ruchi thanawala michael radtke stephen levinson...ruchi thanawala michael radtke stephen levinson...
TRANSCRIPT
Ruchi Thanawala Michael Radtke Stephen Levinson
Readmissions L i t e r a c y

• Discussion of Preventable CHF Readmissions o Magnitude of Problem o Rationale for literacy-focused intervention o Consideration of successful programs to reduce
readmissions o Emulate LEAN-based approach
• Discussion of Impact of Health Literacy on Health Outcomes and Readmissions
• Demonstrate Value of Educational Interventions to Improve Outcomes--Cheaply
• Propose a Literacy Intervention to Impact Readmissions
Agenda

Hospital Readmissions-Magnitude of Problem
1. 1984 22% 60 day readmission rate • Accounted for 24% of Medicare expenditures
2. 2007 MEDPAC 17.6% 30 day readmissions • 76.5 % of readmissions flagged as preventable
3. 2009 19.6% 30 day readmission rate • 56.1% 1 year readmission rate
1. Anderson et al (1984). Hospital Readmissions in the Medicare Population. NEJM 311 2. Medical Payment Advisory Commission Report. 2007 3. Jencks et al (2009). Rehospitalizations Among Patients in the Medicare Fee-
for-Service Program. NEJM 360
CHF Readmissions • 26.9% 30 day readmission rate • 7.6% of all rehospitalizations
Jencks, S. et al (2009) Rehospitalizations among Patients in the Medicare Fee-for Service Program. NEJM 360: 1418-28

% Avoidable Readmissions
Range: 5-79% Median: 27.1%
Van Walraven et al. (2011) Proportion of Readmissions Deemed Avoidable: A Systematic Review. CMAJ 391-402
Literacy Intervention to Reduce CHF Readmissions
Rationale Ethical Imperative • In Line with Hospital Mission • Patient-Centered • Equitable • Effective
Intervention will Improve Outcomes • Improved Health Outcomes • Reduced Hospital Readmissions • Improved Hospital Finances
External Forces
What’s Driving Transitional Care Interventions?
Hospital Readmissions Reduction Program • Reduces Payments for “excess” risk-adjusted
admissions for CHF, MI, and Pneumonia ! 1% in 2013, 2% in 2014, 3% in 2015…
• Public Reporting of 30 Day Readmission Rates on Hospital Compare
Value Based Purchasing • CHF Discharge Instructions

NQF Endorsed Readmission Performance Measures • CHF (0330) • MI (0505) • Pneumonia (0506) • All Cause (1789)
Payment Bundling Finances of Admission and Readmission
What’s Driving Transitional Care Interventions?
Financial Considerations • $10,900 Average Cost to Treat CHF DRG 291* • $8,667 DRG Payment for DRG 291**
**CMS 2011 Final Rule Data
*Healthcare Cost and Utilization Project 2011-AHRQ
$2,233 Payment Gap

Literacy-Based Interventions Proven to Reduce Readmissions
*15
*38
PPCSM Perfecting Patient Care
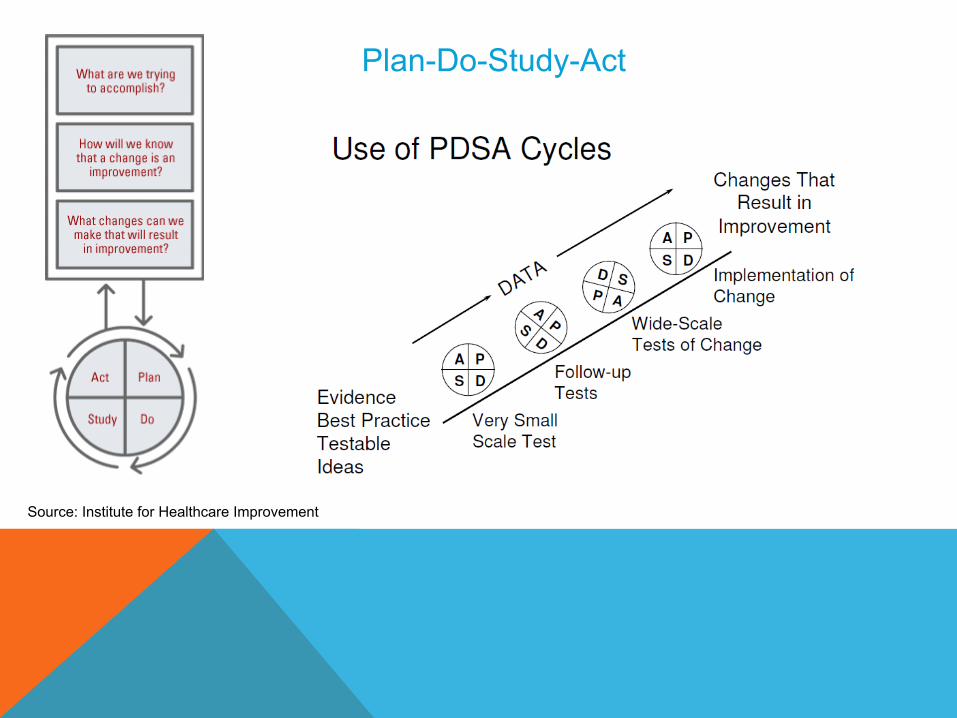
Plan-Do-Study-Act
Source: Institute for Healthcare Improvement
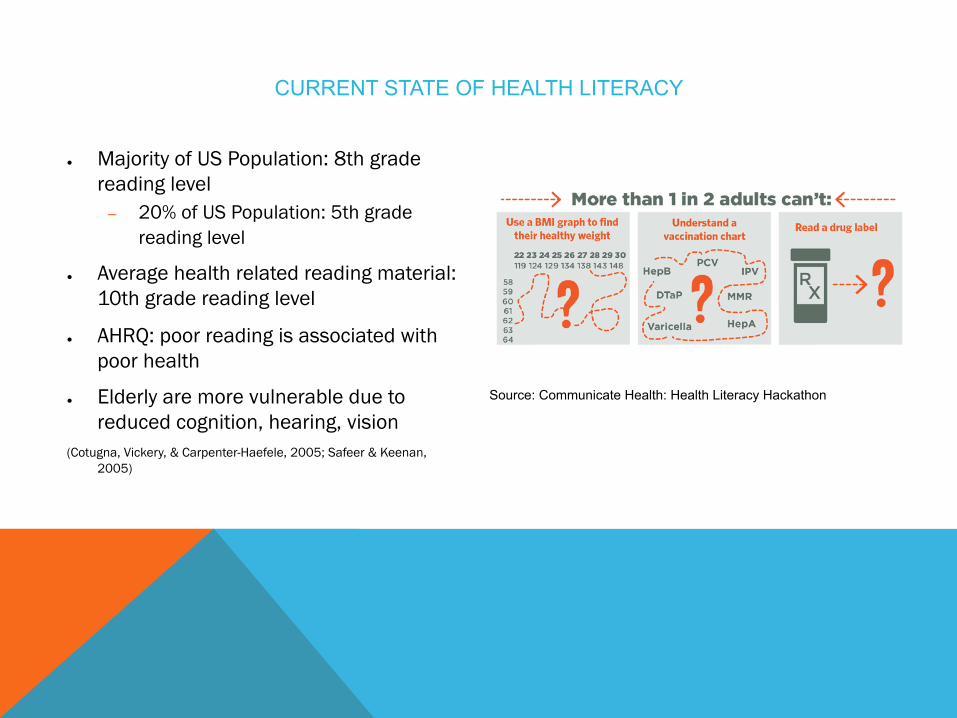
CURRENT STATE OF HEALTH LITERACY
● Majority of US Population: 8th grade reading level
– 20% of US Population: 5th grade reading level
● Average health related reading material: 10th grade reading level
● AHRQ: poor reading is associated with poor health
● Elderly are more vulnerable due to reduced cognition, hearing, vision
(Cotugna, Vickery, & Carpenter-Haefele, 2005; Safeer & Keenan, 2005)
Source: Communicate Health: Health Literacy Hackathon
KEY QUESTIONS
• Does education matter? • How do we make it cost effective?
DOES EDUCATION HELP? • Data support education as a strategy to reduce
admissions (Krumholz 2002) ! Patients given information on CHF in general, medications, lifestyle
effects, recognizing warnings signs, etc. ! Initial phase used experienced RN’s to teach, almost half of patients
had home follow-up ! Second phase included telemonitoring via phone ! Primary endpoint was death or readmission
• Saw lower endpoint rates in intervention group (56.8%) vs. control group (81.8%) ! Admissions in the 12 months after discharge were decreased by
39% ! 193 days was median time after discharge before death or
readmission in intervention group, 126 days for controls.
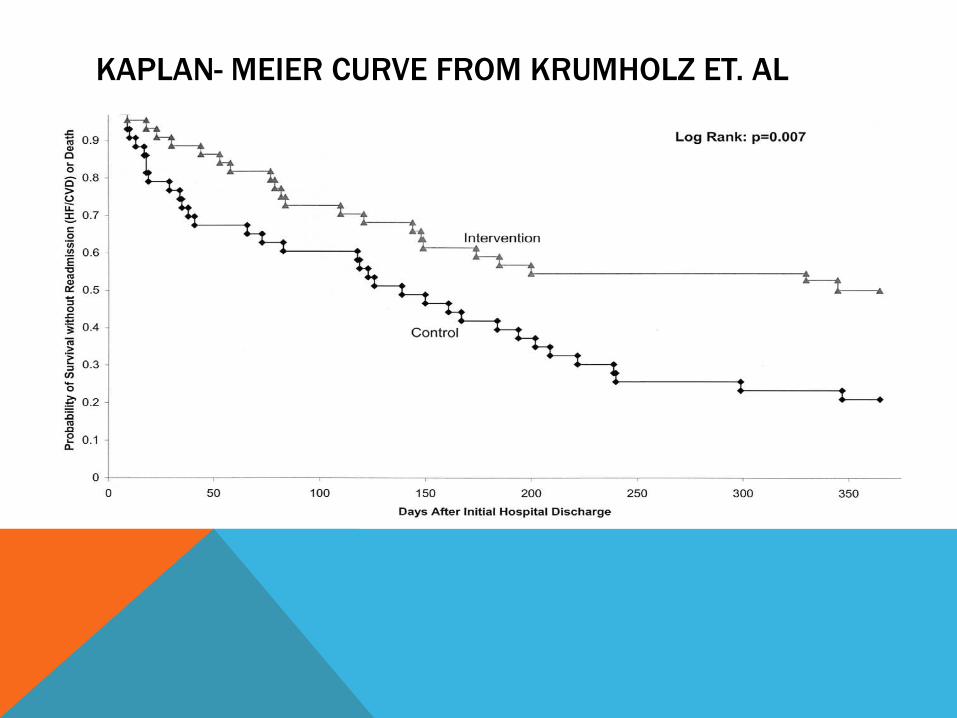
KAPLAN- MEIER CURVE FROM KRUMHOLZ ET. AL
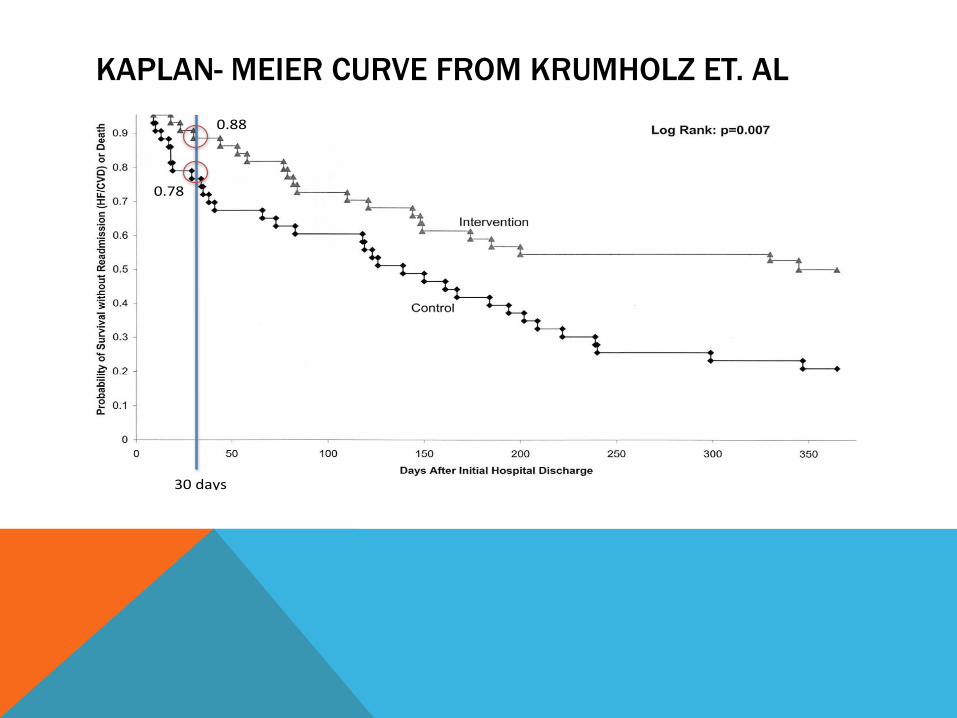
KAPLAN- MEIER CURVE FROM KRUMHOLZ ET. AL
30#days#
0.88#
0.78#
ADDITIONAL SUPPORT FOR EDUCATION IMPACT ON READMISSIONS
• Review&by&Vreeland&et.&al&! Study&by&Harrison&showed&decreased&readmissions&in&within&12&weeks&(31%&with&interven?on,&23%&without)&
! Small&survey&showed&pa?ents&want&informa?on&from&healthcare&professionals&as&well&as&other&pa?ents.&
! Same&survey&also&showed&desire&for&reDretrieval&of&educa?onal&materials.&! Evidence&that&mul?media&improves&various&endpoints&related&to&risks&of&readmission&(eg.&Need&for&diure?cs),&but¬&a&clear&direct&impact&on&readmissions&&
! Other&studies&using&video&showed&no&change&in&readmission&rates.&&• GwadryDSridhar&et.&al.&found&general&trend&towards&decreased&
readmissions&when&pa?ents&had&educa?on&around&discharge&• Simple&tac?c&of&using&cards&to&determine&top&concerns&of&the&pa?ent&
guided&educa?onal&interven?ons&in&one&study&(Luniewski&1999)&

IS IT COST EFFECTIVE? • From&Krumholz&!
! total&cost&of&this&educa?onal&strategy&was&$530&per&pa?ent&
&! Factoring&in&cost&of&readmissions,&this&represented&&
!!!!!$6,985!saved!per!pa/ent!!!
• May¬&even&need&to&pay&someone&to&do&it.&&
COST EFFECTIVE - VOLUNTEERS
• Trained volunteers can provide the education • Sales et. al showed decreased readmissions
when patients had education diet and medications in a 591 bed hospital
• Volunteers&were&preDmed&students&at&local&university,&had&several&hours&of&instruc?on&
• Pa?ents&also&had&followDup&phone&calls&with&scripted&ques?ons&
• 30Dday&readmissions&were&7%&in&interven?on&group,&19%&in&the&control&group&(NNT&of&8)&
KEY&TAKEDAWAY&POINTS&
• Educa?onal&interven?on&has&been&shown&to&decrease&the&risk&of&readmission&for&CHF&
• FollowDup&monitoring&may&be&a&component&of&the&effect&
• NonDprofessional&and&uncompensated&volunteers&may&provide&the&interven?on&effec?vely,&thereby&avoiding&the&need&to&divert&clinical&staff&?me.&&
PROPOSED HEALTH LITERACY INTERVENTION
In our 500-bed community, teaching hospital, we would like to: ● Target: Patients admitted with CHF or complications stemming from CHF
● Approx. 760 CHF admissions/year
● Assess literacy level: During admission or in pre-hospital setting (affiliated ambulatory care setting)
– Score stored in patient's EHR and made part of medical history
● Provide literacy level appropriate content: at discharge and in patient portal
● Assess patient comprehension post discharge: structured questions via automated phone call and patient portal
– First contact within 24-48 hours after discharge – Continue weekly until PCP follow-up
PROPOSED HEALTH LITERACY INTERVENTION
In our 500-bed community, teaching hospital, we would like to: ● Target: Patients admitted with CHF or complications stemming from CHF
● Approx. 760 CHF admissions/year
● Assess literacy level: During admission or in pre-hospital setting (affiliated ambulatory care setting)
– Score stored in patient's EHR and made part of medical history
● Provide literacy level appropriate content: at discharge and in patient portal
● Assess patient comprehension post discharge: structured questions via automated phone call and patient portal
– First contact within 24-48 hours after discharge – Continue weekly until PCP follow-up
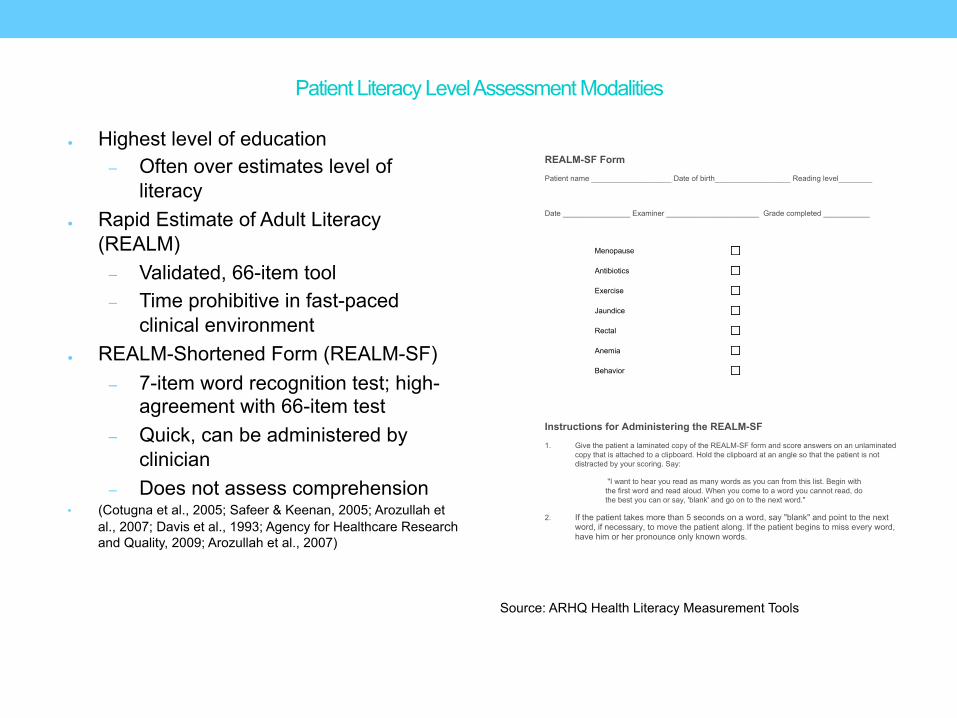
Patient Literacy Level Assessment Modalities
● Highest level of education – Often over estimates level of
literacy ● Rapid Estimate of Adult Literacy
(REALM) – Validated, 66-item tool – Time prohibitive in fast-paced
clinical environment ● REALM-Shortened Form (REALM-SF)
– 7-item word recognition test; high-agreement with 66-item test
– Quick, can be administered by clinician
– Does not assess comprehension • (Cotugna et al., 2005; Safeer & Keenan, 2005; Arozullah et
al., 2007; Davis et al., 1993; Agency for Healthcare Research and Quality, 2009; Arozullah et al., 2007)
Source: ARHQ Health Literacy Measurement Tools
REALM-SF Form
Patient name ___________________ Date of birth__________________ Reading level________
Date ________________ Examiner ______________________ Grade completed ___________
Menopause
Antibiotics
Exercise
Jaundice
Rectal
Anemia
Behavior
Instructions for Administering the REALM-SF
1. Give the patient a laminated copy of the REALM-SF form and score answers on an unlaminated copy that is attached to a clipboard. Hold the clipboard at an angle so that the patient is not distracted by your scoring. Say:
"I want to hear you read as many words as you can from this list. Begin with the first word and read aloud. When you come to a word you cannot read, do the best you can or say, 'blank' and go on to the next word."
2. If the patient takes more than 5 seconds on a word, say "blank" and point to the next word, if necessary, to move the patient along. If the patient begins to miss every word, have him or her pronounce only known words.

Patient Literacy Level Assessment Modalities
Health LiTT
– Created at Feinberg SOM and Mayo Clinic
– Assess comprehension across prose, document, and quantitative literacy
– Composite score
– Self-administered
● Embed in patient portal
Source: (Hahn et al 2011)
PROPOSED HEALTH LITERACY INTERVENTION
In our 500-bed community, teaching hospital, we would like to: ● Target: Patients admitted with CHF or complications stemming from CHF
● Approx. 760 CHF admissions/year
● Assess literacy level: During admission or in pre-hospital setting (affiliated ambulatory care setting)
– Score stored in patient's EHR and made part of medical history
● Provide literacy level appropriate content: at discharge and in patient portal ● Assess patient comprehension post discharge: structured questions via automated
phone call and patient portal – First contact within 24-48 hours after discharge – Continue weekly until PCP follow-up
Workflow from In-hospital setting to post-discharge
In-hospital
1. Provider/Nurse selects focus (general disease mgmt, medications) and form (paper, audio) of content
2. Literacy score for each patient used to determine appropriate content
3. Option to print content (text) and embed in patient portal
4. EHR: Record of material assigned to patient maintained
Post-Discharge
Structured questions in patient portal and/or automated call service; patient preference
Questions derived from those created by SME team
Use of answers: ! Identify changes in health ! Areas of confusion in CHF
management for patient ! Targets for improved education

PROPOSED HEALTH LITERACY INTERVENTION
In our 500-bed community, teaching hospital, we would like to: ● Target: Patients admitted with CHF or complications stemming from CHF
● Approx. 760 CHF admissions/year
● Assess literacy level: During admission or in pre-hospital setting (affiliated ambulatory care setting)
– Score stored in patient's EHR and made part of medical history
● Provide literacy level appropriate content: at discharge and in patient portal
● Assess patient comprehension post discharge: structured questions via automated phone call and patient portal
– First contact within 24-48 hours after discharge – Continue weekly until PCP follow-up

Workflow from In-hospital setting to post-discharge
Database
1. Provider/Nurse selects focus (general disease mgmt, medications) and form (paper, audio) of content
2. Literacy score for each patient used to determine appropriate content
3. Option to print content (text) and embed in patient portal
4. EHR: Record of material assigned to patient maintained
Post-Discharge
Structured questions in patient portal and/or automated call service; patient preference
Questions derived from those created by SME team
Use of answers: ! Identify changes in health ! Areas of confusion in CHF
management for patient ! Targets for improved education
(Source: Sales et al, 2013)

Performance Measures (Off the Shelf)
Process Measures 1. HF pts educated on management—NQMC 3984, NQF 0649 2. Care Transition--% patients receiving transition record at discharge— NQMC 5475, NQF 0647
Outcome Measures 1. 30-day all-cause HF readmission rate—NQMC 8845 2. HCAHPS—Question 19,20 3. CCAT—Score on Communication Climate Assessment Toolkit—NQMC 7555, NQF 1896
Customized Performance Measures
Process • % CHF patients receiving pre-discharge literacy assessment • % discharged CHF patients receiving literacy-adjusted CHF education
Outcome
• % CHF readmission rate • % low literacy CHF patients weighing themselves daily post-hospital discharge • % of low literacy CHF patients exceeding a specified level on a validated
knowledge assessment (e.g. BOOST DKAT or Dewalt Questionnaire) • % discharged low literacy CHF patients who correctly report on post-
discharge phone call their hospital diagnosis (or warning symptoms, or how to take their medications, or dietary restriction)
• % of discharged low literacy CHF patients “highly satisfied” with their educational intervention

Proposed Timeline

Methodology: 0-5 Months
Project Manager/Education Committee
Content Manager (ongoing)
● Medical Health Librarian
– Identify content; send to SME for review; manage periodic review of content; upload content
● Content Sources
– Internet Sources (UpToDate, NCQA)
– Vendors (Healthwise)
– In-house development
Review and “Vet” Content (ongoing)
● Subject Matter Expert Team
– (Cardiologists, Nurse Educator, Pharmacist, PCP, Literacy Expert, Ancillary Care Providers)
– Review content identified by Librarian
– Develop content
– Develop 2-4 questions to assess comprehension, identify responses showing changes in condition (non-life threatening, life-threatening)
Methodology: 5-14 months
Define literacy assessment tools
• Months 5-8
Score Content on Reading Level (ongoing, start at 5 months)
● Written, Audio, and Video Content
– Flesch-Kincaid Readability Ease/Grade level
● Images in content
– SME team assessment of literacy level
Database build and continually update
• Ongoing, start at months 8-10
– Literacy score stored in EHR accessible database
– Database accessible through EHR
User interface development
• Months 10-14
• Clinician-facing interface
• Patient portal interface
• Medical librarian and SME interface for content uploading and editing
IT Resource Requirements Infrastructure/IT Requirements
● Database Architect
● User Interface developer
– Develop web interface to upload content to database, download content for patients, embed content in patient portal
Data Storage/Server Needs Estimate of 1 – 2 GB storage for CHF content
● 100 text files (average file size 1 – 3 MB)
● 100 audio files (average file size 2 – 3 MB)
● 25 video files video file ( average file size 10 – 30 MB)
Source: Univ of Missouri Engineering
Source: www.iconarchive.com
Final Budget 1. Medical Health Librarian (0.5 FTE): $30,000 2. SME members (10/hrs/week/individual): $12,500/individual;
estimate 5 members 3. Database architect (0.5 FTE): $43,750 4. User interface developer (0.5 FTE): $28,600 5. Data storage/server: minimal cost - $10/month 6. Automated call back service: $95/month for 500 calls 7. Content:
1. In-house: included in SME member cost 2. Vendor: use content available under existing licenses (UpToDate) 3. Future: consider targeted patient education vendors
8. Total: $186,069 for 18-month implementation 9. Total: $181,760/year to run program for CHF
Source: Simplyhired.com, Indeed.com, aws.amazon.com, www.call-em-all.com/pricing

Potential Yearly Hospital Cost Savings*
• $138,445 for 62 (30%) fewer Medicare CHF Admissions • $2,410,834 for Elimination of .19% HRRP Penalty
*Based on: ! 500 Beds ! 760 Yearly Medicare CHF Readmissions ! 206 Medicare Readmissions for CHF ! $2,223 Revenue Gap per Admission ! Yearly Medicare Revenue of $1,268,859,856 ! .19% HRRP Penalty in Prior Year
Stretch Goals
Target Goal (Year 1)
• $46,148 for 21 (10%) fewer Medicare CHF Admissions • $120,542 Reduction in .19% HRRP Penalty

Rationale for Intervention • Ethical • Improved Outcomes—Performance Measures
2 Big Problems • CHF Readmissions • Health Literacy
Literacy Intervention for CHF Transitional Care • Assess Patient Literacy • Provide Literacy-Tailored Educational Content
! Maintain Database of Content • Assess Patient Comprehension
Educational Interventions Efficacious for CHF
Recap
Implementation Timeline and Finances

References
1. Anderson, G. F., & Steinberg, E. P. (1984). Hospital Readmissions in the Medicare Population.
New England Journal of Medicine, 311(21), 1349–1353. doi:10.1056/NEJM198411223112105
2. Anderson, G., & Steinberg, E. (1984). Hospital readmissions in the Medicare population. The
New England Journal of Medicine, 311(21), 1349–1353. doi:10.1056/NEJM198411223112105
3. CAHPS 2.0 Adult Core Questionnaire - HCAHPS V8.0 Appendix A - HCAHPS Mail Survey
Materials (English) March 2013.pdf. (n.d.). Retrieved from
http://www.hcahpsonline.org/files/HCAHPS%20V8.0%20Appendix%20A%20-
%20HCAHPS%20Mail%20Survey%20Materials%20(English)%20March%202013.pdf
4. Coleman, E. A., Smith, J. D., Frank, J. C., Min, S.-J., Parry, C., & Kramer, A. M. (2004).
Preparing patients and caregivers to participate in care delivered across settings: the Care
Transitions Intervention. Journal of the American Geriatrics Society, 52(11), 1817–1825.
doi:10.1111/j.1532-5415.2004.52504.x
5. Condel, J. L., Sharbaugh, D. T., & Raab, S. S. (2004). Error-free pathology: applying lean
production methods to anatomic pathology. Clinics in Laboratory Medicine, 24(4), 865–899.
doi:10.1016/j.cll.2004.07.001
6. Costs for Hospital Stays in the United States, 2011 - Statistical Brief #168. (n.d.). Retrieved
February 19, 2014, from http://www.hcup-us.ahrq.gov/reports/statbriefs/sb168-Hospital-Costs-
United-States-2011.jsp
7. Gorenflo, G., & Moran, J. W. (2010, April). The ABCs of PDCA. Retrieved from
http://www.phf.org/resourcestools/Pages/The_ABCs_of_PDCA.aspx
8. Gwadry-Sridhar, Femida H., Virginia Flintoft, Douglas S. Lee, Hui Lee, and Gordon H. Guyatt.
“A Systematic Review and Meta-Analysis of Studies Comparing Readmission Rates and
Mortality Rates in Patients with Heart Failure.” Archives of Internal Medicine 164, no. 21
(2004): 2315.

9. Harrison MB, Browne GB, Roberts J, Tugwell P, Gafni A, Graham ID. Quality of life of
individuals with heart failure: a randomized trial of the effectiveness of two models of hospital-
to-home transition. Med Care. 2002;40:271-282.
10. Health Literacy Universal Precautions Toolkit - healthliteracytoolkit.pdf. (n.d.). Retrieved from
http://www.ahrq.gov/professionals/quality-patient-safety/quality-resources/tools/literacy-
toolkit/healthliteracytoolkit.pdf
11. HealthAffairs. (2013, November 12). Medicare Hospital Readmission Reduction Program.
Robert Wood Johnson Foundation. Retrieved from
http://healthaffairs.org/healthpolicybriefs/brief_pdfs/healthpolicybrief_102.pdf
12. Jack, B., Paasche-Orlow, M., Mitchell, S., Forsythe, Shaula, & Martin, J. (2013, March 5). Re-
Engineered Discharge (RED) Toolkit. Text. Retrieved February 19, 2014, from
http://www.ahrq.gov/professionals/systems/hospital/red/toolkit/index.html
13. Jencks, S. F., Williams, M. V., & Coleman, E. A. (2009). Rehospitalizations among Patients in
the Medicare Fee-for-Service Program. New England Journal of Medicine, 360(14), 1418–1428.
doi:10.1056/NEJMsa0803563
14. June 2007 Report to the Congress: Promoting Greater Efficiency in Medicare -
jun07_entirereport.pdf. (n.d.). Retrieved from
http://www.medpac.gov/documents/jun07_entirereport.pdf
15. Kansagara D, Englander H, Salanitro A, & et al. (2011). Risk prediction models for hospital
readmission: A systematic review. JAMA, 306(15), 1688–1698. doi:10.1001/jama.2011.1515
16. Krumholz, Harlan M, Joan Amatruda, Grace L Smith, Jennifer A Mattera, Sarah A Roumanis,
Martha J Radford, Paula Crombie, and Viola Vaccarino. “Randomized Trial of an Education
and Support Intervention to Preventreadmission of Patients with Heart Failure.” Journal of the
American College of Cardiology 39, no. 1 (January 2, 2002): 83–89. doi:10.1016/S0735-

1097(01)01699-0.
17. Learning to Lead at Toyota. (n.d.). Harvard Business Review. Retrieved February 27, 2014,
from http://hbr.org/2004/05/learning-to-lead-at-toyota/ar/1
18. Luniewski M, Reigle J, White B. Card sort: an assessment tool for the educational needs of
patients with heart failure. Am J Crit Care. 1999;8:297-302
19. Medicare, C. for, Baltimore, M. S. 7500 S. B., & Usa, M. (2012, March 28). CMS-DRG
10/1/10 to 9/30/11. Retrieved February 19, 2014, from
http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Acute-
Inpatient-Files-for-Download-Items/CMS1255464.html
20. Medicare, C. for, Baltimore, M. S. 7500 S. B., & Usa, M. (2013a, August 2). Readmissions-
Reduction-Program. Retrieved February 19, 2014, from
http://www.cms.gov/Medicare/Medicare-Fee-for-Service-
Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html
21. Medicare, C. for, Baltimore, M. S. 7500 S. B., & Usa, M. (2013b, November 14). Hospital
Value-Based Purchasing. Retrieved February 19, 2014, from
http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/hospital-
value-based-purchasing/index.html?redirect=/hospital-value-based-purchasing
22. Medicare Hospital Readmissions Reduction Program. (n.d.). Health Affairs - Health Policy
Briefs. Retrieved February 19, 2014, from
http://www.healthaffairs.org/healthpolicybriefs/brief.php?brief_id=102
23. Methodology: How Value Based Purchasing Payments Are Calculated - Kaiser Health News.
(n.d.). Retrieved February 19, 2014, from
http://www.kaiserhealthnews.org/stories/2013/november/14/value-based-purchasing-medicare-
methodology.aspx

24. Moen, R., & Norman, C. (2010, November). Circling Back. Retrieved from
http://www.apiweb.org/circling-back.pdf
25. National Quality Measures Clearinghouse. Acute myocardial infarction (AMI): hospital 30-day,
all-cause, unplanned risk-standardized readmission rate (RSRR) following AMI hospitalization.
(n.d.). Retrieved from http://www.qualitymeasures.ahrq.gov/content.aspx?id=46498
26. National Quality Measures Clearinghouse. Care transitions: percentage of patients, regardless of
age, discharged from an inpatient facility to home or any other site of care, or their caregiver(s),
who received a transition record (and with whom a review of all included information was
documented) at the time of discharge including, at a minimum, all of the specified elements.
(n.d.). Retrieved from http://www.qualitymeasures.ahrq.gov/content.aspx?id=28140
27. National Quality Measures Clearinghouse. Communication climate: mean scale score for the
“Health Literacy” items on the Patient (or Pediatric) Survey and Staff Survey. (n.d.). Retrieved
from http://www.qualitymeasures.ahrq.gov/content.aspx?id=36866
28. National Quality Measures Clearinghouse. Heart failure (HF): hospital 30-day, all-cause,
unplanned risk-standardized readmission rate (RSRR) following HF hospitalization. (n.d.-a).
Retrieved from http://www.qualitymeasures.ahrq.gov/content.aspx?id=46499
29. National Quality Measures Clearinghouse. Heart failure (HF): hospital 30-day, all-cause,
unplanned risk-standardized readmission rate (RSRR) following HF hospitalization. (n.d.-b).
Retrieved from
http://www.qualitymeasures.ahrq.gov/content.aspx?id=46499&search=heart+failure+readmissi
on+rate
30. National Quality Measures Clearinghouse. Heart failure in adults: percentage of patients with
heart failure diagnosis who were educated on the management of their condition. (n.d.).
Retrieved from
http://www.qualitymeasures.ahrq.gov/content.aspx?id=47033&search=heart+failure+education

31. National Quality Measures Clearinghouse. Pneumonia: hospital 30-day, all-cause, unplanned
risk-standardized readmission rate (RSRR) following pneumonia hospitalization. (n.d.).
Retrieved from http://www.qualitymeasures.ahrq.gov/content.aspx?id=46500
32. National Quality Measures Clearinghouse. Unplanned readmission: hospital-wide, all-cause
unplanned readmission rate (HWR). (n.d.). Retrieved from
http://www.qualitymeasures.ahrq.gov/content.aspx?id=46502
33. Nave, D. (2002). How to compare six sigma, lean and the theory of constraints. Quality
Progress, 35(3), 73–80.
34. Pittsburg Regional Health Initiative. (2011, January). PRHI Readmission Reduction Guie: A
Manual for Prevention Hospitalizations. Retrieved from
http://www.prhi.org/images/stories/docs/ReadmissionReductionGuide-Final2-1-11_000.pdf
35. Raab, S. S., Andrew-JaJa, C., Condel, J. L., & Dabbs, D. J. (2006). Improving Papanicolaou
test quality and reducing medical errors by using Toyota production system methods. American
Journal of Obstetrics and Gynecology, 194(1), 57–64. doi:10.1016/j.ajog.2005.06.069
36. RPIW Participant Fieldbook: Guide to the Rapid Process Improvement Workshop. (n.d.).
Retrieved from http://www.paloalto.va.gov/docs/va_rpiw_fieldbook_paloalto_adaptation.pdf
37. Sales, V. L., Ashraf, M. S., Lella, L. K., Huang, J., Bhumireddy, G., Lefkowitz, L., … Heitner,
J. F. (2013). Utilization of trained volunteers decreases 30-day readmissions for heart failure.
Journal of Cardiac Failure, 19(12), 842–850. doi:10.1016/j.cardfail.2013.10.008
38. Society of Hospital Medicine. (2009). Project Boost Implementation Guide to Improve Care
Transitions: Society of Hospital Medicine.
39. Spear, S., & Bowen, H. K. (1999). Decoding the DNA of the Toyota production system.
Harvard Business Review, 77, 96–108.
40. Swank, C. (n.d.). The Lean Service Machine. Harvard Business Review. Retrieved February 27,
2014, from http://hbr.org/2003/10/the-lean-service-machine/ar/1
41. Veterans Health Administration Systems Improvement Framework. (n.d.). Retrieved from
http://www.paloalto.va.gov/docs/ImprovementGuide.pdf
42. Voehl, F., & Elshennawy, A. (2010). Going Lean in Health Care. Introduction to Service
Engineering, 381–402.
43. Vreeland, Donna G., Ruth E. Rea, and Linda L. Montgomery. “A Review of the Literature on
Heart Failure and Discharge Education:” Critical Care Nursing Quarterly 34, no. 3 (2011): 235–
245. doi:10.1097/CNQ.0b013e31821ffe5d.
44. Walraven, C. van, Bennett, C., Jennings, A., Austin, P. C., & Forster, A. J. (2011). Proportion
of hospital readmissions deemed avoidable: a systematic review. Canadian Medical Association
Journal, 183(7), E391–E402. doi:10.1503/cmaj.101860