safeguarding children - clinical … children - clinical guideline for midwives ... safeguarding...
TRANSCRIPT

Safeguarding Children - Clinical Guideline for Midw ives
Page 1 of 31
SAFEGUARDING CHILDREN - CLINICAL GUIDELINE
FOR MIDWIVES
1. Aim/Purpose of this Guideline
This Safeguarding Children Guideline for Midwives is designed to give guidance on child protection/safeguarding for children up to the age of 18 yrs old and compliment
Cornwall and Isles of Scilly local Safeguarding Children policies and procedures.
2. The Guidance
2.1. Introduction
The local inter-agency procedures are internet based, interactive and regularly updated therefore it is not advisable to print or download any section. They have
been adopted by the South West region and can be found via the Child Protection Health website that can be accessed as detailed www.safechildren-cios.co.uk.
Staff should familiarise themselves with HM Government document “Working Together to Safeguard Children” (2015); RCHT Child Protection and Child Protection
Supervision policies found on the intranet.
Additional Midwifery Safeguarding guidance i.e. report writing, can be found on the shared drive – data11.
It is considered good practice to discuss all issues of Safeguarding Children and cause for concern with your Team Leader/Safeguarding Supervisor. The Named
Midwife or her deputy is also available to discuss issues or concerns raised.
2.2. Role of the Midwife
At booking, an assessment of a woman’s individual needs including a social history,
including the partner, is obtained
Consider Vulnerabilities / Primary Factors (page 2)
Follow the Midwifery Safeguarding Pathway (page 3)
Assess if this is Cause for Concern, Child in Need or Child Protection
If a referral to Social Care is required share with the parents if appropriate. If you
assess that informing the parent(s) is likely to place the unborn child/children at greater risk do not inform them

Safeguarding Children - Clinical Guideline for Midw ives
Page 2 of 31
2.3. Identification of Vulnerabilities / Primary Factors within families which may require Additional Support or a MARU Referral
This is not an exhaustive list.
1 Poor parenting affecting child’s health or development
2 One or both parents under 21 years
3 Step-parent /co-habitee member of household
4 Violence within the family (animals and domestic abuse)
5 History of cruelty (child protection categories)
6 Parents abused / neglected
7 Drug/alcohol abuse of main carers
8 Frequent incidences / injuries
9 Behavioural / emotional vulnerability of child/ren
10 Unreal expectations of the child
11 Failure to thrive
12 Mental illness of main carers
13 Mother suffering with postnatal depression
14 Any factor which makes the professional uneasy
15 Family closing down to outsiders
16 Parents with a learning disability
17 History of criminality
18 Family isolated within the community
19 Homelessness / no fixed abode
20 Late antenatal booking
21 Lack of engagement with community
22 Poor living conditions
23 Poor attendance at appointments
24 Chaotic lifestyle
25 Frequent contact with services
26 FGM
27 Modern Slavery
28 Care leaver / Looked after child
29 Single with no family support
30 Asylum seeker / illegal immigrant/ refugee
31 Sibling within the home with a disability
32 English is not their primary language

Safeguarding Children - Clinical Guideline for Midw ives
Page 3 of 31
Midwifery Safeguarding Pathway
Social Assessment with Community Midwife at Booking
NO SAFEGUARDING CONCERNS
For universal services as per NICE guidelines
VULNERABLE FAMILY / CAUSE FOR CONCERN
Require additional community services / Early Help /Intervention/Support (Child in Need Section 17
Children’s Act 1989) initiate CAF; refer to FIS, Early Help Hub www.cornwallfisdirectory.org.uk or FNP,
SPS,PMHT, Addaction
Requires parental consent Refer to LSCB Threshold Tool
CHILD PROTECTION CONCERNS
A need to protect children who are suffering or are likely to suffer significant harm (Child
Protection Section 47 Children’s Act 1989) MARU referral; best practice is to obtain
parental consent but can be made without.
Complete RCHT Safeguarding Children Record and retain all referrals/correspondence/documentation.
All records to be sent electronically to Team Leaders. Initial Record and Initial Summary of Safeguarding Children (Appendix 3)
Individual Midwives Safeguarding Caseload Card (Appendix 8)
Complete Audit form for Bookings Any referrals to other agencies, including MARU/MARAC/PMHT/SPS/FIS
Subsequent Review (Appendix 4) at least every 6 weeks
Any reports for Case Conferences/Child in Need meetings
Post Conference details (Appendix 5)
Any other correspondences from multi-agencies
A Safeguarding Security Plan (Appendix 6) if needed
Additional Notes (Appendix 7) to be utilised for high risk cases or evidence lack of engagement with midwifery service On discharge to Health Visitor complete a Subsequent Review (Appendix 4) to close the case from midwifery care
Team Leaders will: Commence Chronology (Appendix 9) & Supervision Record (Appendix 10)
Named Midwife for Safeguarding will file all documentation in the newborn’s notes at the end of the midwifery episode of care
If a safeguarding/vulnerable family is identified please place yellow sticker on Maternity Management Plan page of hand held notes
TARIFF INTERMEDIATE onto
STORK INFORM GP & HV

Safeguarding Children - Clinical Guideline for Midw ives
Page 4 of 31
If referral to Social Care is required, complete by approximately 12 weeks gestation, following the dating ultrasound, contact MARU 0300 1231 116 and maintain a
written record of your conversation including the name of the worker you have spoken and any agreed plan. Out of hours URGENT referrals to Social Care 01208
251300
Refer to Cornwall & Isles of Scilly Safeguarding Board Instruction 3 – Arrangements
for pre-birth assessments (Appendix 11)
Ensure that you inform Social Care if the parent(s) are aware of the referral or not
Ensure the appropriate referral form is completed and sent securely electronically within 48 hours of the initial telephone contact
Maintain records of all telephone referrals, discussions, referral forms and send electronically to the Team Leaders with RCHT records of safeguarding as per
Midwifery Safeguarding Pathway
Team leaders will commence Chronology (Appendix 9)
2.4. Safeguarding Supervision
Safeguarding Supervision is an accountable process which supports, assures and
develops the knowledge, skills and values of an individual, group or team. The purpose is to improve the quality of their work to achieve agreed outcomes.
The Community Team Leaders have undertaken supervision training and will support midwives who are working with complex challenging families. This
supervision is evidenced by maintaining a 1 : 1 Safeguarding Supervision Record (Appendix 10).
The Community Team Leaders are responsible to ensure that accurate records are maintained, and are expected to discuss individual safeguarding cases at least
every 6 weeks during a team meeting, offer ongoing support and advice and communicate with the Health Visitors
Midwives can contact the Named Midwife/Nurse for supervision, support and advice via RCHT switchboard
2.5. Information Sharing
Interagency working to safeguard and promote the welfare of children is paramount
(Working Together to Safeguard Children 2015) Refer to Cornwall & Isles of Scilly Safeguarding Children Board Instruction 4 – Information Sharing (Appendix 12)
It is the midwives responsibility to share information with her colleagues/agencies as
appropriate

Safeguarding Children - Clinical Guideline for Midw ives
Page 5 of 31
The midwife will liaise with the Health Visiting Team to arrange a joint antenatal visit after 28 weeks gestation when safeguarding has been identified.
It is the responsibility of the midwife to ensure she effectively informs the team leader using the midwifery safeguarding paperwork
If a woman moves within Cornwall the named midwife is responsible for informing the relevant midwife and for transferring the safeguarding paperwork to the receiving
midwife
If a woman transfers out of Cornwall the named midwife is responsible for contacting the receiving area midwife informing them of the concerns and any plan. Photocopies of the safeguarding paperwork may be sent by recorded delivery.
2.6. Professionals Meetings/Core Group/Case Conference
Attendance at any of the above meetings by the named midwife is vital. If unable to
attend the midwife is responsible to ensure that a representative attends with a detailed update / report in her absence.
Case Conference reports should be written on the appropriate Social Care format utilising the Signs of Safety Model
Reports should be shared with the parents at least 48 hours prior to the conference
Following a safeguarding conference the midwife must complete the Post Conference Details (Appendix 5) and send it electronically to the Named Midwife, or
deputy, for Safeguarding. If the woman is over 36 weeks gestation this should be faxed or emailed to the Delivery Suite Coordinator on duty that day
Guidance for midwives regarding case conference/court proceedings can be found on the midwifery shared drive 11
2.7. Security Issues
In cases where a risk is posed to the newborn of abduction or of violence towards the staff from either the mother, partner or family member a security meeting will be
held
This is the responsibility of the named Social Worker to arrange with the Named Midwife for Safeguarding.
A Safeguarding Children Security Plan (Appendix 6) needs to be recorded and filed in the Safeguarding file on Delivery Suite
2.8. Training
Midwives mandatory training is at level 3 and is booked via RECONSTRUCT website. See Midwives Training Passport for further details. Midwives who are
newly appointed will have to complete training within 3 months of commencing.

Safeguarding Children - Clinical Guideline for Midw ives
Page 6 of 31
2.9. Professional Differences
If professional differences are unable to be resolved discuss initially with the community team leader and/or named midwife for safeguarding and utilise the
safeguarding escalation policy on the intranet
2.10. Professionals with responsibility for Safeguarding Children
These are statutory roles
The Designated Doctor and Nurse take a strategic, professional lead on all aspects
of the heath service contribution to safeguarding children. These posts span Cornwall & Isles of Scilly and includes all providers
The Named Doctors, Nurses and Midwives, play a key role in promoting good
professional practice within their organization, and provide expertise and leadership for their colleagues.
The Named Midwife for Safeguarding Children roles :(see Intercollegiate document Safeguarding Children and Young People 2014 for full description of role)
Provides guidance, monitoring and support to midwives in relation to Safeguarding Children
Monitors implementation of agreed multi-agency plans, in conjunction with the post natal ward manager
Reports serious Safeguarding cases to the Head of Midwifery
Ensures robust written plans are generated and disseminated throughout the maternity services as appropriate
Obtains Safeguarding Children Supervision from the designated or Named
Safeguarding Professional when necessary
Named Midwife will review all Safeguarding Children referrals received to Princess
Alexandra Wing and maintain/update the Supervision paperwork Safeguarding Children File on Delivery Suite/Postnatal Inpatient Ward
Inpatient Team Leaders assist the named midwife in any of the above
The Inpatient Team Leaders can obtain Safeguarding Children support from the named midwife
In the absence of the named midwife this process will be undertaken by the Specialist Midwife for women with Complex Needs

Safeguarding Children - Clinical Guideline for Midw ives
Page 7 of 31
The Specialist Midwife for Women with Complex Needs is a strategic and leadership role in relation to women with mental health, learning disabilities, drugs and alcohol abuse, domestic abuse and young parents
It is the case loading midwife who will continue to be the lead professional for these
women
2.11. Cornwall & Isles of Scilly Safeguarding Children Board (CIOS SCB) The CIOS SCB is a statutory, inter-agency forum. It is a vehicle for agreeing how
different services and professional groups should co-operate to safeguard children in that area and for making sure that arrangements work effectively to bring about good
outcomes for children. It has a role in overseeing quality.
Further information concerning the work and functions of the CIOS SCB can be
found at the SCB website www.safechildren-cios.co.uk
3. Monitoring compliance and effectiveness
Element to be monitored
Clinical Guideline for Safeguarding Children for Midwives
Lead Teresa Phillips
Tool Monthly updates from team leaders of all safeguarding concerns. Regular review of all midwifery safeguarding documentation to
ensure appropriate action has been taken
Frequency Ongoing
Reporting arrangements
Team Leader meetings
Acting on
recommendations and Lead(s)
At the Team leaders meetings an action plan will be agreed and
responsibili ty allocated to the appropriate team leader. Actions will then be reviewed at the next meeting.
Change in
practice and lessons to be
shared
Any changes will be communicated via the monthly midwives
update days and risk management news letters
4. Equality and Diversity
4.1. This document complies with the Royal Cornwall Hospitals NHS Trust service Equality and Diversity statement.
4.2. Equality Impact Assessment
The Initial Equality Impact Assessment Screening Form is at Appendix 9.

Safeguarding Children - Clinical Guideline for Midw ives
Page 8 of 31
Appendix 1. Governance Information
Document Title SAFEGUARDING CHILDREN – CLINICAL
GUIDELINE FOR MIDWIVES
Date Issued/Approved: 17th July 2015
Date Valid From: 17th July 2015
Date Valid To: 17th July 2018
Directorate / Department responsible (author/owner):
Teresa Phillips Named Midwife for Safeguarding Obstetrics & Gynaecology
Contact details: 01872 252684
Brief summary of contents
This guideline is designed to give guidance on child protection/safeguarding children
issues and compliment Cornwall and Isles of Scilly local safeguarding policies and
procedures.
Suggested Keywords: Safeguarding ,children, neglect, child protection, concerns, social, worker, special, violence, domestic, FGM, abuse
Target Audience RCHT PCT CFT
Executive Director responsible for Policy:
Medical Director
Date revised: 17th July 2015
This document replaces (exact title of previous version):
Clinical guideline for safeguarding children
Approval route (names of
committees)/consultation:
Maternity Guideline Group Obs& Gynae Directorate
Divisional Board for noting SCOG
Divisional Manager confirming approval processes
Head of Midwifery
Name and Post Title of additional
signatories Not Required
Signature of Executive Director giving approval
{Original Copy Signed}
Publication Location (refer to Policy
on Policies – Approvals and Ratification):
Internet & Intranet Intranet Only
Document Library Folder/Sub Folder Clinical / Midwifery and Obstetrics

Safeguarding Children - Clinical Guideline for Midw ives
Page 9 of 31
Links to key external standards CQC, Ofsted,
Related Documents:
SW Child Protection procedures
Child Protection and Safeguarding Policy and Procedures
Child Protection/Safeguarding Training Strategy
Child Protection Supervision Policy
Cornwall and the Isles of Scilly Domestic Abuse and Sexual
Violence Strategy 2011-2015 Information Sharing - Local
Safeguarding Children Board
Instruction 4
Training Need Identified? Yes. Refer to section 2.8
Version Control Table
Date Version
No Summary of Changes
Changes Made by
(Name and Job Title)
14/02/2012 V1.0 New Guideline Teresa Phillips – Midwifery
Matron
11 Sep 12 V1.1 Updated contact details of organisations and individuals. Expanded ‘Supervision’ section.
Safeguarding
Midwife/Specialist Midwife
17th July 2015
V1.2
MARU referral included Added LSCB threshold Children on a Child Protection plan team leader will make a chronology to be filed in the baby’s notes following birth Supervision paperwork included Advice upon use of yellow sticker
Teresa Phillips, Community Midwifery Matron &
Outpatient Services/Named Midwife for Safeguarding
All or part of this document can be released under the Freedom of Information
Act 2000
This document is to be retained for 10 years from the date of expiry.
This document is only valid on the day of printing
Controlled Document
This document has been created following the Royal Cornwall Hospitals NHS Trust Policy on Document Production. It should not be altered in any way without the
express permission of the author or their Line Manager.

Safeguarding Children - Clinical Guideline for Midw ives
Page 10 of 31
Appendix 2. Initial Equality Impact Assessment Form
Are there concerns that the policy could have differential impact on: Equality Strands: Yes No Rationale for Assessment / Existing Evidence
Name of Name of the strategy / policy /proposal / service function to be assessed (hereafter referred to as policy) (Provide brief description): SAFEGUARDING CHILDREN - CLINICAL
GUIDELINE FOR MIDWIVES
Directorate and service area: Obs & Gynae Directorate
Is this a new or existing Policy? Existing
Name of individual completing assessment: Teresa Phillips
Telephone: 01872 252684
1. Policy Aim*
Who is the strategy / policy / proposal /
service function aimed at?
This guideline is designed to give guidance on child
protection/safeguarding for children up to the age of 18 yrs and compliment Cornwall and Isles of Scilly local Safeguarding Children
policies and procedures.
2. Policy Objectives*
To ensure all midwives are able to risk assess, recognise and act
upon signs of abuse and potential abuse on children and unborn babies at risk of abuse
3. Policy – intended Outcomes*
Compliance with agreed overarching child protection procedures for Cornwall & IOS and SW Peninsula.
4. *How will you
measure the outcome?
Compliance Monitoring Tool
5. Who is intended to benefit from the
policy?
Unborn babies, children and their families
6a) Is consultation required with the
workforce, equality groups, local interest groups etc. around
this policy?
b) If yes, have these *groups been consulted?
C). Please list any groups who have
been consulted about this procedure.
Yes
Yes
Social Care
Health Visiting Named Nurse for Safeguarding RCHT
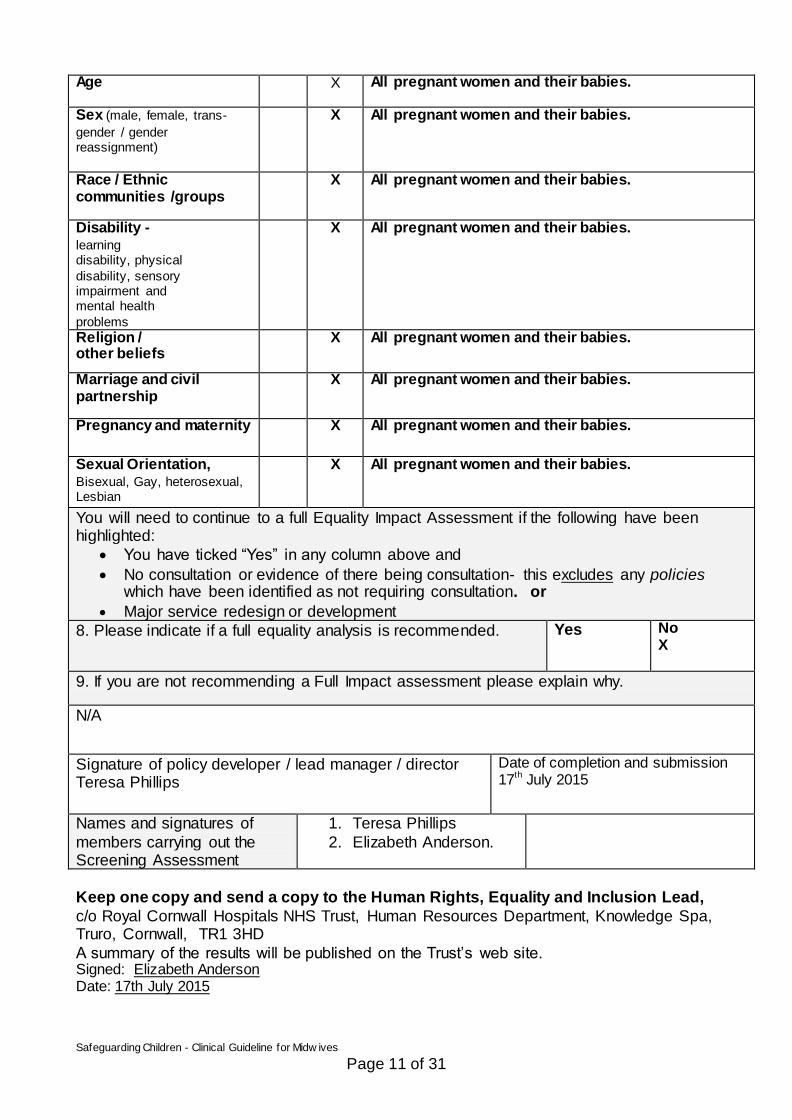
7. The Impact
Please complete the following table.
Safeguarding Children - Clinical Guideline for Midw ives
Page 11 of 31
Age X All pregnant women and their babies.
Sex (male, female, trans-
gender / gender reassignment)
X All pregnant women and their babies.
Race / Ethnic communities /groups
X All pregnant women and their babies.
Disability - learning disability, physical
disability, sensory impairment and mental health
problems
X All pregnant women and their babies.
Religion / other beliefs
X All pregnant women and their babies.
Marriage and civil partnership
X All pregnant women and their babies.
Pregnancy and maternity X All pregnant women and their babies.
Sexual Orientation, Bisexual, Gay, heterosexual, Lesbian
X All pregnant women and their babies.
You will need to continue to a full Equality Impact Assessment if the following have been highlighted:
You have ticked “Yes” in any column above and
No consultation or evidence of there being consultation- this excludes any policies which have been identified as not requiring consultation. or
Major service redesign or development
8. Please indicate if a full equality analysis is recommended. Yes No X
9. If you are not recommending a Full Impact assessment please explain why.
N/A
Signature of policy developer / lead manager / director Teresa Phillips
Date of completion and submission 17th July 2015
Names and signatures of
members carrying out the Screening Assessment
1. Teresa Phillips
2. Elizabeth Anderson.
Keep one copy and send a copy to the Human Rights, Equality and Inclusion Lead,
c/o Royal Cornwall Hospitals NHS Trust, Human Resources Department, Knowledge Spa, Truro, Cornwall, TR1 3HD
A summary of the results will be published on the Trust’s web site. Signed: Elizabeth Anderson Date: 17th July 2015

Safeguarding Children - Clinical Guideline for Midw ives
Page 12 of 31
Appendix 3 Initial Record of Safeguarding Children/Cause for Concern (1 of 2 pages)
Family details and Safeguarding Children 1. Name of professional: 2. GP: 3. CR No:
4. NHS No: 5. Chosen Venue for Birth: 6. EDD: 7. Date:
Woman first name & surname & DOB
Address(es) 1
2 3
4 5
Family Composition Forename Surname (if different to family name)
Details of children
M/F DOB/EDD Address 1 / 2 / 3 / 4
Playgroup/Nursery /School attended
On CPP Date ON/OFF Category On Category Off
Details of Main Carers
Forename Surname M/F DOB Address 1 /2/ 3/ 4
PR* (Tick)
Occupation Relationship to child
* Parental responsibility
Significant others (e.g. Grandparents)
Other Professionals Involved
Name Designation Contact number

Safeguarding Children - Clinical Guideline for Midw ives
Page 13 of 31
:
Appendix 3: (continued) (page 2 of 2)
Woman Name (s): CR No.: E.D.D Midwife: Print Name: Date:
Current Situation Date: Gestation: Safeguarding (section 47) Yes/No Child in Need (section 17) Yes/No Cause for concern Yes/No Primary Risk Factors:
Action taken (to include a summary of contact with the family, any referrals made to other agencies)
If Safeguarding & MARU referral copy to Team Leader If Cause for Concern Early Help Referral or Pre CAF
Action plan (to be completed at session by Midwife and supervisor and to include any advice given)
Signature of Midwife Print name: Date:
Signature of TEAM LEADER: Print name: Date:
Copy to go to:-
1. Team Leader w ho is responsible once reviewed to forward to the Named Midw ife 2. Health Visitor /Safeguarding Lead

Safeguarding Children - Clinical Guideline for Midw ives
Page 14 of 31
Appendix 4: Safeguarding Children: Subsequent Review
Continuation sheet no: AN/PN Date of advice and support :
Woman Name (S): CR No.:
Named Midwife: EDD:
Action plan (to be completed at session by Midwife and Advisor and to include any advice given)
Removed from file Yes No Rationale for removal from advice file
Name of Midwife Completing Update:
Signature of Team Leader Print name: Date:
Current situation and evaluation
Copy to go to:- 3. Team Leader w ho is responsible once reviewed to forward to the Named Midw ife 4. Health Visitor /Safeguarding Lead

Safeguarding Children - Clinical Guideline for Midw ives
Page 15 of 31
Appendix 5. Cornwall & Isles of Scilly Health Trusts - Post Case Conference Details (1 of 2 pages)
NAME/S OF CHILD/REN INVOLVED DOB IF UNBORN BABY EDD MOTHER’S CR No. DATE/PLACE/TIME
ATTENDED BY
INITIAL (I) REVIEW (R ) No longer subject to a CP Plan (D)
CATEGORY (IF REGISTERED) DATE OF NEXT CONFERENCE FAMILY NAME/S NAME OF MOTHER/CARER DOB NAME OF FATHER/CARER DOB NAMES OF OTHER INVOLVED IN CARE e.g. Grandparent DOB
NAME OF SIBLINGS DOB
ADDRESS
SCHOOL/NURSERY IF APPLICABLE
NAMED MIDWIFE
ADDRESS/TEL NO
NAMED HEALTH VISITOR
ADDRESS/TEL NO
GP Please notify GP of outcome of conference
ADDRESS/TEL NO

Safeguarding Children - Clinical Guideline for Midw ives
Page 16 of 31
OTHER AGENCIES INVOLVED
OTHER RELEVANT DETAILS
HEALTH INPUT TO ACTION PLAN DISCHARGE PLANNING MEETING YES/NO TO BE ARRANGED BY SECURITY MEETING YES/NO TO BE ARRANGED BY
CORE GROUP MEMBERS DATE OF CORE GROUP MEETING
SIGNED BY MW………………………………………………PRINT NAME……………………… DATE………………………………………………………….. Only FAX copy to Delivery Suite & Named Midwife for Safeguarding if birth is imminent Send COPIES IMMEDIATELY TO: Midwifery TEAM LEADER
Keep top copy with documentation

Safeguarding Children - Clinical Guideline for Midw ives
Page 17 of 31
Appendix 6 Safeguarding Children Security Plan (1 page only) Name: Date: CR number: EDD: Police log number: Baby subject to Child Protection Plan? YES/NO Any plan for separation of mother and baby after birth?
(Please document detailed arrangements)
Is 24 hour security required? YES/NO
(If yes please detail security arrangements)
Is 24 hour security required? YES/NO
Is a one to one care support worker required whilst an inpatient? YES/NO
Named Social Worker/Care Manager:
Contact number:
Any risk to staff regarding violence/aggression? YES/NO
Risk of baby abduction? YES/NO
cc Security Team Safeguarding File Named Midwife with responsibility for safeguarding children NB: If Security meeting held outside the PAW then fax copy to Named Midwife
Name of agency:
Contact number: Budget number:
Agency funding care? YES/NO Budget number:
Other information:

Safeguarding Children - Clinical Guideline for Midw ives
Page 18 of 31
Appendix 7 Additional Maternity Health Records
CONFIDENTIAL
Women Name/s ………………………….
Unborn EDD………………………………….
Other Children……………………………….
Name DOB NHS Number

Safeguarding Children - Clinical Guideline for Midw ives
Page 19 of 31
Appendix 7 (continued) Additional Midwifery Health Record CONTACT INFORMATION NAME: …………………………………… DOB: ………………………
NHS number: ………..…………………. CR: ……………………….
EDD: ……………………………… RECORD OF CARE
Date
Time Reported Problem/Visit Purpose(Place seen/type of contact) summary of assessment, action plan, evaluation /review date
Signature (Date &
time)
Codes: HV –Health Visitor GP –General Practitioner SW Social Worker MW –Midwife SN –School Nurse NN – Named Nurse, NM – Named Midwife

Safeguarding Children - Clinical Guideline for Midw ives
Page 20 of 31
Appendix 7 (continued) ADDITIONAL CONTACT INFORMATION
NAME: …………………………………… CR: ……………………….
Date
Time Reported Problem/Visit Purpose(Place seen/type of
contact) summary of assessment, action plan, evaluation /review date
Signature (Date &
time)

Safeguarding Children - Clinical Guideline for Midw ives
Page 21 of 31
APPENDIX 8 INDIVIDUAL MIDWIVES SAFEGUARDING /CHILD IN NEED /CAUSE FOR
CONCERN CASE LOAD RECORDS
Midwife ………………………………………………………………
Patient Details EDD
If CIN
Early Help
referral date
If Safeguarding
MARU referral date
& sent to Team
Leader
Up
date
1
Date
/gest
Up
date
2
Date
/gest
Up
date
3
Date
/gest
Up
date
4
Date
/gest
Up
date
5
Date
/gest
Up
date
6
Date
/gest
ICPCC Outcome
Current Situation
(Include here if cases of child in need
become Safeguarding
& date safeguarding paperwork
commenced)

Safeguarding Children - Clinical Guideline for Midw ives
Page 22 of 31
(Need separated one for each case to be completed by Team Leader Only)
WOMAN’S DETAILS NAME: dob:
CR/NHS NUMBER EDD ADDRESS………………………………………………………………………………
…………………………………………………………POSTCODE…………………
Date Case opened
Date Appendix 3 Completed/sent
Dates of Referrals MARU: MARAC: FNP: SPS: PMHT: HV: OTHER:
Date MARU referral sent to T/L
Appendix 4 update 1 Gest: Date: Action:
Appendix 4 update 2 Gest: Date: Action
Appenidx 4 update 3 Gest: Date: Action
Appendix 4 update 4 Gest: Date: Action
Appendix 4 update 5 Gest: Date: Action
Appenidx 4 update 6 Gest: Date: Action
Appenidx 4 update 7 Gest: Date: Action
Date of ICPCC Date: Attended by: Outcome:
Appendix 5 completed & sent
Date:
Birth plan completed & sent
Date:
Date of security meeting (if applicable)
Date:
Dates of Core Group meetings
Date: Date: Date: Date: Date: Date:
Birth outcome Dob: BW: Feeding: Complications: Date Discharged to community:
Postnatal plan completed & communicated
Date: PN visiting Date: Date: Date: Date: Date: Date:
Appendix 4 updates (P/N)
Date: Date: Date:
Discharged from midwifery care
Date: Date transferred to HV : Discussed with HV: yes/no
Case file completed Date:
Case file filed in baby’s medical records
Date: By Who:
APPENDIX 9 MIDWIFERY SAFEGAURDING CHRONOLOGY

Safeguarding Children - Clinical Guideline for Midw ives
Page 23 of 31
APPENDIX 10
1 :1 Safeguarding Supervision Record Name of professional supervisee Date
Time
Brief background if this is the 1st supervision regarding the case.
/Key events since last supervision.
What is working well?
Strengths? Safety?
What are you worried about?
Danger statements
Complicating factors – who is worried about who include unborn children
What are the risks? What we may need clarity
on
Parents/ Carers issues impacting on the child
Parenting Capacity (LD)
Mental Health
Substance Misuse
Domestic Abuse
Scale Scaling e.g. 0 = highest level of concern
10 = no concerns
0 - - - - - - - - - - - - - - - - - - -5 - - - - - - - - - - - - - -- - - - - -10
Safe Goals
What needs to happen to get to 10?
What does this look like?
Child or young person or family
view. What do they want to achieve
from your involvement?
Service Responsibilities/ other
issues discussed On-going Safety Action Plan
Date of next meeting/supervision or supervision complete
Signed supervisor
Signed supervisee

Safeguarding Children - Clinical Guideline for Midw ives
Page 24 of 31
Appendix 11 (Page 1of 3)
Safeguarding Children Board Instruction 3 – Arrangements for pre-birth assessments
Appendix 9 ctd (page 2 of 3)
Cornwall and Isles of Scilly Safeguarding Children Board
CONTEXT Providing early help is more effective in promoting the welfare of children than reacting later. Early help, means
providing support as soon as a problem emerges, at any point in a child’s life. Under the Children Act, 1989, local authorities are required to provide services for children in need for the purpose of safeguarding and promoting their welfare. Local Authorities undertake assessments of
the needs of individual children to determine what services to provide and action to take. Once a referral has been accepted a local authority social worker will make a decision about the
type of response that is required. This will include determining whether: 1. the child and family would benefit from early support services; 2. the child is in need, and should be assessed under section 17 of the Children Act, 1989; or
3. there is reasonable cause to suspect that the child is suffering, or likely to suffer, significant harm, and whether enquiries must be made and the child assessed under section 47 of the Children Act, 1989
Young babies are particularly vulnerable to abuse and work carried out in the antenatal period can help minimise harm if there is early assessment, intervention and support. This multi -agency
protocol sets out how to respond to concerns for unborn children, emphasising clear and regular communication.
Following section 47 enquiries where significant harm is evidence an initial child protection conference should be convened. The ICPC brings together family members (and the child where appropriate), with the supporters, advocates and professionals involved with the child and family, to
make decisions about the child’s future safety, health and development. If concerns relate to an unborn child consideration should be given as to whether to hold a child protection conference prior to the child’s birth. (Working Together 2013)
Actions Agreed Responsible Person South West Child Protection and Safeguarding Procedures – All agencies/professionals
Risks to Unborn Babies http://www.onlineprocedures.
co.uk/swcpp/procedures/knowledgehub/ childrens-development-2/risk-to-unborn-babies-2/
All staff within Cornwall and the Isles of Scilly should be working to the attached Unborn Baby Protocol which has been agreed and endorsed by all LSCBs within the South
West.
Early Identification & Assessment
Safeguarding Children - Clinical Guideline for Midw ives
Page 25 of 31
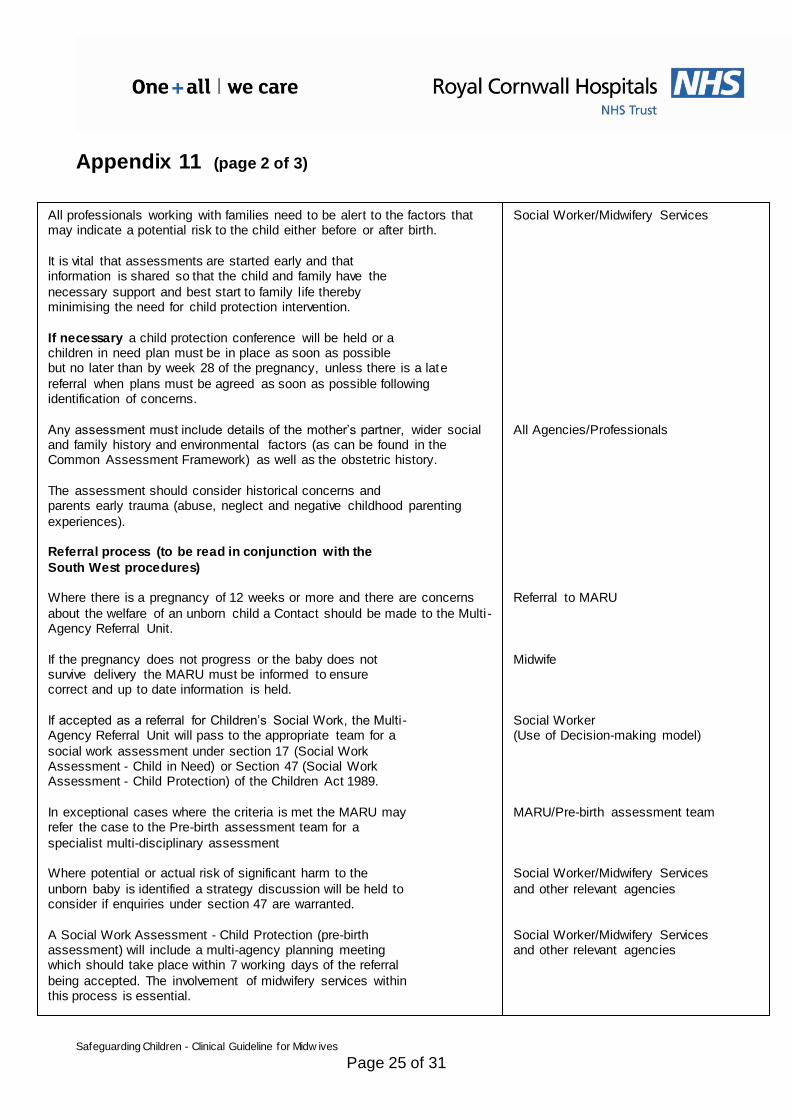
Appendix 11 (page 2 of 3)
All professionals working with families need to be alert to the factors that
may indicate a potential risk to the child either before or after birth.
It is vital that assessments are started early and that information is shared so that the child and family have the
necessary support and best start to family life thereby minimising the need for child protection intervention.
If necessary a child protection conference will be held or a children in need plan must be in place as soon as possible but no later than by week 28 of the pregnancy, unless there is a late
referral when plans must be agreed as soon as possible following identification of concerns.
Any assessment must include details of the mother’s partner, wider social and family history and environmental factors (as can be found in the Common Assessment Framework) as well as the obstetric history.
The assessment should consider historical concerns and parents early trauma (abuse, neglect and negative childhood parenting
experiences). Referral process (to be read in conjunction with the
South West procedures) Where there is a pregnancy of 12 weeks or more and there are concerns
about the welfare of an unborn child a Contact should be made to the Multi -Agency Referral Unit.
If the pregnancy does not progress or the baby does not survive delivery the MARU must be informed to ensure correct and up to date information is held.
If accepted as a referral for Children’s Social Work, the Multi- Agency Referral Unit will pass to the appropriate team for a
social work assessment under section 17 (Social Work Assessment - Child in Need) or Section 47 (Social Work Assessment - Child Protection) of the Children Act 1989.
In exceptional cases where the criteria is met the MARU may refer the case to the Pre-birth assessment team for a
specialist multi-disciplinary assessment Where potential or actual risk of significant harm to the
unborn baby is identified a strategy discussion will be held to consider if enquiries under section 47 are warranted.
A Social Work Assessment - Child Protection (pre-birth assessment) will include a multi-agency planning meeting which should take place within 7 working days of the referral
being accepted. The involvement of midwifery services within this process is essential.
Social Worker/Midwifery Services
All Agencies/Professionals
Referral to MARU
Midwife
Social Worker (Use of Decision-making model)
MARU/Pre-birth assessment team
Social Worker/Midwifery Services
and other relevant agencies
Social Worker/Midwifery Services and other relevant agencies

Safeguarding Children - Clinical Guideline for Midw ives
Page 26 of 31
Appendix 11 (page 3 of 3)
Section 47 enquiries completed through a multi-agency assessment will be recorded as part of the Social Work Assessment - Child Protection and will determine whether an initial
child protection conference is required or whether a child in need of support meeting is more appropriate.
Where Section 47 enquiries conclude that the unborn baby is deemed to be at risk of significant harm an outline child protection plan, identifying specific roles of agencies will be agreed and
recorded as part of the Social Work Assessment - Child Protection. The outline child protection plan will include pre-birth and post-birth actions/issues.
Where it is determined that an initial child protection conference is required it will take place no later than 6 weeks
following the birth of the child. Wherever there is a child protection plan in place pre-birth
there should also be a hospital discharge planning meeting arranged.
(The timing of the initial child protection conference should consider the immediate protection of the child and the health needs of both mother and child. The outline child protection
plan agreed as part of the Social Work Assessment - Child Protection will remain in place until the date of the ICPC.)
Where significant harm is identified at the point of referral or during social work assessment or where other children within the family are subject to child protection plans the case will
be allocated at an early stage to the appropriate Child Protection Team
Siblings already subject to a Child Protection Plan Where the unborn baby/baby has older siblings who are
already subject to a child protection plan and it is agreed by agencies that the (unborn) baby is at risk of significant harm the Social Worker will hold a strategy meeting to initiate a
Social Work Assessment – Child Protection and an ICPC. The date of the ICPC for the (unborn) baby will need to be
aligned with the date of their siblings RCPC. The review child protection conference may need to be brought forward.
Social Worker
Social Worker/Team Manager
Team Manager
Midwife & Social Worker
Social Work Manager
Social Worker
LSCB Instruction regarding arrangements for pre-birth assessments to be disseminated to all staff.
LSCB Agency Members
John Clements Independent Chair Cornwall and Isles of Scilly Safeguarding Children Board - January 2015

Safeguarding Children - Clinical Guideline for Midw ives
Page 27 of 31
Appendix 12 (Page 1 of 5)
Safeguarding Children Board Instruction 4 – Information Sharing
CONTEXT
Working Together (2013)
Information sharing is key to the Government’s goal of delivering better, more efficient public services that are co-ordinated around the needs of the individual. It is essential to enable early intervention and preventative work for safeguarding and promoting welfare and for wider public protection. Information sharing is a vit al element in
improving outcomes for all. Effective information sharing underpins integrated working and is a vital element of both early intervention and
safeguarding. The cross-government guidance ‘Information Sharing: Guidance for practitioners and managers’ and associated training materials provides advice on when and how frontline practitioners can share information legally and professionally. The guidance also covers how organisations can support practitioners and build their
confidence in making information sharing decisions. It is intended for practitioners and managers who have to make decisions about sharing personal information on a case by case basis in all services and sectors, whether they are working with children, young people, adults or families. It is also for those who support these practitioners
and managers and for others with responsibility of information governance. It should be read in conjunction with any specific organisational or professional guidance.
Actions Agreed All staffs to understand information sharing guidance
Myth buster on data protection
• The Data Protection Act 1998 is not a barrier to sharing information but provides a framework to ensure that personal information is shared appropriately.
• Data protection law reinforces common sense rules of information handling. It is there to ensure personal information is managed in a sensible way.
• It helps us strike a balance between the many benefits of public organisations sharing information, and maintaining and strengthening safeguards and privacy of the individual.
• It also helps us balance the need to preserve a trusted relationship between practitioner and client with the need to share information to benefit and improve the life chances of the client or protect the public.
Manager Responsible
All LSCB Agencies
and practitioners
Cornwall and Isles of Scilly
Safeguarding Children Board

Safeguarding Children - Clinical Guideline for Midw ives
Page 28 of 31
Appendix 12 (Page 2 of 5)
All staffs to understand information sharing guidance Seven golden rules for information sharing
1. Remember that the Data Protection Act is not a barrier to sharing information but provides a framework to ensure
that personal information about living persons is shared appropriately. 2. Be open and honest with the person (and/or their family where
appropriate) from the outset about why, what, how and with whom information will, or could be shared, and seek their agreement, unless it is unsafe or inappropriate to do so.
3. Seek advice if you are in any doubt, without disclosing the identity of the person where possible.
4. Share with consent where appropriate and, where possible, respect the wishes of those who do not consent to share confidential
information. You may still share information without consent if, in your judgement, that lack of consent can be overridden in the public interest. You will need to base your judgement on the facts of the
case. 5. Consider safety and well-being: Base your information sharing
decisions on considerations of the safety and well-being of the person and others who may be affected by their actions.
6. Necessary, proportionate, relevant, accurate, timely and secure: Ensure that the information you share is necessary for the purpose for which you are sharing it, is
shared only with those people who need to have it, is accurate and up-to-date, is shared in a timely fashion, and is shared securely.
7. Keep a record of your decision and the reasons for it – whether it is to share information or not. If you decide to share, then record what you have shared, with whom and for what purpose.
The ‘ Seven Golden Rules’ and the following Questions 1- 7 will help support your decision making so you can be more confident that
information is being shared legally and professionally. If you answer ‘not sure’ to any of the questions, seek
advice from your supervisor, manager, named or designated person within your organisation or area, or from a professional body.
1. Is there a clear and legitimate purpose for sharing information?
Why do you or the other person want the information?
What is the outcome you are trying to achieve? Could the aims be achieved without sharing the
information?
All LSCB Agencies and practitioners
All LSCB Agencies and practitioners

Safeguarding Children - Clinical Guideline for Midw ives
Page 29 of 31
Appendix 12 (Page 3 of 5)
Golden rule
Remember that the Data Protection Act is not a barrier to sharing information but provides a framework to ensure that personal
information about living persons is shared appropriately. 2. Does the information enable a living person to be identified?
• If the information is about an identifiable living individual, or could enable a living person to be identified when considered with other information, it is personal information and is subject to data protection
law. This is likely to be the case in the course of your work. You should be open about what information you might need to share and why.
• However, it may not be appropriate to inform a person that information is being shared, or seek consent to this sharing. This is the case if informing them is likely to hamper the prevention or
investigation of a serious crime, or put a child at risk of significant harm or an adult at risk of serious harm.
Golden rule Be open and honest with the person (and/or their
family where appropriate) from the outset about why, what, how and with whom information will, or could be shared, and seek their informed consent, unless it is unsafe or
inappropriate to do so. 3. Is the information confidential? • Not all information is confidential.
• Confidential information is information of a private or sensitive nature that is: • not already lawfully in the public domain or readily
available from another public source; and • has been provided in circumstances where the person giving the information could reasonably expect that it would not be shared with
others. Golden rule
Seek advice if you are in any doubt, without disclosing the identity of the person where possible.
4. Do you have consent to share? • You should seek consent where possible and respect the wishes of those who do not consent to share confidential information. You may
still share information without consent if, in your judgement on the facts of the case, that lack of consent can be overridden in the public interest.
• You do not always need consent to share personal information. There will be some circumstances where you should not seek
consent, for example, where doing so would:

Safeguarding Children - Clinical Guideline for Midw ives
Page 30 of 31
Appendix 12 (Page 4 of 5)
place an adult at increased risk of serious harm; or
prejudice the prevention, detection or prosecution of a serious crime; or
lead to unjustified delay in making enquiries about allegations of significant harm or serious harm
Golden rule
Share with consent where appropriate and, where possible, respect the wishes of those who do not consent to share confidential
information. You may still share information without consent if, in your judgement, that lack of consent can be overridden in the public interest. You need to base your judgement on the facts of the case.
5. Is there sufficient public interest to share the information? • Even where you do not have consent to share confidential information,
you may lawfully share if this can be justified in the public interest. Where consent cannot be obtained or is refused, or where seeking it is unsafe or inappropriate (as explained at Question 4), the question of
whether there is a sufficient public interest must be judged by the practitioner on the facts of each case. A public interest can arise in a wide range of circumstances.
• Where you have a concern about a person, you should not regard refusal of consent as necessarily to mean that you cannot share
confidential information. • In making the decision you must weigh up what might happen if the information is shared against what might happen if it is not, and make a
decision based on professional judgement. Golden rule
Consider safety and well-being: Base your information sharing decisions on considerations of the safety and well-being of the person
and others who may be affected by their actions. 6. Are you sharing information appropriately and securely? • Only share what is necessary to achieve the purpose, distinguishing
clearly between fact and opinion. • Share only with the person or people who really need to know the information.
• Make sure the information is accurate and up-to date. • Understand the limits of any consent given and especially if the information has been provided by a third party.
• Check who will see the information and share the information in a secure way. For example, confirm the identity of the person you are talking to; ensure a conversation or phone call cannot be overheard;
use secure email; ensure that the intended person will be on hand to
receive a fax.

Safeguarding Children - Clinical Guideline for Midw ives
Page 31 of 31
Appendix 12 (Page 5 of 5)
• Establish with the recipient whether they intend to pass it on to other people and ensure that they understand the limits of any consent that has been given.
• Inform the person to whom the information relates that you are sharing the information, if it is safe to do so, and if you have not already told them that their information may be
shared.
Golden rule
Necessary, proportionate, relevant, accurate, timely and secure: Ensure that the information you share is necessary for the purpose
for which you are sharing it, is shared only with those people who need to have it, is accurate and up-to-date, is shared in a timely fashion, and is shared securely.
7. Have you properly recorded your information sharing decision?
• Record your information sharing decision and your reasons, including what information you have shared and with whom, following your agency’s arrangements for recording information and
in line with any local information sharing procedures in place. • If, at any stage, you decide not to share information, you should record this decision and the reasons for it.
Golden rule
Keep a record of your decision and the reasons for it – whether it is to share information or not. If you decide to share, then record what you have shared, with whom and for what purpose
Agency staff can hold professional meetings to share information
and agree how they are going to work together to promote the welfare of and safeguard a child without a social worker being involved at Level 2: Additional Needs where parents/carers and/or
young people have declined to be part of the Common Assessment Framework process. Any agency can convene an information sharing professional
meeting as long as they have informed parents/carers and/or young people what there concerns are and why there is a need to meet with other professionals to share information.
LSCB Members to communicate to all staff
Independent Chair Trevor Doughty Cornwall & Isles of Scilly Safeguarding Children Board Director Children, Schools and Families October 2011
Re-Issued Nov 2013