roslyn b. mannon md, fasn, fast • under an irb approval, blood and urine were obtained from...
TRANSCRIPT

Pre-implantation Kidney Biopsies as a Predictor for Delayed Graft Function
Roslyn B. Mannon MD, FASN, FAST
Professor of Medicine and SurgeryUniversity of Alabama at Birmingham
Birmingham AL, USA

Conflicts of Interest
• I have no conflicts of interest relevant to this presentation• I will not be discussing the use of off label therapeutics

Outline
• Background on deceased donor organs and kidney transplantation
• What is delayed graft function and why does it matter?• What are the metrics for kidney organ discard?• What are predictors of recipient allograft function?• How can we impact kidney graft utilization?
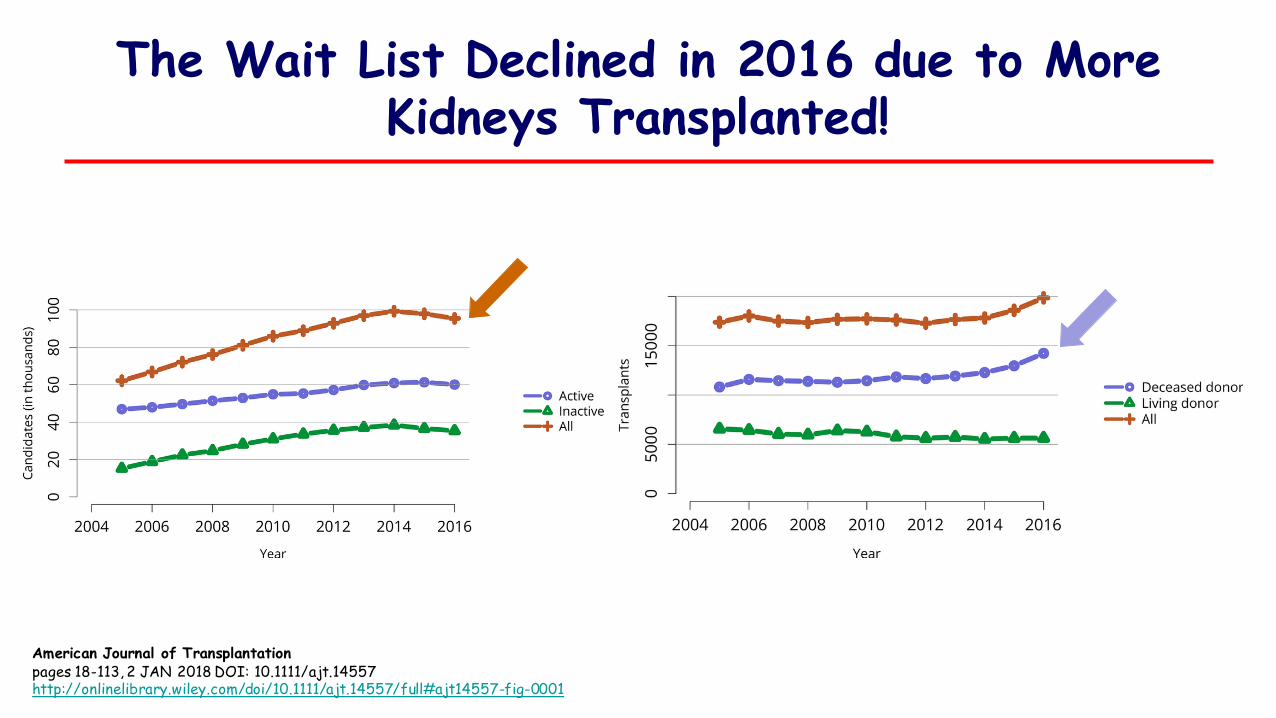
The Wait List Declined in 2016 due to More Kidneys Transplanted!
American Journal of Transplantationpages 18-113, 2 JAN 2018 DOI: 10.1111/ajt.14557http://onlinelibrary.wiley.com/doi/10.1111/ajt.14557/full#ajt14557-fig-0001

American Journal of Transplantationpages 18-113, 2 JAN 2018 DOI: 10.1111/ajt.14557http://onlinelibrary.wiley.com/doi/10.1111/ajt.14557/full#ajt14557-fig-0028
Discard Rates are Still Significant
Other High Discard Groups:• Diabetes• Hypertension• Terminal scr > 1.5
mg/dL• KDPI > 85%

Discard Rates Continue to Rise
• Impact of organ allocation sequence since Dec 2014 leading to more sharing, and longer cold times
• Metrics for patient and graft survival at one year lead to caution in using deceased donor kidneys– It isn’t enough to say that patient survival improved even with a poorly
functioning kidney CT dialysis• Impact of delayed graft function on initial and longer term
outcomes

Risk Factors for Delayed Graft Function
Irish WD. Am Jnl Transplant 2010; 10:2279
Fear of delayed allograft function or need for dialysis post transplantation
• Cost of hospitalization• Complex post management with
dialysis• 41% increase in graft loss at
mean of 3.2y and 38% increase in acute rejection (NDT 2009; 24:1039)
• Less robust kidney function post transplantation

The discard rate for biopsied kidneys remained markedly higher than the rate for non-biopsied kidneys
American Journal of Transplantationpages 18-113, 2 JAN 2018 DOI: 10.1111/ajt.14557http://onlinelibrary.wiley.com/doi/10.1111/ajt.14557/full#ajt14557-fig-0032
~30%

Implantation Biopsy Utility is Disputed
• Retrospective single center review: Poor correlation between first and second biopsies; overlapping percent of gs, limited and inconsistent reporting of IF/TA, arteriolar hyalinosis and ATN). Compared to matched controls and contralateral kidney, 1y graft survival was nearly 80% (Kasiske et al. CJASN 2014; 9:562).
• Multicenter study of procurement biopsies and ATN: DGF more common with ATN on biopsy but no difference in graft failure rates and ATN only found in 17% of biopsies (Hall; CJASN 2017; 9:573)
• Banff Histopathological Consensus Criteria for Pre-Implantation biopsies (Am Jnl Transplant 2017; 17: 140)

What’s Missing? Beyond histology…
• Biochemical, immunological and physiological understanding of brain death and impact on post-transplant function
• Complex interaction of donor characteristics with clinical management of donor, recipient, surgical implantation, post-operative management, and therapeutics
• Call for analysis of discard rate and policies (Kadatz and Gill; CJASN 2018: 13:13)

Goals of UAB Donor Biorepository
• To determine the impact of brain death on donor immune activation, graft immune response and recipient allograft function.
• To assess pre-donation factors including donor management, donor clinical characteristics, and recipient outcomes (when available)
• Assess biological features in discard kidneys

Methods
• Under an IRB approval, blood and urine were obtained from deceased donors after brain death (BDD) and cardiac death (DCD), just prior to organ retrieval and the start of cold preservation.
• Kidney biopsies were obtained immediately after preservation.• As a control, blood and urine were obtained from healthy volunteers
and biopsy tissue from a biospecimen bank at UAB. • Gene expression in kidney biopsies was analyzed by real-time PCR while
serum and urine were analyzed by Luminex™ assay and urine values normalized to urine creatinine.

Donor Demographics and Recipient
Donors (n=34)
Recipients (n=41)
Mean cold ischemia time (CIT; hours) 21 (1->40) ---Mean age (Years) 45 (17-69) 53 (29-72)African American Race 10 (29%) 27 (66%)Male Gender 23 (68%) 26 (63%)KDPI 58 (2-100) ---
34 BDD(68 K)
64 kidneys: Local
4 kidneys: Exported
41 kidneys: Transplanted
23 kidneys: Discarded• Donor age• Poor pump numbers• Organ anatomical damage/defect• Arteriosclerosis• Intimal dissection/surgical cut
68 BDD(136 K)

Gene Expression in BD Donor Kidney Biopsies (n=28)
0.01
0.10
1.00
10.00
100.00
MPO
SOD3 IL4
GZMB
SMAD
7
SMAD
2
PTPR
C
CCL3
ITGA
M
HGF
LTA
CCR2
PRF1
GAPD
H
TNFSF10
TIMP1 C4A
SOD2
TLR1
TLR8 IL8
CD28
TLR2
TNFRSF13B
LTF
BDD only ( ≥ 2-fold vs. Normal kidney)
Relative
mRN
A e
xpre
ssion
↑ - 41 genes upregulated↓ - 9 genes downregulated

Functional Analysis of Gene Expression in BDD Kidney Biopsies (n=28)
1
10
100
Apoptosis/Necrosis
0.01
0.10
1.00
10.00
100.00
HAV
CR1
HMOX1 LTF
MPO
SOD3
SOD2
TLR1
TLR2
TLR4
TLR5
TLR8
Ischemiareperfusion
0.1
1.0
10.0
Cytokines/Chemokines
1
10
100
C3 C4A CLU
Endothelialinjury
1.0
10.0
ITGAL ITGAM
ImmuneActivators
0.1
1.0
10.0
COL1A1 HGF
IGF1
MMP7
SMAD
2SM
AD7
TIMP1
Matrix/Fibrosis
Relative
mRN
A e
xpre
ssion
( ≥2
-fold
chan
ge v
s. H
ealthy
con
trol)

Alteration of Cytokines/Chemokines in Serum and Urine BD Donor Detected by
Luminex
Healthy control, n=11
BDD, n=22(serum), 24(Urine)
Seru
m c
ytok
ines
(p
g/ml)
0
20
40
60
IL-15
Urine
cyt
okine
(p
g/mg
Ucr
)
0
100
200
300
400
IL-6 IL-10 IL-15 EGF
*
*
* *
Serum Urine
*

Urine MCP-1 Expression in BD Donor Correlates with Recipient Renal Function
Cyto
kine
(pg
/ml) Serum MCP-1
0
500
1000
1500
Healthy control (n=11)
DBD (n=22)
Cyto
kine
(pg
/mg
Ucr
)*
Urine MCP-1
0
2000
4000
6000
Healthy control (n=11)
DBD (n=24)0
20406080
100
0 2000 4000 6000 8000
Rho: -0.751, p=0.008
Recipien
tGF
R at
6-m
onth
MCP-1 (pg/mg Ucr)
“Low” “Medium” “High”
Donors
Urine
control discarded0
500
1000
1500
2000
0500
1000150020002500
control discarded0
5001000150020002500
control non-DGF DGF
MCP
-1
(pg/
ml/m
g/m
lCr) *
MCP
-1 (p
g/m
l)0
500
1000
1500
2000
control non-DGF DGF
NS
Serum
Control
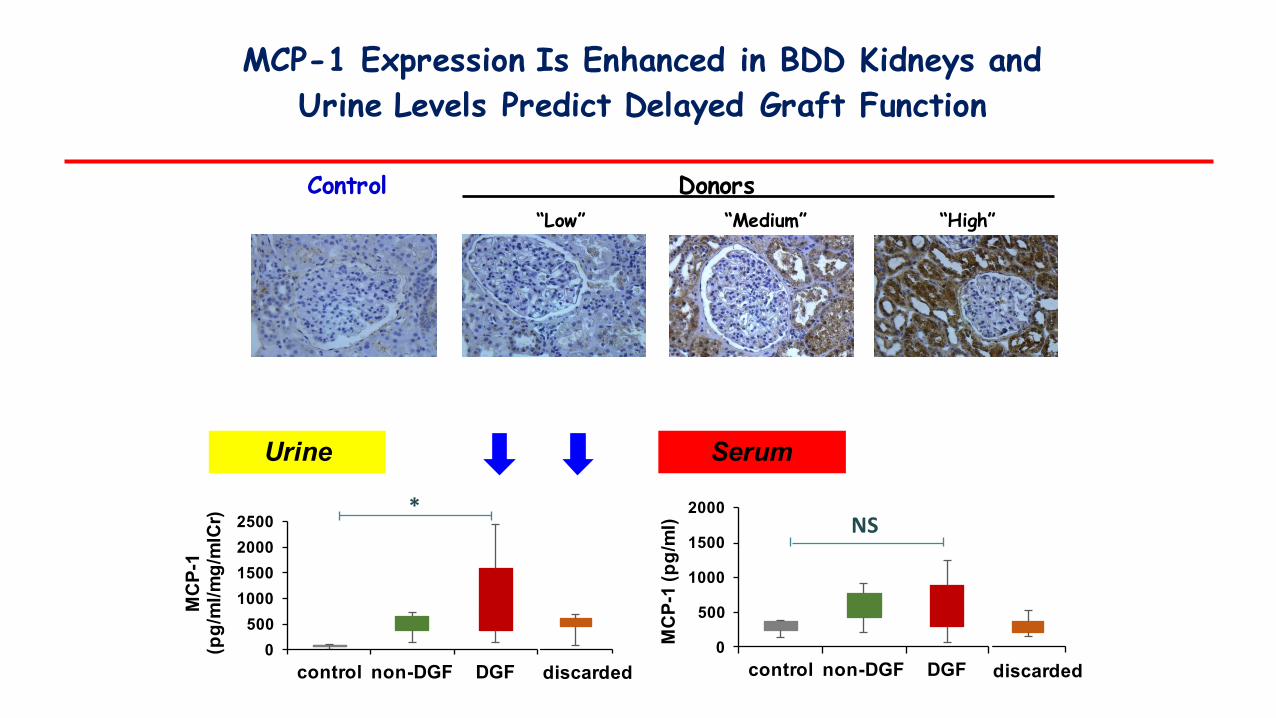
MCP-1 Expression Is Enhanced in BDD Kidneys and Urine Levels Predict Delayed Graft Function

Urine Expression of Neutrophil Gelatinase-Associated Lipocalin (NGAL) is Elevated in BD Donors
NG
AL
(ng/
ml/m
g/m
lCr)
Urine
*
0
100
200
300
400
non-DGF DGFcontrol discarded
*
NG
AL
(ng/
ml)
Serum
0
200
400
600
non-DGF DGFcontrol discarded
** *
*

IL-1
8 (p
g/m
l/mg/
mlC
r)
IL-18 is Increased in Urine and Serum of DGF and Discarded Donors
IL-1
8 (p
g/m
l)
Urine
Serum
0500
1000150020002500
0
500
1000
1500
2000
2500
non-DGF DGFcontrol discarded
non-DGF DGFcontrol discarded
*
*
*
*

Area Under the CurveTest Result Variable(s): urine_IL18
AreaStd.
ErroraAsymptotic
Sig.b
Asymptotic 95% Confidence IntervalLower Bound
Upper Bound
.750 .111 .059 .532 .968a. Under the nonparametric assumptionb. Null hypothesis: true area = 0.5
uIL-018 uNGAL
Area Under the CurveTest Result Variable(s): urine_NGAL
AreaStd.
ErroraAsymptoti
c Sig.b
Asymptotic 95% Confidence IntervalLower Bound
Upper Bound
.692 .111 .121 .475 .910a. Under the nonparametric assumptionb. Null hypothesis: true area = 0.5
ROC of Best Urine Markers

High Mobility Group Box 1 (HMGB1) - Introduction
Damage Associated Molecular Pattern proteins (DAMPs)
High Mobility group box 1 (HMGB1)
Hypoxia, ischemia, trauma
Inflammation, organ injury
200x
200x
Control
CsA

HMGB1 Release is Detected in the Urine and Serum of Deceased BD Donors
0
1
2
3
4
non-DGF DGF
URINE
HM
GB
1 ur
ine
(fold
non
-DG
F)
non-DGF DGF0
1
2
3
SERUM
HM
GB
1 se
rum
(fold
non
-DG
F)
non-DGF DGF
non-DGF DGF
**

0
1000
2000
3000
4000HM
GB1
urin
e(p
g/m
l/mg/
mlC
r)
non-DGF DGFcontrol discarded
**
Quantification of HMGB1 in Urine of Brain Dead Donors: correlation with DGF and Discard

DGF Discardednon-DGF
HMGB1 Translocation is Detected in Kidneys from Brain Dead Donors

HMGB1 Expression in Recipient’s Urine before and after Transplant
Recipient 2
HMGB1(urine)
Pre-transplant
Post-transplant (weeks)
Recipient 1 Recipient 4Recipient 3
+ + + +
40 12 40 12 40 12 40 12 CTL
CTL

• BD donors demonstrate activation of inflammatory pathways that are frequently systemic.
• Among several AKI biomarkers tested, urine MCP-1 and NGAL, as well as serum and urine IL-18, were significantly elevated in donors with DGF or that were later discarded.
• Serum and urine TNFα levels were not discriminatory among donor groups.
• The extent of HMGB1 flux in the donors could be a biologic marker of kidney injury that predicts donor-related DGF and can be an indicator of graft function in Recipients.
Summary

Conclusion
Specific biomarkers to predict kidney injury in recipients following transplantation would provide important information for clinical management and further enhance organ utilization.

Acknowledgments
• UAB Laboratory– Anna Zmijewska– Jianguo Chen – Jarek Zmijewska– Michael Seifert– Miriam Bernard– John Murphy
• Extramural Colleagues– Arthur Matas and the
DeKAF Study Group– CTOT-10/12/15/19/21
Study Groups
• UAB Surgery– Jayme Locke– Carlton Young– Michael Hanaway– Joseph Tector– Jared White– Devin Eckhoff– Stephen Gray


MCP-1 Expression Is Upregulated in the Kidney of BD Donors
Normal“Low” “Medium” “High”
BD Donors
Cytosolic Interstitial Luminal

Summary
• In brain dead donor kidneys, prior to reperfusion and preservation, there is an enhanced expression of genes associated with apoptosis, inflammation, ischemia, and endothelial injury, and upregulation of molecules associated with fibrogenesis.
• Serum levels of IL-6, IL-10, IL-15, and EGF and Urine IL-15 were significantly increased in BD donors compared to normal healthy individuals.
• Urine levels of MCP-1 were significantly elevated compared to normal healthy individuals, but serum levels were not.
• There was a strong negative association between donor urine MCP1 and recipient eGFR at 6months.
• Immunohistochemical staining demonstrated that MCP-1 was enhanced, predominantly expressed in renal tubular epithelial cells, greater in the cortex than medulla.

Conclusions
• BD donors demonstrate activation of inflammatory pathways that are frequently systemic. In the case of MCP-1, localized production in the kidney is enhanced following BD. Further investigation into this pathway may shed light on innate immune activation in the allograft.
• Donor urinary MCP-1 may be a useful noninvasive marker for screening donors and predicting graft outcomes in kidney transplant patients.