scale up ppm in myanmar - world health organization · scale up ppm in myanmar . china laosmagwe...
TRANSCRIPT

Public Private Mix sub group meeting
23 October, 2011
Dr. Thandar Lwin
Programme Manager
National TB Programme, Myanmar
Scale up PPM in Myanmar

CHINA
LAOS
THAILAND
INDIA
BANGLA
DESH
KACHIN
SHAN
SAGAING
CHIN
RAKHINE
MANDALAY
MAGWE
BAGO
AYARWADDY
YANGON
KAYIN
KAYAH
MON
TANINTHARYI
Area - 676,578 sq.km
Regions/States - 14
Districts - 67
Townships - 330
Sub Townships - 60
Wards - 2,781
Village tracts - 13,714
Villages - 64,910
Population - 57 millions
Urban - 30%
Rural - 70%
Myanmar

A major public health problem
Estimated incidence all forms (2010) 384/100,000 pop.
Estimated prevalence of TB (2010) 525/100,000 pop.
Estimated TB mortality (2010) 49/100,000 pop.
(Global TB control: a short update to the 2010 report, WHO, Geneva. 2011)
MDR-TB among new TB patients 4.2% (2007-08)
HIV prevalence among new TB patients 10.4 %
(2010, in 20 sentinel sites)
Magnitude of TB in Myanmar

Achievement of NTP in 2010
Total TB patients notified = 137,403 (CNR = 279/100,000 pop.)
Total smear positive TB patients notified = 48,783 (CNR = 99/100,000 pop.)
New smear positive TB patients notified = 42,318 (CNR = 86/100,000 pop.)
CR = 77%, TSR = 85%

Smear Positive Case Bacteriologically confirm Case
>15 Yrs No. /100,000 95% CI No. /100,000 95% CI
All Participants 123 242.3 (186.1 - 315.3) 311 612.8 (502.2 - 747.6)
Strata Region 70 191.6 (137.4 - 267.3) 192 522.8 (420.9 –649.1)
State 53 369.0 (235.6 - 577.5) 119 838.0 (560.3–1251.5)
Urban/
Rural
Urban 38 330.7 (216.2 – 505.7) 103 903.2 (661.8-1231.5)
Rural 85 216.1 (153.6 – 304.0) 208 526.8
All Age S(+) prevalence 172/100,000 Bac(+) prevalence
434+/100,000
Prevalence of TB among aged 15 years and above (2009-2010)

Background for PPM
• Public-Private Mix-DOTS: PSI and MMA are coordinating with NTP.
• Lab. using by PPs are under EQA (358 public labs + 62 private labs)
• Political commitment - policy on Private- Public Mixed DOT was adopted
in 2003.
• Operational guideline on Public Private Mix was developed by NTP
together with PSI, MMA, JICA and WHO and published in 2005.
• Public-Public Mix-DOTS : 4 Public Hospitals started in 2007
• Other health related department: Ministry of Labors, Ministry of Home
Affairs, Ministry of Defence, Ministry of Railway
• Involvement of INGOs – 11
JATA, UNION, WVI, Pact, AHRN, IOM, Merlin, Malteser, MSF-H,
MSF-Switz, MDM
• Local NGOs – MWAF, MMCWA, MMA, MRCS, MHAA

Current approaches
1. Advocacy meeting and Training on TB control
2. Drugs and lab. Supplies distribution from NTP
3. Endorsement and Dissemination of International Standards for
Tuberculosis Care (ISTC) among Myanmar National Health
Professional Associations
4. Offer of incentives to engage care providers
- NTP - No incentive.
- PSI - To providers, incentives at regular intervals
(transportation, nutrition, money)
- MMA – in kind to PPs, enablers and incentives to patients
5. Supervision, M&E
6. TB screening at work place in collaboration with Occupational Health
7. OR – for involving pharmacies and informal health care providers.

Public Private Mix in Myanmar
• In Public-Public Mix currently there are two main non-NTP care
providers in Myanmar
(1) PSI
(2) MMA
• In collaboration with private parishioners, there are currently three
schemes available for engagement of private parishioners in TB
control:
• Scheme 1-Health Education and proper referral of TB suspects
• Scheme II- Health Education, referral and act as a DOT provider
• Scheme III referral, diagnosis and treatment provision to run an
affiliated DOT clinic

PPM with PSI
• Population Service International (PSI) started the collaboration with
NTP in March 2004.
• PSI organizes the PPs and running the “Sun Quality Clinics’’ as
DOT units.
• PSI is implementing Scheme 3.
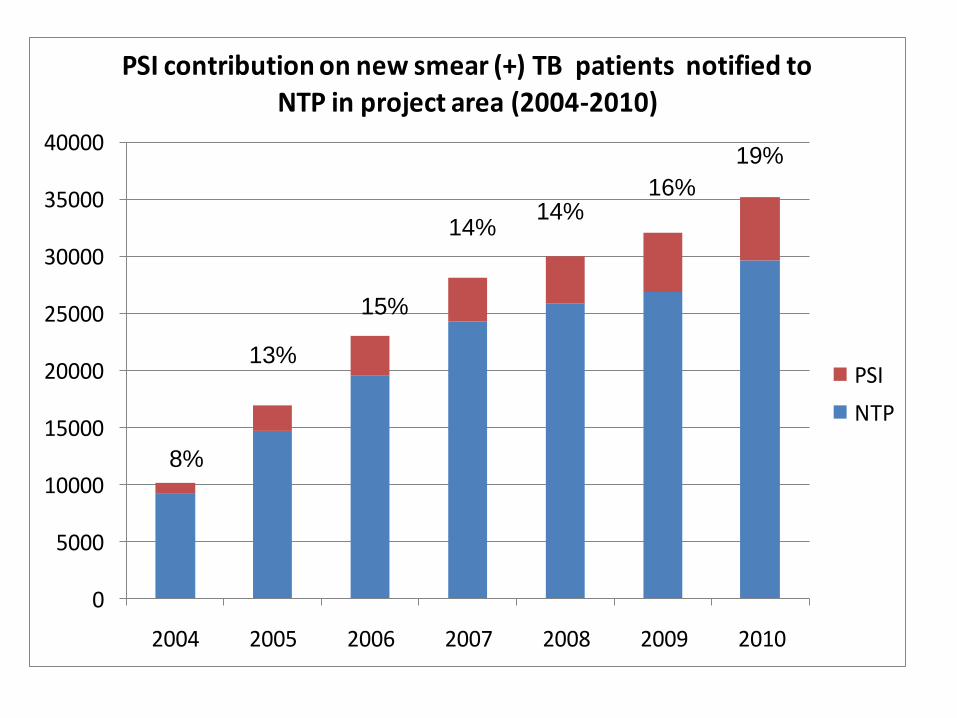
• In 2010 - PSI contributed 12.1% of new smear positive pulmonary
TB patients notified to NTP and achieved Treatment Success Rate
- 85%.

Year No. of
Providers
No. of
State/Region
No. of
Township
2004 101 2 24
2005 222 5 48
2006 316 8 70
2007 413 9 100
2008 505 11 120
2009 623 11 145
2010 731 12 168
2011 up to
July 855 13 189
PSI--Area coverage of PPM-DOTS network
10
108 new providers in 23 new townships in 2011

Year
No. of
Private
Lab
No. of
NTP Lab Total
2004 6 6
2005 19 4 23
2006 23 27 50
2007 31 53 84
2008 35 71 106
2009 40 87 127
2010 42 126 168
2011 up to
July 49 144 193
PSI-- Expansion of sputum microscopy centers
11

0
20000
40000
60000
80000
100000
120000
2004 2005 2006 2007 2008 2009 2010
PSI contribution on all type s of B cpatients notified to NTP in project area (2004-2010)
PSI
NTP
7%
11%
13%
12%
11%
15%
15%
0
5000
10000
15000
20000
25000
30000
35000
40000
2004 2005 2006 2007 2008 2009 2010
PSI contribution on new smear (+) TB patients notified to NTP in project area (2004-2010)
PSI
NTP
8%
13%
15%
14% 14%
16%
19%

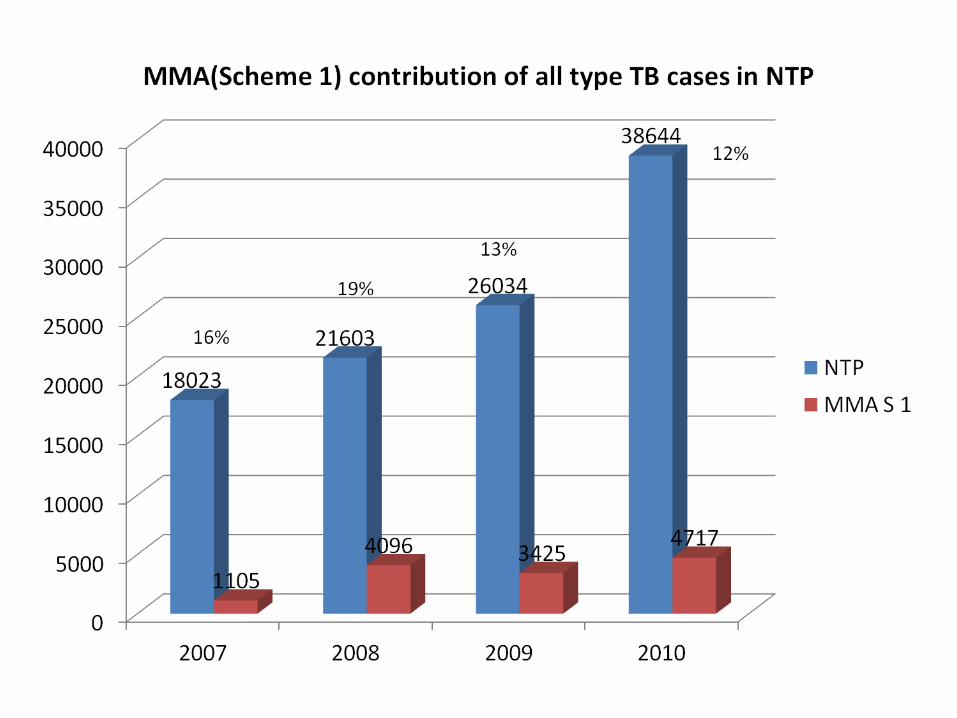
• Myanmar Medical Association (MMA) started in 2005
• MMA use three schemes:
• In 2010, 70 townships have been covered and 914 PPs are
implementing Scheme 1, 118 PPs are implementing Scheme 3.
• In 2011, MMA is planning to implement in 101 townships.
PPM with MMA


0
2000
4000
6000
8000
10000
12000
14000
2007 2008 2009 2010
5793
6778
8108
12253
410
1577 13862009
MMA (Scheme I) contribution on new smear (+) TB patients notified to NTP in the project area (2007-2010)
NTP
MMA S 1
7%23%
17%
16%

0
2000
4000
6000
8000
10000
12000
14000
16000
2007 2008 2009 2010
69627943
9608
14449
425
1736 15112181
MMA (Scheme 1) contribution on total smear (+) TB patients notified to NTP in the project area (2007-2010)
NTP
MMA S 1
6% 22%
16%
15%

0
500
1000
1500
2000
2500
3000
3500
4000
4500
2009 2010
30153506
557
651
MMA (Scheme III) contribution on new smear( +) TB patients notified to NTP in project area (2009-2010)
MMA S III
NTP
(16%)
(16%)

17.8%
17.5%

(16%)

NTP, 80.8%
Hospital, 3.0%
MSF-H, 2.1%
PSI, 12.1%MMA, 1.6%
MDM, 0.2%AHRN (Shan North), 0.2%
Proportion all forms of TB patients contributed by NTP and other reporting units (2010)
22

Treatment outcomes of PSI-PPM DOTS (2004-2010)

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NTP PSI AZG MMA
Treatment outcome of new smear positive TB pateints 2006
Transferred out Defaulted FaiIure Died TSR Cured

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NTP PSI AZG MMA
Treatment outcome of new smear positive TB pateints 2007
Transferred out Defaulted FaiIure Died TSR Cured

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NTP PSI AZG MMA
Treatment outcome of new smear positive TB pateints 2008
Transferred out Defaulted FaiIure Died TSR Cured

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NTP PSI AZG MMA
Treatment outcome of new smear positive TB pateints 2009
Transferred out Defaulted FaiIure Died TSR Cured

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
NTP PSI AZG MMA
Treatment outcome of new smear positive TB pateints 2010
Transferred out Defaulted FaiIure Died TSR Cured

Public-Public Mix – DOTS
• Public-Public Mix (between NTP and public hospitals)
– 9 general hospitals
- 2 TB hospitals
- Specialist hospitals especially treating HIV patients
- 1 Military hospital
- Workers hospital (TB)
- Central jail, Mandalay

0
5000
10000
15000
20000
25000
30000
35000
40000
45000
2004 2005 2006 2007 2008 2009 2010
30977 36212 39874 42120 40703 40742 41706
431
329
367 468 545 647 612
No
of
NS
(+)
TB
ca
se
s
Years
Hospital Contribution in NTP of NS(+) TB cases
NTP total cases
Hospital total cases
1.4%
0.9%
0.9% 1.1% 1.3% 1.6% 1.5%

0
5000
10000
15000
20000
25000
30000
35000
40000
45000
50000
2004 2005 2006 2007 2008 2009 2010
36615 41559 45614 48531 46508 46969 47866
746
579
743 720 795 908 917
No
of
All S
(+)
TB
cases
Years
Hospital Contribution in NTP of All S(+) TB cases
NTP total cases Hospital total cases
2%
1.4%
1.6% 1.5% 1.7% 1.9% 1.9%

0
20000
40000
60000
80000
100000
120000
140000
2004 2005 2006 2007 2008 2009 2010
95977 106684 121878 131090 125157 130217 133316
1932 1307
1715 2457 3582
3806 4087
No
of
All
typ
e T
B c
as
es
Years
Hospital Contribution in NTP of All type TB cases
NTP total cases Hospital total cases
2%
1.2%
1.4%
1.9% 2.9% 2.9% 3.1%

Engage all care providers
National Workshop on ISTC
(March 4-5, 2009)
Dissemination Workshop on ISTC
(August 31, 2009)
Introduction to Regional level Hospitals : 13 / 17

Major barriers to scaling up engagement
• Weakness in coordination between Practitioners
• Conceptual changes among private doctors
• Limitation in resources
• Operational barriers at all levels – transportation, health
seeking behavior of patients, patient support, etc.
• Requirement of ACSM strategy

Planned actions to scale up /
strengthen engagement
1. NTP
- To scale up of PPM hospitals up to 21 hospitals by 2015
- To disseminate ISTC up to district / township level
- To involve informal health care providers and drug sellers in TB control
- PAL – to do situation analysis and resources mobilization
2. PSI
- To expand 100 SQH clinics, 500 SPH workers, 20-25 townships
annually to achieve 15% of national case detection by 2015.
- To involve informal health care providers and drug sellers
- To initiate TB/HIV prevention and control activities
- Financial/ logistic support to MDR cases in close collaboration with NTP

Planned actions to scale up /
strengthen engagement
1. MMA-TB
- Further scale-up of Scheme III,
- To establish more Private Labs and sputum collection centers
- To engage all care providers
- To intensify community based TB care activities
- To strengthen infection control and TB-HIV prevention and control
activities
- To involve informal health care providers : Pharmacists, Traditional
medicine practitioners

Thank you