role of hit vendors in promoting safe use of …...1 role of hit vendors in promoting safe use of...
TRANSCRIPT

1
Role of HIT Vendors in Promoting Safe Use of Biosimilars
Session #312, February 22, 2017
Stella Stergiopoulos, MS, MPH; Senior Project Manager, Tufts CSDD
Thomas Felix, MD, Medical Director, R&D Policy; Global Regulatory Affairs and Safety, Amgen, Inc.

2
Speaker Introduction
Thomas Felix, MD
Medical Director, R&D Policy; Global Regulatory Affairs and Safety
Amgen, Inc.
Add Speaker
Photo Here
3
Speaker Introduction
Stella Stergiopoulos, MS, MPH
Senior Project Manager
Tufts Center for the Study of Drug Development (CSDD)

4
Conflict of Interest
Thomas Felix, MD
Employee and holds stock in Amgen, Inc.

5
Conflict of Interest
Stella Stergiopoulos, MS, MPH
Has no real or apparent conflicts of interest to report.
6
Agenda
• Biologics and Biosimilars: An Overview
• Legislative and Regulatory Activity
– Biosimilar Naming
– Substitution
– Tracking of Adverse Events
• Review of current Adverse Event reporting experiences of Pharmacies,
Practices and Integrated Delivery Networks
• Impact of Biosimilars on Healthcare Information Technology Vendors
• Summary and Open Discussion

7
Learning Objectives
• Assess impact of current biologic and biosimilar legislation and regulations
(biosimilar naming, state substitution, reporting) on your organization, institution
and/or product
• Evaluate current Adverse Event reporting experience and impact on reporting of
biologics and biosimilars through review of research conducted by Tufts
University Center for Drug Development
• Discuss framework of what needs to be done by stakeholders to capture to
support specific product identification, ensure precise product tracking and allow
for accurate, efficient reporting and tracing of Adverse Events associated with
biologics

8
Polling Question• Current Experience with Biosimilars?
– Extensive Experience (Prescribing, Dispensing, Tracking of Adverse Events)
– Moderate Experience
– Limited Experience (Have heard about them, but have not yet prescribed, dispensed or done any tracking of Adverse Events)

9
An Introduction of How Benefits Were Realized for the Value of Health IT
Treatment/Clinical:
• Improved Clinical Documentation and
• Overall Improved patient safety
Electronic Secure Data:
• Improved access for data research
• Data Reporting
10
News about Biologics and Biosimilars is everywhere
11
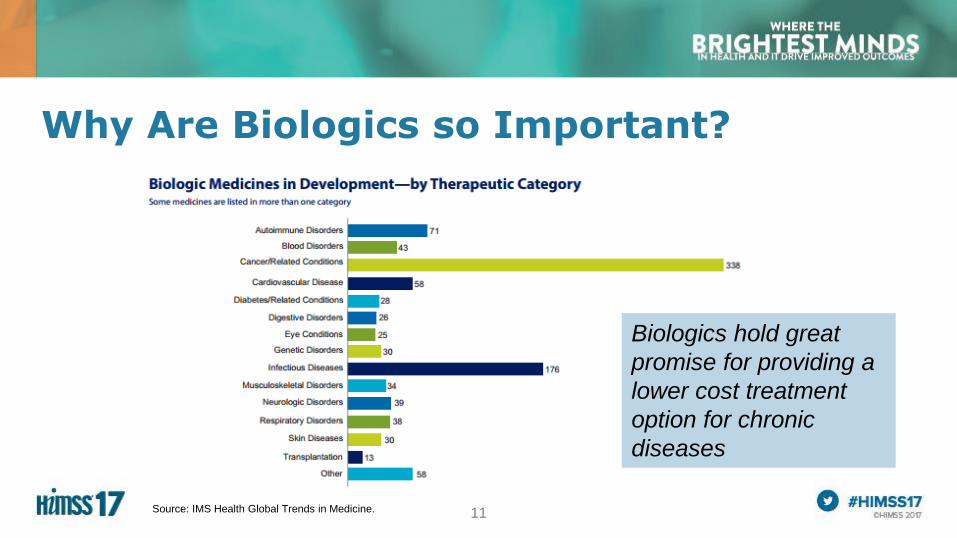
Why Are Biologics so Important?
Biologics hold great
promise for providing a
lower cost treatment
option for chronic
diseases
Source: IMS Health Global Trends in Medicine.

12
Small Molecules Biologic Compounds
a group of atoms joined by
chemical bonds; the smallest
amount of a substance that
possesses its characteristic
properties. Molecule based.
A preparation that is synthesized from living
organisms or their products, especially a
human or animal protein, such as a hormone
or antitoxin, that is used as a diagnostic,
preventive, or therapeutic agent.
• Chemical synthesis
• Predictable chemical
process
• Identical copies possible
• Stable
• Made in living cells
• Unpredictable manufacturing process
• Difficult / impossible to
create identical copy
• Unstable
Generic Molecules Biosimilars
Definition*
Manufacturing
Competitive
products*
Biologics: What are they?
* Source: http://medical-dictionary.thefreedictionary.com/Small+molecule;

13
Biosimilars: What are they?
Generic Molecules Biosimilars
Generic equivalent. A drug that is no
longer under patent protection, which
may be produced by any manufacturer
who follows good manufacturing
protocols. Identical to the innovative
original drug
A biopharmaceutical which is produced by
a different manufacturer after the
expiration of the patent and marketing
exclusivity of an original innovative
biological product (e.g., a therapeutic
monoclonal antibody). Highly similar to
original biologic.
Interchangeable and therefore
substitutable without prescription in all
states (considered therapeutically
equivalent) – Hatch-Waxman Act
(1984)
Not always therapeutically equivalent
and interchangeable (different active
ingredient)
1. Biosimilars: analytical studies show
product is “highly similar”
2. Interchangeable Biosimilar:
Requires biosimilarity AND switching
from original biologic does not impact
safety or efficacy
Definition*
Rules on
Substitution

14
Current Regulatory Activity around Biosimilars
• FDA final guidance on Non-Proprietary biologic product naming released January 2017
• Different naming conventions across regulatory agenciesBiosimilar Naming
• Different rules across countries
• Legislation in 18 states
• FDA Draft Guidance released January 2017
Biosimilar Substitutions and Interchangeability
• Limitations with FDA’s Medwatch
• Limitations for reporting (at hospitals; private practice; retail pharmacies)
Biosimilar tracking and reporting for
ADEs
15
Biosimilars: Legislative and Regulatory Activity
• Biosimilar Naming
• FDA released draft guidance on nonproprietary biologic product naming (Sept 2015)
• Biosimilar Substitutions and Interchangeability
• Legislation in 26 states
• FDA Draft Guidance expected in 2017
• Biosimilar tracking and reporting for adverse drug events (ADEs)
It’s all about patient safety
and holding manufacturers’
accountable
16
FDA Guidance on Biologic Naming
• An FDA-designated suffix be added to the nonproprietary biologic name
• Suffix would be composed of a random set of 4 lowercase letters
• Changing the names of 6 existing reference and biosimilar products
• Add suffix to the nonproprietary name
Guidance seeks to address 2 main issues: Help prevent inadvertent
substitution and provide support for after-market safety monitoring of all
biologic products.
Example:
Nonproprietary name of
reference product:
replicamab-cznm
Biosimilar of that product:
replicamab-hixf
17
• New laws/regulations are emerging around biosimilar substitutions and physician notification
• Amending current statutes and pharmacy board generic substitution rules to accommodate biosimilars
• 28 states are considering or have passed legislation establishing standards for substitution of a biosimilar product
Biosimilar Substitution
A flurry of state-level activities
FDA Draft Guidance around biosimilar substitution was expected in 2016; now delayed
to 2017

18
Biosimilar Substitution NotificationAK
MD
WA
OR
NV
ID
AZ NM
UT CO
WY
MT ND
SD
NE
KS
OK
FL
LA
AR
MO
IA
MN
WI
IL
OH
KY
TN
MS ALGA
SC
NC
VAWV
MI
PA
ME
NY
HI
NH
RI
NJ
MA
DE
DC
CA
TX
IN
VT
CT
In the past four years,
at least 36 states have
considered legislation
establishing state
standards for
substitution of a
“biosimilar.”
Laws have been
passed in 25 States
and PR; 4 states have
pending legislation
Source: National Conference of State Legislatures, State Laws and Regulations
related to Biologic Medications and substitution of biosimilars, April 2016

19
Biosimilar tracking for ADEs
Currently, there is no
pending legislation around
Tracking and reporting ADEs

20
US Health Care Professional Perspectives on Adverse Drug Event Reporting in the Hospital Setting and the Opportunity for Information Technology
Stella Stergiopoulos, Tufts CSDD
Carrie A. Brown, Tufts University
Thomas Felix, Amgen Inc.
Gustavo Grampp, Amgen Inc.
Kenneth A. Getz; Tufts CSDD
Results of study conducted
by Tufts CSDD in 2015 and
2016.
Recently published in the
November, 2016 Issue of
the Drug Safety Journal

21
What is the role of health information technology (HIT) in pharmacovigilance?
• Should not be a barrier to reporting adverse drug events (ADEs)
• Should link patient care, pharmacy and institutional safety systems
– Identifiable patient, reportable event, suspect drug (spontaneous reports)
• Should comply with government policies and standards
– Product-specific and batch-specific tracking of biological products
22
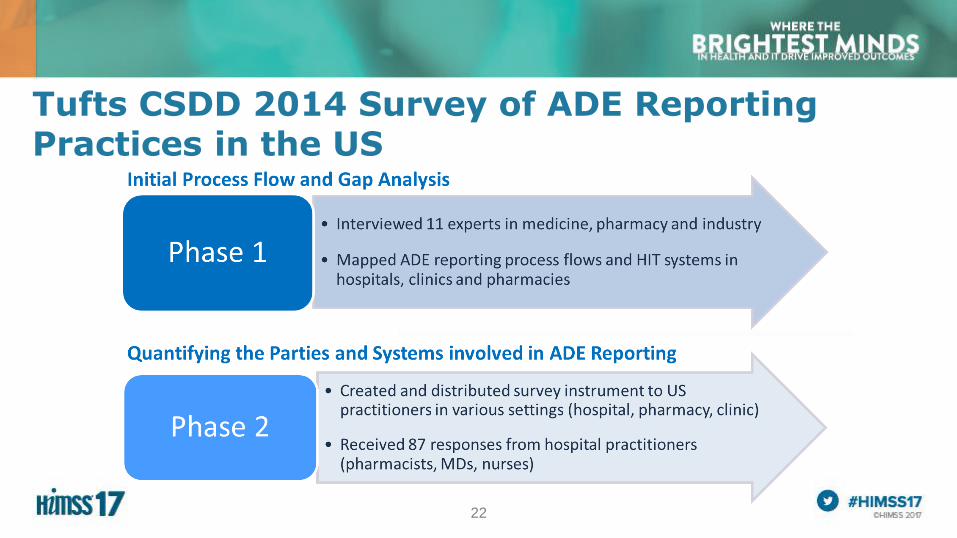
Tufts CSDD 2014 Survey of ADE Reporting Practices in the US

23
Phase 2: Survey findings identified a typical Hospital-based ADE reporting process flow
24
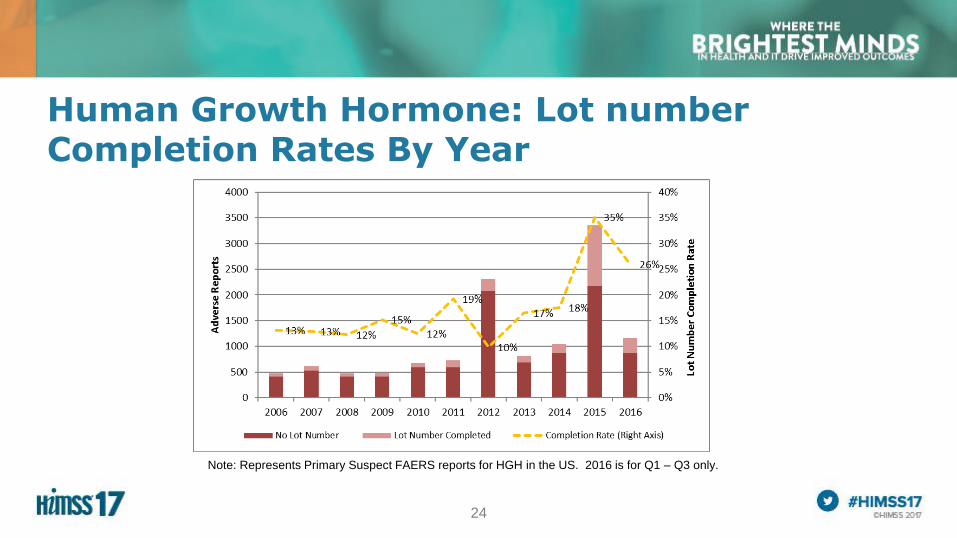
Human Growth Hormone: Lot number Completion Rates By Year
Note: Represents Primary Suspect FAERS reports for HGH in the US. 2016 is for Q1 – Q3 only.
25
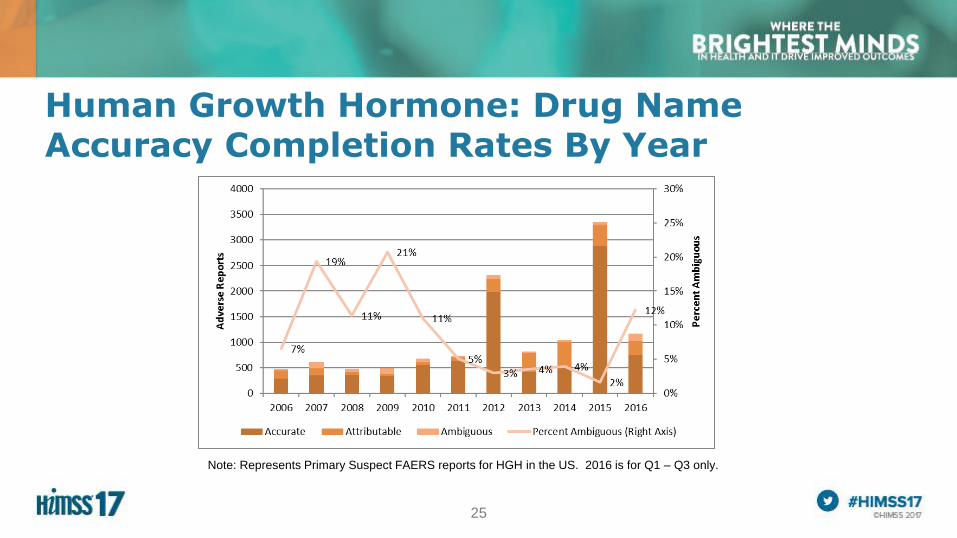
Human Growth Hormone: Drug Name Accuracy Completion Rates By Year
Note: Represents Primary Suspect FAERS reports for HGH in the US. 2016 is for Q1 – Q3 only.
26
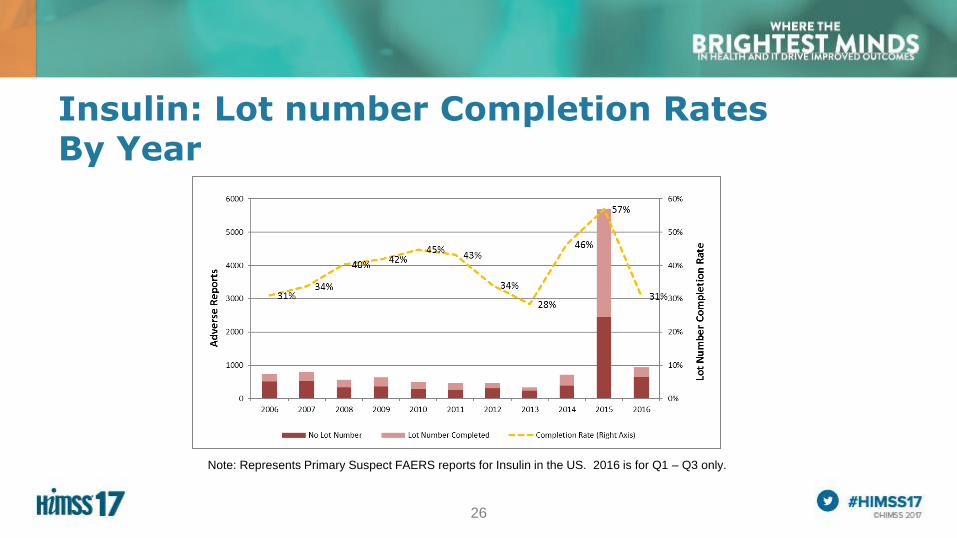
Insulin: Lot number Completion Rates By Year
Note: Represents Primary Suspect FAERS reports for Insulin in the US. 2016 is for Q1 – Q3 only.
27
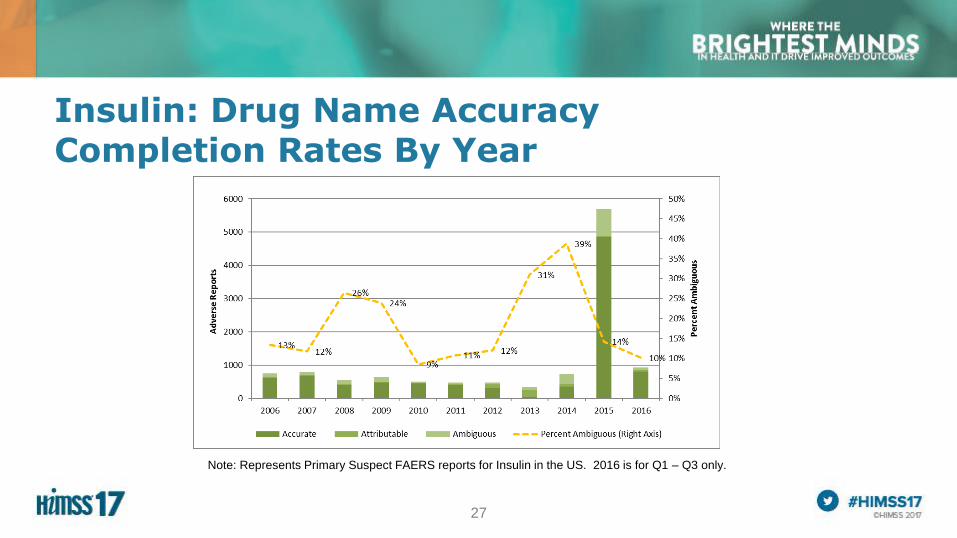
Insulin: Drug Name Accuracy Completion Rates By Year
Note: Represents Primary Suspect FAERS reports for Insulin in the US. 2016 is for Q1 – Q3 only.

28
Polling Question• Current experience with process of reporting ADEs?
– Extensive Experience
– Moderate Experience
– Limited Experience

29
Phase 2 Results: Reason for not reporting ADEs
“Based on your
experience, how often do
each of these reasons
prevent health care
providers from reporting
ADEs to the FDA or the
manufacturer?”
(n = 87)
Lack of system
integration was cited as
a significant reason for
not reporting ADEs
(52%)*

30
Phase 2 Results: Reason for not reporting ADEs
*Question was “Based on your experience, how
often do each of these reasons prevent health
care providers from reporting ADEs to the FDA
or the manufacturer? “ (n=87)
Key details are spread among multiple data sources
– Drug details spread across 4 or more sources (46%, n=74)
– ADE details spread across 3 or more sources (51%, n=69)

31
Limited availability of important drug data elements in HIT systems
Note: N = 63. Question was “Which of the following
data about the particular drug administered to a
particular patient are routinely available in your
electronic systems?”
• Manufacturer (field or NDC code) and lot identifiers are scarce in most systems
• Bar code based systems may improve data capture
32
Study Summary
• Hospital IT systems are an essential source for recording and retrieving ADE and suspect drug information
• Presence of multiple systems that lack integration may be an obstacle to efficient ADE reporting
• Many systems may not capture drug identifiers other than brand and/or INN
• Recommendations:
– Improve access to information: Interoperability/integration of drug identifiers and ADE data from multiple systems
– System designs should permit use of brand names for biologics
– Integrate product-specific data from bar code based systems into other HIT systems to improve lot-level traceability

33
Biologics and Biosimilars: Impact on HIT Vendors
• Biosimilars are here and many more are coming to market
• Biosimilar substitution is not the same as generic substitution
• New rules are in place to notify prescribers when pharmacists substitute biosimiiars
• Point of Care tracking of biosimilar ADEs is essential
• EHRs and Pharmacy Information Systems must adapt to accommodate:
• Biosimilar drug names
• Receipt of substitution notification
• Receipt of expanded drug information from pharmacies on MedHx and RxFill
• Tracking and reporting of biosimilar ADEs at the point of care

34
An Introduction of How Benefits Were Realized for the Value of Health IT
Treatment/Clinical:
• Improved Clinical Documentation and
• Overall Improved patient safety
Electronic Secure Data:
• Improved access for data research
• Data Reporting

35
Questions for Essential Discussion

36
Questions
Please complete online session evaluation: Session #312
Thomas Felix, MD, Medical Director, R&D Policy
Global Regulatory Affairs and Safety, Amgen, Inc.
Stella Stergiopoulos, MS, MPH; Senior Project
Manager, Tufts CSDD