role of echocardiography in guiding the optimal timing of surgery in infective endocarditis
TRANSCRIPT

CARDIOVASCULAR INFECTIONS (D LEVINE, SECTION EDITOR)
Role of Echocardiography in Guiding the Optimal Timingof Surgery in Infective Endocarditis
Sagar Mallikethi Reddy & Sidakpal Panaich &
Luis Afonso
Published online: 19 June 2013# Springer Science+Business Media New York 2013
Abstract Infective endocarditis (IE) is a complex cardiovascu-lar infection with the potential for multiorgan complications.While early surgery can be life saving in IE patients with acuteheart failure and acute valve regurgitation, the appropriate timingof surgery for embolic complications is less certain. The ongoingdebate concerns the ideal timing of surgical therapy and stemsprimarily from a scarcity of therapeutic randomized controlledtrials in this population. Based largely on the evidence fromobservational studies and expert consensus, the European Soci-ety of Cardiology has issued guidelines on the optimal surgicaltiming in IE. Nonetheless, selection bias in published studies andthe clinical complexity of this disease entity continue to posemanagement challenges in the individual patient. In this review,we focus on the cardinal role of echocardiography as a diagnos-tic tool in patients with complicated IE and discuss the availableevidence pertaining to the ideal timing of surgical intervention.
Keywords Infective endocarditis . Echocardiography .
Timing of surgery in infective endocarditis
Introduction
Infective endocarditis (IE) ranks amongst the most life-threatening infectious diseases with an estimated incidenceof 3 to 10 cases per 100,000 person years [1•, 2] and an in-hospital mortality approaching 20 to 25 % [1•, 3]. Approxi-mately half of the patients with IE end up requiring a surgicalintervention [2] in addition to medical therapy to mitigatepotentially lethal complications ensuing from severe valve
dysfunction, uncontrolled sepsis, invasive/destructive disease,congestive heart failure (HF) and embolic stroke [3, 4•].
While guidelines addressing indications for surgery in IE arefairly well codified [2, 5], recommendations on the optimaltiming of surgical intervention are less well defined and remainsomewhat controversial, based on either expert opinion or sup-porting evidence from nonrandomized studies [1•, 2]. A host ofreasons likely account for the scarcity of randomized controlledtrials evaluating management strategies in these patients includ-ing ethical [4•, 6] and logistical considerations [7], financialissues [8] and sample size limitations coupled with the diversityof patients with IE [4•]. Other limitations plaguing observationalstudies in this area relate to treatment and survivor biases. In thiscontext, propensity score matched analyses have gained popu-larity as they attempt to minimize bias and account for con-founders associated with nonrandomized observational data.Nonetheless, recommendations emanating from such studieson timing of surgery are conflicting [1•, 8, 9•, 10].
Echocardiography continues to play a central role in guidingtreatment strategies (medical versus surgical) and in decidingthe appropriate timing of surgery for patients with IE [11••]. Inthis article, we review the role of echocardiography in guidingthe optimal timing of surgical intervention in patients with IE.
The Case for Early Surgery
Broadly speaking, consensus exists for recommending emer-gent surgery in patients with native or prosthetic valve endo-carditis (PVE) complicated by pulmonary edema or cardiogen-ic shock. Likewise, urgent intervention is deemed appropriatein those with persistent or decompensated HF, while electivesurgery is reserved for patients with severe regurgitation not inHF. In terms of mitigating the risk of embolic stroke, resultsfrom a recent, randomized trial in patients with severe aortic ormitral IE suggest that early surgical intervention (within 48 h ofrandomization) reduces the composite endpoint of death andembolic events compared to conventional treatment (delayed
S. Panaich : L. Afonso (*)Division of Cardiology, Detroit Medical Center,Wayne State University, Detroit, MI 48201, USAe-mail: [email protected]
S. M. Reddy : S. Panaich : L. AfonsoDepartment of Internal Medicine, Detroit Medical Center,Wayne State University, Detroit, MI, USA
Curr Infect Dis Rep (2013) 15:335–341DOI 10.1007/s11908-013-0345-1

surgery during hospitalization or during follow-up) by effectivelyreducing the incidence of systemic embolism [12•]. However, thetrial was limited in that it excluded sicker patients with IE such asthose with HF, major stroke, PVE and invasive complications.The European Society of Cardiology guidelines [2] provide thebasis for recommendations outlined in this article. For quickreference, an itemized, tabulated summary of the indicationsand optimal timing for surgical intervention is provided.
Heart Failure
HF is the leading cause of mortality in IE, followed by stroke[9•]. Acute HF typically results from acute valvular (mitral oraortic) regurgitation, cardiac fistula formation, or from a largevegetation causing valvular obstruction [2, 4•]. Acute HF com-plicated by refractory pulmonary edema or cardiogenic shock [2]warrants emergent surgery (within 24 h of diagnosis). Echocar-diography helps identify the underlying mechanism responsiblefor acute mitral regurgitation (MR) or aortic regurgitation (AR)such as flail or ruptured leaflet, leaflet perforation, malcoaptationfrom an interfering vegetation, or ruptured chordae tendineae (inMR), all of which could precipitate HF in the setting of IE [2].Severe acute valvular regurgitation or obstruction with persistentHF or echocardiographic features signifying poor hemodynamictolerance calls for urgent surgery (within a few days of diagno-sis) even in the absence of clinical HF [2, 11••].
In acute severeAR, rapidly increasing left ventricular diastolicpressure typically exceeding left atrial pressure leads to prema-ture closure of themitral valve, a phenomenon best demonstratedon 2D orM-mode echocardiography [13]. In acute severeMR, arapidly decelerating MR signal on continuous wave Dopplerechocardiography (V-wave cut-off sign) [5], moderate to severepulmonary hypertension and elevated left atrial pressures reflectpoor hemodynamic tolerance [2, 5], potentially influencing thedecision to proceed with surgical intervention. Ruptured chordaetendineae, flail leaflets and mitral perforations leading to acuteMR and HF can be identified preoperatively with a great degreeof precision using real time three-dimensional transesophagealechocardiography (RT3DTEE) [14].
Large vegetations can lead to significant valvular obstructionin patients with native or prosthetic endocarditis, manifesting aselevated transvalvular gradients. This entity is easily recognizedand quantified using 2D and continuous wave Doppler echo-cardiography. Finally, patients with severe valvular regurgita-tion without any signs of HFmay undergo elective surgery afterat least 1–2 weeks of antibiotic therapy [2].
Invasive Endocarditis
Invasive endocarditis refers to locally advanced persistent in-fection inside the heart. The spectrum of invasive endocarditis
is wide and ranges from periannular extension, intervalvularfibrosa abscesses, fistulous intracardiac communications tovalve aneurysms and perforations.
& Periannular ExtensionPerivalvular or periannular extension of infection carries
a poor prognosis [15, 16] and is predictive of both incidentHF and death [17]. Besides persistent fever and positiveblood cultures (>7–10 days, despite appropriate antibiotictherapy unrelated to an extracardiac focus), a high index ofsuspicion is imperative for the timely diagnosis of thisdreaded complication. Echocardiographic identification oflocally invasive infection mandates urgent surgical inter-vention typically within a few days of diagnosis [2, 9•,11••]. TEE has a higher sensitivity (76–100 %), specificity(95 %), and positive (87 %) and negative predictive values(89 %) than transthoracic echocardiography (TTE) for thedetection of periannular extension [17].
Periannular extension in aortic IE leading to local inva-sion and destruction around the membranous interventric-ular septum and atrioventricular node may culminate invarying degrees of atrioventricular block frequently requir-ing temporary or permanent pacing support [4•, 17]. Echo-cardiographically determined aortic root thickening is theearliest sign of a developing perivalvular abscess [2, 11••],but with disease progression, focal areas of breakdownmay be visualized either as a solitary or multiple septatehypoechoic areas, interspersed amidst a heterogeneousroot echo texture. Eventually one ormore unroofed abscesscavities may be observed communicating freely with theaortic lumen on color flow Doppler echocardiography.
A conservative approach is typically employed inpatients with a small (<1 cm) uncomplicated abscess;however, serial TEE scans at 2, 4 and 8 weeks aftercompletion of antibiotic therapy [17] to monitor progres-sion are warranted. The sensitivities of TTE and TEE forthe detection of abscesses are 50 % and 90 %, respectively[11••]. However, the specificity is as high as 90 % for bothmodalities [11••]. Here again, RT3DTEE when combinedwith two-dimensional TEE allows improved detection ofthe number, site and size of abscesses [14].
& Intervalvular Fibrosa Complications and FistulousCommunications
The intervalvular fibrosa represents bridging fibroustissue connecting the aortic and mitral valves [18]. IEinvolving the aortic valve if unchecked may progress toinvolve the intervalvular fibrosa forming an abscess thatcould subsequently expand to form a pseudoaneurysm [16].
Pseudoaneurysms involving the aorta on the other handrepresent a contained rupture of this structure, confined bythe adventitia (echocardiographically described as a pulsa-tile, perivalvular echo-free space within which color
336 Curr Infect Dis Rep (2013) 15:335–341

Doppler flow is detected [2]); these focal, saccular out-pouchings typically contain thrombus and are best visual-ized with contrast-enhanced echocardiography. Avariety ofcomplications have been associated with aortic pseudoa-neurysms and these include fistulization between the aortaor left atrium, rupture into the pericardial space leading totamponade, coronary artery compression causing myocar-dial ischemia, pulmonary artery compression, as well asmitral valve compression leading to MR, and eventuallyHF [18]. For pseudoaneurysms, TTE has a detection rate of54 % and that of TEE a detection rate approaching 100 %[18].
Fistulous connections without a pseudoaneurysm canalso develop between the aorta and a cardiac chamber(aortocavitary fistula) or the pericardium causing intracar-diac or pericardial shunts. TTE and TEE detect about 53 %and 97 % of surgically proven fistulous connections, re-spectively [15]. The timing of the surgery in IE complicatedby fistula or pseudoaneurysm may be emergent or electiveand is contingent on the presence or absence of HF, pul-monary edema or shock (Table 1).
& Valve Aneurysms and PerforationsAvalvular aneurysm is defined as a saccular outpouching
or bulging of valvular tissue [11••]. Mitral valve aneurysmsoccur as a result of secondary infection of the ventricularsurface of the valve from the infected aortic regurgitant jet inpatients with aortic IE [11••, 16].Weakening of the surface ofthe aneurysmal wall eventually yields to high chamber pres-sure and thewallmay rupture forming a perforation.Valvularperforations appear echocardiographically as a disruption ofleaflet continuity (distinct from the commissures) with tra-versing color Doppler flow [11••]. Mitral valve aneurysmsleading to mitral perforations are much more common thanaortic perforations from aortic aneurysms [19]. Our limitedexperience in IE patients with valvular perforations showedthat it carries a worse prognosis with a very high in-hospitalmortality, suggesting the need for early surgical intervention[19]. The literature on the timing of surgery in this high-riskpopulation is sparse. TTE and TEE are key to the evaluationof local complications of IE such as valve aneurysms andperforations [11••]. RT3DTEE complements the utility of 2DTEE for the precise detection and localization of such com-plications [14].
Prevention of Systemic Embolism
Systemic embolism, especially cerebral embolism secondaryto dislodgement of cardiac vegetations [2, 11••, 17, 20], is acommon and life-threatening complication affecting up to 20–50 % of patients with IE. The risk increases with size andmobility of vegetations [20–24]. A vegetation size of >10 mm
requires urgent surgery if associated with HF, abscess or per-sistently positive blood cultures, or when further complicatedby one or more embolic episodes despite appropriate antibiotictherapy [2, 4•]. Additionally, mitral valve (particularly anteriorleaflet) IE carries a higher risk of embolization. The risk ofembolism is particularly high early in the course of antibiotictherapy with a dramatic reduction in incidence after 2 weeks[4•]. Enlarging vegetation(s) on follow-up TEE, performedwithin 4–8 weeks of appropriate antibiotic therapy is indicativeof locally uncontrolled infection [17], and deemed an urgentindication for surgery [2]. Negative bacterial cultures and thepresence of large bulky vegetation on TTE or TEE is highlysuggestive of fungal endocarditis [25], an entity for whichelective or urgent surgery is indicated.
While the overall sensitivity of TTE and TEE for detectingvegetations is around 75 % and 85–90 %, respectively, speci-ficity exceeds 90 % for both imaging modalities [11••].RT3DTEE enables accurate determination of the number andsite, and better sizing, of the vegetation [14], providing data thatcould help steer the timing of surgery.
Neurological complications involving cerebral embolismand/or infarction occur in a significant proportion of IE patientswith a high mortality rate [9•]. Although conflicting literatureexists regarding appropriate management of such patients,guidelines recommend urgent surgical intervention if any oneof the indications detailed in Table 1 are met [4•]. Surgery insuch instances should not be delayed given the low rate ofpostsurgical deterioration in postembolic infarct patients, unlessthere is evidence of intracranial hemorrhage, poor neurologicalprognosis and/or severe neurological damage after stroke [4•].
Prosthetic Valve Endocarditis
PVE accounts for 7–25 % of cases of IE and has a mortalityrate of 20–25 % [3]. IE appears to have a predilection forprosthetic aortic valves compared to valves in other loca-tions [4•]. Prosthetic dysfunction occurs as a result of de-hiscence or obstruction, both of which may lead to HF [2,11••]. Mechanical prosthesis infection may lead to perivalv-ular abscess, pseudoaneurysms, dehiscence and fistuliza-tion, whereas bioprosthetic infections manifest as vegeta-tions, leaflet rupture, stenosis or perforation [11••].
Prosthetic valve dehiscence (new paravalvular regurgita-tion on echocardiogram [11••]), obstruction from vegetationor fistula formation all require emergent surgery if associatedwith refractory pulmonary edema or cardiogenic shock. How-ever, elective surgery is recommended if dehiscence is notassociated with clinical and echocardiographic signs of HF[2]. Similar to native valve endocarditis (NVE), vegetationsize, number of embolic episodes and echocardiographic signsof locally uncontrolled infection determine the timing ofsurgery.
Curr Infect Dis Rep (2013) 15:335–341 337
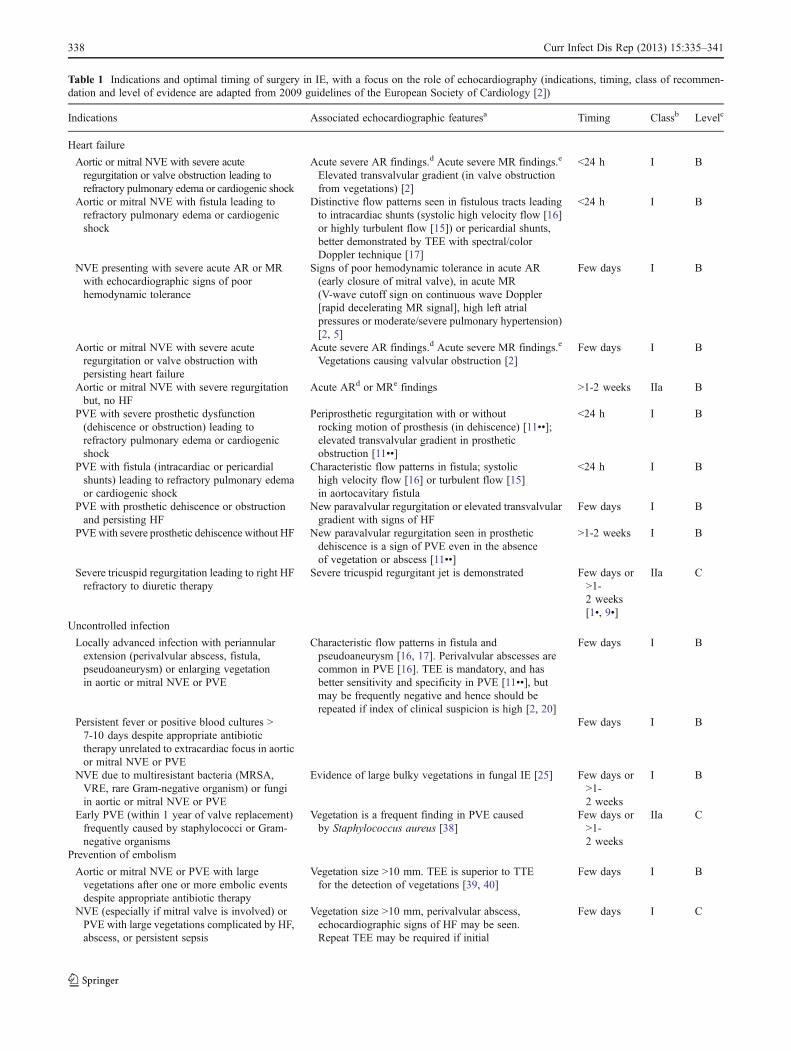
Table 1 Indications and optimal timing of surgery in IE, with a focus on the role of echocardiography (indications, timing, class of recommen-dation and level of evidence are adapted from 2009 guidelines of the European Society of Cardiology [2])
Indications Associated echocardiographic featuresa Timing Classb Levelc
Heart failure
Aortic or mitral NVE with severe acuteregurgitation or valve obstruction leading torefractory pulmonary edema or cardiogenic shock
Acute severe AR findings.d Acute severe MR findings.e
Elevated transvalvular gradient (in valve obstructionfrom vegetations) [2]
<24 h I B
Aortic or mitral NVE with fistula leading torefractory pulmonary edema or cardiogenicshock
Distinctive flow patterns seen in fistulous tracts leadingto intracardiac shunts (systolic high velocity flow [16]or highly turbulent flow [15]) or pericardial shunts,better demonstrated by TEE with spectral/colorDoppler technique [17]
<24 h I B
NVE presenting with severe acute AR or MRwith echocardiographic signs of poorhemodynamic tolerance
Signs of poor hemodynamic tolerance in acute AR(early closure of mitral valve), in acute MR(V-wave cutoff sign on continuous wave Doppler[rapid decelerating MR signal], high left atrialpressures or moderate/severe pulmonary hypertension)[2, 5]
Few days I B
Aortic or mitral NVE with severe acuteregurgitation or valve obstruction withpersisting heart failure
Acute severe AR findings.d Acute severe MR findings.e
Vegetations causing valvular obstruction [2]Few days I B
Aortic or mitral NVE with severe regurgitationbut, no HF
Acute ARd or MRe findings >1-2 weeks IIa B
PVE with severe prosthetic dysfunction(dehiscence or obstruction) leading torefractory pulmonary edema or cardiogenicshock
Periprosthetic regurgitation with or withoutrocking motion of prosthesis (in dehiscence) [11••];elevated transvalvular gradient in prostheticobstruction [11••]
<24 h I B
PVE with fistula (intracardiac or pericardialshunts) leading to refractory pulmonary edemaor cardiogenic shock
Characteristic flow patterns in fistula; systolichigh velocity flow [16] or turbulent flow [15]in aortocavitary fistula
<24 h I B
PVE with prosthetic dehiscence or obstructionand persisting HF
New paravalvular regurgitation or elevated transvalvulargradient with signs of HF
Few days I B
PVEwith severe prosthetic dehiscence without HF New paravalvular regurgitation seen in prostheticdehiscence is a sign of PVE even in the absenceof vegetation or abscess [11••]
>1-2 weeks I B
Severe tricuspid regurgitation leading to right HFrefractory to diuretic therapy
Severe tricuspid regurgitant jet is demonstrated Few days or>1-2 weeks[1•, 9•]
IIa C
Uncontrolled infection
Locally advanced infection with periannularextension (perivalvular abscess, fistula,pseudoaneurysm) or enlarging vegetationin aortic or mitral NVE or PVE
Characteristic flow patterns in fistula andpseudoaneurysm [16, 17]. Perivalvular abscesses arecommon in PVE [16]. TEE is mandatory, and hasbetter sensitivity and specificity in PVE [11••], butmay be frequently negative and hence should berepeated if index of clinical suspicion is high [2, 20]
Few days I B
Persistent fever or positive blood cultures >7-10 days despite appropriate antibiotictherapy unrelated to extracardiac focus in aorticor mitral NVE or PVE
Few days I B
NVE due to multiresistant bacteria (MRSA,VRE, rare Gram-negative organism) or fungiin aortic or mitral NVE or PVE
Evidence of large bulky vegetations in fungal IE [25] Few days or>1-2 weeks
I B
Early PVE (within 1 year of valve replacement)frequently caused by staphylococci or Gram-negative organisms
Vegetation is a frequent finding in PVE causedby Staphylococcus aureus [38]
Few days or>1-2 weeks
IIa C
Prevention of embolism
Aortic or mitral NVE or PVE with largevegetations after one or more embolic eventsdespite appropriate antibiotic therapy
Vegetation size >10 mm. TEE is superior to TTEfor the detection of vegetations [39, 40]
Few days I B
NVE (especially if mitral valve is involved) orPVE with large vegetations complicated by HF,abscess, or persistent sepsis
Vegetation size >10 mm, perivalvular abscess,echocardiographic signs of HF may be seen.Repeat TEE may be required if initial
Few days I C
338 Curr Infect Dis Rep (2013) 15:335–341

TTE is limited in its ability to identify vegetations onprosthetic valves and not very sensitive for the detection ofinvasive disease, making TEE obligatory for optimal manage-ment in PVE [16]. Of note, the overall diagnostic utility ofeven TEE in PVE is low when compared to NVE [2], with asensitivity and specificity ranges 86–94 % and 88–100 %,respectively, for the identification of vegetations [26]. Al-though a combination of TTE and TEE improves diagnosticaccuracy (negative predictive value as high as 95 %), there isstill a risk of missing a small percentage of patients evenwith this approach [26]. Repeat TEE examinations arerecommended in patients with high clinical suspiciondespite a negative initial echocardiogram [11••, 20].
TEE enables more accurate quantification of the vegeta-tion size and early detection of periannular complications inPVE, such as abscess, fistula, or prosthetic dehiscence,thereby influencing the timing of surgery [27]. The sensi-tivity and specificity of TTE for the detection of perivalvularabscess is 28 % and 98 %, and of TEE is 87 % and 95 %,respectively [26]. Indeed, a combined TTE and TEE ap-proach should be pursued as acoustic shadowing significant-ly hampers the utility of isolated TTE or TEE, particularlywhen assessing prosthetic mitral valve function [26]. Ingeneral reverberations and acoustic shadowing are less ofan issue with bioprosthetic than with metallic mechanicalvalves and prostheses in the mitral position [26].
Because of its ability to circumvent many of the afore-mentioned limitations, RT3DTEE should be used preferen-tially to guide surgical decisions in mitral PVE [28, 29].RT3DTEE has been shown to provide better spatial
definition of the anatomic characteristics of prosthetic de-hiscence such as site, location, shape and number of de-hisced segments as well as leaflet mobility, all valuablepreprocedural information that helps guide the timing andtype of surgical intervention [29].
Right-sided Infective Endocarditis
Right-sided endocarditis (RSE) predominantly affects tricus-pid valves [11••, 30] and accounts for 5–10 % of total cases ofIE [2]. It carries a good prognosis [30] with a mortality ratebetween 5 % and 10 % [31, 32]. It is reasonable to performurgent or elective surgery if echocardiography demonstratespersistent tricuspid vegetations exceeding 20 mm in size [1•,2, 9•] following recurrent pulmonary emboli [31]. Urgent orelective surgery is also a reasonable approach to echocardio-graphically detected severe tricuspid regurgitation if this hasled to refractory right HF [1•, 2, 9•]. TTE has a high sensitivityof around 80 % [33] in RSE and usually suffices for thediagnosis. Large vegetation sizes, the relatively anterior posi-tion of tricuspid valve and favorable acoustic windows alsoaccount for the high sensitivity of TTE [16, 32]. However, thesensitivity for RSE decreases to 25 % in patients with im-plantable cardiac devices and TEE is mandatory in suchpatients [32]. TEE is also useful for diagnosing RSE involvingunusual locations such as the Chiari network or the Eustachianvalve [11••, 32]. Although controlled studies on the role of 3DTEE in RSE are lacking [32], the findings of initial studiesinvolving a small number of patients are promising [34].
Table 1 (continued)
Indications Associated echocardiographic featuresa Timing Classb Levelc
echocardiography is negative and suspicionfor IE is high [11••, 20]
Aortic or mitral NVE or PVE with very largevegetation if conservative surgery is feasible
Vegetation size >15 mm Few days IIb C
Persistent tricuspid valve vegetation (>20 mm)after recurrent pulmonary emboli withor without right HF
Vegetations (large, often >20 mm) are usuallylocated on the atrial side of the tricuspid valve[11••]. TTE is sufficient for the diagnosis especiallyin native valve RSE [32]
Few daysor >1-2 weeks[1•, 9•]
IIa C
AR aortic regurgitation, HF heart failure, IE infective endocarditis, LV left ventricle, MR mitral regurgitation, MRSA methicillin-resistantStaphylococcus aureus, NVE native valve endocarditis, PVE prosthetic valve endocarditis, RSE right sided endocarditis, TEE transesophagealechocardiography, TTE transthoracic echocardiography, VRE vancomycin-resistant enterococcia Echocardiographic features for each indication are based on the cited referencesb Class of recommendation: class I evidence and/or general agreement that a given treatment or procedure is beneficial, useful, effective; class IIaweight of evidence or opinion is in favor of usefulness or efficacy of given treatment or procedure, class IIb usefulness or efficacy of giventreatment or procedure is less well established by opinion or evidencec Level of evidence: level B data derived from single randomized clinical trial or large non-randomized studies, level C consensus of opinion ofexperts or small studies, retrospective studies, registriesd Acute severe AR findings: vena contracta >6 mm; pressure half-time <200 ms; holodiastolic flow reversal in abdominal aorta; early closure ofmitral valve; normal LV size and function [37]e Acute severe MR findings: vena contracta >7 mm; pulmonary vein flow reversal; disrupted mitral valve apparatus [37]
Curr Infect Dis Rep (2013) 15:335–341 339

Limitations of Echocardiography
Although, echocardiography is considered invaluable in themanagement of IE, it has its limitations. The sensitivity andspecificity of TTE and TEE are not 100 % [11••] and up to15 % of patients may have negative echocardiographic find-ings [20]. The presence of prosthetic valves and intracardiacdevices further reduces its sensitivity and specificity [11••,20]. Diagnostic accuracy is also influenced by operator expe-rience, transducer position, acoustic shadowing (from thepresence of valve calcifications and metallic prosthesis) andinstrumental settings [35]. The sensitivity of TEE for detectingabscesses is as low as 48 %, if located on a mitral valve in thepresence of calcification in the posterior mitral annulus [36].
Conclusion
Echocardiography plays a pivotal role in the management ofIE. In addition to clinical and laboratory data, the need forsurgery and the optimal timing of intervention are decisionsthat rely heavily on echocardiographic findings. A multidisci-plinary approach involving cardiology, surgery and infectiousdiseases specialties should be adopted to optimize outcomesin patients with complications of IE, pending the availabilityof more randomized controlled trial data in this arena.
Compliance with Ethics Guidelines
Conflict of Interest Sagar Mallikethi Reddy, Sidakpal Panaich, andLuis Afonso, declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent This articledoes not discuss any studies with human or animal subjects performedby any of the authors.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. • Thuny F, Grisoli D, Collart F, Habib G, Raoult D. Managementof infective endocarditis: challenges and perspectives. Lancet.2012;379(9819):965–75. This is an informative literature reviewon the current management of infective endocarditis.
2. Habib G, Hoen B, Tornos P, Thuny F, Prendergast B, Vilacosta I, etal. Guidelines on the prevention, diagnosis, and treatment of in-fective endocarditis (new version 2009): the Task Force on thePrevention, Diagnosis, and Treatment of Infective Endocarditis ofthe European Society of Cardiology (ESC). Endorsed by theEuropean Society of Clinical Microbiology and Infectious Diseases(ESCMID) and the International Society of Chemotherapy (ISC) forInfection and Cancer. Eur Heart J. 2009;30(19):2369–413.
3. Mylonakis E, Calderwood SB. Infective endocarditis in adults. NEngl J Med. 2001;345(18):1318–30.
4. • Prendergast BD, Tornos P. Surgery for infective endocarditis: whoand when? Circulation. 2010;121(9):1141–52. This article reviewsindications and timing of surgery in infective endocarditis based onvarious studies that examined surgical outcomes in endocarditis..
5. Bonow RO, Carabello BA, Chatterjee K, De Leon Jr AC, FaxonDP, Freed MD, et al. 2008 Focused update incorporated into theACC/AHA 2006 guidelines for the management of patients withvalvular heart disease: a report of the American College of Cardi-ology/American Heart Association Task Force on Practice Guide-lines (Writing Committee to Revise the 1998 Guidelines for theManagement of Patients With Valvular Heart Disease): endorsedby the Society of Cardiovascular Anesthesiologists, Society forCardiovascular Angiography and Interventions, and Society ofThoracic Surgeons. Circulation. 2008;118(15):e523–661.
6. Kiefer T, Park L, Tribouilloy C, Cortes C, Casillo R, Chu V, et al.Association between valvular surgery and mortality amongpatients with infective endocarditis complicated by heart failure.JAMA. 2011;306(20):2239–47.
7. Lalani T, Cabell CH, Benjamin DK, Lasca O, Naber C, Fowler JrVG, et al. Analysis of the impact of early surgery on in-hospitalmortality of native valve endocarditis: use of propensity score andinstrumental variable methods to adjust for treatment-selectionbias. Circulation. 2010;121(8):1005–13.
8. D'Agostino Jr RB. Propensity scores in cardiovascular research.Circulation. 2007;115(17):2340–3.
9. • Thuny F, Habib G. When should we operate on patients withacute infective endocarditis? Heart. 2010;96(11):892–7. A reviewof indications and timing of surgery in infective endocarditis withemphasis on prognosis and the need for a multidisciplinary ap-proach for optimal management.
10. Vikram HR, Buenconsejo J, Hasbun R, Quagliarello VJ. Impact ofvalve surgery on 6-month mortality in adults with complicated,left-sided native valve endocarditis: a propensity analysis. JAMA.2003;290(24):3207–14.
11. •• Habib G, Badano L, Tribouilloy C, Vilacosta I, Zamorano JL,Galderisi M, et al. Recommendations for the practice of echocar-diography in infective endocarditis. Eur J Echocardiogr.2010;11(2):202–19. Most recent recommendations from the Euro-pean Association of Echocardiography on the utility of echocardi-ography in the optimal management of infective endocarditis.
12. • Kang DH, Kim YJ, Kim SH, Sun BJ, Kim DH, Yun SC, et al. Earlysurgery versus conventional treatment for infective endocarditis. NEngl J Med. 2012;366(26):2466–73. A notable, randomized con-trolled trial that compared clinical outcomes of early surgery toconventional treatment in patients with left-sided native valve infectiveendocarditis.
13. Hamirani YS, Dietl CA, Voyles W, Peralta M, Begay D, RaizadaV. Acute aortic regurgitation. Circulation. 2012;126(9):1121–6.
14. Hansalia S, Biswas M, Dutta R, Hage FG, Hsiung MC, Nanda NC,et al. The value of live/real time three-dimensional transesophagealechocardiography in the assessment of valvular vegetations. Echo-cardiography. 2009;26(10):1264–73.
15. Anguera I, Miro JM, Vilacosta I, Almirante B, Anguita M, MunozP, et al. Aorto-cavitary fistulous tract formation in infective endo-carditis: clinical and echocardiographic features of 76 cases andrisk factors for mortality. Eur Heart J. 2005;26(3):288–97.
16. Evangelista A, Gonzalez-Alujas MT. Echocardiography in infec-tive endocarditis. Heart. 2004;90(6):614–7.
17. Baddour LM, Wilson WR, Bayer AS, Fowler Jr VG, Bolger AF,Levison ME, et al. Infective endocarditis: diagnosis, antimicrobialtherapy, and management of complications: a statement for health-care professionals from the Committee on Rheumatic Fever, Endo-carditis, and Kawasaki Disease, Council on Cardiovascular Diseasein the Young, and the Councils on Clinical Cardiology, Stroke, and
340 Curr Infect Dis Rep (2013) 15:335–341

Cardiovascular Surgery and Anesthesia, American Heart Associa-tion: endorsed by the Infectious Diseases Society of America. Circu-lation. 2005;111(23):e394–434.
18. Sudhakar S, Sewani A, Agrawal M, Uretsky BF. Pseudoaneurysm ofthe mitral-aortic intervalvular fibrosa (MAIVF): a comprehensivereview. J Am Soc Echocardiogr. 2010;23(10):1009–18. quiz 112.
19. Bachour K, Zmily H, Kizilbash M, Awad K, Hourani R, HammadH, et al. Valvular perforation in left-sided native valve infectiveendocarditis. Clin Cardiol. 2009;32(12):E55–62.
20. Habib G. Management of infective endocarditis. Heart.2006;92(1):124–30.
21. Di Salvo G, Habib G, Pergola V, Avierinos JF, Philip E, Casalta JP,et al. Echocardiography predicts embolic events in infective endo-carditis. J Am Coll Cardiol. 2001;37(4):1069–76.
22. Mugge A, Daniel WG, Frank G, Lichtlen PR. Echocardiography ininfective endocarditis: reassessment of prognostic implications ofvegetation size determined by the transthoracic and the transeso-phageal approach. J Am Coll Cardiol. 1989;14(3):631–8.
23. Cormier B, Vahanian A. Echocardiography and indications forsurgery. Eur Heart J. 1995;16(Suppl B):68–71.
24. Thuny F, Di Salvo G, Belliard O, Avierinos JF, Pergola V, RosenbergV, et al. Risk of embolism and death in infective endocarditis:prognostic value of echocardiography: a prospective multicenterstudy. Circulation. 2005;112(1):69–75.
25. Ellis ME, Al-Abdely H, Sandridge A, Greer W, Ventura W. Fungalendocarditis: evidence in the world literature, 1965–1995. Clin InfectDis. 2001;32(1):50–62.
26. Zoghbi WA, Chambers JB, Dumesnil JG, Foster E, GottdienerJS, Grayburn PA, et al. Recommendations for evaluation ofprosthetic valves with echocardiography and doppler ultrasound:a report From the American Society of Echocardiography'sGuidelines and Standards Committee and the Task Force onProsthetic Valves, developed in conjunction with the AmericanCollege of Cardiology Cardiovascular Imaging Committee, Car-diac Imaging Committee of the American Heart Association,the European Association of Echocardiography, a registeredbranch of the European Society of Cardiology, the JapaneseSociety of Echocardiography and the Canadian Society ofEchocardiography, endorsed by the American College of Cardi-ology Foundation, American Heart Association, European As-sociation of Echocardiography, a registered branch of the Eu-ropean Society of Cardiology, the Japanese Society of Echocar-diography, and Canadian Society of Echocardiography. J AmSoc Echocardiogr. 2009;22(9):975–1014. quiz 82–4.
27. Piper C, Korfer R, Horstkotte D. Prosthetic valve endocarditis.Heart. 2001;85(5):590–3.
28. Sugeng L, Shernan SK, Weinert L, Shook D, Raman J, Jeevanan-dam V, et al. Real-time three-dimensional transesophageal echo-cardiography in valve disease: comparison with surgical findingsand evaluation of prosthetic valves. J Am Soc Echocardiogr.2008;21(12):1347–54.
29. Kronzon I, Sugeng L, Perk G, Hirsh D, Weinert L, Garcia FernandezMA, et al. Real-time 3-dimensional transesophageal echocardiogra-phy in the evaluation of post-operative mitral annuloplasty ring andprosthetic valve dehiscence. J Am Coll Cardiol. 2009;53(17):1543–7.
30. Chan P, Ogilby JD, Segal B. Tricuspid valve endocarditis. AmHeart J. 1989;117(5):1140–6.
31. Martin-Davila P, Navas E, Fortun J, Moya JL, Cobo J, Pintado V,et al. Analysis of mortality and risk factors associated with nativevalve endocarditis in drug users: the importance of vegetation size.Am Heart J. 2005;150(5):1099–106.
32. San Roman JA, Vilacosta I, Lopez J, Revilla A, Arnold R, SevillaT, et al. Role of transthoracic and transesophageal echocardiogra-phy in right-sided endocarditis: one echocardiographic modalitydoes not fit all. J Am Soc Echocardiogr. 2012;25(8):807–14.
33. Berger M, Delfin LA, Jelveh M, Goldberg E. Two-dimensionalechocardiographic findings in right-sided infective endocarditis.Circulation. 1980;61(4):855–61.
34. Naqvi TZ, Rafie R, Ghalichi M. Real-time 3D TEE for the diag-nosis of right-sided endocarditis in patients with prosthetic devices.JACC Cardiovasc Imaging. 2010;3(3):325–7.
35. Feuchtner GM, Stolzmann P, DichtlW, Schertler T, Bonatti J, ScheffelH, et al. Multislice computed tomography in infective endocarditis:comparison with transesophageal echocardiography and intraopera-tive findings. J Am Coll Cardiol. 2009;53(5):436–44.
36. Hill EE, Herijgers P, Claus P, Vanderschueren S, Peetermans WE,Herregods MC. Abscess in infective endocarditis: the value oftransesophageal echocardiography and outcome: a 5-year study.Am Heart J. 2007;154(5):923–8.
37. Stout KK, Verrier ED. Acute valvular regurgitation. Circulation.2009;119(25):3232–41.
38. John MD, Hibberd PL, Karchmer AW, Sleeper LA, Calderwood SB.Staphylococcus aureus prosthetic valve endocarditis: optimal manage-ment and risk factors for death. Clin Infect Dis. 1998;26(6):1302–9.
39. Kini V, Logani S, Ky B, Chirinos JA, Ferrari VA. St John SuttonMG,et al. Transthoracic and transesophageal echocardiography for theindication of suspected infective endocarditis: vegetations, bloodcultures and imaging. J Am Soc Echocardiogr. 2010;23(4):396–402.
40. Reynolds HR, Jagen MA, Tunick PA, Kronzon I. Sensitivity oftransthoracic versus transesophageal echocardiography for the de-tection of native valve vegetations in the modern era. J Am SocEchocardiogr. 2003;16(1):67–70.
Curr Infect Dis Rep (2013) 15:335–341 341