scig vs ivig: let’s give patients the choice! marie-claude levasseur inf. b.sc, d.e.s.s bioethic...
TRANSCRIPT

SCIg vs IVIg: Let’s Give Patients the Choice!
Marie-Claude Levasseur inf. B.Sc, D.E.S.S Bioethic Immunology-Rhumatology
ESID 30 octobre 2014

•Presentation of the context of the study
•Detailed presentation of the research
•Analyse of the result and interpretation
•Plans for the future
Plan
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

CHU Sainte Justine’s situation
SCIG home therapy programm since 2007
Approximately 185 patients on SCIG
Consultant for SCIG teaching programm with adults from other health care centers
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

IVIg and SCIg are equally efficient in patients with PID(1-5)
Use is often base on physician’s and nurse’s opinion on the “idealness” of the candidate.
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

The “ideal” patient- Accept his diagnosis- Active in his treatment- Responsable- Support- Honnest- Good comprenhension capacity- Always on time- Know exactly what he wants- Looks good- Looks “intelligent” - Smells good - E.t.c
Criteria based on “opinion” that sometimes do not match between the perception of the doctor and the nurse!
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

We realize that this perception was changing the way medical team explain the two treatment and was probably influencing the “choice” of the patient.
Not neutral!
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

Retrospective study Tertiary center with pediatric cohort143 patients with PID on Ig remplacement
• Present our experience regarding patient’s behavior when given choice of hospital-based IVIg versus home-based SCIg.
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

All patients, regardless of the physician and nurse’s impression of the “idealness”of the candidates were offered the choice
between hospital-based IVIg and home-based SCIg.
Switch cohort
• Patients already on IVIgwhen the choice of route of
administration was given.
New cohort
• Patients diagnosed after, given the choice at the beginning of Ig replacement.
SCIg availale in Quebec since 2007
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4
1- Physician explained both treatment options in general terms. 2- Clinical nurse provided technical explanation on the methods with written information describing modalities and side effects.
2 Steps:
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

• Clearly indicated that both routes were equally effective
• Patient had the choice to change their mind at a later point in time if desired and as many times has desired
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

Options:400mg/kg/months
IVIG
• Every 4 weeks in our day care center
• 4-6 hours infusion• No fees
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

Options:400mg/kg/months
SCIg
• 3 weeks of 2h teaching sessions• 15 min-60 min infusion once a
week• No fees• Pump provide by the company• 1:1 IV dose• Begin 1-2 weeks after IVIG
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

Demographic characteristics of patients in each cohorts
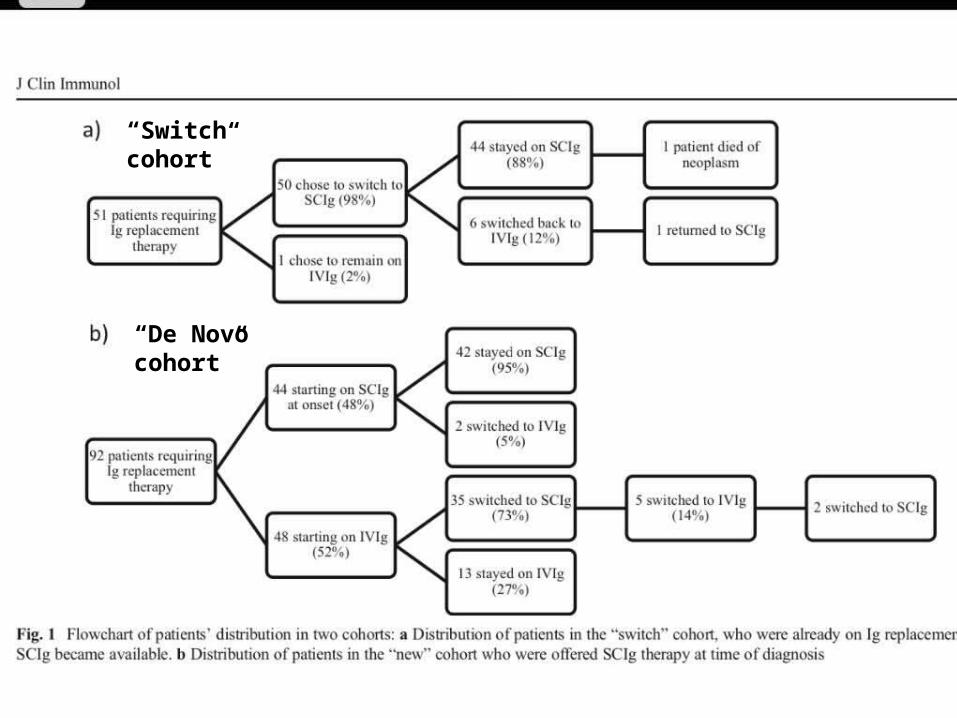
Result
• Analysis of the patient`s choice
“Switch cohort”
“De Novo cohort”

With same informations half choose SCIg, half IVIg, for first infusion.
If they choose IVIg hospital base:
• want to begin with support • afraid to make mistakes• want the child to “get use to it”...• are not ready to prick• still on “shock "of the diagnostic
Result
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4
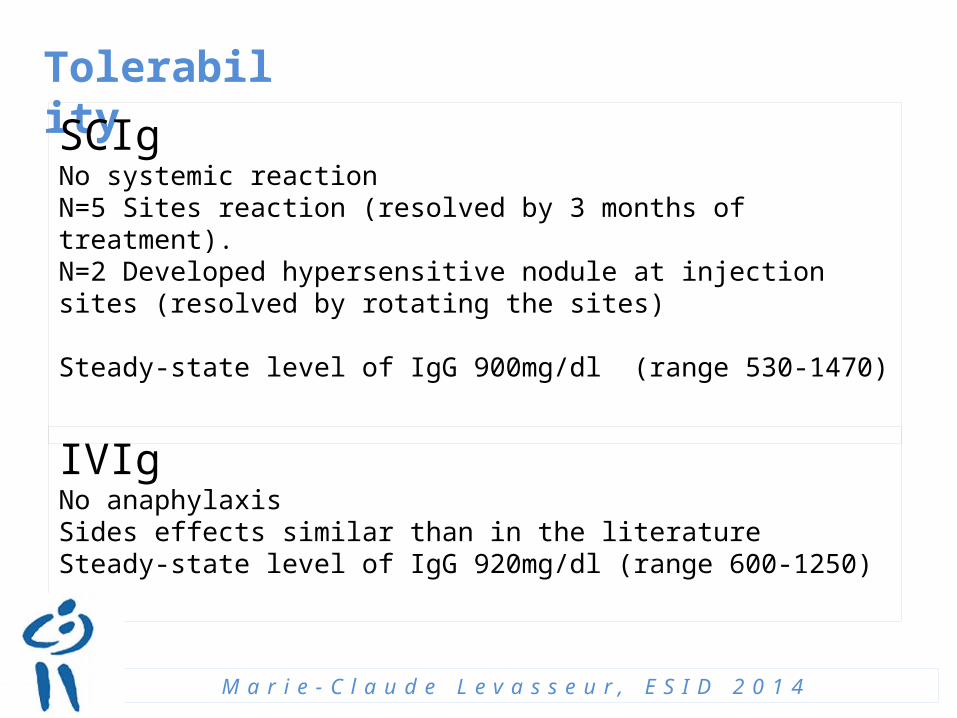
Tolerability
SCIg No systemic reactionN=5 Sites reaction (resolved by 3 months of treatment).N=2 Developed hypersensitive nodule at injection sites (resolved by rotating the sites)
Steady-state level of IgG 900mg/dl (range 530-1470)
IVIgNo anaphylaxisSides effects similar than in the literatureSteady-state level of IgG 920mg/dl (range 600-1250)
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

Together, only a total of 13 patients switched from SCIg to IVIg
Reasons noted:
• Change in family situation (parental medical difficulties)• Pain associated with frequent injection• Compliance issues
Result
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4
Definition of compliance: “the extend to which a person’s behaviour coincides with medical advice”.
North America> 50% of patient with chronic disease don’t respect their medical prescription of treatment
>80% search for health information on the web
With SCIg therapy, how can we measure compliance/adherence?
• Log sheet verification?• Patient questionnaire?• IgG monitoring?
Let the patient decide what’s best for him at this point in his life
Analysis of compliance
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

“Patient partner”
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

Analysis of compliance
SCIg Poor compliance was noted in 3 pts (6%) in the “switch cohort” and 7 pts (9%) in the new cohort
• monoparental families and poor supervision in pre-teenagers and teenagers• attention-deficit disorder in parents or child• parental stress regarding the SCIg modality
We proposed to switch back to IVIg . Two of these returned to SCIg treatment 2 and 23 months later without any relapse of poor compliance.
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

Analysis of patient’s behavior when the choice was offered
Stress in relation to the need to make a choice
• Seems to be more important with the patient from the new cohort, (30%) mention “mild stress”.
Despite this stress, patients mentioned that they were reassured by being offered the possibility of changing treatment modality as they wanted.
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4
Discussion
• 5/6 patient showed a perfect compliance
• Demonstrate that the medical “a priori” can be false.
• Providing patients with the opportunity to be responsible for their own health could be a factor that diminishes poor compliance.
• Patients seems to have strong preference for SCIg, suggestion association with better quality of life (QoL).
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

Discussion
• IVIg can not be delivered at home in Quebec
• Hospital-administered Ig may be unpleasant (set-up, waiting, comfort)
Because SCIg is free in our center, the cost of material was offset by the saving in loss of productivity and cost of travel.
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

Conclusion
• We believe there are no ideal candidates for SCIg and IVIg therapy
• Patients is a partner
• Giving the choice is a feasible, safe and efficient strategy.
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4

REFERENCES
1. Ochs HD, Gupta S, Kiessling P, Nicolay U, Berger M, Subcutaneous Ig GSG. Safety and efficacy of self-administrered subcutaneous immunoglobulin in patient with primary immunodeficiency diseases. J Clin Immunol. 2006;26(3):265-73
2. Berger M Choices in IgG remplacement therapy for primary immune deficiency diseases:subcutaneous IgG vs. Intravenous IgG and selecting and optimal dose. Curr Opin Allergy Clin Immunol.2011;11(6)532-8
3. Chapel HM, Spickett GP, Ericson D, Engl W, Eibls MM, Bjorkander J. The comparison of the efficacy and safety of intravenous versus subcutaneous immunoglobulin replacement therapy. J Clin Immunol. 2000;20(2):94-100.
4. Ballow M.mImmunoglobulin therapy:methods of delivery. The J of allergy and clin immunol. 2008;122(5):1038-9
5. Haddad E, Bames d, Kafal A. Home therapy with subcutaneous immunoglobulins for patients wit primary immunodeficiency disease. Transfusion and apheresis science:official j of the World Apher Asso : official j of the Eur Soc for Haemapheresis 2012;46(3):315-21.
6. Wasserman RL. Progress in gammaglobulin therapy for immunodeficiency: from subcutaneous to intravenous infusion and back again. J Clin Immunol. 2012;32(6):1153-64

MERCI!
Collaborators:
• Kathryn Samaan
• Hugo Chapdelaine
• Anne Des Roches
• Helene Decaluwe
• Elie Haddad
M a r i e - C l a u d e L e v a s s e u r , E S I D 2 0 1 4