sartoris & resnick (1985) - tarsal coalition
TRANSCRIPT

8/10/2019 Sartoris & Resnick (1985) - Tarsal Coalition
http://slidepdf.com/reader/full/sartoris-resnick-1985-tarsal-coalition 1/8
33
RADIOLOGIC
VIGNETTE
TARSAL
COALITION
DAVID J .
SARTORIS
and D O N A L D L. RESNICK
Tarsal coalition,
or
fusion , refers to the union of
2 or more tarsal bones into a single structure, with
consequent absence of normal relative motion be-
tween them (1,2). The connection may be fibrous
(syndesmosis), cartilaginous (synchondrosis),
or
osse-
ous (synostosis) (1,3). Congenital cases are thought to
arise from altered differentiation and impaired segmen-
tation of primordial mesenchyme, resulting in failure
of joint formation (3,4). Incorporation of accessory
ossicles into tarsal articulations has also been pro-
posed as an etiology (5,6). Acquired causes include
trauma, previous surgery, infection, osteoarthritis,
and rheumatoid arthritis (1,3).
Paleopathologic re-
mains have documented the occurrence of this condi-
tion as early as
900-950
AD
(7,8). This vignette
describes the epidemiologic, clinical, radiographic,
and scintigraphic features of the various forms of
tarsal coalition.
Epidemiology
The overall prevalence of tarsal coalition in the
general population is approximately 1 (6,9). In some
instances, particularly those with multiple tarsal fu-
sions,
a
familial tendency has been noted (3,8). Auto-
soma1 dominant inheritance with variable penetrance
has been proposed, based on
a
39 incidence among
first-degree relatives of 31 affected individuals in 1
From the Radiology Service, Veterans Administration
David
J .
Sartoris, MD; Donald L. Resnick, MD.
Address reprint requests to Donald L. Resnick, MD, Radi-
ology Service, VA Medical Center, 3350 La Jolla Village Drive, San
Diego, CA 92161.
Submitted for publication August 16, 1984; accepted in
revised form September
4,
1984.
Medical Center, San Diego, California.
study
8).
Tarsal coalitions may be isolated phenom-
ena or may be associated with congenital malforma-
tion syndromes, including hereditary symphalangism,
Apert’s acrocephalosyndactyly, and the hand-foot-
uterus syndrome (3,10,11). Many cases of peroneal
spastic flatfoot are accompanied by tarsal fusions,
although the former finding may also be caused by a
previous fracture, osteoarthritis, tuberculosis, juvenile
chronic arthritis, or other conditions (12-15).
Clinical manifestations
Signs and symptoms of tarsal coalition general-
ly develop during the second or third decade
of
life
(3,16). This delayed presentation ofa congenital prob-
lem has been attributed to the conversion of fibrous or
cartilaginous union to osseous fusion, the former being
rarely symptomatic (2,3). Typically, vague foot pain
exaggerated by vigorous use or prolonged standing is
noted, often beginning after minor trauma
or
unusual
activity (1,17). Physical examination reveals intermit-
tent or constant peroneal muscular spasm, restricted
subtaiar joint mobility, pes planus, and valgus posi-
tioning of the foot (1,3). Concomitant spasm of the
tibialis anterior may, however, result in varus deformi-
ty, and pes cavus has also been observed (1,3). Tarsal
coalition may present as an incidental radiographic
finding in an asymptomatic individual (3).
Radiographic classification
Solitary tarsal coalitions are categorized
according to the bones that are united (1,3). Calcaneo-
navicular fusions are slightly more common than talo-
calcaneal fusions, whereas talonavicular and calcaneo-
cuboid involvement occur far less frequently (3,9).
Arthritis and Rh eumatism,
Vol. 28,
No. 3 March 1985)

8/10/2019 Sartoris & Resnick (1985) - Tarsal Coalition
http://slidepdf.com/reader/full/sartoris-resnick-1985-tarsal-coalition 2/8
332
SARTORIS
AND
R E S N I C K
Figure 1.
Oblique view demonstrating osseous fusion between the
calcaneus and navicular
arrow).
Secondary degenerative changes
are present in the talonavicular articulation.
Coalitions involving multiple bones or unusual sites
are characteristically associated with other congenital
abnormalities
3).
In general, radiographic findings in
tarsal fusion can be classified as either primary (direct
or indirect visualization of the fibrous, cartilaginous,
or osseous bridge) or secondary (adaptive alterations
in the affected or adjacent bones and articulations) in
type.
Calcaneonavicular coalition.
Normally, an ar-
ticulation does not exist between the calcaneus and the
navicular
3).
In cases of bony coalition, which gener-
ally occurs in children between the ages of 8 and 12
(2,3), routine frontal and lateral radiographs may fail to
demonstrate the site of union between these struc-
tures, although a
45”
medial-oblique view of the foot
establishes the diagnosis (Figure
1 1,3) .
Close ap-
proximation of the adjacent calcaneal and navicular
cortices, particularly in association with bone sclerosis
or irregularity, suggests fibrous or cartilaginous fusion
1,3).
Secondary radiographic signs are less pro-
nounced than those accompanying talocalcaneal coali-
tion, and include hypoplasia of the talar head (1,3)
(Table
1).
Clinical manifestations are also less severe:
spastic flatfoot may be evident, although the condition
is commonly asymptomatic. This coalition may predis-
pose to ankle sprain (3,18). Fracture of an osseous
calcaneonavicular bridge has also been reported 6).
Talocalcaneal coalition.
Fusion of the talus and
the calcaneus occurs most commonly at the level of
the sustentaculum tali and involves the middle facets
of the anterior subtalar joint. Rarely are the anterior
facets or posterior subtalar joint affected (3,17). Talo-
calcaneal coalition is seen more frequently in males
and occurs bilaterally in up to
25
of patients (3,17).
Ossification occurs between the ages of 12 and
16
(2).
Osseous coalitions may be overlooked on standard
frontal and lateral radiographs, or even simulated in
normal feet (3,19). Plain
film
radiography, utilizing
oblique or axial (Harris-Beath views) projections (Fig-
ure
2),
and conventional tomography are more diag-
nostic (1,3). Close apposition, eburnation, or sclerosis
of adjacent articular surfaces implies fibrous or carti-
laginous union (3). The latter may be confirmed by
contrast arthrography of
t h e
talocalcaneonavicular
joint, during which failure of normal opacification of
the fused posterior portion
of
the articular cavity is
noted (Figure 3) (3,20).
The numerous secondary radiographic signs
of
talocalcaneal coalition are summarized in Table 1.
Subtalar rigidity leads to dorsal subluxation of the
navicular, resulting in periosteal elevation and reactive
bone formation at the attachment of the talonavicular
ligament
(1,17).
An osseous outgrowth, or “beak,” is
formed at the dorsal aspect of the talar head adjacent
to the talonavicular articulation (Figure
4 .
Less con-
stantly, a similar excrescence develops on the proxi-
mal-dorsal surface of the navicular (1,3). These find-
ings, best recognized in the lateral projection, are also
observed in diffuse idiopathic skeletal hyperostosis,
acromegaly, rheumatoid arthritis, and other conditions
with altered motion of the talonavicular joint (1,3).
Table
1.
Secondary radiographic signs of tarsal coalition
Calcaneonavicular
Hypoplasia
of
head
of
talus
Talocalcaneal
Osseous excrescence at dorsal aspect of talus
Narrowing of posterior talocalcaneal joint space
Broadening or rounding
of
lateral process
of talus
Ball-and-socket tibiotalar articulation
Failure of visualization
of
middle facets of anterior subtalar joint
Concave undersurface of talar neck with asymmetry
of
talocalcaneonavicular joint

8/10/2019 Sartoris & Resnick (1985) - Tarsal Coalition
http://slidepdf.com/reader/full/sartoris-resnick-1985-tarsal-coalition 3/8
RADIOLOGIC
VIGNETTE
333
A B
Figure 2. Axial Harris-Bea th) views at the level
of
the sustentaculum tali. A , Normal side. B, Osseous talocalcaneal coalition arrow).
Figure
3.
Tornogram lateral view) following contrast injection of talocalcaneona vicular joint rev ealing
absence of opacification posteriorly in region of sustentaculum tali, due to nonosseous talocalcaneal coalition
arrow).

8/10/2019 Sartoris & Resnick (1985) - Tarsal Coalition
http://slidepdf.com/reader/full/sartoris-resnick-1985-tarsal-coalition 4/8
334
SARTORIS
AND
RESNICK
Figure 4 Radiograph (lateral view) showing prominent osseous
excrescence arising from dorsal aspect
of
talar head. Obliteration
of
articular interval between talus and calcaneus also suggests coali-
tion.
However, they are readily distinguished from osteo-
phyte formation related to osteoarthritis of the ankle
or midfoot, and should not be mistaken for excres-
cences which may develop normally at the insertion of
the capsule of the ankle joint in the talar neck (3,21).
At its typical site, talocalcaneal coalition may
lead
to
eversion of the calcaneus, or premature degen-
erative arthritis of the posterior subtalar articulation
(3). Either of these phenomena results in apparent
narrowing
of
the posterior subtalar joint space, a
secondary radiographic sign seen in as many as60 of
patients (3,17). Valgus angulation of the calcaneus
resulting from talocalcaneal fusion leads to broaden-
ing, or rounding of the lateral process of the talus in
approximately
50
of patients (1,3,17). Furthermore,
in the presence of a talocalcaneal coalition, the func-
tions of inversion and eversion which are normally
performed by the subtalar articulations are assumed
by the tibiotalar joint (3,22). This phenomenon con-
verts the normally mesa-shaped superior talar joint
surface
to
a rounded convexity which articulates with
a correspondingly concave distal tibia, a finding that is
termed the “ball-and-socket” ankle joint (Figure 5
(322).
The middle facets of the anterior subtalar joint
are normally seen in tangent ona properly-positioned
lateral radiograph of the foot (Figure
6).
Failure to
visualize this articulation is a helpful ancillary sign of
talocalcaneal coalition, although technical error may
result in false-positive diagnoses (3,17). Comparison
radiographs of the uninvolved foot may be useful in
detecting talocalcaneonavicular joint asymmetry and
associated concavity of the plantar aspect of the talar
neck (3,17). The reliability of these signs depends upon
comparable positioning on the 2 sides
of
the body
(3,171.
Talonavicular coalition. Conventional radio-
graphs, particularly the lateral view, are usually ade-
quate for the diagnosis of this uncommon variety of
tarsal fusion (Figure
7)
(1,3). Osseous bridging occurs
between the ages of 3 and
5
years, and may be
asymptomatic or associated with peroneal spasm (1,2).
Abnormalities of the fifth digit of the hand may occur
concomitantly, and both autosomal dominant and re-
cessive inheritance patterns have been observed
(10,23).
Calcaneocuboid coalition. This extremely rare
entity is readily diagnosed in its osseous form by
routine radiography (1,3). Calcaneocuboid fusion may
be asymptomatic, coexistent with peroneal spasm,
bilateral, or associated with other congenital anoma-
lies (1,3).
Figure
5 Frontal view illustrating typical appearance
of
the “ball-
and-socket’’ ankle joint.

8/10/2019 Sartoris & Resnick (1985) - Tarsal Coalition
http://slidepdf.com/reader/full/sartoris-resnick-1985-tarsal-coalition 5/8
RADIOLOGIC
VIGNETTE
5
A
Figure 6.
A ,
Lateral view of talocalcaneal coalition showing obscuration of middle facets of anterior subtalar oi nt arrowhead), with associated
narrowing
of
the posterior subtalar articulation. B , Lateral view
of
normal foot, for comparison.
Figure
7. Osseous fusion (lateral view) between the talus and navicular
arrow).
8/10/2019 Sartoris & Resnick (1985) - Tarsal Coalition
http://slidepdf.com/reader/full/sartoris-resnick-1985-tarsal-coalition 6/8
336
SARTORIS AND RESNICK
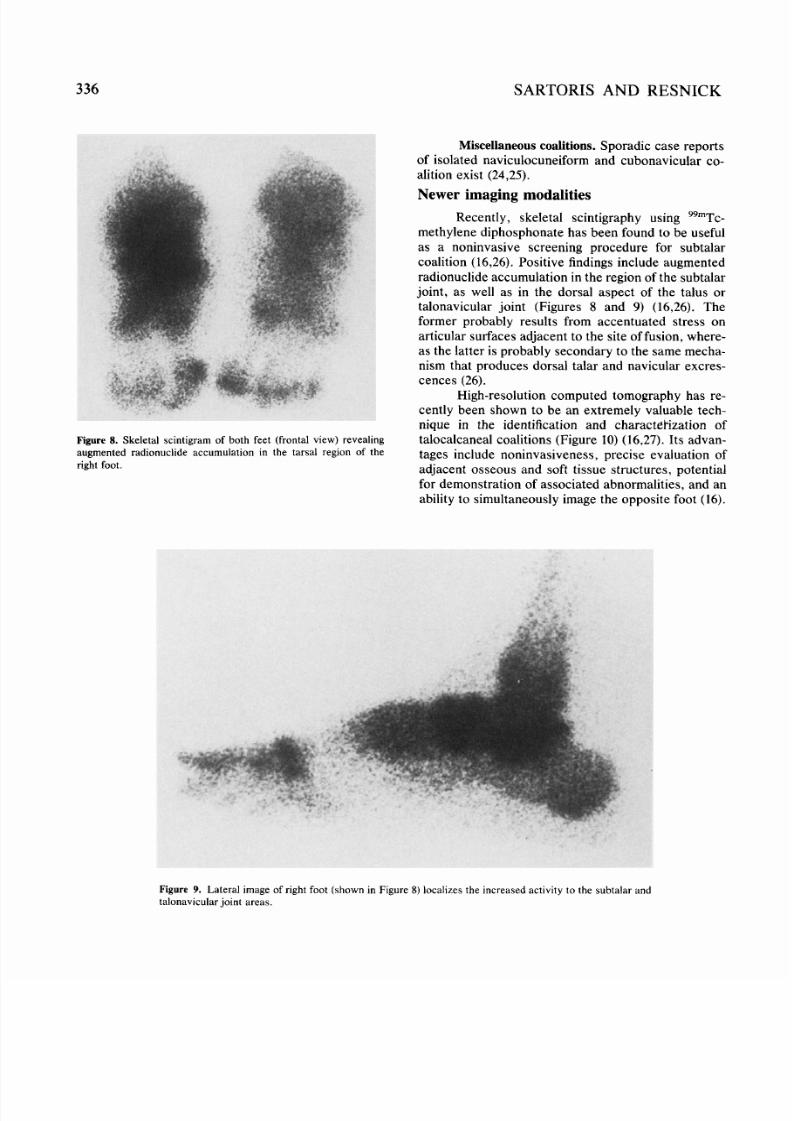
Miscellaneous coalitions. Sporadic case reports
of isolated naviculocuneiform and cubonavicular co-
alition exist (24,25).
Newer imaging m odalities
Recently, skeletal scintigraphy using Y9mT~
methylene diphosphonate has been found to be useful
as a noninvasive screening procedure for subtalar
coalition (16,26). Positive findings include augmented
radionuclide accumulation in the region of the subtalar
joint, as well as in the dorsal aspect of the talus or
talonavicular joint (Figures
8
and
9)
(16,26). The
former probably results from accentuated stress on
articular surfaces adjacent to the site of fusion, where-
as the latter is probably secondary to the same mecha-
nism that produces dorsal talar and navicular excres-
cences (26).
High-resolution computed tomography has re-
cently been shown to be an extremely valuable tech-
nique in the identification and charactlkization of
talocalcaneal coalitions (Figure 10) (16,27). Its advan-
tages include noninvasiveness, precise evaluation
O f
adjacent osseous and soft tissue structures, potential
for demonstration of associated abnormalities, and an
ability to simultaneously image the opposite foot (16).
Figure 8. Skeletal scintigram of both feet (frontal view) revealing
augmented radionuclide accumulation in the tarsal region
of
the
right foot.
Figure 9
Lateral image of right foot (shown in Figure
8)
localizes the increased activity to the subtala r and
talonavicular joint area s.

8/10/2019 Sartoris & Resnick (1985) - Tarsal Coalition
http://slidepdf.com/reader/full/sartoris-resnick-1985-tarsal-coalition 7/8
RADIOLOGIC VIGNETTE
337
Figure 10 Computed tomographic image at the level of sustentacula tali demonstrating osseous bridging of
the middle facets
of
the anterior subtdlarjoinl on the right arrow).The normal appearance of this articulation
is seen in the left foot.
Acknowledgment.
Special thanks are extended to
Geri Hubble
for
typing the manuscript.
REFERENCES
1
Conway J J, Cowell H R: T arsal coalition: clinical signifi-
cance and roentgenographic demon stration. Radiology
2. Cowell HR, Elener V: Rigid painful flatfoot secondary
to
tarsal coalition. CIin Ort hop 17754-60, 1983
3.
Resnick D: Additional congenital or heritable anomalies
and syndromes, Diagnosis of Bone and Joint Disorders
with Emphasis on Articular Abnormalities. Edited by D
Resnick, G Niwayama. Philadelphia, WB S aunders Co.,
4. Wheeler R, Guevera A, Bleck EE: Tarsal coalitions:
review of the literature and case report of bilateral dual
calcaneonavicular and talocalcaneal coalitions. Clin
Orthop
156:
175-177, 1981
5
Galinski AW , Crovo RT, Ditmars JJ Jr: 0 s rigonum as a
cause of tarsal coalition. J Am Podiatry
Assoc
69:191-
196, 1979
6. Richards RR, Evans JG, McGoey PF: Fracture
of
a
calcaneonavicular bar: a complication of tarsal coalition:
a cas e rep ort . Clin Or tho p 185:220-221, 1984
92 99-8
1
1, 1969
198 pp 2559-2565
7. Heiple
K G ,
Lovejoy
CO:
The antiquity of tarsal coali-
tion: bilateral deform ity in a pre-Columbian Indian skel-
eton . J Bone Joint Surg 51A:979-983, 1969
8.
Leonard
MA:
The inheritance of tarsal coalition and its
relationship
to
spastic flatfoot. J Bone Joint Surg
56B 20-526, I974
9. Stormont DM, Peterson HA: The relative incidence of
tarsal coalition. Clin Or th op 181:28-36, 1983
10. C hallis J: Heredita ry transmission
of
talonavicular coali-
tion
in
association with anomaly
of
the little finger. J
Bon e Joint Su rg 56A:1273-1276, 1974
11.
Geelhoed
GW ,
Nee1 JV , D avidson RT: Symphalangism
and tarsal coalitions: a hereditary syndrom e: a report on
two families. J Bone Joint Surg 51B:278-289, 1969
12. James EA: Tarsal coalitions and peroneal spastic flat-
foot. Austral Radiol 14:80-83, 1970
13. Cowell HR: Talocalcaneal coalition and new causes of
peroneal spastic flatfoot. Clin Orthop
85:
16-22, 1972
14. Jayakumar S, Cowell HR: Rigid flatfoot. Clin Orthop
15. Kendrick JI: Tarsal coalitions. Clin Orthop 85:62-63,
1972
16. Deu tsch AL, Resnick
D ,
Campbell G: Computed tomog-
raphy and bone scintigraphy in the evaluation
of
tarsal
coalitio n. Radiology 144:137-140, 1982
17. B eckly DE, Anderson PW , Pedegana LR : The radiology
of
the sub talar joint with special reference to talo-
calcane al coalition. Clin Radiol 26:333-341, 1975
122:77-84, 1977

8/10/2019 Sartoris & Resnick (1985) - Tarsal Coalition
http://slidepdf.com/reader/full/sartoris-resnick-1985-tarsal-coalition 8/8
SARTORIS AND RESNICK
18. Snyder RB, Libscomb A B, Johnston RK : The relation-
ship of tarsal coalitions to a nkle sprains in athle tes. Am J
Sp ort s Me d 9:313-317, 1981
19. Shaffer HA Jr, Harrison RB: T arsal pseudo-coalition-a
positional artifa ct. J Ca n Ass oc Radiol 31:236-237, 1980
20. Kaye JJ , Ghelman B, S chneide r R: Talocalcaneonavicu-
lar joint arth rograph y for suste ntacular-ta lar tarsal coali-
tions. Radiolog y 115:730-731, 1975
21. Keats TE , Harrison RB: Hypertrophy of the talar beak.
Ske letal Radiol 4:37-39, 1979
22. Channon GM , Brothe rton BJ: The ball-and-socket ankle
joint. J Bo ne Joint Surg 61B:85-89, 1979
23. Zeide MS, Wiesel SW, Terry RL: Talonavicular coali-
tion. Clin Or tho p 126:225-227, 1977
24. Gregersen HN: Naviculocuneiform coalition. J Bone
Join t Surg 59A:128-130, 1977
25. Cavallaro DC, Hadden HR: An unusual case of tarsal
coalition:
a
cuboid navicular syno stosis. J Am Podiatry
26. Goldman AB, Pavlov H, Schneider R: Radionuclide
bone scanning in subtalar coalitions: differential consid-
era tio ns. AJR 138:427-432, 1982
27. Azouz EM : Tarsal pseudo-coalition (letter). J Can Assoc
Radiol 33:105, 1982
ASS OC 8171-75, 1978