safety of gi drugs gp cme 2014
TRANSCRIPT
Safety of GI drugsGP CME 2014
Sun 0855-0920
Dr Alasdair Patrick
Macmurray Center
Middlemore Hospital

Disclosure
• Nil

Overview
• GI risks of common drugs– NSAIDs and cox-2 inhibitors
– Aspirin and others
– Warfarin and direct thrombin inhibitors (Pradaxa)
• Risks of GI drugs– Proton pump inhibitors and H2 blockers
– Hepatitis B drugs
– IBD drugs
– Pregnancy

NSAIDs
• Mechanism of action
– Inhibits both cox-1 and 2
• Cox-1
– Housekeeping enzyme
• In most cells
– PG synthesis
• Gastric cytoprotection
• Platelet function
• Vascular homeostasis

Cox-2 inhibitors
• Cox-2
– Undetectable in most tissues
• Increase in inflammatory states
• Paracetamol is a CNS Cox-2 blocker
– Has very little anti-inflammatory activity
• Glucocorticoids also inhibit cox-2
– Probable mechanism for anti-inflammatory effect
Types of NSAIDs
• Short acting (less 6 hrs)
– Ibuprofen (Brufen)
– Diclofenac (Voltaren)
– Indomethacin (Indocid)
• Long acting (more 6 hrs)
– Naproxen (Naprosyn)
– Meloxicam (Mobic)
– Celecoxib (Celebrex)
If have hypoalbuminaemia then have higher free serum concentration
Shorter half life may be safer
Side track: Cardiovascular risk
• Worldwide withdrawal of Rofecoxib (Vioxx)
– VIGOR and APPROVe trial
• On August 19, 2005, a jury in Texas voted 10-2 to hold Merck liable for the death of Robert Ernst, a 59-year-old man who allegedly died of a rofecoxib-induced heart attack.
• The jury awarded Carol Ernst, widow of Robert Ernst, $253.4 million in damages
• For a short course risk is very small

NSAIDs
• There is clear individual response in anti-inflammatory effect for different NSAIDs
– If one not working try another!
• 10-20% experience dyspepsia
– I will not discuss this further
• Two big concerns from GI point of view
– GI bleeding
• Can occur anywhere in the GI tract
– Deranged LFTs
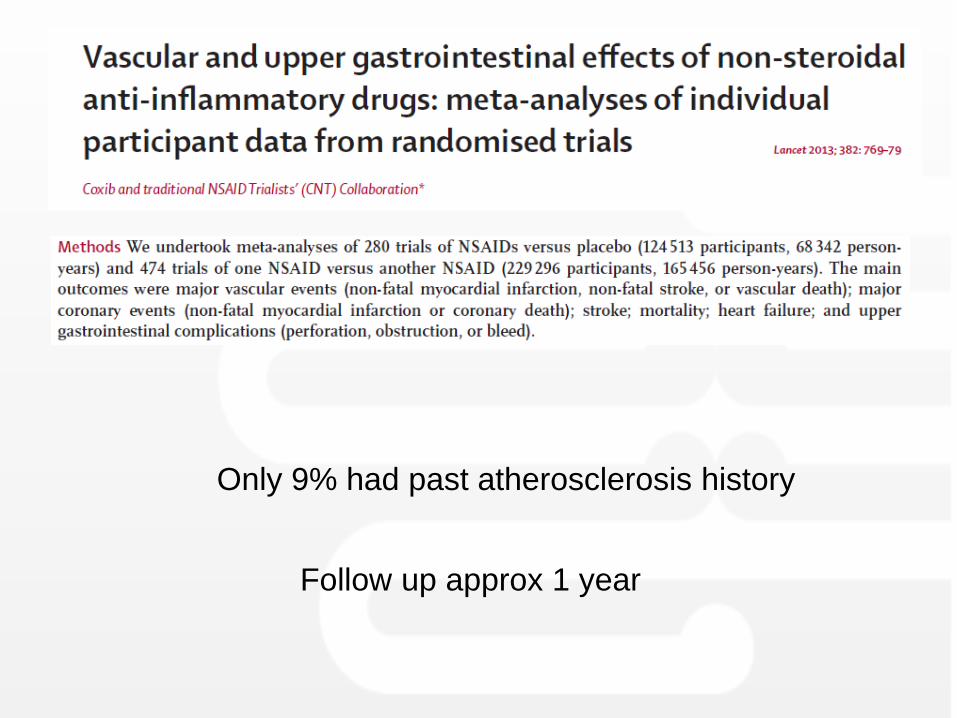
Only 9% had past atherosclerosis history
Follow up approx 1 year

Same risk
Diclofenac prob safest
If worried re cardiac risk
- Naproxen

NSAIDs and LFTs
• Review of 2 million prescriptions for NSAIDs
– 625,307 patients
– 23 cases of liver injury
• 1.1 per 100,000 NSAID prescriptions
• None fatal
• No one NSAID had higher risk
Arch Intern Med. 1994;154(3):311.

Aspirin• Enteric coated aspirin has NOT been shown to
be safer for GI bleeding
BMJ. 2000;321(7270):1183
Dose matters
Risk of bleeding

Generally….
• NSAIDs increase risk 2-4 fold
– 0.2-1.9% per year
• Aspirin has a risk of 0.6-1% per year of bleeding
– Additional 1% risk if combined with clopidogrel
• Co-prescription of a PPI
– Reduces this risk by 50-80%
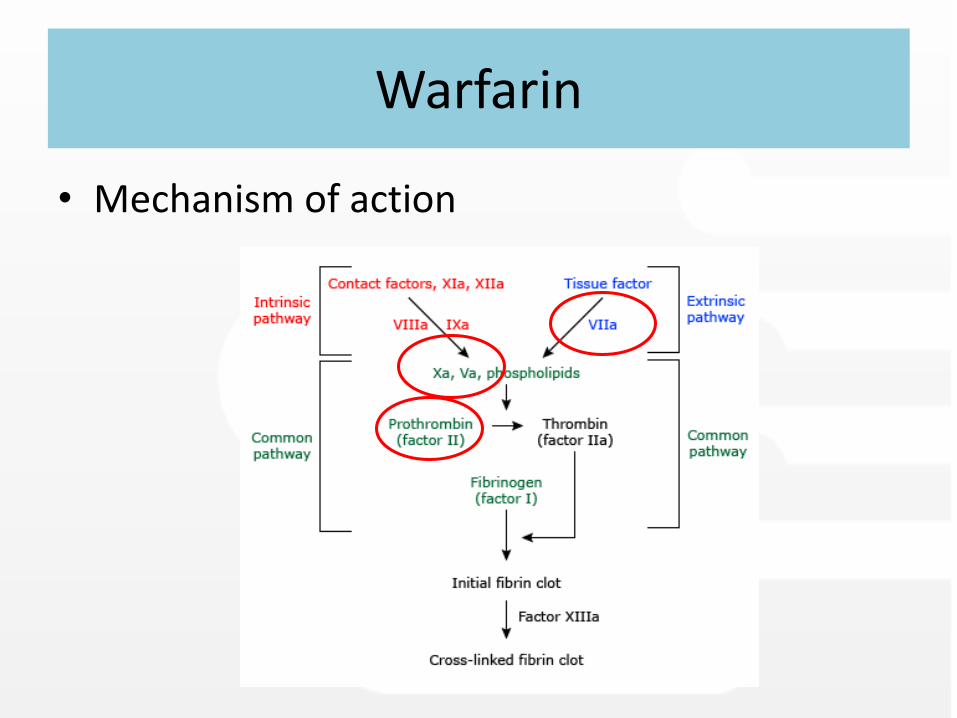
Warfarin
• Mechanism of action
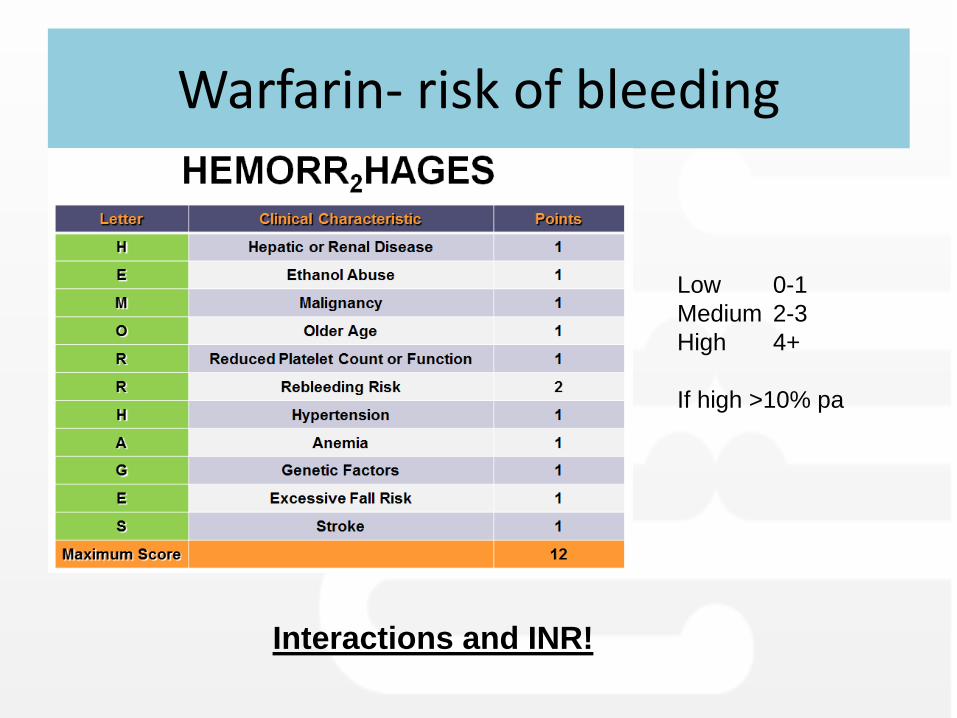
Warfarin- risk of bleeding
Interactions and INR!
Low 0-1
Medium 2-3
High 4+
If high >10% pa

Dipyridamole and Clopidogrel
• Dipyridamole
– Does not seem to increase GI bleed risk
• Clopidogrel
– Thought to have similar risks of bleeding as aspirin and NSAIDs
– If it is combined with aspirin risks increase further
• But a PPI will lower bleeding risk by 87%

Direct thrombin inhibitors
• Mechanism of action
Bleeding risk Pradaxa
• More difficult to reverse
– Can use expensive pro-thrombinex
• USA FDA November 2012
– “rates of bleeding did not appear to be higher than bleeding rates with the use of warfarin”
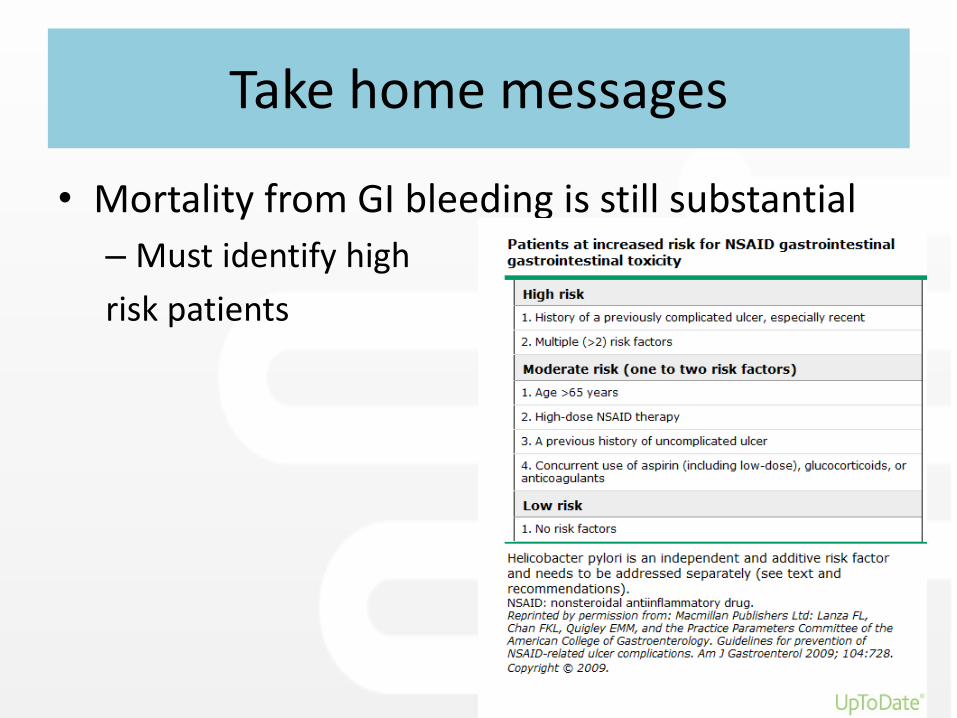
Take home messages
• Mortality from GI bleeding is still substantial
– Must identify high
risk patients

Risk factor stratification for acute GI haemorrhage in users of COX
inhibitors or antiplatelet agents.
Lowest increase in risk
•Age < 65 years
•No other risk factors
Moderate increase in risk
One or two moderate risk factors:
•Age > 65 years
•In combination with another antiplatelet
•In combination with another NSAID
•In combination with oral bisphosphonate
•In combination with serotonin reuptake inhibitor (SSRI)
•In combination with systemic corticosteroids
Highest risk
Three or more moderate risk factors OR any of:
• Previous acute upper GI haemorrhage
• Previous peptic ulcer
• In combination with anticoagulation

Primary prevention for anticoagulants/NSAIDs
• Use short course
• Use Diclofenac if can choose
• Do not use multiple anti-coagulants
• Combine with a PPI• NSAID and PPI same risk as Cox-2 inhibitor

Take home messages
• H pylori is an independent and synergistic risk factor with anti-coagulation
– Meta-analysis of 21 studies (10,146 patients)
• OR of ulcer 2.17 if H pylori positive
• If high risk ethnicity for H pylori then test and treat if need long term NSAIDs or aspirin
– Maori, PI, SE Asian
Clinical gastroenterology and hepatology 2006 Feb;4(2):130-42

Risks of GI drugs themselves
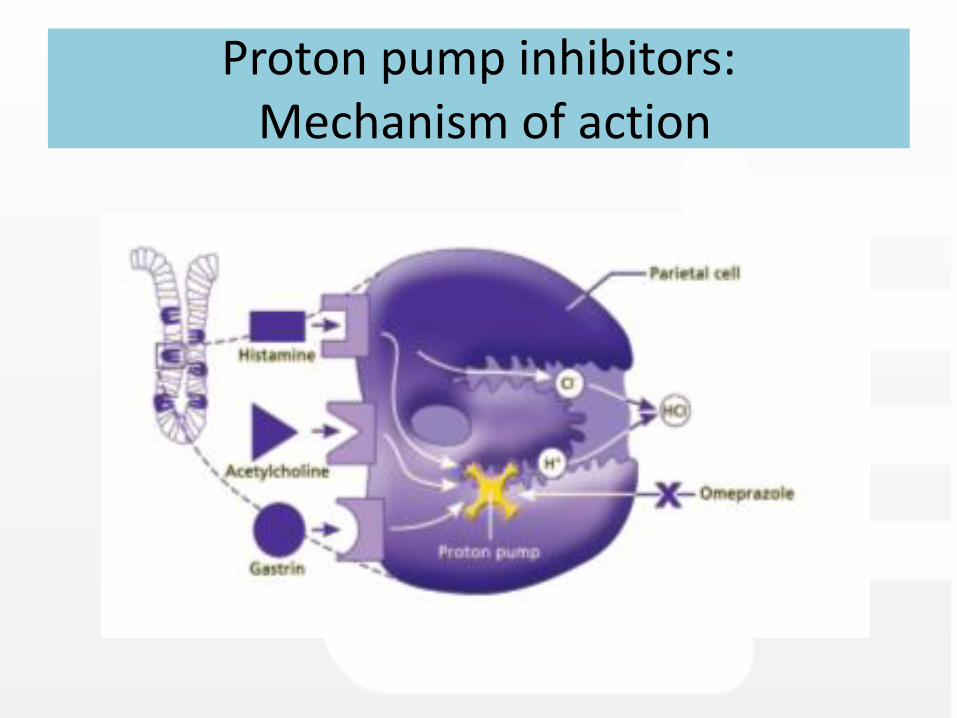
Proton pump inhibitors:Mechanism of action
Proton pump inhibitorsDo not read the fine print!
Rare
Back, leg, or stomach pain
bleeding or crusting sores on the lips
blisters
bloody or cloudy urine
chills
continuing ulcers or sores in the mouth
difficult, burning, or painful urination
fever
frequent urge to urinate
general feeling of discomfort or illness
joint pain
loss of appetite
muscle aches or cramps
pain
red or irritated eyes
redness, tenderness, itching, burning, or peeling of the skin
skin rash or itching
sore throat
sores, ulcers, or white spots on the lips, in the mouth, or on the genitals
unusual bleeding or bruising
unusual tiredness or weakness
Incidence not known
Drowsiness
fast, racing, or uneven heartbeat
mood or mental changes
muscle spasms (tetany) or twitching seizures
nausea or vomiting
trembling

Proton pump inhibitors
• Effect on absorption
– Reduces iron and B12 absorption
• Clinically not important
– Reduces Mg absorption
• Can interact with digoxin and diuretics
• FDA actually suggest checking levels
– Reduces Ca absorption
• All fracture data retrospective
• Nurses health study found 36% increase but absolute risk was low (2.02 v 1.5 per 1000 pt years)
» BMJ 2012:344 e372

Proton pump inhibitors
• Pneumonia
– Is postulated that reduced acid secretion increases upper GI tract colonisation
– OR of pneumonia 1.27 (1.11-1.46)» CMAJ. 2011;183(3):310.
– This result not supported by recent meta-analysis
• Over 4 million NSAID users» Gut 2014; 63:552

Proton pump inhibitors
• C difficile infections
– Can occur in PPI users even without antibiotics
– Risk further increased by antibiotic use
• 15 cases per 1000 v 45 cases per 1000
• Risk is higher with PPI than H2 blocker
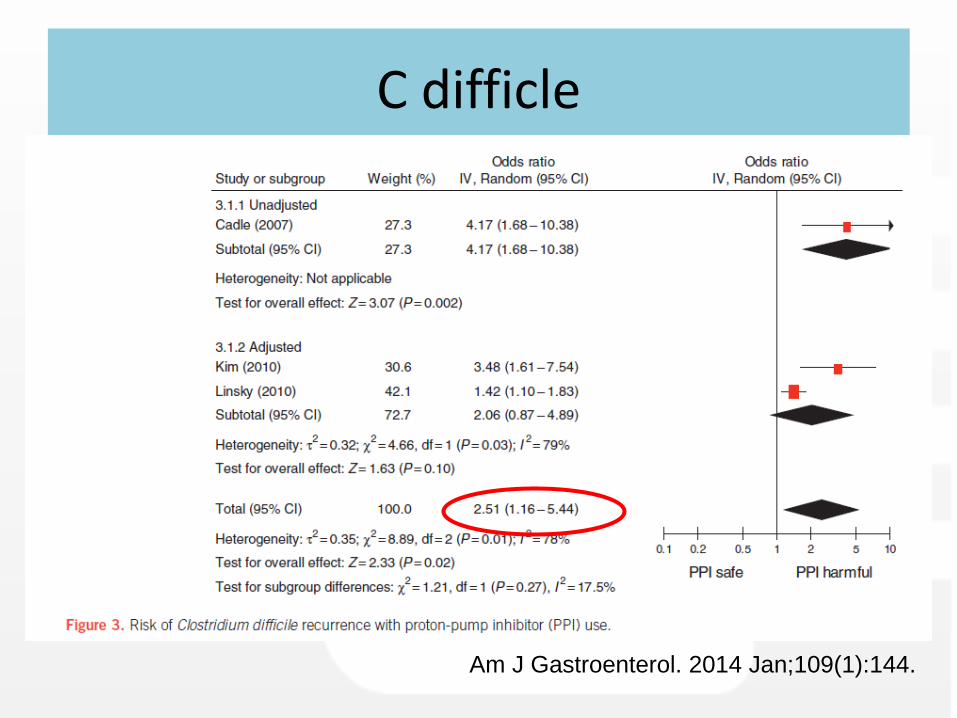
C difficle
Am J Gastroenterol. 2014 Jan;109(1):144.
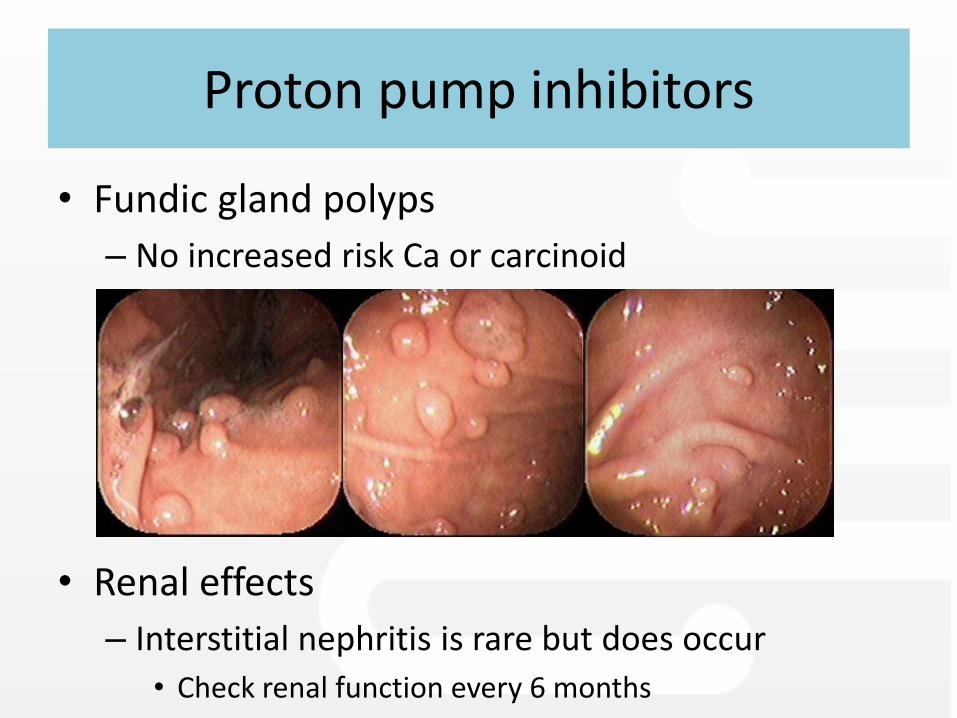
Proton pump inhibitors
• Fundic gland polyps
– No increased risk Ca or carcinoid
• Renal effects
– Interstitial nephritis is rare but does occur
• Check renal function every 6 months

Proton pump inhibitors
• Clopidogrel interaction?
PPI and clopidogrel
• Initially there was concern about PPI reducing clopidogrel effect
– FDA in 2009 suggested physician is consulted if they are going to use both
– Platelet function studies and registry reviews do NOT support this interaction
» NEJM 2010; 363, 1909

H-2 Blockers
• Generally in trials adverse effect rate is similar to placebo
– No different to PPIs
• Possible increased risks
– Gynaecomastia and impotence
– Idiosyncratic myelosuppression
– CNS effects
– QT prolongation

Hepatitis B drugs
• Lamivudine
– Nucleoside analogue
– Main problem is resistance
- Minimal side effects

Other Hep B drugs
• Tenofovir
– Reverse transcriptase inhibitor
– Insomnia, headache, rash, diarrhea, abdo pain
• Entecavir
– Reverse transcriptase inhibitor
– Pedal oedema, renal impairment, headache

IBD drugs
• 5 Asa (Pentasa, Asacol, Asamax)
– First line treatment for mild to moderate disease
– Sulphasalzine rarely used now
– Approx 10% have intolerable side effects

IBD drugs

IBD drugs
• Azathioprine
– All effects are beyond the scope of this talk
• Nausea when first start 10%
• Derranged LFTs- can be severe
• Myelosuppression– Need blood tests 6-8 weekly
• Biologics (Infliximab and Humira)
– Reactivation of infections
– Unusual lymphomas in young men

Pregnancy
• Most GI drugs are safe
• When in doubt look it up!

Conclusion
• Risks of GI bleeding
– Increased for all anticoagulants especially if old, combined drugs and past history
– Need to know risk factors
• Use PPI
• Check for H pylori
• PPI are safe long term but use sensibly
– Dunedin study showing 60% inappropriate use
• Other GI drugs also safe
– Generally continue in pregnancy

Thanks
Dr Alasdair Patrick
Gastroenterologist