ron rapini md, chernosky chair, dept dermatology ... · rare infections ron rapini md, chernosky...
TRANSCRIPT

Rare Infections
Ron Rapini MD, Chernosky Chair, Dept Dermatology, Professor of Pathology
Univ Texas Medical School at Houston &
MD Anderson Cancer Center

No conflicts of
interest – No stock in
stores that sell rapini

Format – presentation of 12 unusual
cases
Well, we won’t get through them all

Case 1. Forearm plaque, 40-year-old woman

Sent biopsy to me for dermpath
second opinion
• Dermatologist: “Probable
keratoacanthoma”
• Dermatopathologist: Yes,
“C/W keratoacanthoma,
transected at base”
“garbage in, garbage out
phenomenon”




“Has patient traveled
anywhere?”
•Answer: Costa Rica
and Missouri

Leishmania – call CDC for N,N,N
media (Nicolle-Novy-MacNeal)
• Ship to you free of charge
• Speciation done by CDC in Atlanta,
Georgia, USA
• Speciation important for prognosis
determination

Two weeks post-excision: very happy (like most of my patients)

Rx recommended by
CDC• Ketoconazole 200 mg t.i.d for one
month
(many other anecdotal treatments
have been used: itraconazole,
allopurinol, topical antimony,
cryotherapy, etc)

After one month ketoconazole


Sporotrichoid – “SLANT”
• S = Sporotrichosis
• L = Leishmaniasis
• A = Atypical mycobacteria
• N = Nocardiosis
• T = Tularemia

Time to refer to infectious disease
service for IV Pentostam (antimony)
– CDC ships free of charge
• Antimony causes EKG abnormalities – patient found to have cardiomyopathy
• So… was treated with good result with IV pentamidine

Leishmaniasis sp.• L. tropica = oriental sore, Middle East, self-
healing
• L. mexicana = Central and South America,
self-healing
• L. braziliensis = Central and South America,
aggressive course with risk mucocutaneous
spread
This patient grew L. panamensis, related to
braziliensis

L.guyanensis -
Equador

L.guyanensis -
Equador

L.guyanensis - Equador

L.guyanensis -
Equador


L.guyanensis –
Equador –
sporotrichoid!

Case 2:
Photo by KhanhNguyen MD


Case 2
• Lived in a refugee camp for 10 years
• Admitted to hospital 3 days after arrival
in the US
• No HIV meds, CD4 = 8
• Fever, sepsis, malaise, weight loss
• Cachectic, hypotensive,
lymphadenopathy, rales,
hepatosplenomegaly



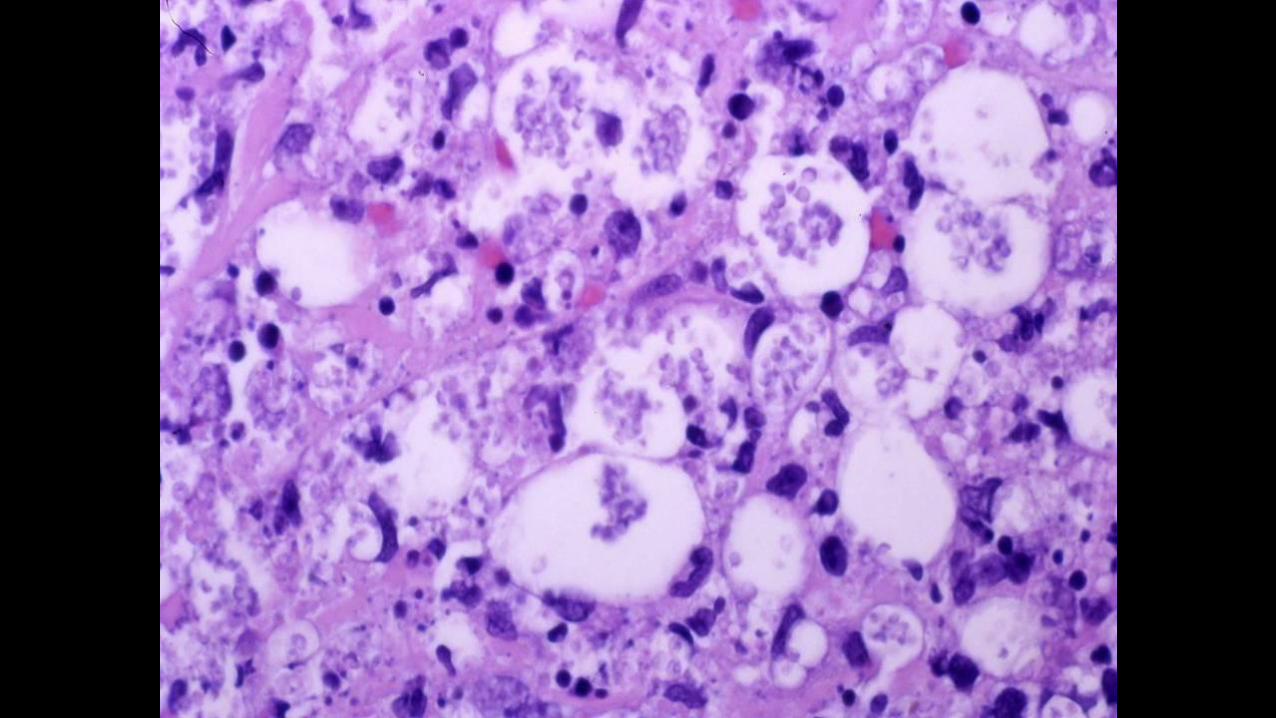






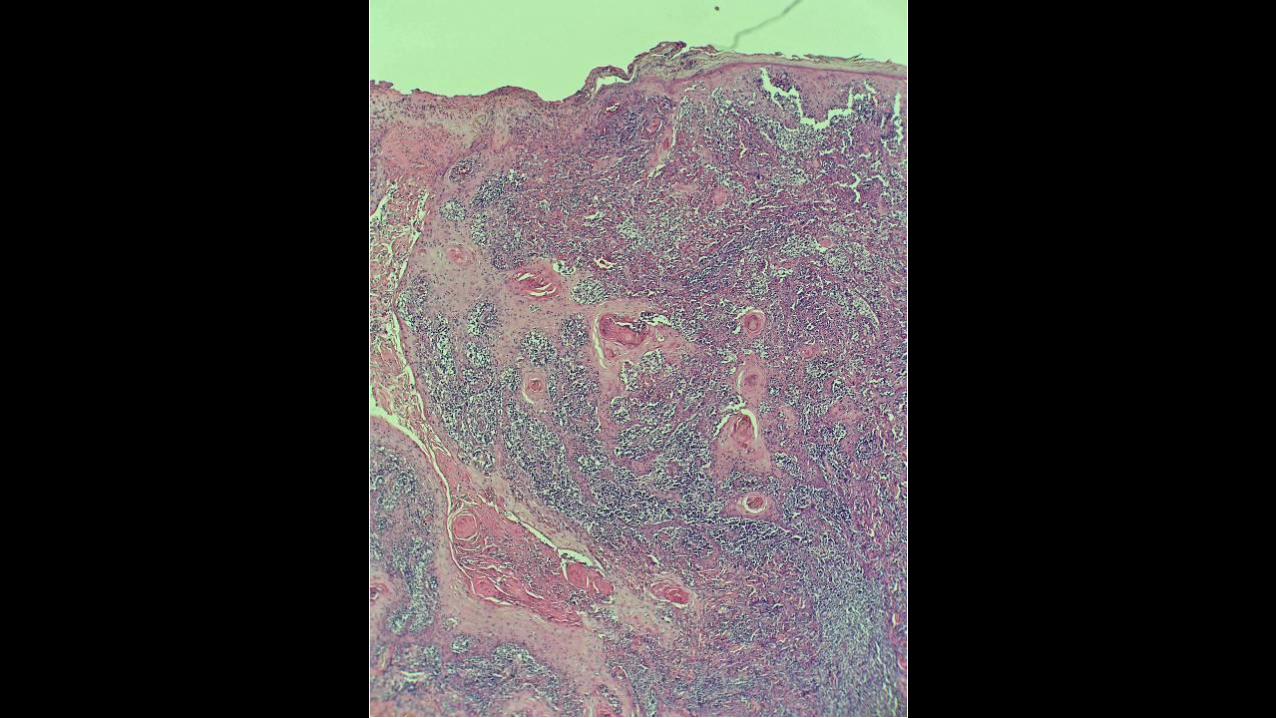
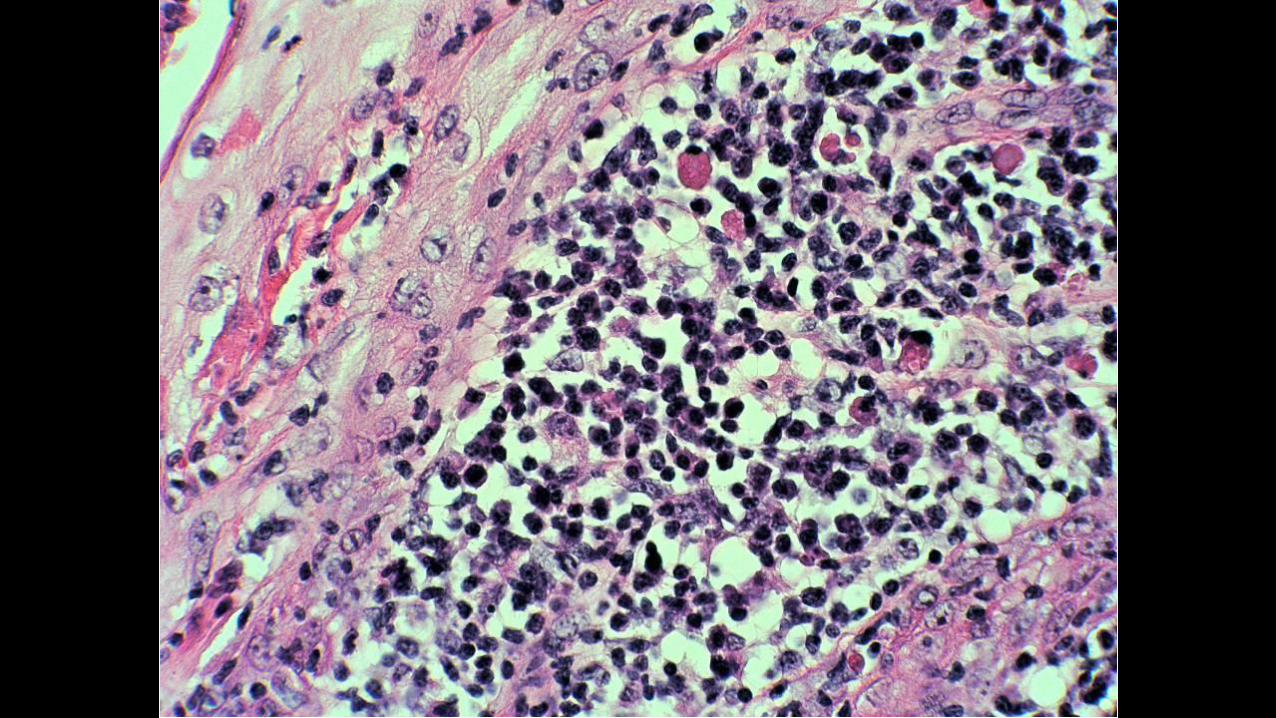
Talaromyces (formerly Penicillium) marneffei

Talaromyces (Penicillium) marneffei - GMS
Nguyen K, Taylor S, Wanger A, Ali A, Rapini RP: A
case of Penicillium marneffei in a US hospital. J Am
Acad Dermatol 54:730-732, 2006

Histoplasma

Leishmania

Cryptococcus

Penicilliosis• Endemic in Southeast Asia
• Mainly in the immunosuppressed
• AIDS-defining disorder
• Reservoir uncertain – bamboo rat?
• Probably acquired by inhalation
• Average CD4 count is 64 cells/mL

Penicilliosis findings
• Papules resemble molluscum, acne
• Face (forehead) more than arms, trunk,
sometimes mouth
• Infection can be localized or disseminated
• Bone marrow 54%
• Blood 15% (intracellular or extracellular)
• Liver, spleen, lung
• ELISA, PCR has been used to identify

Penicillium marneffei• The only dimorphic Penicillium
species (but now is Talaromyces)
• Mold at 25 degrees, yeast at 37
• Organism at high power divides by
fission, not by budding
• Some cells elongated like sausages,
some with crosswalls

Penicilliosis treatment• High mortality without treatment
• Responds in 7 days with treatment, but long term treatment needed, often recurs
• Liposomal amphotericin B (Ambisone), itraconazole, ketoconazole, voraconazole
• Our patient did well on Ambisone and itraconazole

Case 3
• “Doc, I think I’ve got worms in
my head so I shaved my head
so you can see them”

“I just got back from Belize, in
Central America, where I was
looking for reptiles for the
Houston zoo.”





Anus
Dermatobia hominis





As in most of my patients,
the treatment was curative,
and he never came back

Several months later…
• Another patient, also having returned from Belize, working in oil exploration, complained: “I think I have some kind of worm in my leg, because I can see him moving in this hole.”
(case 4)




Human bot fly,
Dermatobia hominis
Furuncles with “breathing holes”
Travel to Central or South
America
Surgery not needed – use pork
fat, beef, petrolatum, gum, etc!


Specific myiasis – a particular
maggot prefers a specific host
Nonspecific myiasis – flies lay
eggs on any old rotting flesh
(such as old leg ulcer)

“Specific” myiasis• Cordylobia
(tumbu fly)
• Dermatobia (human botfly)
• Callitroga (screw worm)
• Chrysomya (Old World screw worm)
• Africa
• Central and S.
America
• Warm western
hemisphere
• Ethiopia

Specific myiasis (worldwide)
• Hypoderma
• Oestrus
• Gasterophilus
• Cuterebra
• Wohlfahrtia
• Cattle botfly
• Sheep botfly
• Horse botfly
• Rodent botfly
• Flesh fly

Courtesy Phil Cohen MD
Case 5: “Something is
biting me”



4-5 mm when unfed!

Bedbugs
• Everyone knows about
them, but few patients and
dermatologists have seen
them
• Three species: Cimex
lectularius is most common

Bedbugs
• Hide in bedclothes, mattresses, bed
frame, cracks in building, under
wallpaper
• Often congregate; if many, there
can be a sweet odor
• Feed only 5 minutes at night
• Painless bite, but saliva causes
urticaria, rarely bullae

Bedbugs
• Also bite chickens, bats, some
domestic animals
• Urticarial reaction to saliva
injected through sucking tube
mouthpart
• Hepatitis B DNA found in
bedbugs; unproven to spread this
and other infectious agents

Bedbugs Rx
• Heat: 120 degrees F to kill them
• Or freeze them several days
• Insecticides are not highly
effective. Pyrethroids will kill
them but not prevent egg laying
and will not repel them

Bedbugs Rx
• Bedbug sniffing dog
• Nightwatch trap: kairomones and
carbon dioxide attractant
• Hotels want to sue
bedbugregistry.com

Bedbugs PREVENTION
• Keep suitcase far from bed and
keep it zipped up
• Put suitcase on the stand with the
metal legs

Case 6 Forearm ulcer after local trauma in
Mexico
DP-88-4892

DP-88-4892

DP-88-4892
Gram stain

DP-88-4892 GMS

Nocardia asteroides
Nocardia braziliensis• Pulmonary, CNS, Skin
• Gram+, GMS+, AFB+
• Sulfur granules sometimes
• Grows is 2-5 days in blood agar or routine culture,
but lab has to hold it longer
• Aerobic, unlike Actinomyces

Case 6 Nocardiosis
• Primary inoculation non-systemic form often resolves spontaneously
• Trimethoprim-sulfamethoxazole DS bid for 2 to 4 weeks
• F/U on this case – healed readily with above Rx

7. Brown macule, palm

7. Tinea nigra• Brown patch may resemble lentigo,
macular SK, pigmented Bowen’s
• Surgery sometimes done when mistaken for melanocytic neoplasm
• Culture or KOH prep positive
Formerly Cladosporium, Exophiala, then Phaeoannellomyces
Now Hortaea werneckii
Times are a changin’ – constant renaming
• Penicillium marneffei, now Talaromyces
• Cladosporium, Exophiala,
Phaeoannellomyces, now Hortaea
werneckii
• Pityrosporum orbiculare or ovale, now
Malassezia furfur
• Paracoccidiodes loboi, Lobo loboi, now
Lacazia
Times are a changin’ – nonfungi too
• Chancroid’s Calymmatobacterium,
Donovania, now Klebsiella granulomatis
• Cat scatch’s Rochalimaea, now Bartonella
henselae

Me too’s – additional agents
• Leprosy’s Mycobacterium leprae, also M.
lepromatosis
• Coccidioidomycosis’ Coccidioides
immitis, also C. posadasii
• S. Amer Blasto’s Paracoccidioides
braziliensis, also P. lutzii


Tinea nigra


prep from culture, tinea nigra

Another one,
case 7b

This time, tinea nigra proven from KOH prep
without biopsy

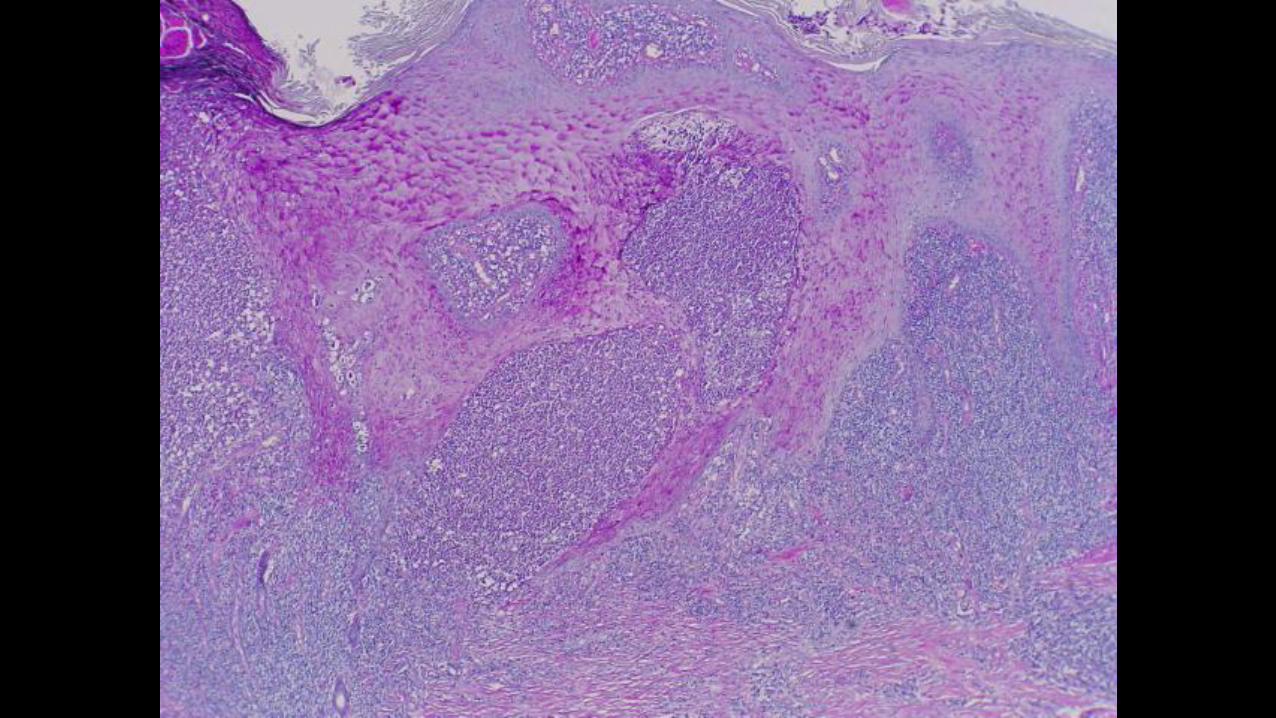
8. Rare annular form of chromomycosis
VA 82-1225

VA 82-1225

VA 82-1225


8. Chromomycosis
• Usually adult males, esp farmers
• Black dots may be seen
• KOH may be positive
• Culture for speciation
• Excision may be curative as
opposed to antifungal Rx

Chromomycosis SMA 1986 #17

Chromomycosis SMA 1988 #23

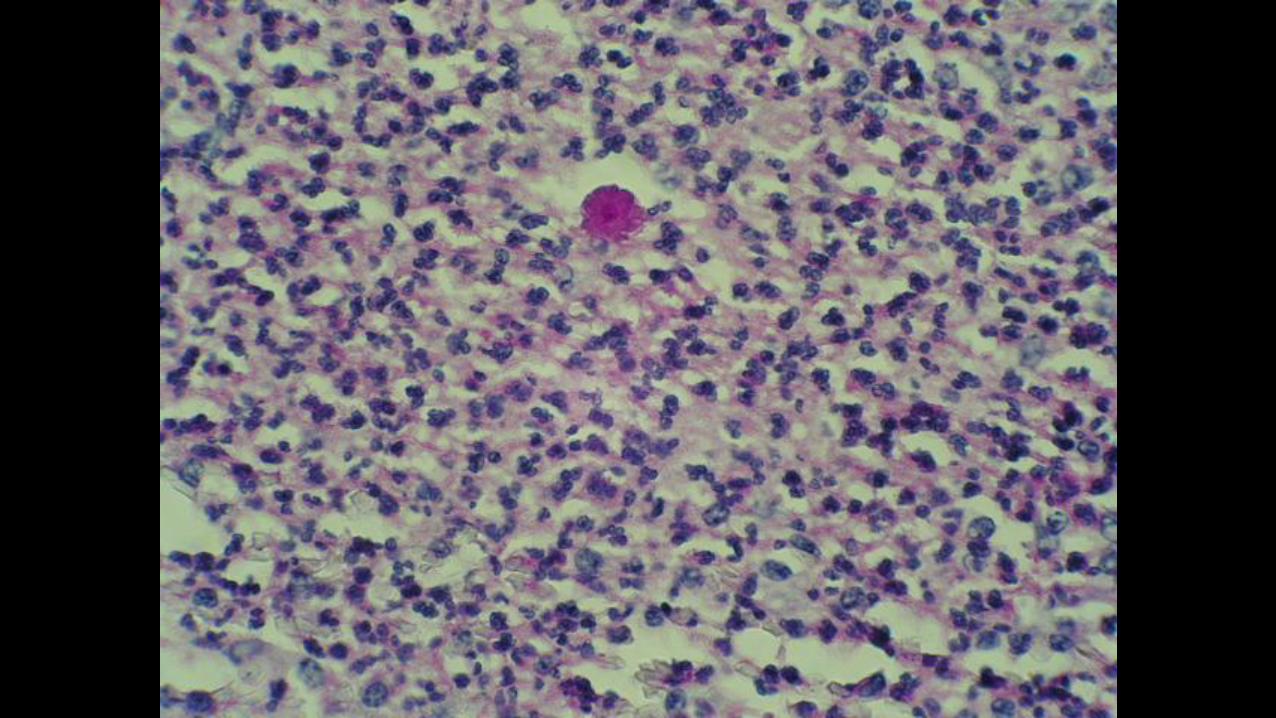
8. Chromomycosis• Pseudocarcinomatous hyperplasia
• Intraepithelial microabscesses
• Granulomatous inflammation
• Copper pennies = Medlar bodies =
sclerotic bodies, 6-12 microns,
planate-dividing (cissiparity)
• Phaeohyphomycosis is different
(brown hyphae instead of spores)

Chromomycosis
Dematiaceous (brown) fungi
• Phialophora verrucosa
• Fonsecaea pedrosoi
• Fonsecaea compacta
• (Hormodendrum)
• Exophiala sp
• Cladosporium carrionii

Dematiaceous fungi
• The brown pigment is indeed melanin – can
do Fontana melanin stain (not needed)

Case 9
Phaeohyphomycosis
• Painful nodule on knee x 1 year:
“KA vs prurigo”



Phaeohyphomycosis – hyphae

Sulfur
granule
from
draining
sinus tract
of
Mycetoma

10. Sporotrichosis: DP03-3123



Sporotrichosis: Asteroid bodies


Sporotrichosis: yeast and cigar bodies

Sporotrichosis histology
• Often see NO organisms, deeper
levels help
• Most commonly just see budding
yeast averaging 3-8 microns
• Sometimes cigar bodies
• Sometimes asteroid bodies

Sporotrichosis –
often Sporotrichoid
spread

Case 11 complaint of worms/fibers –jungle of Peru



I gave a talk at AAD in 2007 on
Morgellons disease when it was
“new” – one of the biggest
mistakes of my life
Now the dermatologists in Houston send
them all to me, or eventually the
patients find me, as they go from doc
to doc, and I average one of these per
week

History of Morgellons disease
• pronounced mor-GELL-uns
• Named in 2002 by Mary Leitao.
• Woman with B.S. in Biology who says her
son suffers from the condition, founded the
Morgellon’s Research Foundation

History of Morgellons disease
• Sir Thomas Browne in 1674: “children of
Languedock, called the Morgellons,” wherein
they break out with “harsh Hairs on their
Backs”
• Described in 1544 by Faventinus as an
intercutaneous worm of children that
“protrude their little heads”

Morgellons Research Foundation
http://www.morgellons.org/
• 9045 registered households in Feb 2007
• #1 California, #2 Texas
• #1 Nurses, #2 Teachers

2012: The Morgellons Research
Foundation (MRF) is no longer
an active organization and is not
accepting registrations or
donations.
The MRF donated remaining
funds to the Oklahoma State
University Foundation to support
their Morgellons disease
research.

Charles Holman Morgellons
Disease Foundation
Named for husband of
affected patient (an RN)
10th Annual Conference on
Morgellon’s Disease (and rally)
April 29, 2017 – May 1, 2017
Austin, Texas

Morgellons disease: a chemical and light
microscopy study
Middelveen MJ, Rasmussen EH, Kahn DG,
Stricker RB. J Clin Exp Dermatol Res. 2012
“This study puts the final nail in the coffin of
delusional disease that these patients have been labeled
with,” stated Dr. Stricker . “It proves that Morgellons
disease is a physiologic illness.”

Telling The Truth You Were
Never Supposed To Know
http://www.morgellonsexposed.com/
“People who suffer from Morgellons
disease are NOT delusional no matter
what the CDC or the mainstream press
would have you believe.”

Morgellons Research Foundation
Case Definition (CDC also investigated)
1. Skin lesions
2. Crawling sensations
3. Fatigue
4. Cognitive difficulties (“brain fog”)
5. Behavioral effects (“labeled as delusional parasitosis”)
6. Fibers (usually white, also blue, green, red, black, fluoresce with Wood’s lamp)

Morgellon’s disease online
• Google search:
15,400 hits as of 2007
1,270,000 results in Aug 2012
191,000 results Mar 2017
• A “disease caused by the internet?” or
“mass hysteria” vs a bonafide unidentified
fiber or organism

“Morgellon’s is biowarfare”
• www.rense.com
• “…may be a logical reason for our
advanced high-tech medical system to
drag its feet”

http://rense.com/Datapages/morgdat1.htm
CDC creeps formally call Morgellon
an hallucination
The CDC and NIH knew and know

http://www.cdc.gov/unexplaineddermopathy/
Clinical, Epidemiologic, Histopathologic and Molecular
Features of an Unexplained Dermopathy
Michele L. Pearson1, Joseph V. Selby2, Kenneth A. Katz3,
Virginia Cantrell2, Christopher R. Braden4,
Monica E. Parise5, Christopher D. Paddock6, Michael R.
Lewin-Smith7, Victor F. Kalasinsky8, Felicia C.
Goldstein9, Allen W. Hightower5, Arthur Papier10,
January 2012 | Volume 7 | Issue 1 | e29908
www.plosone.org

Usefulness of term Morgellon’s
• “A rapport-enhancing term” but “should
not validate a condition” and doc should
clarify “not infectious agent” per Drs
Murase, Wu, Koo. JAAD 2006
• Better than putting “Delusions of
parasitosis” on path requisition: patients
often ask for copy of path report
• Use term R/O “acariasis” instead
Morgellon’s disease treatment –
my non-expert approach (don’t
want to be labeled as an expert)
My approach: Serious look for bugs by
scraping or biopsy, give antiparasite
treatment along with SSRI or other psych
drug for the “stress” – be gentle and
empathetic - they won’t go to psych and
many get angry

A thrip (Thysanoptera): sucks plant juices:
(sometimes they bring in real, but
irrelevant bugs)
Morgellon’s disease treatment –
off-label drugs to gain rapport
(to add to “stress treatment”)
• Topical permethrin, lindane
• Topical crotamiton is also antipruritic
• Topical sulfur products (rosacea products)
• Oral ivermectin

Morgellon’s disease off-label treatment –
treat the stress AND the ?parasites
• pimozide: no prolonged Q-T problems or tardive
dyskinesia if less than 10 mg/day – may not need
EKG. Start 1 mg/day, increase by 1 mg/day every 4
– 7 days. Most patients effective at 4 – 6 mg/day.
Claimed to be antipruritic. Treat extrapyramidal
effects with benztropine myselate 1 – 4 mg IM or
diphenhydramine 25 mg q.i.d

Morgellon’s disease off-label treatment –
treat the stress AND the ?parasites
• olanzapine: start 5 – 10 mg/day, effective dose
10 – 15 mg/day: weight gain, hyperlipidemia,
diabetes, less extrapyramidal
• risperidone: for bipolar or schizophrenic
disorders
• quetiapine: for psychosis

Other drugs off label (I am not expert – better to use
with psychiatrist if you can get patient to agree to it)
• SSRI: citalopram
• SSRI: escitalopram
• SSRI: paroxetine
• SSRI: sertraline
• SSRI: fluvoxamine
• Antidepressant: duloxetine

Alternative approach (not favored by me)
• Confront these patients and tell them
you think they are delusional and that
they need psych drugs
• Tell them they can continue to be
frustrated and go from derm to derm
until they finally have the insight to take
the psych drugs

“Morgellon’s”
I think that these patients at least
need to be taken seriously and a
sincere look for parasites ought to
be undertaken on the first visit

Case 12. Poor old woman, saw multiple docs, labeled
as crazy Morgellon’s disease patient – brought in
the usual “bug” samples to examine
She had had exterminators come
to her house on at least three
occasions

This thing fell from her coat
onto the floor as she was
leaving the exam room!
