safety and efficacy of pegfilgrastim in patients receiving myelosuppressive chemotherapy
TRANSCRIPT

Safety and Efficacy of Pegfilgrastim in Patients ReceivingMyelosuppressive Chemotherapy
Jeffrey Crawford, M.D.
The major dose-limiting toxicity associated with myelosuppressivechemotherapy is neutropenia, which can be ameliorated with proactiveadministration of granulocyte colony-stimulating factor (G-CSF).Pegfilgrastim is a long-acting G-CSF, recently approved by the Food and DrugAdministration. The efficacy and safety of pegfilgrastim administeredonce/chemotherapy cycle have been evaluated in clinical trials involvingpatients treated with myelosuppressive chemotherapy for breast cancer, lungcancer, non-Hodgkin’s lymphoma, and Hodgkin’s disease. Two pivotal phaseIII trials in patients with breast cancer showed that pegfilgrastim is as effectiveas filgrastim regarding the primary efficacy end point, which was duration ofgrade 4 (severe) neutropenia in cycle 1 of myelosuppressive chemotherapy.Secondary end points were the frequency of fever with neutropenia (febrileneutropenia), duration of neutropenia in cycles 2–4, depth of the absoluteneutrophil count (ANC) nadir, and time to ANC recovery in cycles 1–4.Once/cycle pegfilgrastim 100 µg/kg or 6 mg was as safe and effective as dailyfilgrastim 5 µg/kg in reducing the frequency and duration of severeneutropenia. A trend toward a greater reduction in the overall frequency offebrile neutropenia with pegfilgrastim was observed. The availability ofpegfilgrastim simplifies the use of prophylactic G-CSF, with the potential toincrease patient convenience and adherence in management of chemotherapy-induced neutropenia.(Pharmacotherapy 2003;23(8 Pt 2):15S–19S)
Chemotherapy-induced neutropenia and itscomplications are the primary dose-limitingadverse events associated with cytotoxicchemotherapy.1, 2 Febrile neutropenia is a life-threatening complication of myelosuppressivechemotherapy and can result in hospitalizationand treatment with empiric broad-spectrumantibiotics. Granulocyte colony-stimulatingfactor (G-CSF) acts on the hematopoietic systemto stimulate the proliferation and differentiationof neutrophil precursors, producing mature,functional neutrophils. During infection withneutropenia the amount of endogenous G-CSF inthe blood increases, reducing neutrophil
maturation time from 5 days to 1 day andresulting in a rapid release of mature neutrophilsfrom the marrow into the circulation while alsoenhancing neutrophil function.1, 3
Purifying and cloning a recombinant human G-CSF, filgrastim, facilitated development of thedrug for clinical administration. Filgrastim wasthe first G-CSF approved by the Food and DrugAdministration (FDA) for decreasing thefrequency of infection, as manifested by febrileneutropenia, in patients treated with myelo-suppressive chemotherapy.4 It is indicated foradministration in patients with nonmyeloidmalignancies treated with myelosuppressivechemotherapy that is associated with a significantfrequency of grade 4 (severe) neutropenia withfever (febrile neutropenia).4
Filgrastim has revolutionized the ability tosupport patients treated with chemotherapy.
From the Department of Medicine, Duke UniversityMedical Center, Durham, North Carolina.
Address reprint requests to Jeffrey Crawford, M.D., DukeComprehensive Cancer Center, Duke University MedicalCenter, P.O. Box 25176, Morris Building, Durham, NC27710; e-mail: [email protected].

Supplement to PHARMACOTHERAPY Volume 23, Number 8, 2003
When administered in conjunction withmyelosuppressive chemotherapy 24 hours afterthe start of chemotherapy, filgrastim has led to areduction in the frequency of febrile neutropeniaand infections; the frequency, duration, andseverity of intravenous antibiotic therapy; andhospitalizations for febrile neutropenia.5–7 Inaddition, when filgrastim is started in the firstchemotherapy cycle, it improves delivery of theplanned chemotherapy dose and reduces delaysin treatment.1, 6 Moreover, filgrastim is welltolerated; the most common adverse event isbone pain, which is generally manageable withnonnarcotic analgesics.4
A drawback to filgrastim is its short serumhalf-life of approximately 3.5 hours. Its rapidclearance from the circulation necessitates dailyinjections during the neutropenic period,complicating its administration in many patients.Proteins to which polyethylene glycol (PEG)molecules have been attached often have slowerclearance, longer serum half-lives, extendedbiologic activity, and less immunogenicity andantigenicity.8, 9 Pegfilgrastim, created by thecovalent binding of a 20-kD PEG molecule to theN-terminal methionine residue of the filgrastimprotein, has reduced renal clearance and acorresponding increase in serum half-life, whilemaintaining its safety and efficacy.10 Thepharmacokinetic characteristics of pegfilgrastimand the development of pegfilgrastim bypegylation are discussed elsewhere in thissupplement11, 12; the clinical efficacy and safety ofpegfilgrastim are discussed here.
Efficacy of Pegfilgrastim in Clinical Trials
Early Efficacy Studies
A dose-ranging study that compared pegfilgrastim30, 100, and 300 µg/kg given once/chemotherapycycle with filgrastim 5 µg/kg administered dailywas conducted in patients with non–small celllung cancer.13 Thirteen patients were givencarboplatin at an area under the serum concen-tration–time curve (AUC) of 6 mg/ml • minute.They were also given paclitaxel 225 mg/m2 as a24-hour infusion followed by growth factorsupport 24 hours later. The study drugs werecompared before and after cycle 1. Both pegfil-grastim and filgrastim given in the absence ofchemotherapy produced peaks in absoluteneutrophil count (ANC) on day 3 after theiradministration. The increase in ANC wassustained longer with a single dose of pegfil-grastim (all three doses) than with 5 daily doses
of filgrastim.13
After chemotherapy, the ANC nadirs occurredon approximately day 7 and were identical (0.1 x103/mm3) with a single dose of pegfilgrastim 30µg/kg and filgrastim 5 µg/kg/day. The neutrophilnadirs were higher with pegfilgrastim 100 and300 µg/kg (0.65 x 103/mm3 and 0.7 x 103/mm3,respectively) in these small cohorts. Serum levelsof pegfilgrastim remained elevated throughoutthe ANC nadir period and rapidly declinedduring neutrophil recovery, indicatingneutrophil-mediated clearance.13
Another dose-finding study compared theadministration of a single injection ofpegfilgrastim 30, 60, or 100 µg/kg with dailyinjections of filgrastim 5 µg/kg in patients withbreast cancer treated with doxorubicin anddocetaxel every 3 weeks for at least four cycles.14
Administration of study drugs was started 24hours after chemotherapy was begun. Thefrequency of severe neutropenia in cycle 1 was95%, 90%, and 74% in patients who were givenpegfilgrastim 30, 60, and 100 µg/kg, respectively,and 76% in those given filgrastim. The mean ±SD duration of severe neutropenia in cycle 1 was2.7 ± 1.3, 2.0 ± 1.2, and 1.3 ± 1.1 days withpegfilgrastim 30, 60, and 100 µg/kg, respectively,and 1.6 ± 1.3 days with filgrastim. It waspossible to deliver more than 90% of thechemotherapy doses on time in patients given asingle dose of pegfilgrastim 100 µg/kg. Theplanned dose of the chemotherapy (defined as≥ 80% of the planned dose in cycle 1) was alsodelivered in all cycles.14
Similar protection against chemotherapy-induced neutropenia was seen in patients withnon-Hodgkin’s lymphoma or Hodgkin’s diseasewho were given a single dose of pegfilgrastim 100µg/kg (29 patients) or filgrastim 5 µg/kg/day (31patients) 24 hours after a 5-day ESHAP chemo-therapy regimen of etoposide 40 mg/m2/day ondays 1–4, methylprednisolone 250–500 mg/dayon days 1–5, cisplatin 25 mg/m2/day on days 1–4,and cytarabine 2000 mg/m2 on day 5, repeatedevery 21–28 days.15 The frequency of severeneutropenia with pegfilgrastim and filgrastim inthe first chemotherapy cycle was 69% and 68%,respectively; the frequency in the second cyclewas 23% and 36%, respectively. Mean ± SDduration of severe neutropenia was 2.8 ± 2.6 dayswith pegfilgrastim and 2.4 ± 2.7 days withfilgrastim in the first cycle and 0.4 ± 0.9 and 0.6± 1.1 days in the second cycle.15 Patients treatedwith filgrastim were given a median of 11injections/cycle.
16S
SAFETY AND EFFICACY OF PEGFILGRASTIM Crawford
Pivotal Clinical Trials
Two large randomized controlled phase IIIclinical trials compared once/chemotherapy cyclepegfilgrastim with daily filgrastim in patientswith breast cancer.16, 17 The trials, which wereidentical in design, differed only in mode ofpegfilgrastim dosing: one used weight-baseddosing of 100 µg/kg,16 the other a fixed dose of 6mg.17 Patients in both studies were treated withdoxorubicin 60 mg/m2 followed by docetaxel 75mg/m2 every 3 weeks for up to four cycles. Onday 2 of each cycle, about 24 hours afterchemotherapy, patients were given a singlesubcutaneous injection of pegfilgrastim followedby daily injections of placebo, or were given dailysubcutaneous injections of filgrastim thatcontinued either for 14 days or until a postnadirANC of 10 x 103/mm3 was reached, whicheveroccurred first. The next chemotherapy cycle wasadministered only in patients with completehematopoietic recovery (defined as ANC > 1 x103/mm3 and platelet count > 100 x 103/mm3).The trials were designed to show the noninferiorityof pegfilgrastim; the primary end point wasduration of severe neutropenia in cycle 1, definedas ANC < 0.5 x 103/mm3. The frequency offebrile neutropenia, duration of severe (grade 4)neutropenia in cycles 2–4, depth of the ANCnadir, and time to ANC recovery were secondaryend points.
A total of 296 patients were treated in theweight-based dosing trial.16 Pegfilgrastim 100µg/kg was noninferior to filgrastim 5 µg/kg/daywith respect to duration of severe neutropenia incycle 1, in which a mean ± SD of 1.7 ± 1.5 dayswas reported with pegfilgrastim and 1.8 ± 1.4days with filgrastim. In cycles 2–4 thedifferences in duration of severe neutropeniawere statistically significant in favor ofpegfilgrastim (Table 1).16 Furthermore, theoverall frequency of febrile neutropenia wassignificantly lower with pegfilgrastim (9% vs
18%, p=0.029), and a trend was observed towardlower frequency of severe neutropenia and higherANC nadir with pegfilgrastim.16
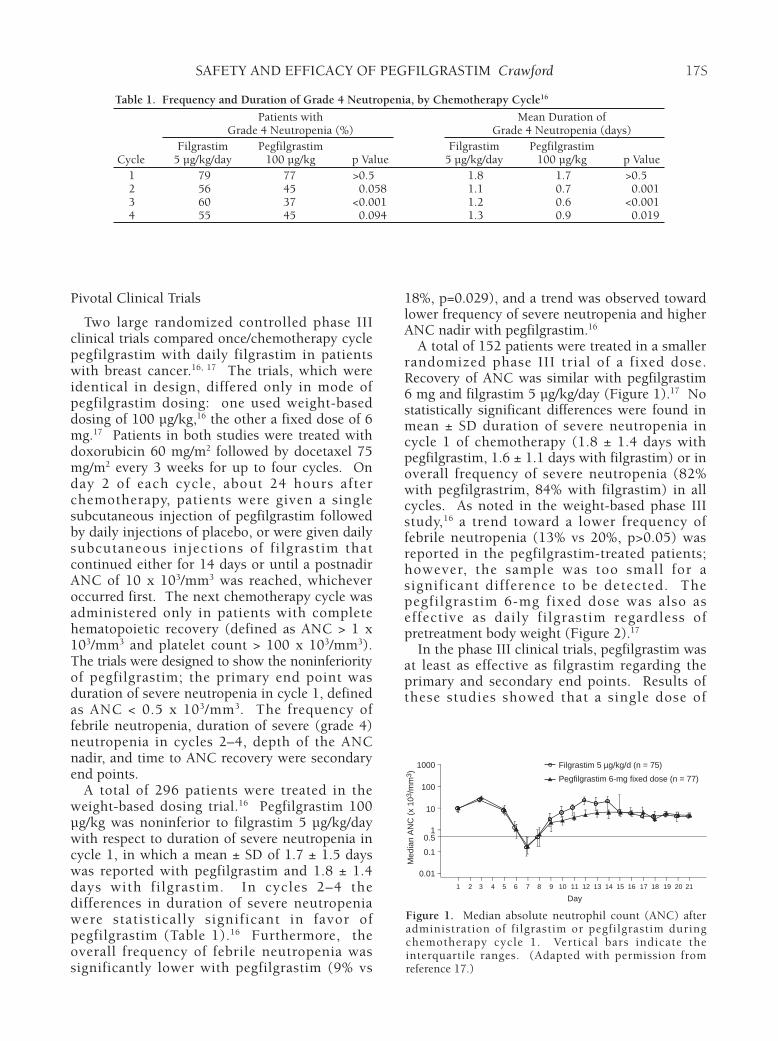
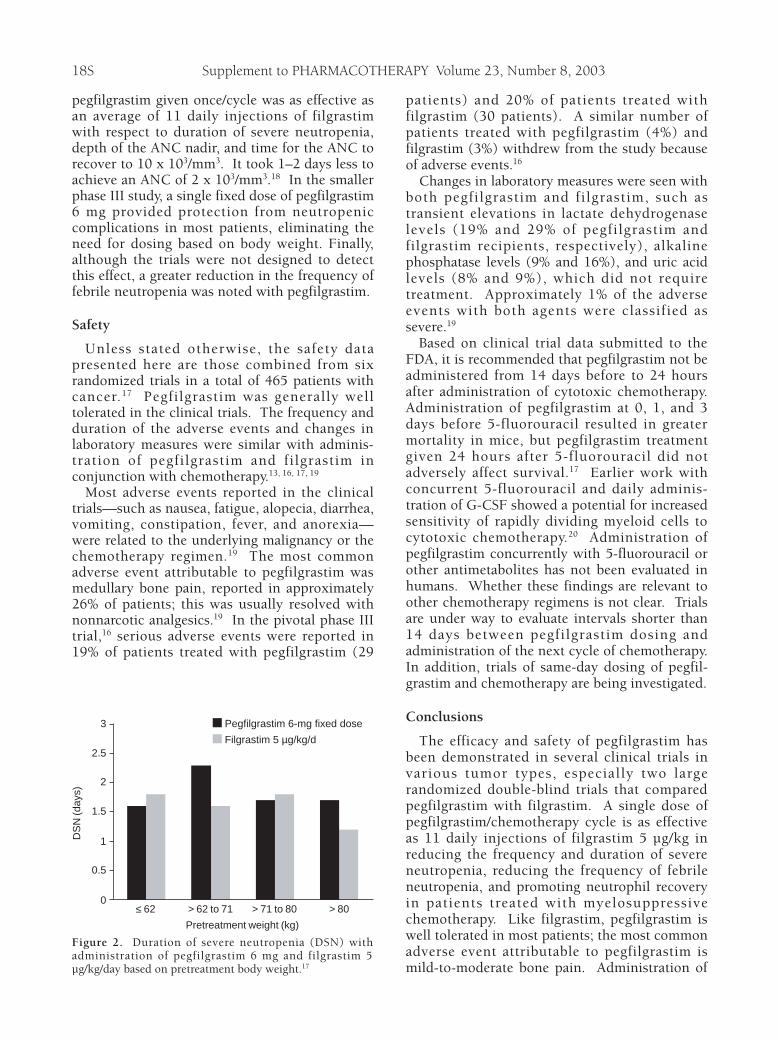
A total of 152 patients were treated in a smallerrandomized phase III trial of a fixed dose.Recovery of ANC was similar with pegfilgrastim6 mg and filgrastim 5 µg/kg/day (Figure 1).17 Nostatistically significant differences were found inmean ± SD duration of severe neutropenia incycle 1 of chemotherapy (1.8 ± 1.4 days withpegfilgrastim, 1.6 ± 1.1 days with filgrastim) or inoverall frequency of severe neutropenia (82%with pegfilgrastrim, 84% with filgrastim) in allcycles. As noted in the weight-based phase IIIstudy,16 a trend toward a lower frequency offebrile neutropenia (13% vs 20%, p>0.05) wasreported in the pegfilgrastim-treated patients;however, the sample was too small for asignificant difference to be detected. Thepegfilgrastim 6-mg fixed dose was also aseffective as daily filgrastim regardless ofpretreatment body weight (Figure 2).17
In the phase III clinical trials, pegfilgrastim wasat least as effective as filgrastim regarding theprimary and secondary end points. Results ofthese studies showed that a single dose of
17S
Table 1. Frequency and Duration of Grade 4 Neutropenia, by Chemotherapy Cycle16
Patients with Mean Duration ofGrade 4 Neutropenia (%) Grade 4 Neutropenia (days)
Filgrastim Pegfilgrastim Filgrastim PegfilgrastimCycle 5 µg/kg/day 100 µg/kg p Value 5 µg/kg/day 100 µg/kg p Value
1 79 77 >0.5 1.8 1.7 >0.52 56 45 0.058 1.1 0.7 0.0013 60 37 <0.001 1.2 0.6 <0.0014 55 45 0.094 1.3 0.9 0.019
Figure 1. Median absolute neutrophil count (ANC) afteradministration of filgrastim or pegfilgrastim duringchemotherapy cycle 1. Vertical bars indicate theinterquartile ranges. (Adapted with permission fromreference 17.)
1 2 3 4 5 6 7 8 9 10 11
Day
12 13 14 15 16 17 18 19 20 21
1000 Filgrastim 5 µg/kg/d (n = 75)
Pegfilgrastim 6-mg fixed dose (n = 77)100
10
Med
ian
AN
C (
x 10
3 /m
m3 )
1
0.1
0.01
0.5
Supplement to PHARMACOTHERAPY Volume 23, Number 8, 2003
pegfilgrastim given once/cycle was as effective asan average of 11 daily injections of filgrastimwith respect to duration of severe neutropenia,depth of the ANC nadir, and time for the ANC torecover to 10 x 103/mm3. It took 1–2 days less toachieve an ANC of 2 x 103/mm3.18 In the smallerphase III study, a single fixed dose of pegfilgrastim6 mg provided protection from neutropeniccomplications in most patients, eliminating theneed for dosing based on body weight. Finally,although the trials were not designed to detectthis effect, a greater reduction in the frequency offebrile neutropenia was noted with pegfilgrastim.
Safety
Unless stated otherwise, the safety datapresented here are those combined from sixrandomized trials in a total of 465 patients withcancer.17 Pegfilgrastim was generally welltolerated in the clinical trials. The frequency andduration of the adverse events and changes inlaboratory measures were similar with adminis-tration of pegfilgrastim and filgrastim inconjunction with chemotherapy.13, 16, 17, 19
Most adverse events reported in the clinicaltrials—such as nausea, fatigue, alopecia, diarrhea,vomiting, constipation, fever, and anorexia—were related to the underlying malignancy or thechemotherapy regimen.19 The most commonadverse event attributable to pegfilgrastim wasmedullary bone pain, reported in approximately26% of patients; this was usually resolved withnonnarcotic analgesics.19 In the pivotal phase IIItrial,16 serious adverse events were reported in19% of patients treated with pegfilgrastim (29
patients) and 20% of patients treated withfilgrastim (30 patients). A similar number ofpatients treated with pegfilgrastim (4%) andfilgrastim (3%) withdrew from the study becauseof adverse events.16
Changes in laboratory measures were seen withboth pegfilgrastim and filgrastim, such astransient elevations in lactate dehydrogenaselevels (19% and 29% of pegfilgrastim andfilgrastim recipients, respectively), alkalinephosphatase levels (9% and 16%), and uric acidlevels (8% and 9%), which did not requiretreatment. Approximately 1% of the adverseevents with both agents were classified assevere.19
Based on clinical trial data submitted to theFDA, it is recommended that pegfilgrastim not beadministered from 14 days before to 24 hoursafter administration of cytotoxic chemotherapy.Administration of pegfilgrastim at 0, 1, and 3days before 5-fluorouracil resulted in greatermortality in mice, but pegfilgrastim treatmentgiven 24 hours after 5-fluorouracil did notadversely affect survival.17 Earlier work withconcurrent 5-fluorouracil and daily adminis-tration of G-CSF showed a potential for increasedsensitivity of rapidly dividing myeloid cells tocytotoxic chemotherapy.20 Administration ofpegfilgrastim concurrently with 5-fluorouracil orother antimetabolites has not been evaluated inhumans. Whether these findings are relevant toother chemotherapy regimens is not clear. Trialsare under way to evaluate intervals shorter than14 days between pegfilgrastim dosing andadministration of the next cycle of chemotherapy.In addition, trials of same-day dosing of pegfil-grastim and chemotherapy are being investigated.
Conclusions
The efficacy and safety of pegfilgrastim hasbeen demonstrated in several clinical trials invarious tumor types, especially two largerandomized double-blind trials that comparedpegfilgrastim with filgrastim. A single dose ofpegfilgrastim/chemotherapy cycle is as effectiveas 11 daily injections of filgrastim 5 µg/kg inreducing the frequency and duration of severeneutropenia, reducing the frequency of febrileneutropenia, and promoting neutrophil recoveryin patients treated with myelosuppressivechemotherapy. Like filgrastim, pegfilgrastim iswell tolerated in most patients; the most commonadverse event attributable to pegfilgrastim ismild-to-moderate bone pain. Administration of
18S
Figure 2. Duration of severe neutropenia (DSN) withadministration of pegfilgrastim 6 mg and filgrastim 5µg/kg/day based on pretreatment body weight.17
0
0.5
1
1.5
2
2.5
3 Pegfilgrastim 6-mg fixed dose
Filgrastim 5 µg/kg/d
≤ 62 > 80> 62 to 71
Pretreatment weight (kg)
> 71 to 80
DS
N (d
ays)

SAFETY AND EFFICACY OF PEGFILGRASTIM Crawford
pegfilgrastim should provide numerous clinicalbenefits for patients, with greater adherence dueto the simplified once/cycle dosing regimen, thusimproving disease management and outcomes inpatients treated with myelosuppressivechemotherapy.
References1. Dale DC. Colony-stimulating factors for the management of
neutropenia in cancer patients. Drugs 2002;62(suppl 1):1–15.2. Lyman GH, Kuderer N, Greene J, Balducci L. The economics
of febrile neutropenia: implications for the use of colony-stimulating factors. Eur J Cancer 1998;34:1857–64.
3. Welte K, Gabrilove J, Bronchud MH, Platzer E, Morstyn G.Filgrastim (r-metHuG-CSF): the first 10 years. Blood1996;88:1907–29.
4. Amgen Inc. Neupogen (filgrastim) prescribing information.Thousand Oaks, CA; 2001.
5. Crawford J, Ozer H, Stoller R, et al. Reduction by granulocytecolony-stimulating factor of fever and neutropenia induced bychemotherapy in patients with small-cell lung cancer. N Engl JMed 1991;325:164–70.
6. Trillet-Lenoir V, Green J, Manegold C, et al. Recombinantgranulocyte colony stimulating factor reduces the infectiouscomplications of cytotoxic chemotherapy. Eur J Cancer1993;29A:319–24.
7. Pettengell R, Gurney H, Radford JA, et al. Granulocytecolony-stimulating factor to prevent dose-limiting neutropeniain non-Hodgkin’s lymphoma: a randomized controlled trial.Blood 1992;80:1430–6.
8. Veronese FM. Peptide and protein PEGylation: a review ofproblems and solutions. Biomaterials 2001;22:405–17.
9. Mehvar R . Modulation of the pharmacokinetics andpharmacodynamics of proteins by polyethylene glycolconjugation. J Pharm Pharm Sci 2000;3:125–36.
10. Crawford J. Pegfilgrastim administered once per cycle reduces
incidence of chemotherapy-induced neutropenia. Drugs2002;62(suppl 1):89–98.
11. Zamboni WC. Pharmacokinetics of pegfilgrastim. Pharmaco-therapy 2003;23(8 pt 2):9S–14.
12. Molineux G. Pegylation: engineering improved biopharma-ceuticals for oncology. Pharmacotherapy 2003;23(8 pt 2):3S–8.
13. Johnston E, Crawford J, Blackwell S, et al. Randomized, dose-escalation study of SD/01 compared with daily filgrastim inpatients receiving chemotherapy. J Clin Oncol 2000;18:2522–8.
14. Holmes FA, Jones SE, O’Shaughnessy J, et al. Comparableefficacy and safety profiles of once-per-cycle pegfilgrastim anddaily injection filgrastim in chemotherapy-inducedneutropenia: a multicenter dose-finding study in women withbreast cancer. Ann Oncol 2002;13:903–9.
15. Vose JM, Crump M, Lazarus H, et al . Randomized,multicenter, open-label study of pegfilgrastim compared withdaily filgrastim after chemotherapy for lymphoma. J Clin Oncol2003;21:514–19.
16. Holmes FA, O’Shaughnessy JA, Vukelja S, et al. Blinded,randomized, multicenter study to evaluate single adminis-tration pegfilgrastim once per cycle versus daily filgrastim as anadjunct to chemotherapy in patients with high-risk stage II orstage III/IV breast cancer. J Clin Oncol 2002;20:727–31.
17. Green MD, Koelbl H, Baselga J, et al. A randomized double-blind multicenter phase III study of fixed-dose single-administration pegfilgrastim versus daily filgrastim in patientsreceiving myelosuppressive chemotherapy. Ann Oncol2003;14:29–35.
18. Meza L, Hackett J, Neumann T. Time to absolute neutrophilcount (ANC) recovery following filgrastim in patients withbreast cancer. Presented at the annual meeting of the AmericanCollege of Clinical Pharmacy, Albuquerque, NM, October20–23, 2002.
19. Amgen Inc. Neulasta (pegfilgrastim) prescribing information.Thousand Oaks, CA; 2002.
20. Meropol NJ, Miller LL, Korn EL, et al. Severe myelo-suppression resulting from concurrent administration ofgranulocyte colony-stimulating factor and cytotoxicchemotherapy. J Natl Cancer Inst 1992;84:1201–3.
19S