role of dphs in tobacco endgame - wordpress.com · role of dphs in tobacco endgame malaysia ......
TRANSCRIPT
Role of DPHS in Tobacco endgame Malaysia
Dr Lydia Mason Dental Public Health Specialist
BDS ,MPH(OH)University Malaya
Dr L Mason 12 March 2017 1 8th MADPHS Conference 2017
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 2
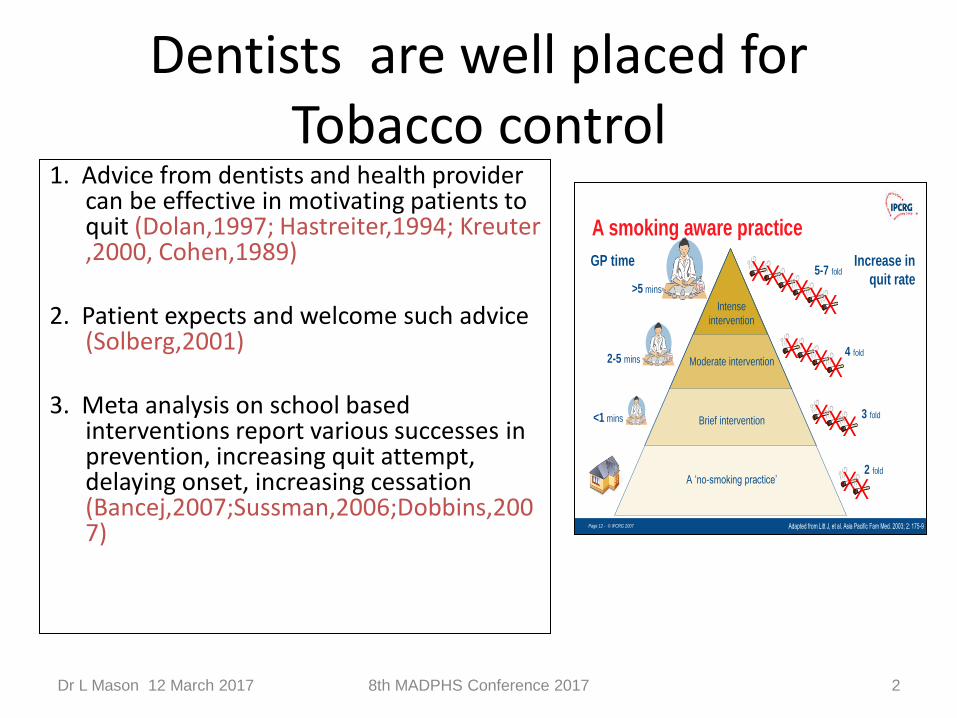
1. Advice from dentists and health provider can be effective in motivating patients to quit (Dolan,1997; Hastreiter,1994; Kreuter ,2000, Cohen,1989)
2. Patient expects and welcome such advice
(Solberg,2001) 3. Meta analysis on school based
interventions report various successes in prevention, increasing quit attempt, delaying onset, increasing cessation (Bancej,2007;Sussman,2006;Dobbins,2007)
Page 12 - © IPCRG 2007Page 12 - © IPCRG 2007Page 12 - © IPCRG 2007
A smoking aware practice
Adapted from Litt J, et al. Asia Pacific Fam Med. 2003; 2: 175-9
Increase in
quit rate
GP time
A ‘no-smoking practice’
Brief intervention
Moderate intervention
Intense
intervention
>5 mins
<1 mins
2-5 mins
2 fold
3 fold
4 fold
5-7 fold
Dentists are well placed for Tobacco control
Tobacco use : A public health problem
• Tobacco consumption continues to be the leading preventable cause of death in the world.
• As research and findings continue to show the negative effects of tobacco consumption on health and the number of affected people increases, the list of conditions caused by tobacco consumption has grown.
Dr L Mason 12 March 2017 3 8th MADPHS Conference 2017
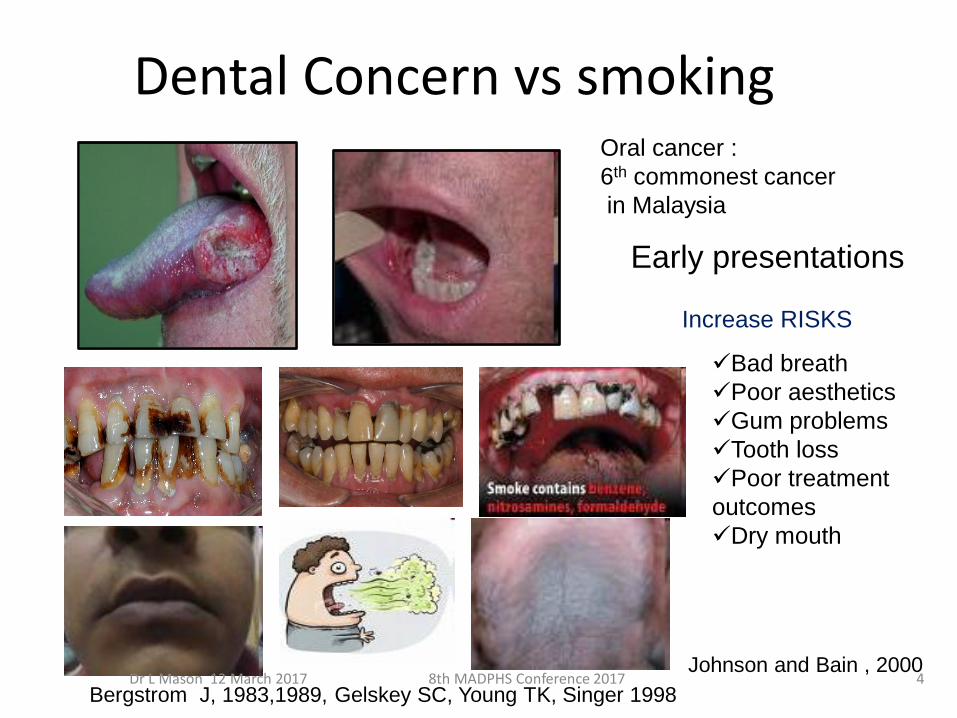
Dental Concern vs smoking Oral cancer :
6th commonest cancer
in Malaysia
Bad breath
Poor aesthetics
Gum problems
Tooth loss
Poor treatment
outcomes
Dry mouth
Increase RISKS
Johnson and Bain , 2000
Bergstrom J, 1983,1989, Gelskey SC, Young TK, Singer 1998
Early presentations
Dr L Mason 12 March 2017 4 8th MADPHS Conference 2017
Magnitude of the problem
• Currently, there are an estimated 1.3 billion
smokers in the world. The death toll from tobacco consumption is now 4.9 million people a year;
• If present consumption patterns continue, the
number of deaths will increase to 10 million
by the year 2020, 70% of which will occur in
developing countries
Dr L Mason 12 March 2017 5 8th MADPHS Conference 2017
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 6
MALAYSIA SCENARIO
• Smoking is the #1 cause of preventable death in Malaysia: – 11,000 deaths every year
• 20% of all deaths
• 90% of all preventable deaths
• Half of all smokers will die from their addiction, losing, on average, 15 years of their life and quality of Life
Harms the economy and sustainable development
Widen gap of poverty ( lower social economic grps most affected)
5 million smokers@ average 14 sticks/day is equivalent to
5 Million x rm17/pack = RM105 Million /day
Tobacco use = Regressive habits
Addictive and need to consume more to get similar effect as years go by
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 7
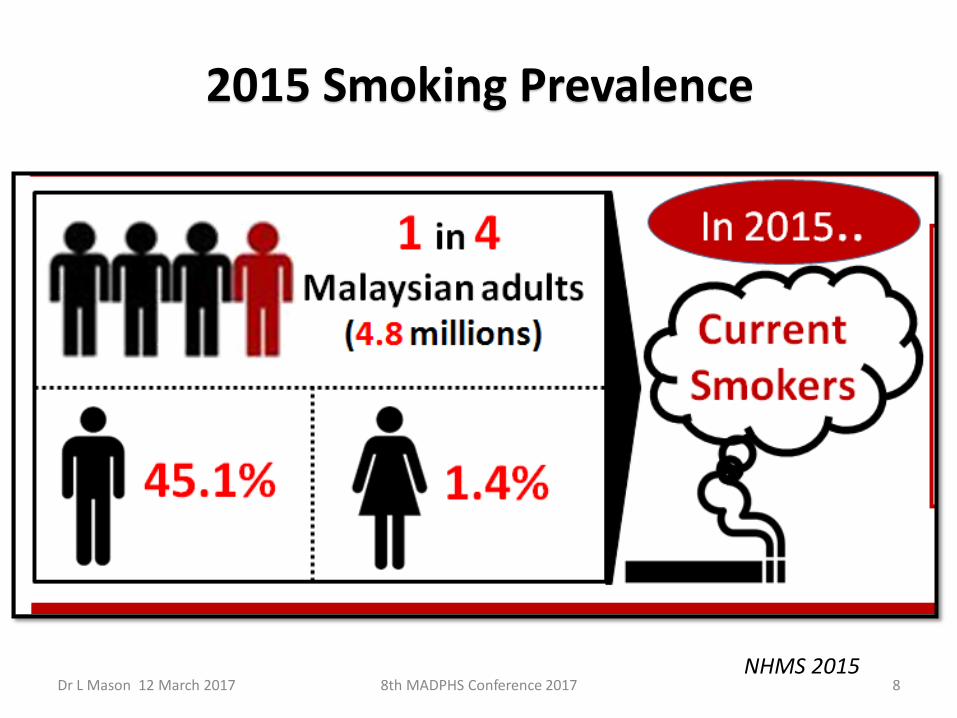
2015 Smoking Prevalence
NHMS 2015 Dr L Mason 12 March 2017 8 8th MADPHS Conference 2017
The sad thing is ….. those who consume tobacco are not the only ones exposed to its negative effects.
Dr L Mason 12 March 2017 9 8th MADPHS Conference 2017
Passive smokers
• Millions of people, including one half of the
world’s children, are exposed to second-hand tobacco smoke, known also as passive smoking
• Passive smoking is a health problem that requires society’s active effort
Dr L Mason 12 March 2017 10 8th MADPHS Conference 2017
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 11
Passive smoker– at home
• Approximately 30-40% of Malaysians are exposed to second hand smoke in their homes
• Children and women are most likely to be exposed
DPHS • DPHS have a prominent role to play in tobacco
control.
• They have the trust of the population, the media and opinion leaders, and their voices are heard across a vast range of social, economic and political arenas
Dr L Mason 12 March 2017 12 8th MADPHS Conference 2017
Role
1. Protecting people from taking up tobacco consumption;
2. Promoting cessation
3. Protecting non-smokers from the exposure to tobacco smoke
4. Regulating tobacco products.
Dr L Mason 12 March 2017 13 8th MADPHS Conference 2017
DPHS placements
• MOH-different level of care
• MOD
• MOHE
• Universities (Public and Private)
• Solo practices (DPHS in Private practice)
• Members of NGOs
• Alliance
Dr L Mason 12 March 2017 14 8th MADPHS Conference 2017
As health professional
• DPHS can educate the population on the harms of tobacco use and exposure to second-hand smoke.
• Get involved actively in early prevention and
• Offer help to tobacco users to overcome their addiction and
• Provide quit advises
Dr L Mason 12 March 2017 15 8th MADPHS Conference 2017
At Community level
• DPHS professionals can be initiators or supporters of some of the policy measures by engaging in efforts to promote smoke-free environment and extending the availability of tobacco cessation resources to their caption groups
Dr L Mason 12 March 2017 16 8th MADPHS Conference 2017
At Societal level
• DPHS can add their voice and their weight to national and global tobacco control efforts like
tax increase campaigns and become involved at the national level in promoting the WHO Framework Convention on Tobacco Control (WHO FCTC )
Dr L Mason 12 March 2017 17 8th MADPHS Conference 2017
Leadership
DPHS should become a role model for other professional organizations and society by embracing the tenants of the Health Professional Code of Practice on Tobacco Control.
Dr L Mason 12 March 2017 18 8th MADPHS Conference 2017
Research for evidence
• No matter where DPHS are
• We need evidence for best practice
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 19

Advocacy for policy
• Watchdog
• Refer SEATCA
• Professional voice
• Build sound Public
Health Policy*
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 20

Opportunity for partnership and Alliance
In any setting
• Global
• Local
• Community
• Alliance with other Stake holders and NGOs
Dr L Mason 12 March 2017 21 8th MADPHS Conference 2017
WHO FCTC
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 22
Price and tax measures to reduce the demand for tobacco,
and
Non-price measures to reduce the demand for tobacco,
namely:
Protection from exposure to tobacco smoke;
Regulation of the contents of tobacco products;
Regulation of tobacco product disclosures;
Packaging and labelling of tobacco products;
Education, communication, training and public awareness;
Tobacco advertising, promotion and sponsorship; and,
Demand reduction measures concerning tobacco
dependence and cessation
Illicit trade in tobacco products; Sales to
and by minors; and, Provision of support
for economically viable alternative activities
Member States that
have signed the
Convention indicate
that they will strive in
good faith to ratify,
accept, or approve it,
and show political
commitment not to
undermine the
objectives set out in it. We are signatories to FCTC and it is legal binding

Dr L Mason 12 March 2017 8th MADPHS Conference 2017 23
A Global Thrust To Counter A Global Threat : FCTC + MPOWER + ENDGAME
FCTC (2003):Now 174 Countries Subscribe To The Treaty .Malaysia has signed and ratified.
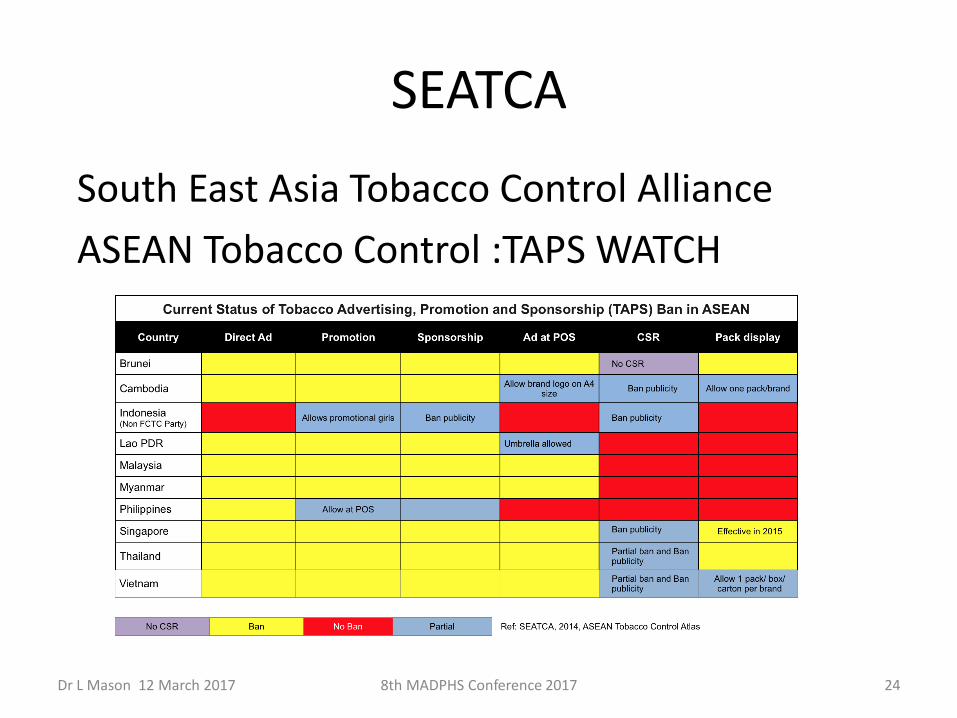
SEATCA
South East Asia Tobacco Control Alliance
ASEAN Tobacco Control :TAPS WATCH
Dr L Mason 12 March 2017 24 8th MADPHS Conference 2017
SEATCA is committed to work hand in hand with countries in ASEAN to promote health and save lives by
1. fast-tracking and effectively implementing the
evidence-based tobacco control measures contained in
the WHO FCTC.
promote increased participation and cooperation among
tobacco control advocates at the regional level,
organize regional forum for sharing lessons and best practices in advancing tobacco control policies,
act as a regional leader on issues that are priorities in all the countries in the region
Dr L Mason 12 March 2017 25 8th MADPHS Conference 2017
DPHS in Universities • Capacity and capability building
• Curriculum/ teaching /building tobacco control skills
• Screening and intervention
• Cognitive behavioral therapy
• Balance decision guide
• Quit clinic with or without NRT
• Research community
Dr L Mason 12 March 2017 26 8th MADPHS Conference 2017
DPHS in the Army
• ADS
• Clinical setting
Dr L Mason 12 March 2017 27 8th MADPHS Conference 2017
DPHS in MOH
• Clinical setting
• School based approach
• Outreach programmes
Dr L Mason 12 March 2017 28 8th MADPHS Conference 2017

Dr L Mason 12 March 2017 8th MADPHS Conference 2017 29
School based tobacco use prevention interventions has been
shown be effective in smoking prevention, control and
cessation.
Sources:Dobbins,2007; Grimshaw and Stanton ,2006; Sussaman, 2006;
MMWR,1994;Bancej et al,2007;
The most promising one for MOH
The school based –dental approach
• Ambitious concept
• Achievable strategies
Dr L Mason 12 March 2017 30 8th MADPHS Conference 2017
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 31
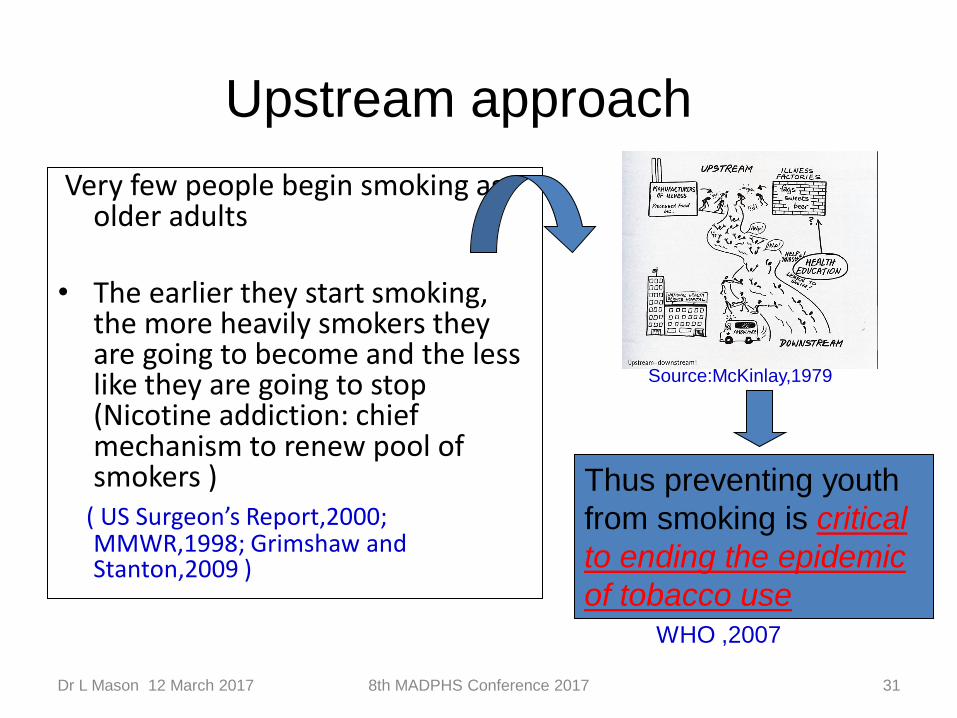
Very few people begin smoking as older adults
• The earlier they start smoking,
the more heavily smokers they are going to become and the less like they are going to stop (Nicotine addiction: chief mechanism to renew pool of smokers )
( US Surgeon’s Report,2000; MMWR,1998; Grimshaw and Stanton,2009 )
Thus preventing youth
from smoking is critical
to ending the epidemic
of tobacco use WHO ,2007
Source:McKinlay,1979
Upstream approach

Dr L Mason 12 March 2017 8th MADPHS Conference 2017 32
Rationale why school service is targeted
1.Adolescents are difficult to enrolled in clinic based quit clinic services due to many barriers. (Disciplinary ,punitive, privacy , consent, time ,transport, money )and are helpless on their own.
2.School-based setting provide ease of enrollment , follow up, reduce barriers ,decrease attrition .Socially acceptable (do not discriminate smokers/non smokers) and F.O.C.
3. Use of SDS can optimize service and reduce costs
4. Adolescents = a caption group who can be used to promote health to their peers, families and communities
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 33
Rationale for using SDS
1. Potentially high number of adolescent smokers attending the SDS every year (From and annual pool of 7 million students )
2. Annual OH screening (From primary 1- Form 5): allow for long term follow up to follow through the stages of change in smoking behaviour
3. Detection of nicotine stain on teeth and smokers breath during oral examination provides an opportunity for teachable moments in TC as well as detection of smokers.
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 34
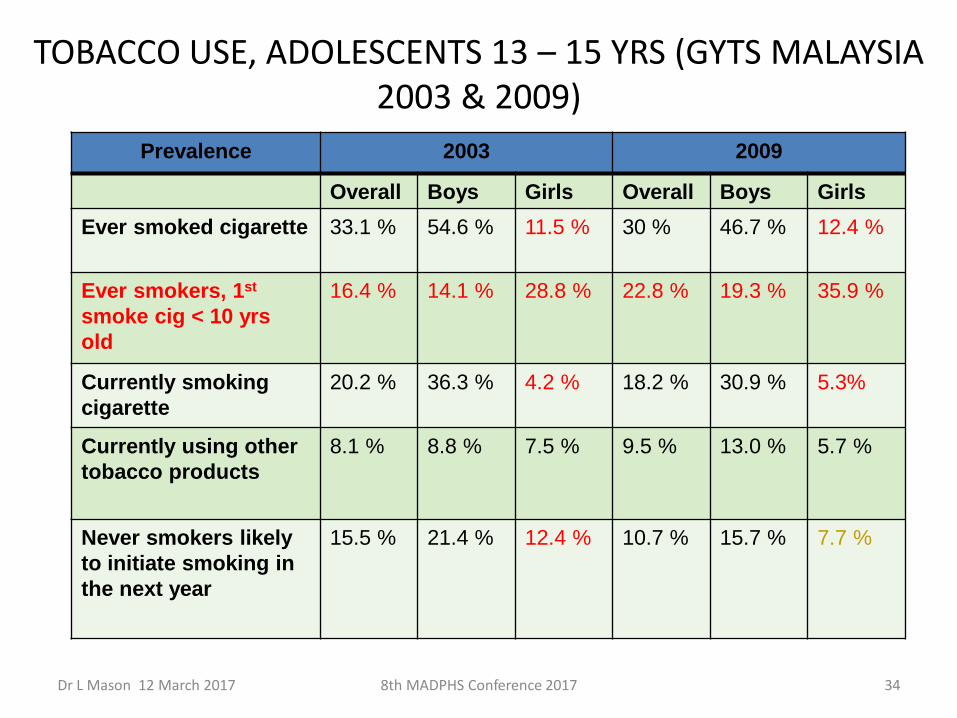
TOBACCO USE, ADOLESCENTS 13 – 15 YRS (GYTS MALAYSIA 2003 & 2009)
Prevalence 2003 2009
Overall Boys Girls Overall Boys Girls
Ever smoked cigarette 33.1 % 54.6 % 11.5 % 30 % 46.7 % 12.4 %
Ever smokers, 1st
smoke cig < 10 yrs
old
16.4 % 14.1 % 28.8 % 22.8 % 19.3 % 35.9 %
Currently smoking
cigarette
20.2 % 36.3 % 4.2 % 18.2 % 30.9 % 5.3%
Currently using other
tobacco products
8.1 % 8.8 % 7.5 % 9.5 % 13.0 % 5.7 %
Never smokers likely
to initiate smoking in
the next year
15.5 % 21.4 % 12.4 % 10.7 % 15.7 % 7.7 %
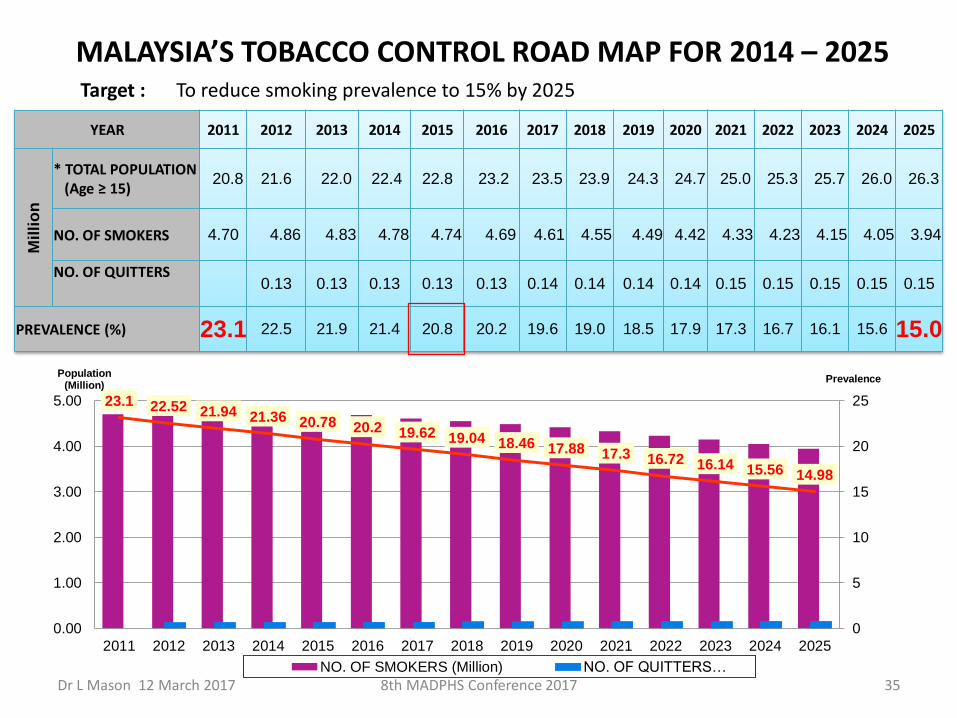
YEAR 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 2023 2024 2025
Mil
lio
n
* TOTAL POPULATION (Age ≥ 15)
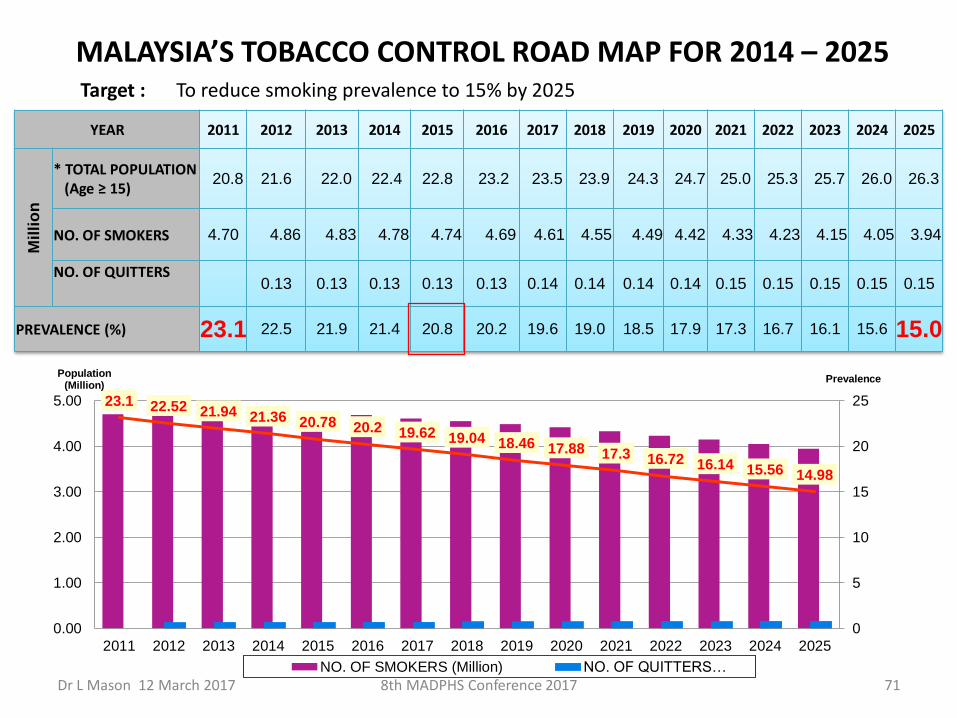
20.8 21.6 22.0 22.4 22.8 23.2 23.5 23.9 24.3 24.7 25.0 25.3 25.7 26.0 26.3
NO. OF SMOKERS 4.70 4.86 4.83 4.78 4.74 4.69 4.61 4.55 4.49 4.42 4.33 4.23 4.15 4.05 3.94
NO. OF QUITTERS
0.13 0.13 0.13 0.13 0.13 0.14 0.14 0.14 0.14 0.15 0.15 0.15 0.15 0.15
PREVALENCE (%) 23.1 22.5 21.9 21.4 20.8 20.2 19.6 19.0 18.5 17.9 17.3 16.7 16.1 15.6 15.0
MALAYSIA’S TOBACCO CONTROL ROAD MAP FOR 2014 – 2025 Target : To reduce smoking prevalence to 15% by 2025
23.1 22.52 21.94 21.36 20.78 20.2 19.62 19.04 18.46 17.88 17.3 16.72 16.14 15.56 14.98
0
5
10
15
20
25
0.00
1.00
2.00
3.00
4.00
5.00
2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 2023 2024 2025
Population (Million)
NO. OF SMOKERS (Million) NO. OF QUITTERS…
Prevalence
Dr L Mason 12 March 2017 35 8th MADPHS Conference 2017
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 36
Endgame Concepts On The Table
‘Endgame’ is a strategic plan to reduce prevalence within a set period (E.g. To < 5% globally by the year 2045)
• De-normalizing tobacco use
• Tobacco-free Generation Malaysia (No sale to those born after the year 2009) (S’pore , Thailand : those born from 2000)
• Focusing on supply-side measures; nicotine regulation
taxation and price controls
• Addressing tobacco as a systemic issue
• Removing profitability from the business of tobacco
• Making the tobacco industry liable
Our Biggest hope=endgame reforms
• Tobacco free generation
• Those born from 2009 onwards
• As of 2016 –we have data serveillance
• We will follow through cohorts
• We will produce serveillance data for the country
• Work with PAKEJ IMFREE ( HED,MySIHAT,MOE)
Dr L Mason 12 March 2017 37 8th MADPHS Conference 2017
Endgame reforms
• Children born from 2009 onwards –don’t smoke/use tobacco
• Decline in onset /initiation
• Decline in prevalence
• Increase in quit
• Smoking gets to a tipping point where it becomes easier to regulate OR even ban
Dr L Mason 12 March 2017 38 8th MADPHS Conference 2017
Endgame reforms
• High public understanding of the tobacco burden
• Rapid reduction in tobacco use prevalence
• Support from all stake holders and civil societies movement
• Strong leadership
• Strong Political Will ***
Dr L Mason 12 March 2017 39 8th MADPHS Conference 2017

WHA78
END GAME OF TOBACCO
15% <5%
2025 2045
Dr L Mason 12 March 2017 40 8th MADPHS Conference 2017
Can DPHS help fast track ???
Development of personal skills in Tobacco intervention
Dr L Mason 12 March 2017 41 8th MADPHS Conference 2017
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 42
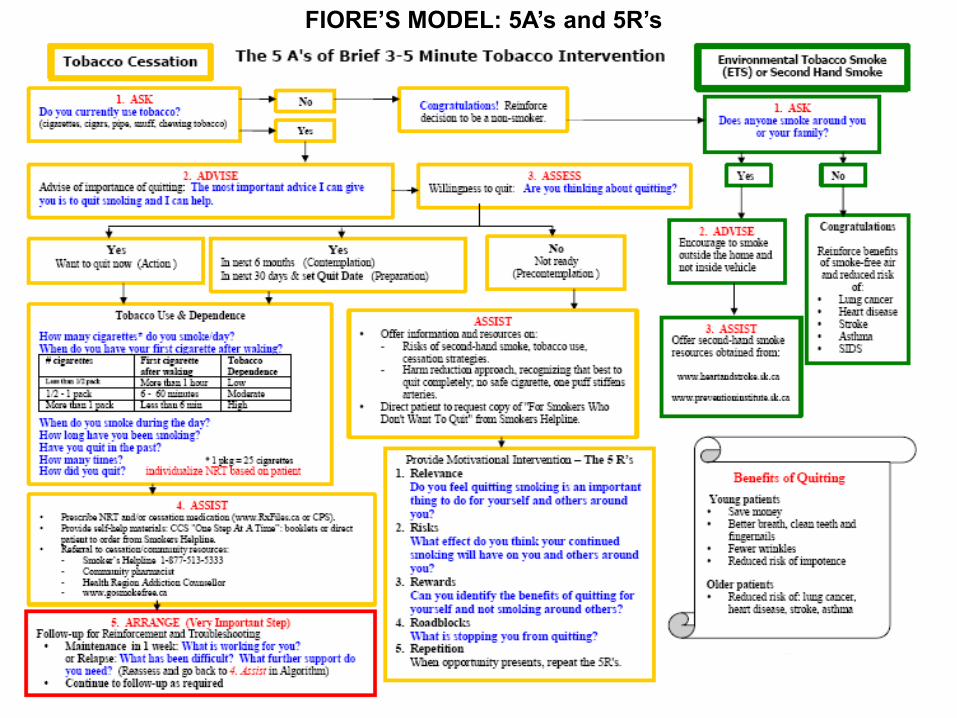
FIORE’S MODEL: 5A’s and 5R’s

Cigarette pattern • Cigarette record (time, situation, urge, mood)
No Time Activity Urge
Mood
1 Strong , Moderate Light
Sad Angry Relax
2
3
4
5
6
7
8
10
Dr L Mason 12 March 2017 43 8th MADPHS Conference 2017
Tests for level of addiction
The Fagerstrom Nicotine Dependence Questionnaire
AND OR validation with Smokerlyzer
Dr L Mason 12 March 2017 44 8th MADPHS Conference 2017
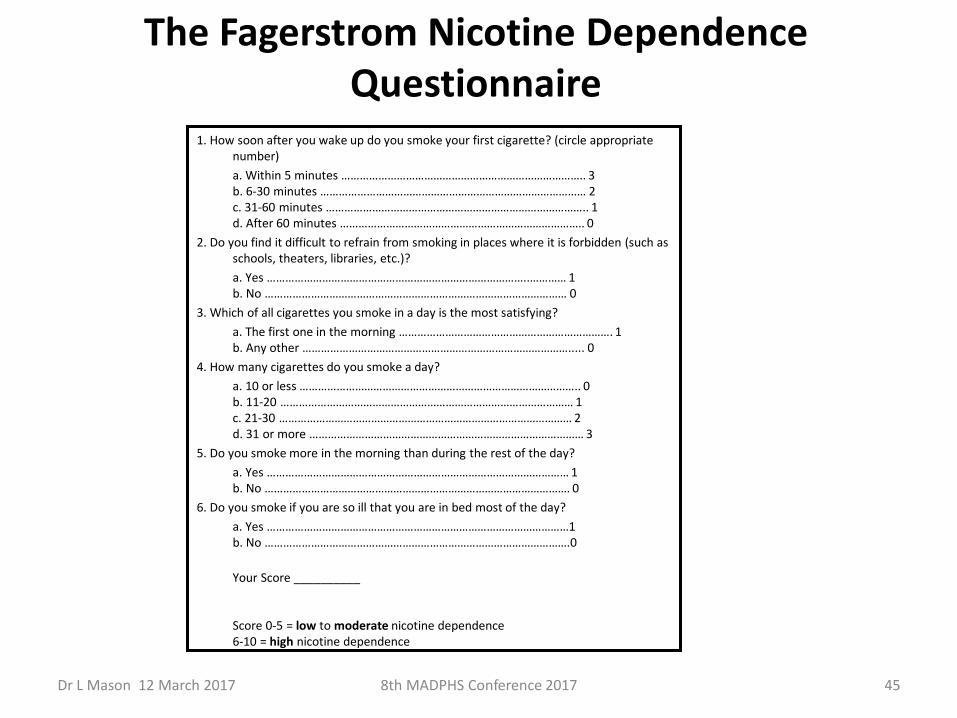
The Fagerstrom Nicotine Dependence Questionnaire
1. How soon after you wake up do you smoke your first cigarette? (circle appropriate number)
a. Within 5 minutes …………………………………………………………………….. 3 b. 6-30 minutes …………………………………………………………………………… 2 c. 31-60 minutes ………………………………………………………………………….. 1 d. After 60 minutes …………………………………………………………………….. 0
2. Do you find it difficult to refrain from smoking in places where it is forbidden (such as schools, theaters, libraries, etc.)?
a. Yes …………………………………………………………………………..………… 1 b. No ……………………………………………………………………………………… 0
3. Which of all cigarettes you smoke in a day is the most satisfying?
a. The first one in the morning ……………………………………………………………. 1 b. Any other ……………………………………………………………………………..... 0
4. How many cigarettes do you smoke a day?
a. 10 or less ……………………………………………………………………………….. 0 b. 11-20 …………………………………………………………………………………… 1 c. 21-30 …………………………………………………………………………………… 2 d. 31 or more ……………………………………………………………………………… 3
5. Do you smoke more in the morning than during the rest of the day?
a. Yes ……………………………………………………………………………………… 1 b. No ………………………………………………………………………………………. 0
6. Do you smoke if you are so ill that you are in bed most of the day?
a. Yes ………………………………………………………………………………………1 b. No ……………………………………………………………………………………….0
Your Score __________ Score 0-5 = low to moderate nicotine dependence 6-10 = high nicotine dependence
Dr L Mason 12 March 2017 45 8th MADPHS Conference 2017
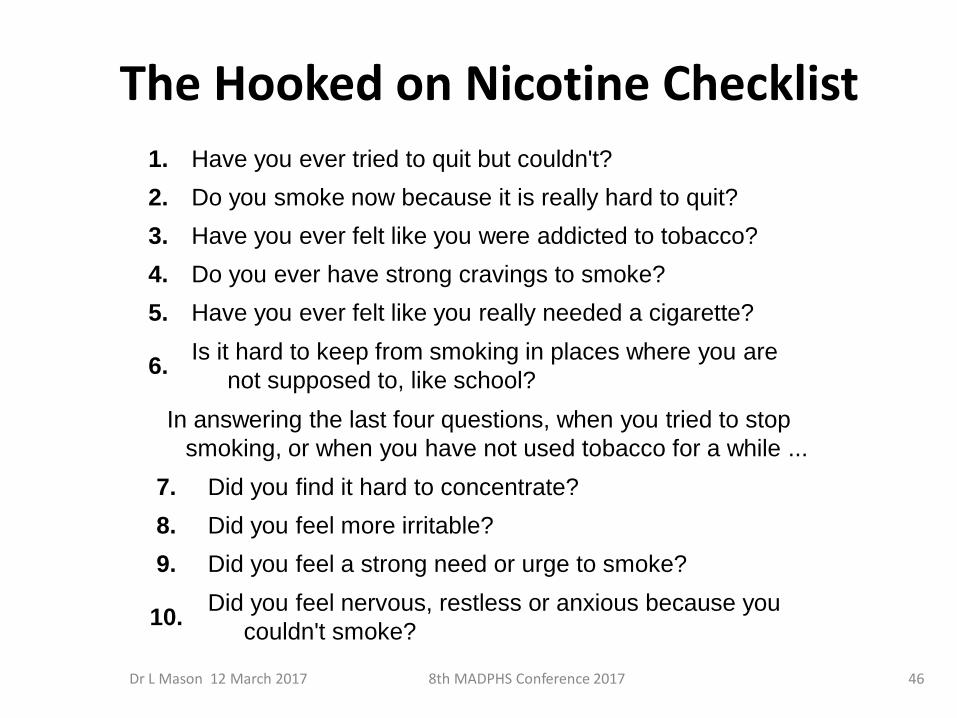
The Hooked on Nicotine Checklist
1. Have you ever tried to quit but couldn't?
2. Do you smoke now because it is really hard to quit?
3. Have you ever felt like you were addicted to tobacco?
4. Do you ever have strong cravings to smoke?
5. Have you ever felt like you really needed a cigarette?
6. Is it hard to keep from smoking in places where you are
not supposed to, like school?
In answering the last four questions, when you tried to stop
smoking, or when you have not used tobacco for a while ...
7. Did you find it hard to concentrate?
8. Did you feel more irritable?
9. Did you feel a strong need or urge to smoke?
10. Did you feel nervous, restless or anxious because you
couldn't smoke?
Dr L Mason 12 March 2017 46 8th MADPHS Conference 2017
The Horn’s test
1.Find out why they smoke
2. List the reasons in order of priority
3. Discuss strategies to deal with the problems
Dr L Mason 12 March 2017 47 8th MADPHS Conference 2017
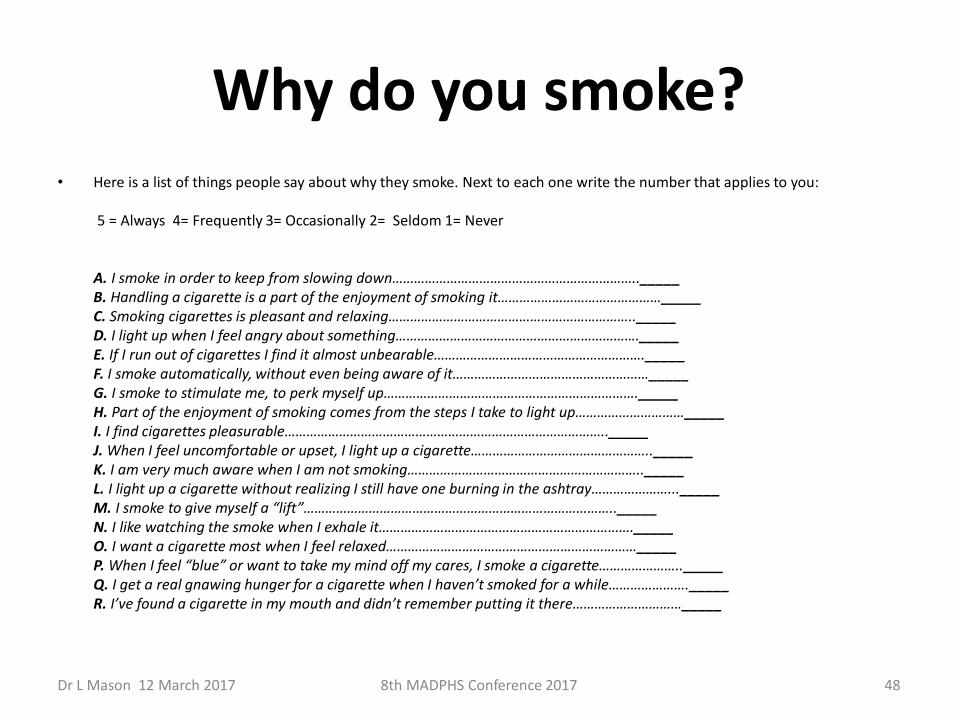
Why do you smoke? • Here is a list of things people say about why they smoke. Next to each one write the number that applies to you:
5 = Always 4= Frequently 3= Occasionally 2= Seldom 1= Never A. I smoke in order to keep from slowing down………………………………………………………….._____ B. Handling a cigarette is a part of the enjoyment of smoking it………………………………………_____ C. Smoking cigarettes is pleasant and relaxing………………………………………………………….._____ D. I light up when I feel angry about something…………………………………………………………._____ E. If I run out of cigarettes I find it almost unbearable…………………………………………………._____ F. I smoke automatically, without even being aware of it………………………………………………_____ G. I smoke to stimulate me, to perk myself up……………………………………………………………._____ H. Part of the enjoyment of smoking comes from the steps I take to light up…………………………_____ I. I find cigarettes pleasurable…………………………………………………………………………….._____ J. When I feel uncomfortable or upset, I light up a cigarette………………………………………….._____ K. I am very much aware when I am not smoking……………………………………………………….._____ L. I light up a cigarette without realizing I still have one burning in the ashtray…………………..._____ M. I smoke to give myself a “lift”………………………………………………………………………….._____ N. I like watching the smoke when I exhale it……………………………………………………………._____ O. I want a cigarette most when I feel relaxed……………………………………………………………_____ P. When I feel “blue” or want to take my mind off my cares, I smoke a cigarette………………….._____ Q. I get a real gnawing hunger for a cigarette when I haven’t smoked for a while…………………._____ R. I’ve found a cigarette in my mouth and didn’t remember putting it there…………………………_____
Dr L Mason 12 March 2017 48 8th MADPHS Conference 2017
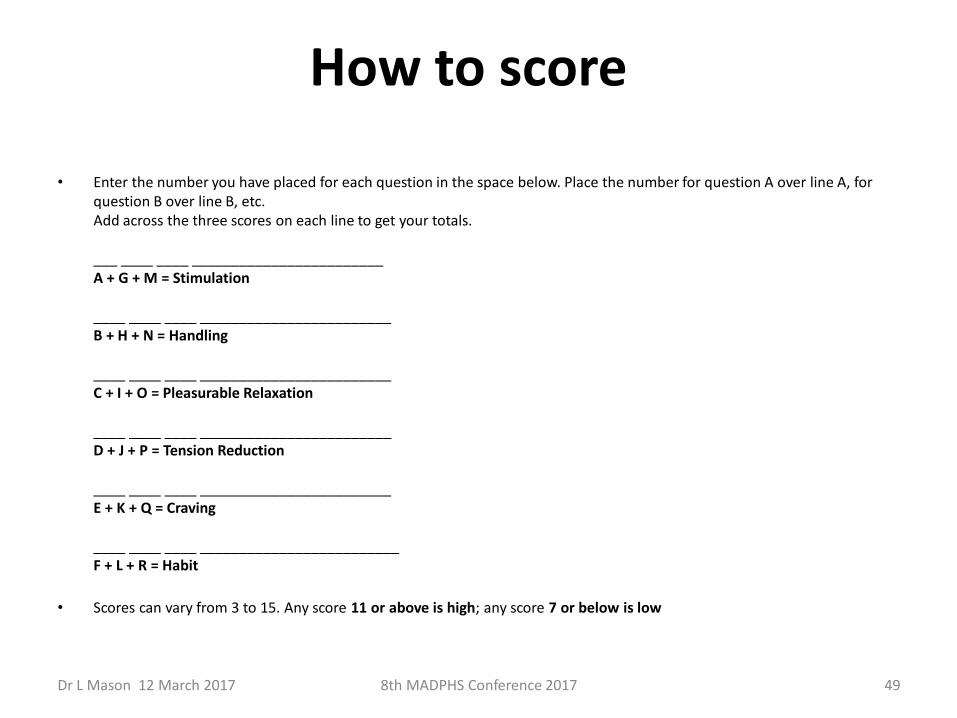
How to score
• Enter the number you have placed for each question in the space below. Place the number for question A over line A, for question B over line B, etc. Add across the three scores on each line to get your totals. ___ ____ ____ ________________________ A + G + M = Stimulation ____ ____ ____ ________________________ B + H + N = Handling ____ ____ ____ ________________________ C + I + O = Pleasurable Relaxation ____ ____ ____ ________________________ D + J + P = Tension Reduction ____ ____ ____ ________________________ E + K + Q = Craving ____ ____ ____ _________________________ F + L + R = Habit
• Scores can vary from 3 to 15. Any score 11 or above is high; any score 7 or below is low
Dr L Mason 12 March 2017 49 8th MADPHS Conference 2017
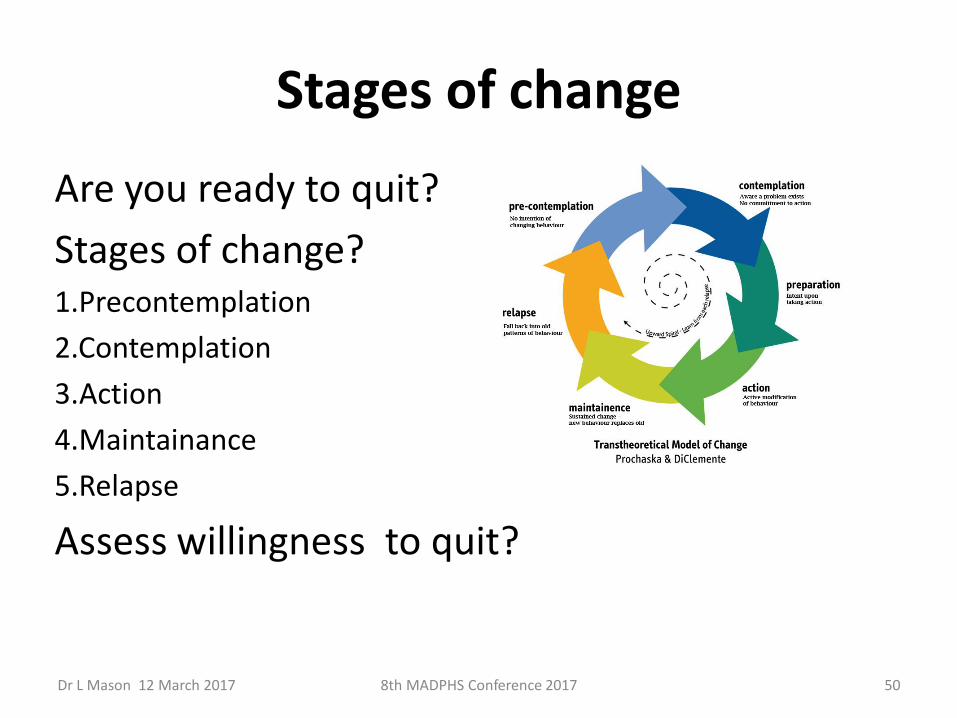
Stages of change
Are you ready to quit?
Stages of change? 1.Precontemplation
2.Contemplation
3.Action
4.Maintainance
5.Relapse
Assess willingness to quit?
Dr L Mason 12 March 2017 50 8th MADPHS Conference 2017
Dealing with ambivalence
Dr L Mason 12 March 2017 51 8th MADPHS Conference 2017
Decision-Making Worksheet The pros and cons of quitting
Pros
1.Good things about smoking
2.Good things about quitting
3.Reasons for making a change
Cons
1.Not so good things about smoking
2.Not so good thing about quitting
3.Reason for staying the same
Dr L Mason 12 March 2017 52 8th MADPHS Conference 2017
Reasons for wanting to quit What are some reasons for you to quit using
tobacco? ___ Health ___ Family health ___ Cost ___ It’s a bad habit ___ Good role model ___ Social pressure ___ I don’t like being addicted ___ My family wants me to quit ___ Doctor’s advice ___ I have no reason to quit ___ Other ___________________________________________
Dr L Mason 12 March 2017 53 8th MADPHS Conference 2017
Barriers and roadblocks
What do you think are your barriers to quitting tobacco use right now? ___ I don’t believe I can do it. ___ I enjoy tobacco use too much. ___ I have too many friends/ family who use tobacco. ___ I don’t believe using tobacco will hurt me. ___ I have too much stress in my life to quit now and I won’t be able to deal with it without using tobacco. ___ If I quit I will gain weight. ___ Using tobacco is the least of my problems right now. ___ Quitting might hurt my recovery from alcohol or other drugs. ___ I will miss or crave tobacco too much. ___ I will become too nervous or anxious or tense when I quit. ___ Other ______________________________________________
Dr L Mason 12 March 2017 54 8th MADPHS Conference 2017
Motivation and efficacy
Use the scale below to answer the following 4 questions. ______________________________________ 0 1 2 3 4 5 6 7 8 9 10 Not at all Extremely
a. How motivated are you to become tobacco-free at this time? ___ ___
b. How confident are you in your ability to become tobacco-free at this time? ___ ___
c. How effective do you believe your skills are for becoming tobacco-free? ___ ___
d. How much effort are you willing to put into becoming tobacco-free at this time? ___ ___
Dr L Mason 12 March 2017 55 8th MADPHS Conference 2017
Preparing them to quit
• Anticipate challenges
– Ask about cues to use tobacco
• Practice problem-solving
– enlisting help from friends or parents, quitting with a friend, getting parents to quit
• Prescribe or provide information about pharmacotherapy
– Pharmacotherapy can be used, but has not been shown effective with teens (Mixed results…)
• Help the teen set a quit date
• Document your advice
• PLAN pathway to quit
Dr L Mason 12 March 2017 56 8th MADPHS Conference 2017
Anticipate Tobacco Withdrawal
• Cigarette craving
• Anxiety
• Irritability
• Headache
• Insomnia
• Drowsiness
• Constipation
• Increased appetite
• Poor attention
• Impaired cognitive performance
• Decreased heart rate
Symptoms occur within hours of stopping smoking, and may persist for weeks
Dr L Mason 12 March 2017 57 8th MADPHS Conference 2017
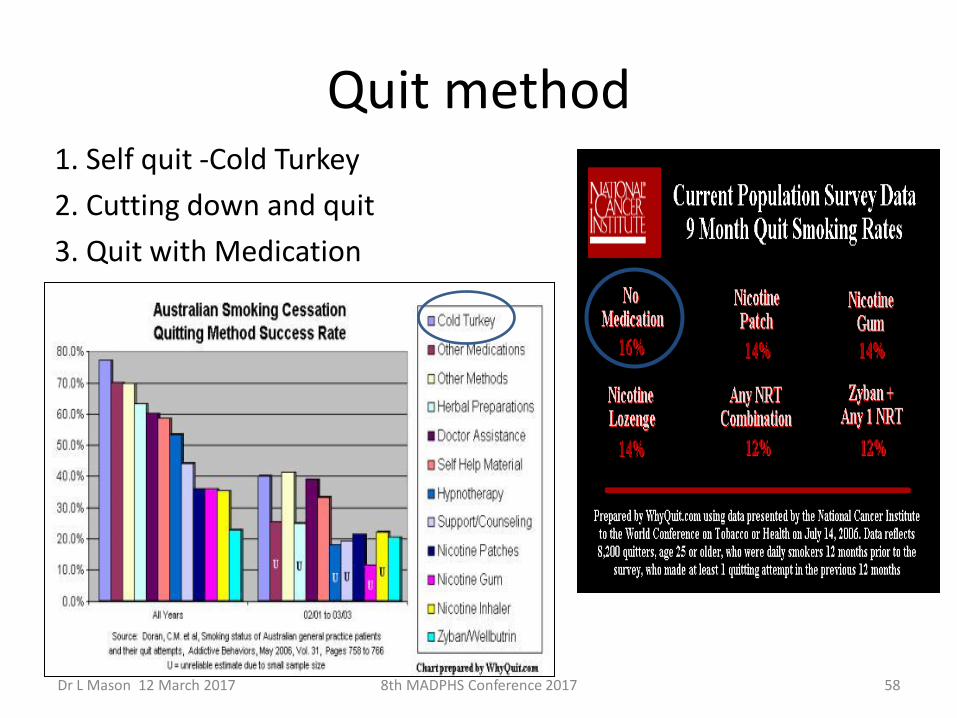
Quit method 1. Self quit -Cold Turkey
2. Cutting down and quit
3. Quit with Medication
58 8th MADPHS Conference 2017 Dr L Mason 12 March 2017
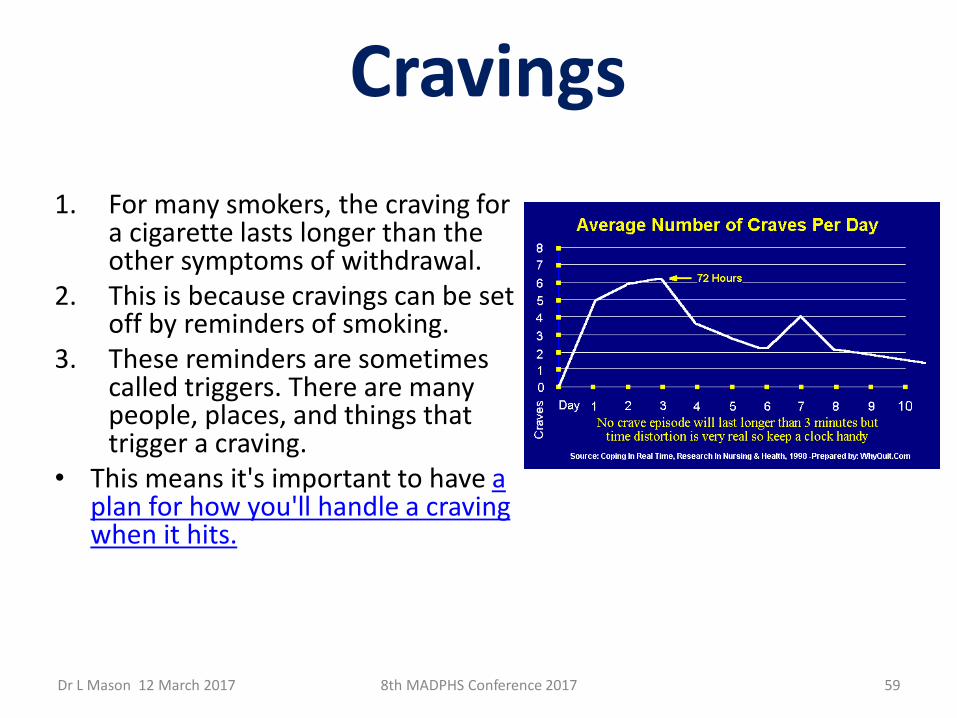
Cravings
1. For many smokers‚ the craving for
a cigarette lasts longer than the other symptoms of withdrawal.
2. This is because cravings can be set off by reminders of smoking.
3. These reminders are sometimes called triggers. There are many people, places, and things that trigger a craving.
• This means it's important to have a plan for how you'll handle a craving when it hits.
59 8th MADPHS Conference 2017 Dr L Mason 12 March 2017
Withdrawal
1. Although withdrawal can be uncomfortable and some people may feel high levels of symptoms‚ there is no health danger from nicotine withdrawal.
2. In fact‚ quitting smoking is the best thing you can do for your health.
3. Even extreme withdrawal symptoms will fade in a week or so.
If you feel very sad and depressed …See a doctor
60 8th MADPHS Conference 2017 Dr L Mason 12 March 2017
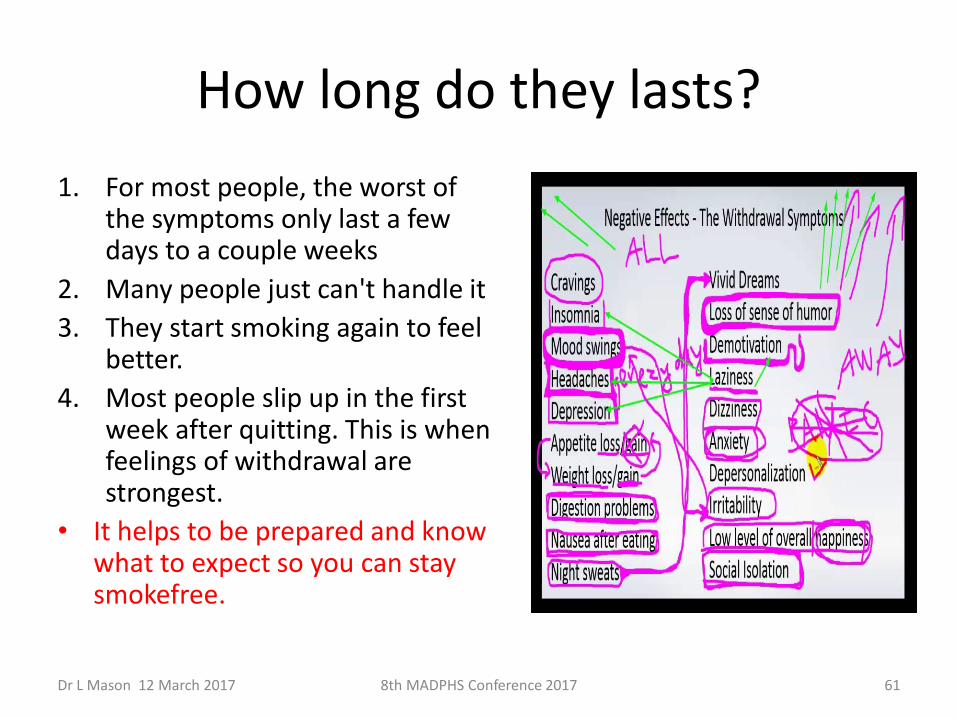
How long do they lasts?
1. For most people, the worst of the symptoms only last a few days to a couple weeks
2. Many people just can't handle it
3. They start smoking again to feel better.
4. Most people slip up in the first week after quitting. This is when feelings of withdrawal are strongest.
• It helps to be prepared and know what to expect so you can stay smokefree.
61 8th MADPHS Conference 2017 Dr L Mason 12 March 2017
Who should consider medication?
1. Those who have tried several times without success
2. Smokes one pack per day or more
3. Bothered by cravings and withdrawals for nicotine
62 8th MADPHS Conference 2017 Dr L Mason 12 March 2017
Learning from failures 1. Most people who have quit smoking
were unsuccessful at least once in the past.
2. Try not to view past attempts to quit as failures.
3. See them as learning experiences. Expect relapses when you try to quit. On the average one need to undergo 6-7 cycles before final success.
“Quit smoking for a healthier you. Every
cigarette you don’t smoke is doing you good.”
63 8th MADPHS Conference 2017 Dr L Mason 12 March 2017
Motivational Interviewing
• motivation to change by exploring and resolving ambivalence
Prof Wee will elaborate tomorrow
Dr L Mason 12 March 2017 64 8th MADPHS Conference 2017
Cognitive behavioural therapy (CBT)
• is a talking therapy that can help you manage your problems by changing the way you think and behave
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 65

Motivation and benefit
Dr L Mason 12 March 2017 66 8th MADPHS Conference 2017
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 67
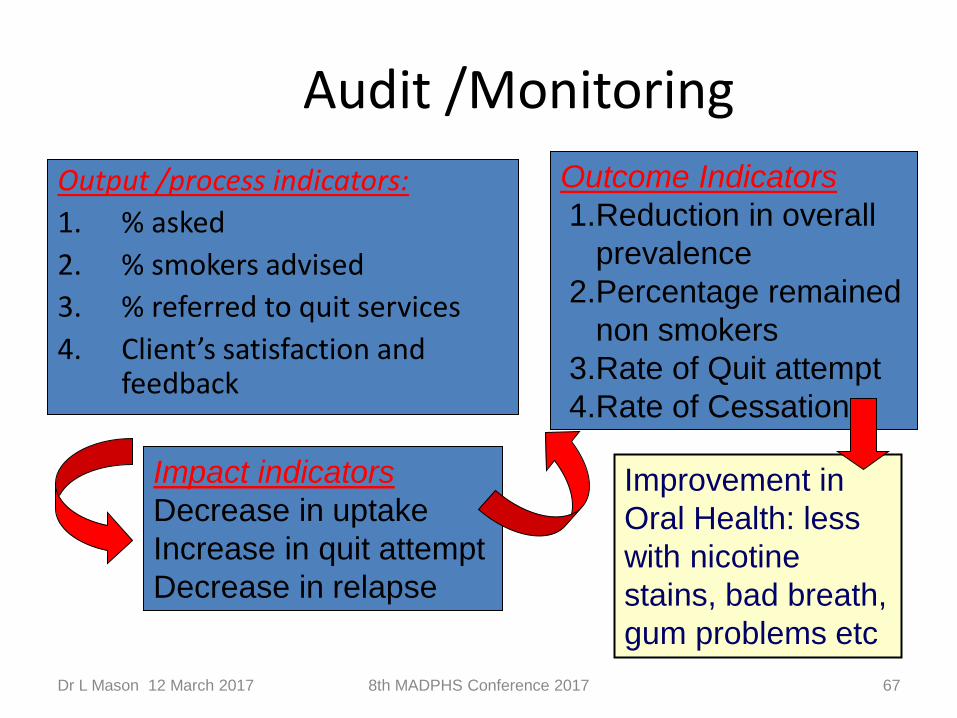
Audit /Monitoring
Output /process indicators:
1. % asked
2. % smokers advised
3. % referred to quit services
4. Client’s satisfaction and feedback
Outcome Indicators
1.Reduction in overall
prevalence
2.Percentage remained
non smokers
3.Rate of Quit attempt
4.Rate of Cessation
Impact indicators
Decrease in uptake
Increase in quit attempt
Decrease in relapse
Improvement in
Oral Health: less
with nicotine
stains, bad breath,
gum problems etc
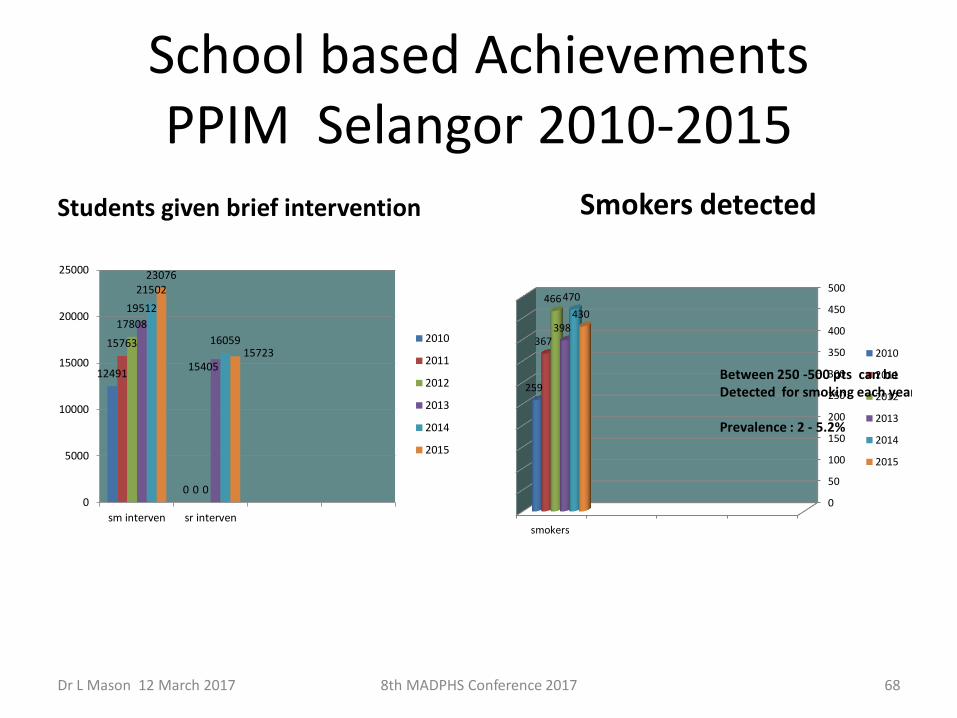
School based Achievements PPIM Selangor 2010-2015
Students given brief intervention Smokers detected
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 68
12491
0
15763
0
17808
0
19512
15405
21502
16059
23076
15723
0
5000
10000
15000
20000
25000
sm interven sr interven
2010
2011
2012
2013
2014
2015
0
50
100
150
200
250
300
350
400
450
500
smokers
259
367
466
398
470
430
2010
2011
2012
2013
2014
2015
Between 250 -500 pts can be Detected for smoking each year Prevalence : 2 - 5.2%
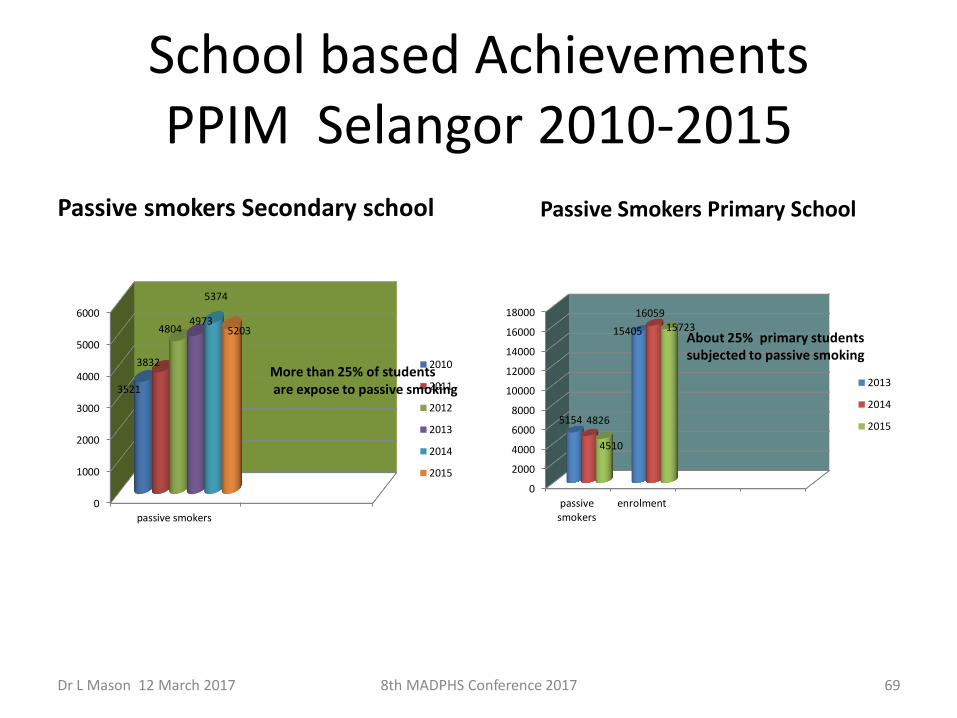
School based Achievements PPIM Selangor 2010-2015
Passive smokers Secondary school Passive Smokers Primary School
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 69
0
1000
2000
3000
4000
5000
6000
passive smokers
3521
3832
4804 4973
5374
5203
2010
2011
2012
2013
2014
2015
More than 25% of students are expose to passive smoking
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
passivesmokers
enrolment
5154
15405
4826
16059
4510
15723
2013
2014
2015
About 25% primary students subjected to passive smoking
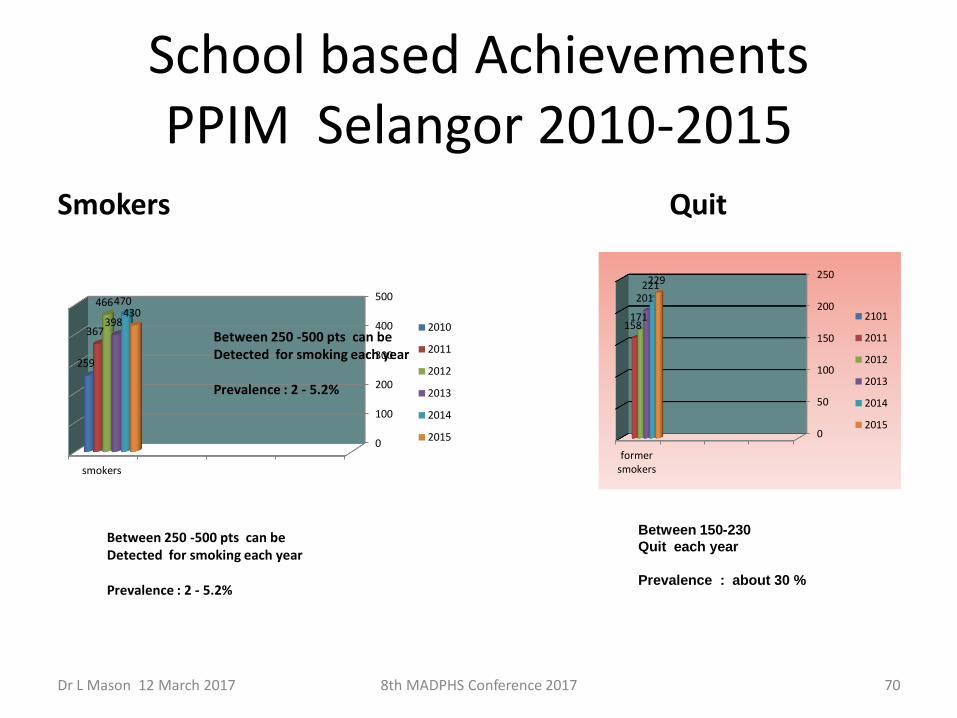
School based Achievements PPIM Selangor 2010-2015
Smokers Quit
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 70
0
50
100
150
200
250
formersmokers
158 171
201 221 229
2101
2011
2012
2013
2014
2015
0
100
200
300
400
500
smokers
259
367
466
398
470 430
2010
2011
2012
2013
2014
2015
Between 250 -500 pts can be Detected for smoking each year Prevalence : 2 - 5.2%
Between 150-230
Quit each year
Prevalence : about 30 %
Between 250 -500 pts can be Detected for smoking each year Prevalence : 2 - 5.2%
YEAR 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 2023 2024 2025
Mil
lio
n
* TOTAL POPULATION (Age ≥ 15)
20.8 21.6 22.0 22.4 22.8 23.2 23.5 23.9 24.3 24.7 25.0 25.3 25.7 26.0 26.3
NO. OF SMOKERS 4.70 4.86 4.83 4.78 4.74 4.69 4.61 4.55 4.49 4.42 4.33 4.23 4.15 4.05 3.94
NO. OF QUITTERS
0.13 0.13 0.13 0.13 0.13 0.14 0.14 0.14 0.14 0.15 0.15 0.15 0.15 0.15
PREVALENCE (%) 23.1 22.5 21.9 21.4 20.8 20.2 19.6 19.0 18.5 17.9 17.3 16.7 16.1 15.6 15.0
MALAYSIA’S TOBACCO CONTROL ROAD MAP FOR 2014 – 2025 Target : To reduce smoking prevalence to 15% by 2025
23.1 22.52 21.94 21.36 20.78 20.2 19.62 19.04 18.46 17.88 17.3 16.72 16.14 15.56 14.98
0
5
10
15
20
25
0.00
1.00
2.00
3.00
4.00
5.00
2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 2023 2024 2025
Population (Million)
NO. OF SMOKERS (Million) NO. OF QUITTERS…
Prevalence
Dr L Mason 12 March 2017 71 8th MADPHS Conference 2017
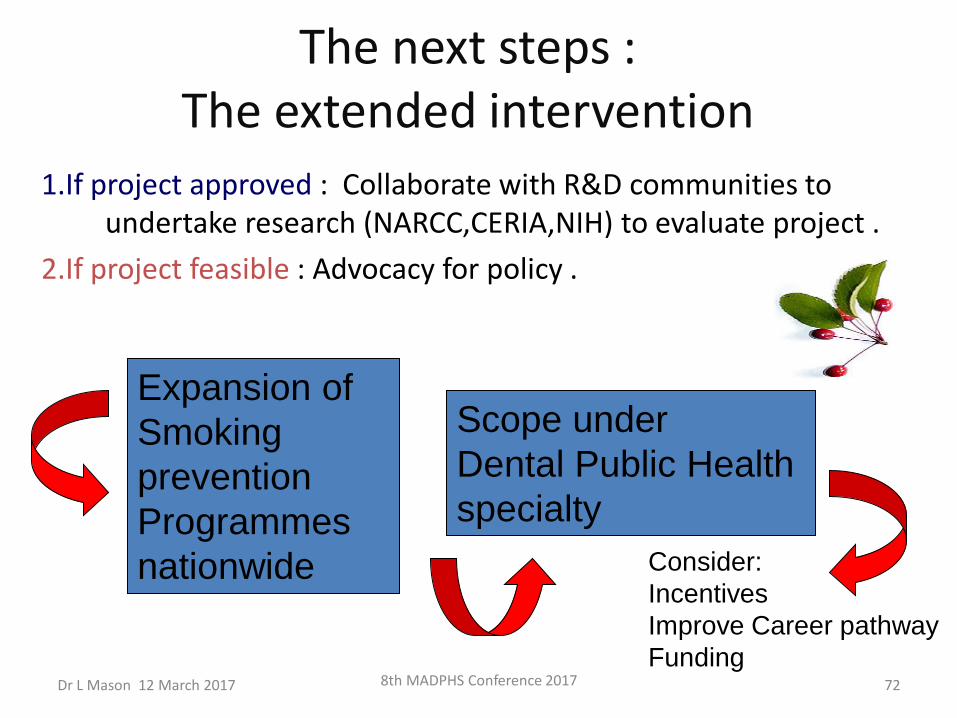
The next steps : The extended intervention
8th MADPHS Conference 2017 72
1.If project approved : Collaborate with R&D communities to undertake research (NARCC,CERIA,NIH) to evaluate project .
2.If project feasible : Advocacy for policy .
Expansion of
Smoking
prevention
Programmes
nationwide
Scope under
Dental Public Health
specialty
Consider:
Incentives
Improve Career pathway
Funding Dr L Mason 12 March 2017
Future Direction
• Can we propose M’sian school base Tobacco endgame to FCTC ?
• 176 WHO member country can benefit from this
• Imply room for global expansion
• We could be consultant for APW Tobacco Endgame for WHO if this happens
(APW =acceptance performance for work)
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 73
DPHS Role and Contributions ??
Dr L Mason 12 March 2017 74 8th MADPHS Conference 2017
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 75
DPHS contributions in Tobacco control 1.To the MOH organization
Establishment of health surveillance systems ( Routine cohort data) Improve utilization of quit clinic
Consolidations of health services vs smoking 2.To the country
Improve health of population , QoL Reduce costs treating smoking related disease 3.To the school children and adolescents
Improve access to care and prevention 4.To the Dental Services Added value to SDS and dental professionals
5. To the world if globally implemented*
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 76
Issues and Challenges
1. Lack of confidence
2. Time constraints
3. Patient resistant
4. Confidentiality
5. Supportive environment
6. Leaderships**, organizations
7. Limitations :Validation of self –report
8. Budget for sustainability
Urine cotinine
Serum cotinine
Salivary cotinine
Breath analyzer
Dip stick
Another individual
Nothing that cannot be resolved ***

Conclusion
• Governments and legislators have a role to play for smoke free Malaysia, but they are not the only ones.
• Society at large needs to be involved in the struggle against tobacco.
Dr L Mason 12 March 2017 77 8th MADPHS Conference 2017
FOR SURE …..
Within society, one group of professionals has
a special role to play because they practice their
profession in a particular sector –
The Dental Public Health Specialist
Dr L Mason 12 March 2017 78 8th MADPHS Conference 2017
Dr L Mason 12 March 2017 8th MADPHS Conference 2017 79
Thank you
You and I , Together we can make a difference