*John W. Stockstill, DDS, MS, University
of Nebraska Medical Center, College of Den-tistry, Department of Adult Restorative Den-tistry
The placebo effect has, un-til recent times, been inauspi-ciously misinterpreted or ne-glected as a key variable inbasic human clinical investi-gations. Its role in the healingresponse has been questionedand debated for centuries, butonly within the last thirtyyears has it become a moreclearly defined therapeuticphenomenon.Of special interest to den-
tistry is the application of theplacebo in clinical studies, es-pecially those studies investi-gating the treatment ofchronic myofascial pain. Spe-cifically, the placebo effecthas been incorporated as astandard in the design ofmany splint, pain manage-ment, and subjective pain re-sponse studies.The intent of this literature
review is to shed some lightupon the placebo effect andits role in the investigation,immediate treatment, andextended management ofchronic myofascial pain.
change due to mere passage oftime, repeated testing, or other'spontaneous' influences occurringwhile on placebo." Both terms areused interchangeably.'
Historically, before the onset of"modern" pharmaceutical involve-ment in medicine, many "medica-tions" were, in fact, placebos in the
literal sense that the actual phar-macological and medicinal mecha-nism(s) of the drugs were largelyunknown or misunderstood.' Butthe patient was "given" the sub-stance (usually by a learned personsuch as a physician) and often gotbetter as suggested, with the pa-tient's expectations (following thesuggestion) becoming their reality.Therefore, the history of medica-tions in healing prior to modernexperimental pharmacological andpsychological techniques can be at-tributed in part to the placebo ef-fect.In a speech before The Royal
Society of Medicine in 1953, J.H.Gaddum redefined the terms"dummy medication" (that whichis intended to have no effect) and"placebo."' While the dummy tab-let was given simply to "have noeffect" and be neutral in its func-tion, the placebo was recognized asbeing able to possibly cause psy-chological or physical changesthrough therapeutic suggestionand the strength of symbolism.What is interesting is that the twoterms, "dummy" and "placebo,"were used independently and whileone was taken to mean "have noeffect-dummy," the other wasthought to be capable of producingat least some type of change, albeita change of unpredictable nature.Eventually, the two terms wereconsolidated into the more com-monly used "placebo." However, aquestion still remained as to themechanism or interrelationship ofthe mental suggestion and the ob-servable physical change.
VOLUME 56 NUMBER 2

THE PLACEBO EFFECT 15
Another commonly accepted ob-servation was the concept of place-bos and physiologic effects. Prior to1955, it seemed that most membersof the medical community hadsome understanding of the role ofthe placebo in both clinical treat-ment and research. The placebowas expected to have no physiolog-ical effect as, for example, in painrelief. It was simply used to screenout those reacting to it in order tomore clearly interpret laboratoryor clinical results. The consolida-tion of the terms "dummy" and"placebo" into simply "placebo" byBeecher in 1955 actually ushered inthe dual concepts of the psycholog-ical as well as physical changes thatcould be elicited in a patient. Also,the implication of psychologicalsuggestion and its impact on physi-cal changes were now being madeand became a part of the newand growing "psychophysiological"school of thought.A basic understanding of possi-
ble mechanisms of action of bothpain systems and the placebo mustbe in hand before logical argu-ments and conclusions can bedrawn concerning their interrela-tionship.
PAIN
By definition, pain is "a more orless localized sensation of discom-fort, distress, or agony, resultingfrom the stimulation of specializednerve endings.5 In addition, pain isa subjective experience involvingsensory and emotional influencesassociated with actual or potentialtissue damage. Perception of pain(nociception) is dependent upondefinite physicochemical and neu-rologic modes of transmission aswell as the psychological makeupof the individual. These psycholog-ical elements play a much greaterpart in chronic pain than in acutepain, which is predominantlyviewed as being heavily influencedby the initial response to nocicep-tive stimuli.4'7 Psychological fac-tors such as conditioning, learned
pain behavior, past experiences,anxiety, and depression all play im-portant roles in the perception andmanagement of pain, especiallychronic pain, where these determi-nants seem more critically in-volved."The mechanism of action of the
placebo in the pain response maybe explained as being a combina-tion of neurophysiological and psy-chological factors. Explanationsfor its role(s) in nociceptive re-sponses have included neurochem-ical reactions involving the releaseof endogenous opiates9 as well asfluctuations in catecholaminesand steroid levels.'
Psychological involvement in theplacebo effect has been examinedin the doctor-patient relation-ship1413 and can be extremely de-pendent upon the psychologicalmake-up of the individua114-16 as
well as the expectations of thepatient.2'4'7.1.7 Therefore, it seemsquite appropriate to label the pla-cebo effect in pain perception andresponse as being a combination ofneurochemical and psychologicalfactors, neither being independentof the other.
STUDIES
The focus of much attention indental research over the pasttwenty years has been on the psy-chophysiological factors involvedin temporomandibular joint disor-ders (dysfunction) and chronic my-ofascial pain. Reports on TM disor-der treatment have included theuse of medications, surgery, orcombinations of both,18-2° as wellas "no treatment" interventionsuch as mock equilibration.' Psy-chological management of chronicmyofascial pain has been heavilydocumented and involves the tech-niques of counseling, hypnosis,biofeedback, and behavior mod-ification:7'22'23A factor common to all of these
intervening techniques has beenthe introduction of the placebo as aform of comparison and as means
of ruling out nonintervention re-sponses. Since chronic pain can berelated to anxious or depressivestates and since these states appearto be susceptible to placebotherapy,24,25 it seems logical to ex-perimentally test the effects oftreatment modalities (both "real"and placebo) in terms of their inde-pendent effects as well as their in-teractions with each other. The fol-lowing studies attempted toexercise this logic in terms of thechronic facial pain associated withTM disorders such as MyofascialPain Dysfunction.
I. MEPROBAMATE STUDY
Medication studies abound inthe literature on pain control, andseveral seem particularly pertinentin the treatment of chronic myofas-cial pain. In 1971, Greene andLaskin studied the effects of Mep-robamate, a combinationtranquilizer/muscle relaxant, onMPD syndrome.26 Ninety patientswith MPD syndrome were ran-domly selected and were assignedto an initial "Meprobamate only"group or "placebo only" group. Afour day supply of medication wasdispensed in a double-blind man-ner. Patients were instructed to re-turn on the fifth day at which timethey either received the same medi-cation or were "switched over" tothe second group for another fiveday period. During the course ofthe study, the patients were askedto assess the intensity of eight sub-jective symptoms (such as mastica-tory muscle pain and joint pain) aswell as three objective symptoms(clicking, crepitation, etc.) on atreatment evaluation form. Tosummarize results, 58% showedimprovement using Meprobamateand 31% showed improvement tak-ing the placebo. Subjective symp-toms improved most frequentlyand objective symptoms seemedless affected by either drug. Thepossibility of the lingering effectsof one drug on another were takeninto account by the authors. No
SUMMER 1989

16 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
attempt was made to classify pa-tients as being acute or chronicmyofascial pain patients.
II. SPLINT STUDY
In addition to the use of medica-tion, other treatment techniqueshave been investigated relative tomyofascial pain and the placeboresponse. Greene and Laskin(1972) examined the efficacy ofthree different types of splints inthe treatment of myofascial pain ina mixed group of acute and chronicpain patients.' The splint designsincluded full arch coverage, ante-rior coverage only (cuspid to cus-pid), and a placebo splint coveringonly the palate with no extensionover dental arches. Seventy-one pa-tients with MPD symptoms (masti-catory muscle pain, limitation, de-viation on opening) were chosenfor participation. Each patient wasgiven the non-occluding splint towear for 1-2 weeks. If the patientsreceived relief with the placebo(non-occluding) splint, they wereallowed to continue in the study ordiscontinue treatment (NOTE: 11chose to discontinue). Those whoreported no improvement movedon to the anterior platform splint.The full coverage splint was wornby those patients receiving little orno symptom relief with the firsttwo splints.
Results indicate that 28 of 71patients (40%) received some im-provement of symptoms with thenon-occluding placebo splint.Thirty of 60 patients (50%) im-proved with the anterior platformsplint, and 35 of 44 patients (80%)showed improvement after wear-ing the full coverage splint. Thedesign of this experiment resem-bles to some degree a triple-blindprocedure where a preliminary
study with placebos is carried out,after which the placebo reactorsare excluded for the remainder ofthe study. Even though the aim ofthis design attempts to exclude orreduce placebo effects, it is inter-esting to note that in most experi-mental settings, a placebo is effec-tive between 30-66% of time,regardless of preventive measurestaken.3•6The authors' findings indicate
that certain splint designs may besuperior to others in terms ofsymptom relief. They also point outthe potential psychological effectsof a placebo in that 40% of theparticipants reported some im-provement with a non-occludingsplint. In other published studies,there seems to be a strong tendencyfor many MPD patients to respondpositively to placebo therapies; thatis, an improvement in subjectivesymptoms but little or no improve-ment in signs of the disorder.21'28Several experimental issues seem
open to question. No time period isgiven for "duration of symptoms"prior to testing. In fact, the testgroups could be assumed to bemixtures of both acute and chronicmyofascial pain patients. Stern-bach (1978) and Turk (1983) havepostulated that responses to acuteand chronic pain are, in fact, quitedifferent.7•8 This difference in re-sponse to nociceptive stimuli couldpossibly be manifested in totallydifferent responses to treatment,causing questions to be raised con-cerning "improvement" data. Re-garding splint design, an argumentcould be made in defense of thenon-occluding placebo splint. In anexcellent review of intraoral appli-ance design and theory, Clark(1984) raised the issue of "cognitiveawareness" with respect to any typeof corrective device being worn by
the patient. The presence of anyintraoral appliance may constantlyremind the patient to alter usual orparafunctional behavior. Thismodification may decrease harm-ful or abnormal masticatory mus-cle activity exhibited at anytime ofday or night, resulting in eventualpain reduction. Hypothetically,"learning to alter, reduce, orchange a harmful behavior is ageneral theory that applies to mostsuccessful therapeutic interven-tions."'
III. REVIEW OF STUDIES
A very thorough assessment ofseveral studies over a period of 11years involving standard reversibletechniques and placebos in thetreatment of MPD was reported byGreene and Laskin (1983). Themain objective was to correlate thepatients' long-term status to theirinitial treatment response. Treat-ment techniques included splints,biofeedback therapy, medication,mock equilibration, and placebos.All treatments were considered re-versible and all treatments requiredsome cooperation and active par-ticipation from the patients. Analy-ses of results indicated that at theend of treatment, 74% of 175 pa-tients were greatly improved orsymptom free, 25% showed little orno improvement, and 1% were ac-tually worse. On the follow-up in-terview, 53% were symptom freeand 37% reported occasional orminor symptoms. Furthermore,8% said their condition was thesame as before treatment, and 2%reported feeling worse. (NOTE:The authors combined "symptomfree" and "minor symptoms" intoone group having a 90%improvement.)30No indication is given of how
many patients reporting were in
VOLUME 56 NUMBER 2

THE PLACEBO EFFECT 17
the actual placebo groups. In orderto draw logical conclusions on pla-cebo effectiveness, it would be in-teresting to see what percentage ofthe total number responding weregiven placebo treatment, and mightthis placebo group make up theusual 33-66% of patients respond-ing positively to a placebo.An additional question to ad-
dress in similar studies would bewhat percentage of patients "getbetter" or improve over time inde-pendent of treatment selected. Theinteraction of time coupled withpsychological support (doctor-pa-tient relationship) has been investi-gated to some degree but furtherinvestigation into "time" and thecyclic remission of pain should beundertaken.12
PROBLEMS AND PITFALLS
The placebo, by definition, is in-ert chemically and its makeup ren-ders it "unreactive." Beecher addedthat the strength of the placebo didnot come from how much wasgiven or how long it was taken, butcame from the patients' mental ex-pectations as well as the undetect-able nature of the placebo by theobserver or subject.4 Frank at-tributes the strength of the placeboto this same "hope of relief' held bythe patient and states that‘'symptom relief and improvedfunction are intimately related toincreased satisfaction and dimin-ished frustration" brought on byintervention.2 However, the prob-lem arises when full disclosure ofdouble-blind design is made to aparticipant. In other words, when apatient becomes aware of the na-ture of a double-blind study (medi-cation vs. placebo, for example), heor she is in fact informed to somedegree that "some of the patients
will get the real medication andothers will get the control." Thisidea of "openness" or being honestdoes in fact suggest that the patientmay or may not receive a control orplacebo. To follow Beecher's line ofreasoning, the unique ability of aplacebo to be used to study thereaction or processing componentof suffering seems to be a bittainted in that the slightest sugges-tion of its possible use on a patientcould modify that particular pa-tient's eventual response and treat-ment outcome. Thus, in being can-did and as straightforward as onecan be with patients in an experi-mental setting, the strength of theplacebo can be reduced or com-pletely lost, dependent on the de-gree of information given and themental acuity of the patient in "per-ceiving" change in a condition suchas chronic myofascial pain.In addition, significant differ-
ences in personality structure ofthe individual may be suggestive oftheir statistically falling within ei-ther placebo reactor or non-reactorgroups. Aberrations in personality(depressive, anxious, or neuroticconditions have been found to bestrongly suggestive of how patientscan be expected to react to place-bos. For example, in the absence ofverbal suggestion by the attendingclinician, placebo responderstended to be those asymptomaticindividuals previously diagnosed asbeing depressed and hypochondri-acal. However, following strongverbal suggestion, the placebo re-sponders tended to be those sub-jects previously classified as beingmore neurotic and hysterical."Social and emotional character-
istics of patients may also play arole in response to placebos. Forexample, self-reliant, independentindividuals were found to respond
more favorably to placebo inter-vention. Those subjects classifiedas leading lifestyles of reduced self-reliance and responsibility reactedunfavorably (nonresponder) to theprescribed placebo.'
SIDE EFFECTS
Just as all drugs have "beneficial"aspects, placebos are no differentin exhibiting side effects. These in-clude nausea, itching, headache,and drowsiness. Several investiga-tors, including Wolf, have recordedthese side effects in similar studiesand describe these "placebo reac-tions" as being "objective changesat the end organ which may exceedthose attributable to potent phar-macological action."3 Also, an in-teresting point is made by J.D.Frank in his text Persuasion andHealing (1961) concerning placeboside effects. He hypothesizes that,since some patients fear drugs andmistrust doctors, this pain and mis-trust could be strong enough tocause severe physiological changessuch as nausea, itching, anddiarrhea.2Although the pertinent psycho-
logical factors of fear and distrustmust be included in explaining neg-ative side effects, one area lackingin suggestive information is that ofpatient tolerance to the placebo it-self. Since lactose seems to be theplacebo of choice for human medi-cation studies, there would seem tobe a valid question regarding its usein lactose intolerant patients. Thesepatients exhibit bloating, nausea,and diarrhea when exposed tomoderate amounts of lactose.'Unfortunately, there seems to belittle if any published informationconcerning the use of a lactose ver-sus non-lactose placebo to accountfor possible lactose intoleranceproblems.
SUMMER 1989

18 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
CONCLUSION AND SUMMARY
The clinical effectiveness of pla-cebo has been demonstrated inmany experimental situations. Theplacebo may function in a physio-logical manner by stimulating orenhancing the release of endoge-nous opiates of the midbrain. Itspsychological role in healing maybe due to one or more of the follow-ing: the patient's expectations, cog-nitive awareness, doctor-patient re-lationship, or the suggestive natureof prescribed medication. The pla-cebo seems to be most effectivewhen the painful or stressful condi-tion is most severe, and its potencyseems to be greater when the paincomplaints are acute rather thanchronic.To conclude, in terms of the pla-
cebo effect in pain patients, partic-ularly chronic pain patients, "non-specific or placebo effects appearto be one of the most potent, butlargely underrated therapeutic mo-dalities available to every clinicalsituation."" A
References
1. Gaddum, J.H., Walter Earnest DixonMemorial Lecture: Clinical Pharmacol-ogy, Proc. Roy. Soc. Med., 47:195-204,1954.
2. Frank, J.D., Persuasion and Healing,Johns Hopkins Press, 1961.
3. Jospe, M., The Placebo Effect in Healing,D.C. Health Publishers, 1978.
4. Beecher, H.K., The Powerful Placebo,JAMA, pp. 1602-1606, Dec. 24,1955.
5. Dorland's Illustrated Medical Dictio-nary, 24th Edition, 1965.
6. Epstein, J.B., Understanding Placebosin Dentistry, JADA, 109(1):71-74, July1984.
7. Sternbach, R.A., The Psychology of Pain,Raven Press, New York, 1978.
8. Turk, D.C., Meichenbaum, D., and Ge-nest, M., Pain and Behavioral Medicine:A Cognitive-Behavioral Perspective, Guil-ford Press, New York, 1983.
9.
10.
11.
12.
13.
14.
20.
21.
22.
Levine, J.D., Gordon, N.C., and Fields,H.L., The Mechanism of Placebo Anal-gesia, Lancet, pp. 654-657, Sept. 23,1978.Clark, G.T., Rugh, J.D., and Handleman,S.L., Nocturnal Masseter Muscle Activ-ity and Urinary Catecholamine Levels inBruxers, J Dent Res, 59:1571-1576,1980.Selye, H., The General Adaptation Syn-drome and the Disease of Adaptation, JClin Endocrinol, 6:117,1940.Laskin, D.M., Greene, C.S., Influence ofthe Doctor-Patient Relationship on Pla-cebo Therapy for Patients with Myofas-cial Pain-Dysfunction (MPD) Syn-drome, JADA, 85:892-894,1972.Evans, F.J., The Placebo Response inPain Control, Psychopharmacol Bul.,17(2):72-76, April 1981.Shipman, W.G., Greene, C.S., Laskin,D.M., Correlation of Placebo Responsesand Personality Characteristics in Myo-fascial Pain-Dysfunction (MPD) Pa-tients, J Psychosomatic Res, 18:475-483,1974.Moertel, C., Taylor, W. Roth, A., Tyce,F., Who Responds to Sugar Pills? MayoClin Proc, 57:96-100,1976.Wilkins, W., Psychotherapy: The Power-ful Placebo, J Con Clin Psycho!,52(4):570-573,1984.Gowdey, C.W., A Guide to the Pharma-cology of Placebos, Can Med Assoc J,128:921-925, April 15,1983.Henny, F.A., Surgical Treatment of thePainful Temporomandibular Joint,JADA, 79:171-177, July 1969.Kochan, E., Treatment of Temporo-mandibular Joint Disturbances withHyaluronidase, J Oral Surg, 9:513, May1956.Poswillo, D., An Experimental Investi-gation of the Effects of Intra-ArticularHydrocortisone and High Condylec-tomy on the Mandibular Condyle, J OralSurg, 30:161, Aug. 1970.Goodman, P., Greene, C.S., Laskin,D.M., Response of Patients with Myo-fascia] Pain-Dysfunction Syndrome toMock Equilibration, JADA, 92:755-758,April 1976.Dohrmann, R.J., Laskin, D.M., Treat-ment of Myofascial Pain-DysfunctionSyndrome with EMG Biofeedback, JDent Res, Vol. 55 (abstract No.751):B249,1976.
23. Moss, R.A., and Gramling, S.E., TheRole of Clinical Psychology in the Treat-ment of Craniomandibular Disorders, JCraniomandib Pract 2(2):l59-164,1984.
24. Seltzer, S.; Dewart, D.; Pollack, R.L.;Jackson, E. The effects of dietary tryp-tophan on chronic maxillofacial painand experimental pain tolerance. J Psy-chiatr Res, 17(2):181-186,1982/1983.
25. Greene, C.S.; Olson, R.E.; Laskin, D.M.• Psychological factors in the etiology,
progression, and treatment of MPD syn-drome. JADA, 105:443-448, Sept. 1982.
26. Greene, C.S. and Laskin, D.M. Mep-robamate therapy for the myofascialpain-dysfunction (MPD) syndrome: adouble-blind evaluation. JADA, 82:587-590, March 1971.
27. Greene, C.S. and Laskin, D.M. Splinttherapy for the myofascial pain-dysfunction (MPD) syndrome: a com-parative study. JADA, 84(3):624-628,1972.
28. Rubinoff, M.S.; Gross, A.; McCall, W.D.,Jr. Conventional and nonoccludingsplint therapy compared for patientswith myofascial pain dysfunction syn-drome. JAGD 35(6):502-506,1987.
29. Clark, G.T. A critical evaluation of or-thopedic interocclusal appliance ther-apy: design, theory, and overall effec-tiveness. JADA, 108:359-363, March1984.
30. Greene, C.S. and Laskin, D.M. Long-term evaluation of treatment for myo-fascial pain-dysfunction syndrome: acomparative analysis. JADA, 107:235-238, August 1983.
31. Wolf, S.; Pinsky, R.H. Effects of placeboadministration and occurrence of toxicreactions. JAMA, 155:339-341,1954.
32. Goodhart, R.; and Shils, M.E. ModernNutrition in Health and Disease. 5thedition, Lea and Febiger, 1973.
33. Zarb, G. and Carlsson, G. Temporoman-dibular Joint Function and Dysfunction.C.V. Mosby Co., 1979, St. Louis.
Reprint requests to:Dr. John W. StockstillCollege of DentistryUniversity of NebraskaLincoln, NE 68583-0740
VOLUME 56 NUMBER 2

MOTIVATIONS FOR TREATMENT AND OUTCOMES OF CARE 19
Motivations for Treatment andOutcomes of Care
The Relationship between Motivation for Seeking DentalTreatment and the Evaluation of Outcomes of Care
Susan Reisine*Judith Weber**
Although considerable researchhas been conducted on factors in-fluencing the use of dental services,the motivations of patients enter-ing treatment remain poorly under-stood. Numerous studies haveshown the importance of percep-tions, demographic, economic, andaccess factors in predicting whowill visit the dentist in a givenyear.' However, once people entercare, the importance of these fac-tors diminishes and relatively littleis known about those who com-plete care or how perceived needrelates to satisfaction with treat-ment. Health care is an on-goingprocess, and future utilization islikely to be dependent on satisfac-tion with past treatment. There-fore, there is a need to learn moreabout how dental conditions affectpeople in their everyday lives, themotivations people have for enter-ing care, and how people evaluatethe care they receive. Althoughmany factors affecting dental utili-zation have been studied, few stud-ies have examined the relationshipbetween patients' motivations forseeking care and whether they eval-uate the outcomes of treatment interms of their previous expecta-tions. A better understanding ofthis relationship could provide in-sights into improving dental treat-ment.Several indicators of dental satis-
faction have been developed as anoutcome measure in patient evalu-ation of health care.' A large litera-ture on patient satisfaction with
*Susan Reisine, Ph.D., University of Con-necticut School of Dental Medicine, Depart-ment of Behavioral Sciences.**Judith Weber, M.S.W., University of Con-necticut School of Dental Medicine, Depart-ment of Behavioral Sciences.
both medical and dental treatmentsuggests that satisfaction with careis a multidimensional concept.3A5Dimensions of dental satisfactioninclude technical quality of care,access, cost, pain and atmosphere.Studies of dental patient satisfac-tion show that both patient andgeneral populations are satisfiedwith dental care and that age, edu-cation and income are significantfactors in explaining satisfactionwith care.' Although sociodemo-graphic characteristics are impor-tant variables to consider, it may bemore critical to dental care deliveryto determine why people enter careand whether patients have realistictreatment goals.
Kiyak's study of orthognathicsurgery is one of the few to examinemotivations of patients enteringcare and to assess satisfaction withtreatment longitudinally:5'7 Shefound that patients' perceivedproblems with oral functioningwere the primary motivation forseeking treatment, although per-ceived functional problems werenot related to patient satisfaction24 months after surgery. Satisfac-tion with surgery seemed to berelated only to esthetics, in thatpatients who perceived improve-ments in esthetics generally ratedsatisfaction high, regardless ofother functional problems. The re-sults of this series of studies sug-gest that oral surgery patients usedifferent criteria in evaluating theneed for care as compared to thecriteria in evaluating the outcomesof dental treatment.This paper analyzes patients' mo-
tivations for entering more com-mon dental treatment programs.We expect that patients' motiva-tions for treatment and subsequent
evaluation of care will be sensitiveto dental conditions and will differfrom those of oral surgery patients.The main aims of the paper are todescribe patient motivations andevaluations of care and to analyzethe relationships among motivesfor treatment, patient satisfaction,evaluation of treatment outcomesand whether patients' treatment ex-pectations were met. Because num-ber of visits as an indicator of timespent in treatment could influencepatient satisfaction, this variable isincluded as a control variable.
MethodsSubjects
Patients were recruited fromnine private dental practices in theHartford, CT area and were invitedto participate in a longitudinalstudy to assess how common butserious dental problems affect peo-ple in their everyday lives. Patientswith temporomandibular joint dys-function (TMJ), recurrent peri-odontitis and patients needing den-tures were referred by their dentistsand had to meet the selection crite-ria as follows. Patients had to beover the age of 18, English speak-ing, and have no other major sys-temic illness. For the TMJ category,patients had to have at least 20teeth, pain on opening, clicking orpopping on opening or tendernessof the massiter muscles. For theperiodontal category, patients hadto have at least 20 teeth and anaverage pocket depth of 5 millime-ters. For the denture category, pa-tients had to have loose or ill-fittingdentures or broken dentures inneed of replacement. A group ofdental patients being seen on recallwas selected as well, as a compari-
VOLUME 56 NUMBER 2

20 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
son group. For this group, the re-call group, patients had to be re-turning for a 6 month check-up andprophylaxis visit and have no activedental disease.
Sample Size
The sample was one of conve-nience in that the main objective ofthe study was to assess the feasibil-ity of using quality of life indicatorsin a sample of dental patients withserious dental problems. As such, itis not a representative sample andthe results should be viewed assuggestive rather than definitive.Since patients were referred fromprivate dental practices, there islikely to be some bias from staffreferral into the study as well asself-selection bias. Of the 242 pa-tients referred into the study, 63%(152) of those asked to participatecompleted questionnaires at thetime of their initial evaluation atthe dental practice. At 6 months thesample consisted of 103 patients:30 TMJ, 16 periodontal, 15 dentureand 42 patients on recall. The attri-tion rate for the sample from initialevaluation to 6 months into treat-ment was 32.3%.
Procedure
Patients completed mailed ques-tionnaires prior to their initial visitto the dentist, at one month intotreatment and at six months. Thequestionnaires collected data onsociodemographics, reasons forseeking treatment, total number ofvisits, improvement in functioningas a result of treatment, patientsatisfaction, and whether or notexpectations for treatment weremet.
Measures
Motivations for Seeking Treat-ment: This instrument was adaptedfrom Kiyak's problems with oralfunctioning scale which was usedin her study of orthognathic sur-gery patients to assess why patientswere seeking this treatment. It iscomposed of 16 items comprising 4subscales related to function, es-thetics, health and social reasons
for entering treatment. Patientsrated the relative importance ofseeking treatment for these reasonson a four-point scale from 1, notvery important to 4, very impor-tant. Scores on the subscale itemswere summed and divided by thetotal number of items to obtain asubscale score which ranges from 1to 4. The alpha reliability on thisscale was .92.
Patient Satisfaction: The Davies-Ware Dental Satisfaction Question-naire (DSQ)2 was modified andused to assess general patient satis-faction on 5 dimensions: cost, ac-cess, pain, quality of care, and totalaccess which consisted of cost, ac-cess and convenience. The ques-tionnaire consists of 17 statementsand participants rated their agree-ment with each statement on a fivepoint scale, from 1 strongly agreeto 5, strongly disagree. Scores oneach of the items are summed toprovide an overall score whichranges from 17 to 85. Alpha reli-ability on this scale was .86.Improvement as a Result of
Treatment: This scale was adaptedfrom Kiyak's problems with oralfunctioning scale. This scale con-sisted of the same 16 items as thereasons for treatment scale and pa-tients were asked to rate how muchimprovement they experienced intheir condition from, 1 much betterto 5, much worse. A score of 3indicated no change in their condi-tion. Scores on the subscale itemswere summed and divided by thetotal number of items to obtain asubscale score which ranges from 1to 5. Alpha reliability on this scalewas .98.Evaluation of Expectations of
Treatment Being Met: Assessmentof whether patients' treatment ex-pectations were met was based onone item on which patients wereasked to rate on a scale of 1 to 10how well their expectations abouttreatment were met, with 10 beingmet very well and 1 being not metat all.Dental Appointments: Informa-
tion on total number of appoint-ments was gathered from patientself-reports on the questionnaires
mailed at one month and sixmonths after the initial visit to thedentist.
Data Analysis
Frequencies and mean scoreswere used to describe the sample.Analysis of variance (ANOVA) wasconducted to determine the effectof dental condition and the covari-ates age, income and education onthe outcome measures. Repeatedmeasures analysis (MANOVA) wasused to assess whether patterns ofresponse about reasons and expec-tations differed by dental condi-tion. Pearson product moment cor-relation analyzed the relationshipbetween reasons for treatment andtreatment outcomes.
ResultsDescriptive Characteristics ofthe Sample
Table 1 presents a description ofthe sociodemographic characteris-tics and utilization rates of the par-ticipants at 6 months. The variablesage, education and income appearto have a strong effect on condi-tion. TMJ patients are mostlyyoung, highly educated womenwho tend to be unmarried. Denturepatients tend to be older, less well-educated men, considerably less af-fluent than the other groups. Theperiodontal group consists of anequal proportion of men andwomen who are more likely to bemarried and generally middle-aged. The recall group are the mostaffluent, are also well educated andover 75% are women. Most of theparticipants remaining in treat-ment 6 months after their initialevaluation at the dentist had dentalinsurance. Denture patients are theexception with only 21.4% havinginsurance. The final sample(n = 103) did not differ signifi-cantly on these variables from thesample at baseline (n = 152).
Patients in the study have a rela-tively high number of dental ap-pointments compared to nationalstatistics. The average number ofdental visits per person in the
SUMMER 1989

MOTIVATIONS FOR TREATMENT AND OUTCOMES OF CARE 21
Table 1. Descriptive characteristics of the sample by treatmentgroup (n=103)
TMJ Periodontal Denture RecallVariables (n=30) (n=16) (n=15) (n=42)
Mean Age 34.0 52.2 62.8 43.9(s.d) (13.4) (9.3) (10.7) (14.6)
Family Income $24,500 $27,000 $14,500 $30,500(s.d) ($7,000) ($5,500) ($7,000) ($4,500)% Employed 86.2% 87.5% 20% 76.2%% Women 86.2% 50% 40% 78.6%')/0 Married 37.9% 87.5% 53.3% 66.7%% Dental
Insurance 69% 73.3% 21.4% 68.3%Mean YearsEducation 14.8 13.8 11.4 14.3(s.d) (2.5) (2.2) (1.9) (2.8)
Total Numberof Appointments 6.2 6.0 5.9 2.6(s.d) (4.0) (3.3) (4.1) (3.0)
United States in 1983 was 1.9 over-all and for those having at least onedental appointment the averagenumber was 3.4 visits.' The highernumber of visits per patient in thestudy may indicate the greatertreatment needs of our partici-pants.
Patients in the treatment condi-tions do not differ significantlyfrom each other on average num-ber of visits. Recall patients havesignificantly fewer dental appoint-ments than the treatment groups,but they still have a higher numberthan the national average.
Fig. 1 presents the mean scoresof patients on reasons for enteringtreatment before entering treat-ment. It illustrates a profile ap-proach used to analyze differentresponse patterns on patients' rea-sons for entering treatment at base-line by condition.' The sample con-sists of those patients whoremained in the study at 6 months.Again, the final and original sam-ples do not differ in any systematicway on this variable or any subse-quent variables under study.For all groups general health
concerns and fear of losing teethare important considerations inseeking dental treatment. Estheticand social reasons are somewhat tomoderately important for all pa-
tients, as well. There is, however, asignificant difference among thetreatment groups in their rating ofthe importance of function as areason for treatment. The dentureand the TMJ patients score signifi-cantly higher than the recall groupon the importance of functionalproblems as a reason for treat-ment (Scheffe test; F = 6.31; 3df;p < .05).
VeryImportant
Moderatelyimportant 3-
Figure 1 also demonstrates thatthe pattern of patient's reasons forseeking treatment vary by condi-tion. Multivariate analysis of vari-ance finds a significant conditionby scale interaction (F = 4.00; 9 df;p < .001), indicating that patients'reasons for entering treatment varyaccording to dental condition. Peri-odontal and recall patients arecharacterized by remarkably simi-lar profiles, although periodontalpatients have somewhat higherscores. General health concerns aremost important followed by esthet-ics, social concerns and function.This finding is surprising since theclinical oral health status of thesepatients are so different, and maybe an indication that periodontalpatients may not be aware of theclinical status of their dentition.TMJ patients rate function as be-
ing most important which is mostlikely related to the relative severityof their functional symptoms, fol-lowed by general health concerns,esthetics and social considerations.Denture patients, again, rate func-tion as most important but esthet-ics are also important to denturepatients, as expected.Figure 2 presents the mean
scores on patients' perceived im-
4-
Somewhatimportant 2
Not importantat all 1
*---• Denture
O o Perio
N----• TMJ
D'"""43 Recall
.••• „El.0'• .... ••
R. .,,•• •• .••''• •• .... • ......i. , • .
.••• •„,..•.....• • ..cr ...•a• -,..c• ..."
...4......„.... ... .....0, isr
Function Esthetics HealthFigure 1. Mean scores on patients' reasons for treatment by condition.
Social
VOLUME 56 NUMBER 2
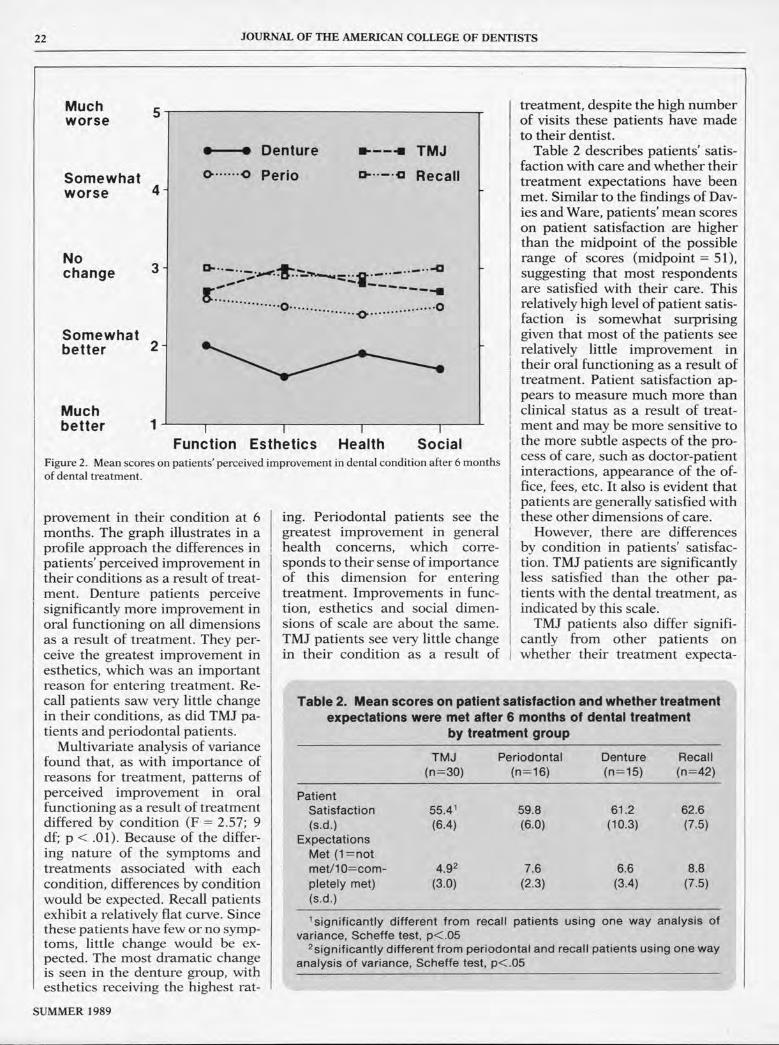
22 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
Muchworse
Somewhatworse 4 -
5
Nochange
Somewhatbetter 2-
3-
Muchbetter 1
•—• Denture
O 0 Perio
TMJ
43 Recall
-------- 0 ................ .0. ................ 0
Function Esthetics Health SocialFigure 2. Mean scores on patients' perceived improvement in dental condition after 6 monthsof dental treatment.
provement in their condition at 6months. The graph illustrates in aprofile approach the differences inpatients' perceived improvement intheir conditions as a result of treat-ment. Denture patients perceivesignificantly more improvement inoral functioning on all dimensionsas a result of treatment. They per-ceive the greatest improvement inesthetics, which was an importantreason for entering treatment. Re-call patients saw very little changein their conditions, as did TMJ pa-tients and periodontal patients.
Multivariate analysis of variancefound that, as with importance ofreasons for treatment, patterns ofperceived improvement in oralfunctioning as a result of treatmentdiffered by condition (F = 2.57; 9df; p < .01). Because of the differ-ing nature of the symptoms andtreatments associated with eachcondition, differences by conditionwould be expected. Recall patientsexhibit a relatively flat curve. Sincethese patients have few or no symp-toms, little change would be ex-pected. The most dramatic changeis seen in the denture group, withesthetics receiving the highest rat-
ing. Periodontal patients see thegreatest improvement in generalhealth concerns, which corre-sponds to their sense of importanceof this dimension for enteringtreatment. Improvements in func-tion, esthetics and social dimen-sions of scale are about the same.TMJ patients see very little changein their condition as a result of
treatment, despite the high numberof visits these patients have madeto their dentist.Table 2 describes patients' satis-
faction with care and whether theirtreatment expectations have beenmet. Similar to the findings of Dav-ies and Ware, patients' mean scoreson patient satisfaction are higherthan the midpoint of the possiblerange of scores (midpoint = 51),suggesting that most respondentsare satisfied with their care. Thisrelatively high level of patient satis-faction is somewhat surprisinggiven that most of the patients seerelatively little improvement intheir oral functioning as a result oftreatment. Patient satisfaction ap-pears to measure much more thanclinical status as a result of treat-ment and may be more sensitive tothe more subtle aspects of the pro-cess of care, such as doctor-patientinteractions, appearance of the of-fice, fees, etc. It also is evident thatpatients are generally satisfied withthese other dimensions of care.However, there are differences
by condition in patients' satisfac-tion. TMJ patients are significantlyless satisfied than the other pa-tients with the dental treatment, asindicated by this scale.TMJ patients also differ signifi-
cantly from other patients onwhether their treatment expecta-
Table 2. Mean scores on patient satisfaction and whether treatmentexpectations were met after 6 months of dental treatment
by treatment group
TMJ(n=30)
Periodontal(n=16)
Denture(n=15)
Recall(n=42)
PatientSatisfaction 55.4' 59.8 61.2 62.6(s.d.) (6.4) (6.0) (10.3) (7.5)
ExpectationsMet (1=notmet/10=com- 4.92 7.6 6.6 8.8
pletely met)(s.d.)
(3.0) (2.3) (3.4) (7.5)
'significantly different from recall patients using one way analysis ofvariance, Scheffe test, p<.052significantly different from periodontal and recall patients using one way
analysis of variance, Scheffe test, p<.05
SUMMER 1989

MOTIVATIONS FOR TREATMENT AND OUTCOMES OF CARE 23
tions were met. TMJ patients fellbelow the midpoint (on a scale of 1to 10), showing that their expecta-tions for treatment have not beenmet very well. This is a strikingresult in comparison to the scoresof the other patients who scorerelatively high on having theirtreatment expectations met. Al-though not significantly different,recall patients score the highest onhaving their expectations met, asexpected. Interestingly, althoughdenture patients report the mostimprovement with their conditionas a result of treatment, they scorelower than the periodontal patientson having treatment expectationsmet.Table 3 reports on the relation-
ships among patient satisfaction,expectations met, patients' motiva-tions for entering treatment andtheir evaluation of treatment out-comes. Four major points can bemade about these outcome vari-ables from the correlations. First,patient satisfaction is unrelated inany systematic way to either moti-vations for treatment or perceivedimprovement in clinical status. Theonly significant relationship be-tween satisfaction and motivationsfor treatment is between satisfac-tion and the social subscale. Thosewho rate social functioning asmore important as a reason forentering treatment tend to be lesssatisfied with dental care. This
finding further supports the notionthat patient satisfaction goes be-yond clinical health concerns andis more sensitive to the way inwhich care is provided. This aspectof care should receive more atten-tion from dentists.As expected, patient satisfaction
is positively correlated with havingtreatment expectations met. Thatis, those whose expectations aremet, are more satisfied with care.Patient satisfaction is also nega-tively related to number of appoint-ments, indicating that those withfewer appointments are more satis-fied. This result indicates patients'dissatisfaction with having treat-ment spread out over many visits.Second, as with satisfaction, hav-
ing treatment expectations met isnot systematically related to eithermotivations or perceived improve-ment. Having expectations met isonly significantly associated withthe function subscale on motiva-tions for treatment and improve-ment in condition. These signifi-cant negative correlations denotethe importance of oral functioningin patients' treatment expectations.The lower patients rate function inimportance for treatment, and themore improvement they see in thisarea, the more likely they are tohave had their expectations abouttreatment met. These results aredifficult to interpret, but suggestthat when expectations are rela-
tively low it is more likely thatexpectations will be met. Further,because of the dentists' skills intreating the functional aspect ororal health status, expectationsabout function can be more easilymet.Third, the correlations among
reasons for treatment and per-ceived improvement in treatmentare significant. The consistent neg-ative direction of the relationshipsindicates that the higher patientsrate the importance of each dimen-sion for seeking treatment, themore improvement they perceiveon that dimension. However, thecorrelations are fairly modest sug-gesting that motivations for treat-ment are only of minor importancein the evaluation of treatment out-comes.
Finally, number of appointmentsis negatively associated with per-ceived improvement in condition.Patients with more visits perceivethe most improvement in their con-dition. Therefore, although pa-tients are less satisfied with havingto visit the dentist more frequently,having more visits appears to beeffective in improving the patientsperceived oral health status.
Effects of Covariates
Sociodemographic variablessuch as age, income and educationare differentially distributedamong treatment groups and were
Table 3. Pearson correlations among patients satisfaction, treatment expectations, importance of reasons
for treatments and improvement in condition
2 3 4 5 6 7 8 9 10 11
1. Patient Satis.2. Expections MetImportance of Reasons for Treatment3. Function4. Esthetics5. Health6. SocialImprovement in Condition7. Function8. Esthetics9. Health10. Social11. Total Appointments
29 NS NS NS -.19 NS NS NS NS -.28-.23 NS NS NS -.19 NS NS NS NS
.58 .48 .62.73 60
68
-.25-.24-.27-.30
-.22-.25-.22-.26
-.18-.23-.29-.28
-.28-.28-.27-.34
72 .79 82.85 .87
.87
NSNSNSNS
-.24-.25-.22-.24
VOLUME 56 NUMBER 2

24 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
not expected to independently af-fect motivations or the variablesmeasuring outcomes of treatment.Analysis of variance was conductedto test this hypothesis by enteringcondition first and then determin-ing whether sociodemographic fac-tors had a significant effect on thedependent measure. Age does nothave a significant effect on any ofthe measures independent of con-dition. When condition is enteredfirst in the analysis of variance andeducation and income are enteredas covariates, education has a sig-nificant independent effect on den-tal satisfaction, expectations, andhealth and social reasons for treat-ment. Those with higher educationare more satisfied with care, aremore likely to have their treatmentexpectations met and rate socialand general health reasons as moreimportant motivations for treat-ment.Income does not have a signifi-
cant independent effect on patientsatisfaction, expectations or resultsof treatment independent of condi-tion. However, income has a signif-icant independent effect on healthreasons for treatment. Those withhigher incomes rate health reasonsfor seeking treatment more impor-tant that those with less income.
DiscussionThe aim of this paper was to
explore the relationship betweenpatients' motivation for enteringdental treatment and patients' eval-uation and satisfaction with treat-ment outcomes. The most signifi-cant finding of the study suggeststhat reasons for treatment and eval-uation of results are sensitive todental condition. Analysis of thedata show that in this sample pat-terns of responses on patients' rea-sons for treatment, results of treat-ment, expectations and patientsatisfaction vary by condition andthat selected sociodemographicfactors remain as an important in-dependent influences on these out-comes.Reasons for treatmentFor all patients, health concerns
were an important motivation for
seeking dental treatment. The re-sults of the study further show thatmany patients may not make dis-tinctions between oral health andgeneral health issues. In contrast toKiyak's findings, problems withfunction were not the primary mo-tivation for all patients seekingtreatment. For the periodontal andrecall groups, health reasons werethe most important and functionwas the least important reason forseeking care. However, for the den-ture and TMJ groups, problemswith oral functioning were the pri-mary reason for seeking care, withhealth reasons following veryclosely. TMJ dysfunction and den-ture replacement and their treat-ment may more closely parallel thetreatment needs of the oral surgerypatients studied by Kiyak.Given that reasons for entering
care differed by group, it may beimportant for dentists to considerthese differences when treating pa-tients. It is especially interesting tonote that periodontal and recallpatients have similar response pat-terns to questions about their careseeking motivations. Perhaps den-tists should stress the importanceof health and esthetics when treat-ing periodontal patients, especiallythe role of oral health in relation togeneral health.
Improvement in conditions
As expected, there was a signifi-cant correspondence between pa-tients' motives for treatment andtheir evaluation of the results oftreatment. In general, patients whosought treatment for problemswith oral functioning tended to seeimprovement in that area. Simi-larly patients who sought treat-ment for reasons of esthetics orhealth perceived improvement inthose areas. The largest correlationbetween reasons and results was inthe social interaction subscale indi-cating that dental diseases have astrong social component. However,despite their level of statistical sig-nificance, the magnitude of the cor-relations was fairly modest.Similar to the findings of Kiyak,
patient motivations for entering
treatment may not correspond totheir evaluation of outcomes. Den-ture patients, for example, scorehigh on function as a reason fortreatment yet saw the greatest ' im-provement in esthetics. TMJ pa-tients, on the other hand, exhibit apattern of responses characteristicof a chronic pain population, re-porting little improvement in prob-lems and being most disappointedin the results of treatment.
Patient satisfaction
As expected, most patients arerelatively satisfied with dental careand satisfaction is correlated withexpectations being met and fewerdental appointments. This findingwould suggest that dentists can im-prove satisfaction with care byscheduling the fewest possible ap-pointments for treating a patient.Most noteworthy is the lack of aclear relationship between motiva-tions, evaluations and satisfaction,indicating that satisfaction encom-passes a much broader conceptthan the four dimensions of thescales studied.
Conclusions
The results of the study should beviewed cautiously since the find-ings are suggestive and limited to aselect sample of dental patientswith serious dental problems. Al-though patient motivations for en-tering treatment were found to varyby condition, a common findingwas that all patients in the samplewere motivated by general healthconcerns. This has practical impli-cations for dentists in stressing totheir patients the importance ofmaintaining oral health. Future re-search should be aimed at learningmore about patients' motives andexpectations for treatment in rela-tion to patient satisfaction andevaluation of the results of dentalcare. A
References
1. Gift, H.C., "Utilization of professionaldental services", in Social Sciences andDentistry: Volume II, edited by Cohen,L. K. and Bryant, P. S., London: Quintes-
Continued on page 25
SUMMER 1989

WHY NOT YOU IN THE FDI? 25
WHY NOT YOU IN THE FDI?
Robert W. Elliott, Jr.*
There is only one international den-tal organization that encompasses thetotal spectrum of our profession. Thatis the Federation Dentaire Internation-ale.When we consider that there are over
150,000 dentists in the USA and about500,000 worldwide you would thinkthat there would be a great number ofus who would be "Supporting mem-bers" of the FDI, especially when indi-vidual dues are only $30.00 per year.
Surprisingly, there are less than1,100 dentists in the USA who aremembers.Well, you ask, why should I belong?
That is a relevant question and one thatdeserves an answer—let me give youmy thoughts.This international body needs and
merits our participation to show theworld that we care about others thanourselves and more practically to assistthe group financially as we benefitfrom its efforts.As you know, the American College
of Dentists accomplishes its goalsthrough Commissions which superviseworking groups. The FDI achieves itsobjectives in the identical fashion. Ithas four Commissions, each of whichhas four to eight working groups. TheseCommissions are: Dental Educationand Practice, Research and Epidemiol-ogy, Dental Products, and Federal Den-
*Robert W. Elliott, Jr., ACD ImmediatePast President.
tal Services. The working groups con-sider an area of need or a specialproject and develop guidance for gen-eral use or for an individual nation, asrequested. These reports are reviewedby the sponsor Commission and pub-lished as position papers. In countrieswith few resources, or not as advanceddentally as the United States of Amer-ica, these reports are much in demand.The FDI also participates with the
World Health Organization (WHO) injoint working groups. This contributesto the recognition of dentistry in inter-national health circles.
Specifically, FDI President CarltonWilliams states, "The FDI/WHO jointworking group's effort that is so con-suming at the moment is the AIDSprogram headed by Dr. Jens Penboy ofCopenhagen. This project will continuefor at least one more year as a largenumber of countries are finding thematerial very helpful."Dr. Jan Erik Alilberg, Executive Di-
rector of the FDI states in a recent issueof the FDI NEWS, "Much of the workdone by the FDI for the benefit of theindividual dentist is assimilated in 'endproducts' which bear no mark of theFDI contributions. A good example isstandardization of dental materials.Probably only a very small proportionof practicing dentists know that behindthe ISO standard for every materialthey use, the FDI has been heavilyinvolved in its preparation." We mustremember, too, that the fantastic revo-lution in Oral and Maxillofacial surgery
ACD Reception AtFDI MEETING
The European Section of the Ameri-can College of Dentists is holding a"No Host" reception during the FDIMeeting in Amsterdam on Wednes-day, September 6, 1989 at Mid-dayin the Garden Hotel. ACD Fellowsand their spouses are cordially in-vited. Those wishing to attendshould forward $15.00 per person,by check, made out to Derrick-ACDAccount as soon as possible. Send tothe Section Secretary, Dr. DonaldDerrick, 140 Park Lane, Suite 21,London Wl, England.
was fathered in Switzerland and En-gland, and Branemark of Sweden hasshown us the way in implants while theearly interest in periodontics camefrom European exiles such as Gottlieb,Orban and Wienman.
Additionally, the FDI NEWS, pub-lished six times a year, will keep youposted on what is happening in ourprofession worldwide.So you see, the FDI provides an indis-
pensable, international forum for ourprofession. The FDI needs your sup-port—for $30.00, tax deductible, youcan become a Supporting Member—why not send your check today toFDI, USA Section, 211 East ChicagoAvenue, Chicago, IL 60611?P.S. I'm a member. Why not you? A
Continued from page 24sence Publishing Company, Ltd., 1984.
2. Davies, A.R., Ware, J.E. Measuring pa-tient satisfaction with dental care. Soc.Sci. Med., 15A:751-760, 1981.
3. Chapko, M. K., Bergner M., Green K.et al., Development and validation of ameasure of dental patient satisfaction.Med. Care, 23:39— 49, 1985.
4. Kress, G., Improving patient satisfaction,Int. Dent. J. 37:117-120, 1987.
5. Ware, J.E., Davies, A.A., Stewart, A.L.,The measurement and meaning of pa-tient satisfaction, Hlth. & Med. CareServ. Rev. 1:1-15, 1978.
6. Kiyak, H.A., McNeill, R.W., West, R.A.,et al. Predicting psychologic responses toorthognathic surgery, J. Oral & Maxillof.Surg., 40:150-55, 1982.
7. Kiyak, H.A., Hohl, T., West, R.A., et al,Psychologic changes in orthognathic sur-gery patients: A 24-month follow up. J.Oral Maxillof. Surg., 42:506-512, 1984.
8. National Center for Health Statistics,"Use of dental services" in Advance DataFrom Vital and Health Statistics, No. 122DHHS Pub. No. (PHS) 86-1250. PublicHealth Service, Hyattsville, Md., August8, 1986.
9. Bergner, M. "The Sickness Impact Profile(SIP)", in Assessment of Quality of Life inClinical Trials of Cardiovascular Thera-pies, edited by Wenger, N.K. Mattson,M.E. et al., New York, N.Y.: LeJacq Pub-lishing Inc., 1984, pp. 152-159.
Reprint requests to:Dr. Susan ReisineSchool of Dental MedicineUniversity of ConnecticutFarmington AvenueFarmington, CT 06032
SUMMER 1989
26 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
NEWSOF
FELLOWS Wesley J. Dunn, the founding
Dean of the Faculty of Dentistry ofthe University of Western Ontario,was recently elected the 50th Presi-dent of the Royal College of DentalSurgeons of Ontario which is the121 year old governing body ofdentistry in Ontario. Dr. Dunnpracticed in Toronto until 1955,when he was appointed Registrarof the Faculty of Dentistry at theUniversity of Toronto, a position heheld until his appointment as Deanof Dentistry at the University ofWestern Ontario in 1965. Dr. Dunnhas served as the Editor of theJournal of the Canadian Dental As-sociation and as Chairman of theCouncil on Education of the Cana-dian Dental Association. He hasalso served as President of theAmerican Association of DentalEditors, President of the Associa-tion of Canadian Faculty's of Den-tistry and Organizing Secretary ofthe Canadian Society of Dentistryfor Children.
Wesley J. Dunn
Robert F. Streelman of Wyo-ming, Michigan, recently receivedthe 1989 Distinguished ServiceAward of the West Michigan Dis-trict Dental Society. Active in hiscommunity and church, Dr. Streel-man has served as President of theWest Michigan Dental Society andis currently the President of theWest Michigan Dental Foundation.
Gordon H. Rovelstad, the Exec-utive Director of the American Col-lege of Dentists, was the recipientof the American Society of Den-tistry for Children's 1988 Award ofExcellence for his significant con-tributions to the advancement ofthe dental health of children. Dr.Rovelstad received his D.D.S.,M.S.D. and Ph.D. degrees fromNorthwestern University and prac-ticed pedodontics in Elgin and inChicago from 1948-1953 and inJackson, Mississippi from1974-1981. Dr. Rovelstad servedwith distinction in the UnitedStates Navy Dental Corps and re-ceived the Meritorious ServiceMedal in 1969 and the Legion ofMerit Award in 1972. His extensiveresearch in salivary gland physiol-ogy, dental caries etiology and epi-demiology and in oral biology, re-sulted in a substantial number of
Robert F. Streelman
scientific articles and presenta-tions.Dr. Rovelstad has also held many
academic appointments at variousuniversities. He served as theChairman of the Department of Pe-diatric Dentistry from 1975-1976and as Assistant Dean, EducationalPrograms from 1976-1981 at theUniversity of Mississippi. Dr. Rov-elstad is a Diplomate of the Ameri-can Board of Pedodontics and hasserved as a member of the Examin-ing Board and as the President ofthe American Board of Pedodon-tics. He has also served as the Pres-ident of the American Academy ofPedodontics, as well as the Presi-dent of the International Associa-tion for Dental Research and theAmerican College of Dentists. Dr.Rovelstad has served as ExecutiveDirector of the American College ofDentists since 1981.
ACD Executive Director, Gordon H. Rovelstad, center, received the American So-
ciety of Dentistry for Children's Award of Excellence during the Spring Meeting
of the ACD Board of Regents. The Award was presented by ACD Regent Prem S.Sharma, right, who is also the Immediate Past President of the American Societyof Dentistry for Children. ACD President James A. Harrell, Sr., is pictured at left.
VOLUME 56 NUMBER 2

NEWS OF FELLOWS 27
Harald Loe, Director of the Na-tional Institute of Dental Research,was recently the recipient of theSurgeon General's Exemplary Ser-vice Award which is given to civilservice employees of the PublicHealth Service who have "exempli-fied the highest leadership andcommitment to meeting the initia-tives of the office of the SurgeonGeneral and to the mission of thePHS." Dr. Loe was also recentlyhonored by the Swedish Dental So-ciety with the presentation of itsinternational prize of 100,000Swedish kronor. Dr. LOe receivedthe award during ceremonies inStockholm in connection with the25th anniversary of the SwedishNational Dental Research meeting.The award has been established tohighlight the importance of dentalresearch, its international scopeand its continuing development.A native of Norway, Dr. Loe re-
ceived his Doctor of Dental Surgeryand Doctor of Odontology degreesfrom the University of Oslo. Prior
Erbert W. D'Anton, Professorand Chairman of the Departmentof Oral Biomaterials at the Univer-sity of Texas, Dental Branch, atHouston, will retire shortly fromhis academic position. Dr. D'Antonreceived his D.D.S. degree from St.Louis University Dental School in1946 and joined the faculty of theUniversity of Texas, Dental Branch,at Houston in 1948. He was ap-pointed Chairman of the Depart-ment of Oral Biomaterials in 1956.Dr. D'Anton is a member of severalprofessional organizations and hasserved as the Vice President of theSupreme Chapter of OmicronKappa Upsilon. He has also servedon the Editorial Staff of the Hous-ton District Dental Society and wasa Test Construction Committeemember of the National Board ofDental Examiners.
Dr. Lae, on the left, seen receiving his award from Surgeon General C. EverettKoop.
to his appointment as NIDR Direc-tor, he served as Dean of the Uni-versity of Connecticut School ofDental Medicine. Dr. Lae has re-ceived a total of 9 honorary degreesfrom universities in 5 countries. Inaddition, he has received numer-ous awards, including the Alpha
Allen M. Ito
Omega Achievement Medal Award,the Alfred C. Fons medal of Out-standing Achievement in the inter-est of humanity from the Connecti-cut State Dental Association andthe International Association forDental Research award for basicresearch in periodontology.
Allen M. Ito of Honolulu wasrecently honored by the HawaiiDental Association by being pre-sented the Association's Distin-guished Service Award. Dr. Ito wasrecognized for his extensive serviceto the dental profession and forbeing a role model as an outstand-ing member of the profession. Dr.Ito has served for many years as theChairman of the Library Commit-tee and co-Chairman of the TableClinic Committee of the HawaiiDental Association. His untiring ef-forts in promoting continuing edu-cation programs have been of im-mense value to his fellow prac-titioners in Hawaii. Dr. Ito alsofounded "Operation Book Shelf' asa project of the Hawaii Section andhas been responsible for collectingdental books and literature frommembers of the profession andshipping them to dental schools inthe Pacific Basin countries.
SUMMER 1989
Erbert W. D'Anton

28 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
Lloyd E. Church of Bethesda,Maryland, was presented an em-broidered judo uniform at the an-nual meeting of the AmericanAcademy of the History of Den-tistry during the American DentalAssociation's annual session inWashington, D.C. The judo uni-form, a gift from Dr. NorinagaMoriyama, of Tokyo, Japan, was inappreciation of the extensive helpprovided by Dr. Church to the To-kyo Dental College and also to re-place the judo uniform that Dr.Church lost during his trip fromTokyo to Washington, D.C. in 1948.Dr. Church received his D.D.S.
degree in 1944 from the Universityof Maryland. A man of many tal-ents, he helped pay for his dentaleducation by playing cornet in alocal jazz band, by being a memberof a survey crew for the West Vir-ginia State Road Commission andby serving as a member of thePinkerton Detective Agency. In1946, he enlisted in the U.S. ArmyDental Corps and was assigned tothe 361st Station Hospital in To-kyo, Japan. He served as a dentalmember of the special securitymedical team at Sugamo Prisonduring the war trials and provideddental services for the prisonersand military personnel at theprison. While serving in Japan, heheard that the Tokyo Dental Col-lege had lost all of its dental equip-ment and supplies and proceededto assist them in refurnishing theirclinics. A nearby judo school heardabout Dr. Church's help to the Den-
tal College and offered to give judolessons to him. The offer was ac-cepted and before leaving Japan,Dr. Church earned the prestigiousblack belt in judo.Following an honorable dis-
charge from the military in 1948,Dr. Church was on his way back toWashington, D.C. when he losthis prized judo uniform. Dr.Moriyama, a graduate of the TokyoDental College, brought and pre-sented the new judo uniform to Dr.Church in appreciation of the helpthat Dr. Church had given to hiscollege and to replace the one thatwas lost 40 years earlier.Following his return to Washing-
ton, D.C., Dr. Church went intoprivate practice and received anM.S. degree in 1951 and the Ph.D.degree in 1959 from the Universityof West Virginia. He served on thefaculty of the dental and medicalschool of the Medical College ofVirginia and of the George Wash-ington University School of Medi-cine. In addition, he was affiliatedwith the Armed Forces Institute ofPathology and served as a seniorresearch scientist at the NationalBiomedical Research Foundation,as well as a member of the Univer-sity of Maryland School of Medi-cine. He conducted extensive re-search in a variety of areas and wasalso very active in several profes-sional and community organiza-tions. Dr. Church currently servesas the Book Review Editor of theBulletin of the History of Dentistry.
Norinaga Moriyama of Tokyo on the right, seen presenting an embroidered judo
uniform to Dr. Church at the annual meeting of the American Academy of the
History of Dentistry in Washington, D.C.
Anthony M. Schiano was hon-ored by the Palisades General Hos-pital in North Bergen, New Jerseyfor his many years of outstandingand dedicated service to the dentalstaff. Dr. Schiano is a former Chiefof the Oral and Mwdllofacial Sur-gery Section, Department of Sur-gery, and former Chairman of theBoard of the Palisades GeneralHospital Association. He is a Diplo-mate of the American Board of Oraland Maxillofacial Surgery and hasserved as a president of the HudsonCounty Dental Society.
Anthony M. Schiano on the left, waspresented an engraved plaque by an-other Fellow of the College, HarveySalb.
Ralph S. Kaslick was recentlyappointed Director of the Depart-ment of Dentistry at the GoldwaterMemorial Hospital on Roosevelt Is-land, New York. Dr. Kaslick willalso serve as Clinical Professor ofPeriodontics at NYU College ofDentistry. He served as AssistantDean, Academic Affairs at FairleighDickinson University, College ofDental Medicine and then as Deanfrom 1976-1987. Dr. Kaslick alsoserved as the Acting Provost from1983 to 1985.
Ralph S. Kaslick
VOLUME 56 NUMBER 2

NEWS OF FELLOWS 29
Ray Victor Smith was presentedwith a medallion and citation at theColorado Section's annual meetingin recognition of 50 years as aFellow of the American College ofDentists. James H. McLeran, Deanof the University of Iowa College ofDentistry, and associate Iowa DeanJohn C. Montgomery were also atthe meeting to recognize Dr.Smith's 53 years of full-time teach-ing. Dr. Smith graduated from theCollege of Dentistry, University ofIowa, in 1914 and following twoyears of general practice, joined thefaculty of dentistry at Iowa. Start-ing as a demonstrator in Crownand Bridge, over a period of 7years, he rose to the rank of Profes-sor and Head of the Department ofCrown and Bridge. He retired fromthis position in 1959, but continuedto teach part-time at the Universityof Iowa in the Oral Hygiene Depart-ment until 1969.Dr. Smith served as the Chair-
man of the Dental Aptitude TestingCommittee of the American Associ-ation of Dental Schools from 1932until his retirement in 1959 andwas a consultant to the Council onDental Education of the AmericanDental Association and the Veter-ans Administration.
Raymond J. Fonseca, Professorand Chairman of Oral Medicine,Pathology and Surgery at the Uni-versity of Michigan School of Den-tistry, has been appointed Dean ofthe University of PennsylvaniaSchool of Dental Medicine, effec-tive July 1. Dr. Fonseca received hisD.M.D. degree from the Universityof Connecticut School of DentalMedicine and completed his oralsurgery residency at Parkland Me-morial Hospital in Dallas, Texas.He is the Vice President of theSociety of Editors in Oral and Max-illofacial Surgery and an examinerfor the American Board of Oral andMaxillofacial Surgery. He is also aSection Editor for the Journal ofAdult Orthodontic and OrthognaticSurgery, as well as a Section Editorof the Journal of Oral and Mwdllo-facial Surgery.
Ray Victor Smith, center, was honored for 50 years of Fellowship in the College at theColorado Section Meeting. Also pictured is ACD Regent Thomas W. Slack, left, whopresented the ACD Citation, and Colorado Section Chairman David H. Werldng.
Edgar C. Hatcher, Jr.
Raymond J. Fonseca
Edgar C. Hatcher, Jr. of Bristol,Tennessee, recently received anhonorary degree of Doctor of Sci-ence from Nan Nam University,Taejon, Republic of Korea. Dr.Hatcher was recognized for hiscontribution to dentistry andhigher education both in theUnited States and in other parts ofthe world.Dr. Hatcher is the Editor Emeri-
tus of the Journal of the TennesseeDental Association and receivedthe William J. Gies Editorial Awardin 1985 for excellence in dentaljournalism. He was also the recipi-ent of the 1986 Golden Pen Award,presented by the International Col-lege of Dentists. Dr. Hatcher ad-dressed the commencement cere-monies of the Han Nam Universityin Korea before receiving his hon-orary degree.
SUMMER 1989

30 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
SECTION ACTIVITIES
CarolinasThe Carolinas Section held its
annual meeting at the Omni Hotelin Charleston, South Carolina, Feb-ruary 3-5. The meeting, attendedby 43 Fellows and their guests, con-sisted of a scientific program, busi-ness meeting and social activities.The Section voted to make a pledgeof $1,000 to the "Campaign for the90's" to be paid over a five-yearperiod. Dr. Fitzhugh N. Hamrickwas recognized at the meeting andpresented with a certificate of ap-preciation for his outstanding ser-vice to the dental profession. Newofficers were elected as follows:Chairman, John B. Sowter; ViceChairman, William R. Chapmanand Secretary/Treasurer, Dudley C.Chandler, Jr.
MarylandSeventy Fellows attended the an-
nual business meeting of the Mary-land Section recently at the Mary-land University Club to conduct theSection's official business. Themeeting was presided over by JohnF. Hasler, Section Chairman and,following reports by several com-mittees, the following officers wereinstalled: Chairman, J. RichardCrouse; Vice Chairman, Don N.Brotman; Secretary, W. MichaelKenney; Treasurer, Frank Romeoand Editor, Harry W. Dressel, Jr.
Photographed at the Carolinas Section meeting are, from the left: Howard W.Higgins; William R. Chapman, John B. Sowter, Dudley C. Chandler, Jr., JamesH. Gaines; James A. Harrell, Sr., President of ACD and Chris C. Scures, Regent,Regency 3.
Howard W. Higgins, on the left, seen presenting a certificate of appreciation foroutstanding service to the dental profession to Fitzhugh N. Hamrick.
Photographed at the Maryland Section's annual business meeting are, from theleft: Past Regent, Joseph P. Cappuccio; Ruth S. Friedman, Regent, Regency 2; J.Richard Crouse; W. Michael Kenney and John F. Hasler.
VOLUME 56 NUMBER 2

SECTION ACTIVITIES 31
HawaiiFellows of the Hawaiian Section
are actively participating in makingarrangements for the 1989 AnnualMeeting of the College which willbe held at the Ilikai Hotel inWaikiki, on November 3. James A.Harrell, Sr., President of the Col-lege, and Mae Hom of the nationaloffice staff attended the HawaiiSection's meeting recently to final-ize plans for the annual meetingand convocation. All Fellows at-tending the Honolulu meeting arein for a very special treat, as asuperb, informative and entertain-ing program has been arrangedwhich will also emphasize theuniqueness of Hawaii. The currentofficers of the Hawaii Section are:Chairman, Kanemi Kanazawa;Vice Chairman, John M. Fujioka;and Secretary/Treasurer, Harry H.Morikawa.
Victor J. Niiranen, left, retired Navy Cap-tain, is pictured with ACD President JamesA. Harrell, Sr. during the Hawaii SectionMeeting. Dr. Niiranen has been very activein the Hawaii Section, was instrumentalwith the shipment of books and periodi-cals to dental libraries in the Far East andis also an accomplished artist. He is cur-rently the President of the National Soci-ety of Arts and Letters.
St. LouisThe St. Louis Section held its
annual meeting recently in Brent-wood, Missouri and elected the fol-lowing officers: Eugene J. McCabe,Chairman; Richard W. Brand,Chairman-Elect; and Joseph M.Grana, Secretary/Treasurer.
Photographed at the meeting of the Hawaii Section are from the left: Lewis S.Earle, ADA 5th District Trustee; James A. Harrell, Sr., President, ACD; Arthur A.Dugoni, President, ADA; and Kanemi Kanazawa, Chairman, Hawaii Section.
At the Hawaii Section Meeting are, from the left, Section Secretary-TreasurerHarry H. Morikawa, Section Chairman Kanemi Kanazawa, ACD ComptrollerMae Hom, Section Vice Chairman John M. Fujioka and ACD President James A.Harrell, Sr.
Photographed at the St. Louis Section meeting are, from the left: Chairman Eu-gene J. McCabe, Past Chairman Warren H. Speiser, Secretary-Treasurer JosephM. Grana and Chairman Elect Richard W. Brand.
SUMMER 1989

32 JOURNAL OF THE AMERICAN COLLEGE OF DENTISTS
STATEMENT OF OWNERSHIP AND CIRCULATIONTHE JOURNAL OF THE AMERICAN COLLEGE OF
DENTISTS is published quarterly by the American College ofDentists, Suite 352N, 7315 Wisconsin Avenue, Bethesda,Maryland 20814. Editor Keith P. Blair, D.D.S., Managing EditorGordon H. Rovelstad, D.D.S.The American College of Dentists is a non-profit organization
with no capital stock and no known bondholders, mortgages orother security holders. The average number of readers of eachissue produced during the past 12 months was 4864; none sold
through dealers and carriers, street vendors or counter sales;4508 copies distributed through mail subscriptions; 4508 totalpaid circulation; 356 distributed as complimentary copies. Forthe Summer, 1987 issue the actual number of copies printedwas 5058; none sold through dealers, etc.; 4403 distributedthrough mail subscriptions; 4403 total paid circulation, 284distributed as complimentary copies; 4687 copies distributed intotal. Statement filed with the U.S. Postal Service, September26, 1988.
INSTRUCTIONS FOR AUTHORS
INTRODUCTION
The Journal of the American College of Dentists is publishedquarterly in order to promote the highest ideals in health care,advance the standards and efficiency of dentistry, develop goodhuman relations and understanding, and extend the benefits ofdental health to the greatest number. It is the official publicationof the American College of Dentists which invites submission ofessays, editorials, reports of original research, new ideas, ad-vances and statements of opinion pertinent to dentistry. Papersdo not necessarily represent the view of the Editors, EditorialStaff or the American College of Dentists.
EDITORIAL POLICY
The editorial staff reserves the right to edit all manuscripts to fitwithin the space available to edit for conciseness, clarity, andstylistic consistency. A copy of the edited manuscript will be sentto the author. All manuscripts are refereed anonymously. Onlyoriginal articles that have not been published and are not beingconsidered for publication elsewhere will be considered forpublication in the Journal unless specifically requested otherwiseby the Editor.The primary author must ensure that the manuscript has been
seen and approved by all co-authors. Initial receipt of allmanuscripts submitted will be acknowledged and, at the con-clusion of the review procedure, authors will be notified of (1)acceptance, (2) need for revision, or (3) rejection of their papers.
PREPARATION OF MANUSCRIPTS
Papers should be in English, typed double space on white 8-1/2X 11 paper. Left hand margins should be at least 1-1/2 inches toallow for editing.
All pages, including Title Page, Tables and Figure legends,should be numbered consecutively in the top right-hand corner.The first page should list title of manuscript with the first letters ofthe main words capitalized (do not use Part I, etc.), author's (orauthors') initials and name(s) in capitals (no titles or degrees),complete professional address(es) (including ZIP or Postal Code),a short title of NOT more than 45 characters in block capitals, and,as a footnote, any change in corresponding author's address sincethe paper was submitted. With multiple authors, relate them totheir respective institutions by superscript numbers. The firstauthor is assumed to be the one to whom correspondence andreprint requests should be directed unless otherwise stated.The second page should be an abstract of 250 words or less
summarizing the information contained in the manuscript.Authors should submit an original and four copies of the
manuscript and three original sets of illustrations to: Dr. Keith P.Blair, Editor.
Dorland's Illustrated Dictionary will be used as the authority foranatomical nomenclature. The American Heritage Dictionary will
be used as the authority for spelling nonmedical terms. TheAmerican English form of plurals will be used where two areprovided. The Index Medicus and Index to Dental Literature serveas authorities for standard abbreviations.
CORRESPONDENCE
Address all manuscripts and related corrrespondence to: TheEditor, JOURNAL OF THE AMERICAN COLLEGE OF DEN-TISTS, Suite 352N, 7315 Wisconsin Ave., Bethesda, MD 20814-3202.
REFERENCES
A list of references should appear chronologically at the end of thepaper consisting of those references cited in the body of the text.This list should be typed double space and follow the form ofthese examples:
1. Smith, J.M., Perspectives on Dental Education, Journal ofDental Education, 45:741-5, November 1981.
2. White, E.M., Sometimes an A is Really an F. The Chronical ofHigher Education, 9:24, February 3, 1975.
Each reference should be checked for accuracy and complete-ness before the manuscript is submitted. The accuracy andcompleteness of references are major considerations in deter-mining the suitability of a manuscript for publication. Referencelists that do not follow the illustrated format and punctuationor which are not typed double spaced will be returnedfor retyping.
REPRINTS
A form for reprints will be sent to the corresponding author afterthe manuscript has been accepted and edited. He/she then shallinform all other authors of the availability of reprints andcombine all orders on the form provided. The authors shall stateto whom and where reprint requests are to be sent. Additionalcopies and back issues of the Journal can be ordered from theBusiness Manager of the Journal.
COPYRIGHT POLICY
All manuscripts must be accompanied by the following state-ment, signed by one author: "The undersigned author transfers allcopyright ownership of the manuscript entitled (name of thearticle) to the American College of Dentists should the work bepublished. The undersigned author warrants that the article isoriginal, is not under consideration by another journal, and hasnot been published previously. I sign for and accept responsibilityFor releasing this material on behalf of any and all coauthors".Authors will be consulted, when possible, regarding republicationof their materials.
VOLUME 56 NUMBER 2

OFFICERS
President TreasurerJAMES A. HARRELL, SR. ROBERT C. COKER180-G Parkwood Prof. Center 1100 Florida AvenueElkin, NC 28621 New Orleans, LA 70119
President-Elect Immediate Past President
W. ROBERT BIDDINGTON ROBERT W. ELLIOTT, JR.
West Virginia Univ. Med. Ctr. 8732 Falls Chapel Way
Morgantown, WV 26505 Potomac, MD 20854
Vice PresidentROBERT E. DOERR2021 Pauline CourtAnn Arbor, MI 48103
Regency 1
EditorKEITH P. BLAIR4403 Marlborough AvenueSan Diego, California 92116
Executive DirectorGORDON H. ROVELSTAD7315 Wisconsin AvenueBethesda, Maryland 20814
SUMNER H. WILLENS400 Paradise RoadSwampscott, MA 01907
REGENTS
Connecticut, Maine, Massachusetts, New Hampshire, NewYork, Quebec, Rhode Island, Vermont
Regency 2 RUTH S. FRIEDMANGateway Towers, Apt. 26CPittsburgh, PA 15222
Delaware, District of Columbia, Europe, Maryland, NewJersey, Pennsylvania, Puerto Rico
Regency 3 CHRIS C. SCURES2122 E. Robinson St.Orlando, FL 32803
Alabama, Florida, Georgia, North Carolina, South Carolina,Virginia
Regency 4 JULIANN S. BLUITTNUDS, 311 E. Chicago Ave.Chicago, IL 60611
Illinois, Indiana, Kentucky, Ohio, West Virginia
Regency 5 PREM S. SHARMA1900 W. Woodbury LaneGlendale, WI 53209
Iowa, Kansas, Manitoba, Michigan, Minnesota, Nebraska,North Dakota, South Dakota, Oklahoma, Ontario, Wisconsin.
Regency 6 ROBERT E. LAMB3808 Martha LaneDallas, Texas 75229
Arkansas, Louisiana, Mississippi, Missouri, Tennessee, Texas
Regency 7 THOMAS W. SLACK3015 Jet WirT DriveColorado Spnngs, CO 80916
Arizona, Southern California, Colorado, Nevada, NewMexico, Utah, Wyoming.
Regency 8 CHARLES V. FARRELL1800 C. Street, Su. M-23Bellingham, WA 98225
Alaska, Alberta, British Columbia, Northern California,Hawaii, Idaho, Montana, Oregon, Washington, Saskatchewan

American College of Dentists7315 Wisconsin Avenue
Bethesda, Maryland 20814
Return Postage Guaranteed
fowiitc?1/4,‘/Ai OM"
IZa11111).
Adhesive Bonding of Composites
The Placebo Effect
Dental Insurance
Motivations for Treatment
Second Class PostagePAID
at Bethesda MDand at Additional Mailing Office