scally and donaldson (1998). clinical quality and good
TRANSCRIPT

1
IQC/2013/23 Improvement and Quality Committee
13 June 2013
NHS TAYSIDE CLINICAL GOVERNANCE FRAMEWORK
‘Clinical governance is a system through which NHS organisations are accountable for continuously improving the quality of their services and safeguarding high standards of care by
creating an environment in which excellence in clinical care will flourish.’ Scally and Donaldson (1998).
Clinical Quality and Good Clinical Governance
=
Patient Safety, Patient Experience, Clinical Effect iveness and Clinical Outcomes 1. INTRODUCTION This Clinical Governance framework for NHS Tayside provides a shared vision within NHS Tayside, to describe a robust Clinical Governance framework providing assurance about the quality of care delivered from the point of care (the clinical microsystem), to the Board. This is a dynamic document focusing on contemporary Clinical Governance. It will continue to be updated as we progress our model of contemporary clinical governance throughout 2013/14 and we expect to have a fully tested and implemented assurance and escalation system in place by April 2014. This framework provides and explains the principles NHS Tayside Board applies to achieving and maintaining safe, better quality and well-governed care and services for patients. It sets these principles in the context of the Board’s strategic approach to providing healthcare – the Business Plan, supporting patients and managing clinical risk and the requirements of the organisations that regulate the work of the Board. The report of the Mid Staffordshire public inquiry into failings there stated that the problems were systemic (Francis 2013). Jeremy Hunt the Health Secretary has also stated that ‘everyone can sense that there are little bits of Stafford dotted around the system' (Hunt, 2013). McSherry (2013) states that clinical governance can be used as a cultural barometer; a system that can quickly gauge the temperature or atmosphere in a clinical team, department or organisation. This framework is important for all staff, as all staff have a clinical governance responsibility and accountability; importantly the Board needs to ensure engagement by all staff. The indicators of success for this framework are an improvement in the patient experience (measured through Patient Experience programme) and an improvement in local outcome measures (key quality indicators).
Item 7.3

2
Principles of Clinical Governance in NHS Tayside:
• Patient at the centre of their care • Communication • Multi-professional working • Focus on improving care • Move from minimising/mitigating risk to managing risk • Make it real for staff and patients • Retain a focus on clinical safety, effectiveness, outcomes and patient experience • Utilise a wide range of information sources • Utilise systematic planning and implementation cycles • Marry national regulation to local priorities
This framework incorporates both quality improvement and quality assurance as part of a continuous cycle of improvement. It is an overarching document covering all aspects of quality and clinical governance within NHS Tayside. Quality includes the nationally defined quality ambitions of ensuring a person centred approach to delivery of care or services, safety and clinical effectiveness (including efficiency). To ensure this the completed Equality Impact Assessment supports and informs priorities from an Equality, Diversity and Spirituality perspective. NHS Tayside already has a number of related specialist strategies and policies; which are considered in conjunction with this document, and in addition, TCOE and the Business Support Unit provide much valued support and advice to the clinical areas. Tayside Centre for Organisational Effectiveness (TC OE) TCOE is committed to NHS Tayside being the "best at getting better." To enable this TCOE supports development of its staff in skills and knowledge for Quality Improvement together with programmes to promote great leadership along with developing culture and values through staff engagement that supports patient centred and compassionate care and supports our quality ambitions. TCOE Improvement Academy and Faculty support clinical teams and staff to deliver education that supports safer clinical practice and innovate ways of working. Links to Risk Management Strategy and SEM Policy: Risk Management Strategy 2012-2015 Significant Event Management Policy

3
2. DEFINITION AND UNDERSTANDING OF CLINICAL GOVERNA NCE AND QUALITY Governance is defined as, “the systems, processes and actions by which (Boards) lead and control their functions in order to meet their obligations and to achieve their goals” (The Verita Brief - Governance, 2009). Clinical Governance is a core component of overall Governance in healthcare services. Front line staff and clinicians operate on a foundation of good clinical governance principles and practice which, by their very nature, are dynamic and responsive in nature - changing to emergent internal and external governance requirements. This dynamic means that good governance is a combination of corporate structures, communication, systems and processes providing assurance and also enabling and supporting professionals and services delivering governance. The underpinning processes are not always immediately visible to those on the front line but this will become explicit. Perversely it is sometimes more evident when good Governance, including good Clinical Governance systems are not in place or not operating well. In the Business world these manifest as Business Failures or crises (Enron et al), and in healthcare as failures to keep safe, or provide care to minimal acceptable standards (Shipman, Mid Staffordshire Hospitals etc). The work of the Clinical Governance and Risk team is to make relevant these processes to front line staff whilst at the same time meeting the internal and external regulator and assurance requirements. Wherever possible they strive to deal with these as efficiently and mutually as possible. Importantly all staff are responsible and accountable for clinical governance; the Quality Clinical Governance and Risk Team provide advice, direction and support. The box below describes the roles different staff have in the organisation with regard to clinical governance.
CLINICAL GOVERNANCE ROLES All staff in NHS Tayside has a responsibility for clinical governance. The responsibility they have is dependent on the member of staff’s role. Clinical and Professional Leads All clinical leads are responsible for providing professional advice and leadership to healthcare professionals, promoting high standards of care and development of clinical practice. This includes offering advice about current clinical governance practice, quality, safety, and service development, being an active member of clinical governance and risk management groups and supporting the continuous improvement of care. Clinical leads and SCN’s work together to ensure robust multi-professional clinical governance structure and meetings which feed up the line to the CQF and I and Q. Managers All managers are responsible for effective clinical governance and risk management measures within their own area. NHS Tayside has an established framework for the management of risk and the implementation of continuous improvement and all line managers must be committed to implementing these. They own these processes and take action, both proactively and reactively, in relation to workforce development, risk management and dealing with patient feedback. In addition they ensure a high quality service to patients by the continual development of practice according to research evidence and national standards. Staff All staff have a general responsibility to initiate action by suggesting and implementing improvements to services and in exercising professional responsibility for both themselves and their peers within an open, just and fair culture. It is vital that all staff take responsibility for promoting the health, safety and security of patients and carers, the public, colleagues and themselves.

4
Origins of Clinical Governance The concept of Clinical Governance was introduced to the NHS in 1999 through Health Services Circular 1999/065: Clinical Governance in the new NHS. It was described as a “framework through which NHS organisations are accountable for continually improving the quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish.” (Scally and Donaldson 1998).
Formal NHS Scotland Health Department guidance on Clinical Governance consists of:
MEL (1998) 75 MEL (2000) 29 HDL (2001) 74 New guidance on healthcare governance, including clinical governance, is imminent from the Scottish Government Health department. In addition there are draft Healthcare Improvement Standards for clinical governance that are out for consultation. In 2005 the Scottish paper Building a Health Service Fit for the Future identified the challenges to health and well being of an ageing population, persistent health inequalities and a growth in long term conditions. The report stressed that the then model of healthcare was not sustainable in the longer term, and a new model that transformed the quality and accessibility of services was required. This report was followed by Better Health Better Care (2007) which identified the need to provide a health service which ‘works together with its partners, places the patient at the heart of everything it does, integrates care, realises efficiencies and ensures the highest standards of quality and safety’. One of the objectives within Better Health Better Care was continuous improvement, with an assurance that NHS Scotland would be focused on improving quality, addressing excessive variation in practice, and ensuring the highest standards of patient safety. Clinical Governance Today Clinical governance is a system, or framework, for co-ordinating the following activities and themes to inform and progress the improvement in NHS Tayside’s services, ensuring they are safe, effective, person centred and based on the best available evidence and practice.
• Service user, carer and public involvement • Patient/carer experience and feedback to inform practice • Clinical effectiveness • Clinical risk management • Patient safety • Education, training and development • Use of information • Outcome measures • Staffing, skill mix and staff management • Clinical audit

5
The diagram below shows the scope of clinical governance.

6
The NHS Scotland Healthcare Quality Strategy This was published in 2010 with four quality ambitions: Person Centred Mutually beneficial partnerships between patients, their families and those delivering healthcare services which respect individual needs and values and which demonstrate compassion, continuity, clear communication and shared decision making. Safe There will be no avoidable injury or harm to people from healthcare they receive and an appropriate, clean and safe environment will be provided for the delivery of healthcare services at all times. Effective The most appropriate treatments, interventions, support and services will be provided at the right time to everyone who will benefit, and wasteful or harmful variation will be eradicated. Quality Infrastructure Create the necessary governance and delivery structures across NHS Scotland so that the interventions we pursue are clearly and appropriately integrated, aligned and managed. Quality and Clinical Governance are interdependent and delivered by quality improvement and quality assurance making up a cycle of continuous improvement. Clinical Governance systems identify areas for improvement through monitoring of measures, standards, incidents and processes. Quality improvement initiatives are developed and implemented using the Model for Improvement, and then the clinical governance systems monitor and review the outcomes and experiences of patients for improvements. Clinical governance aims to strengthen quality, and all aspects of service design and delivery at an individual, team and organisational level. Care governance is the overarching approach to providing NHS Tayside with assurance about clinical governance, quality and standards of care and patient, family, carer and staff feedback. Clinical Governance includes the concepts of “patient safety” and “clinical quality”. It “encapsulates an organisation’s statutory responsibility for the delivery of safe, high quality patient care and it is the vehicle through which that accountable performance is made explicit and visible.” (Halligan, 2005). Therefore, Guidance on Clinical Governance states that all Boards have an explicit responsibility for:
• Ensuring that Clinical Governance principles, processes and systems are embedded through the Board and within the organisation.
• Ensuring compliance with the statutory duty of quality and principles of Clinical Governance and patient safety.
• Ensuring that at a local level they have in place systems and processes to ensure the delivery of safe, high quality care.
• Ensuring the implementation of the national quality imperatives e.g. Healthcare Improvement Scotland directives, standards and guidelines
• Ensuring participation in national confidential inquiries. • Ensuring that all clinicians are involved in regular clinical audit and review of clinical services. • Assessing performance and identifying training needs for all staff. • Developing an open culture within the organisation where incidents are reported and lessons
are learned. • Ensuring effective risk management processes and accounting for Clinical Governance
responsibilities when signing their statement of internal control. • Monitoring trends in key clinical quality and clinical outcome measures. • Maintaining a focus on continuous, demonstrable improvement in the quality of patient
experience and improvement in health care outcomes.

7
• Involving partners in service provision in Clinical Governance activities. • Assuming and making clear the joint accountability for services which are provided on a multi-
agency, multi-sector basis. • Reporting to the relevant Commissioners on Clinical Governance activities.
3. AIMS OF CLINICAL GOVERNANCE AND THIS FRAMEWORK The vision for NHS Tayside is for better health and better care for the people of Tayside. National and international evidence indicates that better quality, safer care is more efficient and delivers financial benefits; and a motivated highly performing workforce produces better outcomes of care for patients. The terms quality and excellence are not clearly definable and therefore there is a need to define clinical governance in more objective terms. Examples of the outcomes of safe, effective and person centred care include:
• Reduced mortality • Reduced avoidable harm • Improved patient experience • Delivery of evidenced based care • Safely reducing cost and improving productivity
Clinical Governance focuses on a number of activities which achieve measurable improvements in patient experience of care and outcome of care within the Institute of Medicine’s six dimensions of quality:
• Safe • Effective • Person centred • Timely • Efficient • Equitable
The aim of this framework is also to describe a structure to deliver this vision, enabling clinical governance to be part of core work at both strategic and clinical practice level. 5. LOCAL CONTEXT It is recognised that a systematic approach to assessing and managing clinical governance is required to deliver high quality patient care. As accountable officer the Chief Executive has overall responsibility for corporate governance including clinical governance. The responsibility for ensuring that NHS Tayside has effective arrangements and processes in place for clinical governance is discharged through the Improvement and Quality Committee with senior professional leadership provided by the Medical Director, Nurse Director and Chief Operating Officer, General Manager Access Directorate and Director of Tayside Centre for Organisational Effectiveness, who are the nominated executive leads for clinical governance. In this function the Medical Director, Nurse Director and Chief Operating Officer are supported by the Head of Clinical Governance and Risk. The framework:
• Provides a mechanism of the guiding principles and quality goals for NHS Tayside • Identifies how clinical governance is implemented within NHS Tayside • Outlines the organisational structures and lines of accountability for quality, clinical governance
and risk management • Identifies the support for implementing clinical governance

8
• Provides a framework for agreeing, implementing and monitoring an annual Clinical Governance work programme
• Describes the engagement
At the micro-system level, (the local point that the patient and/or carer interacts with the healthcare service) key quality indicators (KQIs) are determined by the patient, carer and healthcare team. Clinical governance activities are focused around developing, implementing, monitoring and reviewing these indicators using the Model For Improvement. Reliable measuring, reporting and monitoring of these indicators are being progressed using e-health solutions such as Qlikview. Examples of these KQIs include: incidence of falls; infection rates and incidence of complaints, other indicators are more local such as adherence to stroke standards, monitoring of complication rates, and level of self care for patients with a long term condition. Indicators are currently at varying levels of ‘maturity’; clinical governance systems, processes and support will focus on making these more reliable and consistent at the micro-system and improve reliable reporting from micro-system to Board. Table 5 shows a current example of the reporting tool used in the Access Directorate. A series of workshops have been agreed, the first held in April 2013, started the process of achieving reliability with a whole systems approach to Clinical Governance. Another 2 workshops are planned over summer 2013 and the framework will be updated in terms of the output from these, as they occur. Operating Model of Clinical Governance The core elements of the operational framework:
To provide assurance that the Organisation provides safe and effective care with outcomes that meet published standards; evidences learning from feedback, incidents and complaints and meets patients expectations. This aim is underpinned by assurance of:
• reliable provision of safe and effective care
• reliable risk management processes
9
• a culture that listens to and acts on patient and public experience
• productive and efficient care
Table 3 and 4 shows the assurance process flow from patient to Board and Board to patient. Directorate / CHP Arrangements Each Directorate and CHP is required to have a local Clinical Quality, Governance and Risk Group which meets regularly to discuss and oversee all governance issues. To ensure accountability the Directorate / CHP are required to submit a summary of their findings and minutes of meetings to the Clinical Quality Forum. Each Directorate / CHP are required to ensure there is sufficient clinical representation on the group. Key Quality Indicators Whilst the main delivery of governance occurs within each of the Directorates /CHP’s and corporate departments the Chief Operating Officer has a crucial role through EMT in:
• Providing direction and impetus for action
• Facilitating change within directorates / CHP’s,
• Agreeing a core set of KQI’s and providing the directorates / CHP’s with the tools, skills and methodologies to support their clinical governance plan.
• Ensuring consistency of approach and linkages through divisions and corporate departments through each directorate / CHP:
o agreeing the service specific KQI’s to ensure improvement year on year
o providing assurance (evidenced by KQI’s, walkabouts, HEI reports etc) to demonstrate compliance with standards and other relevant measures.
o Share and learn from areas of good practice both when things go well and when things could be improved.
The core set of KQI’s are outlined in Table1 through which compliance with the framework will be monitored. THE ROLE OF THE BUSINESS UNIT IN SUPPORTING CLINICA L GOVERNANCE
The BU is an enabler that supports the organisation in quality measurement, performance monitoring and reporting through the provision of high quality, timely and accessible information to clinicians and managers. A range of quality assurance information and reports are being provided. This is being enhanced by the development of dashboards that provide near time information and measurement systems that will support clinicians and managers to monitor how safe and appropriate the care and treatment they provide is and to identify opportunities for improvement to ensure a high quality and reliable patient experience. The dashboard programme is informed by a number of operational key quality performance indicators to provide quality improvement and performance information at a patient, ward/ team/department and service level as well as higher level aggregated information for clinicians, managers and multi-disciplinary teams. Investment is being made in supporting the development of relevant clinical outcome measures, patient safety and experience measures that will be displayed in a way that supports easy interpretation of the information to underpin improvement, performance management and assurance.

10
NHS Tayside, through its investment in QlikView and CKHS, has started to align its use of measures for performance management and quality assurance through the Business Unit. This is augmented by regular reports at all levels of the organisation that show trends against compliance levels for key quality indicators including those for patient safety. Over time the range of indicators are being extended and will reflect the national Quality Measures Framework. A network of Business Intelligence Hubs aligned to operational service provision are being established, which bring together a range of risk, safety, patient experience, business analysis information and improvement support staff to:
• Familiarise and empower local teams to own, understand and use the business intelligence systems available;
• Support front line staff, clinical leaders and managers to triangulate near real-time data across a number of key measures to support identification of areas of risk and where improvements are required;
• Reduce duplication of data entry, which in turn releases time for clinical care; • Support clinical service teams to understand how to use their data to identify areas of
concern and demonstrate measurable improvements in quality of care; • Assist in the provision of intelligent information and regular reports to support effective
decision making at patient level through to board and national assurance levels.
11
NHS Tayside Strategic Goals
The overall vision of NHS Tayside is
‘Working with you for better health and better care’
The values of NHS Tayside are:
● Valuing People ● Valuing Health ● Valuing Quality
The Strategic Aims of NHS Tayside are:
• Contribute to closing the health inequalities gap within a generation • Improve health life expectancy by supporting people to look after themselves • Ensure that services meet agreed quality standards, especially patient experience • Be cost effective in all decisions, actions and services
To achieve this, the Board needs to provide services based on the following principles:
• Person/Patient Centred care • Clinical excellence • Valued & skilled workforce • Effective partnerships
and to run an organisation that is:
• Well governed • Financially viable • Legally constituted • Upholds the values & principles of the NHS
These goals and principles bring the aspirations of NHS Tayside together. These aspirations are:
a) Provide services that are safe, person centred, delivered in appropriate environments and sensitive to the needs of the individual
b) Retain the confidence of patients, carers and partner organisations by upholding the principles of the NHS
c) Be an excellent employer maximising the skills and talents of our valued workforce d) Ensure a firm financial foundation underpins delivery of our vision e) Work in partnership with other organisations and local councils to develop seamless provision f) Through the use of evidence based practice, provide high quality services, to establish a
reputation for exceptional standards of care g) Use our positive reputation to develop new services and expand existing ones h) Provide and develop services that are efficient, cost effective and responsive to the needs of
the people who use them i) Work with our members to achieve our vision
The implications of these aspirations on clinical strategy are the need for a robust approach to risk management. All key risks in NHS Tayside are recorded in the Electronic Risk Register and are divided into one of two categories of either Corporate or Operational Risk.

12
Corporate Risks are risks which are at the highest level within the Organisation. These are always owned by an Executive Director and are reported to the most appropriate Standing Committee of Tayside NHS Board on a biannual basis. The corporate risk profile of NHS Tayside is regularly reviewed and mapped with the corporate objectives of the organisation by the Risk Management Department in conjunction with the Deputy Chief Executive on an annual basis and all corporate risks must be agreed by the Strategic Risk Management Group before entry into the risk profile.
Operational Risks are all other key risks which are owned by a member of staff, who has received Electronic Risk Register User Training, within NHS Tayside. However, these must be linked to a parent Corporate Risk. These operational risks are reviewed as portfolios of risk by an identified lead individual through the Critical Systems Checklist.
If it is felt that any existing Operational risk should be altered to Corporate status as it has implications for the whole organisation, a proposal detailing the risk and the reasons behind this must be presented to the Strategic Risk Management Group for approval and allocation.
• a risk management framework • a clinical governance framework • a governance committee and supporting structures • an assurance framework • a comprehensive risk register • training and support for NHS Tayside Board members and members of staff
Good clinical governance relies on many aspects coming together: patients, carers and the public being involved in their own care and in the work of NHS Tayside; clinical effectiveness; motivated workforce; effective structures systems and processes for clinical risk management, education, training and development, use of information, clinical audit. The duties of NHS Tayside Board are to:
• Ensure that required standards are achieved • Investigate and take action to address sub-standard performance • Plan and drive for continuous improvement • Identify, share and ensure the delivery of the best possible practice • Identify and manage risks to maintaining and improving the quality of care • Tie these together with external stakeholder consultation and internal service/staff engagement

13
Table 1 Strategic Clinical Governance Planning Process using Key Quality Indicators as the high level focus.
Patient Safety Clinical Effectiveness Patient Experience Clinical Outcomes
1.
Review existing KQIs with Stakeholders
Review existing KQIs with Stakeholders Dates in each?
Review existing KQIs with Stakeholders
Review KQIs with Stakeholders
2.
Commence Consultation on KQIs 2013’14 with Stakeholders
Commence Consultation on KQIs 2013’14 with Stakeholders
Commence Consultation on KQIs 2013’14 with Stakeholders
Commence Consultation on KQIs 2013’14 with Stakeholders
3.
Identify Top 3 issues at; National Local area Stakeholder
Identify Top 3 issues at; National Local area Stakeholder
Identify Top 3 issues at; National Local area Stakeholder
Identify Top 3 issues at; National Local area Stakeholder
4.
Identify Top 3 issues from; Incidents Complaints & feedback Clinical Audits Research evidence SIGN Guidelines Patients Issues Staff Issues
Identify Top 3 issues from; SIGN Guidelines Research evidence Clinical Audits Staff Issues Patients Issues Incidents Complaints & feedback
Identify Top 3 issues from; Patients Issues Staff Issues Complaints & feedback Incidents Clinical Audits Research evidence SIGN Guidelines
Identify Top 3 issues from; Patients Issues Staff Issues Complaints & feedback Incidents Clinical Audits Research evidence SIGN Guidelines
5.
Identify Top 3 issues at; Organisational Business Unit Team/Service
Identify Top 3 issues at; Organisational Business Unit Team/Service
Identify Top 3 issues at; Organisational Business Unit Team/Service
Identify Top 3 issues at; Organisational Business Unit Team/Service
6.
In each case ensure they are; High Impact Part of service delivery Goals & plans SMART Have clear ways of monitoring achievement
In each case ensure they are; High Impact Part of service delivery Goals & plans SMART Have clear ways of monitoring achievement
In each case ensure they are; High Impact Part of service delivery Goals & plans SMART Have clear ways of monitoring achievement
In each case ensure they are; High Impact Part of service delivery Goals & plans SMART Have clear ways of monitoring achievement
7. Bring these together to form the Board Top 3 at Team/Service, Business Unit & Organisational level
8.
Board use decision making criteria to recommend final set of draft KQIs for next year (e.g. 2013’14)
9. Complete Stakeholder consultation to challenge and confirm KQIs for next year

14
Table 2: Quality Goals The table below describes the principle quality dimensions relating to clinical governance and the goals associated with them. The Quality Goals provide a framework for NHS Tayside to bring together a wide range of initiatives and programmes all of which contribute to improving the quality of patient care. A range of strategies and plans pre-exist to oversee these individual initiatives and programmes as well as action plans and programme plans which drive the process of implementation. These initiatives are implemented in partnership with staff side and by a number of departments including Safety, Clinical Governance and Risk, Service Improvement, Organisational Development, Nursing and Midwifery Directorate, Medical Education, Public Engagement Team, and Communications Team.
Quality Dimension Quality Goal Patient Safety We must do no harm to patients:
• This means ensuring the environment is safe and clean, reducing avoidable harm such as drug errors or rates of healthcare associated infections
Patient-Focussed Services Quality of care includes quality of caring:
• Planning and delivery of services should be designed using patient centred principles • Patients should be treated with consideration and respect • Patients should be involved in and informed about all decisions on their “pathway of care” • Patients should know that privacy, dignity and confidentiality will be respected
Clinical Effectiveness and Research
Patients should receive treatment, care and support for health improvement based on the best evidence available:
• Healthcare professionals are encouraged to ensure that their practice is based on the best evidence available
• We will support healthcare professionals in the achievement of this aim by ensuring that clinical evidence is integral to all clinical care and by the development of a research
culture • Good practice will be disseminated and under performance will be addressed
Continuous Improvement We will continually and systematically review and improve our health care processes and
working practices to improve care for patients: • This will be based on the development of care models and whole system patient
pathways including focusing on prevention, health improvement and maximizing self care
• We will promote the importance of co-operative and collaborative partnerships with all agencies to bring about improvements in health in the general population and to ensure that patients receive comprehensive care
• This will be part of a culture of continuous improvement
Fairness and Consistency We will promote equality of access, treatment and opportunity for all and work to reduce inequalities in health:
• We will work to understand better the particular health and healthcare needs of our different communities and influence the design and delivery of services accordingly
• We will aim to have a community that is well informed, motivated and interested in its own health
Competence and Continuous Learning
Patients should have services provided by staff that are trained for the job and take part in ongoing training:
• We will ensure that we have appropriately qualified staff (trained for the job and working to national standards and competencies) and ensure continuing professional development of all our healthcare professionals
• Our staff will have equality of access to training and development opportunities
Risk Management We will minimise the chances of things going wrong:
• We will learn from incidents and near-misses • We will manage risks by targeting underlying system weaknesses
Governance and Leadership
We will ensure that there is a robust framework, systems and processes for clinical governance which is monitored for effectiveness and reviewed:
• We will ensure there is a strong role for clinical leadership in clinical governance

15
• We will measure and understand what we do and make data on how well we are doing this widely available to staff, patients and the public in order to help us understand variation and best practice and focus on improvement
• We will work within a Rights Based Practice and within legal frameworks

16
Table 3 – Levels of Clinical Governance and Roles
Levels Roles Leads Groups Achieved by
Teams, Individuals, Local care governance groups at the micro-system
Putting Strengthening Quality Goals into practice
All clinical and support staff
Wards, Teams, Departments, Services
• Professional Codes of Practice • CPD • Audit • Evidence Based Practice • Personal Reflection
Support Departments And Directorates
Supporting the Quality Goals
Clinical Governance Clinical Leads
Head of QCG&RM
Service Improvement Leads
Clinical Effectiveness
Research &
Development Manager
Risk Managers
Public involvement
Clinical Governance
and Risk Management Department
Public Involvement team
Collaborative and Improvement Programmes
Practice
Development Centre
Practice Development Nursing Team for Mental Health
Organisational Development
Communications Department
Providing support and advice to all levels in the organisation Core support in clinical effectiveness, research & development, patient safety, risk management, patient feedback and service reviews
Management Boards, Groups and Teams Care Governance group/ Improvement And Quality Committee
Delivering Quality Goals
Associate Medical Directors
Associate Nurse
Directors
Associate Director of AHPs
General Managers
Clinical Directors
MCN Clinical Leads
GP Leads
Senior Nurses
Partnership
Directorate Clinical Governance Meetings
Joint CHP Clinical Governance and
Risk Management
Board
Managed Clinical Networks
Ensuring systems are in place to deliver to Clinical Governance Principles Framework Development
NHS Tayside Board
Overseeing the Quality Goals
Non Executives
Chief Executive
Medical Director
Nurse Director
AHP Deputy Director
Director of Public
Health
Other Executive
Directors
CG Clinical Leads
Chair Area Clinical
Forum
Chair Area Partnership Forum
Health and Clinical Governance
Committee
Health and Clinical Governance Steering Group
Area Clinical Forum
and Professional
Advisory Committees
Act as guardians of the Clinical Governance Goals. By visiting different parts of the organisation to: o Learn about good practice o Listen to accounts of how principles are being applied o Identify areas of concern

17
The Clinical Governance structure for NHS Tayside enables the:
• Definition of the overall scope of clinical governance • Provision of an assurance that a structure is in place to improve the quality of care • Assurance through monitoring of a demonstrable improvement in the quality of care
One workshop has been held and two additional workshops have been arranged to ensure a Tayside wide approach to robust local clinical governance systems and structures. All clinical areas and communities have local structures that report via specialty/directorate /CHP to the Clinical Quality Forum, and onto the Improvement and Quality Committee as described in the following diagram

18
Clinical Governance and Risk Reporting Framework Clinical Governance Framework informed through work shops
Improvement & Committee Receives assurance from
Clinical Quality Forum
Clinical Quality Forum
To manage the clinical governance and quality assurance activities within NHS Tayside
Directorate and CHP Clinical Governance Leads •Risks •Red Incidents •Complaints/Claims •SCEA/ Ombudsman •External body recommendations •Person centred care/stories/experience •Public involvement •Patient safety •Clinical effectiveness to include inspections and s tandards
Provides assurance to CQF that a robust mechanism exists to review and implement improvements
Hub Working
Safety Clinical Governance and Risk Team
Provide support and leadership to NHS Tayside services to deliver and give assurances to patients, the public and NHS Tayside Board
Safe, Effective and Person Centred Care
NHS Tayside Board
Audit Committee
Strategic Risk Management Group
Evaluating systems and process for RM, monitor corporate risk profile
Reviewing the systems and processes in place for risk management
Operational Risk/H&S Management Group
Table 4

19
� RELIABLE PROVISION OF SAFE AND EFFECTIVE CARE
Compliance with SPSP, CQI and HAI Measures and Reduction in Preventable Harm
REF: MEASURE
● Non-Compliant ● Compliant
TARGET Feb 2013 TREND
(Please be aware of chart axis varies depending on information and targets)
1 SB
% compliance with hand hygiene (Opportunity) ≥95%
97.5%
●
2 SB
% compliance with hand hygiene (Technique) ≥95%
96.21%
●
3 SL
Staphylococcus Aureus
Bacteraemia Rate (per 1000 AOBD)
<0.1 0
●
4 JH/ LH
Pressure ulcer incidence rate <0.1 0.02
●
5 JH/ LH
Falls incidence rate <0.2 0.04
●
6 JH / LH
Surgical site infection rate 0
Not submitted
●
7 JH / LH
Medication error numbers 0 0
●
8 EH/CC
Incorrect Blood Component Transfused
0
Not submitted
●
9 DS
Number of outstanding IR(ME)R non-compliances
0 0
●
10 DS
Number of Ionising Radiation Regulations standards not met 0
0
●
11 DG
Number of Clinical Pathology Accreditation standards not
met 0
0 ●
.
Table 5
20
4. REFERENCES Department of Health, 1997. The New NHS. London. Stationery Office. National Health Service and Community Care Act, 1990. London. HMSO. Halligan, Prof A - Clinical Governance: assuring the sacred duty of trust to patients. Clinical Governance Support Team: 2005 McSherry, R et al 2013. Can clinical governance act as a cultural barometer? Nursing Times 109: 19 12-15 Scally and Donaldson L.J. British Medical Journal 1998; 317: 61-65 APPENDICES Appendix 1 – Strategic Risk Management Group Terms of Reference
21
RISK MANAGEMENT
Strategic Risk Management Group Terms of Reference
Author: Tayside NHS Board Corporate Services and Safety, Governance and Risk Department
Review Group: Strategic Risk Management Group
Review Date: April 2014 Last Update: April 2013
Document No: 1 Issue No: 3
UNCONTROLLED WHEN PRINTED
Signed: Executive Lead – Chief Executive (Authorised Signatory)
Appendix 1

22
NHS TAYSIDE STRATEGIC RISK MANAGEMENT GROUP (SRMG) TERMS OF REFERENCE (APRIL 2013) 1. Chairperson and Executive Lead The appointed Chairperson of the Strategic Risk Management Group is the Accountable Officer and Chief Executive of NHS Tayside. The Lead Officers of the SRMG are the Safety, Governance and Risk Co-ordinator and the Board Secretary. 2. Support Officer Items for the agenda should be submitted to the Board Secretary who, in conjunction with the Safety, Governance and Risk Co-ordinator, are responsible for all communications in relation to the NHS Tayside SRMG.
The Board Secretary and the Safety, Governance and Risk Coordinator are also responsible for ensuring Agendas/Papers for the SRMG are sent electronically to the Committee Support Officer in advance of the meeting.
The Committee Support Officer is Alison Hodge who can be contacted on 01382 740761, X40761 or [email protected]
3. Purpose of Group The purpose of the SRMG is to:
• Develop, review, revise and monitor the Corporate Risk Profile of NHS Tayside ensuring risk is mitigated to the lowest possible level.
• Ensure NHS Tayside’s Risk Management and Health and Safety arrangements are robust and comply with National Policy as an integral part of a modern Health Service.
• Identify and assign responsibility for any aspect of risk throughout the organisation.
• Ensure the embedding of Risk Management and Health and Safety into all aspects of planning, business management and service provision within Tayside NHS services.
• Approve, monitor and evaluate progress against an annual Risk Management workplan and report progress to the Audit Committee in order to provide assurance, including setting and monitoring Risk Management Key Performance Indicators.
• Monitor all arrangements to ensure that NHS Tayside’s emergency preparedness and business continuity functions are fully addressed to comply with the Civil Contingencies Act 2004.
• Approve, monitor and evaluate the progress against an annual Resilience workplan.
• Assign responsibility for any aspect of NHS Tayside’s emergency preparedness and business continuity functions as required.
• Ensure that risks associated with Healthcare Associated Infection are embedded into all aspects of planning, business management and service provision and delivery.

23
4. Membership Deputy Chief Executive (Chair) Medical Director Nurse Director Director of Human Resources Director of Finance Director of Public Health
Executive Team Members:
Director of Operations Employee Director Board Secretary Chief Operating Officer
In attendance:
Resilience Planning Officer, or nominee Director, OHSAS, or nominee Lead Infection Control Doctor, or nominee Chair of Resilience Planning Advisory Group Safety Governance and Risk Coordinator, or nominee Associate Medical Director – Primary Care, or nominee 2 * Staff Side Representatives
The Chief Executive has delegated responsibility to the Deputy Chief Executive to be the Chair.
The Group may establish working groups for activities such as the audit of particular practices or any other subject which members consider relevant to the objectives of the Group.
5. Quorum
No business shall be transacted at a meeting of the group unless the following are present:
• at least four Executive Directors or Executive Team Members including the Deputy Chief Executive or his nominee;
• a representative of Safety, Governance and Risk; • a representative of Resilience Planning.

24
6. Frequency of meetings
NHS Tayside SRMG meetings are held quarterly. The Chairperson may decide to hold additional meetings or defer a meeting with the agreement of the NHS Tayside SRMG members.
A single additional meeting will be held in March for the sole purpose of scrutinising, reviewing and evaluating the Organisation’s Corporate Risk Profile.
The dates schedule is as follows:
Tuesday 30 April 2013 9.30 – 11.30
am Seminar Room, Kings Cross
Tuesday 27 August 2013 9.30 – 11.30 am
Seminar Room, Kings Cross
Tuesday 29 October 2013 9.30 – 11.30 am
Seminar Room, Kings Cross
Tuesday 21 January 2014 9.30 – 11.30 am
Seminar Room, Kings Cross
Tuesday 4 March 2014** 9.30 – 11.30 am
Seminar Room, Kings Cross
** This meeting will be single item agenda meeting for the review of the annual Corporate Risk Profile.
7. Remit
Risk Management
• Produce a Strategy and associated implementation plan and processes through identified Executive Lead Directors.
• Discuss, agree and prioritise the component risks that will formulate the Corporate Risk Profile. This will be undertaken through exercises such as horizon scanning, receipt of legislation, journal articles to ensure NHS Tayside addresses new and emerging risk management issues.
• Agree tolerance levels for each risk identified within the Corporate Risk Profile and monitor progress of risk control.
• Monitor improvement over time in relation to the Corporate Risk Profile with a particular focus on identifying and exploring special and common cause variation and ensure that reports are provided to the Board and its Committees on relevant Corporate Risks.
• Provide assurance on the effectiveness and performance of risk management systems across organisation to the NHS Tayside Audit Committee including setting and monitoring of Risk Management KPIs.
• Set a framework for risk tolerance for all risks within the parameters set by the Board.
• Ensure that the NHS Tayside risk register is being adequately maintained and used as a driver for Risk Management through the appropriate allocation of resources and incorporation into strategic and operational plans as required.

25
• Seek out and implement best practice in risk management in healthcare and consider its application in NHS Tayside.
• Ensure that roles and responsibilities relating to risk management are specified to support their integration with all aspects of organisational management.
• Develop a scheme of delegation for corporate risks to be escalated to Tayside NHS Board as required.
• Act as the final point for escalation of risks and to identify and assign executive responsibility for any aspect of risk which is not being managed appropriately.
• Ensure risk management is embedded at all levels of NHS Tayside including its governance structures.
• Ensure that HAI is incorporated into the risk management framework.

26
Health and Safety
• Identify the key statutory requirements for health and safety and ensure they are understood across all services
• Develop a strategic health and safety framework that facilitates the planning of health and safety systems with the appropriate resources against an achievable time-frame
• Ensure that the roles and responsibilities relating to health and safety management are specified to support their integration with all aspects of organisational management
• Ensure the Service Partnership Agreement with OHSAS delivers compliant Occupational Health and Safety services to the workforce and demonstrates continuous improvement. Ensure that NHS Tayside addresses new and emerging work related health issues. Ensure an appropriate health and safety training and development plan which meets Statutory Health and Safety Regulations
• Develop new ways to establish and maintain an effective health and safety culture so that all staff take their responsibilities seriously, the workforce is fully involved and risks are properly managed.
• Ensure that HAI is incorporated into the Health and Safety framework
Resilience Planning
• Review and approve the Resilience Planning Policy every two years
• Ensure roles and responsibilities relating to Resilience Planning are specified to support their integration with all aspects of organisational management
• Ensure Resilience Planning is embedded at all levels of NHS Tayside including its governance structures
• Review and approve all NHS Tayside’s Emergency procedures
• Ensure that planning and executing of all components of NHS Tayside responses to major incidents, emergencies and outbreaks are carried out and lessons learned are embedded in future plans.
8. Authority
The SRMG is authorised by the NHS Tayside Executive Team to explore and implement any activity within its Terms of Reference. To complete this, the SRMG is authorised to seek any information it requires from any employee.
In order to fulfil its remit, the SRMG may obtain whatever professional, technical or other advice it requires, and may commission work to be delivered on its behalf. 9. Reporting Arrangements Minutes of the Strategic Risk Management Group will be forwarded to the following:
Management Governance NHS Tayside Executive Team Audit Committee Operational Risk/Health and Safety Management Committee
Audit Committee
Drugs and Therapeutics Committee Internal Audit

27
10. Reporting Schedule
Risk Management and Health and Safety
Presentation of Corporate Risk Profile to Tayside NHS Board
January and April
SRMG Committee Annual Report to Audit Committee
May / June
Mid Year SGR Progress Update Report to Audit Committee
November/December
Annual (Year End) Report to Audit Committee May
Resilience Planning
Presentation of Emergency Planning Annual Report to Tayside NHS Board
November
11. Reporting Arrangements

28
Risk Management and Health and Safety
TAYSIDE NHS BOARD
• Quarterly presentation of Corporate Risk Profile • Presentation of Corporate Risks relating to Emergency and Continuity
Planning and Pandemic Influenza by Risk Owner
Audit Committee
To review the systems and processes for Risk Management as part of the framework of Internal Control and Corporate Governance
• Biannual reports from Corporate Risk Owners with risks aligned to this committee • Annual Committee Report from SRMG • Minutes from Op RHSMG and SRMG • Mid Year and Annual SGR Report on effectiveness, adequacy and robustness of the risk management systems
Improvement and Quality Committee To review progress on all aspects of Clinical Governance and Patient Safety • Biannual report from Clinical
Governance • Biannual report from Risk
Owners with risks aligned to this committee
Finance and Resources Committee Responsible for reviewing Corporate Risks relating to the financial position on Tayside NHS Board • Biannual reports from
Corporate Risk Owners with risks aligned to this committee
• Annual Report from Safety, Governance and Risk in relation to Policy Management
Staff Governance Committee Responsible for reviewing Corporate Risks relating to staff and workforce issues. • Biannual reports from
Corporate Risk Owners with risks aligned to this committee
Clinical Quality Forum
Responsible for overseeing the safety, clinical governance and clinical risk management structures, ensuring adequate clinical governance support is provided and where appropriate establish review groups and monitor their achievement against their work programme. Objectives
• Annual Committee Report to Improvement and Quality Committee
• Minutes to Improvement and Quality Committee
Strategic Risk Management Group
Responsible for evaluating the systems and processes for risk management and monitoring the Corporate Risk Profile of NHS Tayside and ensuring it is aligned to the organisations Corporate Objectives
• Annual Committee Report from Op RHSMG • Quarterly review of Corporate Risk Profile inclusive of Tolerance
Levels • Annual Committee Report to Audit Committee • Minutes to Audit Committee, Drugs and Therapeutics Committee
and Internal Audit
Operational Risk/Health and Safety Management Group
Responsible for the Operational overview of risk/health and safety issues
• Bimonthly reports from SGR, Resilience Planning, Infection Control, Internal Audit, Complaints and Claims, Health and Safety including Fire Safety, Localities
• Minutes from AIM Group, Locality RHSM Groups and Radiation Protection Committee • Annual Committee Reports from Locality RMHS Groups and AIM Group • Annual Committee Report to Strategic Risk Management Group • Minutes to Audit Committee, Drugs and Therapeutics Committee, Secondary Care Quality and Clinical Governance Forum, Area Partnership Forum
Angus Locality RMG
• Annual Committee Report to Op RHSMG
• Minutes to Op RHSMG
P&K Locality RMG
• Annual Committee Report to Op RHSMG
• Minutes to Op RHSMG
Dundee Locality RMG
• Annual Committee Report to Op RHSMG
• Minutes to Op RHSMG
Key: Minutes to:
Reports to
29
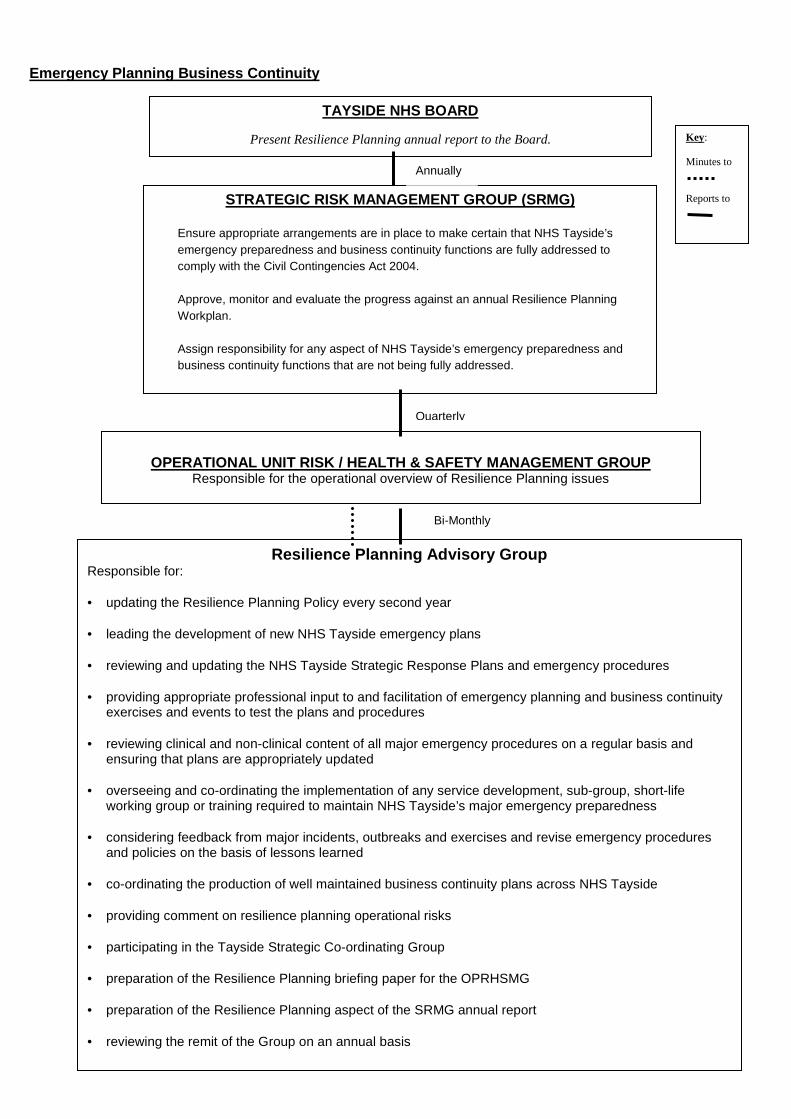
Emergency Planning Business Continuity
TAYSIDE NHS BOARD
Present Resilience Planning annual report to the Board.
STRATEGIC RISK MANAGEMENT GROUP (SRMG)
Ensure appropriate arrangements are in place to make certain that NHS Tayside’s emergency preparedness and business continuity functions are fully addressed to comply with the Civil Contingencies Act 2004. Approve, monitor and evaluate the progress against an annual Resilience Planning Workplan. Assign responsibility for any aspect of NHS Tayside’s emergency preparedness and business continuity functions that are not being fully addressed.
OPERATIONAL UNIT RISK / HEALTH & SAFETY MANAGEMENT GROUP
Responsible for the operational overview of Resilience Planning issues
Resilience Planning Advisory Group Responsible for: • updating the Resilience Planning Policy every second year • leading the development of new NHS Tayside emergency plans
• reviewing and updating the NHS Tayside Strategic Response Plans and emergency procedures • providing appropriate professional input to and facilitation of emergency planning and business continuity
exercises and events to test the plans and procedures • reviewing clinical and non-clinical content of all major emergency procedures on a regular basis and
ensuring that plans are appropriately updated • overseeing and co-ordinating the implementation of any service development, sub-group, short-life
working group or training required to maintain NHS Tayside’s major emergency preparedness • considering feedback from major incidents, outbreaks and exercises and revise emergency procedures
and policies on the basis of lessons learned • co-ordinating the production of well maintained business continuity plans across NHS Tayside • providing comment on resilience planning operational risks • participating in the Tayside Strategic Co-ordinating Group • preparation of the Resilience Planning briefing paper for the OPRHSMG • preparation of the Resilience Planning aspect of the SRMG annual report • reviewing the remit of the Group on an annual basis
Annually
Quarterly
Bi-Monthly
Key: Minutes to
Reports to