root cause analysis (rca) concise investigation report
TRANSCRIPT
Page 1 of 12
Root Cause Analysis (RCA) Concise Investigation Report
Pressure Ulcer (PU)
Root Cause Analysis (RCA) is a well-recognised way of offering a framework for
reviewing patient safety incidents (also investigations claims and complaints). This
process can identify what, how, and why patient safety incidents such as pressure
ulcer(s) have happened. Analysis can then be used to:
Identify areas for change;
Develop recommendations, and;
Look for new solutions.
Ultimately, they should help prevent incidents from happening again.
1. Incident number: ……………………………………………………………………...
2. Date safeguarding alert completed: ………………………………………………
3. Report author: ………………………………………………………………………...
4. Job title: ………………………………………………………………………………
5. Date report completed: ……………………………………………………………
6. Improvement plan completed and attached (Appendix 1) Y / N
Insert organisational logo
Page 2 of 12
1. Concise Incident description
Name of service: …………………………………… (At time of incident)
Type of service: ……………………………………..
(E.g. nursing, domiciliary, residential)
Name of service user General Practitioner……………………………….. Date PU identified: ………………………………………………………… Time PU identified: ……………………………………… PU category: Category 3 Category 4
Brief description of incident
(Factual)
………………………………………………………………………………………… ………………………………………………………………………………………… ………………………………………………………………………………………… …………………………………………………………………………………………
Actual effect on service user and/or service
(How has this impacted on their condition) ………………………………………………………………………………………… ………………………………………………………………………………………… …………………………………………………………………………………………
IMPORTANT NOTES – PLEASE READ BEFORE COMPLETING FORM
Type in RED is for guidance purposes only but can be used in conjunction with relevant information. The aim
of this template is to guide the investigation of how the pressure ulcer(s) developed and to recognise any
lessons learnt to ensure mitigating risks can be identified to reduce the risk of a similar event from occurring.
Please answer all questions together with any supporting information in BLACK. If not relevant to
investigation insert N/A
Page 3 of 12
Information and evidence gathered (E.g. review of incident form, care record, medical records, protocols, policies, training records, appraisal records, national best practice guidelines, clinical studies, phone records, BNF, map of site, photographs, equipment maintenance schedules etc.) - ………………………………….. -…………………………….. .
-…………………………………… -………………………………
-…………………………………… -……………………………...
-…………………………………… -………………………………
Involvement and support provided for the service user involved (How have they been informed of the incident? What has been discussed with the service user/relative/those close to them?) …………………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………
………………………………………………………………………………………………..
…………………………………………………………………………………………………
…………………………………………………………………………………………………
………………………………………………………………………………………………..
Limitations to this report …………………………………………………………………………………………………
…………………………………………………………………………………………………
………………………………………………………………………………………………..
Page 4 of 12
2. Chronology (factual)
Provide a brief timeline of events leading up to the pressure ulcer identification
Date: Details:
Page 5 of 12
3. Analysis of treatment a. Past medical history
Has there been a recent change in medical condition? Y / N List co-morbidities
……………………………………………………………………………………………………………... ……………………………………………………………………………………………………………. …………………………………………………………………………………………………………….
State which of the following are applicable
□ Skin or wound infection
□ Other infection
□ Pyrexia
□ Anaemia
□ End of life
□ Previous pressure ulcer damage
□ Other specify (such as peripheral vascular disease, diabetes, immobility, CVA, steroids, weight loss) …………………………………………………………………………………………………………
b. Summary of pressure ulcer risk assessment and care
Please state dates of risk assessments………………………………………………………………..
Type of risk assessment tool used ……………………………………………………………………
Overall risk level at time pressure ulcer identified……………………………………………………
(e.g. No Risk <4, Low Risk 4-9, Medium Risk 10-14, High Risk >15) c. Key points of preventative plan – (state if in place and specific details)
Did the service user have a pressure ulcer preventative plan in place? (e.g. SSKIN bundle or specific pressure ulcer care plan) Y / N
Surface
Was the preventative plan explicit in what equipment was required? Y / N (State mattress and/or cushion) ……………………………………………………………………………
Skin
Was a skin inspection undertaken as per the assessed frequency? Y / N
Page 6 of 12
Keep moving.
- State repositioning regime at time of identification of PU …………………………………………
- State Waterlow score at time of identification of PU ……………………………………………
- Was the Waterlow score completed on admission to care facility? Y / N
- Was the Waterlow score updated monthly or as per clinical condition dictated? Y / N
Incontinence
- Date of incontinence and moisture assessed: ………………………………………………………
(date/state if no problems identified)
Nutrition.
- Nutrition assessed Y / N Date completed …………………………………………………………
- Were any risks/issues highlighted …………………………………………………………………..
……………………………………………………………………………………………………………….
- Level of risk at time pressure ulcer identified ……………………………………………………..
(0 – 6 Low Risk, 7 – 13 Medium Risk, 14 – 21 High Risk)
d. Reporting
- There was / was not evidence of late reporting (delete as applicable)
e. Mental Capacity
Did you need to undertake a mental capacity assessment in relation to care received? Y / N
If so did the person’s capacity influence decisions made in respect of pressure area care? Y / N
f. Pressure ulcer history
Has the service user had a pressure ulcer previously? Y / N
Is it the same location as current pressure ulcer? Y / N
g. Current Treatment
Is the service user responding to treatment? Y / N
Has a photograph been taken of the wound? Y / N Date: ………………………………
Page 7 of 12
4. Good practice Points in the incident or investigation process where care and/or practice had an important positive impact and may provide valuable learning opportunities. (E.g. good practice, involvement of the patient, staff openness etc.)
………………………………………………………………………………………………………………………………………………………
…………………………………………………………………………………………………………………………………………………………
5. Care Delivery, Contributory factors, Systems, Recommendations
Care/service delivery Problems (CPD/SDP)
Contributory Factors Systems Recommendations
CDP – is a problem that arises in the process of care. (be precise) SDP – acts or omissions that are identified during the analysis of the service users patient safety incident but are not associated with direct provision of care (be precise)
The fishbone diagram (appendix 2 ) will assist you to identify contributory factors
(e.g. policies and supervision)
2 sorts of recommendations you will be making; (1) To improve existing systems which are not working as well as they might. (2) To implement missing systems
Page 8 of 12
Care/service delivery Problems (CPD/SDP)
Contributory Factors Systems Recommendations
Page 9 of 12
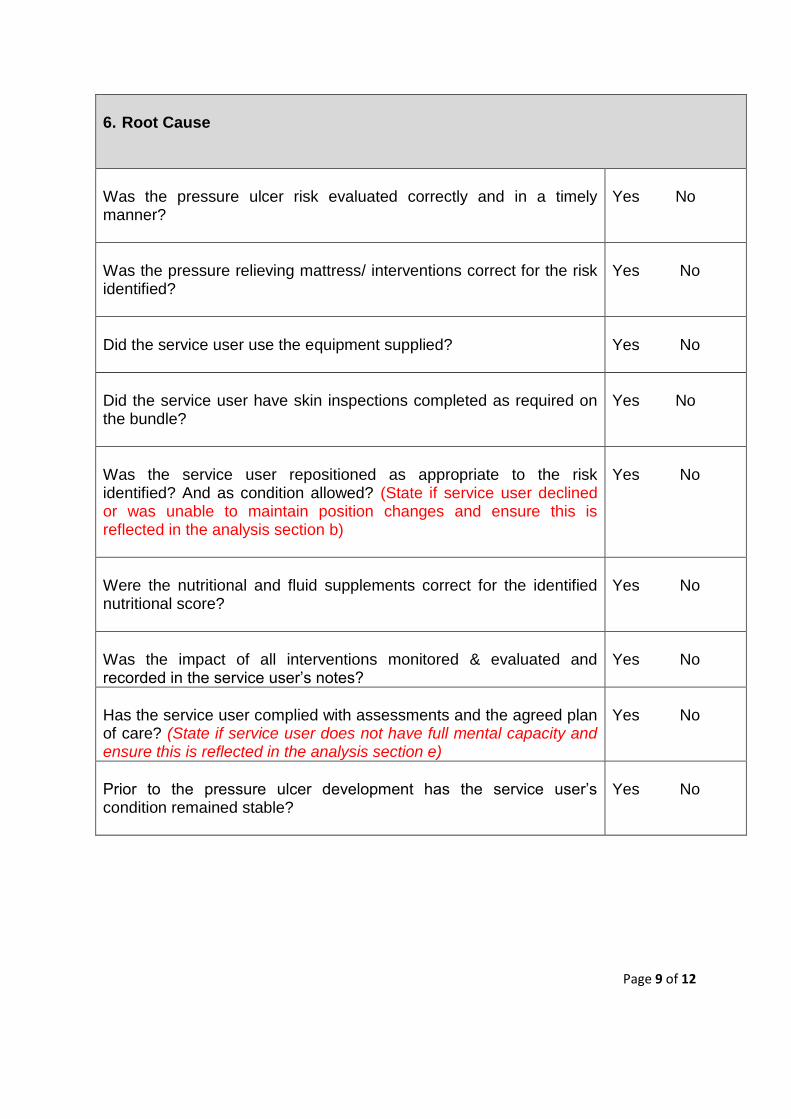
6. Root Cause
Was the pressure ulcer risk evaluated correctly and in a timely manner?
Yes No
Was the pressure relieving mattress/ interventions correct for the risk identified?
Yes No
Did the service user use the equipment supplied?
Yes No
Did the service user have skin inspections completed as required on the bundle?
Yes No
Was the service user repositioned as appropriate to the risk identified? And as condition allowed? (State if service user declined or was unable to maintain position changes and ensure this is reflected in the analysis section b)
Yes No
Were the nutritional and fluid supplements correct for the identified nutritional score?
Yes No
Was the impact of all interventions monitored & evaluated and recorded in the service user’s notes?
Yes No
Has the service user complied with assessments and the agreed plan of care? (State if service user does not have full mental capacity and ensure this is reflected in the analysis section e)
Yes No
Prior to the pressure ulcer development has the service user’s condition remained stable?
Yes No
Page 10 of 12
7. Lessons learnt …………………………………………………………………………………………………
………………………………………………………………………………..…………………
……………………………………………..……………………………………………………
8. Arrangements for shared learning Describe how learning has been or will be shared with staff and other organisations (e.g. through bulletins, newsletters, team meetings, professional networks, reporting, etc.)
…………………………………………………………………………………………………
…………………………………………………………………………………………………
…………………………………………………………………………………………………
9. Appendices
Appendix 1 – Improvement Plan
Appendix 2 – RCA investigation – Fishbone Diagram tool
Developed: April 2015 Next review date: April 2016
Developed by; Quality and Safety Herefordshire Clinical Commissioning Group (HCCG)
Page 11 of 12
Appendix 1 Improvement plan
SIRI/Frameworki number ……………………………………… Incident form number: ………………………………….
Recommendations
Actions required to implement
recommendations
By Whom
By When
Date completed and evidence of
implementation
1
2
3
4
Page 12 of 12
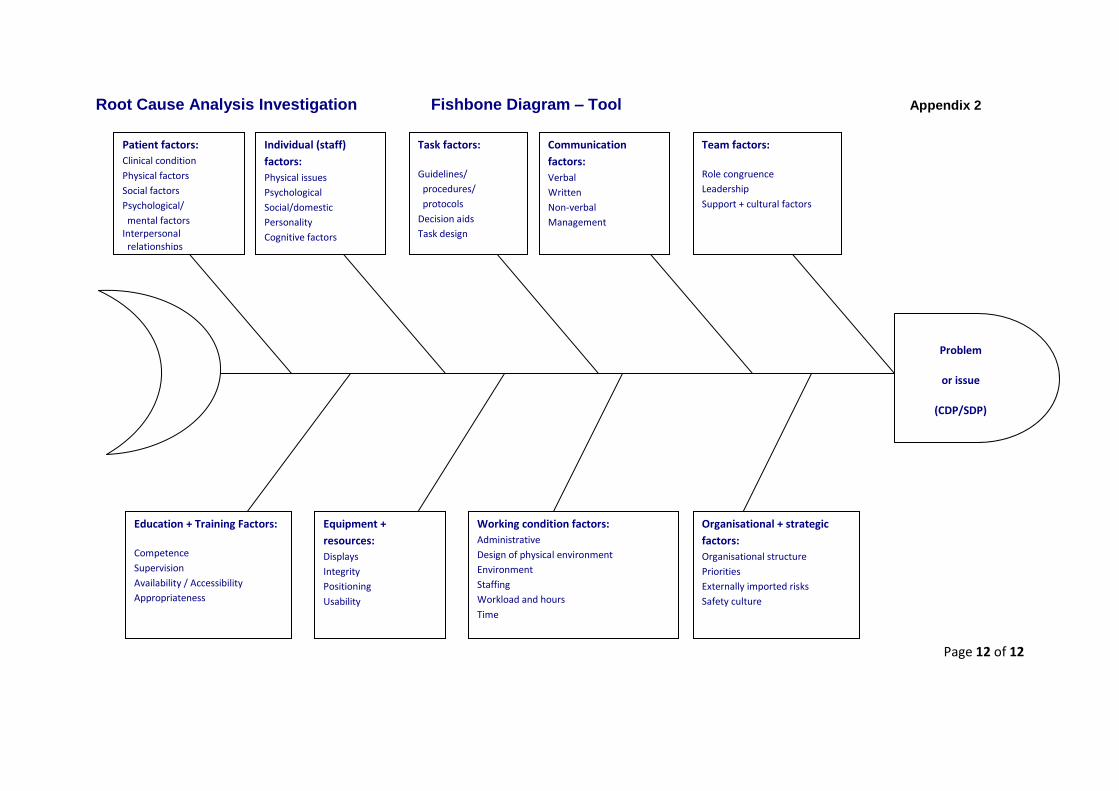
Root Cause Analysis Investigation Fishbone Diagram – Tool Appendix 2
Patient factors:
Clinical condition
Physical factors
Social factors
Psychological/
mental factors Interpersonal relationships
Individual (staff)
factors:
Physical issues
Psychological
Social/domestic
Personality
Cognitive factors
Task factors:
Guidelines/
procedures/
protocols
Decision aids
Task design
Communication
factors:
Verbal
Written
Non-verbal
Management
Team factors:
Role congruence
Leadership
Support + cultural factors
Education + Training Factors:
Competence
Supervision
Availability / Accessibility
Appropriateness
Equipment +
resources:
Displays
Integrity
Positioning
Usability
Working condition factors:
Administrative
Design of physical environment
Environment
Staffing
Workload and hours
Time
Organisational + strategic
factors:
Organisational structure
Priorities
Externally imported risks
Safety culture
Problem
or issue
(CDP/SDP)