role of bariatric surgery in obesity and diabetes of bariatric surgery in obesity and diabetes. ......
TRANSCRIPT
Role of Bariatric Surgery in Obesity and Diabetes
Cleveland Clinic Bariatric and Metabolic Institute Endocrinology, Diabetes and Metabolism
Philip R. Schauer, MD Professor of Surgery, Cleveland Clinic Lerner College of Medicine
Director: Bariatric and Metabolic Institute (BMI)

Presenter Disclosure Philip R. Schauer MD
Board Member/Advisory Panel: Surgiquest Consultant: Ethicon, Lilly, Nestle’, Novo Nordisk, Quadrant
HealthCom, Inc. Research Support: Ethicon, NIH Stock/Shareholder: Surgiquest, SEHQC LLC, ReMedyMD
Dr. Schauer does not intend to discuss any off-label use/unapproved use of drugs or devices

ObesityWeek.com

A1C < 7% 52.5%
BP < 130/80 51.1%
LDL < 100mg/dl 56.2%
All 3 18.8%
NHANES data 2007-2010, n = 4,926
Bariatric Surgery Could Potentially Improve Success in Achieving all 3 Targets of Therapy
Diabetes Care 2013
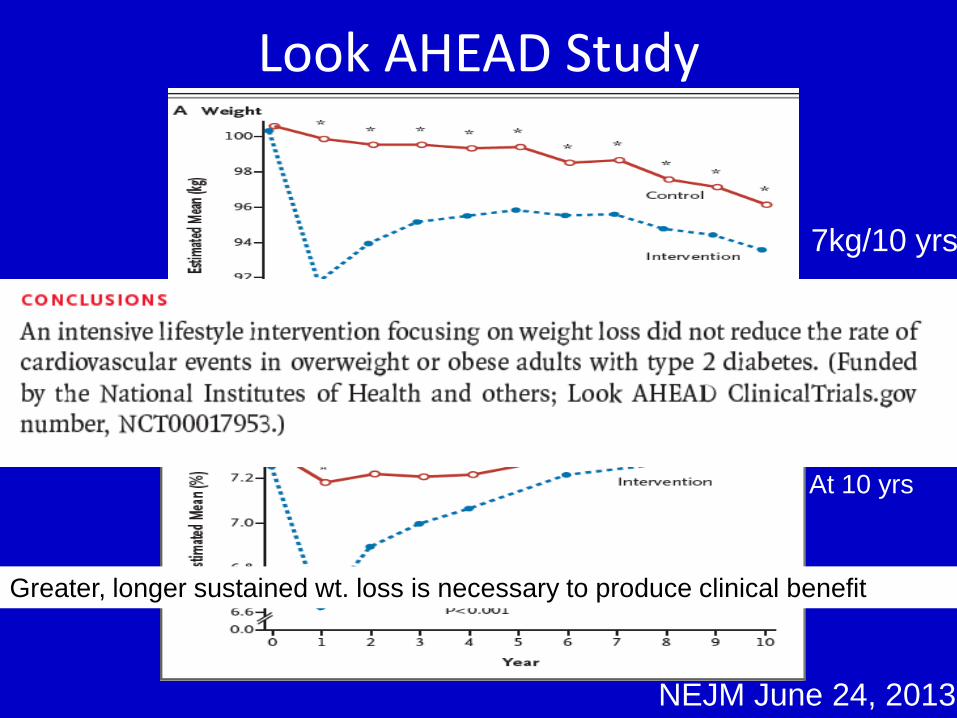
Look AHEAD Study
NEJM June 24, 2013
7kg/10 yrs
HbA1c No change At 10 yrs
Greater, longer sustained wt. loss is necessary to produce clinical benefit

Bariatric/Metabolic Surgery 2014
55% 35% 8% 2%

Laparoscopic Open

Safety of Bariatric Surgery in Obese Patients
Weighing benefits with risk
o 30-day mortality 0.3% o Major morbidity 4.3% o ONE TENTH THE RISK OF CORONARY BYPASS SURGERY
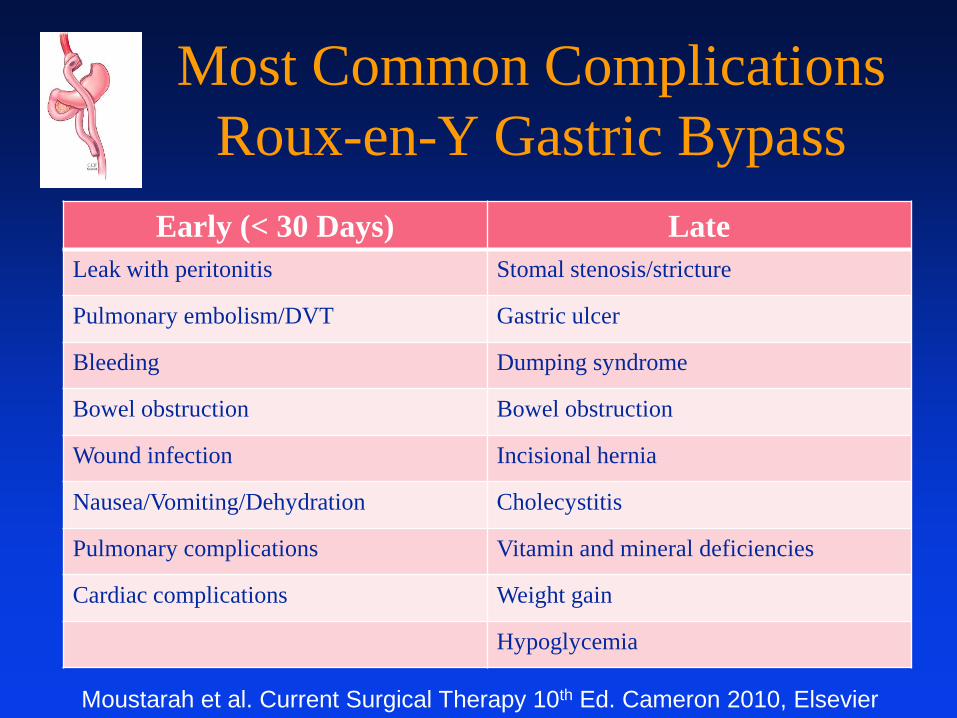
Most Common Complications Roux-en-Y Gastric Bypass
Early (< 30 Days) Late Leak with peritonitis Stomal stenosis/stricture
Pulmonary embolism/DVT Gastric ulcer
Bleeding Dumping syndrome
Bowel obstruction Bowel obstruction
Wound infection Incisional hernia
Nausea/Vomiting/Dehydration Cholecystitis
Pulmonary complications Vitamin and mineral deficiencies
Cardiac complications Weight gain
Hypoglycemia
Moustarah et al. Current Surgical Therapy 10th Ed. Cameron 2010, Elsevier

73 studies (3 RCT’s)

What about the effect of surgery on Long-term Morbidity/ Mortality
How Durable is the effect of surgery?
5.5
6.0
6.5
7.0
7.5
8.0
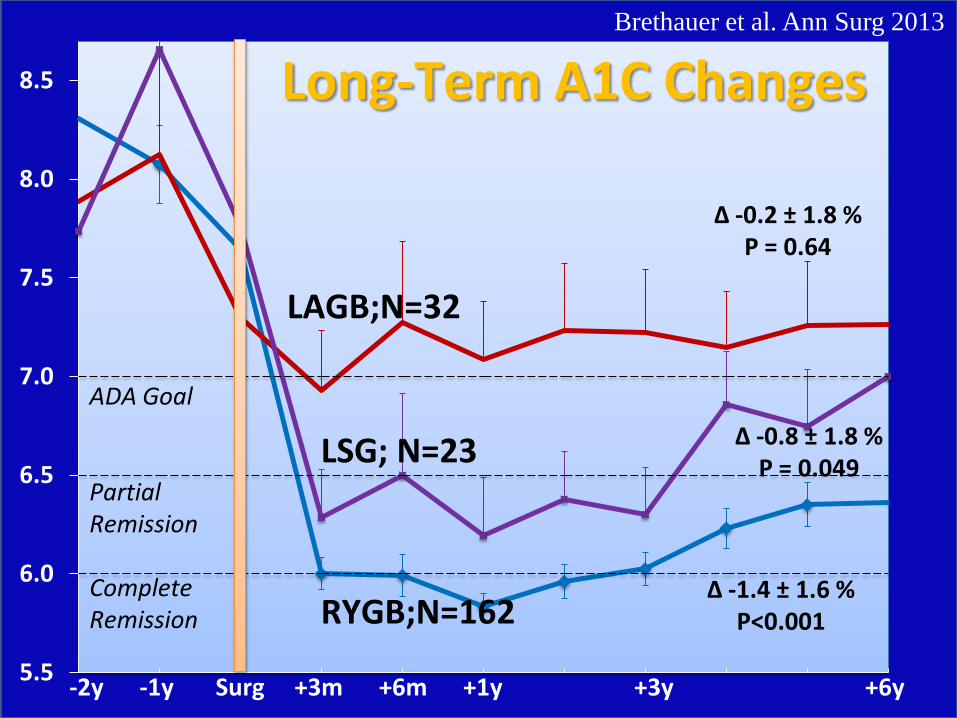
8.5 Long-Term A1C Changes
LSG; N=23
RYGB;N=162
-2y -1y Surg +3m +6m +1y +3y +6y
Δ -1.4 ± 1.6 %
P<0.001
LAGB;N=32
Δ -0.8 ± 1.8 %
P = 0.049
Δ -0.2 ± 1.8 %
P = 0.64
ADA Goal
Partial Remission
Complete Remission
Brethauer et al. Ann Surg 2013

SOS JAMA 2012
Look Ahead

Surgery associated with:
•Reduced all cause mortality
•Reduced CV events (fatal and nonfatal)
•Reduced Cancer mortality
•Reduced microvascular complications

Effect on Long-term Mortality Compared to Non-Operated Controls
Study Procedure F/U Mortality
Reduction
MacDonald,1997 RYGB 9 yrs 88%
Flum, 2004 RYGB 4.4yrs 33%
Christou, 2004 RYGB 5 yrs 89%
Sowemimo, 2007 RYGB 4.4 yrs 50%
O’brien, 2006 LAGB 12 yrs 73%
Adams, 2007 RYGB 8.4 yrs 40%
Sjostrom, 2007 VBG/other 14 yrs 31%
Perry, 2008 (Medicare) RYGB, VBG, LAGB
2 yrs 48 % age < 65
34% age > 65 Maciejewski, 2011 RYGB 6.7 yrs None*

RCT’s Comparing Bariatric Surgery with Medical Therapy
for T2DM

Published online March 31, 2014
Funded by Ethicon/NIH

Baseline Characteristics
Parameter Medical Therapy (n=40)
Bypass (n=48)
Sleeve (n=49)
Age (yrs) 50.3 48.0 47.8
Females 67% 58% 78%
Duration of diabetes (yrs) 8.8 8.0 8.3
HbA1c (%) 9.0 9.3 9.5
Body Mass Index (kg/m2) 36.4 37.1 36.1
≥ 3 diabetes medications 61% 52% 46.9%
Insulin use 51.2% 46% 44.9%
Depression 32% 37% 46%
Microvascular complications 20% 42% 29%
Note: Based on analyzed population Schauer et al. NEJM 2014

Primary and Secondary Endpoints at 36 Months
Parameter Medical Therapy (n=40)
Bypass (n=48)
Sleeve (n=49)
P Value1
P Value2
HbA1c ≤ 6% 5% 37.5% 24.5% <0.001 0.012 HbA1c ≤ 6% (without DM meds) 0% 35.4% 20.4% <0.001 0.002
HbA1c ≤ 7% 40% 64.6% 65.3% 0.02 0.02 Change in FPG (mg/dL) -6 -85.5 -46 0.001 0.006 Relapse of glycemic control 80% 23.8% 50% 0.03 0.34
% change in HDL +4.6 +34.7 +35.0 <0.001 <0.001 % change in TG -21.5 -45.9 -31.5 0.01 0.01
1 Gastric Bypass vs Medical Therapy; 2 Sleeve vs Medical Therapy
Schauer et al. NEJM 2014

0.0
-0.5
-1.0
-1.5
-2.0
-2.5
-3.0
-3.50 3 6 12 24 36
0.0
-0.5
-1.0
-1.5
-2.0
-2.5
-3.0
-3.50 3 6 12 24 36
Change in HbA1c
Change in HbA1c (%)
P<0.001
P<0.001
Value at Visit Baseline Month 6 Month 12 Month 24 Month 36Medical 9.0 (8.5) 7.1 (6.8) 7.5 (6.9) 7.7 (7.3) 8.4 (7.6)Gastric Bypass 9.3 (9.2) 6.3 (6.2) 6.3 (6.1) 6.5 (6.4) 6.7 (6.6)Sleeve 9.5 (8.9) 6.7 (6.4) 6.6 (6.4) 6.8 (6.8) 7.0 (6.6)
Value at Visit Baseline Month 6 Month 12 Month 24 Month 36Medical 9.0 (8.5) 7.1 (6.8) 7.5 (6.9) 7.7 (7.3) 8.4 (7.6)Gastric Bypass 9.3 (9.2) 6.3 (6.2) 6.3 (6.1) 6.5 (6.4) 6.7 (6.6)Sleeve 9.5 (8.9) 6.7 (6.4) 6.6 (6.4) 6.8 (6.8) 7.0 (6.6)
Medical Sleeve Gastric Bypass

Change in Body Mass Index
Change in BMI
(Kg/M2)
-12.0
-10.0
-8.0
-6.0
-4.0
-2.0
0.0
-12.0
-10.0
-8.0
-6.0
-4.0
-2.0
0.0
90 3 6 12 24 360 3 6 12 24 369
P=0.006
P<0.001
P<0.001
Value at Visit Baseline Month 6 Month 12 Month 24 Month 36Medical 36.4 34.6 34.2 35.0 34.8Gastric Bypass 37.1 28.2 26.7 27.3 27.9Sleeve 36.1 28.3 27.1 27.9 29.2
Value at Visit Baseline Month 6 Month 12 Month 24 Month 36Medical 36.4 34.6 34.2 35.0 34.8Gastric Bypass 37.1 28.2 26.7 27.3 27.9Sleeve 36.1 28.3 27.1 27.9 29.2
Medical Sleeve Gastric Bypass

Change in Diabetes Medications
Schauer et al. NEJM 2014
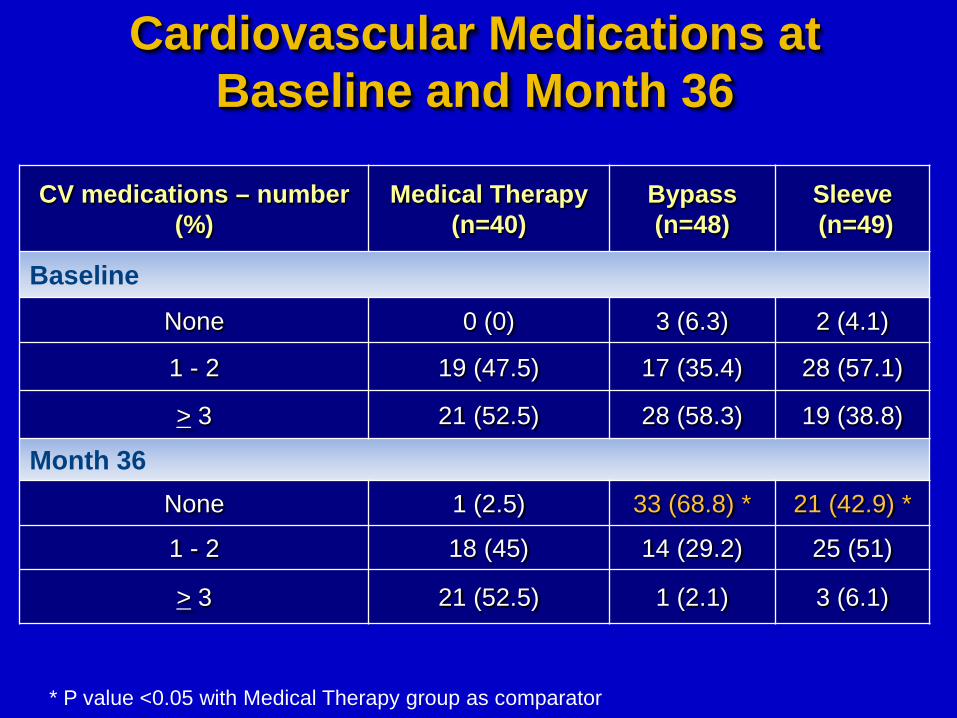
Cardiovascular Medications at Baseline and Month 36
CV medications – number (%)
Medical Therapy (n=40)
Bypass (n=48)
Sleeve (n=49)
Baseline None 0 (0) 3 (6.3) 2 (4.1)
1 - 2 19 (47.5) 17 (35.4) 28 (57.1)
> 3 21 (52.5) 28 (58.3) 19 (38.8)
Month 36 None 1 (2.5) 33 (68.8) * 21 (42.9) *
1 - 2 18 (45) 14 (29.2) 25 (51)
> 3 21 (52.5) 1 (2.1) 3 (6.1)
* P value <0.05 with Medical Therapy group as comparator

Change in Quality of Life Measures
Physical Functioning
Role Limitations
Physical Health Components
Mental Health Components
** **
* <0.05 ** <0.001 (Compared to IMT) **
*
* %
% *
*

Summary: QOL Changes
• Gastric Bypass: 5/8 domains improved
• Sleeve Gastrectomy: 2/8 domains improved
• Intensive Med Rx: 0/8 domains improved

BMI < 35 vs. BMI ≥ 35 Change in HbA1c

Adverse Events through 36 Months
•No Deaths
•Reoperations: 4 (sleave leak, gallstones, bleeding, abd pain)

Adverse Events through 36 Months

Adverse Events through 36 Months
No Difference Between Groups
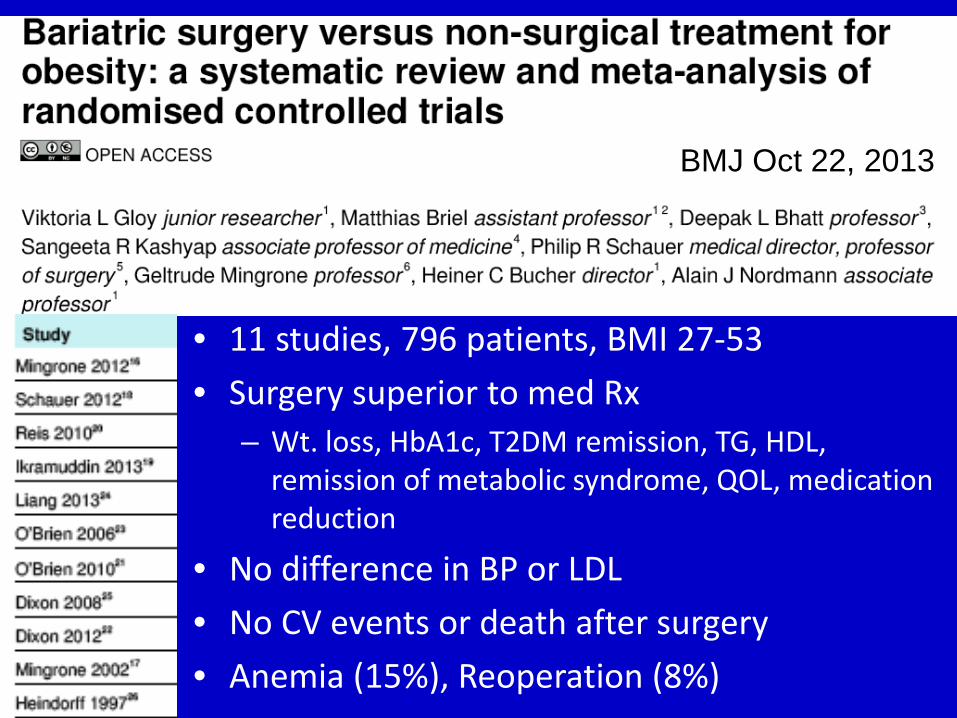
BMJ Oct 22, 2013
• 11 studies, 796 patients, BMI 27-53 • Surgery superior to med Rx
– Wt. loss, HbA1c, T2DM remission, TG, HDL, remission of metabolic syndrome, QOL, medication reduction
• No difference in BP or LDL • No CV events or death after surgery • Anemia (15%), Reoperation (8%)

Surgical vs Medical Treatments for Type 2 Diabetes Mellitus: A Randomized Clinical Trial
Anita P. Courcoulas, MD, MPH; Bret H. Goodpaster, PhD; Jessie K Eagleton, MPH; Steven H. Belle, PhD, MScHyg; Melissa A. Kalarchian, PhD; Wei Lang, PhD; Frederico G.
S. Toledo, MD; John M. Jakicic, PhD
Roux-en-Y Gastric Bypass Surgery or Lifestyle With Intensive Medical Management in Patients With Type 2 Diabetes Feasibility
and 1-Year Results of a Randomized Clinical Trial Florencia Halperin, MD; Su-Ann Ding, MD; Donald C. Simonson, MD, MPH, ScD;
Jennifer Panosian, BA; Ann Goebel-Fabbri, PhD; Marlene Wewalka, MD; Osama Hamdy, MD, PhD; Martin Abrahamson, MD; Kerri Clancy, RN;
Kathleen Foster, RN; David Lautz, MD; Ashley Vernon, MD; Allison B. Goldfine, MD
2 More Recent RCT’s JAMA Surgery June 4, 2014
Both Show Superiority of Surgery vs. Intensive Medical RX
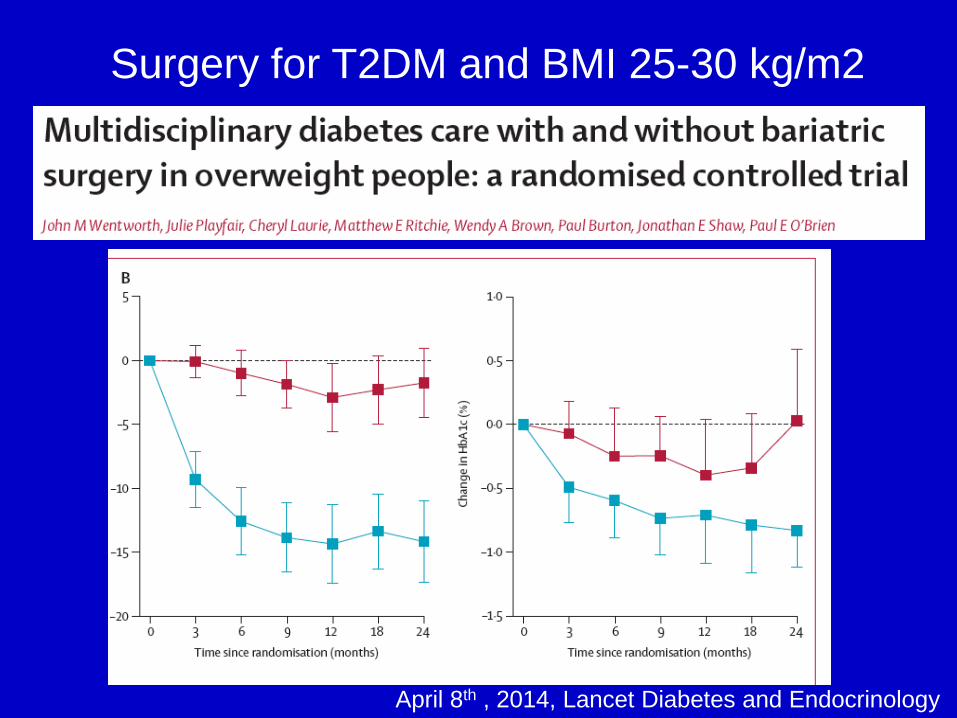
April 8th , 2014, Lancet Diabetes and Endocrinology
Surgery for T2DM and BMI 25-30 kg/m2
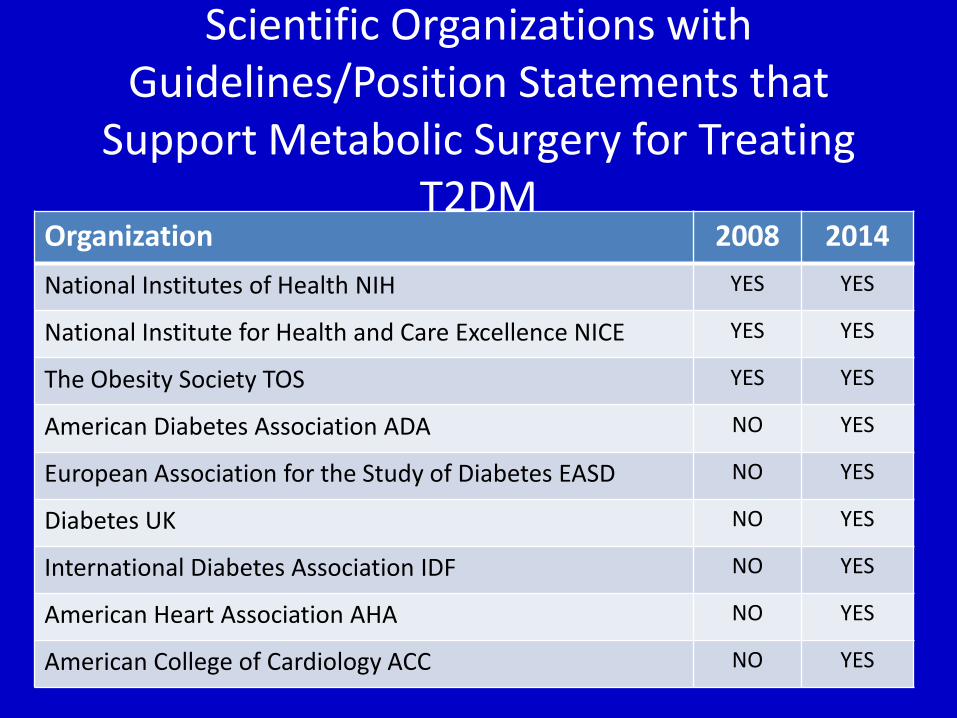
Scientific Organizations with Guidelines/Position Statements that
Support Metabolic Surgery for Treating T2DM
Organization 2008 2014 National Institutes of Health NIH YES YES
National Institute for Health and Care Excellence NICE YES YES
The Obesity Society TOS YES YES
American Diabetes Association ADA NO YES
European Association for the Study of Diabetes EASD NO YES
Diabetes UK NO YES
International Diabetes Association IDF NO YES
American Heart Association AHA NO YES
American College of Cardiology ACC NO YES
International Diabetes Federation Guidelines
• Surgery should be an accepted option in people who have type 2 diabetes and BMI of 35 or more
• Surgery should also be considered as an alternative treatment option in persons with BMI 30 to 35 when diabetes cannot be adequately controlled by optimal medical regimen, especially in the presence of other major cardiovascular disease risk factors
• In Asian, and some other ethnicities of increased risk, BMI action points may be lower e.g. BMI 27.5 to 32.5
Bariatric Surgical and Procedural Interventions in the Treatment of Obese Patients with Type 2 Diabetes
Download at www.idf.org

Summary Bariatric Surgery for T2DM
• 14 RCT’s (>950 patients, BMI 25-52) show that surgery results in superior glycemic control compared to medical Rx ( up to 3 year follow-up)
• CV risk factors improved with surgery
• Surgery significantly improves quality of life
• Surgery reduces mortality/CV events (non-RCT, SOS)
• Perioperative morbidity <5%, mortality < 0.3%
Conclusion Bariatric Surgery for T2DM
Patients with uncontrolled T2DM (HbA1c >7.0%) and Obesity (BMI > 30) should be considered for bariatric surgery

THANK YOU! Role of Bariatric Surgery in
Obesity and Diabetes
Cleveland Clinic Bariatric and Metabolic Institute Endocrinology, Diabetes and Metabolism
Philip R. Schauer, MD Professor of Surgery, Cleveland Clinic Lerner College of Medicine
Director: Bariatric and Metabolic Institute (BMI) [email protected]