role of cbt in copd management simon dupont hillingdon hospital
TRANSCRIPT
Role of CBT in COPD management
Simon DupontHillingdon Hospital

Resources
Demands
Resources
1. Physical health
2. Skills and experience
3. Emotional make-up
4. Social support
5. Ability to relax
Demands
• Demands of everyday life: daily hassles
• Life changes (e.g. giving up work, bereavement)
• Social factors (problems in relationships, loneliness)
• Health issues (exacerbations of illness)
• Personal factors (feelings of low self-esteem)
STRESS
What is stress?
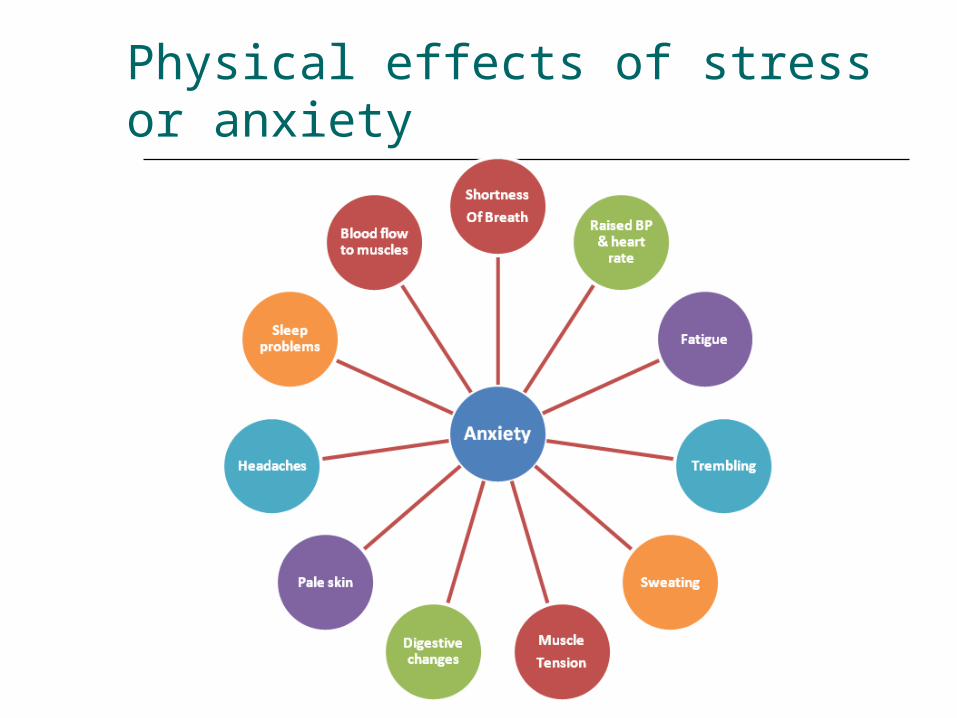
Physical effects of stress or anxiety

Emotional effects of stress or anxiety
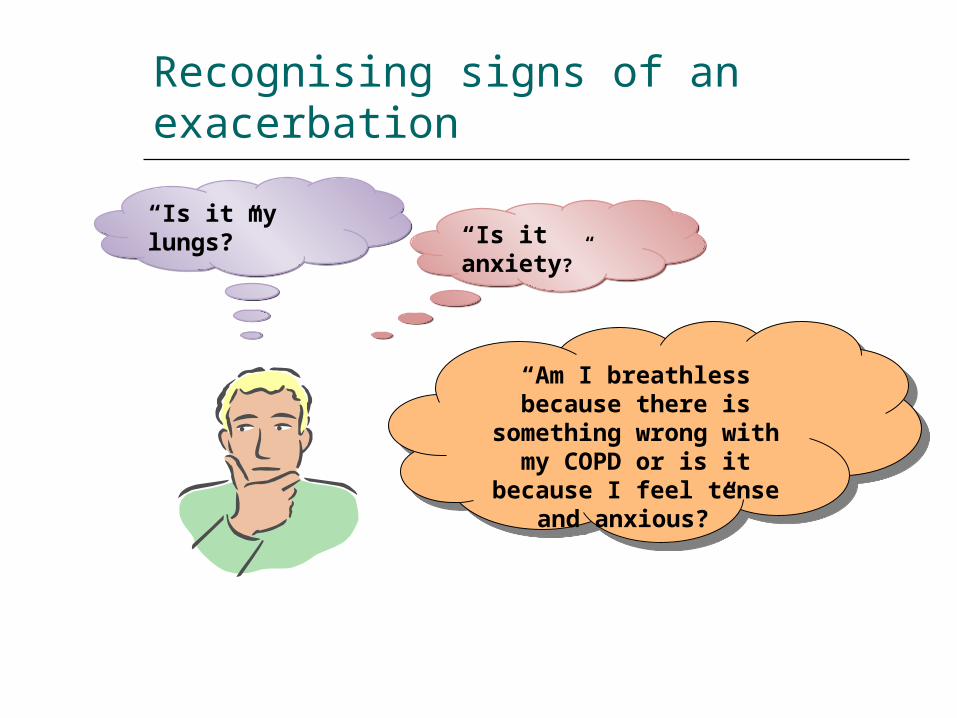
Recognising signs of an exacerbation
“Am I breathless because there is
something wrong with my COPD or is it
because I feel tense and anxious?”
“Am I breathless because there is
something wrong with my COPD or is it
because I feel tense and anxious?”
“Is it anxiety?”“Is it anxiety?”“Is it my lungs?”“Is it my lungs?”

CBT cycle

Rationale for CBT
It is not events themselves that cause distress but what they mean to us
Meaning is influenced by past experiences, past learning, our individual rules and the beliefs that we have developed
The way in which we interpret events can be biased and cause undue distress
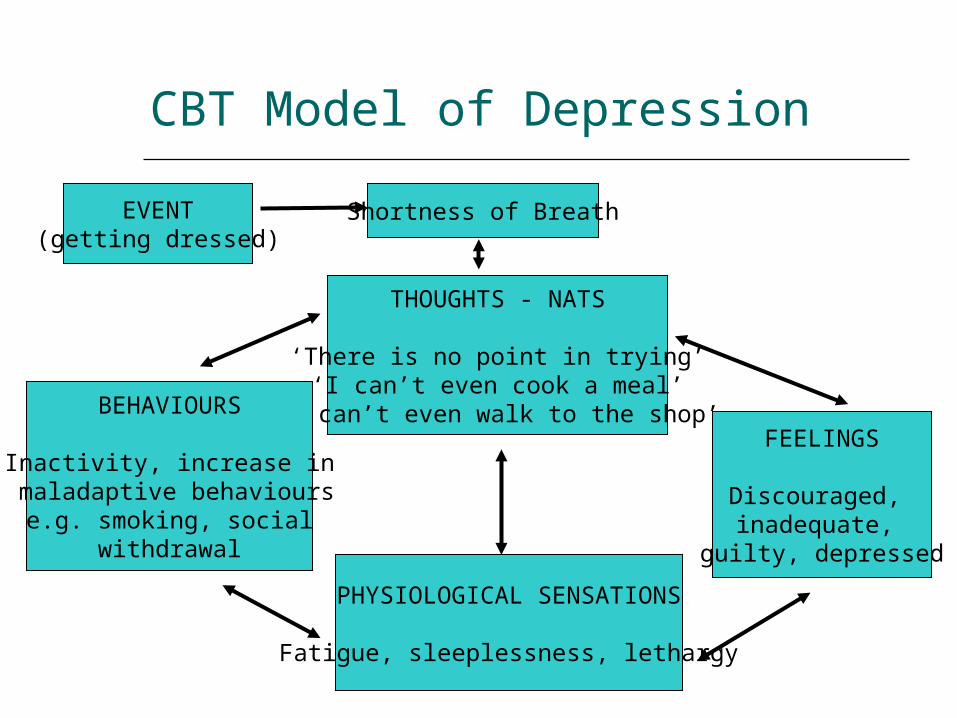
CBT Model of Depression
Shortness of Breath
FEELINGS
Discouraged, inadequate,
guilty, depressed
THOUGHTS - NATS
‘There is no point in trying’‘I can’t even cook a meal’
‘I can’t even walk to the shop’
PHYSIOLOGICAL SENSATIONS
Fatigue, sleeplessness, lethargy
BEHAVIOURS
Inactivity, increase in maladaptive behaviours
e.g. smoking, social withdrawal
EVENT(getting dressed)

Bob’s example…
Bob has COPD. That morning he was in a hurry, worrying about being late for an appt. Breathing got worse, increased anxiety “I can’t get my breath back”…further anxiety…
Heart pounding, gasping for breath, sick, sweaty, dizzy, out of control “I’m dying”, “It’s getting worse” = PANIC ATTACK
Family also frightened, feel helpless – call an ambulance
Negative Automatic Thoughts
Just pop into your head
Are involuntary
Do not always fit the facts
Affect how you feel
Affect what you do

Unhelpful thinking
CatastrophisingThoughts about worst possible outcome. “I’m out of breath, my lungs are being damaged, I’m about to die”.
Generalisation“ Because I’m short of breath in this shop, I’ll also be short of breath
in all shops”.
All or nothing thinking“Because I cannot do it as before I will not do it at all”. People give up activities that have become harder
Mind readingPeople think they know what other people are thinking and assume that it is negative without checking it out.

Practical tips- help patient to ID and challenge NATS
Identify NATS/images What went through your mind before you started feeling
that way?
Challenge the thoughts What’s the evidence for and against the thought? Are there any thinking errors? What would happen if the thought remains unchallenged? Is there another way of thinking about this?
Whittington psychology pilot
Psychology-led sessions:
anxiety and breathlessness living with a breathing problem /
managing low mood goal setting managing flare-ups relaxation sleep
Psychology pilot
2 sessions a week for one year
Modifying the education sessions to be more interactive with a focus on supporting self-management and building self-efficacy
Switch from rolling programme to stop-start
Psychologist attended assessments and the PR group once a week
Psychologist offered individual therapy to any patients showing high levels of distress or other potential barriers to completion

Conclusions of Whittington
Addressing psychological barriers to attendance at PR may improve completion rates
Improving completion is important in reducing future hospital resource usage
Targeting self-efficacy (mastery) in the context of PR may be a primary factor in improving self-management skill and completion of PR

Invite to PR
Accept and start PR
If anxious or depressed,
frequent A&E attenders, offer
psychology input
Complete psychology
sessions then offer PR
Complete PR
Complete PR
Issues with attendance at PR/ freq A&E attenders/would
benefit from additional input for anxiety or
depression
Offer psychology
input. Complete alongside
PR or rejoin PR
Combining PR & CBT
How to assess - starter for ten
Do you think
anxiety
has contributed to
any of your hospital admissions?

THE GAD-2
Over the last 2 weeks, how often have you Not Several More than Nearlybeen bothered by the following problems? at all days half the every day
days(Use “✔” to indicate your answer)
1. Feeling nervous, anxious or on edge 0 1 2 3
2. Not being able to stop or control worrying 0 1 2 3
If total score is 3 or more, complete GAD-7
Assessment - anxiety
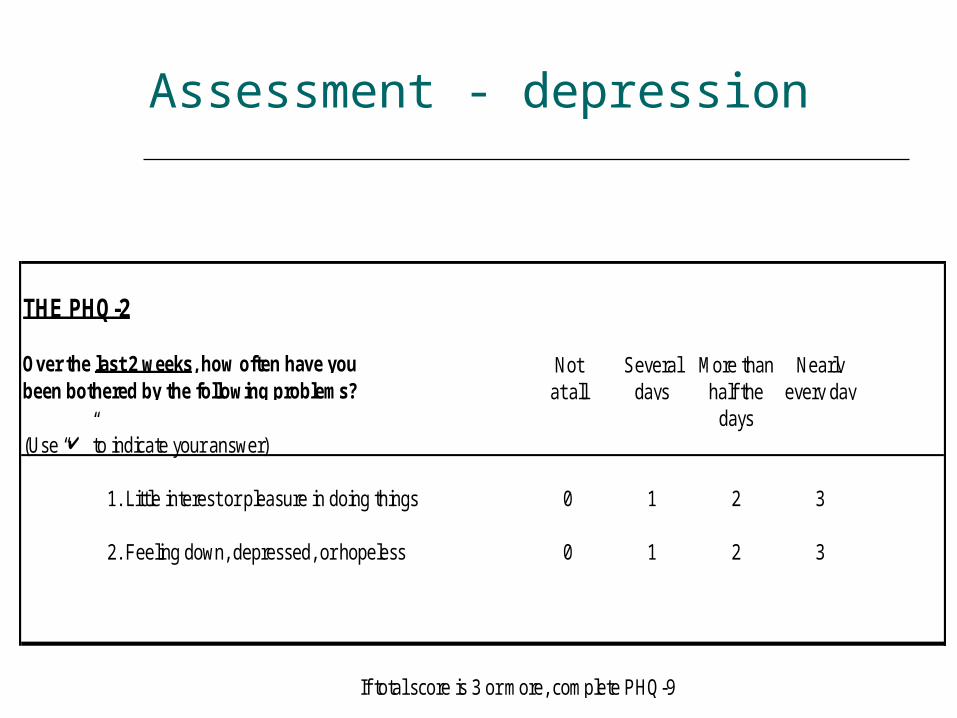
Assessment - depression
THE PHQ-2
Over the last 2 weeks, how often have you Not Several More than Nearlybeen bothered by the following problems? at all days half the every day
days(Use “✔” to indicate your answer)
1. Little interest or pleasure in doing things 0 1 2 3
2. Feeling down, depressed, or hopeless 0 1 2 3
If total score is 3 or more, complete PHQ-9
Open Style of Consultation
BATHE technique - Lieberman & Stuart 1993
Background – what’s going on in your life?
Affect – how do you feel about this?
Trouble – what troubles you about that?
Handling – how are you handling that?
Empathy – that must be difficult for you
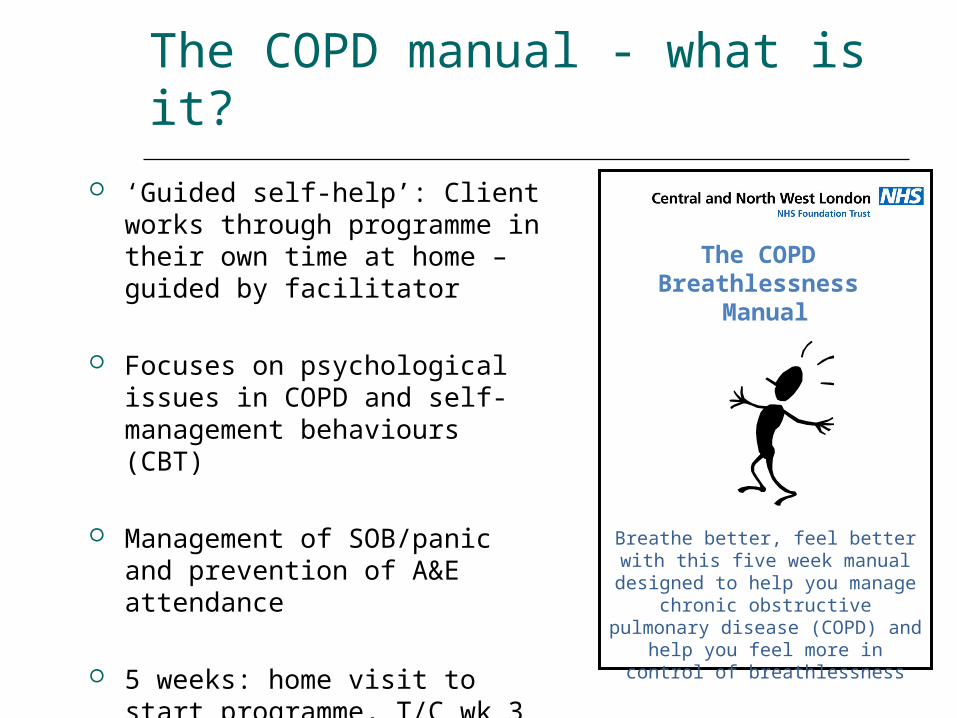
The COPD manual - what is it?
‘Guided self-help’: Client works through programme in their own time at home – guided by facilitator
Focuses on psychological issues in COPD and self-management behaviours (CBT)
Management of SOB/panic and prevention of A&E attendance
5 weeks: home visit to start programme, T/C wk 3 & 6
The COPD Breathlessness
Manual
Breathe better, feel better with this five week manual designed
to help you manage chronic obstructive pulmonary disease (COPD) and help you feel more
in control of breathlessness
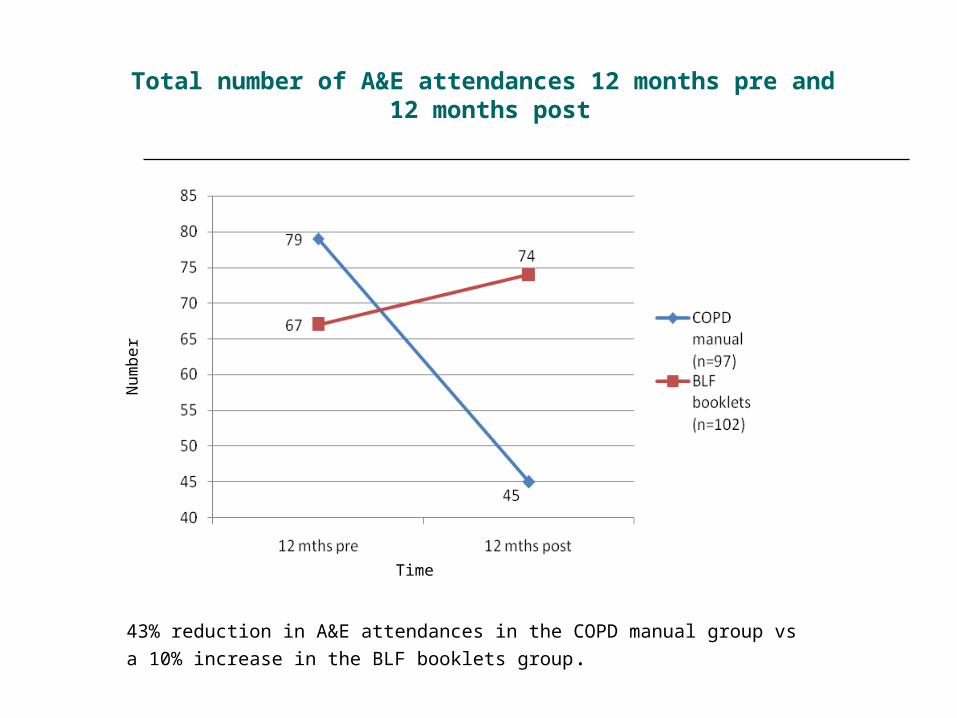
Total number of A&E attendances 12 months pre and 12 months post
43% reduction in A&E attendances in the COPD manual group vs
a 10% increase in the BLF booklets group.
Time
Num
ber
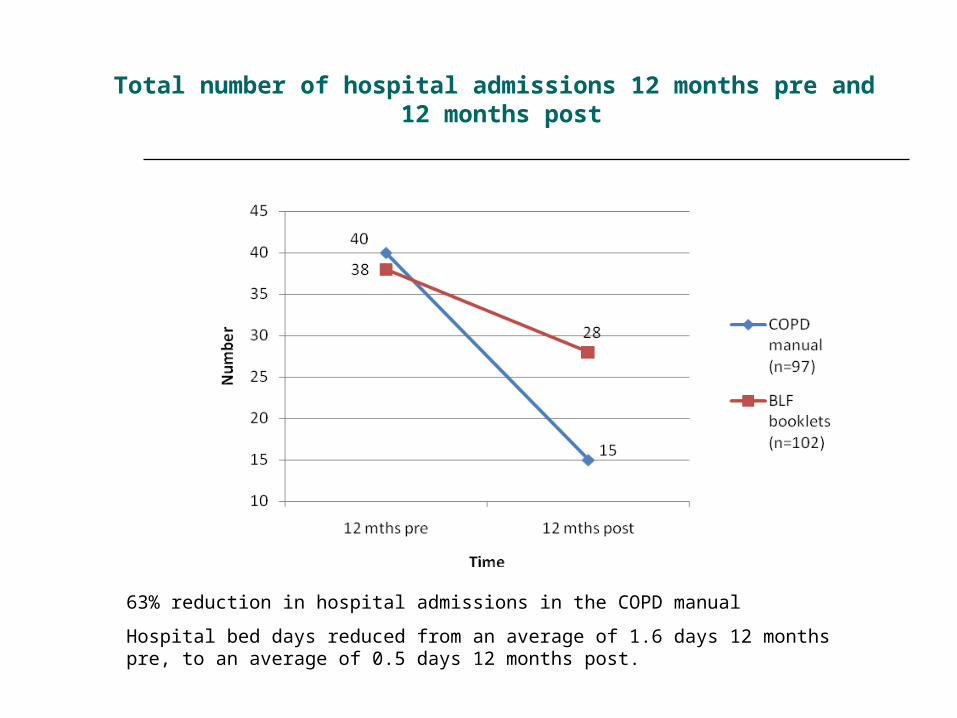
Total number of hospital admissions 12 months pre and 12 months post
63% reduction in hospital admissions in the COPD manual
Hospital bed days reduced from an average of 1.6 days 12 months pre, to an average of 0.5 days 12 months post.

Anxiety changes over time Depression changes over time
HA
D s
core
s
HA
D s
core
s
Time Time
Changes in Anxiety and Depression over time

Websites
By Chris Williams: www.livinglifetothefull.com (for users) www.fiveareas.com (for practitioners)
From NHS Choices website: www.fearfighter.com

Books on Prescription
http://readingagency.org.uk/about/BoP%20core%20booklist%20with%20copyright.pdf