school of management. jurisdictional change and nursing’s professionalization: liberating nurses...
TRANSCRIPT

SEMINARSEMINAR
School of Management

Jurisdictional Change and Nursing’s Professionalization: Liberating Nurses or Losing the Plot?
Carole Doherty
Lecturer in Healthcare Management

Structure of Presentation
• Introduction – context of research, NHS Plan (DH, 2000)
• Theory – conceptual framework uses the sociology of professions and in particular Abbott’s (1988) work on jurisdictional change
• Methods – mixed methods, questionnaire data supported by in-depth interviews
• Findings – nurses’ roles have altered with nurses now performing tasks traditionally carried out by doctors. This has resulted in intra-occupational differentiation. Specialist nurses have experienced greater clinical autonomy but ward sisters have experienced greater subordination
• Conclusion – overall government intervention in the division of labour may have been detrimental to the quality of essential aspects of patient care such as assisting patients with feeding

Background
• NHS Modernization
◦ Break down the traditional, inflexible divides between occupational groups in the Service
◦ Challenge to the medical profession’s monopoly
◦ Opportunity for the professionalization of nursing

Research Questions
• Have changes to nursing’s jurisdiction aided its professionalization?
• What have been the intra-occupational consequences of jurisdictional change?
• Do nurses aspire towards the professionalization of their occupation?

Conceptual Framework
• Sociology of Professions
• The application of abstract knowledge to practice has both objective and subjective properties.
• Subjective properties are socially constructed, this creates dynamism in ‘the system of professions’ (Abbott, 1988)
• Jurisdiction – an area of practice over which an occupation has authority to act
• Three areas for competition:◦ The State including the legal system◦ Public opinion◦ The workplace

Jurisdictional Change
• Possible outcomes:
◦ Full jurisdiction◦ Subordination◦ Intellectual jurisdiction◦ Sharing of the jurisdiction◦ Advisory control◦ Client differentiation

Nursing’s History
• Modern form emerged in 1850s◦ Occupational strategy based on practical not theoretical
knowledge◦ Broad and uncertain jurisdiction
• Attempts to professionalize◦ 1900s, resulted in subordination◦ 1990s, resulted in weakened labour market position

Study Design and Methods
• Mixed methods◦ Quantitative data – patterns and trends in nurses’ job
attitudes, differences and similarities between the respective nursing jobs
◦ Qualitative data – underlying processes and organizational structures that might account for differences in job attitudes, the effect of changes to nursing’s jurisdiction, factors influencing nurses’ job aspirations
• Data analysis◦ Abbott’s (1988) categorizations of professional work,
descriptive statistics, t tests to compare differences in job attitudes, content analysis using matrix

Changes to JurisdictionKey Tasks Staff Nurse Ward Sister Specialist Nurse Total
N=115 N=64 N=62 N=241 % % % %
Routine tasksRequest x-rays 18 27 39 26Request blood tests 55 73 74 65Administer a range of medications using PGDs 66 73 68 69Admit patients with specific conditions within agreed Protocols 16 20 34 22Discharge patients, with specific conditions within agreed protocols 17 36 48 30Diagnosis and inference Make referrals for doppler/ultrasound to confirm DVT 3 2 6 4Make referrals for abdominal ultrasound 3 4 6 4Make referrals directly to consultant medical staff 15 33 77 36Inference and treatmentTrained as a supplementary prescriber 2 2 19 6Diagnosis, inference and treatmentInterpret x-rays and initiate treatment 1 2 18 5Interpret blood test results and initiate treatment 24 31 58 35Receive referrals directly from GPs10196827Receive referrals directly from hospital consultants or junior doctors acting on their behalf 25 33 81 41Prescribe medicines from the nurse prescribers' formulary 11 9 23 14 Initiate and administer thrombolysis under PGDs 4 3 2 3Make 'do not resuscitate' decisions 0 0 2 <1Take written consent from patients for procedures you perform 8 5 27 12Perform minor surgery 1 2 13 4Perform out patient procedures that require written consent 2 3 16 6Run a nurse led clinic 6 8 50 19
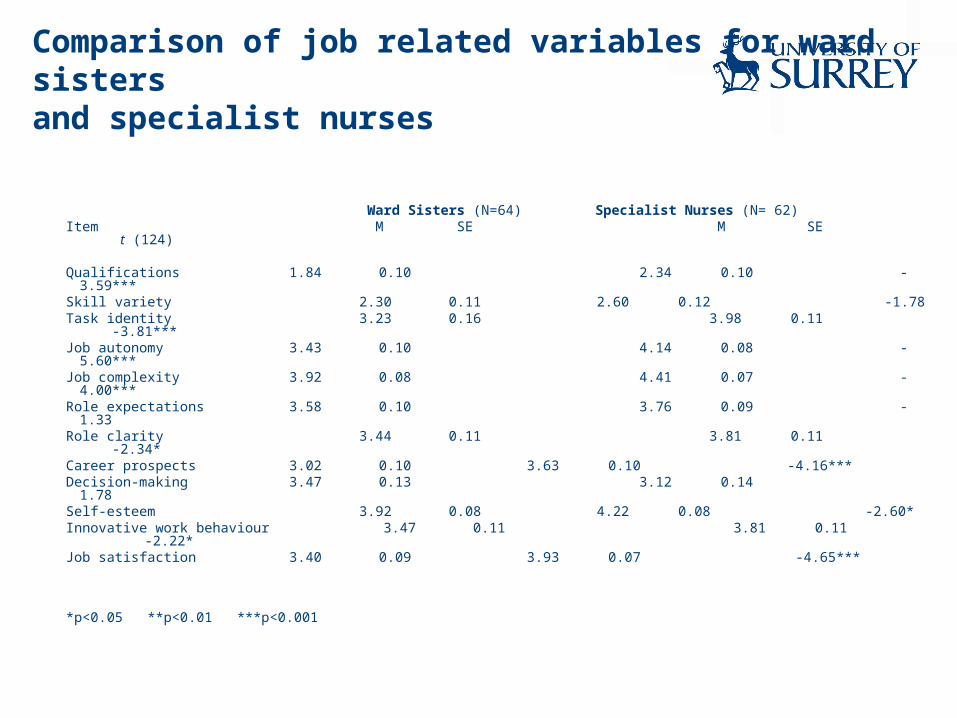
Comparison of job related variables for ward sisters and specialist nurses
Ward Sisters (N=64) Specialist Nurses (N= 62)Item M SE M SE t (124)
Qualifications 1.84 0.10 2.34 0.10 -3.59***Skill variety 2.30 0.11 2.60 0.12 -1.78Task identity 3.23 0.16 3.98 0.11 -3.81***Job autonomy 3.43 0.10 4.14 0.08 -5.60***Job complexity 3.92 0.08 4.41 0.07 -4.00***Role expectations 3.58 0.10 3.76 0.09 -1.33Role clarity 3.44 0.11 3.81 0.11 -2.34*Career prospects 3.02 0.10 3.63 0.10 -4.16***Decision-making 3.47 0.13 3.12 0.14 1.78
Self-esteem 3.92 0.08 4.22 0.08 -2.60*Innovative work behaviour 3.47 0.11 3.81 0.11 -2.22*Job satisfaction 3.40 0.09 3.93 0.07 -4.65***
*p<0.05 **p<0.01 ***p<0.001

Effects of Jurisdictional Change
• Doing doctors’ work and losing nursing
‘…that’s all they [nurses] do for the first two hours in the morning they do IV antibiotics then they’re doing another lot of taking bloods and I’ve very sadly looked at what’s going on in the rest of the ward in terms of patients are lying in wet beds, patients’ mouth care isn’t being done…..Bells are going everywhere patients are calling for the toilet and I just feel we have got to take a step back and look really at what nursing is about and go back to not basic nursing care but essential nursing care. I think we’ve really lost it. I really, really do I think we’ve lost the plot.”
Ward sister, 23 years experience
‘You can tend to neglect the patient because the fundamental parts of nursing seem to be missed a lot of the time now. ….the essence of nursing has been taken away from us because we’ve got to take bloods, do ECG’s, we put venflons in. They are all things that the doctors did at one time. Now we do it all.
Staff nurse, 7 years in nursing

Intellectual jurisdiction
‘For us here the patient is our sole responsibility it doesn’t go to anyone else. We see them we make a diagnosis and we decide upon a treatment that’s lovely. Because that’s your patient and you make all the decisions and you’ve administered it from a-z’
Ward sister – 26 years experience who also
practised as an emergency nurse practitioner
‘Its becoming more and more autonomous as things have gone on. It used to be very doctor orientated you used to do what the doctor said. How nursing has progressed…..it is definitely developing towards more specialist type areas so you become a practitioner in your own right alongside the doctor side of it.’
Staff nurse A&E

Sharing the jurisdiction
‘I see new patients in their [consultants’] clinics …new referrals from GPs... I can decide what I’m going to do for that patient without having to go and feedback to the consultant. I have that amount of autonomy with the role……. I work with the registrars in clinic so basically anything that the registrar sees I will see and go and feedback to the consultant in the same way’
Specialist nurse
‘Basically I work with the consultant surgeons assisting them with patients during their peri-operative period. It means that I can see them pre-op, take consent in out-patients and explain procedures to them, participate during surgery either as a first or second assistant or perform surgery depending on how big the surgery is. I do my operations independently under local anaesthetic.’
Specialist nurse

Professionalization?
• Job aspirations
◦ Twenty-seven percent of ward sisters wished to become specialist nurses
◦ Not one of the specialist nurses were inclined to become ward sisters
◦ Aspirations among the staff nurse group were equally split between specialist nurse and ward sister jobs
Professionalization?
• Ward sister◦ ‘So where will I be in 5 years time, I probably still will be in the NHS but
that’s probably because my bank manager needs me to be here rather than I want to be here because I don’t see nursing getting any better I just see it getting worse, it getting more and more stressful.’
• Specialist nurse◦ ‘There is no limit to what can be done in this post. I wouldn’t like to go
back to being a ward sister there is no challenge, after a time every day is similar…even now there are times that I look at something and think what do I do. Every day is different.’
• Staff nurse◦ ‘….you don’t deal with the patients as much and that’s not what I came
into nursing to do to be a nurse.’

Conclusions
• Government intervention in the division of labour can have significant intra-occupational consequences for a subordinate occupation and impact on aspects of the dominant occupation’s monopoly
• Complex and multifaceted outcomes of change to the division of labour within a single occupation - suggesting a need to move beyond single occupational categories in studies of occupations
• Greater subordination has given rise to concerns that the work traditionally performed by nurses may become lost, opening the potential for further weakening of nursing’s labour market position
• The structure of the ward sisters’ job appears to constrain their opportunities. This finding adds to discussion about the role of structure and government policy in understanding changes to the division of labour (Bach et al., 2007)

SEMINARSEMINAR
School of Management