sci ence. ti me f or john s u t o go
TRANSCRIPT
Time for John Su to goBy Steve Kirsch
Dr. John Su is the top VAERS expert at the CDC.
Su claims that VAERS is only slightly underreported this year. That’s impossible. That’s not what thedata says at all. His erroneous claim has profound implications on safety that jeopardizes millionsof lives worldwide as I’ll explain below.
I have repeatedly attempted to alert Dr. Su about his mistake. He has ignored me.
At this point, it’s crystal clear that he’s either incompetent or corrupt, or both. I don’t know which oneit is, but either way, he needs to resign. If he doesn’t resign, he should be fired.
Anyone can calculate the VAERS URF. It isn’t rocketscience.
ANYONE can calculate the VAERS underreporting factor (URF) using a method that is well known toDr. Su since it was described in a paper that he wrote.
My calculation is explained in detail here. I got 41. I did everything by the book. I used the CDCmethodology, I used the VAERS data from HHS, and I used the anaphylaxis data from the Blumenthalstudy published in JAMA, one of the world’s top medical journals. I further confirmed the Blumenthalnumbers using the Hashimoto study which was published in another peer-reviewed journal. Youreally can’t get any better than that.
I also confirmed my URF estimate using the serious adverse event rate from the “gold standard”Pfizer clinical trial which the FDA has certified is correct since they granted full approval of the drug(see Critical Appraisal of VAERS Pharmacovigilance: Is the U.S. Vaccine Adverse EventsReporting System (VAERS) a Functioning Pharmacovigilance System? by Jessica Rose). Notethat Rose calculated a URF of 31 which is less than mine because drug manufacturers significantlygame both the adverse event reporting systems (making it difficult to report adverse events) and thecomposition of the cohort (chosen to be much healthier than “normal”).
In short, the value of 41 that I calculated is more than reasonable.
The problem is Dr. Su thinks the URF is completely different. He thinks it is close to 1. But he’sactually never bothered to calculate the correct value. There is no document that exists showing thecalculation. This is why the CDC and FDA have consistently refused to provide it. Because it does notexist.
Page 1

Watch this video from August 30, 2021 (which starts at 16:11) and stop at 17:56. Dr. Brooks asks,“What is the potential for underreporting …for example can we extrapolate out if there is in fact moreMyocarditis out there that is just not coming to VAERs?” Dr. John R. Su responded, “Previousreports have demonstrated that VAERs does capture a substantial proportion of adverse events outthere…. with respect to Myocarditis… it’s my recollection that reporting rates are roughly comparableto what has been seen in other surveillance systems like the Vaccine Safety Datalink (VSD)…. I doanticipate some underreporting … that being said for Myocarditis they do capture a good proportionof what’s out there…. In terms of what we are capturing we are getting a good number.”
In other words, he basically has admitted he never really calculated the number because if he did,he would have mentioned it.
VSD is even more underreported than VAERSDr. Su admitted VAERS reporting rates are comparable to VSD. In fact, in many cases, VSD is evenmore underreported than VAERS (as we will show next). Thus, it is completely nonsensical to useVSD to determine the VAERS URF. Yet this is what five CDC authors do in this paper!
For example, for myocarditis, you can see this very clearly on slide 13 in Grace Lee’s ACIPpresentation where VAERS is actually reporting slightly more events per million than VSD! That’ssimply impossible if VSD is a fully reported system or even close to a fully reported system.
The same underreporting is true for anaphylaxis reports: both VSD and VAERS have similar rates(VSD data showed 5 cases per million doses as you can see here Aug 30, 2021 ACIP Meeting -Safety update for COVID-19 vaccines, whereas VAERS showed 5.97 per million doses). So onceagain, VAERS, an underreported system, is reporting events at a higher rate than VSD.
Using VSD to establish a URF for VAERS is thus idiotic. You are benchmarking two underreportedsystems against each other. The CDC did this in their paper because they are inept.
To benchmark VAERS against VSD is to cause a further downward bias in the counts.
It is unacceptable that the lead researcher on evaluating the VSD or VAERS safety signals for theCDC thinks VAERs has "captured a good proportion of what's out there.” That is simply not reality.
VAERS is typically underreported by a factor of 10 to100
Dr. Su should know that VAERS is normally underreported by a factor between 9.5 and 95 with 95%confidence as noted in Advanced Clinical Decision Support for Vaccine Adverse Event Detection
Page 2
and Reporting). So thinking the URF is close to 1 is ridiculous. There is no evidence that this is thecase. There is only hand waving and wishful thinking that justifies this value, not data (unless youhold the ridiculous belief that VSD is fully reported).
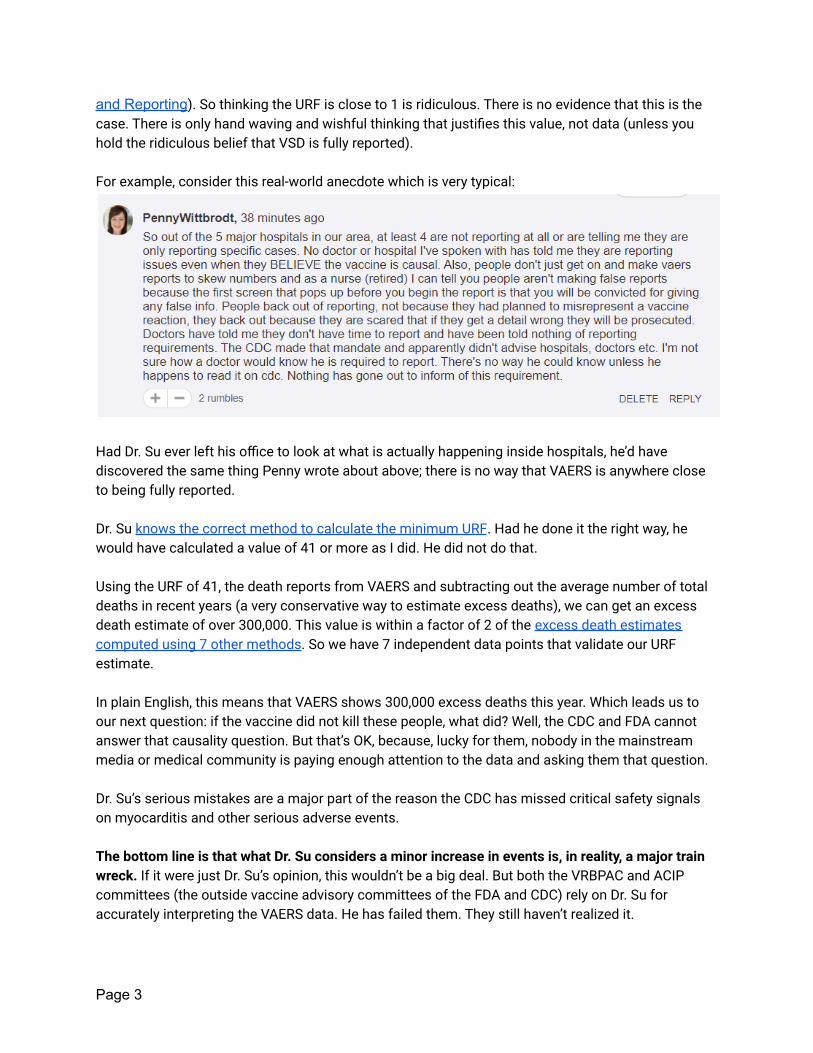
For example, consider this real-world anecdote which is very typical:
Had Dr. Su ever left his office to look at what is actually happening inside hospitals, he’d havediscovered the same thing Penny wrote about above; there is no way that VAERS is anywhere closeto being fully reported.
Dr. Su knows the correct method to calculate the minimum URF. Had he done it the right way, hewould have calculated a value of 41 or more as I did. He did not do that.
Using the URF of 41, the death reports from VAERS and subtracting out the average number of totaldeaths in recent years (a very conservative way to estimate excess deaths), we can get an excessdeath estimate of over 300,000. This value is within a factor of 2 of the excess death estimatescomputed using 7 other methods. So we have 7 independent data points that validate our URFestimate.
In plain English, this means that VAERS shows 300,000 excess deaths this year. Which leads us toour next question: if the vaccine did not kill these people, what did? Well, the CDC and FDA cannotanswer that causality question. But that’s OK, because, lucky for them, nobody in the mainstreammedia or medical community is paying enough attention to the data and asking them that question.
Dr. Su’s serious mistakes are a major part of the reason the CDC has missed critical safety signalson myocarditis and other serious adverse events.
The bottom line is that what Dr. Su considers a minor increase in events is, in reality, a major trainwreck. If it were just Dr. Su’s opinion, this wouldn’t be a big deal. But both the VRBPAC and ACIPcommittees (the outside vaccine advisory committees of the FDA and CDC) rely on Dr. Su foraccurately interpreting the VAERS data. He has failed them. They still haven’t realized it.
Page 3

CDC cannot identify a safety signal to save their lifeThe fact that the CDC is still clueless about serious and obvious adverse events such as death andpulmonary embolism can also be credited to Dr. Su. He’s supposed to recognize safety signals.
For example, watch these 2 videos on Rumble:1. TFNT11: The FDA's BIG mistake2. TFNT10: Myocarditis deception
You don’t have to believe those videos. You can check it out for yourself since all of the data is inplain sight.
For example, here are the VAERS results for pulmonary embolism, a very serious life-threateningcondition that is clearly caused by the COVID vaccines:
Page 4

Now, let’s do the same query but for all vaccines over a 5 year period prior to COVID. We get:
There are 2,629 cases reported for the COVID vaccines, compared to an average of 2.8 cases peryear in a “normal” year (14/5=2.8).
That’s an elevated reporting rate of 938! How can they miss a serious adverse event like this? Moreimportantly, If it wasn’t the vaccine that caused this elevation, then what did?
The CDC and FDA refuse to tell us. Crickets.
I will bet anyone in the world $10M that both death and pulmonary embolism is elevated by thesevaccines and caused by these vaccines. Will anyone take my bet? Of course not because nobodyreally believes the CDC is telling the truth. Everyone believes they are incompetent to find safetysignals that are in plain sight. That’s why nobody in the world will take my bet. Nobody.
Page 5
This leads us all to the inevitable conclusion that all of the safety monitoring people at the FDA andCDC are either completely incompetent or corrupt or both. Clearly they can’t find a safety signal tosave their lives. And as far as I can tell, they absolutely refuse to listen to any outside input tellingthem of the problem.
The bottom line is that the US needs competent individuals to monitor vaccine safety. Dr. Steven A.Anderson at the FDA and Dr. John Su at the CDC are simply not up to the task. They have found nosafety signals at all. The only signal they did find, the myocarditis signal, came from Israel. They hadto acknowledge it when they couldn’t bury the story.
With no safety signals to investigate, John and Steven should be lonelier than the Maytag repairman.They should welcome a call reporting a safety signal. Instead, they ignore any such calls and emailsas too bothersome to respond to. If Congress requests their email records, they will see this firsthand. Of course, that will never happen since there isn’t any accountability. So these people fearnothing.
How to screen people who can spot safety signalsI think I can help the CDC and FDA hire the talent they need.
Working with experts, we have designed a highly sophisticated 3 question test that can quicklyidentify highly skilled individuals who are capable of spotting vaccine safety signals.
QUESTION 1In which year is myocarditis elevated (assume the number of people vaccinated in all years isroughly the same and the age distributions are comparable)?
Page 6

QUESTION 2In which year are deaths elevated? (same assumptions as above)
QUESTION 3Do all of these bars appear to be the same height?
Page 7

Any candidate who is able to correctly answer all three questions would be a substantial upgradefrom the staff today.
How can the CDC and FDA not know the URF?All of my emails to both the FDA and CDC asking them for the URF this year have been met withsilence.
That’s standard operating procedure for these agencies when you bring up uncomfortable questions.For example, the CDC did the same thing to ICAN attorney Aaron Siri when he asked them the samequestions I asked them (see page 1 which incorporates the CDC response to the original letteron pages 2 and 3). Siri asked his questions right after the Blumenthal paper on anaphylaxis waspublished in JAMA on March 8, 2021. He’s absolutely brilliant. As soon as that paper was publishedhe was right on the case with his letter. They ignored him.
Here’s the question you have to ask: if a brilliant attorney (Aaron Siri) can calculate the correct URFand a Silicon valley tech entrepreneur (me) can calculate the correct URF, then how is it that nobodyat the FDA and CDC can calculate the URF?
They won’t tell me. And the NY Times and the Wall St. Journal will never ask that question.Investigative journalism that goes against the current false narrative is non-existent. It’s sad.
There is no debate: John Su has failed his primaryjob function and nobody will defend himI did a survey to see if other people agreed with the arguments presented in this op-ed.
Page 8

Clearly, this is not a close call. Rarely do I see surveys that are this lopsided...475 to 0.
Dr. Su is clearly unwilling (and I would argue also unable) to defend himself. Is there a single personat the CDC or FDA who will rise in defense of Dr. Su and agree to discuss this in a public recordedforum?
Please respond in the comments below if you work at the CDC or FDA and will publicly defend John’swork in an open debate since he will not.
You cannot do a proper risk-benefit analysis onserious adverse events without knowing the URFJohn Su must know that the correct URF is required to calculate a proper risk-benefit analysis. Itwas his job to compute this. He’s failed the CDC and he’s failed the American people. Hisincompetence has led to the death or disability of well over 500,000 Americans who should havebeen warned about the serious adverse events caused by these vaccines, such as death.
And even if I’m totally wrong about the URF and John is right, it’s still a disaster because virtually allthe 7,848 deaths can be easily shown to be causal using the Bradford-Hill criteria for causality. Johnnever mentions that. That easily exceeds the COVID vaccine stopping condition of 9 myocarditiscases that was originally set by the CDC. He should have been yelling at the top of his lungs, “STOPTHE VACCINE; IT IS KILLING TOO MANY PEOPLE.” Had Dr. Su done his job, these safety signalswould have been spotted in January 2021 and the vaccines stopped.
Page 9

Myocarditis implicationsThe implications of a URF of 41 for VAERS is extraordinary.
Let’s take myocarditis, for example. From Slides 4, 5, and 8 of the myocarditis presentation atthe October 26 VRBPAC meeting, we learn two important things:
1. There is at least a 75-fold increase in the rate of myocarditis for fully vaccinated 16 yearold boys over the baseline rate expected
2. Myocarditis is clearly caused by the vaccines. It is dose dependent and there are nocases in the comparison interval (per slide 8)
The FDA and CDC and their outside committees have considered a 75X increase in heartdamage for kids to be an acceptable risk. They accept 75 myocarditis cases per million boysfully vaccinated is “ok” which is 1 in every 13,000 teenage boys being vaccinated. That’s wellnorth of the original 9 myocarditis cases stopping condition. But everyone forgot about that.
But that’s not the actual rate because VAERS is at least 41 times underreported for myocarditis.For the purposes of this section, we’ll just be very conservative and assume that the URF for allevents is only 41.
So now we have 1 in every 325 teenage boys who will develop myocarditis. This of courseis a train wreck no matter how you look at it. But since Dr. Su never tells anyone about the rightURF value, nobody knows and everyone thinks it’s pretty rare. Problem solved!
Unfortunately, just because we don’t know the risk, doesn’t mean the problem goes away.
The elephant in the room boils down to two questions:1. Will 20% of these kids who are injured today from myocarditis die in 1 year from now as
is typical?2. Will 50% of those kids die in 5 years from now as is typical?
FDA panel member Dr. Eric Rubin (who happens also to be Editor-In-Chief of the New EnglandJournal of Medicine, arguably the top medical journal in the world) addressed this question atthe last FDA meeting. Here’s what he said:
Page 10

Dr. Rubin basically said we don’t have a clue but we’ll find out over the next 5 years sincewe are experimenting on your kids. Not just a subset of kids... pretty much all your kids.President Biden’s goal is to run the experiment on 100% of your kids; the under 5 yearsold category is next.
I give Dr. Rubin credit for his complete honesty. It’s something we so rarely see in the medicalprofession.
The myocarditis rates for 5 to 11 year olds will likely be less than 1 in 325 kids because the ratesseem to have a relative peak at 16 year olds. But still, that’s an unacceptable risk. Even if weare only permanently damaging the hearts of 1 in 1,000 kids, how can you justify doing that for28 million kids in order to maybe save around 14 lives from COVID. That’s nonsensical. We’d bedamaging 28,000 kids to save maybe 14 lives (since about half the 1 in 1 million kids who areestimated to die are estimated to be immune to COVID). Even the kids themselves can figureout that’s a bad deal (which is why we don’t tell them).
But myocarditis isn’t the only symptom. It’s not even the most dangerous symptom. What aboutdeath, for example?
Page 11
For kids in the 5 to 11 age group, the VAERS data shows (extrapolating) that we’ll killsomewhere around 22 kids per million doses. So for 28 million kids in that range, the vaccine isexpected to kill about 616 kids in order to save 14 kids from dying from COVID. So we will killaround 44 kids for every kid that we save from COVID.
In most societies, this would be unthinkable. It would be unethical and immoral. But not intoday’s society. Because today we have been brainwashed into believing the vaccines areperfectly safe, despite irrefutable evidence that that is untrue.
We are told to focus only on the COVID lives saved and ignore any deaths due to the vaccine,no matter how strong the evidence for that.
People like me who tell people to look at the data are labelled as spreaders of misinformation.
This is a successful strategy: it has led companies, hospitals, cities, and school boards tomandate vaccination without allowing any scientific debate on the matter whatsoever! Fullcensorship is applied to anyone with a view that is not aligned with the mainstream “safe andeffective” narrative. And the more you know, the more they censor you. This is why people likeRobert Malone, Peter McCullough, Byram Bridle, Bret Weinstein, Robert F. Kennedy, Jr., JosephMercola, and others will never appear on mainstream media.
This is why nobody from the CDC or FDA or any mainstream medical institution will debate theteam of scientists and statisticians that I work with on a regular basis. The evidence just isn’t ontheir side. So they refuse. Every time. They will never do what the public overwhelmingly wants:an open discussion. I even offered an unrestricted research grant to get people to debate. Theycould name their price. Nobody was interested.
TrialSiteNews even offered to host a debate. Nobody from the pro-vaccine side would consentto do it. Nobody from the drug companies either. Wow. Just wow. Not even the drugcompanies were willing to defend their own product. No wonder they need liabilityprotection.
Why is nobody in the medical community calling forDr. Su to resign?The case against Dr. Su is blatantly obvious to anyone who looks at the evidence.
I had expected that someone in the medical community, in Congress, in the FDA, CDC, or NIH,or in the mainstream media would call Dr. Su out for misrepresenting the URF, but nobody has.Nobody. It’s unbelievable.
In other words, what nearly the entire medical community is saying to the world is effectively,“Look, we don’t care if the people at the CDC whose work we rely on are incompetent. We
Page 12

completely trust them. If the CDC says the vaccines haven’t killed anyone and that myocarditisis the only adverse event, we believe them. There is no need for us to double check their work.The CDC calls the shots. Whatever they say, goes. When they say masks don’t work, theydon’t. When they change their mind and say they do, they do. We do not want to lose our NIHfunding or have our license to practice medicine revoked; that’s what’s important to us. Thequality of the science? Not so much.”
None of the ACIP or VRBPAC committee members noticed that they never calculated the URF.Nobody asked to see the calculation. This is pretty stunning.
The committees are pretty much asleep at the wheel anyway so I’m not surprised. They neverdemanded a rigorous risk benefit analysis for justifying the 5 to 11 EUA. Toby Rogers, an expertin vaccine risk benefit analyses, said, “The FDA’s risk-benefit analysis in connection with Pfizer’sEmergency Use Authorization (EUA) application to inject children ages 5 to 11 with theirCOVID-19 vaccine is one of the shoddiest documents I’ve ever seen.” Wow. That’s quite anaccomplishment. Toby has seen a lot of documents.
No one else has stepped up to the plate to do what is right. Not even Senator Rand Paul.
Thus, the burden now falls upon the retired high technology executives in Silicon Valley to pointout the obvious mistake. People like me.
The public deserves transparency in regulatory governance, science and evidence-based publichealth policy and medicine, and therefore, I will continue to publish articles that are unbridled intheir critical evaluation of the specific individuals involved in decision-making that affect us all.
John Su must go. He has no excuses. He won’teven defend himself.I asked Dr. Su by both email and voicemail to respond to this op-ed before I published it. He ignoredall my requests. Tom Shimabukuro was provided a copy as well. No response from him either.
If Dr. Su doesn’t resign, he should be fired and either replaced with someone who knows how tocorrectly interpret the VAERS data, or the interpretation of such data taken out of the hands ofanyone associated with HHS.
Dr. Su, it is time for you to go.
Page 13