safe placement of nasogastric feeding tubes
TRANSCRIPT

Safe Placement of Nasogastr ic Feeding TubesA guide to inter pretation of the check Xray
Authors : Dr D Hughes and Dr J Per r ing

NG Feeding Tubes
Over 790,000 nasogastric tubes are used in the NHS each year
Introducing fluids or medication into the respiratory tract or pleura via a misplaced nasogastric or orogastric tube is a Never Event
NPSA 2005 March 2011 21 deaths and 79 cases of harm due to misplaced NG tubes
NRLS/StEIS 2011 2016 95 further incidents
Single greatest cause of harm was due to misinterpretation of x-rays Accounted for ~ 50% of all incidents and deaths

First L ine Testing
First line testing of nasogastric tube position is by
measuring the pH of aspirate Nasogastric aspirate must be tested using pH paper that is CE marked
and intended by the manufacturer to test human gastric aspirate
The tube should only be used if 0.5mL or more of aspirate is obtained
with a pH between 1 and 5.5 as the safe range, and each test result as
well as the length of the tube is documented on a chart or in the
patient’s care record
If a positive result is not achieved an X-ray needs to be
taken

Second L ine Test
Second line testing of nasogastric tube position is by X-ray
The X-ray request must be clearly marked for ‘NG tube position’
Once taken the X-ray must be reviewed by an appropriately trained person and the findings clearly documented in the patient’s notes before feeding can be started
If it is ‘safe to feed’ this must be documented
Do NOT inter pret an X- ray for NG tube position unless
you are trained to do so
R educing the r isk of feeding through a misplaced nasogastr ic tube
How to analyse check X-rays accurately to detect correct tube placement

Inter pretation of check X- rays
In order to determine whether a nasgastric (NG) tube is in a safe position for feeding, the following questions should be answered: Can I identify the carina? Can I see the tube bisect the carina? Can I identify the diaphragm and see the tube passing
below it? Which way does the tube pass below the diaphragm? Can I see the tip of the tube?

Identifying the car ina
The carina (the point at which the trachea divides into right and left main bronchi) usually lies at the level of the 4th or 5th thoracic vertebra
The carina can usually be seen on a standard chest X-ray
When checking NG tube position, the tube should be seen to pass into the area underneath the carina, therefore “bisecting” it
This does not mean that the tube has to pass precisely in the midline or divide the carina into equal halves
The diagram on the next slide illustrates this

Identifying the car ina
Carina
Right main bronchus
The area under the carinawhich the tube must pass through to bisect it
Bisecting the carina – the tube does not have to pass precisely down the midline but must enter the area underneath the carina

Identifying the car ina
Can you identify the carina and whether the NG tube bisects it in this X-ray?

Identifying the car ina
The NG tube crosses the left main bronchus and does bisect the carina

Identifying the car ina
The carina can be seen and the NG tube deviates to the right at the carina to pass along the expected course of the right main bronchus
The NG tube tip is projected over the right lower zone, likely to be in the right lung base
A central line is also seen, tip projected over the SVC
Feeding should not occur andthis tube should be removed

B eyond the car ina
Sometimes the carina can be unclear If you are unsure whether the NG tube bisects
the carina, follow the tube further down Does it pass down the midline to the level of the
diaphragm? When passing below the diaphragm, does it deviate
immediately to the left? If you can answer “yes” to both questions, the
tube can be assumed to be in the stomach

B eyond the car ina
The carina is a little difficult to see in this patient
The tube passes straight down the midline and deviates immediately to the left below the diaphragm
It would be acceptable to feed this patient nasogastrically
B eyond the car ina
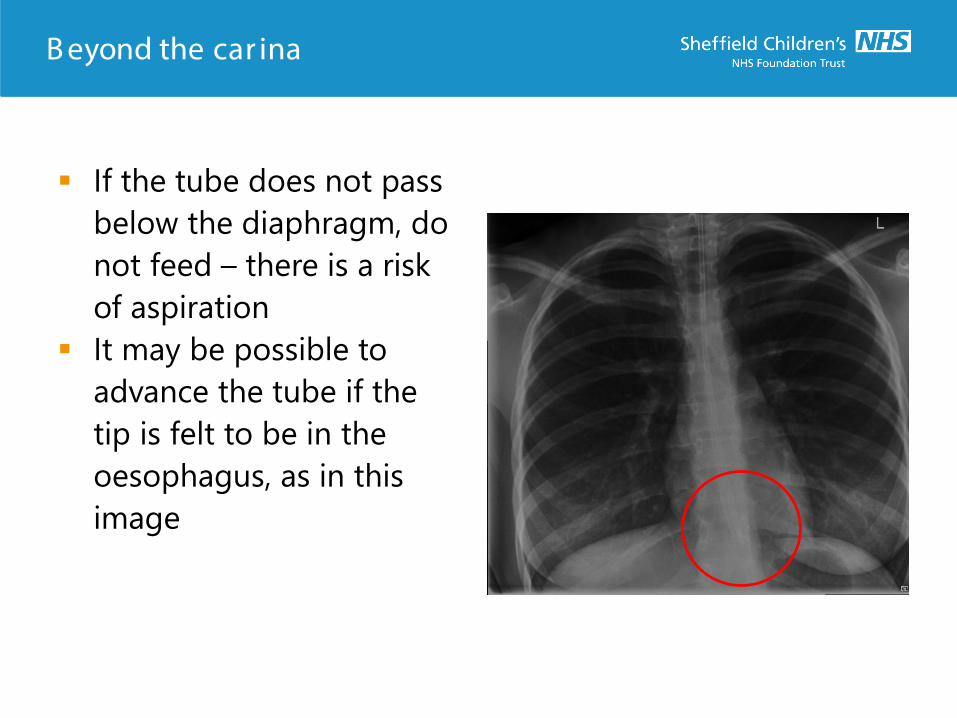
If the tube does not pass below the diaphragm, do not feed – there is a risk of aspiration
It may be possible to advance the tube if the tip is felt to be in the oesophagus, as in this image

B elow the diaphragm
If the tip of the NG tube cannot be seen and no aspirate can be obtained the tube may still be within the stomach, or it could be trans-pyloric, into the small bowel
Options include pulling the tube back slightly and rechecking the aspirate, or re X-raying
Ideally the tip of the tube should always be included on the image

B elow the diaphragm
This image shows an NG tube with its tip in the stomach (circled)
The other feeding tube is transpyloric, passing along the expected course of the duodenum
An impedance probe is also seen, located in the oesophagus, as intended

E xample 1
This NG tube bisects the carina, passes down the midline and below the diaphragm to the left
This is in a suitable position for feeding

E xample 2
This NG tube bisects the carina, passes down the midline and below the diaphragm to the left. Its tip is seen in the fundus of the stomach
This is in a suitable position for feeding

E xample 3
This NG tube bisects the carina and passes straight down the midline but it doesn’t deviate to the left below the diaphragm
There is also a right pneumothorax (circles)
A “straight tube” like this in a neonate is very suspicious for an oesophageal perforation
The tube should not be used but can be left in place until a further tube is passed alongside – once this is confirmed to be satisfactory, the original tube can be removed
E xample 4
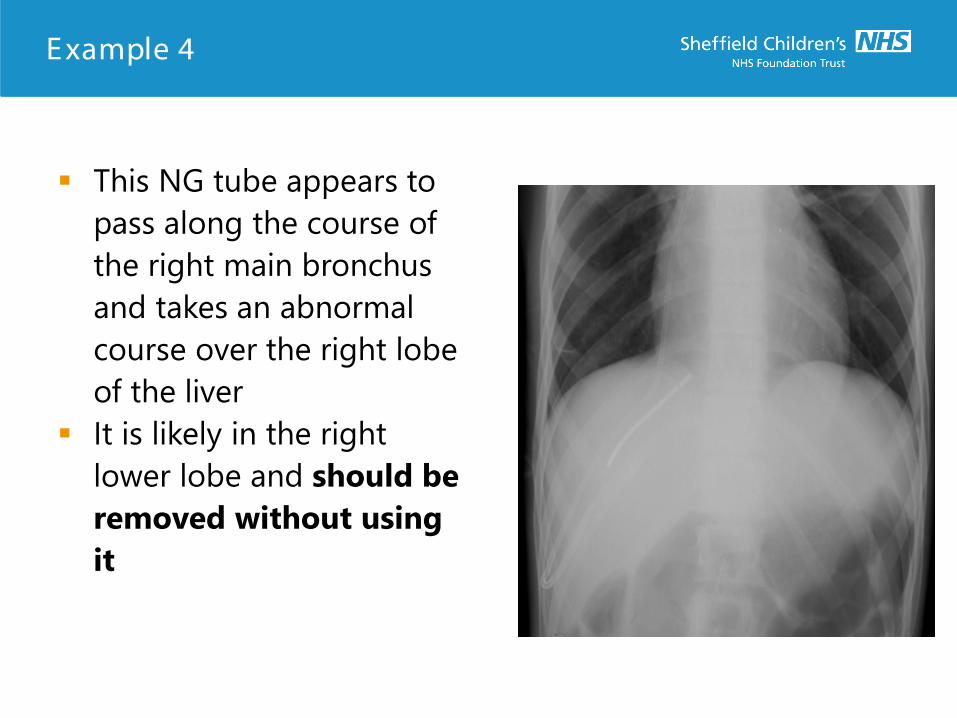
This NG tube appears to pass along the course of the right main bronchus and takes an abnormal course over the right lobe of the liver
It is likely in the right lower lobe and should be removed without using it

E xample 5
This is tricky as the carina is not seen and the patient has a scoliosis
However, the mid portion of the tube deviates to the left above the diaphragm and there is evidence of a left pneumothorax (circled) which is suspicious for tube placement within the lung
At the very least, a full chest X-ray should be performed to see the entire path and the tube should not be used

Summar y
Can I identify the whole length of the tube and its tip?
Can I identify the carina, and does the tube bisect it, passing down the midline to the diaphragm?
Can I identify the diaphragm and see the tube passing to the left below it?
If you can answer “yes” to all 3 questions, then the tube can be considered safe for feeding

R eferences
NHS Improvement Resource set - Initial placement checks for nasogastic and orogastric tubes. July 2016
NHS Improvement Patient Safety Alert: Nasogastric tube misplacement: continuing risk of death and severe harm. July 2016
Reducing the risk of feeding through a misplaced feeding tube. NHS E-learning module (accessed 8.5.18)