save the meniscus - organizers-congress.org · badminton and alpine skiing. ... microsoft...
TRANSCRIPT

Save the meniscus
Daniel FRITSCHY

The case of the day…
• 48 y. old female patient, sports teacher• no health problem• no medical antecedents• right knee pain since 6 mo. without anyaccident
• has difficulties to demonstrate exercices in herclass, has pain when she pratices her sports : badminton and alpine skiing

The case of the day…
• right knee dry and stable• slight varus axis deviation• pain on the medial femoro‐tibial joint line• no jump of the meniscus• imaging


The meniscus history
• anatomy and function• the surgical saga• the advent of MRI• the future

superior view of the menisci

the meniscus : wedge and shock absorber

the lateral meniscus the medial meniscus has less‐ moves forward in extension mobility‐ moves backward in flexion

mobility of the menisciin rotation
range of motion of the menisci

vascularization of the meniscus
Surgery of the meniscus
1731 Bass describes the meniscus pathology
1867 Bradhurst performes the first meniscectomy
1921 Bircher presents 18 cases of kneearthro‐endoscopy

The meniscal tears
• vertical• horizontal• radial• flap (bucket handle)• degenerative

injury mechanism :maximum flexion crushesthe posterior horn= vertical oroblique tears
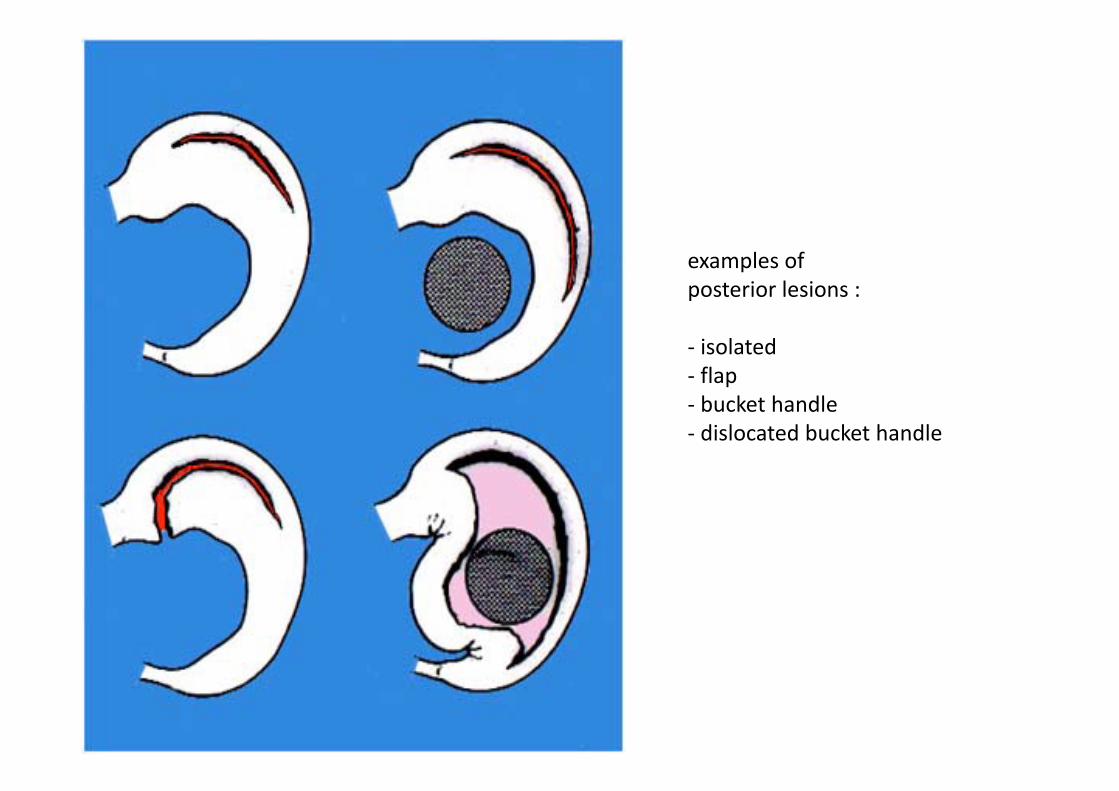
examples ofposterior lesions :
‐ isolated‐ flap‐ bucket handle‐ dislocated bucket handle
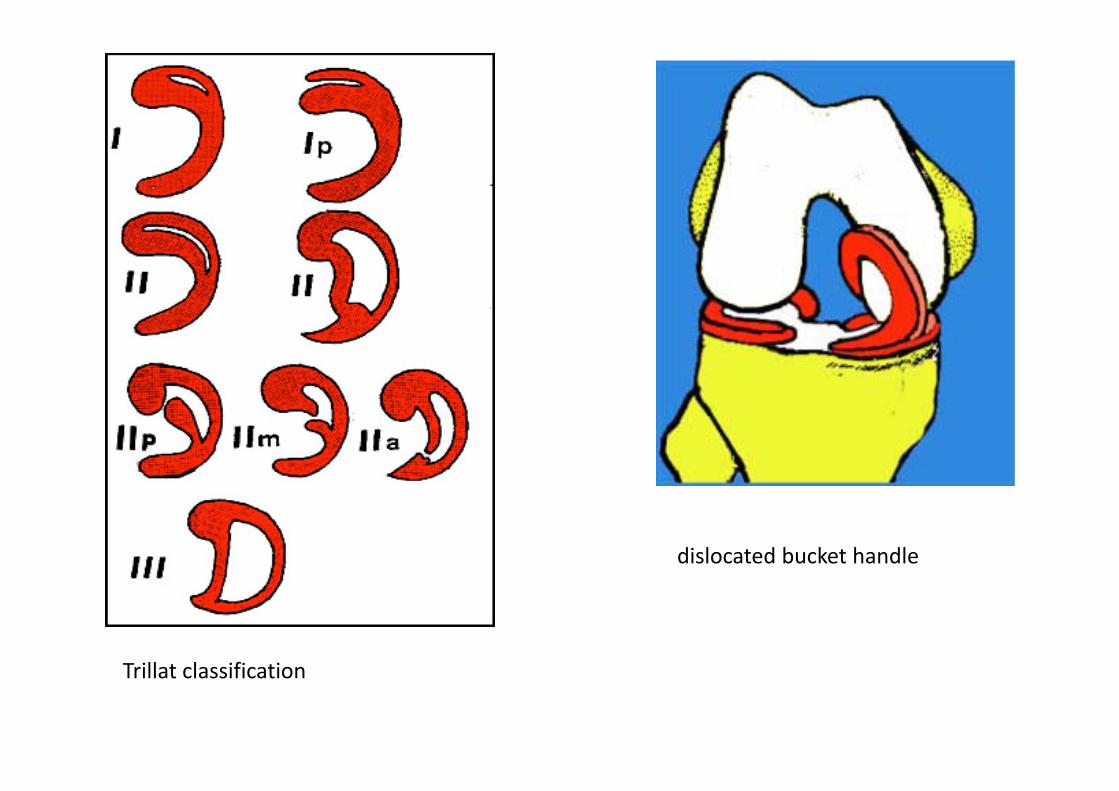
Trillat classification
dislocated bucket handle

The meniscal suture
• 1883 Annandale presents the first meniscal suture
• 1936 King controls the healing of a meniscal suture in the rabbit
• 1976 series of DeHaven (5, 10 y.)

all-inside

all-inside :T-FIX technique

Meniscal sutures and fixations complications
• medial saphenous nerve lesions (up to 43%, 8% of permanent damage)
• infections• cartilage lesions (ex : arrow)• failure : 5‐10%






gonarthrosis : 3 signs described byFairbank (1948)
‐ flattening of the femoral condyle
‐ narrowing of the joint line
‐ apparition of marginal osteophytes

The MRI advent
• detailed anatomical description• less demand on arthrography• radiologist analysis• « significant » influence on therapeuticdecisions




MRI dangers
• patient and doctor read the report of the radiologist
• …and the images…• MRI should not take the place of the anamnesis and the clinical examination
• increase of surgical indications based on MRI

The case of the day…
• 48 y. old female patient, sports teacher• no health problem• no medical antecedents• right knee pain since 6 mo. without anyaccident
• has difficulties to demonstrate exercices in herclass, has pain when she pratices her sports : badminton and alpine skiing

The case of the day…
• right knee dry and stable• slight varus axis deviation• pain on the medial femoro‐tibial joint line• no jump of the meniscus• imaging

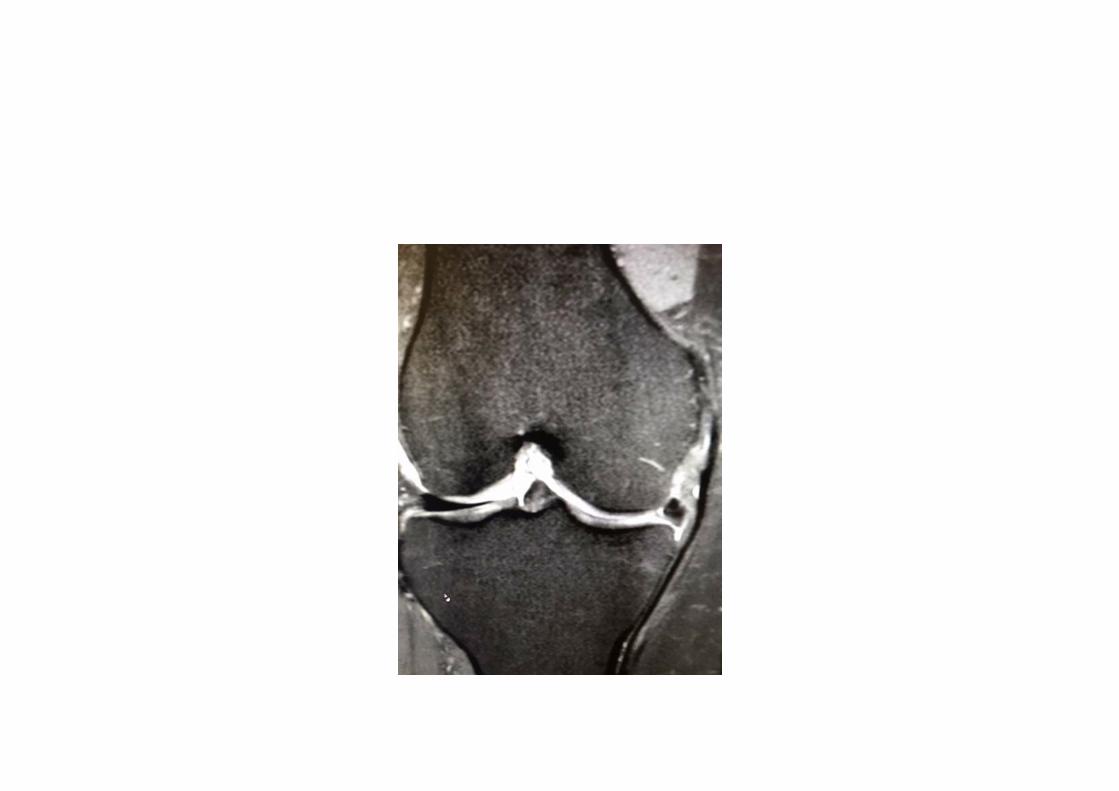
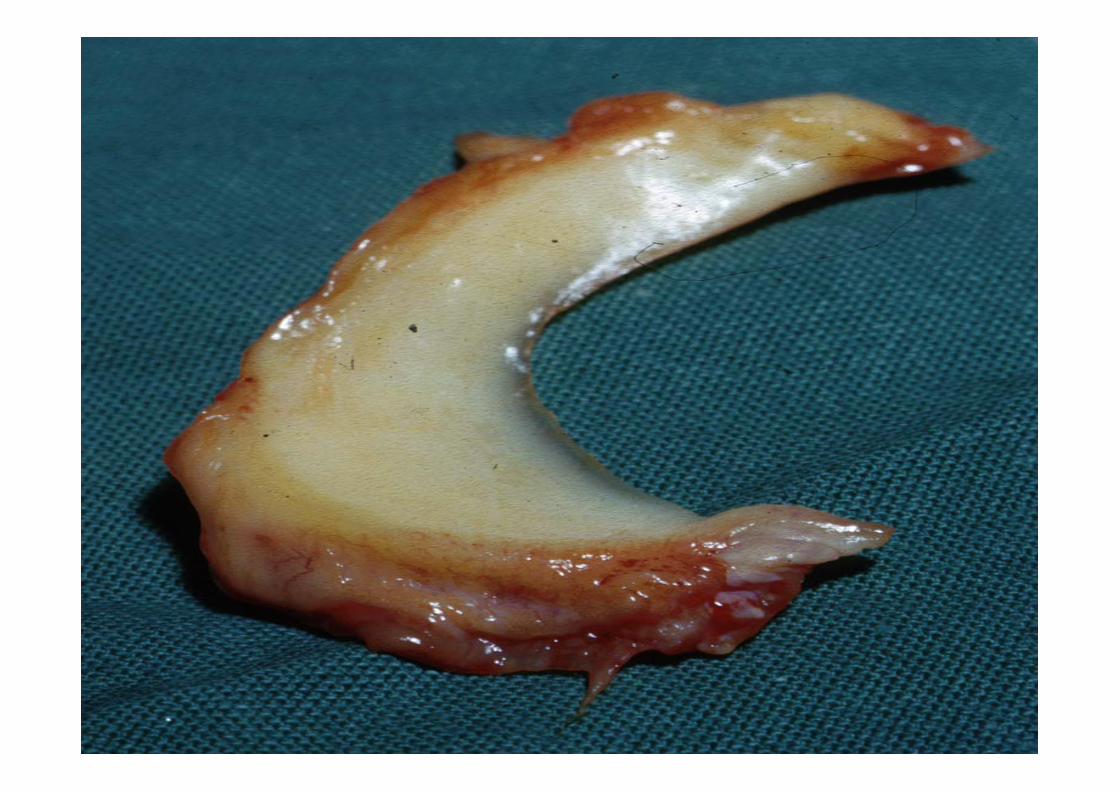
What do we see here ?



Extrusion of the meniscus
• > 3 mm• high correlation witharthrosisLerer DB, Skeletal Radiol 2004
• with painful arthrosisGale DR, Osteoarthritis Cartilage 1999
• loss of the meniscalfunction








Do not forget…

Meniscal lesions
• traumatic :• tears, often with a mobile flap• peripheral desinsertion• extension deficit, jump (ressaut)
• degenerative : no accident history, gradualdevelopment of a joint line pain, no jump atclinical ex.

Meniscal lesions
• traumatic lesion : surgery is possible• degenerative lesion : prudence, in principle no surgery
• in theory : save the the meniscus
The future
• allografts : limited hope, no meniscus tissue bankin Europa… except Ghent in Belgium
• synthetic meniscus…nothing new since the CMI• 2003 : first sequencing of the human genome (3 billions of bases or nucleotides, Adenin, Cytosin, Thymin, Guanin)
• development of the personalized medicine• meniscus autograft, reconstructed from stem cells and growth factors ? We may dream…!


Remember !