scienza alimentazione e nutrizione umana gastroenterologia · 5. hepatic encephalopathy, 6....
TRANSCRIPT
Scienza Alimentazione e Nutrizione Umana
GastroenterologiaProf. Stefano Fiorucci
Liver Cirrhosis and its
complications
1
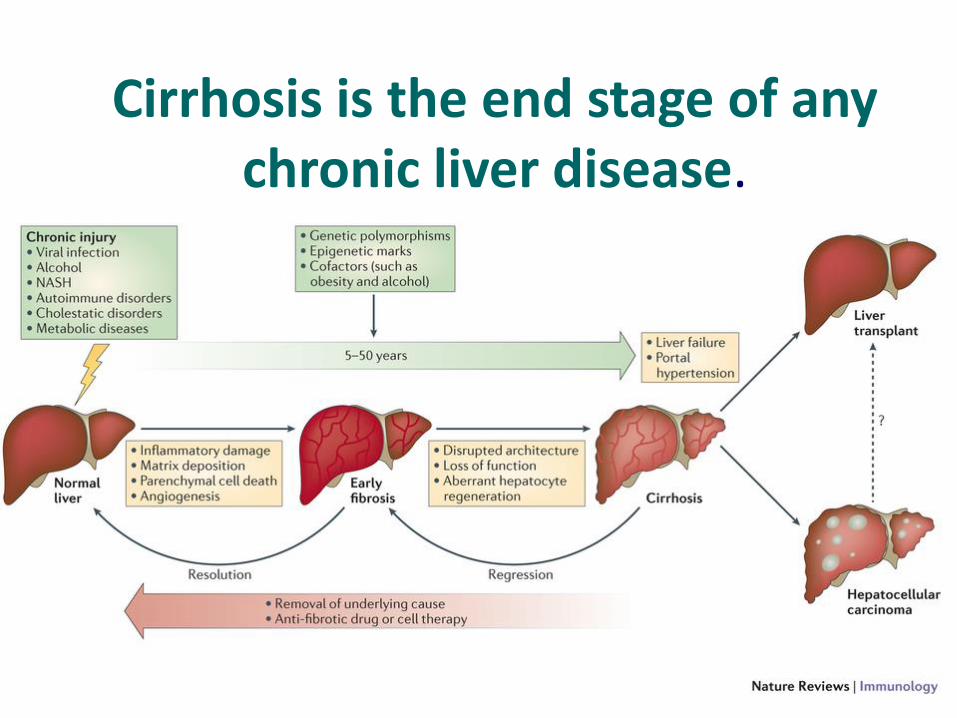
Cirrhosis is the end stage of any chronic liver disease.
2
Liver cirrhosis: epidemiology
• Approximately 29 million people in the European Union suffer from a chronic liver condition
• Liver cirrhosis is responsible for an estimated 170,000 death per year in Europe
• Liver cancer is responsible for around 47,000 deaths per year in the EU
• Hepatocellular carcinoma (constituting 70-90% of cases of primary liver cancer) is the fifth most common cause of cancer in Europe
• Prevalence might be 0.3% in Italy (over 150.000)
3
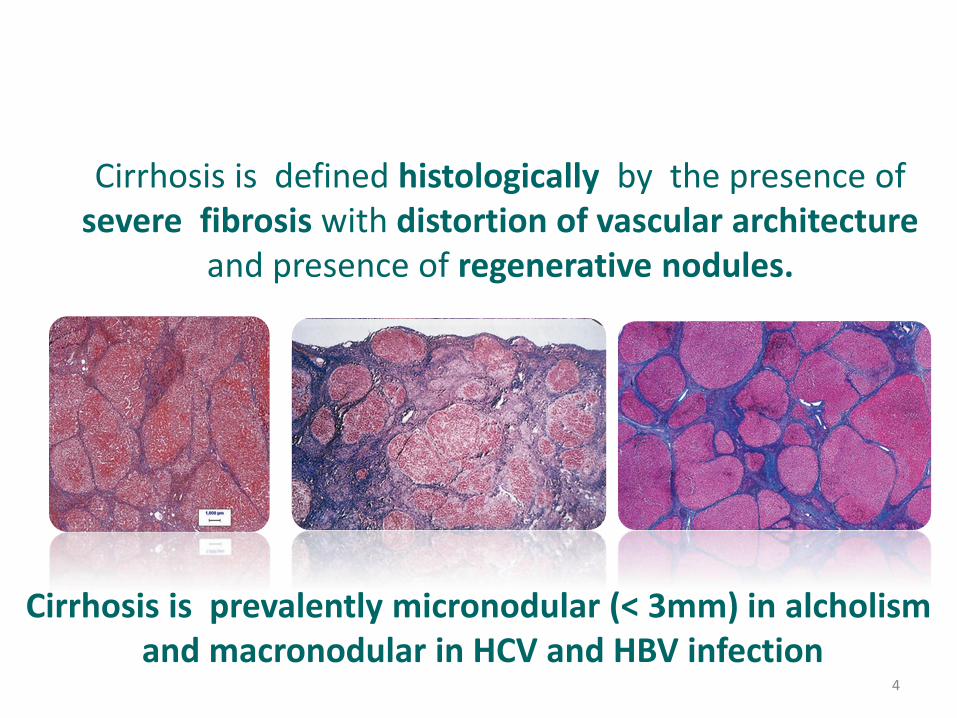
Cirrhosis is defined histologically by the presence of severe fibrosis with distortion of vascular architecture
and presence of regenerative nodules.
Cirrhosis is prevalently micronodular (< 3mm) in alcholismand macronodular in HCV and HBV infection
4
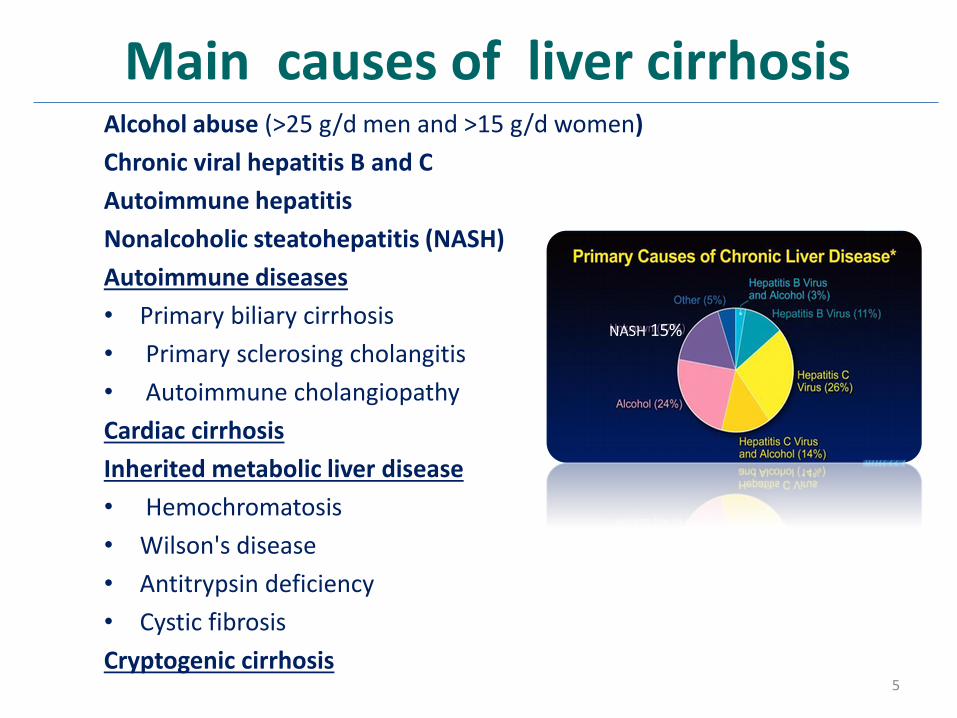
Main causes of liver cirrhosisAlcohol abuse (>25 g/d men and >15 g/d women)
Chronic viral hepatitis B and C
Autoimmune hepatitis
Nonalcoholic steatohepatitis (NASH)
Autoimmune diseases
• Primary biliary cirrhosis
• Primary sclerosing cholangitis
• Autoimmune cholangiopathy
Cardiac cirrhosis
Inherited metabolic liver disease
• Hemochromatosis
• Wilson's disease
• Antitrypsin deficiency
• Cystic fibrosis
Cryptogenic cirrhosis
NASH 15%
5
Liver cirrhosis: general
• The main pathologic features consist of the development of fibrosis to the point that there is architectural distortion with the formation of regenerative nodules.
• This results in a decrease in hepatocellular mass, and thus function, and an alteration of blood flow. The induction of fibrosis occurs with activation of hepatic stellate cells, resulting in the formation of increased amounts of collagen and other components of the extracellular matrix.
6
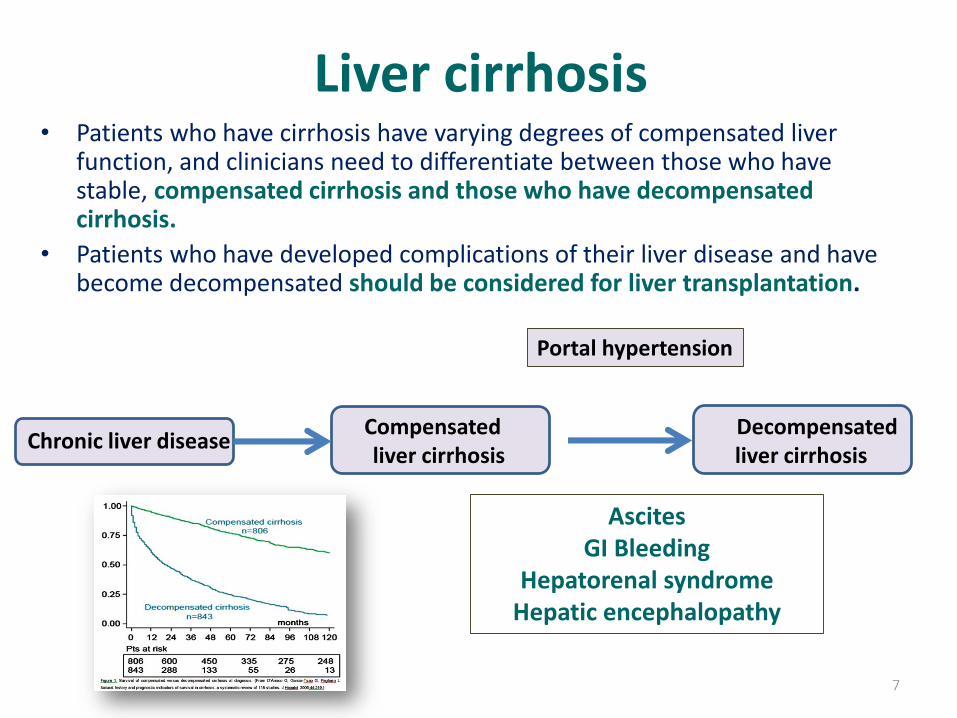
Liver cirrhosis• Patients who have cirrhosis have varying degrees of compensated liver
function, and clinicians need to differentiate between those who have stable, compensated cirrhosis and those who have decompensated cirrhosis.
• Patients who have developed complications of their liver disease and have become decompensated should be considered for liver transplantation.
Compensated Decompensatedliver cirrhosis liver cirrhosis
Portal hypertension
7
AscitesGI Bleeding
Hepatorenal syndromeHepatic encephalopathy
Chronic liver disease
Liver cirrhosisThe clinical course of patients with advanced cirrhosis isoften complicated by a number of important sequelaethat can occur regardless of the underlying cause of the
liver disease.
These include:
1. Portal hypertension and gastroesophageal variceal hemorrhage,
2. Splenomegaly,
3. Ascites and spontaneous bacterial peritonitis
4. Hepatorenal syndrome,
5. Hepatic encephalopathy,
6. Hepatocellular carcinoma
8
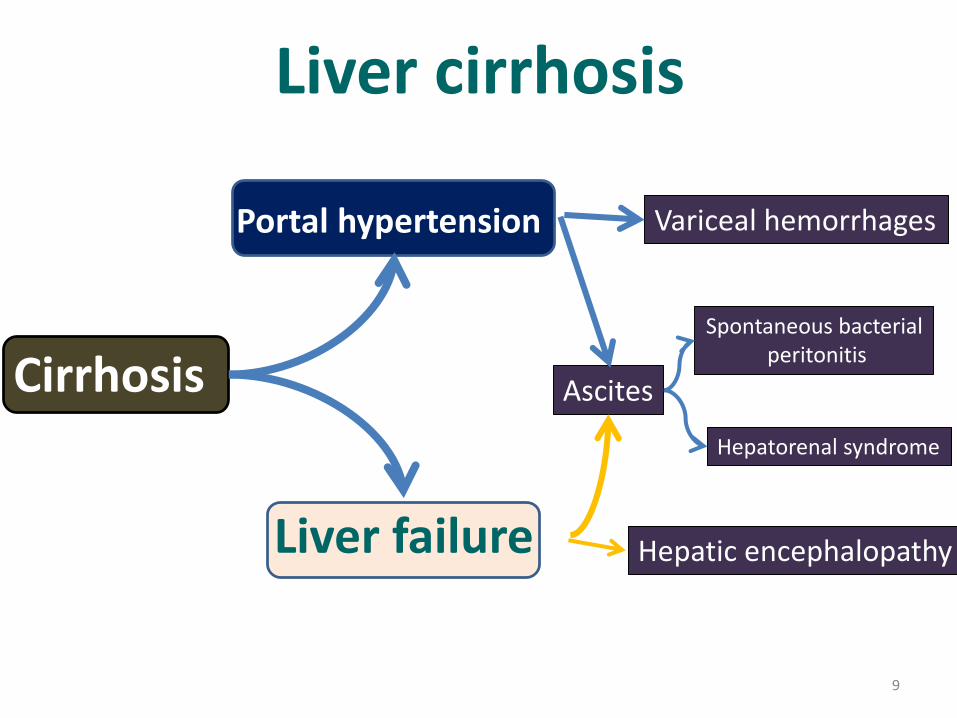
Liver cirrhosis
Cirrhosis
Portal hypertension
Liver failure
Variceal hemorrhages
Ascites
Hepatic encephalopathy
Spontaneous bacterialperitonitis
Hepatorenal syndrome
9
Cirrhosis diagnosis
• Liver biochemistry• Liver biopsy• Staging of fibrosis (transient elastography)• Endoscopy (esophageal varices)• Imaging studies- Sonography- CT - MR
Aim of the diagnosis: to define the cause, to stage the severity of liver diseaseto detect the presence of complications (compensated vs decompensated)
10
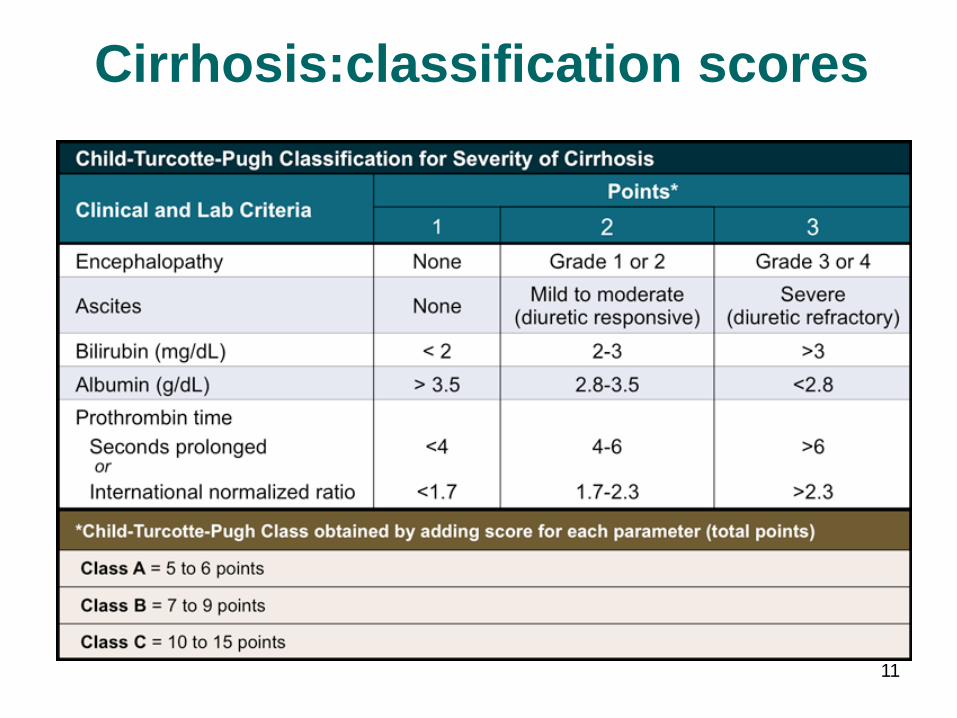
Cirrhosis:classification scores
11
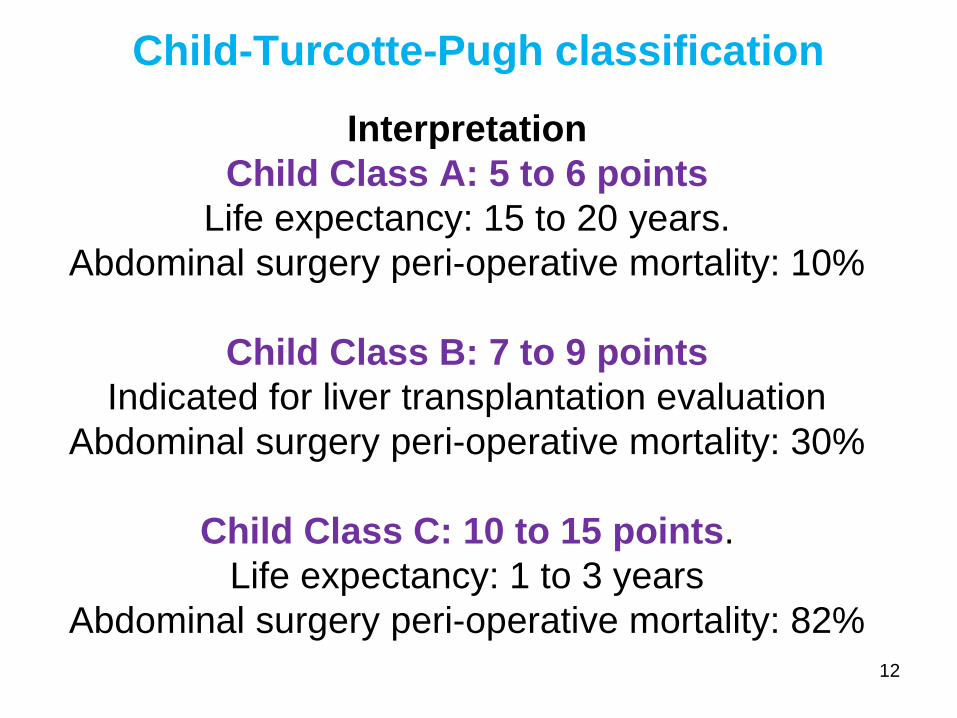
Interpretation
Child Class A: 5 to 6 points
Life expectancy: 15 to 20 years.
Abdominal surgery peri-operative mortality: 10%
Child Class B: 7 to 9 points
Indicated for liver transplantation evaluation
Abdominal surgery peri-operative mortality: 30%
Child Class C: 10 to 15 points.
Life expectancy: 1 to 3 years
Abdominal surgery peri-operative mortality: 82%
Child-Turcotte-Pugh classification
12
Metabolic changes in
complicated cirrhosis
13
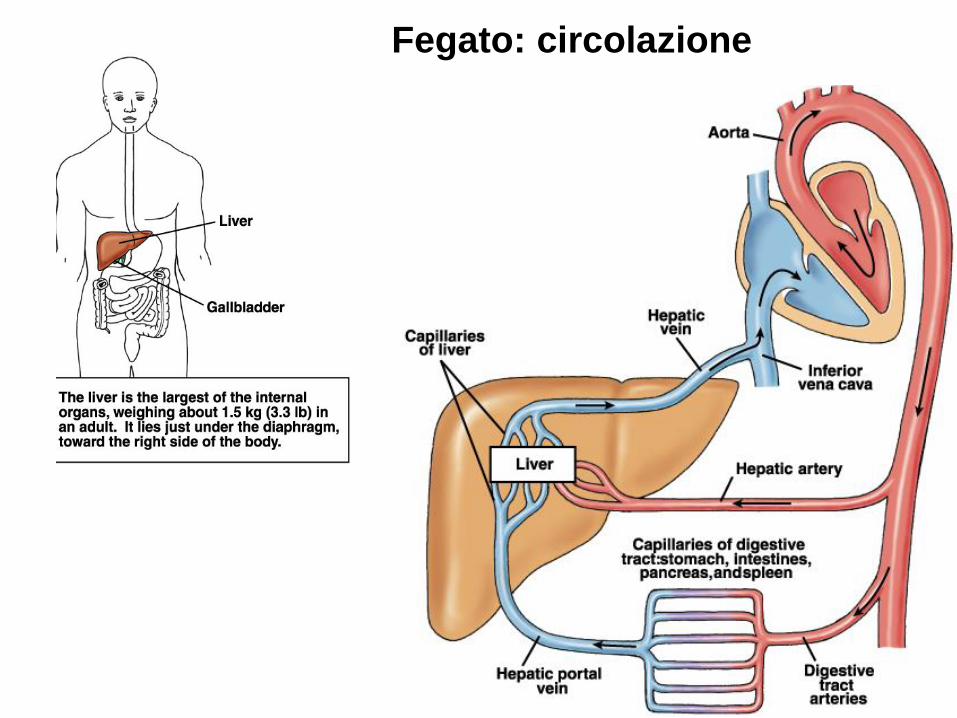
Fegato: circolazione
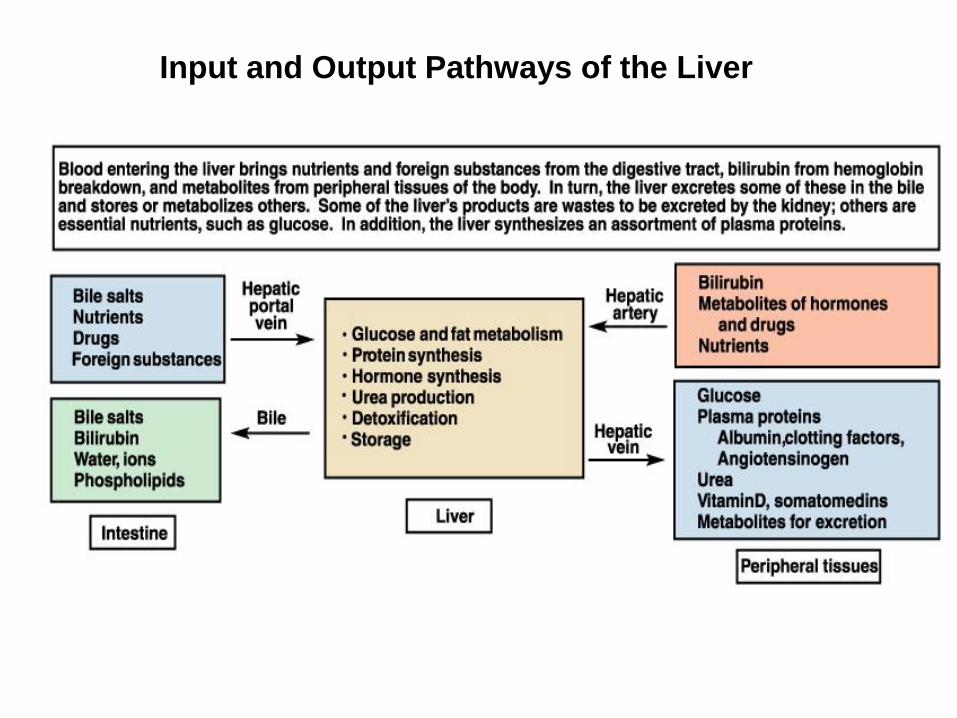
Input and Output Pathways of the Liver
16
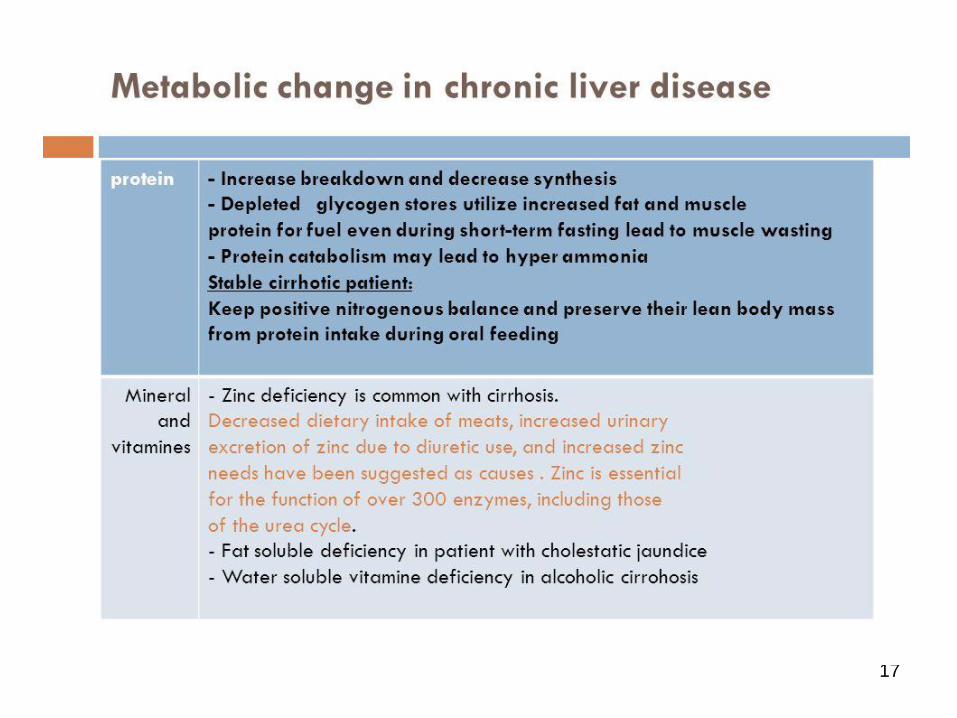
17
18
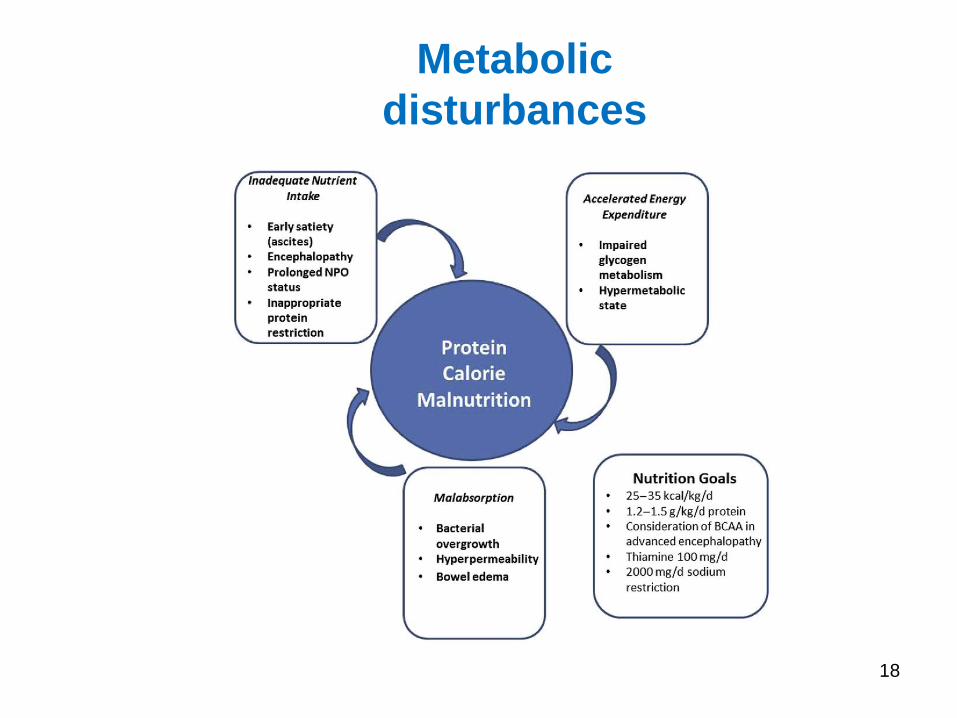
Metabolic
disturbances
19
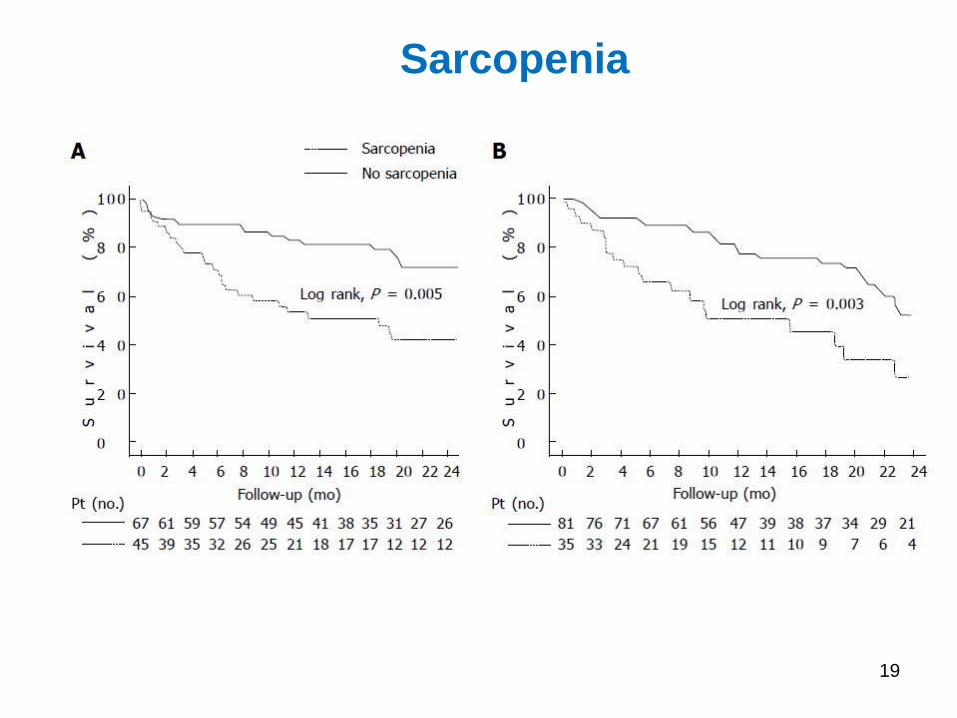
Sarcopenia
20
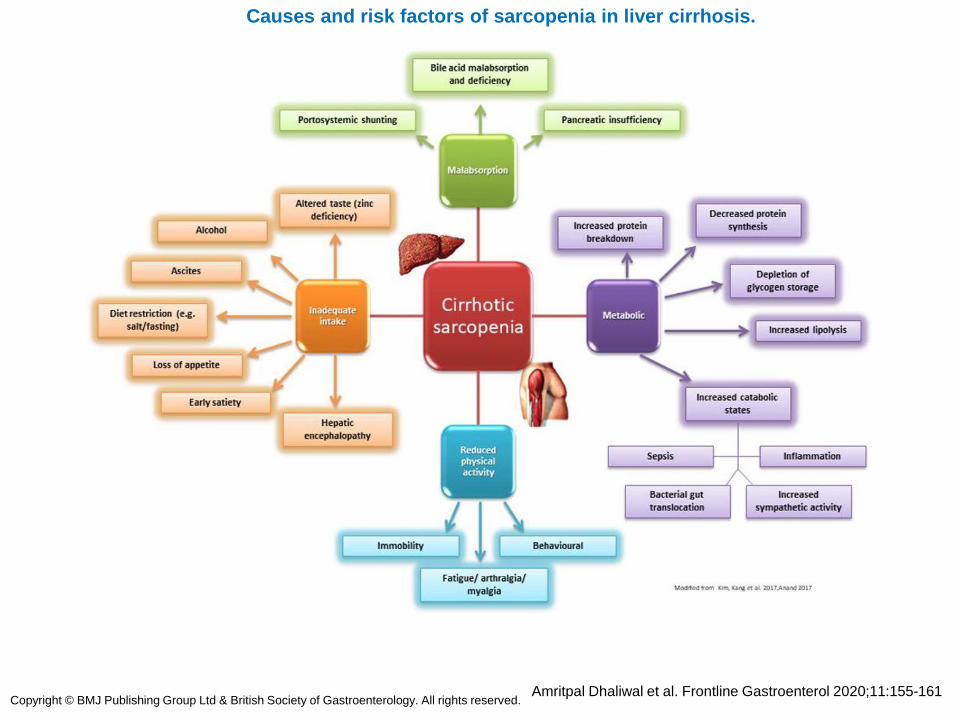
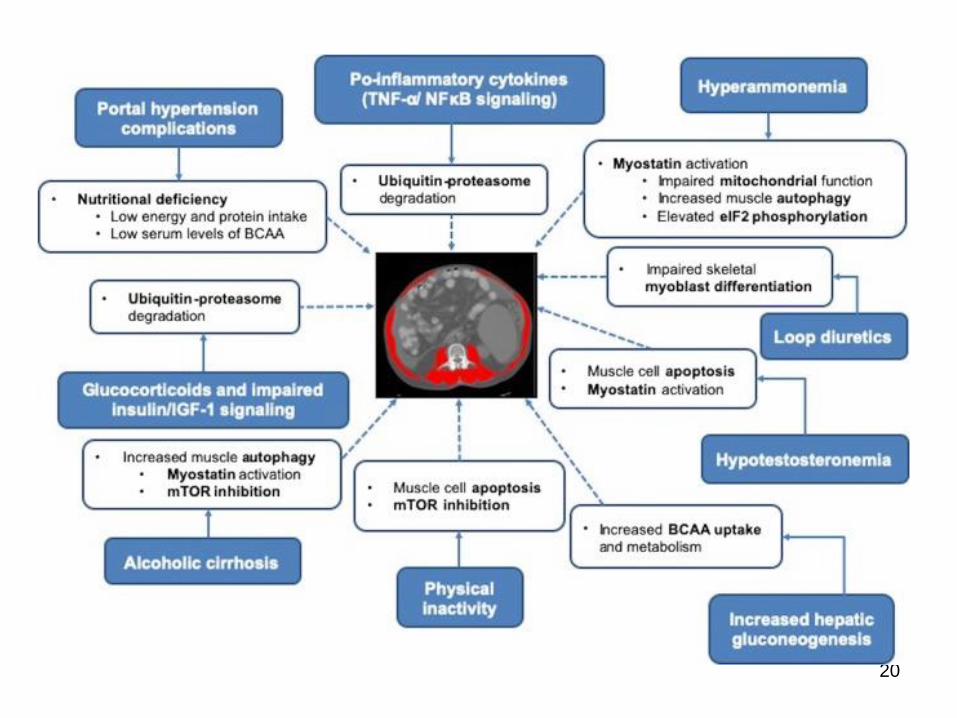
Causes and risk factors of sarcopenia in liver cirrhosis.
Amritpal Dhaliwal et al. Frontline Gastroenterol 2020;11:155-161Copyright © BMJ Publishing Group Ltd & British Society of Gastroenterology. All rights reserved.
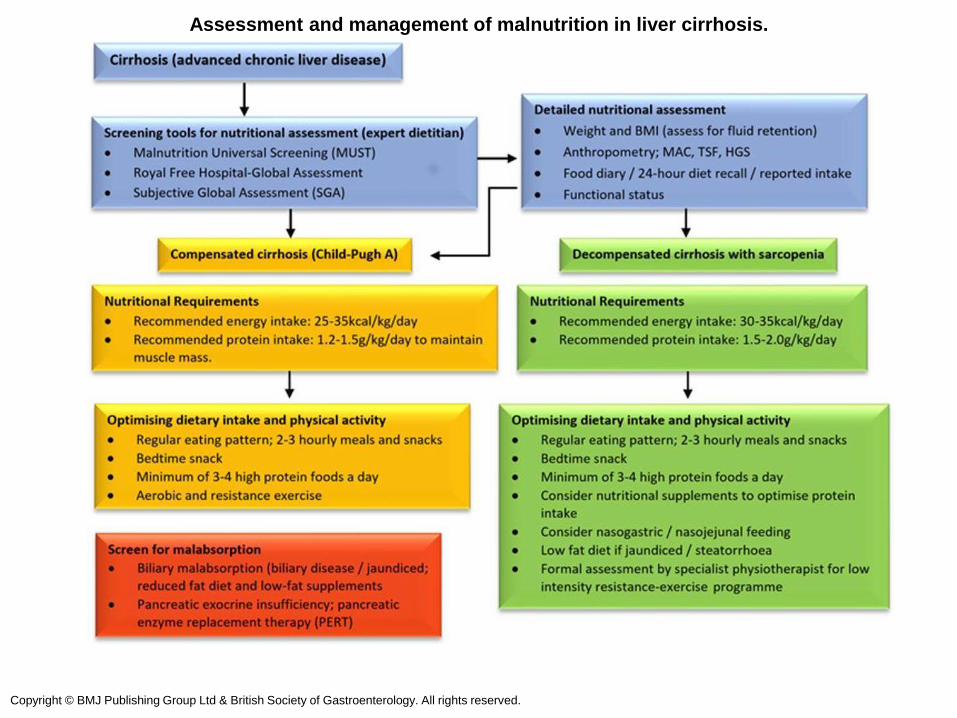
Assessment and management of malnutrition in liver cirrhosis.
Copyright © BMJ Publishing Group Ltd & British Society of Gastroenterology. All rights reserved.
Liver cirrhosis
Most complications of liver cirrhosisresult from portal hypertension
What mechanisms lead to
portal hypertension?
23
Portal hypertension
In liver cirrhosis
portal hypertension is causedprimarly by increased
intrahepatic resistance caused by liver fibrosis at the perisinusoidal
level
24
Portal hypertensionPortal hypertension is defined as the elevation of the hepatic venous
pressure gradient (HVPG) to >5 mmHg.
Portal hypertension is caused by a combination of two simultaneously occurring hemodynamic processes:
(1) increased intrahepatic resistance to the passage of blood flow through the liver due to cirrhosis and regenerative nodules, and
(2) increased splanchnic blood flow secondary to vasodilatation within the splanchnic vascular bed.
Direct measurement of portal pressure is invasive, inconvenient, and clinically impractical.
25
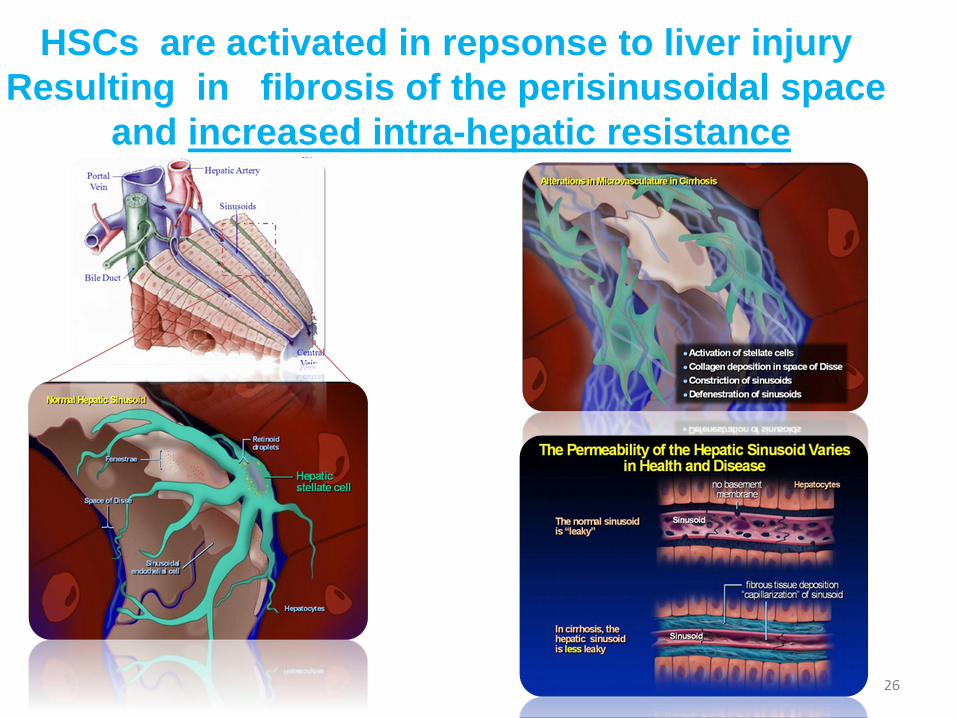
HSCs are activated in repsonse to liver injury
Resulting in fibrosis of the perisinusoidal space
and increased intra-hepatic resistance
26
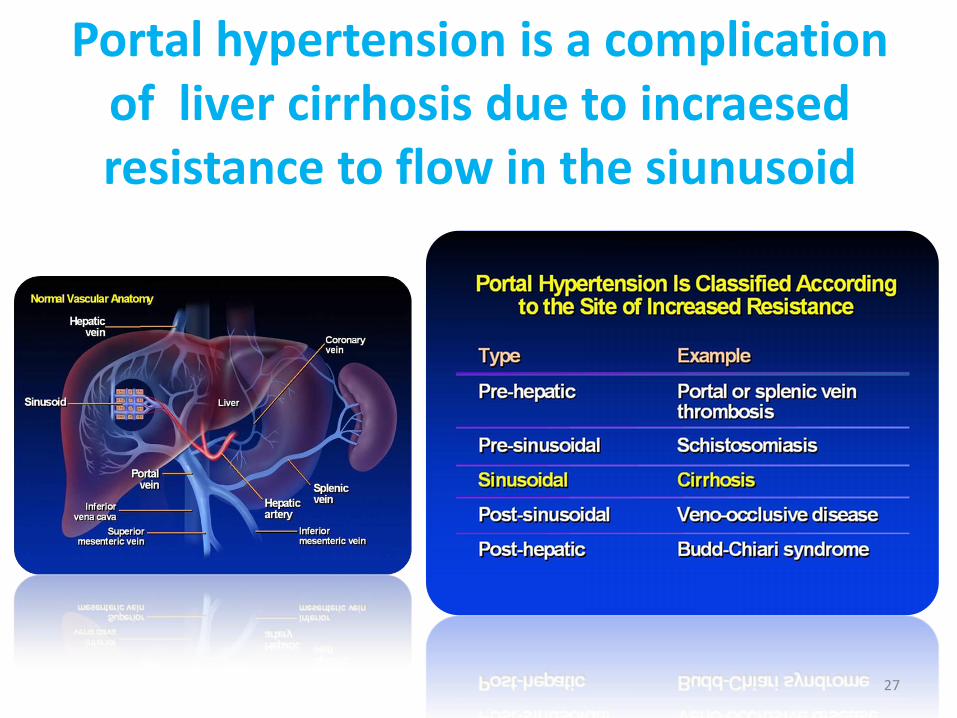
Portal hypertension is a complicationof liver cirrhosis due to incraesedresistance to flow in the siunusoid
27
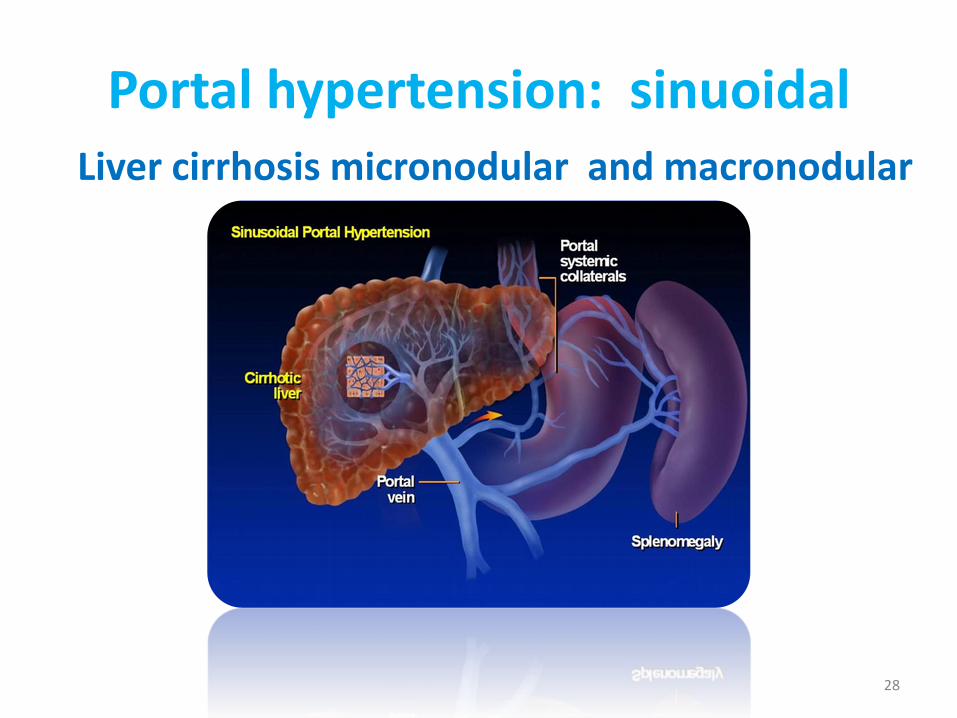
Portal hypertension: sinuoidalLiver cirrhosis micronodular and macronodular
28
Portal hypertensionPortal hypertension is directly responsible for the three major complications of cirrhosis,
• variceal hemorrhage,
• ascites
• hepatorenal syndrome.
Variceal hemorrhage is an immediate life-threatening problem with a 20–30% mortality associated with each episode of bleeding.
In addition portal hypertension contributes to indirectlyto development of hepatic encephalopaty
29
Portal hypertension: systemichemodynamic effects
The progressive course of cirrhosis with portal hypertension and arterial
vasodilatation leads to the developmentof central hypovolaemia, hyperdynamic
circulation and activation of vasoconstrictor systems (renin &
angiotensin) causing variouscomplications, including hepatorenal
syndrome and hepato-pulmonarysyndrome 30
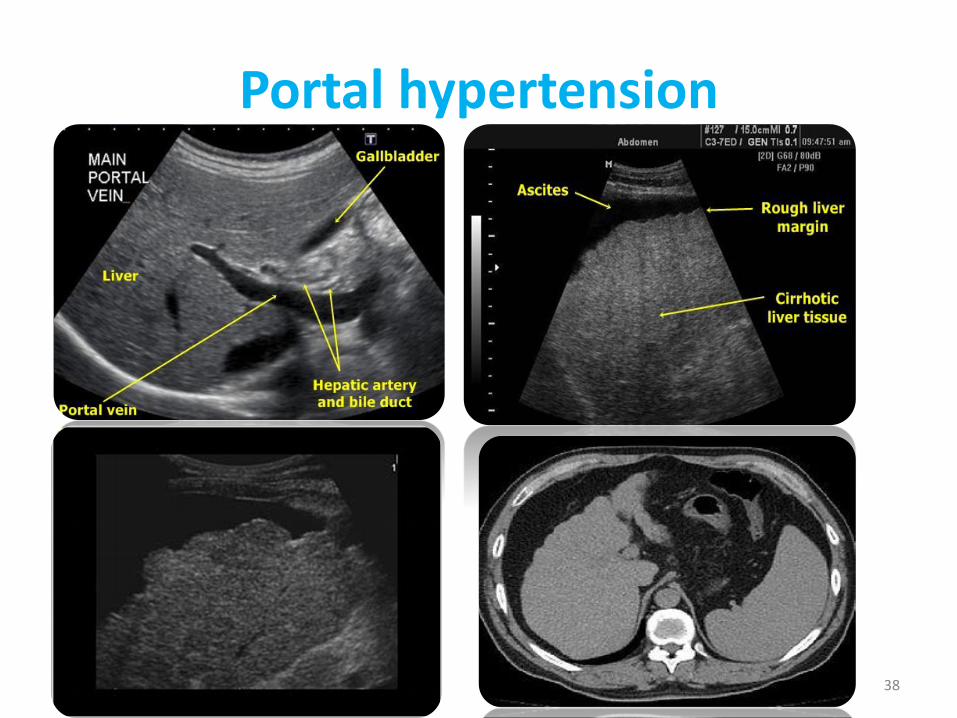
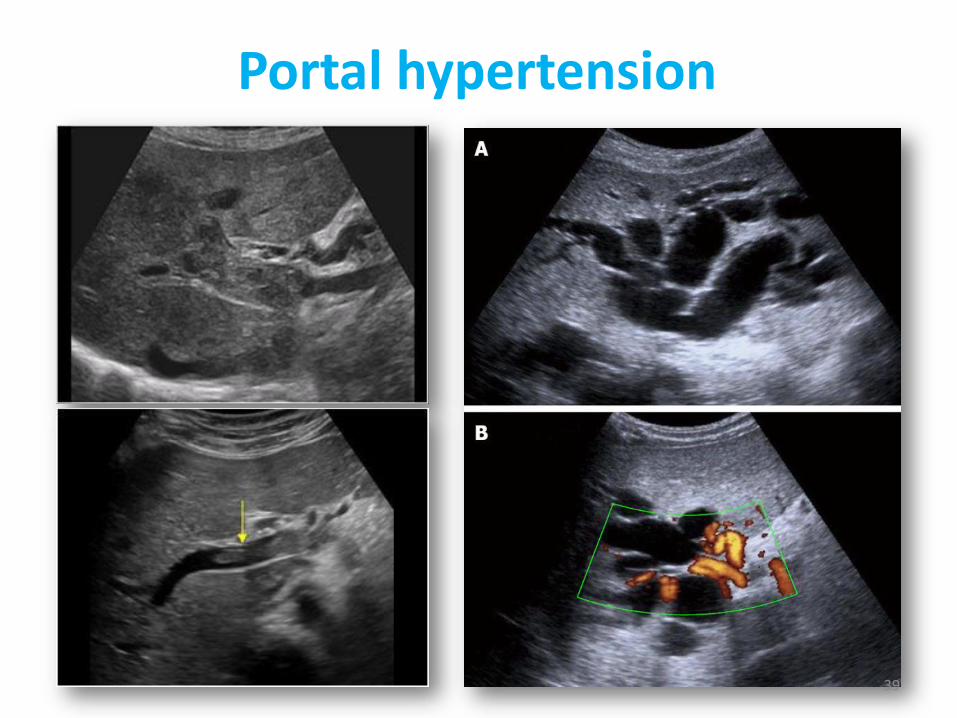
Portal hypertension
Diagnosis- Indirect measurement of portal pressure
- Imaging of liver and spleen and portal system and collateral circulation
Sonography
CT/angiography
- Detecting and grading varices in the GI tract
Endoscopy
31
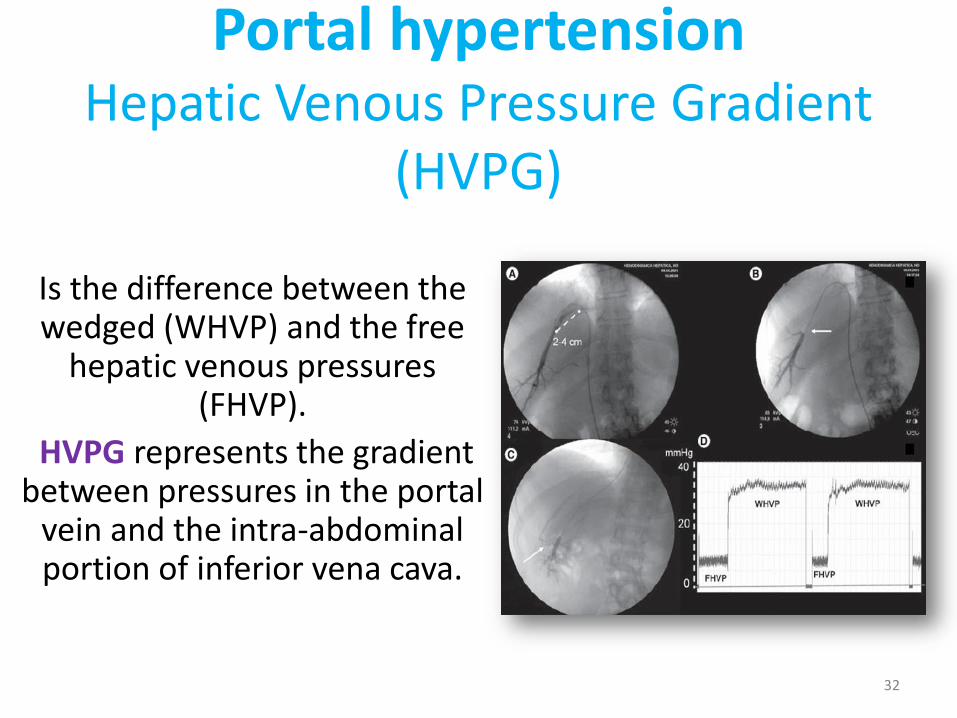
Portal hypertensionHepatic Venous Pressure Gradient
(HVPG)
Is the difference between the wedged (WHVP) and the free
hepatic venous pressures (FHVP).
HVPG represents the gradient between pressures in the portal
vein and the intra-abdominal portion of inferior vena cava.
32
Portal hypertensionThe normal HVPG value is between 1 to 5 mmHg.
Pressure higher than this defines the presence of portal hypertension, regardless of clinical evidence.
HVPG >or= 10 mmHg (clinically significant portal hypertension) is predictive of the development of complications of cirrhosis, including death.
HVPG above 12 mmHg is the threshold pressure for variceal rupture.
33
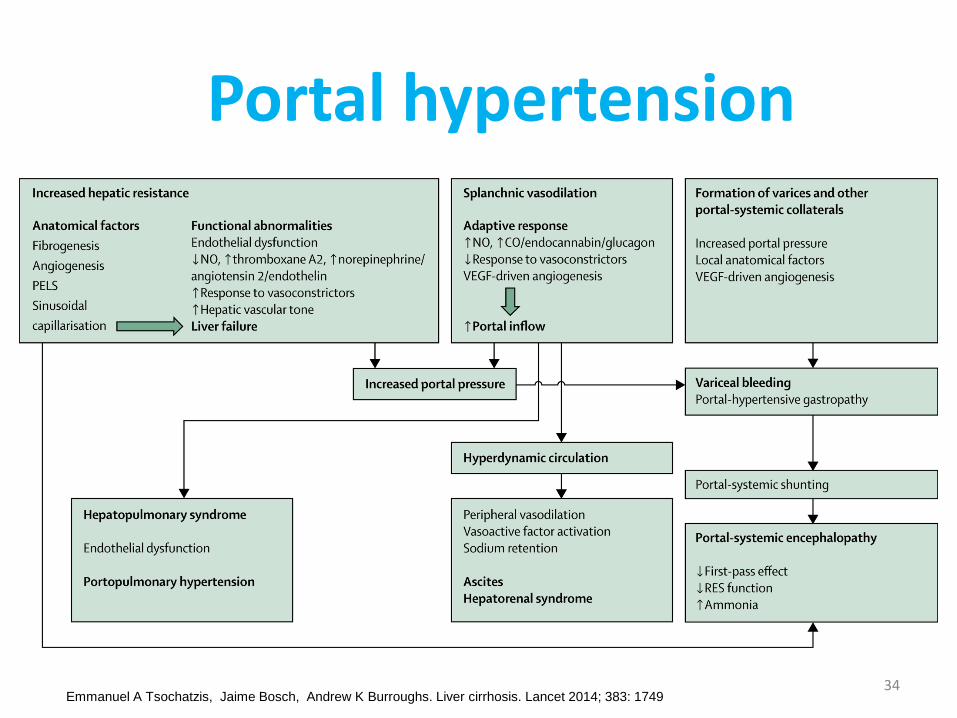
Portal hypertension
Emmanuel A Tsochatzis, Jaime Bosch, Andrew K Burroughs. Liver cirrhosis. Lancet 2014; 383: 174934
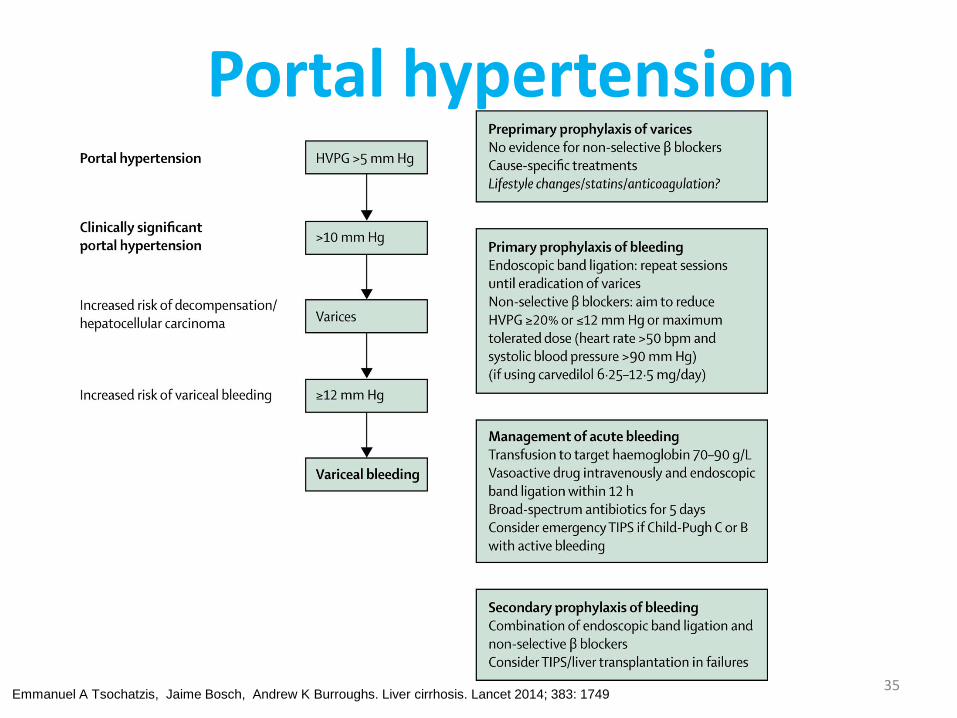
Portal hypertension
Emmanuel A Tsochatzis, Jaime Bosch, Andrew K Burroughs. Liver cirrhosis. Lancet 2014; 383: 174935
Portal hypertension: diagnosis
• In patients with cirrhosis who are being followed chronically, the development of portal hypertension is usually revealed by the presence of:
1. thrombocytopenia;
2. the appearance of an enlarged spleen;
3. or the development of ascites, encephalopathy and/or esophageal varices with or without bleeding.
36
Portal hypertension: diagnosis
In previously undiagnosed patients, any of these features should prompt further evaluation to
determine the presence of portal hypertension and liver disease.
• Abdominal imaging, either by sonography, CT or MRI, can be helpful in demonstrating a nodular liver and in finding changes of portal hypertension with intraabdominal collateral circulation.
• Varices should be identified by endoscopy37
Portal hypertension
38
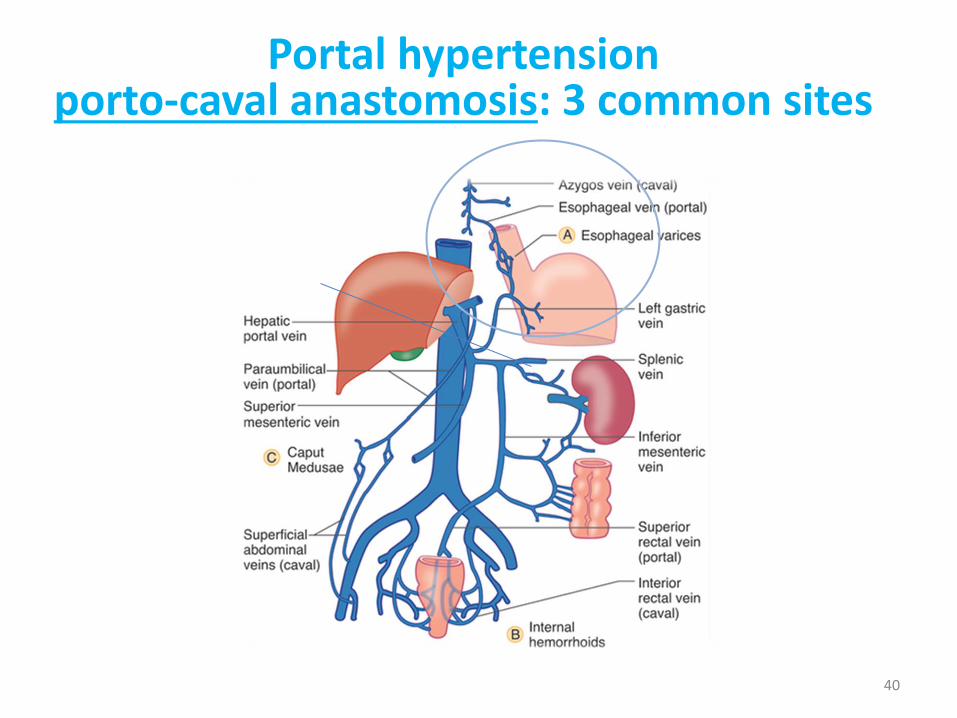
Portal hypertensionporto-caval anastomosis: 3 common sites
40
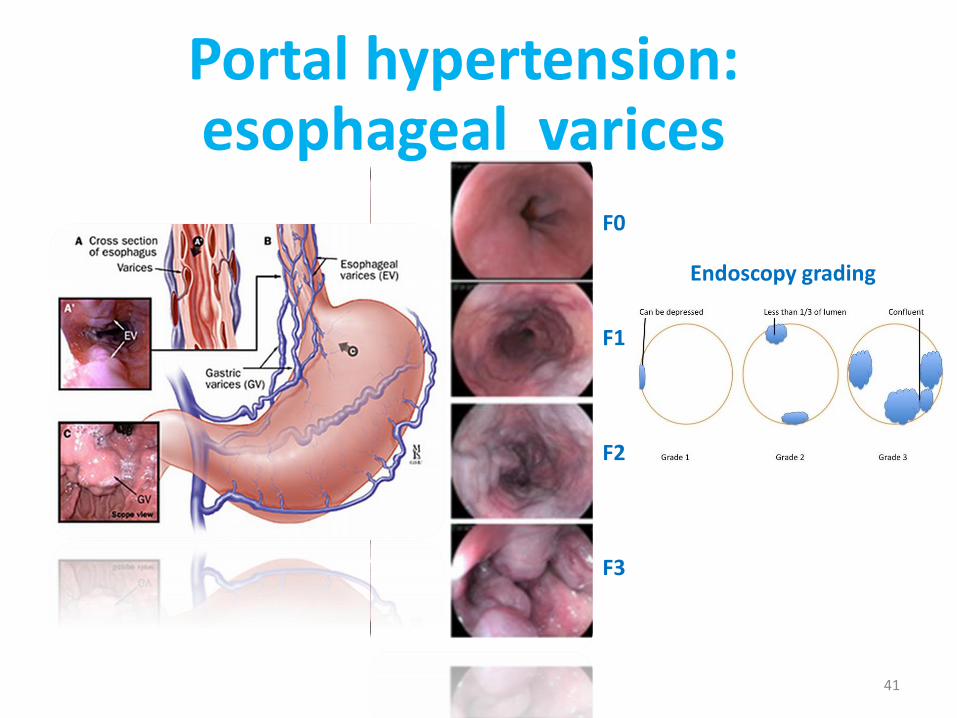
Portal hypertension: esophageal varices
F0
F1
F2
F3
F0
F1
F2
F3
41
Endoscopy grading
F0
F1
F2
F3
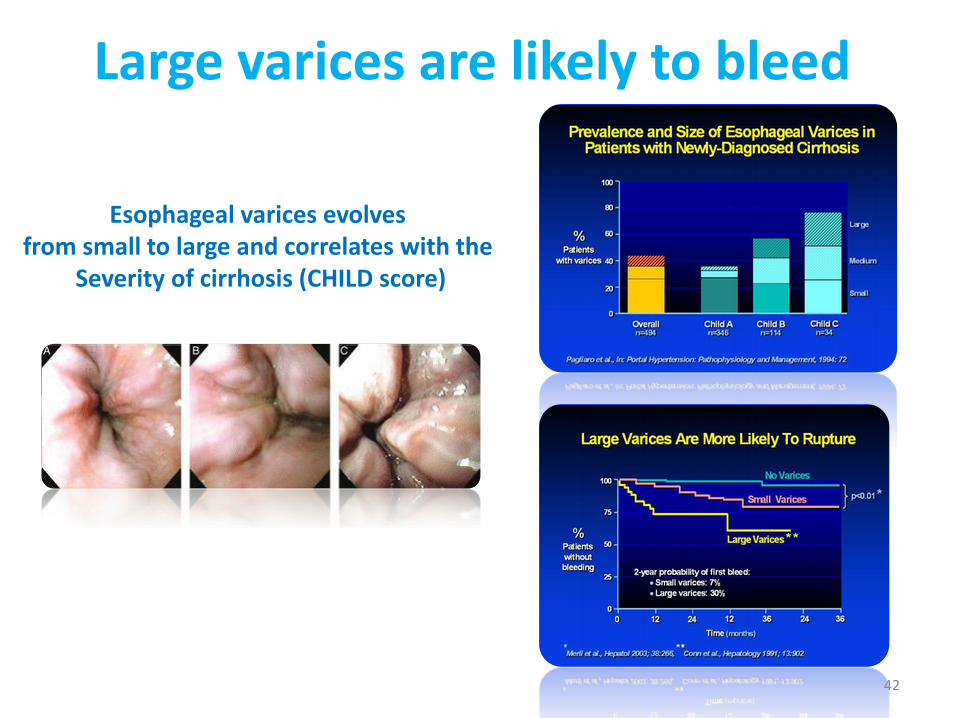
Large varices are likely to bleed
42
Esophageal varices evolvesfrom small to large and correlates with the
Severity of cirrhosis (CHILD score)
Variceal Hemorrhage: profilaxis of first bleeding
Treatment for variceal hemorrhage as a complication of portal hypertension is divided into two main categories:
(1) primary prophylaxis
(2) Secondary prophylaxis prevention of re-bleeding once
43
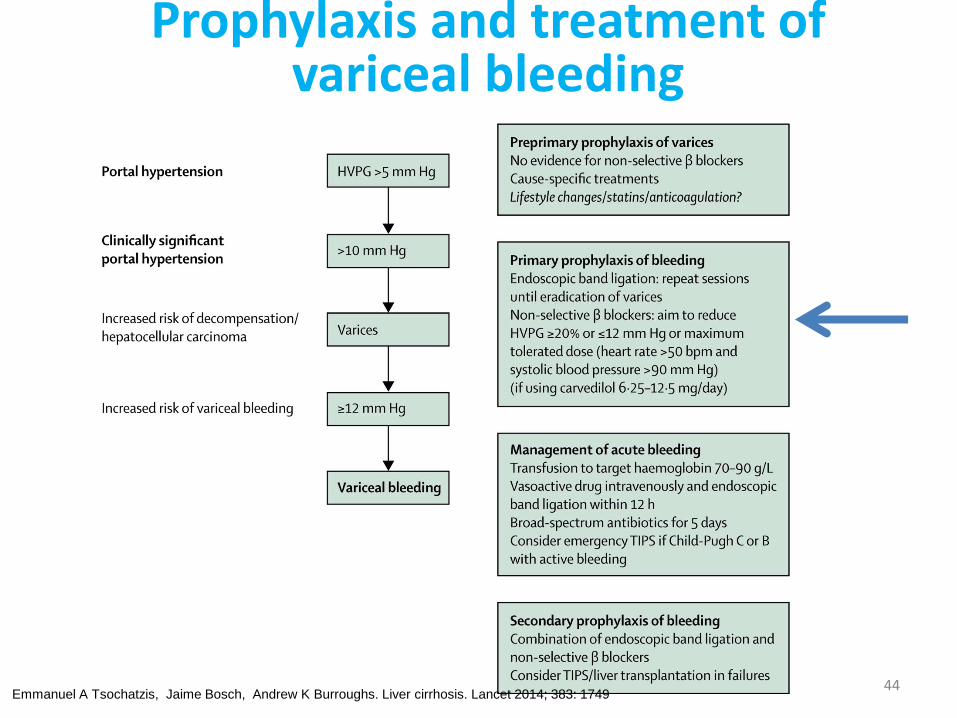
Prophylaxis and treatment of variceal bleeding
Emmanuel A Tsochatzis, Jaime Bosch, Andrew K Burroughs. Liver cirrhosis. Lancet 2014; 383: 174944
Liver cirrhosis
Ascites
45
Liver cirrhosis: splenomegaly and its clinical effects
• Congestive splenomegaly is common in patients with portal hypertension.
• Clinical features include the presence of an enlarged spleen on physical examination and the development of thrombocytopenia and leukopenia in patients who have cirrhosis. Some patients will have fairly significant left-sided and left upper quadrant abdominal pain.
• Splenomegaly itself usually requires no specific treatment, although splenectomy can be successfully performed under very special circumstances.
• Hypersplenism with the development of thrombocytopenia is a common feature of patients with cirrhosis and is the first indication of portal hypertension.
46
Liver cirrhosis: complications
Ascites
Ascites is the accumulation of fluid within the peritoneal cavity.
The most common cause of ascites is portal hypertension related to cirrhosis.
However, clinicians should remember that malignant or infectious causes of ascites can be present as well, and careful differentiation of these other causes are obviously important for patient care.
47
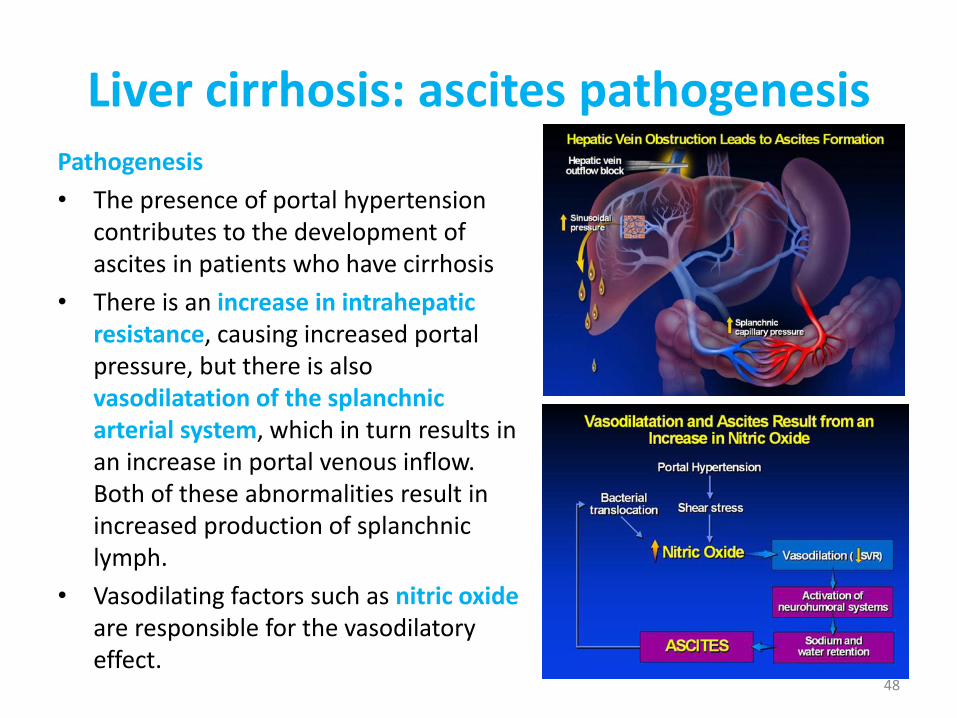
Liver cirrhosis: ascites pathogenesisPathogenesis
• The presence of portal hypertension contributes to the development of ascites in patients who have cirrhosis
• There is an increase in intrahepatic resistance, causing increased portal pressure, but there is also vasodilatation of the splanchnic arterial system, which in turn results in an increase in portal venous inflow. Both of these abnormalities result in increased production of splanchnic lymph.
• Vasodilating factors such as nitric oxide are responsible for the vasodilatoryeffect.
48
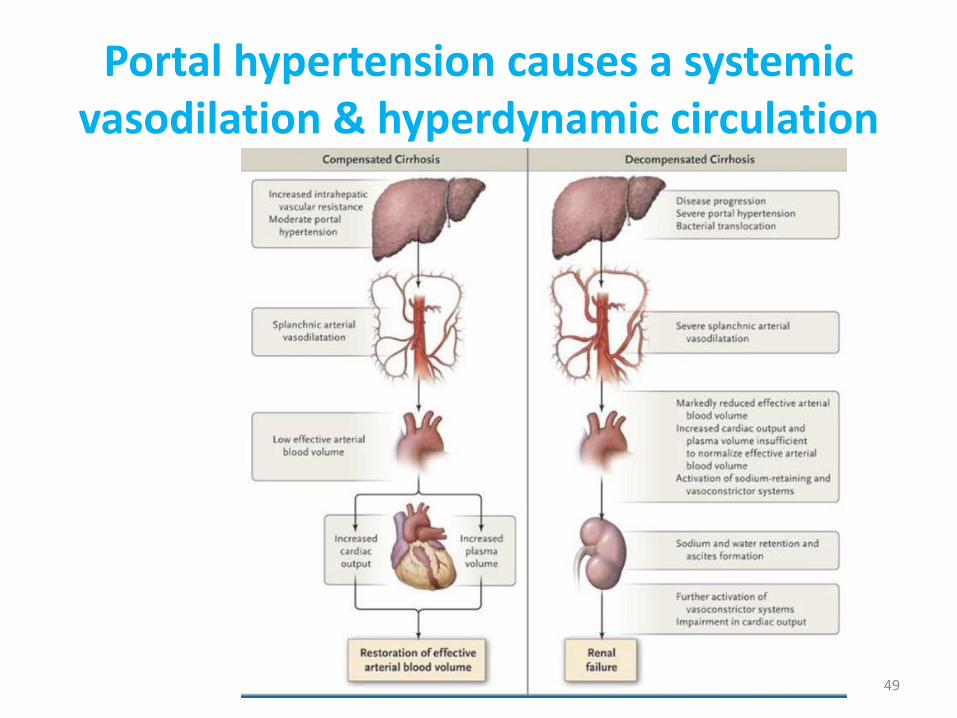
Portal hypertension causes a systemicvasodilation & hyperdynamic circulation
49
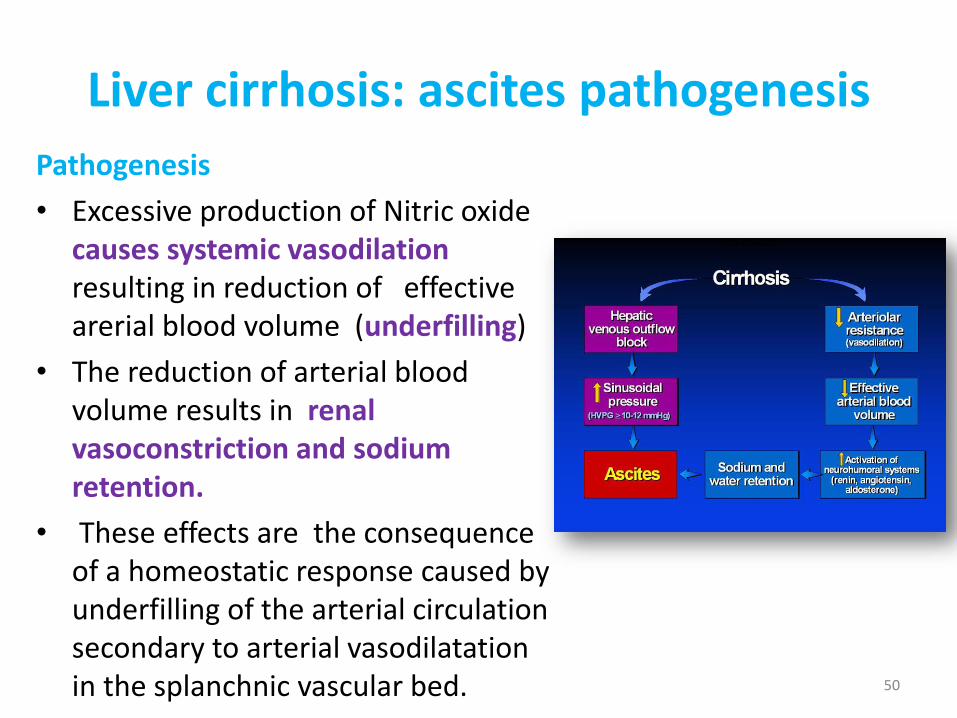
Liver cirrhosis: ascites pathogenesis
Pathogenesis
• Excessive production of Nitric oxide causes systemic vasodilation resulting in reduction of effective arerial blood volume (underfilling)
• The reduction of arterial blood volume results in renal vasoconstriction and sodium retention.
• These effects are the consequence of a homeostatic response caused by underfilling of the arterial circulation secondary to arterial vasodilatation in the splanchnic vascular bed. 50
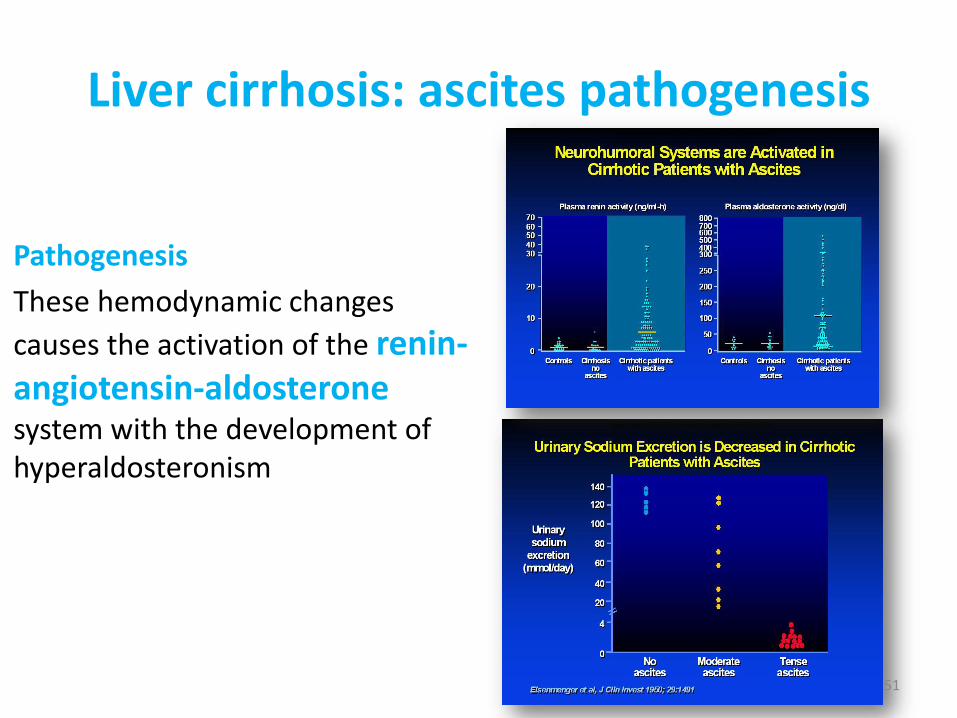
Liver cirrhosis: ascites pathogenesis
Pathogenesis
These hemodynamic changes
causes the activation of the renin-angiotensin-aldosteronesystem with the development of hyperaldosteronism
51
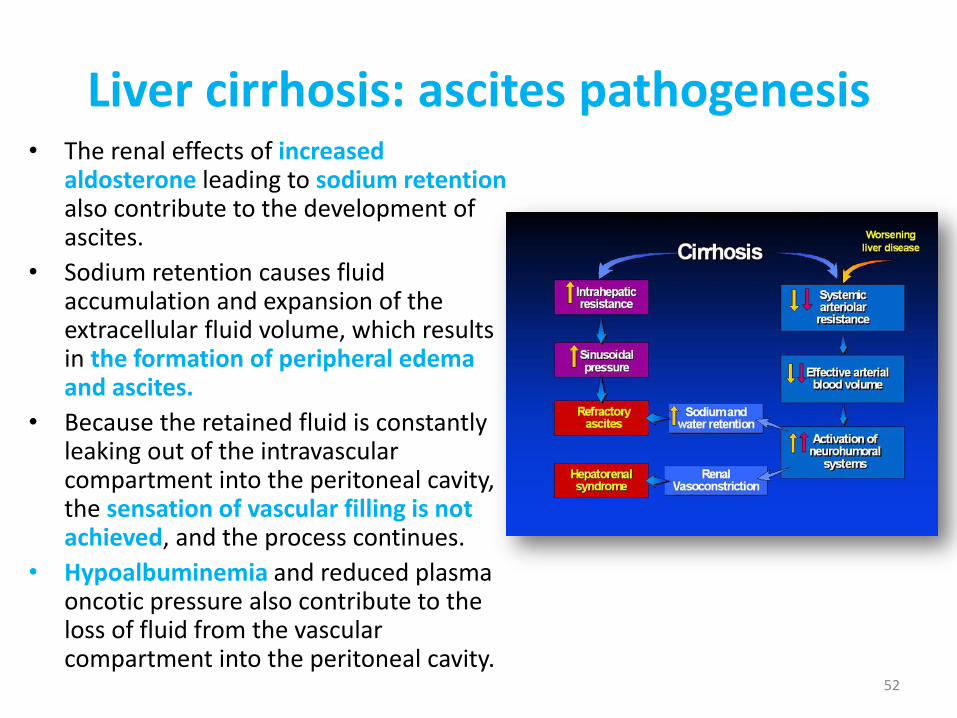
Liver cirrhosis: ascites pathogenesis• The renal effects of increased
aldosterone leading to sodium retention also contribute to the development of ascites.
• Sodium retention causes fluid accumulation and expansion of the extracellular fluid volume, which results in the formation of peripheral edema and ascites.
• Because the retained fluid is constantly leaking out of the intravascular compartment into the peritoneal cavity, the sensation of vascular filling is not achieved, and the process continues.
• Hypoalbuminemia and reduced plasma oncotic pressure also contribute to the loss of fluid from the vascular compartment into the peritoneal cavity.
52
Liver cirrhosis: ascites
Clinical• Patients typically note an increase in abdominal girth that is often
accompanied by the development of peripheral edema.
• The development of ascites is often insidious, and it is surprising that some patients wait so long and become so distended before seeking medical attention.
• Patients usually have at least 1–2 L of fluid in the abdomen before they are aware that there is an increase.
• If ascitic fluid is massive, respiratory function can be compromised, and patients will complain of shortness of breath. Hepatic hydrothorax may also occur in this setting, contributing to respiratory symptoms. Patients with massive ascites are often malnourished and have muscle wasting and excessive fatigue and weakness.
53
Liver cirrhosis: ascitesDiagnosis
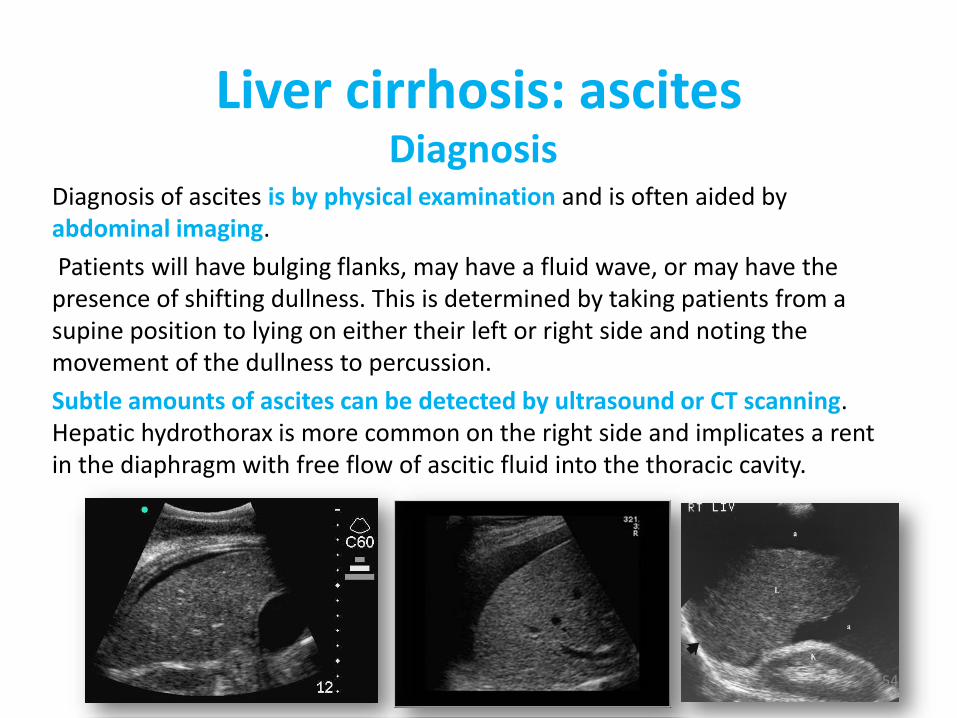
Diagnosis of ascites is by physical examination and is often aided by abdominal imaging.
Patients will have bulging flanks, may have a fluid wave, or may have the presence of shifting dullness. This is determined by taking patients from a supine position to lying on either their left or right side and noting the movement of the dullness to percussion.
Subtle amounts of ascites can be detected by ultrasound or CT scanning. Hepatic hydrothorax is more common on the right side and implicates a rent in the diaphragm with free flow of ascitic fluid into the thoracic cavity.
54
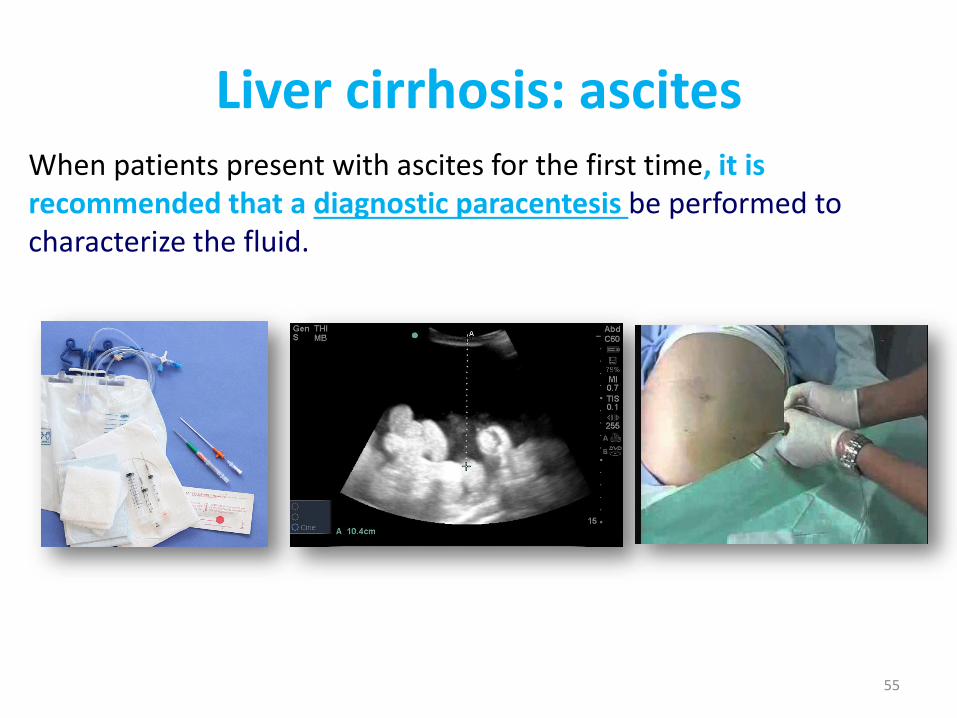
Liver cirrhosis: ascitesWhen patients present with ascites for the first time, it is recommended that a diagnostic paracentesis be performed to characterize the fluid.
55
Treatment• Patients with small amounts of ascites can usually be managed with
dietary sodium restriction alone.
• Most average diets contain 6 to 8 g of sodium per day and if patients eat at restaurants or fast food outlets, the amount of sodium in their diet can exceed this amount. Thus, it is often extremely difficult to get patients to change their dietary habits to ingest < 2 g of sodium per day, which is the amount that is recommended.
• Patients are frequently surprised to realize how much sodium is in the standard diet and thus it is important to make educational pamphlets available to the patient.
• Often, a simple recommendation is to eat fresh or frozen foods, avoiding canned or processed foods, which are usually preserved with sodium.
Liver cirrhosis: ascites
56
• When a moderate amount of ascites is present, diuretic therapy is usually necessary.
• Traditionally, spironolactone at 100–200 mg/d as a single dose is started, and furosemide may be added at 40–80 mg/d, particularly in patients who have peripheral edema.
• In patients who have never received diuretics before, the failure of the above-mentioned dosages suggests that they are not being compliant with a low-sodium diet.
• If compliance is confirmed and ascitic fluid is not being mobilized, spironolactone can be increased to 400–600 mg/d and furosemide increased to 120–160 mg/d.
Liver cirrhosis: ascites
57
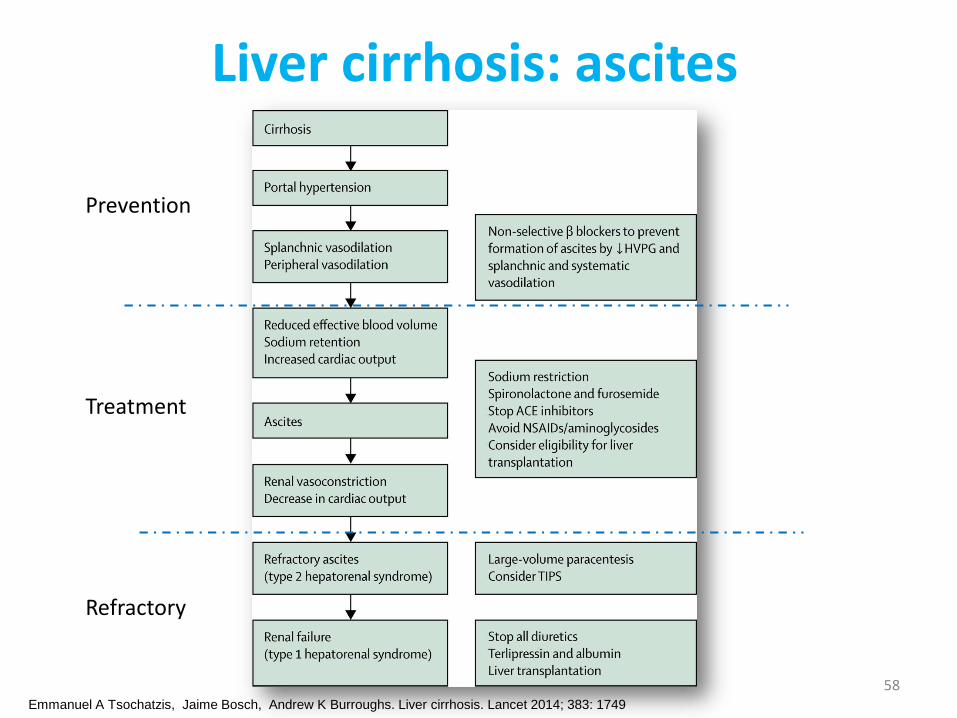
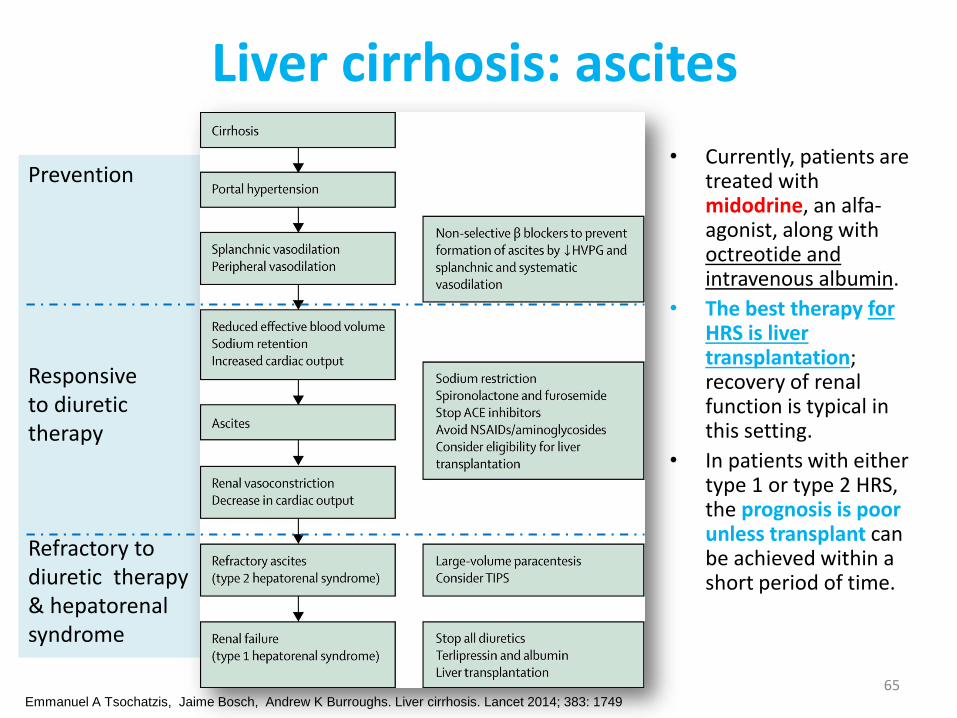
Liver cirrhosis: ascites
Prevention
Treatment
Refractory
Emmanuel A Tsochatzis, Jaime Bosch, Andrew K Burroughs. Liver cirrhosis. Lancet 2014; 383: 1749
58
• If ascites is still present with these dosages of diuretics in patients who are compliant with a low-sodium diet, then they are defined as having refractory ascites, and alternative treatment modalities including repeated large-volume paracentesis, or a TIPS procedure should be considered .
• Recent studies have shown that TIPS, while managing the ascites, does not improve survival in these patients. Unfortunately, TIPS is often associated with an increased frequency of hepatic encephalopathy and must be considered carefully on a case-by-case basis.
• The prognosis for patients with cirrhosis with ascites is poor, and some studies have shown that <50% of patients survive 2 years after the onset of ascites. Thus, there should be consideration for liver transplantation in patients with the onset of ascites.
Liver cirrhosis: refractory ascites
59
Spontaneous Bacterial Peritonitis • SBP is a common and severe complication of ascites
characterized by spontaneous infection of the ascitic fluid without an intraabdominal source.
• In patients with cirrhosis and ascites severe enough for hospitalization, SBP can occur in up to 30% of individuals and can have a 25% in-hospital mortality rate.
• The diagnosis of SBP is made when the fluid sample has an absolute neutrophil count >250/mm3
Liver cirrhosis: ascites
60
Liver cirrhosis
Hepatorenal syndrome
61
Hepatorenal SyndromeThe hepatorenal syndrome (HRS) is a form of functional renal failure without renal pathology that occurs in about 10% of patients with advanced cirrhosis or acute liver failure.
There are marked disturbances in the arterial renal circulation in patients with HRS; these include an increase in vascular resistance in the kidney accompanied by a reduction in systemic vascular resistance.
The reason for renal vasoconstriction is most likely multifactorial and is poorly understood.
Liver cirrhosis: complications
62
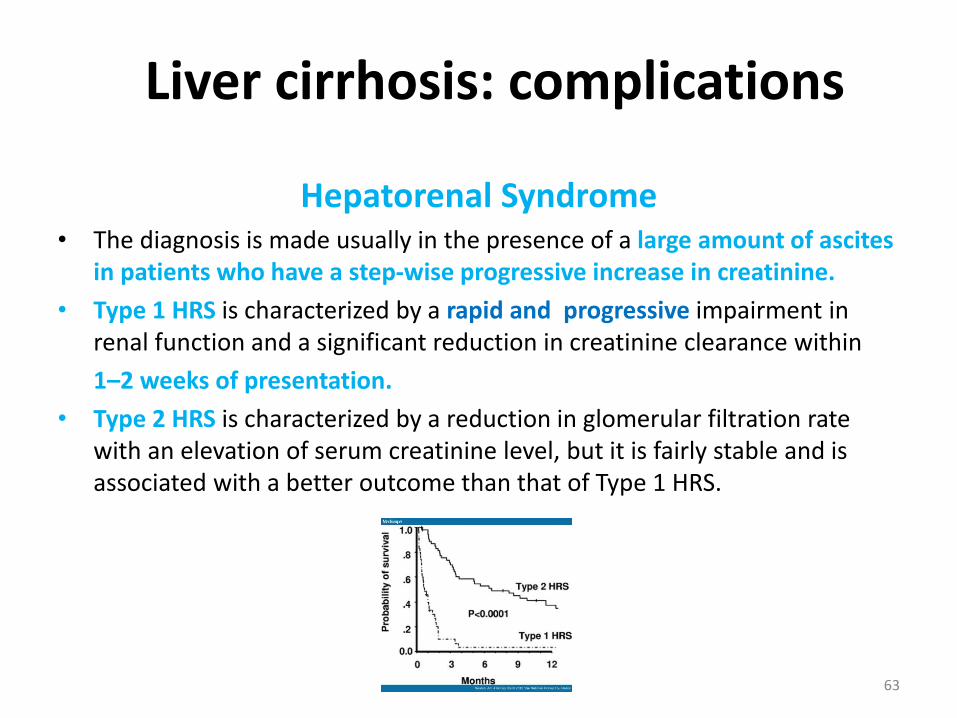
Hepatorenal Syndrome• The diagnosis is made usually in the presence of a large amount of ascites
in patients who have a step-wise progressive increase in creatinine.
• Type 1 HRS is characterized by a rapid and progressive impairment in renal function and a significant reduction in creatinine clearance within
1–2 weeks of presentation.
• Type 2 HRS is characterized by a reduction in glomerular filtration rate with an elevation of serum creatinine level, but it is fairly stable and is associated with a better outcome than that of Type 1 HRS.
Liver cirrhosis: complications
63
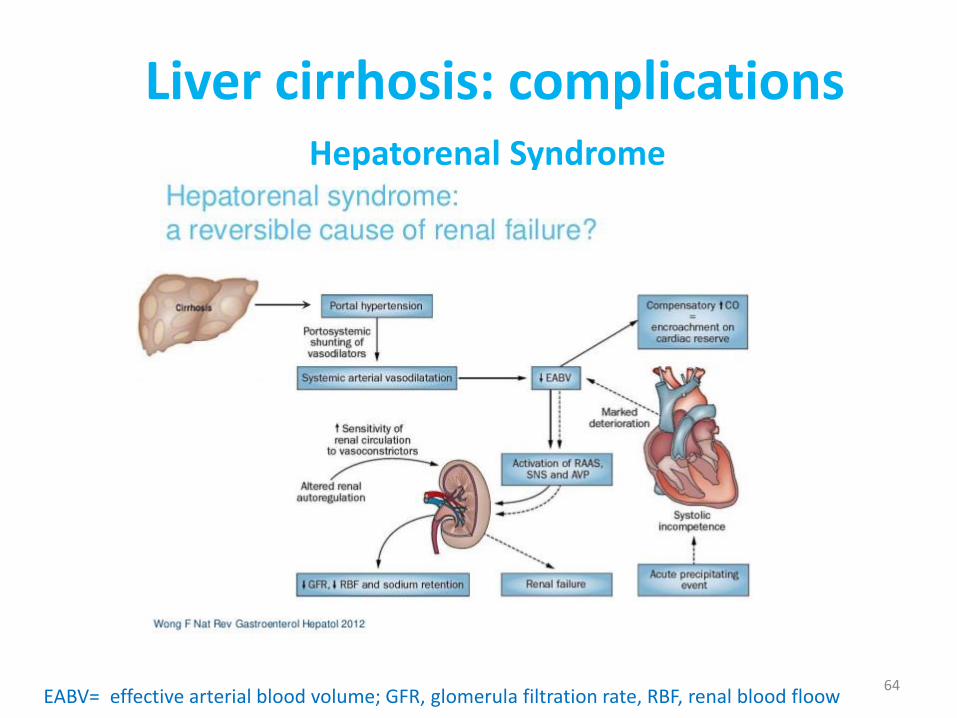
Hepatorenal Syndrome
Liver cirrhosis: complications
EABV= effective arterial blood volume; GFR, glomerula filtration rate, RBF, renal blood floow64
Prevention
Responsive to diuretictherapy
Refractory todiuretic therapy& hepatorenalsyndrome
Liver cirrhosis: ascites
• Currently, patients are treated with midodrine, an alfa-agonist, along with octreotide and intravenous albumin.
• The best therapy for HRS is liver transplantation; recovery of renal function is typical in this setting.
• In patients with either type 1 or type 2 HRS, the prognosis is poor unless transplant can be achieved within a short period of time.
Emmanuel A Tsochatzis, Jaime Bosch, Andrew K Burroughs. Liver cirrhosis. Lancet 2014; 383: 1749
65
Liver cirrhosis
Hepatic encephalopathy
66
Portosystemic encephalopathy is a serious complication of chronic liver disease and is broadly defined as an alteration in mental status and cognitive function
occurring in the presence of liver failure.
• In acute liver injury with fulminant hepatic failure, the development of encephalopathy is a requirement for a diagnosis of fulminant failure.
• Encephalopathy is much more commonly seen in patients with chronic liver disease.
Liver cirrosis: complicationsHepatic Encephalopathy
67
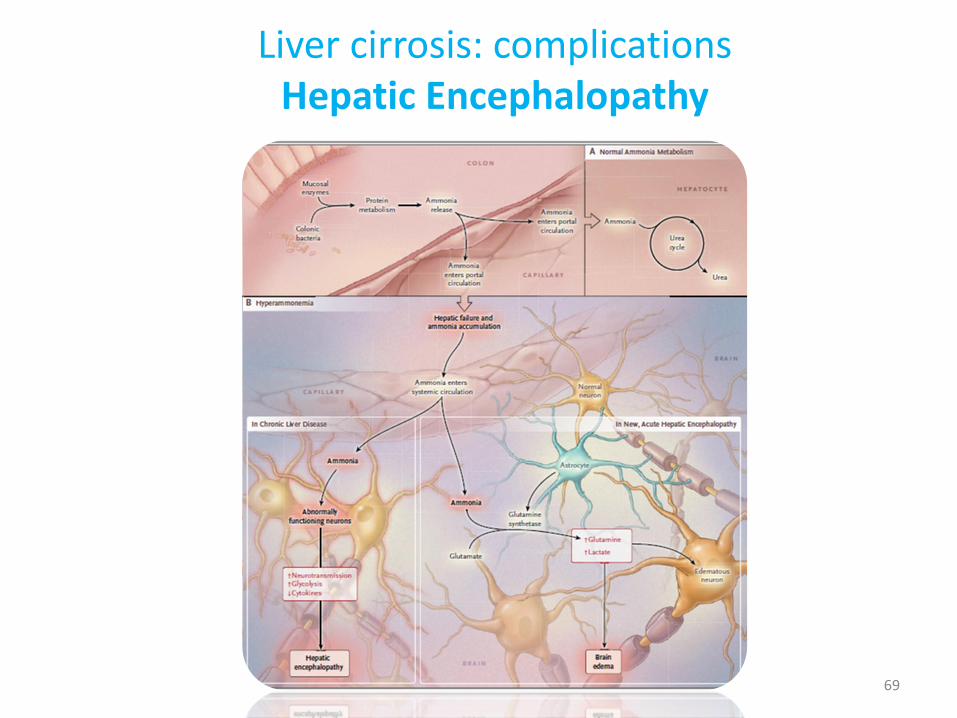
Gut-derived neurotoxins that are not removed by the liver because of vascular shunting and decreased hepatic mass get to the brain and cause the symptoms that we know of as hepatic encephalopathy.
Ammonia levels are typically elevated in patients with hepatic encephalopathy, but the correlation between severity of liver disease and height of ammonia levels is often poor, and most hepatologists do not rely on ammonia levels to make a diagnosis.
Other compounds and metabolites that may contribute to the development of encephalopathy include certain false neurotransmitters and mercaptans.
Liver cirrosis: complicationsHepatic Encephalopathy
68
Liver cirrosis: complicationsHepatic Encephalopathy
69
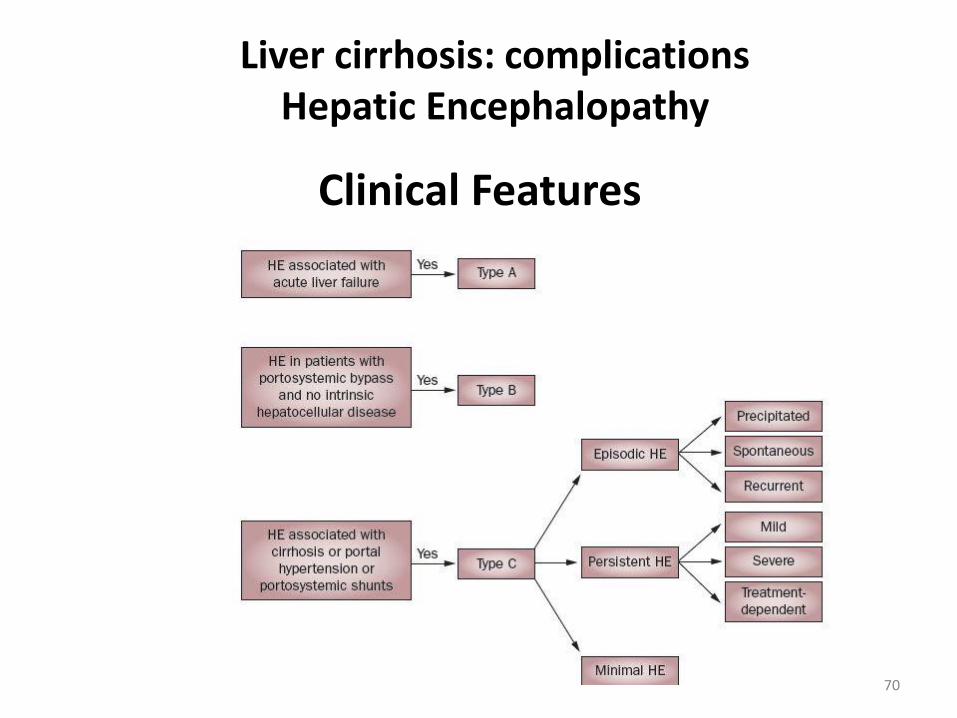
Clinical Features
Liver cirrhosis: complicationsHepatic Encephalopathy
70
• In patients with cirrhosis, encephalopathy is often found as a result of certain precipitating events such as diuretic therapy, infection, an increased dietary protein load, or electrolyte disturbances ( reduced K and Na).
• Because precipitating events are so commonly found, they should be sought carefully.
• If patients have ascites, this should be examined (paracentesis) to rule out infection.
• Evidence of GI bleeding should be sought, and patients should be appropriately hydrated.
• Electrolytes should be measured and abnormalities corrected.
• In patients presenting with encephalopathy, asterixis is often present.
• Asterixis can be elicited by having patients extend their arms and bend their wrists back. In this maneuver, patients who are encephalopathic have a "liver flap"—i.e., a sudden forward movement of the wrist.
Liver cirrhosis: complicationsHepatic Encephalopathy
71
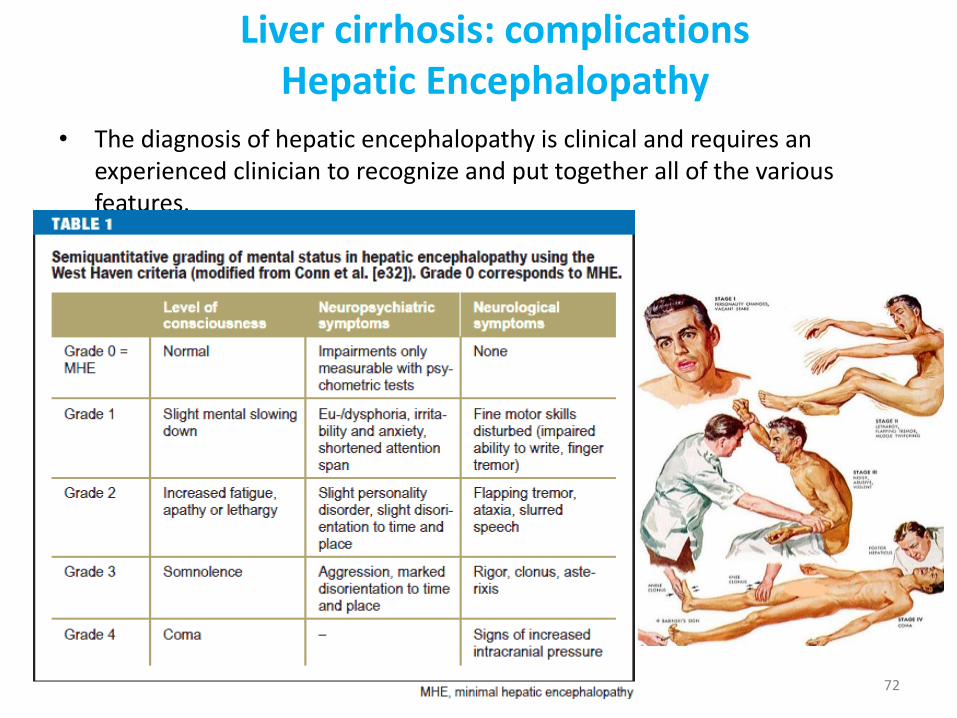
• The diagnosis of hepatic encephalopathy is clinical and requires an experienced clinician to recognize and put together all of the various features.
Liver cirrhosis: complicationsHepatic Encephalopathy
72
Treatment
• Treatment is multifactorial and includes management of the above-mentioned precipitating factors. Sometimes hydration and correction of electrolyte imbalance is all that is necessary. In the past, restriction of dietary protein was considered for patients with encephalopathy; however, the negative impact of that maneuver on overall nutrition is thought to outweigh the benefit when treating encephalopathy, and it is thus discouraged.
• There may be some benefit to replacing animal-based protein with vegetable-based protein in some patients with encephalopathy that is difficult to manage.
• The mainstay of treatment for encephalopathy, in addition to correcting precipitating factors, is to use lactulose, a nonabsorbable disaccharide, which results in colonic acidification. Catharsis ensues, contributing to the elimination of nitrogenous products in the gut that are responsible for the development of encephalopathy. The goal of lactulose therapy is to promote 2–3 soft stools per day.
Liver cirrhosis: complicationsHepatic Encephalopathy
73
• Patients are asked to titrate their amount of ingested lactulose to achieve the desired effect.
• Poorly absorbed antibiotics are used as adjunctive therapies for patients who have had a difficult time with lactulose.
• The alternating administration of neomycin and metronidazole has commonly been employed to reduce the individual side effects of each: neomycin for renal insufficiency and ototoxicity and metronidazole for peripheral neuropathy.
• More recently, rifaximin has been very effective in treating encephalopathy without the known side effects of neomycin or metronidazole.
Liver cirrhosis: complicationsHepatic Encephalopathy
74
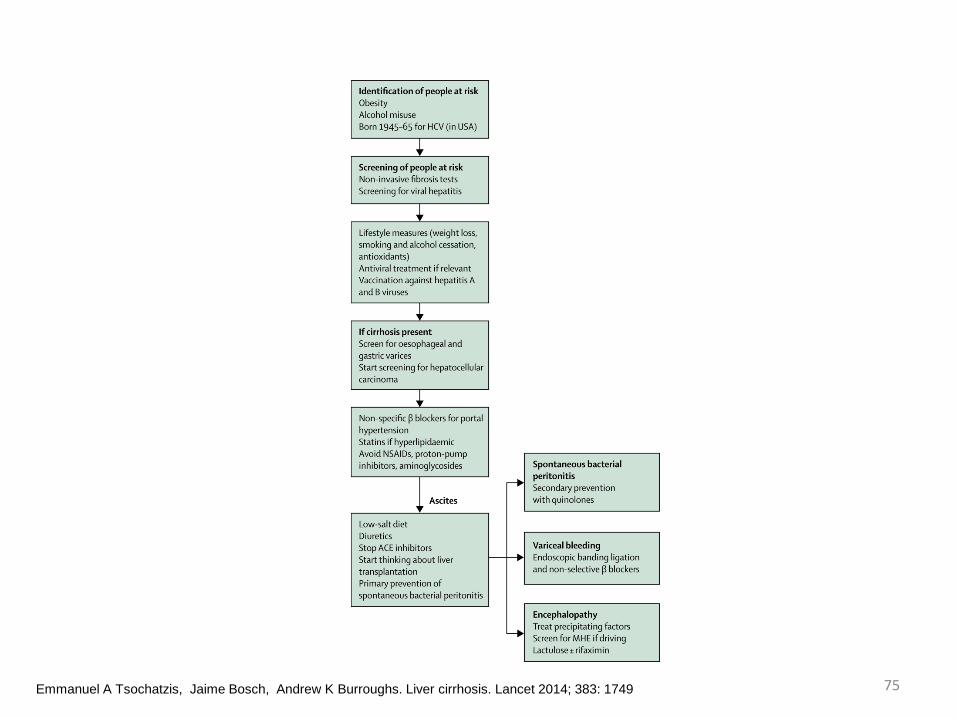
Emmanuel A Tsochatzis, Jaime Bosch, Andrew K Burroughs. Liver cirrhosis. Lancet 2014; 383: 1749 75