school of mri 201 · pdf fileschool of mri 2016 advanced mr imaging of the musculoskeletal...
TRANSCRIPT

School of MRI 2016 Advanced MR Imaging of the Musculoskeletal System
November 10-12, 2016 Menton/FR
ESMRMB



AIMS
1. How I perform, read and report a hip exam
2. Labral anatomy and pathology
3. Femoroacetabular impingement (& extraarticular)
4. Bone marrow edema: The many facesESMRMB

Pulse sequences
T1-w TSE coronal
Turbo STIR coronal
PD/T2-w TSE/FS axial
PD-w TSE/FS sagittal
FS 3D-T1 GRE or FS PD-w, oblique axial
MR scanner 1.5-3T, Phased array coil
1. MR technique and reporting
ESMRMB

3T
Better SNR and contrast resolution at the same acquisition time
Less MR arthrograms
Courtesy: Eracleous, CY
ESMRMB

Reporting:
1. Overall appearance of hip joints. Congenital dysplasia?
2. Femoral head sphericity
3. Articular cartilage
4. Labra: compare with clinical symptoms and physical examination
5. Bone marrow: exclude AVN, TOH. Quick look at SI joints.
6. Soft tissues: tendons, bursae, muscles (piriformis - quadratus femoris)
X-rays: Coverage: CE angle
Acetabular version: “8” sign
ESMRMB

• 0.8ml Gd-DTPA in 100ml normal saline
• 12ml of this solution are mixed to 5ml of non-
ionic iodinated contrast and 2ml lidocaine 1%
• 8-15 ml of solution, fluoroscopy, 22G needle
• MR arthrography within 30min
MR arthrography
ESMRMB

T1-w TSE+FS
single side, small FOV/high resolution
axial, sagittal, coronal,
oblique axial
Single axial PD-w TSE/FS
both sides
MR arthrography
ESMRMB

3T
FS T1-w TSE
2.5mm
3D T1-w GRE
0.8mmESMRMB

Stoller et. al., Interactive hip
2. Acetabular labra
ESMRMB

Labral lesions classification
Czerny, Radiology 1996
Normal
ESSR 2014 / P-0049
FS T1 arthro
ESMRMB

Stage IAFS PD
FS T1 MRa ESMRMB

STIR: 110kg, female 65 y/o
Stage IB
FS PD
FS T1 MRa
ESMRMB

Stage IIA
FS T1 MRa
ESMRMB

Stage IIB FS T1 MRa
FS PD ESMRMB

Stage IIIA
Stage IIIB
ESMRMB

FAI
Trauma: acute, overuse
DDH
SFCE, LPC, OA, iliopsoas impingement
Labral pathology
Blenkenbaker DG, Tuite MJ. Magn Reson Imaging Clin N Am 2013
ESMRMB

Labral stress test
Tears:
92% anterior/anterosuperior
Dinauer PA, et al. AJR 2004
ESMRMB

Labral tear IIIAMRa
Labral tear IIAMRa
Windsurfing 20 y/o,m Mountain skiing 32 y/o, f
Plain MRI: sens 30%, acc 36%MR arthro: sens> 90%, acc> 91%, specificity ~100%
Czerny, Radiology 1996Freedman BA, et al. Artrhoscopy 2006
Toomayan GA, et al. AJR 2006
ESMRMB

49f, pilatesESMRMB

Deficient acetabular coverage of the FH
hip instability OA
Anterolateral migration of the FH chronic stresses
at the acetabular rim
Enlarged labrum initially maintains the FH within the joint
Chronic shear stress labral tear
Developmental Dysplasia of the Hip
ESMRMB

Center-edge angle:
Quantifies coverage of the femoral head by the acetabulum
Abnormal <25° adults,
<20° children and adolescents
DDH
ESMRMB

Normal DDH
29f
24f
Smaller weight bearing surface
Increased stress on cartilage and labrum
ESMRMB

CT/MRI measurements
Dysplastic AASA<50o m, PASA<90o
Normal
63o m, 64o f
105o
49f
42o
100o
105o
45o
ESMRMB

59f, pain right hip 7y
40o
20o ESMRMB

DDH OA
33 y/o, wrestling
55fpain and “clicking” sensation
ESMRMB

Tear: frequent frequent
Swelling: frequent no
Cysts: frequent rare
DDH FAI-trauma
ESMRMB

Overview Labra
Significant anatomic variation – age related changes
Tears cause hip mechanical pain MR arthro
Match the clinical info with lido-related pain reduction
Labral cysts: with/without tears, often related to DDH
ESMRMB

Crete
ESMRMB

3. Impingement meaning
A painful syndrome due to abnormal contact of two
distinct anatomic structures at motion
ESMRMB
Impingement syndromes
Intra-articular
• Femoroacetabular
• Cam type
• Pincer type
• DDH
Extra-articular
• Ischiofemoral
• Snapping internal type
• Iliopsoas imp. S.
• Snapping extenral type
• Iliotibial band imp. S.
• SubspineESMRMB

Femoro-acetabular Impingement
Abnormal contact femur-acetabulum
ESMRMB

• Predictor of early onset hip OA
• Wagner S, et al. Osteoarthritis Cartilage 2003
• Ganz R, et al. Clin Orthop 2003
• Beck M, et al. J Bone Joint Surg Br 2005
• Patterns of labral and chondral injury from FAI
appear to be unique to its distinct type
• Lavigne M, et al. Clin Orthop 2004
Established knowledge FAI
ESMRMB

CAM FAI“Pistol grip” deformity
Abnormal FH-neck offset associated with FAI
Premature OA
MR artrhography
AS acetabular cartilage degeneration-tear
AS labral tear
Abnomral alpha angle
ESMRMB

39 y/o f, pain bilateral
Natural history of CAM FAI
ESMRMB

56 y/o
Natural history of CAM FAI
ESMRMB

39 male
Tae Kwon Do
T1-w
PD FS
Early osteoarthritisESMRMB

24 male, football 34 male, jogging
ESMRMB

a
Normal a angle<55o
University of CreteNotzli HP et al. JBJS Br 2002
ESMRMB

How to use alpha angle?
• “Moderate evidence that a angle at baseline is
associated with progression of FAI to labral tear”
• “Ro measurements are best used in combination
with pt Hx and clinical findings to determine
prognosis and plan of care”
• Wright AA, et al. J Sci Med Sport 2014
ESMRMB

Important
Lifestyle !!!!
α angle 55o symptomatic
α angle 85o asymptomatic
ESMRMB

Pincer FAIovercoverage
• Acetabular retroversion
• Coxa profunda
• Protrusio acetabulumESMRMB

PINCER FAI: abnormal acetabulumovercoverage
Crossover or 8 signESMRMB

Coxa profunda
ESMRMB

Protrusio acetabuli:
Projection over the ilioischial line
>3 mm men, > 5 mm women
ESMRMB

Acetabular retroversion
L>5mm
Pfirrmann et al. Radiology 2006
ESMRMB

Herniation pit fibrocystic changes
• 33% Leunig et al, Radiology 05
• 24%, James et al, AJR 06
• 21%, Pfirrmann et al, Radiology 06
• 15%, Gerguis et al, Skeletal Radiol 05
• 5%, Kassarjian et al, Radiology 05
Leunig M, et al. Radiology 05
Pfirrmann CW, et al. Radiology 06
ESMRMB

Pincer FAI
Kassarjian, et al. Radiology 2005
R L
• Repetitive contact anterosuperiorly• Labral degeneration/tear• +/- intralabral cysts or ossification• Acetabular cartilage lesions superiorly, smaller than in CAM• Contre-coup chondral lesions
ESMRMB

To sum up
• FAI: cam -pincer: OA
• Labral and chondral degeneration and tear:
prompt diagnosis
MR arthrographyESMRMB

IFI syndrome
Taneja AK, et al. MRI Clin N Am 13
First described in 1977 (Johnson KA. JBJS Am)
Pain due to narrowing of the space between the l.
trochanter and ischial tuberosity
Entrapment of the quadratus femoris m.
Two types
Primary of congenital
Secondary or acquired
Tumors, hematoma,
apophysitis, myositis
ossificans
ESMRMB

IFI
IFS > 2 cmTorriani M et al. AJ R 2009
ESMRMB

IFIs ESMRMB

Track athlete, 14fPain 1yBilateral ischiofemoral impingement syndrome
Edema
Weekend athlete, 44f
ESMRMB

Elite athletes
Artistic Gymnastics
62.5%
Asymptomatic !!!!!
Papavasiliou A, Bintoudi A, Karantanas ASkeletal Radiol 2014
ESMRMB

Snapping hip syndrome
• External
• Iliotibial band
• Internal or anterior
• Iliopsoas tendon
48 m, long distance runner, pain right
16 m, elite sailor
ESMRMB

Subspine impingement
ESMRMB

4. What does BME represent?
• Oedema
• Haemorrhage
• Necrosis
• Inflammation
• Better to use the term
Bone marrow “edema-like”
ESMRMB

Bone marrow “oedema”: MRI findings
• Low SI on T1-w
• High SI on FS PD/T2-w, STIR
• Enhancement on fat suppressed T1-w
Impossible with
oedema alone
ESMRMB

Transient BME synd./TOH - RMO
Insuff. Fx
BME in AVN
BMEs hip
ESMRMB

TRANSIENT BONE MARROW OEDEMA SYNDROME
(TRANSIENT OSTEOPOROSIS OF THE HIP)
• Acute disabling hip pain - functional disability
• Curtiss-Kincaid, 3d trimester pregnancy (JBJS am 1959)
• TOH introduced by Lequesne (Ann Rheum Dis 1968)
• Wilson: “acute bone marrow edema”, pts (-) X-Rays
(Radiology 1988)
• Middle-aged men - pregnant women (M/F:3-4/1)
ESMRMB

Transient osteoporosis
X-Rays: (+) in 3-8 w from onset
Scintigraphy / MRI: early diagnosis
pain l. hip, 7w
ESMRMB

TRANSIENT BONE MARROW OEDEMA SYNDROME
(TRANSIENT OSTEOPOROSIS OF THE HIP)
• Clinical course: up to 4 to 9 m, rapid aggravation of pain and
functional restriction of the hip during the 1st month after onset
• All cases are self-limited, WB protection, pain killers
• Histology: BME, inflammation, bone desorption and
formation, No necrosis (Berger CE et al. Bone 03; Karantanas AH. Eur Radiol 2007)
ESMRMB
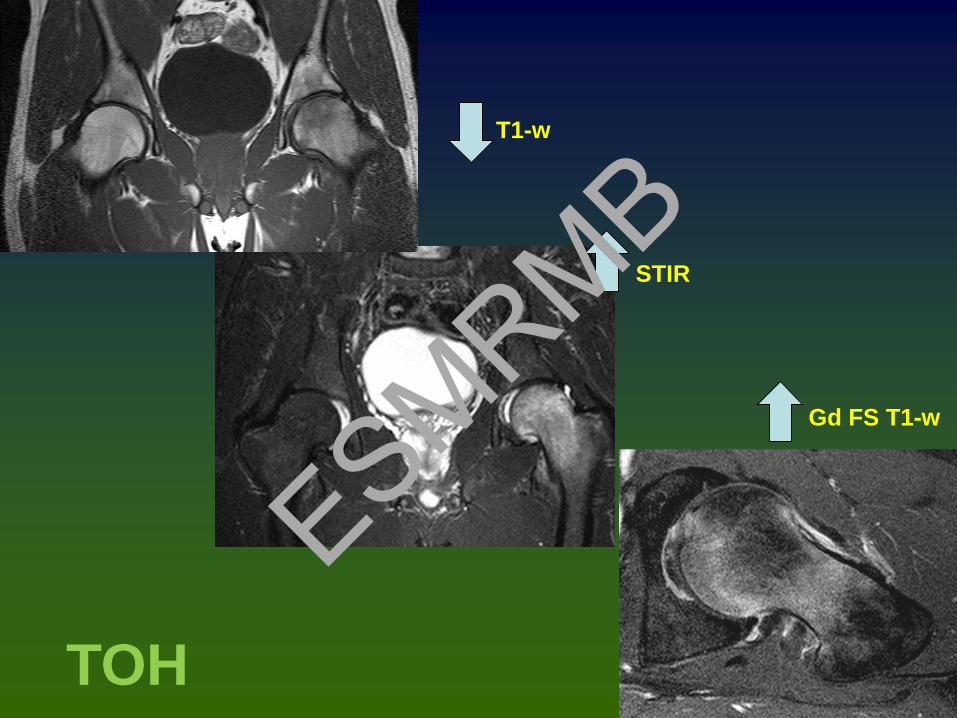
T1-w
STIR
Gd FS T1-w
TOH
ESMRMB

STIR
T1
T2-w FSPain bilateral 3d trimester, few days postpartum, 32 y/o
STIR
TOH
ESMRMB

TO hip, 55y male
Malizos KN, Karantanas AH. EJR 04 Peak enhancement > 40s
STIR
T1CE-FS T1
FS T2-w
ESMRMB

Fat-suppressed contrast-enhanced T1-w
“Oedema like” area enhances
Synovitis and joint fluid: constant findings
Transient osteoporosis
ESMRMB

Subchondral lesions
50%
Occult epiphyseal stress or
insufficiency fractures
University of Crete
Transient osteoporosis
ESMRMB

• Medial and anterior aspect
• “sparing” sign ~90%
Transient osteoporosis
STIR
CE FS T1-w
ESMRMB

• “sparing” sign
• 90% at diagnosis, disappears with disease progression
• 20% migratory pattern
Transient osteoporosis
ESMRMB

Regional migratory osteoporosis
?? Systemic osteopenia
20% of TOH casesESMRMB

Regional Migratory Osteoporosis
• First described by Duncan in 1969
• Arthralgia migrating in other joints or the same joint
• Weight bearing joints lower appendicular skeleton
• Clinical findings, x rays, MRI: similar to TOH
• Migration proximal to distal, intervals up to 9 months
• All cases transientESMRMB

April 06
June 06
Aug 07
Oct 07
35 male
?? Systemic osteopenia
21/22 males*
* Karantanas AH, et al.
Eur J Radiol 08
ESMRMB

Insufficiency fractures
Pain 2m leftFew m prior to current MRI, pain right
65f, DEXA+
ESMRMB

Insufficiency fractures
Pain 1m right
58f, DEXA+
ESMRMB

Insufficiency fractures64m, ca prostate,hormone therapy, RTH 5m ago, pain both hips
ESMRMB

TOH/aBMEs
RMO
Insuff. Fx
Osteopenia
Microtrabecular fractures
ESMRMB

Transient osteoporosis:
early reversible avascular
necrosis??
Definitely not!!!!
TOH is a distinct clinical entity
ESMRMB

Avascular necrosis
Young adults
Deterioration despite treatment
Femoral head common location
Subchondral fractures, progressive arthropathy
following collapse of the articular surface
ESMRMB

“Band like” sign
ESMRMB

“Band like” sign
ESMRMB

Pain and AVN
Marrow oedema
Collapse
Joint effusion
Never before “bands”, result of collapse
T1-w
Symptomatic
Karantanas AH.
Expert Opin Med Diagn. 2013
ESMRMB

50 y/o, f, bilateral AVN, pain right side
3y later
THA
“Crescent” sign
ESMRMB

Asymptomatic right
Symptomatic left
FS CE T1-w
ESMRMB

We discussed
• 1. How to perform and report a hip MRI exam
• 2. The labral anatomy and pathology
• 3. The FAI and other impingement syndromes
• 4. The many faces of HIP BME syndromesESMRMB

Thank you
ESMRMB