safeguarding information on mobile devices agatha christie
TRANSCRIPT

OFFICAL PUBLICATION OF THE COLLEGE OF AUDIOLOGISTS AND SPEECH-LANGUAGE PATHOLOGISTS OF ONTARIO
VOLUME 8 ISSUE 2 MAY 2010
www.caslpo.com
www.andrewjohnpublishing.com
Publications Agreement Number 40025049 • ISSN 1713-8922
Safeguarding Information
on Mobile Devices
Agatha Christie – Helping
to Unravel the Mystery of
Alzheimer’s Disease

5 Message from the RegistrarBrian O'Riordan
CASLPO TODAY M A Y 2 0 1 0
cont
ents
7 Council Highlights:March 2010
CASLPO NEWS
8 Competency Profile Validation: An UpdateBy Karen Luker, Deputy Registrar
8 CASLPO Task Force: Assistive Devices ProgramBy Karen Luker, Deputy Registrar
9 Friday October 1, 2010 – Mark This Date For Your Registration Renewal!By Gregory Katchin, Director of Finance and Colleen Myrie, Manager of Registration Services
FEATURE
17 Agatha Christie – Helping to Unravel the Mystery of Alzheimer’s DiseaseBy Sherry Hinman
19 Andy Barrie: Good CompanyBy Sherry Hinman
DEPARTMENTS
10 CASLPO Participates in the Development of National Standards for the Professions
11 2009 Registration Statistics
11 2011: The New Self Assessment Tool OnlineBy Carol Bock, Deputy Registrar
12 Ontario Legislature Passes Labour Mobility ActBy Karen Luker, Deputy Registrar, and Colleen Myrie, Manager of Registration
14 A Quick Guide to the Harmonized Sales TaxBy Gregory P. Katchin, Director of Finance
15 Members Suspended for Failure to Complete the Annual Renewal Requirements For 2009/2010By Gregory Katchin, Director of Finance and Colleen Myrie, Manager of Registration Services
15 Were You Selected For a Peer Assessment This Year? 6 Top Questions AnsweredBy Carol Bock, Deputy Registrar
21 Safeguarding Information on Mobile Devices
17
19
www.caslpo.com

CASLPO NEWS
y t
MESSAGE FROM THE REGISTRAR
Beginning of an Exciting Journey
In the last issue of this magazine, CASLPO’s President, Meg Petkoff, commentedon my beginning an exciting journey as the new Registrar of the College. Howright she was. My first four months on the job have certainly been eventful. I haveattended many Council committee meetings, including those affecting matters ofRegistration, Quality Assurance, Practice Issues, and Complaints. I also attendedmy first CASLPO Executive and Council meetings. All the staff and members ofCouncil have been most generous with their time and helpful in welcoming me tothe regulatory family.
I have placed a premium on meeting with members of the College and withgraduating students in speech-language pathology and audiology. There have alsobeen meetings with officials in the Ministry of Health and Long-Term Careconcerning the Assistive Devices program (ADP), and with representatives of OSLAand AHIP. I also attended a planning retreat with other college registrars under theauspices of the Federation of Health Regulatory Colleges of Ontario (FHRCO).Plans are proceeding for a June CASLPO Council strategic priority-setting exercise.That session will hopefully produce a new vision and workplan that will guide usinto the future. Already work is under way to revamp our website and to revise ourgovernance bylaws. Look for your chance soon to provide input on a new set ofregulations for registration procedures, resulting from advice received from theOffice of the provincial Fairness Commissioner and in order for us to be compliantwith the new Ontario Labour Mobility Act. I also wish to thank the many memberswho have taken the time to submit comments to me on our newly revised draftRecords Regulation.
Recently, the Minister of Health and Long-Term Care imposed what is effectivelya two-year hiatus on the work of the Health Professions Regulatory AdvisoryCouncil (HPRAC). It is this agency which provides advice to the m inister onmatters such as changes in professional scopes of practice. This means that we willlikely have to continue to wait for the government to address much needed changesin the scopes of practice and use of the title doctor for those registered withCASLPO. However, we will renew our efforts to resubmit our requests for changesand seek to have them addressed as soon as the opportunity presents.
CASLPO continues to work with other provincial regulatory bodies for audiologistsand speech-language pathologists across Canada to form an effective nationalassociation of regulators. In this regard, there will be crucial meetings at the endof May with our counterparts in other provinces in order to make progress onseveral outstanding issues relating to the harmonization of registrationrequirements and essential professional competencies. A recent example of thevalue in such forums was the publication in March of national Infection Preventionand Control Guidelines for Speech-Language Pathologists and Audiologists. Thesedocuments, which were formulated through a process of interorganizationalcollaboration, have been sent to members and are posted on the College website.
Finally, one of the most important duties of any Registrar is to listen. So, Iencourage members to contact me at any time at [email protected] to shareyour insights and concerns about the work of the College. With your assistanceand dedication, I hope to continue to go forward on the “exciting journey” as yourRegistrar.
Brian O’Riordan, Registrar
CASLPO College of Audiologists and Speech-Language Pathologists of OntarioOrdre des audiologistes et des orthophonistes de l’Ontario
A: 3080 Yonge St., Suite 5060, Toronto, ON M4N 3N1T: 416-975-5347/1-800-993-9459F: 416-975-8394E: [email protected] | W: www.caslpo.com
R E G I S T R A R
Brian O'RiordanExt: 215 | [email protected]
D E P U T Y R E G I S T R A R
Carol Bockext 227 | [email protected]
D E P U T Y R E G I S T R A R
Karen LukerExt: 226 | [email protected]
D I R E C T O R O F F I N A N C E
Gregory KatchinExt: 217 | [email protected]
M A N A G E R O F R E G I S T R A T I O N S E R V I C E S
Colleen MyrieExt: 211 | [email protected]
M A N A G E R O F S U P P O R T S E R V I C E S
Carol LammersExt: 214 | [email protected]
A D M I N I S T R A T I V E A S S I S T A N T
Camille PrashadExt: 213 | [email protected]
A D M I N I S T R A T I V E A S S I S T A N T
Linda MeissenheimerExt: 210 | [email protected]
M A N A G I N G E D I T O R
Scott [email protected]
A R T D I R E C T O R / D E S I G N E R
Andrea Brierley905.522.0788 | [email protected]
S A L E S A N D C I R C U L A T I O N C O O R D I N A T O R
Brenda Robinson905.628.4309
A C C O U N T I N G
Susan McClungC L A S S I F I E D A D V E R T I S I N G :
Brenda Robinson905.628.4309
G R O U P P U B L I S H E R
John D. Birkby
S U B S C R I P T I O N R A T E SInstitution: $60.00, Individuals: $34.00, Single copy: $13.00
Canadian subscribers add 5% GST
US and International subscribers remit in US dollars
CASLPO Today is published quarterly by Andrew John Publishing Inc. withoffices located at 115 King Street West, Suite 220 Dundas, ON L9H 1V1. Wewelcome editorial submissions but cannot assume responsibility or commit-ment for unsolicited material. Any editorial materials, including photographs,that are accepted from an unsolicited contributor will become the property ofAndrew John Publishing Inc. The publisher shall not be liable for any of theviews expressed by the authors of articles or letters published in CASLPOToday, nor shall theses opinions necessarily reflect those of the publisher.
F E E D B A C K : We welcome your views and comments.Please send them to:115 King Street West, Suite 220 Dundas, ON L9H 1V1
Copyright 2010 by Andrew John Publishing Inc. All rights reserved.Reprinting in whole or in part is forbidden without the express consent ofthe publisher.
Publications Agreement Number 40025049 | ISSN 1713-8922Return undeliverable addresses to: Andrew John Publishing Inc. 115 KingStreet West, Suite 220 Dundas, ON L9H 1V1

Council met on March 5, 2010 and the following are thehighlights:
1. President’s RemarksA special welcome to Brian O’Riordan, Registrar and a thank youto the Search Committee for the work involved in selecting Brian.
A thank you to current staff for continuing the good work duringthe transition to a new Registrar and a special thank you andremembrance to past staff, Barbara Meissner Fishbein, LynneLatulippe, and David Hodgson for their contributions in makingthe College what it is today.
2. Position Statement on Audiologists’ Relationships withOther Service ProvidersStaff updated Council on the status of this position statement andthe history behind it. This document was deferred to the June 2010Council meeting.
3. Position Statement on Audiologists Completing ADPHearing Device ApplicationsStaff updated Council on the status of this position statement andthe Registrar briefed Council on the concerns regarding ADPmentioned in the Auditor General’s Report. Staff updated Councilas well on the formation and status of a CASLPO task force toreview members’ concerns regarding the ADP report and otherissues surrounding ADP. This document was deferred to the June2010 Council meeting.
4. CASLPO/OSLA ConferenceStaff updated Council on the letter of agreement signed by OSLAand CASLPO for this conference as well as work being done todevelop an agenda for the conference.
5. Executive Committee ReportDiscussion took place regarding the role of Council members oncethey are elected to Council. A suggestion was made to incorporatethis into an article for CASLPO Today.
6. SLP Practice Committee ReportCouncil requested that all Committee chairs work more closely incollaboration with staff to prepare Committee agendas, minutesas well as reports to Council and that this be a consistent practicefor all staff and committee chairs.
7. 2010 Election datesCouncil approved the motion that the 2010 election date be set forMay 31, 2010 for District 6 (Member-at-Large)
8. Governance Policy and Bylaw ReviewThe Registrar presented an update on the status and timeline ofthe Governance Policy and Bylaw Review in preparation for theJune Council meeting.
For more information on any of these topics please contactBrian O’Riordan, Registrar at 416-975-5347 ext 215 or byemail at [email protected].
MARCH 2010 COUNCIL HIGHLIGHTS NEWS
www.caslpo.com
CASLPO-OSLA 2010 CONFERENCE
October 21-22, 2010
is the first CASLPO-OSLA joint conference and will offer the most current regulatory information and professional learning opportunities in one location!
Join us at the Sheraton Parkway Toronto North Hotel and Conference Centre, Richmond Hill (highway 7 and Leslie)
accessible by Viva public transit from the Yonge-Finch subway or by car with complimentary parking!
Check the OSLA website for Early Bird Pre-registration in early May 2010.
.caslpo.comwww
Pre-registration in early May 2010. Check the OSLA we
subway or by car with complimentary parking! accessible by Viva public tra
Conference Centre, Richmond Hill (highway 7 and Leslie) Join us at the Sheraton Parkway Toronto North Hotel and
n early May 2010. bsite for Early Bird
omplimentary parking! ansit from the Yonge-Finch d Hill (highway 7 and Leslie)
way Toronto North Hotel and

In the last issue of CASLPO Today,members were encouraged tocomplete a survey to validatecompetency profiles for the practice ofaudiology and speech-languagepathology. Readers will recall thatCASLPO has been involved in acollaborative effort to create updatedinter-provincial standards for practiceand education in the form ofcompetency profiles. Regulatory bodies,professional associations, and Canadianuniversities associated with theprofessions have been working togetherwith the support of funding fromHuman Resources and SkillsDevelopment Canada (HRSDC).CASLPO acts as the project manager onbehalf of HRSDC, thus coordinatingthe group’s activities and monitoringthe budget on a quarterly basis. Whencompleted and validated, the practicecompetencies will identify the job tasks,and minimum level of proficiency inthese tasks, that are required in eachprofession.
At the time of publication, more than1,600 practitioners across the countryhad completed the survey in either French or English. This representsapproximately 20% of practicing speech-language pathologists and audiologists
across the country and is considered agood response rate.
In recognition of the contribution madeby those practitioners that completedthe survey, each participant had theirname entered into a draw and becameeligible to win one of four charitablecertificates. We are pleased to announcethe following winners:
Carolyn Spriet, audiologist (Ontario)and Claire Chamberland, speech-language pathologist (Quebec), eachreceive a $150 certificate, payabletoward the continuing educationactivity of their choice in 2010. Theseprizes were provided by the CanadianAlliance of Regulators.
Leslie Ann Harvie, speech-languagepathologist (Ontario) and Julie Tran,audiologist (Quebec), each receive a$100 certificate, payable toward the2010 CASLPA Conference or a CASLPAwebinar. These prizes were provided by the Canadian Association of Speech-Language Pathologists andAudiologists.
Next StepsThe closing date for the completion ofthe survey was April 18, 2010. Following
this, the working group will considerthe responses and will finalize theprofiles based on validation dataobtained. The group’s work is led byCatalysis Consulting of Kamloops,British Columbia. It is expected that thefinal profiles will be available to thepartner organizations by the end of July2010.
HRSDC is currently considering theinterorganizational partners’ nextproposal, which involves developing aframework to assess competence. Thepartners expect that this project willresult in a paper which will outline bestpractices in competency assessment,and identify tools which organizationsmay access or develop to ensure entry-to-practice competence for newentrants to the profession. The issue ofcontinuing competence will also beaddressed in this paper.
CASLPO will remain involved in allaspects of the competency projects, andwill provide updates in future issues ofCASLPO Today.
Please do not hesitate to contact Karen Luker, Deputy Registrar, [email protected] for additionalinformation.
CASLPO NEWS
COMPETENCY PROFILE VALIDATION: An Update
Karen Luker, Deputy Registrar
The Assistive Devices Program is aprogram of the Ministry of Health
and Long-Term Care which providesfinancial assistance to the public ofOntario in obtaining various assistivedevices including those devices for theircommunication needs. These devices
may include hearing aids, listeningdevices such as FM systems, voiceoutput communication aids, andartificial larynges. CASLPO memberswho are registered as authorizers withthe Assistive Devices Program (ADP)are required to abide by specific policies
and procedures set by the program.
The auditor general of Ontario’s annualreport for 2009 included a chapter onthe Assistive Devices Program. Anumber of concerns surrounding thereimbursement of hearing aids and FM
CASLPO Task Force: Assistive Devices ProgramBy Karen Luker, Deputy Registrar

systems were identified. As a result ofthis report, the ministry hosted ameeting in January 2010, includingrepresentatives from ADP and severalregulatory colleges (e.g., College ofOccupational Therapists, College ofRespiratory Technologists, College ofOptometrists, and CASLPO). Theobjective of the meeting was to begin adialogue with colleges, with theultimate goal to establish a mechanismto better monitor the activities of ADPauthorizers. The outcome of themeeting resulted in ADP identifying aneed to meet with individual colleges.
From the members’ perspective,audiologists and speech-language
pathologists have expressed someconcerns of their own regarding theAssistive Devices Program. Forexample, authorizers are required toobtain the signature of a physician oranother audiologist, attesting that the applicant has a hearing loss which is significant enough to warrant the need for a hearing aid. This could be compared to a physicianrecommending a radiograph, buthaving to request that another physicianverify the validity of the request prior toproceeding.
In anticipation of a meeting with ADP,CASLPO established a task force to actin an advisory capacity on matters
involving the Assistive DevicesProgram. Members of the task forceinclude practicing audiologists from thepublic and private sector, an academicmember, and College staff. A firstmeeting was held on March 24, 2010 toidentify issues and strategies inpreparation for CASLPO’s meetingwith ADP representatives.
At this time, CASLPO invites membersto submit any information, questions orconcerns on this topic in confidence, viaemail, to [email protected]. Updateson the activities of the Task Force willbe included in future issues of CASLPOToday.
CASLPO NEWS
For members who are away fromtheir email during the summer
months, the College wishes to providethis early reminder that it is a member’sresponsibility to renew their certificateof registration by October 1 of eachyear, even if the member fails to receivea notice from the College. Theregistration renewal deadline for2010/2011 is Friday, October 1, 2010.
To ensure that you receive the College’semail reminders regarding theregistration renewal, you shouldconfirm that the College has yourcurrent e-mail address on file. Alsoremember to check your spam or junk mail folders regularly, because a CASLPO email message couldmistakenly be directed to a spam orjunk folder by your service provider. Ifyou will be away from your office in thesummer, please ensure that the Collegehas an email address for you that youcan access while away from the office.
The College’s online renewal systemwill be available to members as of
August 3, 2010. To renew online, youneed your registration number andyour date of birth to login.
You can also renew using a paperrenewal form if you downloadCASLPO’s 2010/2011 renewal packagefrom our website on or after August 3,2010. If you would like the College tosend you a renewal package, you mustmake a request by telephone, email, orfax before September 17. After this date,a renewal package may not get to you intime by regular mail for you to meet theOctober 1 deadline.
To avoid the late payment fee, do notwait until the last minute to completeyour registration either online or bymail. You can post-date your cheque upto October 1, 2010 and it will not bedeposited until that date.
If you are planning to change your classof registration, please be advised thatyou will not be permitted to renewonline and must download the paperversion of CASLPO’s renewal form and
send it to the College by mail orelectronically by fax or email, in timefor the October 1 deadline.
If you are planning not to renew yourcertificate of registration, do not letyour registration lapse. You must adviseCASLPO in writing via regular mail,fax, or by email that you wish to resignfrom the College. If you fail to renewyour membership with the College anddo not resign, your membership will besuspended for non-payment of fees andeventually revoked. A permanent recordof the suspension would be entered inthe register, which would be included inall requests for verification of amember’s registration status with theCollege.
If you have a question regarding yourregistration or renewal, please call 416-975-5347 or toll-free at 1-800-993-9459 and ask for eitherGregory Katchin at extension 217 orColleen Myrie at extension 211.
FRIDAY OCTOBER 1, 2010 – MARK THIS DATEFOR YOUR REGISTRATION RENEWAL!
By Gregory Katchin, Director of Finance and Colleen Myrie, Manager of Registration Services

Together with its partners, CASLPOrecently released new InfectionPrevention and Control Guidelines forSpeech Language Pathology and forAudiology. These new guidelines arethe result of CASLPO’s participation inthe Canadian InterorganizationalGroup for Audiology and Speech-Language Pathology.* The group bringstogether a number of organizationswho have an interest in the bettermentof the professions, including regulatorybodies, professional associations, anduniversities across Canada. Theguidelines reflect these organizations’commitment to providing professionals
with tools to assist them in theprovision of high quality services totheir patient/clients.
It is the intent of these new guidelines to assist in clinical practice and decision-making, while accommodatingvariations in practice settings. Membersare encouraged to reflect on theirindividual practice and their typicalassessment and intervention proceduresas they review the contents of theguidelines. In some instances, therecommendations will already be anintegral component of a member’spractice, where in other instances, a
change or shift in clinical practice maybe required. Members should also beaware of, and comply with, employerand/or agency policies, occupationalhealth and safety legislation, and anyadditional standards related to infectionprevention and control.
The guidelines are now available onCASLPO’s website and will be printedand sent to all members for inclusion intheir Desk Reference. The adoption ofthese guidelines will serve to replaceguidelines which were previouslypublished by CASLPO. Members are,therefore, encouraged to becomefamiliar with the new documents, andto replace any existing documents intheir Desk Reference as soon as theyreceive the hard copy.
The guidelines can be found byselecting the “Practice Standards” tab atwww.caslpo.com.
We wish to acknowledge and thank themany members of CASLPO whocontributed hours of hard work to thedevelopment of the new documents.The process involved in creating thenew guidelines is a successful model of interorganizational policycollaboration.
Next Steps: Autism andAuditory ProcessingDisordersFollowing the successful completion ofthis project, the InterorganizationalGroup for Audiology and Speech-Language Pathology has approved itsnext two projects:
1. The development of guidelines for auditory processing disorders
2. The development of guidelines addressing the role of the speech-language pathologist in the assessment and treatment of autism spectrum disorders
CASLPO NEWS
Knowledge and Feelings TowardWorking with Persons Livingwith HIV/AIDS: A Survey ofCanadian Speech-LanguagePathologists and AudiologistsYou are invited to take part in a survey on communication disorder servicesavailable to individuals with HIV/AIDS. This study is being conducted by TaraWilson, a graduate student in speech-language pathology, and Dr. Ellen Hickey,PhD, at the School of Human Communication Disorders at DalhousieUniversity. To access the survey, please logon to:
English: https://surveys.dal.ca/opinio/s?s=8087Français: https://surveys.dal.ca/opinio/s?s=8327
Thank you for your participation!
CASLPO Participates in the Development of National
Standards for the Professions
Working groups have been appointedand directed to develop these guide-lines, which are scheduled to becompleted by the end of the summer.All partner organizations will then beconsulted in an effort to approve andadopt the guidelines as soon as possibleafterward.
*The Interorganizational Group forAudiology and Speech-Language Pathologyis composed of regulatory bodies(represented by the Canadian Alliance of
Regulators), professional associations(represented by the Canadian Association of Speech-Language Pathologists andAudiologists, the Canadian Academy ofAudiology, and all provincial/territorialassociations), and universities (representedby the Canadian Council of UniversityPrograms – SLP/Audiology). It was createdin 2007 to bring together all organizationsconcerned with the practice of theprofessions. Its primary objective is thedevelopment and harmonization ofstandards across the country.
CASLPO NEWS
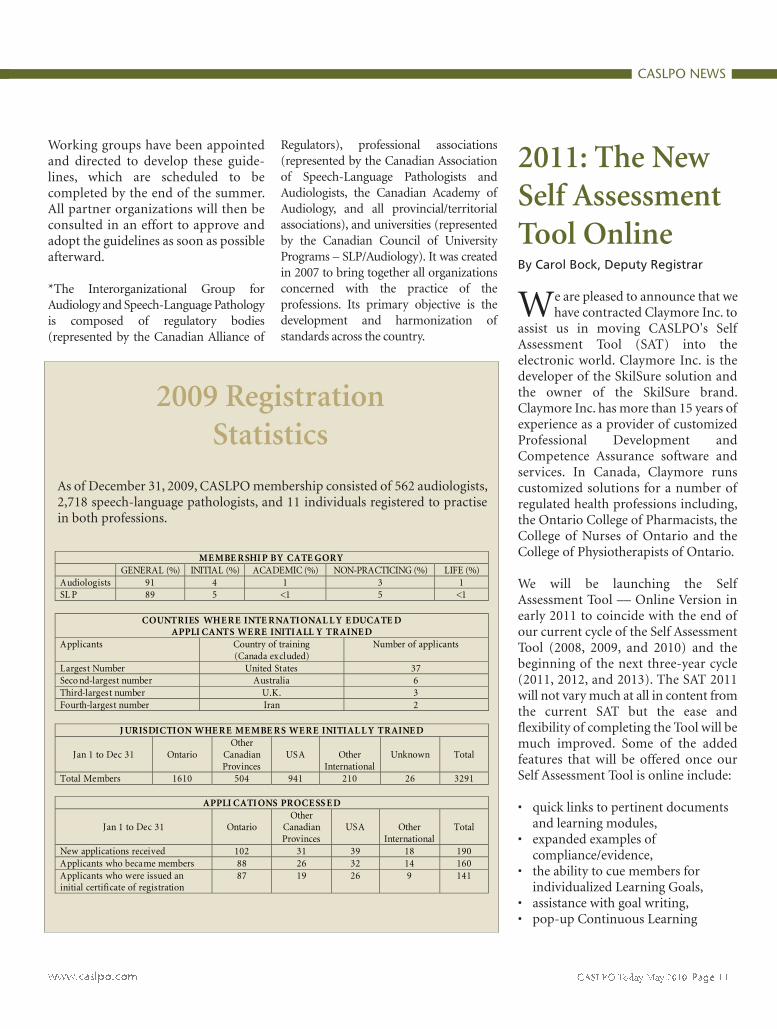
ME MBE R SHI P BY CATE GOR Y GENERAL (%) INITIAL (%) ACADEMIC (%) NON-PRACTICING (%) LIFE (%) Audiologists 91 4 1 3 1 SL P 89 5 <1 5 <1
COUNTRIES WHE R E INTE R NATIONAL L Y E DUCATE D APPLI CANTS WE RE INITI ALL Y TR AINE D
Applicants Country of training (Canada excluded)
Number of applicants
Largest Number United States 37 Seco nd-largest number Australia 6 Third-largest number U.K. 3 Fourth-largest number Iran 2
J URISDICTION WHE R E ME MBE R S WE R E INITIAL L Y TR AINE D
Jan 1 to Dec 31
Ontario Other
Canadian Provinces
USA
Other
International
Unknown
Total
Total Members 1610 504 941 210 26 3291
APPLI CATI ONS PROCE SS E D
Jan 1 to Dec 31
Ontario Other
Canadian Provinces
USA
Other
International
Total
New applications received 102 31 39 18 190 Applicants who became members 88 26 32 14 160 Applicants who were issued an initial certificate of registration
87 19 26 9 141
2009 Registration Statistics
As of December 31, 2009, CASLPO membership consisted of 562 audiologists,2,718 speech-language pathologists, and 11 individuals registered to practisein both professions.
2011: The NewSelf AssessmentTool OnlineBy Carol Bock, Deputy Registrar
We are pleased to announce that wehave contracted Claymore Inc. to
assist us in moving CASLPO's SelfAssessment Tool (SAT) into theelectronic world. Claymore Inc. is thedeveloper of the SkilSure solution andthe owner of the SkilSure brand.Claymore Inc. has more than 15 years ofexperience as a provider of customizedProfessional Development andCompetence Assurance software andservices. In Canada, Claymore runscustomized solutions for a number ofregulated health professions including,the Ontario College of Pharmacists, theCollege of Nurses of Ontario and theCollege of Physiotherapists of Ontario.
We will be launching the SelfAssessment Tool –– Online Version inearly 2011 to coincide with the end ofour current cycle of the Self AssessmentTool (2008, 2009, and 2010) and thebeginning of the next three-year cycle(2011, 2012, and 2013). The SAT 2011will not vary much at all in content fromthe current SAT but the ease andflexibility of completing the Tool will bemuch improved. Some of the addedfeatures that will be offered once ourSelf Assessment Tool is online include:
• quick links to pertinent documents and learning modules,
• expanded examples of compliance/evidence,
• the ability to cue members for individualized Learning Goals,
• assistance with goal writing, • pop-up Continuous Learning

Activity Credit (CLAC) limits in thevarious categories,
• the capacity to collate aggregate datathat reflect trends in practice setting,CLACs, geographical needs for member education, etc., and
• the capacity to securely upload evidence for storage.
Although the Tool will also be availableto those who would prefer it in hardcopy, we are planning a roll-outschedule that will allow all members touse the online version. It is anticipatedthat a prototype will be available forJune, 2010, followed by a version thatwill be ready for a limited (50participants) pilot run in July, 2010. Theprogram will then be ready for the
“live” run in January, 2011.
This spring and summer, CASLPO willbe asking members to assist us in thepilot version. Why might you volunteerto participate? Well, if you do volunteeryou will be taken out of the general poolfor selecting members for the SATsubmission for three years. You willhave significant input to the final designof the program, and you will be able toclaim additional CLACs.
If you are interested please contact Carol Bock at 416-975-5347, toll-free at 1-800-993-9459 x 227, or via email [email protected] for furtherinformation.
CASLPO NEWS
Amendments to the Agreement onInternal Trade (AIT) endorsed by
Canada’s premiers in January 2009committed all provinces and territoriesto improving labour mobility forcertified workers in professions andtrades.
As a result, all provinces have beendirected to develop and approvelegislation to support theircommitment to implement the labourmobility provisions of the AIT. InOntario, the Ontario Labour MobilityAct was passed by the Legislature onDecember 15, 2009. This legislationensures that workers who are certifiedto practice in a province or territory willbe entitled to be certified in thatoccupation in Ontario without havingto complete additional materialtraining, experience, examinations orassessments. The Act recognizes thatOntario regulators can set standards
that are considered necessary to protectthe public. At the same time, itencourages regulators to work withtheir colleagues across Canada toachieve common standards, wherepossible.
Other key elements of the legislationinclude the following:
• Allowing workers to apply for certification in Ontario without having to be a resident of Ontario;
• Allowing the responsible minister toreview a regulator’s practices and take all necessary steps to ensure those practices comply with the Labour Mobility Code that is set outin the Act;
• Enabling the Ontario government toimpose fines on regulators who do not remove mobility barriers such asadditional material testing and training.
Frequently AskedQuestions Regarding theOntario Labour Mobility Actand CASLPO’s RegistrationRequirements
What impact will this have onCASLPO members?
Audiologists and speech-languagepathologists who currently work inOntario will not be directly affected.The Act applies to individuals fromother regulated provinces who areapplying to work in Ontario. If you arethinking of moving to anotherprovince, be aware that each provincehas been directed to enact labourmobility legislation which will facilitatethe transfer of workers from onejurisdiction to another. Check with theprovince in question to see if itslegislation has been approved.
Ontario Legislature Passes Labour Mobility ActBy Karen Luker, Deputy Registrar, and Colleen Myrie, Manager of Registration

My agency is considering hiring anaudiologist from Alberta. What doesthis legislation mean for us?
The intent of the legislation is to allowpractitioners to move from oneregulated province to another with-out having to undergo additional training, experience, examinations orassessments. If the applicant is amember of the Alberta College ofSpeech-Language Pathologists andAudiologists, CASLPO cannot imposeadditional requirements, with a fewexceptions. For example, a regulatorybody can require an applicant toprovide evidence of good character andlanguage proficiency.
Is the Canadian Alliance of Regulatorsdoing anything to facilitate labourmobility?
In the last eight months, the CanadianAlliance of Regulators (CAR) has beenworking on the following:
• harmonizing registration standards for all Canadian graduates, and
• outlining a process for the consistentassessment of credentials and equivalencies for internationally trained applicants.
CAR will be completing this work in thenext few months, and will be seekingthe adoption of national standards fromits constituents later this year.
I thought there was already a mutualrecognition agreement between theprovinces to allow SLPs andaudiologists to be recognized in allprovinces?
A Mutual Recognition Agreement wasin fact signed in 2001, and amended in2005. This agreement ensured that amember in good standing in a regulated
province would be accepted by anotherregulated province without additionalscrutiny.
The Agreement on Internal Tradeendorsed by the provincial premiers inJanuary 2009 has altered theapplicability of the professions’ MutualRecognition Agreement (MRA). Forinstance, the AIT applies only toregulated provinces. Unregulatedprovinces are no longer recognizedunder this agreement.
I am a Speech-Language Pathologistworking in Ontario. I am consideringa move to British Columbia. I haveheard that BC is requiring that allapplicants pass the CASLPAexamination prior to becomingmembers of their College. Is this true?
Since the AIT was amended in January2009, every province has been directedto develop and approve legislation tosupport their commitment to theAgreement. As of the date ofpublication of this issue of CASLPOToday, Bill 9 – 2009 had received firstreading in British Columbia’sParliament. The Bill allows certifiedworkers from other jurisdictions topractice their occupations in BC inaccordance with the AIT, and, inparticular, provides that BC regulatorsmust consider and apply the provisionsof the AIT when workers who arecertified for an occupation in asignatory jurisdiction apply to obtainBC certification for that occupation.British Columbia’s College bylaws statethat a member in good standing ofanother regulated province does notneed to complete the CASLPAexamination.
I have had a query from someone whohas been working in Halifax for sixyears, who may want to fill a maternityleave at our centre. I feel he is well
qualified and want the process to be asquick as possible. What are therequirements?
Because Nova Scotia is not a regulatedprovince, this applicant will not cometo Ontario with a certificate ofregistration from a regulator, and theOntario Labour Mobility Act does notapply to him. CASLPO will have toverify his credentials. If the applicantgraduated from an accredited Canadianuniversity, he would be granted acertificate of registration following theregular application process. If hegraduated from a university outside ofCanada, his application must undergoa full assessment of his academiccredentials and clinical experience.
I recently spent some time in England,and worked with a few speech-language pathologists who said theymight be interested in coming toCanada. They have lots of experience,and have indicated a willingness towork in my remote community. Canthe Labour Mobility Act help them?
Unfortunately, no. The Ontario LabourMobility Act (and the Agreement onInternal Trade) is meant to facilitate thetransfer of licensed workers from oneregulated Canadian province toanother. The SLPs will have to submit acomplete application to CASLPO, andmust undergo a full assessment of theiracademic credentials and clinicalexperience. If, however, anotherCanadian province had granted them acertificate of registration (if they hadworked in Manitoba prior to coming toOntario, for example), the Act wouldapply and no additional requirementswould be imposed on them at this time.
What about graduates of Americanprograms? Many of them are certifiedby the American Speech-Language-Hearing Association (ASHA). Can they
CASLPO NEWS

work in Ontario based on the mutualrecognition agreement?
CASLPO has always conductedassessments of American applicants’credentials as it is the regulator’smandate to do so; it cannot assign thisresponsibility to an association. ASHA’smutual recognition agreement is signedwith CASLPA, which provides a
voluntary certification program.Graduates of American universities,even if they are Canadian citizens, haveto undergo a full assessment of theiracademic and clinical credentials as doother internationally trained applicants,in order that CASLPO can ensure thatthe public of Ontario has access tocompetent professionals. It should alsobe noted that ASHA’s credential
assessment is based on differentrequirements than those of CASLPO,therefore an “automatic” transfer is notpossible.
Questions related to the OntarioLabour Mobility Act or the College’sregistration process may be addressed toColleen Myrie at [email protected] orKaren Luker at [email protected].
CASLPO NEWS
The Ontario and federalgovernments plan to merge the 8%
Ontario Retail Sales Tax with the 5%federal Goods and Services Tax (GST)into the new 13% Harmonized SalesTax (HST) on July 1, 2010. This new taxwill be federally administered and willuse the same tax base and structure asthe federal GST, with few exceptions.
In the past the College of Audiologistsand Speech-Language Pathologists ofOntario (CASLPO) has not beenrequired to charge GST on its annualmembership fees. Going forward,because “membership fees” currentlyare exempt from GST and HST in thoseprovinces where HST is currentlycharged, CASLPO is advised that it willnot be required to charge the new HSTbeginning on July 1, 2010 on itsmembership fees in Ontario.
However, CASLPO members in privatepractice in Ontario (who supply and bill audiology or speech-languagepathology services) will need todetermine whether or not they will berequired to charge the new HST ontheir billings beginning July 1. Because
each member’s circumstances areunique to them, they should consultwith their tax adviser to determinewhether or not to become HST-registered.
A broad guideline is that if a member iscurrently exempt from having to chargethe 5% GST, it is likely that such amember will continue to be exemptfrom having to charge the new 13%HST on the services they provide andinvoice on or after July 1, 2010. And if amember is currently GST-registeredand is required to charge the 5% GST, itis likely that such a member will berequired to charge the new 13% HST onthe services they provide on or after July1, 2010, regardless of when they bill forthose services (before or after July 1).
If a member is currently exempt fromhaving to charge the 5% GST as a “smallsupplier,” they should note that theyhave to register for GST/HST when theyno longer qualify as a small supplier.That occurs when their total worldwidetaxable supplies of goods and servicesexceed the small supplier limit of$30,000 in a single calendar quarter or
in four consecutive calendar quarters.
This link to the Canada Revenue Agency(CRA) website provides information tohelp members decide if they need orwish to register for GST/HST, and itdescribes options they may have insetting up a GST/HST account.http://www.cra-arc.gc.ca/tx/bsnss/tpcs/gst-tps/rgstrng/menu-eng.html
This link to CRA provides memberswith information on how the GST/HSTworks, what is the harmonized sales tax(HST) and what CRA defines as taxable,zero-rated, and exempt supplies.http://www.cra-arc.gc.ca/tx/bsnss/tpcs/gst-tps/gnrl/menu-eng.html
At the time of this writing, some of thetechnical details and forms are not yetavailable. This article cannot encompassevery situation and it should not berelied upon by CASLPO members tomake taxation and business decisions. Itis best to speak to a taxation expert whocan advise you on your own particularcircumstances and taxation status.
A Quick Guide to the Harmonized Sales TaxBy Gregory P. Katchin, Director of Finance

If a member is no longer practising inOntario and chooses not to renew theirmembership with CASLPO, themember must officially resign from theCollege rather than let theirmembership lapse. To resign from theCollege, a member must send aresignation letter to the Collegeindicating the effective date and thereason for their resignation or completethe resignation section of the paperversion of CASLPO’s AnnualRegistration Renewal Form.
Once a certificate is suspended, apermanent record of the suspension
must be entered in the register. Thisinformation will be included on allrequests for verification of themember’s registration status with theCollege.
Each year, the College publishes a list ofsuspended members. The main purposeof this list is to alert employers ofaudiologists and speech-languagepathologists as to which members aresuspended and might be continuing topractise, unaware of their suspension.
The following individuals weresuspended on February 2, 2010 for
failure to complete the annual renewalrequirements for 2009/2010 inaccordance with section 24 of theHealth Professions Procedural Code:
Reg # Member Name
1060 Jean Maureen Bale1668 Danielle Kaplan2162 Andrew Rekret2404 Erin Yuet Tjam3024 Josée Lucie Levasseur4573 Beverly Ann D'Cunha5062 Sarah Jane Schwab5073 Yang B. Kim5170 Shara Leanne Futa
CASLPO NEWS
Members Suspended for Failure to Complete theAnnual Renewal Requirements For 2009/2010By Gregory Katchin, Director of Finance and Colleen Myrie, Manager of Registration Services
1. Why Was I Selected?
Luck of the draw! Every year 250members are randomly selected by anoutside information technology serviceto submit their Self Assessment Tool(SAT). The 30 members who areselected for the peer assessment areselected from among the 250. However,the 30 members are selected beforeCASLPO receives their SATs so there isno possibility of selecting the membersfor peer assessment based on how theyfilled out their SAT. It is completelyrandom. Once selected for a peerassessment, though, the member is thenremoved from the general pool orsubsequent selection for five years.
2. If there are indicators identified aspartially compliant or non-compliantduring my peer assessment, will I bereferred to the Inquiries, Complaints,and Reports Committee-ICRC?
No. The Quality Assurance Program isthen intended to be a practiceenhancement process rather than apunitive process. The Peer Assessors areexperienced and skilled at identifyingareas for enhancement and providingsuggestions for better ways to managepractice challenges. Similarly, theQuality Assurance Committee thatreviews the peer assessment reportsfocuses attention on practiceenhancement and will generate
suggestions for improvement for themember. Furthermore, the RegulatedHealth Professions Act, 1991 does notallow information about a member thatcomes to the Quality AssuranceCommittee to be shared with any otherCommittee of CASLPO.
3. Will the peer assessment focus onmy clinical skills?
No. The peer assessment process doesnot include observing members withpatients/clients so it is not possible toevaluate this aspect of your practice.Primarily the assessment is limited todocument reviews and conversationswith you. Although some aspects of
Were You Selected For a Peer Assessment This Year?6 Top Questions Answered
By Carol Bock, Deputy Registrar

your knowledge of the practicestandards will reflect to some degreeyour clinical practice, this process doesnot attempt to evaluate your clinicalskills.
4. Can I count Continuing LearningActivity Credits (CLACs) that are notrelated to my goals?
No. All Learning Activities must beconnected to a Learning Goal. However,you can revise your goals so that yourLearning Activities do relate. YourLearning Goals are not set in stone andcan be revised at any point to includelearning opportunities when they ariseand to address practice demands as theychange.
5. Once I have submitted my packageof evidence is there any opportunity tochange or add to it?
Yes. Often members cannot includeevidence for all the indicators due to thefact that some types of evidence are notamenable to copying and transmitting
(e.g., videos, materials that are threedimensional, etc.). For this reason, it isperfectly acceptable to demonstrate theevidence when the peer assessor makestheir site visit. It is preferable to have asmuch evidence sent in as possible; inorder to make the site visit moreefficient and valuable for the member.
6. How is my peer assessor assigned tome?
You are matched with the peer assessorbased on several factors, including, areaof clinical practice, potential conflict ofinterest or bias, geographical proximity,and the preferred time for assessment.Once the best match is made, you willbe provided with the name of yourassessor, usually through email. You willbe granted one veto opportunity, asstipulated in the Quality AssuranceRegulation. Once you accept the peerassessor, then the College informs thepeer assessor, provides them with thenecessary contact information and thepackage of evidence from you. It is thenup to you and your peer assessor to
arrange a site visit. It should be notedthat because of the limited number ofpeer assessors, the match is not alwaysperfect. The peer assessment is intendedto evaluate practice standards that applyacross all settings and does not requireassessors to have precise knowledge ofevery practice setting. You can be sure,however, that your peer assessor willhave had practical experience workingwith the populations that are on yourcaseload.
The peer assessment process is designedto enhance your practice and is bestviewed as an opportunity to developprofessionally. However, it is notunusual to feel some apprehension oruncertainty. If you have any questionsat any point in the peer assessmentprocess or you if would like the benefitof speaking with other members who have been through the process, do not hesitate to contact Carol Bock at416-975-5347, toll-free at 1-800-993-9459 x 227, or via email at [email protected].
CASLPO NEWS

FEATURE
Hercule Poirot and Miss Marple solvedmany a mystery under British crimewriter Agatha Christie’s pen, but thegrande dame of mystery novels herselfmay help unravel one of the greatestmysteries – Alzheimer’s disease.
At a conference in March 2009,University of Toronto English professorIan Lancashire and computer scienceprofessor Graeme Hirst presented apaper entitled, “Vocabulary Changes inAgatha Christie’s Mysteries as anIndication of Dementia: A Case Study.”This paper describes the results of afascinating study in which the works ofAgatha Christie were analyzed andcompared for specific aspects of writtenlanguage. The results were nothingshort of astounding.
Regina Jokel, speech-language path-ologist, part-time scientist at Baycrestand assistant professor of speechpathology at the University of Toronto,
was approached as a consultant to theresearch because of her expertise indementia, through her course,Neurocognitive CommunicationDisorders.
The researchers examined the first50,000 words within 14 of Christie’sworks, spanning her 53-year writingcareer. These 14 included her earliesttitles, The Mysterious Affair at Styles,published in 1920 when she was 30, andThe Secret Adversary, published twoyears later at age 32, as well as her finalthree novels, which she wrote in her 80s:Nemesis (1971), Elephants CanRemember (1972), and Postern of Fate(1973), as well as nine others over herlifetime. Jokel says they examined threeaspects of Christie’s writing: vocabularyrichness, specificity of words, andamount of repetition.
The first aspect, vocabulary richness,was based on the number of differentwords she used in each book. Theydiscovered a significant decline with agein the size of her vocabulary from herearlier to her later works. In fact, theword types fell by one fifth, and by thetime she wrote Elephants CanRemember, when she was 81, hervocabulary had dropped by nearly 31%. The second aspect they looked at wasthe frequency of use of indefinite terms,such as “thing,” “anything,” or“something.” The analysis showed thatChristie’s use of vague terms increasedsignificantly with age, from 0.27% inher first book to 1.23% in her last. Thefinal aspect studied was the number ofrepeated phrases. Once again, theyfound a decline in her writing as sheaged, which they described as a declinein lexical richness. In their paper, the
researchers explained that, while bothindefinite words and repetitionsincrease with normal aging, they do sosignificantly more in the language ofpeople with Alzheimer’s disease.
This analysis was not the first of itskind. In fact, it confirmed the results ofa 2004 study by Peter Garrard of theInstitute of Cognitive Neuroscience atUniversity College London. Garrardcarried out a similar study on the worksof British novelist Iris Murdoch, whohad been diagnosed with Alzheimer’sdisease at the age of 76, the yearfollowing the publication of her finalnovel. Believing that evidence ofMurdoch’s dementia was apparent inher writing prior to her diagnosis,Garrard and his colleagues comparedher early books with her final one.Using the same three aspects, theyfound very similar results to those in theU of T study – her language hadbecome simpler with age, and hervocabulary had shrunk.
Though Christie was never assessed for,or diagnosed with, Alzheimer’s diseaseor any other type of dementia, her laterworks were described as “muddled andmeandering,” and some believe hernovel Elephants Can Remember mighthave been a sign of her defensivenessover her declining mental function. Intheir paper, the authors say, “…her lastnovels reveal an inability to create acrime solvable by clue-detectionaccording to the rules of the genre thatshe helped to create.”
Jokel says this research was only abeginning. “What was published wasthe first part of the research,” she says.But their findings only opened up a
Agatha Christie – Helping to Unravel the Mystery ofAlzheimer’s Disease
By Sherry Hinman
Agatha Christie

host of other questions, which led tofurther research. “The second part isnot yet published so I can’t say toomuch about it.” She did say that theyfound some things they expected, somethey didn’t expect, and some they arestill trying to reconcile. “The vocabularyfindings are well documented, but manyof the other measures had not beenused previously.”
It is reasonable to question the degreeto which these findings are attributableto Alzheimer’s disease and are not justpart of the normal aging process. Jokelsays there are “several really goodstudies done on the written language ofAlzheimer’s. While some aspects oflanguage do decline with normal aging,vocabulary is something that ‘getsbetter with age,’ and this is especiallytrue of seasoned writers. With normalaging, we get a little less specific, andour retrieval is somewhat slower, butour vocabulary becomes richer.”
Jokel points out that slower retrievaltime doesn’t affect written languagenearly as much as it does spokenlanguage. “Written language isforgiving,” she says. “We can slave overone word, and this is more acceptablethan in speech.”
In a Macleans magazine articlepublished in April 2009, Dr. MorrisFreedman, head, Division of Neurology,and Director, Behavioural NeurologyProgram at Baycrest, is quoted as saying
“Because writing is a learned, not anatural skill, it breaks down early.”
Jokel agrees with this statement. “Wetend to lose skills acquired later,” shesays. “Writing is also one of the mostcomplex tasks; if one component breaksdown, the person can’t compensate.Impaired writing is one of the firstlanguage symptoms to be noticeable insomeone with Alzheimer’s.”
Jokel says it was fortunate to be able tocompare the findings about Murdoch,who was diagnosed with Alzheimer’sdisease, with their own about Christie,who was not. They are also comparingboth sets of results with a detailedanalysis of the works of P.D. James.James is an active, productive writerwhose books are still being published atthe age of 89, and whose writing doesnot show any signs of decline.Interestingly, these three authors havemuch in common: all are female, olderwriters, in the mystery genre.
While the findings are tantalizing, onemight ask how applicable they are to thegeneral public. After all, not manypeople are published authors; can theresults be extended in a useful way tothe rest of the world? Jokel observes thatmany people, after they leave school,don’t write any more. But with theInternet, there are many more who usewritten language to correspond throughemail, maintain a website, or blog abouttheir experiences. So there may be more
opportunity for writing samples.“People in their 60s and 70s are morecomputer savvy,” she reminds us.
Jokel is unsure where the research willeventually lead. This will be up to “thefathers of the project,” as she refers tothem. Her own interest would be to doa similar analysis to distinguish betweennon-fluent progressive aphasia,semantic dementia (fluent variant ofnon-fluent progressive aphasia) andAlzheimer’s disease. She would like tosee the computer analysis they usedeventually become available toclinicians working with an agingpopulation, and use it for earlydiagnosis of Alzheimer’s and otherdementias.
But that is the future. For now, Jokelsays she is thrilled with how muchpublicity this research has garnered. “Ihave been doing research on languagefor the past 20 years and there’s beenvery little mention of it. This hasbrought language into focus inmagazines that do not usually talkabout it.”
Sherry Hinman is a freelance writer andeditor. She is also a professor in theCommunicative Disorders AssistantProgram, Durham College; workedclinically as an SLP for fourteen years;and served three years on the CASLPOCouncil.
FEATURE

FEATURE
“When I was a little boy, myhobby was marionettes. In a
way, radio is a little like that. Peopledon’t see the person pulling the string.You’re heard but not seen.” AndyBarrie, who recently left his role as hostof CBC Radio One’s enormouslypopular Metro Morning show, truly hasan insider’s perspective on theuniqueness of radio as a mode ofcommunication.
Despite the seemingly one-sided natureof communication in radio, though,Barrie says, “Radio is conversation. And
it’s company. It’s company withsomeone on whom you project whoyou need that person to be.” And if youthink about it, that conversation is oftenone-on-one. “When you’re on theradio,” he explains, “you’re oftentalking to one person at a time. Manytimes, with television, a few peoplewatch together, but people usually listento the radio alone.”
On a given day, Barrie might do asmany as 10 interviews, so he has anexperienced perspective on one-on-onecommunication. “Most conversation iswaiting,” he says. “Communication is asense of engagement and attentiveness.It’s a sense of trust. You convey that youreally want to hear what the otherperson is saying; you’re genuinelyinterested.”
The rich tones of Barrie’s voice havebeen heard over the airwaves for a longtime – 45 years, if you count hisneophyte days in his 20s on TheSuppertime Show at university in NewHampshire. He was born in Baltimore,Maryland, and worked as an announcerand reporter in several U.S. cities untilthe late ‘60s. Then, after he had been inthe army for a year-and-a-half, he gothis orders to be shipped to Vietnam.
Barrie was a conscientious objector, andcrossed the border into Canada in late1969. “It was a fascinating time,” hesays. “Pierre Elliott Trudeau and Nixonwere in power and the contrast wasastonishing. I am grateful to Canada; Iliked being a part of a country thattreasured the individual over thecommunity.” Barrie later received ageneral discharge and became aCanadian citizen.
“It’s really important to realize that,when it comes to immigration, youimmigrate to a city, not a country,”Barrie explains. “I came to Montreal[and CJAD radio] and it was three yearsafter Expo. This was a time ofexcitement. Montreal was feeling goodabout itself.” Barrie says he felt noantagonism toward the United Statesbut left because he became disaffectedwith the war in Vietnam. “Canadaprovided sanctuary.”
Although Barrie has been in Canada for40 years, he still sees being animmigrant as an important piece of hisidentity. This immigrant identity hasblended with the national culture of theCBC – where he’s worked since hemoved to Toronto in 1995 – to becomea critical part of his truly Canadianpersona.
As he leaves the on-air role he has heldat the CBC for the past 15 years, he hashis eye on, among other possibilities,projects that benefit new Canadians.He’s quoted as saying, “What I want todo is find ways that the CBC canproactively support those new to thecountry – those who don’t speak one ofthe official languages – and to educatethem on the culture. That’s what I’d liketo do.”
When asked what he meant by this, hereplied, “I’ve thought about how toeducate someone who is new toCanada. How do they learn words like“Inukshuk” and “Screech”? I can’t thinkof any better way to expose newCanadians than the CBC. I was a newCanadian myself. No one tells youabout the FLQ, Rogers Pass, Terry Fox,the Canada-Russia series. This is the
Andy Barrie: Good Company
By Sherry Hinman
At this fall’s CASLPO-OSLAConference 2010, the luncheonkeynote address will be given byAndy Barrie, long-time host of CBCRadio One’s Metro Morning show.We thought you’d like a sneak peekinto what you can expect from thiswarm and well-respected veteran ofthe airwaves.

‘soft’ part of becoming a Canadian.”
He goes on to describe how the CBCwebsite houses a wealth of material onall subjects Canadian – written, audioand video. “We could make thisinformation available as a resource. Wecould package it specifically for newCanadians,” he says.
A recently published article describesBarrie’s honesty, warmth and“irresistibly self-deprecating wit.” Threeyears ago, he wrote an email to his staffin which he relayed the news that he’dbeen diagnosed with early stageParkinson’s disease. In that email, it’seasy to see evidence of all three of thosequalities as he shared his difficult news.In one line he poignantly wrote,“However there’s one PD symptom thatdoes need mentioning – the muscles ofthe face can sometimes take on anexpression that can look either pissed-off or not-at-home. Of coursesometimes I am p.o.’d or not there. Ifyou’re not sure, ask.”
He’s known for coming straight to thepoint when he’s interviewing others,and was as blunt in his communiqué.“PD is not contagious and it’s not fatal.But it doesn’t go away by itself, and itdoes get worse.” His message was neversugar-coated but it was moving just thesame. He ended it by offering to acceptadvice and answer any questions, andthanked his colleagues “for being, all ofyou, such very human beings.”
While Barrie doesn’t seem to have anydifficulty with his speech, he is awarethat for some people with Parkinson’sit could be affected later on. “I don’twant to gradually erode,” he says. “It’sa bit like dancers who break their leg.It’s sobering to have had a career invoice and possibly lose the ability totalk.”
He also has clear views on hearing andhearing aids. In a radio job he haddecades ago, he says he was exposed to50,000 watts of feedback and “it blewout my hearing.” He’s worn a hearingaid ever since. “It blows me away thatpeople who need a hearing aid don’twear one,” he says. His advice to otherswith a hearing loss? “If you’re askingyourself, ‘When do I need a hearingaid?’ the answer is, When you’reunwilling to inflict the need to repeat,on others.”
On Barrie’s last morning on the MetroMorning show at the end of February,he told listeners, “This is only ‘aurevoir.’” He is not retiring from radio,nor is he leaving the CBC, just the on-air side of the business. In February,when he’d announced his departuredate, he said, “Well, it’s that part of theconversation where it’s time to say, well,enough about me.”
Barrie’s got plenty of plans about howhe’ll carry out his work away from themicrophone, including mentoring newhosts. But his listeners will certainlymiss his voice. Asked how he would liketo be remembered by listeners whothink back to his time on air, he says, “Itgoes back to my definition of radio. Iwant to be remembered as being ‘goodcompany.’ Like someone you’re livingwith or talking to on a long car ride. Notjokes all the time. I want people to say,‘He stimulated, informed andchallenged us’. I want them to say, ‘Hemoved us.’” And there’s not a singledoubt – they will.
Sherry Hinman is a freelance writer andeditor. She is also a professor in theCommunicative Disorders AssistantProgram, Durham College; workedclinically as an SLP for fourteen years;and served three years on the CASLPOCouncil.
FEATURE
FEATURE
In 2007, the Office of the Informationand Privacy Commissioner ofOntario (IPC) issued an order directedto all Ontario health informationcustodians not to transport personalhealth information on laptops or othermobile computing devices unless theinformation was encrypted. Thisdirection was included in a 2007 orderunder the Personal Health InformationProtection Act (PHIPA).
In December 2009, a USB keycontaining the health information ofalmost 84,000 patients who attendedH1N1 flu vaccination clinics in theDurham Region was lost. This resultedin an investigation into the incident by
the IPC, who deemed it a major privacybreach. The main issue related to thefact that the personal healthinformation stored on the USBmemory stick was not encrypted; had itbeen, this would have merely been thephysical loss of a single USB key.
The Privacy Commissioner, AnnCavoukian, was distressed by thisincident in light of the order issued in2007. “Some health informationcustodians are encrypting personalhealth information placed on mobiledevices, while others are encrypting all health information,” says Dr. Cavoukian. “But some custodianshave not yet taken such necessary steps.
Health information custodians cannotwait until they become a victim beforetaking concrete action to protect thepersonal health information, for whichthey are responsible.”
As part of the order issued to theDurham Region following itsinvestigation, Dr. Cavoukian included amessage which is directed to everyhealth information custodian inOntario. The contents of this messageare reprinted below.
Commissioner’s MessageAnn Cavoukian, PhD
Health information custodians inOntario are required under the Act totake reasonable steps to ensure thatpersonal health information isprotected against theft, loss andunauthorized use or disclosure. In 2007,following the loss of a laptop containingpersonal health information, I sent aclear message warning all custodiansagainst storing personal healthinformation on mobile devices, that areespecially vulnerable to both loss andtheft. In Order HO-004, I outlined anew standard to be followed – a multi-layered approach to guard againstunauthorized access to personal healthinformation stored on mobile devices.
It is always preferable to avoid storingany personally identifiable healthinformation on mobile devices.
Safeguarding Information on Mobile Devices
The following is the first of a two-part article on the issue of encryption of personal health information, whichhas garnered much attention in the last few years. The first article summarizes a recent order issued by theInformation and Privacy Commissioner/Ontario; it outlines some of the risks and methods associated withdealing with personal health information on mobile devices. The second part of the article, to be published inthe next issue of CASLPO Today, will propose specific encryption methods and solutions which may be used bymembers. CASLPO hopes that these articles will encourage members to become more aware of the need toensure the protection of personal health information on all electronic devices, and to discuss encryption needswith their employers.

However, where personal healthinformation must be stored on suchdevices, the following measures arenecessary:
• only the minimal amount of information necessary should be stored, and for the minimal amount of time necessary to complete the work;
• whenever possible, personal health information should be de-identifiedor coded, in a manner such that the identities of the individuals whose personal health information is storedon the device could not be readily ascertained if the information were accessed by unauthorized persons;
• if the information is coded, the codethat is needed to unlock the identitiesof individuals should be stored separately on a secure computing device, such as a central server in a health care facility;
• the use of strong password protection; and, most important;
• the use of strong encryption.
The Act requires custodians to notifyindividuals if their personal healthinformation is lost, stolen or accessed byunauthorized persons. Consequently,privacy breaches tend to be both time-consuming and costly, and often resultin irreparable damage to a custodian’sreputation and image. While I acceptthat custodians may not be able tototally eliminate the loss or theft ofmobile devices, what I cannot accept isthat the information contained thereinis not encrypted. Unauthorized accessto health information stored on thesedevices that happen to be lost or stolenmay clearly be prevented through theuse of encryption technology. However,despite strong incentives to avoidprivacy breaches and the availability ofencryption to prevent such breaches,unencrypted mobile devices continuedto be used. This is both distressing andcompletely unacceptable.
Multiple factors may contribute to thefailure to adequately safeguard personalinformation. First, there may be a lack of understanding about thevulnerabilities, threats, and risks to theinformation stored on mobile devices,or a lack of awareness about whatconstitutes reasonable safeguards forpersonal health information stored onsuch devices. Second, there may bechallenges in implementing enterprise-wide solutions that allow custodians toeffectively manage and control themanner in which all of their agents andelectronic service providers collect, use,disclose, retain, transfer, and dispose ofpersonal health information on theirbehalf. Third, while this is difficult tobelieve, some custodians may haveinterpreted Order HO-004 narrowly asapplying only to mobile computingdevices such as laptops and personaldigital assistants, without recognizingthat other portable data storage devices,such as USB memory sticks, posesimilar risks. The stolen laptop thatresulted in HO-004 and the lost USBmemory stick resulting in the currentOrder are instances of a growing classof security and privacy problems,namely data leakage and data lossassociated with all portable storagedevices. My office is taking steps toensure that all of these issues areaddressed.
As the health sector moves towardselectronic health records and electronicsystems of personal health information,public confidence in custodians’ abilityto protect all types of health records isessential. Privacy breaches stemmingfrom the use of technology, without thenecessary privacy and securitysafeguards such as encryption, willinevitably be viewed as harbingers ofthe state of privacy once the healthsector makes the transition to electronichealth information. In my view, this iscompletely understandable. After all, ifcustodians cannot be trusted to protect
the personal health information storedon a simple portable device such as aUSB key, how will they ever manage toprotect the massive amounts ofpersonal health information that willeventually reside within complexsystems of interoperable electronichealth records?
It is vital that custodians recognize that any breaches stemming from the improper implementation ofinformation technologies will not onlybe costly for the responsible custodian,but will also reinforce skepticism aboutthe health sector’s ability to protectprivacy in context of eHealth, ingeneral. Increased skepticism will likelyhave a chilling effect on the acceptanceand adoption of all types of new healthinformation technology, includingelectronic health records. Given recentsetbacks in the eHealth agenda inOntario, additional barriers or delaysare the last thing the health sector needsat this point in time. Therefore, it isessential that all custodiansdemonstrate both their commitmentand their capacity to protect personalhealth information stored in all
FEATURE

formats, now. Otherwise, the transitionto the use of electronic health recordswill be far from smooth.
In recognizing the broader implicationsof large scale breaches of healthinformation and the need to ensure thatimmediate steps are taken to preventavoidable breaches involving mobiledevices, I approached the Ministry ofHealth and Long-Term Care. They havecommitted to work together with myoffice to develop a communicationsstrategy to help ensure that the entirehealth care sector in Ontario adoptsreasonable safeguards to protectpersonal health information stored onall types of electronic devices. As a firststep in this strategy, I contacted thechief medical officer of health for theprovince of Ontario who issued amemo to all medical officers of health,warning about the need to encryptpersonal health information onportable devices such as USB memorysticks. A more detailed strategy forpromoting awareness and complianceamong all health informationcustodians is currently underdevelopment and will be finalized earlyin 2010.
However, enhanced awareness is onlypart of the solution. As storage capacityincreases while costs decreasedramatically, portable storage devicesare proliferating in informationintensive sectors, such as the healthsector. In this environment, it will be achallenge for health informationcustodians to establish effectivemanagement and control over all oftheir data resources, as well asmaintaining effective accountability forthe standards required under the Act,and widely expected by the public.
As I have stated over the years, in lightof the proliferation of new informationand communication technologies, the future of privacy requires a
comprehensive and proactive approach,which I have called Privacy by Design,whereby both privacy and security are effectively baked into theinformation eco-system, end-to-end,and throughout the entire data life-cycle, from initial collection through tofinal disposal.
While encryption is a key component ofany security solution for protectinghealth information on portable devices,it must be deployed in a holistic andproportional manner in order to betruly effective. Depending on theoperating context, some encryptionsolutions are better than others. Thosethat are added on, after the fact,requiring users to actively encrypt filesby creating passwords or launching asoftware program every time that healthinformation is stored on a portabledevice, may be less effective than otherencryption solutions. Weak or stolenpasswords effectively negate thepotential security benefits ofencryption. Confusing or complexsoftware interfaces and protocols willalso result in users abandoning securesystems and resorting to insecure“workarounds.” Users also may beunaware that when encryptedinformation is transferred from onestorage device (e.g., laptop computer)to another (e.g., a USB key), theencryption does not necessarilyaccompany the data. Once the data isintentionally or unintentionallydecrypted back to plaintext, it is outthere in plain view, becomingvulnerable to a wide range ofunintended uses.
Doing away with mobile devicesentirely by locking down all USB ports,in favour of the exclusive use of securechannels and “thin clients,” is anotherapproach that may be feasible in someinstances but not others. Thin clients,sometimes described as “dumbterminals,” are display and input
devices which do not process data andinput locally, but rather transmit inputto a computer to which they areconnected and display the resultingoutput. They often have limited localdata storage and output capacities.Since the vast majority of the processingof information is done centrally in suchsystems, the security risks are generallyconfined to the central server. However,while it may be easier to manage thesecurity risks, establishing andmaintaining secure channels and thinclients tends to be operationallycomplex and costly to the enterprise,requiring employees to manageidentification and authenticationcredentials in a consistently secure way.Additionally, locking down USB portsacross an enterprise may rob anorganization of the benefits ofconnecting other useful, risk-freedevices to those ports, such as a mouseor keyboard.
Ideally, organizations should implemententerprise-wide encryption solutionsthat would only permit the use ofauthorized portable storage devices toconnect to specifically-authorized USBports, where the encryption is bothautomatic and seamless. Only deviceswith authorized USB ports would beable to view, access and decrypt the datastored on an authorized portablestorage device. Thus, in the event thatan authorized portable storage devicewas lost or stolen, any personal healthinformation stored on the device wouldbe inaccessible to anyone who found it.Further, it would simply not be possibleto use an unauthorized mobile device
FEATURE

with such a protected system. Themanagement of this type ofarrangement would have to becentralized, easy to set up andadminister, and, ideally, low in cost. Inaddition, all transactions would alsoneed to be logged.
A local Ontario company, CryptoMill,has developed such an enterprise-classsecurity solution that offers this degreeof functionality. Their solution calledSEAhawk, allows organizations toeffectively lock down information assetsto registered devices only, such as USBmemory sticks.
Had such a solution been implementedin Durham Region, the personal healthinformation contained on the USBmemory stick that was lost would havebeen encrypted in a manner that wouldhave locked out all unauthorizedparties, only allowing an authorizedcomputer to decrypt it. Further, anyfiles stored on the USB memory stickwould essentially be invisible to anyonewho found it or stole it. Anyone,including staff, plugging the USBmemory stick into their own computerwould either find an encrypted vault –an invisible directory, or else beprompted to format an unrecognizeddrive, effectively erasing its contents.
If an encrypted USB memory stick waslost, there would be no cause for alarmon the part of the organization, whichwould have a high degree of confidencethat the stored data would not becompromised. There would be no needto invoke the time-consuming andexpensive breach management processinvolving notification, investigation,and remediation.
To their credit, both CryptoMill andDurham Region have been workingtogether non-stop to apply theSEAhawk encryption solutionthroughout the Durham Region. With
the release of this order, its adoptionwill be well underway.
Privacy by Design is systemic,embedded, and proactive in nature,thereby serving to prevent privacymishaps before they occur. It comesbefore the fact of a data breach, not after.While it is true that we cannot eliminatehuman error, we most certainly caneliminate personal information frombeing revealed, in the process. Humanerror, in this instance, is not anacceptable excuse. While the loss of aUSB memory stick may not have beenprevented, the loss of personallyidentifiable data certainly could havebeen. Don’t blame human error –blame the lack of encryption of easilylost or stolen mobile devices.
CASLPO would like to extend its sinceregratitude to the Information andPrivacy Commissioner/Ontario forpermission to reprint this information.
FEATURE
WINDSOR ESSEX COUNTY PEDIATRIC FEEDING/DYSPHAGIA GROUP
presents
SUZANNE EVANS MORRIS, Ph.D. “FEEDING THE WHOLE CHILD:
A Mealtime Approach”
“INSPIRATION”
CLASSIFIED